
Abstract
Purpose
Multi-stranded hamstring-tendon autografts have been widely used for anterior cruciate ligament reconstruction (ACLR) surgeries. Recently, smaller diameter hamstring autografts have been linked with the risk of failure or graft rupture. However, there is limited evidence concerning the optimal diameter of the hamstring autografts for ACLR. The current systematic review and meta-analysis analysed the association of ACLR failure with the diameter of hamstring autografts.
Methods
A systematic search of three major scientific databases (Pubmed, EMBASE, and Cochrane library) was conducted to identify studies that presented ACLR failure-related outcomes with different diameters of hamstring autografts. The pooled data from the included studies were analysed to investigate the association between ACLR failure and the cut-off diameters of 6, 7, 8, and 9 mm. Subgroup analyses based on the level of evidence and follow-up duration were also performed at each cut-off diameter.
Results
Of the 2282 studies screened, 16 reported failure rates with hamstring autografts of different diameters, 15 of which were included in the meta-analysis. A graft diameter ≥ 7 mm was associated with significantly lower ACLR failure rates than a graft diameter < 7 mm (p = 0.005), based on pooled data of 19,799 cases. Age < 20 years and higher physical activity were associated with significantly higher ACLR failure rates.
Conclusion
The current systematic review suggests that the hamstring graft diameter for ACLR should be more than 7 mm considering the significantly higher failure rates with graft diameters less than 7 mm.
Level of evidence
Level IV
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Hamstring tendons are among the most commonly used autografts for anterior cruciate ligament reconstruction (ACLR) surgeries [21]. The easy harvesting techniques, lesser graft site morbidity, and favourable functional outcomes are the significant factors contributing to their widespread use in ACLR [30]. However, hamstring autografts have been reported to carry a higher risk of failure or rupture, especially in younger populations, than quadriceps and patellar tendon autografts [19, 27]. Recently, hamstring autografts with a smaller diameter have been linked with the risk of failure or graft rupture [2, 5, 8, 14,15,16, 22,23,24,25, 28, 33,34,35]. Subsequently, some authors have advocated increasing the number of strands to increase the graft width [5, 18, 20]. Few previous reviews attempted to address graft size concerns, but those were based on limited clinical evidence and included only a few comparison groups [6, 11, 17, 31].
The current systematic review and meta-analysis aimed to analyse the risk of ACLR failure secondary to graft rupture with hamstring autografts at cut-off graft diameters of 6, 7, 8, and 9 mm. This analysis intends to propose a safe cut-off for the optimal diameter of hamstring autografts for ACLR. Currently, the evidence concerning the safety of hamstring autografts for ACLR is limited. Due to the limited number of studies and patients included in the previous reviews, a larger volume-based analysis is desirable for more concrete recommendations. Due to variations of the graft diameters among individuals and populations, different graft diameters’ safety needs to be investigated. The current systematic review and meta-analysis attempt to address the limitations of the previous reviews by involving a larger number of studies, a markedly larger volume of patients undergoing ACLR, and inclusion of level II studies that were not included in the previous reviews.
Materials and methods
A systematic review and meta-analysis to address the above-mentioned purpose were conducted according to the stipulated guidelines in the Cochrane handbook of systematic review and meta-analysis of interventions.
Searching strategy
Following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines, two authors independently searched the Pubmed, EMBASE, and Cochrane library databases on May 5, 2020, using the following specific keywords: anterior cruciate ligament, ACL, graft, tendon, hamstring, revision, failure, size, diameter, and dimensions. A secondary manual search was done by scrutinising bibliographies of publications identified for additional articles. The Cochrane Central Register of Controlled Trials (CENTRAL) was searched to identify any unpublished or ongoing trials. The search strategy was not restricted to the year of publication or language. The detailed search strategy is described in Online Resource 1.
