
Abstract
Purpose
Posterior tibial slope (PTS) represents an important risk factor for anterior cruciate ligament (ACL) graft failure, as seen in clinical studies. An anterior closing wedge osteotomy for slope reduction was performed to investigate the effect on ACL-graft forces and femoro-tibial kinematics in an ACL-deficient and ACL-reconstructed knee in a biomechanical setup.
Methods
Ten cadaveric knees with a relatively high native slope (mean ± SD): (slope 10° ± 1.4°, age 48.2 years ± 5.8) were selected based on prior CT measurements. A 10° anterior closing-wedge osteotomy was fixed with an external fixator in the ACL-deficient and ACL-reconstructed knee (quadruple Semi-T/Gracilis-allograft). Each condition was randomly tested with both the native tibial slope and the post-osteotomy reduced slope. Axial loads (200 N, 400 N), anterior tibial draw (134 N), and combined loads were applied to the tibia while mounted on a free moving and rotating X–Y table. Throughout testing, 3D motion tracking captured anterior tibial translation (ATT) and internal tibial rotation (ITR). Change of forces on the reconstructed ACL-graft (via an attached load-cell) were recorded, as well.
Results
ATT was significantly decreased after slope reduction in the ACL-deficient knee by 4.3 mm ± 3.6 (p < 0.001) at 200 N and 6.2 mm ± 4.3 (p < 0.001) at 400N of axial load. An increase of ITR of 2.3° ±2.8 (p < 0.001) at 200 N and by 4.0° ±4.1 (p < 0.001) at 400 N was observed after the osteotomy. In the ACL-reconstructed knee, ACL-graft forces decreased after slope reduction osteotomy by a mean of 14.7 N ± 9.8 (p < 0.001) at 200 N and 33.8 N ± 16.3 (p < 0.001) at 400N axial load, which equaled a relative decrease by a mean of 17.0% (SD ± 9.8%), and 33.1% (SD ± 18.1%), respectively. ATT and ITR were not significantly changed in the ACL-reconstructed knee. Testing of a tibial anterior drawing force in the ACL-deficient knee led to a significantly increased ATT by 2.7 mm ± 3.6 (p < 0.001) after the osteotomy. The ACL-reconstructed knee did not show a significant change (n.s.) in ATT after the osteotomy. However, ACL-graft forces detected a significant increase by 13.0 N ± 8.3 (p < 0.001) after the osteotomy with a tibial anterior drawer force, whereas the additional axial loading reduced this difference due to the osteotomy (5.3 N ± 12.6 (n.s.)).
Conclusions
Slope-reducing osteotomy decreased anterior tibial translation in the ACL-deficient and ACL-reconstructed knee under axial load, while internal rotation of the tibia increased in the ACL-deficient status after osteotomy. Especially in ACL revision surgery, the osteotomy protects the reconstructed ACL with significantly lower forces on the graft under axial load.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Reconstruction of the anterior cruciate ligament (ACL) leads to good functional outcome in the vast majority of patients; however, a certain number of patients have to undergo revision or even multiple-revision ACL reconstructions secondary to graft failure [16, 19, 34]. It is well accepted that revision ACL reconstruction is associated with worse functional outcomes and higher failure rates compared to primary ACL reconstruction [12, 36]. Aside from well-known factors such as technical errors, repeat trauma, and biological reasons, considerably less attention has been paid to anatomic factors such as the sagittal inclination of the tibial plateau, also referred to as the posterior tibial slope (PTS) [30]. Biomechanically, an increased PTS produces an anteriorly directed shear force when a compressive load is applied to the knee joint, resulting in anterior tibial translation (ATT) [5, 11, 21, 28]. Since the ACL is the primary restraint against ATT, the PTS may, therefore, affect the in situ forces of the native and reconstructed ACL [7]. Based on clinical studies, there is growing evidence that an increased PTS has a negative effect on knee stability after ACL reconstruction and represents an important risk factor for graft failure [2, 17, 18, 27, 33]. Therefore, an anterior closing wedge tibial osteotomy has been suggested in the setting of revision ACL reconstruction to reduce the PTS and potentially lower forces in the ACL graft [3, 4, 29]. Whereas clinical studies have reported promising results, only few studies have analyzed the biomechanical effects of a slope-reducing osteotomy [4, 29, 31, 37]. Therefore, the biomechanical benefit on ACL grafts through correction of bony alignment is clinically relevant. The purpose of this study was, therefore, to investigate the effect of the slope-reducing osteotomy on ACL-graft forces and femoro-tibial kinematics in an ACL-deficient and ACL-reconstructed knee in a biomechanical setup. Furthermore, the effects of slope-reducing osteotomy on anterior drawer and combined applied loads were also investigated. The hypotheses were that slope reduction results in (1) decreased anterior tibial translation, (2) decreased forces in the reconstructed ACL under axial loading, and (3) reduced anterior tibial translation within an anterior drawer.
Materials and methods
Specimen
This study was reported to the institutional review board (IRB) of the University of Connecticut, Farmington, CT, USA (IRB Mech-18-1). It was documented that de-identified specimens do not constitute human subjects research, and no further IRB approval was required. A total of 25 fresh-frozen cadaveric knees were CT-scanned and measured for their native slope, which was calculated as an average between lateral and medial tibial slope versus the proximal tibial shaft [14]. Out of these, ten specimens with the highest native tibial slope were selected for the study group (average, standard deviation): posterior tibial slope: (10° ± 1.4, age 48.2 year ± 5.8, bone mass density 0.817 g/cm2 ± 0.266, weight 154 lbs ± 55.4, ratio male/female 1/1, and right/left 4/6). Prior to this, two additional specimens were used for piloting of the setup and sample calculation. Ten specimens were obtained from Medcure (MedCure, Inc., Cumberland, RI, USA) and 15 from Science Care (Science Care, Phoenix, AZ, USA).
Specimen preparation
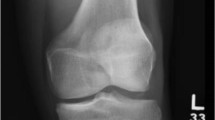
Cadavers were thawed overnight at room temperature for 24 h prior to testing. They were inspected via CT scan to confirm only mild to moderate degenerative changes and confirm ligamentous integrity. The skin and soft tissue were kept completely intact 10 cm proximal and 10 cm distal to the joint line. The femur, tibia, and fibula were dissected and potted in a polyvinyl chloride (PVC) pipe using plaster of Paris. With radiographic C-arm control, two Steinman pins were placed in the proximal tibia, 15 mm distal to the tibial joint line and parallel to the articular surface to later control the tibial slope. Two more pins were placed