Inclusion and exclusion criteria
Titles and abstracts of all search results were screened to include the studies that were relevant to the risk of ACLR failure secondary to graft rupture with hamstring autografts, and full texts of the selected studies were thoroughly reviewed by two reviewers. ACLR failure was defined as at least one of the following outcomes:
-
(1)
Revision ACLR surgery secondary to the graft rupture;
-
(2)
radiological evidence of graft rupture during the follow-up period;
-
(3)
an absolute displacement of > 10 mm assessed through the KT1000 arthrometer [1];
-
(4)
anterior tibial displacement of ≥ 3 mm side to side difference compared to healthy knee [1];
-
(5)
a positive pivot shift test graded + 2 or + 3 in comparison to the healthy knee, with or without knee pain or inflammation [26];
-
(6)
Clinical assessment suggestive of International Knee Documentation Committee (IKDC) grade C or D [7];
Only studies that had a minimum mean follow-up of 1 year were included. Editorials, expert opinions, letters, abstracts-only publications, reviews, case reports, biomechanical and cadaveric studies, animal studies, technical tips, and notes were excluded. Studies that analysed the ACLR failure secondary to factors other than graft rupture, like tunnels malposition and malalignment, inability to return to desired activity level, and postoperative complications such as infection and stiffness, etc. were also excluded.
Data extraction
The primary author’s name, year of publication, study design, level of evidence, the smallest and largest diameter of the hamstring grafts used, the sample size of the ACLR performed using hamstring autografts, mean age, male–female distribution, and the mean follow-up duration of each of the included studies were filled in a prespecified form. The discrepancies in data charting were settled through the reevaluation of the concerned studies and mutual discussion.
Quality and risk of bias assessment
In addition to recording the design and level of evidence of the included studies, the risk of bias assessment was separately performed by two authors. Conflicting opinions were settled through discussion and mutual consensus. The Newcastle–Ottawa Quality Assessment Scale was considered for evaluating non-randomised studies [40], and the Cochrane Risk of Bias Tool for Randomized Controlled Trials was considered for randomised studies [36].
Statistical analysis
Review Manager (RevMan, Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) was used to perform a meta-analysis of the included studies. The dichotomous data were analysed using the combined estimates of the risk ratios (RR) correlating the hamstring autograft diameter’s variation to the failure of ACLR at the aforementioned cut-off values of hamstring autograft diameter. The continuous data were analysed using weighted mean differences (WMD) and 95% confidence intervals (95% CI) of the diameter of hamstring autografts in ACLR failure patients versus those belonging to the non-failure group. The dichotomous and continuous data related to the influence of factors other than the graft diameters on the ACLR failure were analysed in the same way. Studies with incomplete dichotomous or continuous data, not contributing to any of the above-stated analyses, were excluded from the meta-analysis. The comparison groups’ analyses, with more than 75% of heterogeneity, were not considered due to the included studies’ highly non-uniform results [12]. The fixed-effect model of analysis was used for non-heterogeneous comparisons, and the random-effect model of analysis was used for heterogeneous comparisons. Separate subgroup analyses for level II and level III–IV studies, and those with follow-up of < 2 years and ≥ 2 years were performed at each cut-off diameter. A p value of < 0.05 indicated statistical significance.
Results
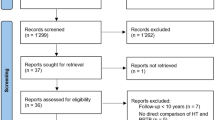
The searching strategy resulted in 2282 results (Pubmed: 954, Embase: 1184, Cochrane library: 134, others: 10). After excluding duplicates (n = 848), 1434 results were considered for the title and abstract screening. Title and abstract screening resulted in 16 relevant studies for the current meta-analysis (Table 1). Out of those 16 studies, one study (Andernord et al. [2]) had incomplete information for the performed quantitative analyses. The remaining 15 studies were considered for the meta-analysis (Fig. 1). All included studies were non-randomised ones. The risk of bias assessment using the Newcastle–Ottawa Quality Assessment Scale for the non-randomised studies suggested a good quality of the included studies with all studies scoring ≥ 7.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for the current meta-analysis
The detailed results of ACLR failure risk among the different dichotomous comparison groups are provided in Table 2.
Outcome meta-analysis
-
1.
Influence of graft diameter on ACLR failure: a statistically significant association (p = 0.0001) was observed between the smaller diameter grafts and ACLR failure after pooling the data of three eligible studies (Fig. 2) [33, 35, 42].
-
2.
Failure rates at different cut-off diameters: no statistically significant differences in ACLR failure rates were observed among the comparison groups at the cut-off diameters of 6, 8 and 9 mm. According to the follow-up duration and evidence level, the differences in ACLR failure rates at these cut-off diameters remained statistically insignificant upon subgrouping. Concerning the cut-off diameter of 7 mm, significantly higher ACLR failure rates were observed with graft diameter < 7 mm compared to graft diameter ≥ 7 mm (p = 0.005, Fig. 3a). The results remained statistically significant upon subgrouping of this comparison according to follow-up duration (≥ 2 years follow-up, p = 0.02), and < 2 years follow-up, p = 0.008), and among level III-IV studies (p = 0.007). However, no statistically significant differences were observed in level II studies subgroup.

Forest plot of continuous hamstring graft diameter data suggests a significant association between ACLR failure and smaller graft diameter

Forest plots of statistically significant associations of ACLR failure with dichotomously grouped variables. Significantly lower risk of ACLR failure was observed with hamstring graft diameter ≥ 7 mm (a), with age more than 20 years (b), and with lower activity levels (c)
Additionally, significantly higher ACLR failure rates were observed with graft diameter ≤ 7 mm compared to graft diameter > 7 mm upon subgrouping into level III–IV studies (p = 0.008), and studies with < 2 years follow-up (p = 0.03). The results of other comparisons at the cut-off diameter of 7 mm were statistically insignificant.
Other factors influencing ACLR outcomes
-
1.
Age and sex distribution: Analysis was performed at the cut-off ages of 20 years and 25 years as those were the commonly used cut-off ages among the included studies. At the cut-off age of 20 years, a significantly higher risk of ACLR failure was observed at age < 20 years compared to age ≥ 20 years (p = 0.01, Fig. 3b). No statistically significant association was found at the cut-off age of 25 years. Concerning the influence of gender on ACLR failures rates, a statistically significant association between gender and failure rates could not be established.
-
2.
Influence of activity level: For the impact of Tegner activity scores on ACLR failure rates, the analysis was inconclusive considering high heterogeneity levels (I2 = 90%). The dichotomous division of the patients into high/strenuous activity and low/mild to moderate activity levels suggested a statistically significant association of the higher activity levels to the ACLR failure (p = 0.003, Fig. 3c).
-
3.
Role of BMI (body mass index): a statistically significant association between ACLR failure and BMI at the cut-off level of 25 kg/m2 could not be established from the available data.
Discussion
The current analysis results suggest that the hamstring autograft diameter should be > 7 mm for the ACLR surgeries. The failure rates with a graft diameter of < 7 mm were significantly higher than those with a graft diameter ≥ 7 mm. However, significantly higher ACLR failure rates were observed with ≤ 7 mm as well < 7 mm graft diameters in the subgroup analyses of level III–IV studies, suggesting a preference towards graft diameter > 7 mm. Concerning the previously advocated cut-off diameter of 8 mm [6, 11], the current analysis could not find a statistically significant association at this cut-off diameter. There is limited and non-supportive evidence for graft diameters ≤ 6 mm. The present analysis results support the previous meta-analysis findings by Kang et al. [17], which suggested the cut-off diameter of 7 mm for the hamstring autograft-based ACLR. Their conclusions were based on pooled data from 1648 cases and had a statistical significance at p = 0.03. However, the present comparison included a larger volume of data from 19,799 cases and still found statistical significance at p = 0.005. This comparison further strengthens the applicability of the cut-off diameter of 7 mm for hamstring autograft selection. The subgroup analyses considering the differences in the evidence level, and follow-up durations helped in a more comprehensive analysis. The other reviews that investigated the graft diameter for ACLR were based on limited evidence. While the review by Rahardja et al. [31], predicted the risk of ACLR failure with smaller autografts, it could not reach substantial conclusions owing to low-quality evidence. The current analysis results differ from the findings of the systematic review by Conte et al. [6], and the narrative review by Figueroa et al. [11]. Conte et al. [6], concluded that a graft diameter ≤ 8 mm had a 6.8 times higher risk of failure than a graft diameter > 8 mm. However, their review was based on only three studies (two level-III studies and one level-IV study). Two of their included studies had “zero” failures with a graft diameter > 8 mm. Thus, their favourable conclusions were most likely skewed toward a graft diameter > 8 mm. The review by Figueroa et al. [11] had quoted the same finding. The current analysis can be considered more comprehensive because it is based on a larger cohort of evidence that analysed five level-II studies, eight level-III studies, and three level-IV studies. Moreover, the data volume for the analysis of 8 and 7 mm cut-off diameters in previous studies were markedly smaller than the present analysis. The systematic review by Kang et al. [17] had maintained a follow-up threshold of 2 years. However, in the current analysis, studies with a minimum mean follow-up of 1 year were included considering that the highest risk of rupture is during the first 12 months after ACLR [32]. This time frame includes the stage of revascularisation when the graft is weakest; by the end of this period, patients usually return to their pre-injury activities [10]. The follow-up duration was not considered in the eligibility criteria in the review by Rahardja et al. [31].
All but one of the included studies contributed to the one or more segments of the current meta-analysis. The study by Andernord et al. [2], due to non-availability of the variance related data of their results, and subgroup sample sizes, could not be added to the pooled analysis. The authors had analysed ACLR failure due to graft rupture among 4882 patients undergoing hamstring autograft-based ACLR. However, no statistically significant differences were observed at different cut-off diameters of the autograft. Their research provided an important finding that metal interference screw fixation of a semitendinosus tendon autograft on the tibia had a significantly reduced risk of early revision surgery. Two of the included studies described the proportions of the different graft diameters in failure cases and matched controls with a fixed case–control ratio of 1:3 [33, 35]. The studies concluded that the likelihood of graft rupture decreases with an increase in graft diameter. In the current analysis, these studies were analysed based on the continuous data related to the mean graft diameters in failure and matched control groups. While these studies examined large sample sizes, graft failure’s actual incidence could not be predicted due to a lack of continuous cohort-based data.
The biomechanical basis for smaller grafts’ failures is their mismatch with the ultimate failure load and stiffness of the native anterior cruciate ligament (ACL). The change in graft strength with a 1-mm increase in its diameter is most remarkable from 6 to 7 mm [3]. This change in strength correlates well with a higher failure rate in grafts with diameters < 7 mm. Although the 8- and 9-mm diameter grafts would have higher tensile strengths than the 7-mm diameter grafts, the clinical applicability of 7 mm diameter autografts is not ruled out. The ultimate load to failure for the native ACL lies between 1725 and 2160 N, and that of 7-mm diameter hamstring graft is 3263 ± 677 N.
Among the studies that presented the graft diameter distribution information, the 8-mm diameter graft was most prevalent. The 7 mm graft was either the second or third most common graft diameter in most studies (Fig. 4) [22, 24, 28, 34, 38, 41]. The graft diameters less than 7 mm and more than 9 mm represented the extremes and were least prevalent. The current meta-analysis supports the clinical applicability of graft diameters > 7 mm.

Percentage distribution of graft diameters among studies analysing the impact of graft diameter on ACLR outcomes
In addition to graft diameter, surgeons should also consider various other factors that can influence ACLR outcomes. A smaller graft diameter and such contributing factors can further add to the risk of ACLR failure. Young age, male gender, and high activity sports participation are the crucial factors contributing to a higher risk of graft rupture [4, 39, 42]. The evidence supporting shorter height, female patients, especially those with small diameter grafts, lower body weight, or BMI as risk factors for ACLR failure is very limited [22, 28, 39]. Significant association of ACLR failure with age < 20 years and higher physical activity levels was observed in the present analysis. However, a statistically significant association of ACLR failure with gender and BMI could not be established. Besides these patient-related factors, surgeons’ expertise and volume of ACLR surgeries, type of grafts, graft fixation techniques and devices, and return to sports timing can also impact the ACLR outcomes. The ACLR techniques used in the studies included in the present analysis were non-uniform. Among the nine studies presenting ACLR technique-related information, six studies had used anatomical ACLR technique [15, 16, 23, 38, 41, 42], one had used transtibial method [28], and two had used both anatomical and transtibial techniques [22, 24]. As far as the femoral fixation is concerned, suspensory fixation was used in six studies [16, 22, 24, 38, 41, 42], bioabsorbable screws were used in two studies [15, 23], bioabsorbable cross pins were used in one study [28], and varying fixation options were used in three studies [2, 34, 35]. For tibial fixation, interference screws with or without additional augmentation were used in six studies [15, 16, 22, 23, 38, 41], conventional screws were used in two [28, 42], and variable methods were used in four studies [2, 24, 34, 35]. The non-uniform and incomplete data on ACLR methods can impact the ACLR outcomes but is beyond the scope of the current analysis. The timing for return to sports varied between 6 and 12 months with three studies considering 6 months [16, 22, 24], one study considering seven months [23], three studies having variable criteria of 6–12 months [42], 8–12 months [15], and 9–12 months for the return to sports [41]. Again, this variable rehabilitation can contribute to the variation in ACLR outcomes, but a quantitative analysis could not be performed because of their lack of standardisation.
The most optimal ways to prevent graft-related complications are to anticipate them preoperatively. Preoperative magnetic resonance imaging and ultrasound have recently been used to predict hamstring graft diameters with reasonable accuracy [9, 37]. Ho et al. [13] found a positive correlation of the patient’s height and weight with graft diameter and derived separate equations for male and female patients.
When smaller hamstring autografts are predicted, surgeons have a choice to either opt for alternative autografts, such as patellar tendon and quadriceps or increase the strands of the hamstring autograft. Five strand autografts have been used for patients with a quadruple graft diameter < 7 mm, and have low revision rates (comparable to 8 mm quadruple grafts) [5, 18]. The allograft augmentation may appear as an attractive alternative for smaller grafts; however, the current evidence does not support that. Instead, some evidence suggests that allograft augmentation may increase failure rates [17, 29].
There are some limitations of the current analysis. First, due to the lack of randomised level I evidence, and only a few level II studies, most of the interpretations were based on level III and IV studies. It may be challenging to perform level I studies for ideal graft diameter for ACLR considering the ethical concerns, and individual variations in graft diameters. The subgroup analyses of level II studies did not reveal any significant graft diameter associations with ACLR failure at any of the cut-off diameters, which suggests that further quality evidence is required. Second, the graft diameter distribution among the groups was non-uniform throughout the studies with a smaller number of cases in the groups on both the extremes. This non-uniform distribution can potentially underestimate or overestimate the failure rates among these groups. Thirdly, other outcomes related to rehabilitation and return to the original activity level with different graft diameters cannot be predicted with the current analysis; only ACLR failure-related outcomes were analysed. Lastly, the influence of varying surgical techniques, surgeon’s technical expertise, the volume of qualified surgeons in centres performing ACLR, graft fixation methods, graft preparation methods, postoperative protocol, return to activity, anthropometric and demographic parameters, and other potential confounding variables cannot be controlled in this analysis. Some of the included studies are quite old, and their surgical techniques, fixation methods and surgeons’ expertise may differ considerably from the current scenario.
Therefore, further evidence in the form of prospective studies is needed to address these concerns. Nevertheless, the current study attempted to provide a more comprehensive analysis by pooling a larger volume of ACLR case data than previous reviews with a broader analysis at multiple cut-offs of graft diameter and several other factors influencing the ACLR outcomes. The concerns regarding the heterogeneous pooling of different levels of studies, and follow-up durations have been addressed by subgroup analysis at each cut-off diameter of hamstring autograft.
Conclusions
The current systematic review and meta-analysis predict that the hamstring graft diameter for ACLR should be more than 7 mm. Besides this, a threshold towards larger diameter grafts should be considered for patients younger than 20 years of age and those involved in strenuous activities.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- ACLR:
-
Anterior cruciate ligament reconstruction
- BMI:
-
Body mass index
- CENTRAL:
-
Cochrane Central Register of Controlled Trials
- CI:
-
Confidence interval
- CS:
-
Case series
- IKDC:
-
International Knee Documentation Committee
- NR:
-
Not reported
- PCC:
-
Prospective case–control study
- PCS:
-
Prospective cohort study
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- RCC:
-
Retrospective case–control study
- RCS:
-
Retrospective cohort study
- RR:
-
Risk ratio
- WMD:
-
Weighted mean difference
References
Alford JW, Bach BR Jr (2005) Arthrometric aspects of anterior cruciate ligament surgery before and after reconstruction with patellar tendon grafts. Tech Orthop 20(4):421–438
Andernord D, Björnsson H, Petzold M, Eriksson BI, Forssblad M, Karlsson J et al (2014) Surgical predictors of early revision surgery after anterior cruciate ligament reconstruction: results from the Swedish national knee ligament register on 13,102 patients. Am J Sports Med 42(7):1574–1582
Boniello MR, Schwingler PM, Bonner JM, Robinson SP, Cotter A, Bonner KF (2015) Impact of hamstring graft diameter on tendon strength: a biomechanical study. Arthroscopy 31(6):1084–1090
Rahardja R, Zhu M, Love H, Clatworthy MG, Monk AP, Young SW (2020) Rates of revision and surgeon-reported graft rupture following ACL reconstruction: early results from the New Zealand ACL Registry. Knee Surg Sports TraumatolArthrosc 28(7):2194–2202
Calvo R, Figueroa D, Figueroa F, Vaisman A, Schmidt-Hebbel A, Morales N et al (2017) Five-strand hamstring autograft versus quadruple hamstring autograft with graft diameters 8.0 millimeters or more in anterior cruciate ligament reconstruction: clinical outcomes with a minimum 2-year follow-up. Arthroscopy 33(5):1007–1013
Conte EJ, Hyatt AE, Gatt CJ Jr, Dhawan A (2014) Hamstring autograft size can be predicted and is a potential risk factor for anterior cruciate ligament reconstruction failure. Arthroscopy 30(7):882–890
Grassi A, Kim C, MarcheggianiMuccioli GM, Zaffagnini S, Amendola A (2017) What is the mid-term failure rate of revision ACL reconstruction? A systematic review. ClinOrthopRelat Res 475(10):2484–2499
Duerr RA, Garvey KD, Ackermann J, Matzkin EG (2019) Influence of graft diameter on patient reported outcomes after hamstring autograft anterior cruciate ligament reconstruction. Orthop Rev (Pavia) 11(3):8178
Leiter J, Elkurbo M, McRae S, Chiu J, Froese W, MacDonald P (2017) Using pre-operative MRI to predict intraoperative hamstring graft size for anterior cruciate ligament reconstruction. Knee Surg Sports TraumatolArthrosc 25(1):229–235
Falconiero RP, DiStefano VJ, Cook TM (1998) Revascularization and ligamentization of autogenous anterior cruciate ligament grafts in humans. Arthroscopy 14(2):197–205
Figueroa F, Figueroa D, Espregueira-Mendes J (2018) Hamstring autograft size importance in anterior cruciate ligament repair surgery. EFORT Open Rev 3(3):93–97
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Ho SW, Tan TJ, Lee KT (2016) Role of anthropometric data in the prediction of 4-stranded hamstring graft size in anterior cruciate ligament reconstruction. ActaOrthopBelg 82(1):72–77
Inderhaug E, Drogset JO, Lygre SHL, Gifstad T (2020) No effect of graft size or body mass index on risk of revision after ACL reconstruction using hamstrings autograft. Knee Surg Sports TraumatolArthrosc 28(3):707–713
Jurkonis R, Gudas R, Smailys A (2018) Influence of graft diameter on functional outcomes after anterior cruciate ligament reconstruction: a prospective study with a 1-year follow-up. Med SciMonit 24:4339–4345
Kamien PM, Hydrick JM, Replogle WH, Go LT, Barrett GR (2013) Age, graft size, and Tegner activity level as predictors of failure in anterior cruciate ligament reconstruction with hamstring autograft. Am J Sports Med 41(8):1808–1812
Kang H, Dong C, Wang F (2019) Small hamstring autograft is defined by a cut-off diameter of 7 mm and not recommended with allograft augmentation in single-bundle ACL reconstruction. Knee Surg Sports TraumatolArthrosc 27(11):3650–3659
Krishna L, Tan XY, Wong FKL, Toh SJ (2018) A 5-strand hamstring autograft achieves outcomes comparable to those of a 4-strand hamstring autograft with a graft diameter of 8 mm or more in anterior cruciate ligament reconstruction. Orthop J Sports Med 6(3):2325967118760815
Laboute E, James-Belin E, Puig PL, Trouve P, Verhaeghe E (2018) Graft failure is more frequent after hamstring than patellar tendon autograft. Knee Surg Sports TraumatolArthrosc 26(12):3537–3546
Walczak BE, Hetzel SJ, Akoh CC, Baer GS (2019) Intraoperative conversion to five-strand hamstring autograft configuration significantly increases anterior cruciate ligament graft diameter independent of patient characteristics. J Knee Surg. https://doi.org/10.1055/s-0039-3400955
Vinagre G, Kennedy NI, Chahla J, Cinque ME, Hussain ZB, Olesen ML et al (2017) Hamstring graft preparation techniques for anterior cruciate ligament reconstruction. Arthrosc Tech 6(6):e2079–e2084
Magnussen RA, Lawrence JT, West RL, Toth AP, Taylor DC, Garrett WE (2012) Graft size and patient age are predictors of early revision after anterior cruciate ligament reconstruction with hamstring autograft. Arthroscopy 28(4):526–531
Marchand JB, Ruiz N, Coupry A, Bowen M, Robert H (2016) Do graft diameter or patient age influence the results of ACL reconstruction? Knee Surg Sports TraumatolArthrosc 24(9):2998–3004
Mariscalco MW, Flanigan DC, Mitchell J, Pedroza AD, Jones MH, Andrish JT et al (2013) The influence of hamstring autograft size on patient-reported outcomes and risk of revision after anterior cruciate ligament reconstruction: a Multicenter Orthopaedic Outcomes Network (MOON) Cohort Study. Arthroscopy 29(12):1948–1953
Murgier J, Powell A, Young S, Clatworthy M (2020) Effectiveness of thicker hamstring or patella tendon grafts to reduce graft failure rate in anterior cruciate ligament reconstruction in young patients. Knee Surg Sports TraumatolArthrosc. https://doi.org/10.1007/s00167-020-05973-y
Samitier G, Marcano AI, Alentorn-Geli E, Cugat R, Farmer KW, Moser MW (2015) Failure of anterior cruciate ligament reconstruction. Arch Bone JtSurg 3(4):220–240
Nyland J, Collis P, Huffstutler A, Sachdeva S, Spears JR, Greene J et al (2020) Quadriceps tendon autograft ACL reconstruction has less pivot shift laxity and lower failure rates than hamstring tendon autografts. Knee Surg Sports TraumatolArthrosc 28(2):509–518
Park SY, Oh H, Park S, Lee JH, Lee SH, Yoon KH (2013) Factors predicting hamstring tendon autograft diameters and resulting failure rates after anterior cruciate ligament reconstruction. Knee Surg Sports TraumatolArthrosc 21(5):1111–1118
Pennock AT, Ho B, Parvanta K, Edmonds EW, Chambers HG, Roocroft JH et al (2017) Does allograft augmentation of small-diameter hamstring autograft ACL grafts reduce the incidence of graft retear? Am J Sports Med 45(2):334–338
Shaerf DA, Pastides PS, Sarraf KM, Willis-Owen CA (2014) Anterior cruciate ligament reconstruction best practice: a review of graft choice. World J Orthop 5(1):23–29
Rahardja R, Zhu M, Love H, Clatworthy MG, Monk AP, Young SW (2020) Factors associated with revision following anterior cruciate ligament reconstruction: a systematic review of registry data. Knee 27(2):287–299
Salmon L, Russell V, Musgrove T, Pinczewski L, Refshauge K (2005) Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthroscopy 21(8):948–957
Snaebjörnsson T, HamrinSenorski E, Ayeni OR, Alentorn-Geli E, Krupic F, Norberg F et al (2017) Graft diameter as a predictor for revision anterior cruciate ligament reconstruction and KOOS and EQ-5D values: a cohort study from the swedish national knee ligament register based on 2240 patients. Am J Sports Med 45(9):2092–2097
Snaebjörnsson T, Hamrin-Senorski E, Svantesson E, Karlsson L, Engebretsen L, Karlsson J et al (2019) Graft diameter and graft type as predictors of anterior cruciate ligament revision: a cohort study including 18,425 patients from the Swedish and Norwegian national knee ligament registries. J Bone Joint Surg Am 101(20):1812–1820
Spragg L, Chen J, Mirzayan R, Love R, Maletis G (2016) The Effect of autologous hamstring graft diameter on the likelihood for revision of anterior cruciate ligament reconstruction. Am J Sports Med 44(6):1475–1481
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I et al (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366:l4898
Vardiabasis N, Mosier B, Walters J, Burgess A, Altman G, Akhavan S (2019) Can we accurately predict the quadruple hamstring graft diameter from preoperative magnetic resonance imaging? Orthop J Sports Med 7(3):2325967119834504
Wang J, Wang H, Lin L, Yu J (2019) Analysis of Influence Factor for the Failure of Anterior Cruciate Ligament Reconstruction. ZhongguoXiu Fu Chong Jian WaiKeZaZhi 33(12):1543–1546
Webster KE, Feller JA, Leigh WB, Richmond AK (2014) Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med 42(3):641–647
GA Wells, B Shea, D O'Connell, J Peterson, V Welch, M Losos, et al. (2020) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 6 May 2020.
Wernecke GC, Constantinidis A, Harris IA, Seeto BG, Chen DB, MacDessi SJ (2017) The diameter of single bundle, hamstring autograft does not significantly influence revision rate or clinical outcomes after anterior cruciate ligament reconstruction. Knee 24(5):1033–1038
Yamanashi Y, Mutsuzaki H, Iwai K, Ikeda K, Kinugasa T (2019) Failure risks in anatomic single-bundle anterior cruciate ligament reconstruction via the outside-in tunnel technique using a hamstring autograft. J Orthop 16(6):504–507
Funding
None.
Author information
Authors and Affiliations
Contributions
AZA contributed to the concept, design, data analysis, manuscript preparation, manuscript editing, and manuscript review. ASBN contributed with manuscript preparation, and manuscript editing. AK contributed with data acquisition, data analysis, manuscript preparation, manuscript editing, and manuscript review. MK contributed to data acquisition, data analysis. SD contributed to data acquisition, data analysis. SM contributed to the literature review, manuscript editing, and manuscript review.
Corresponding author
Ethics declarations
Conflict of interest
None of the authors has any conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Alomar, A.Z., Nasser, A.S.B., Kumar, A. et al. Hamstring graft diameter above 7 mm has a lower risk of failure following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 30, 288–297 (2022). https://doi.org/10.1007/s00167-021-06503-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06503-0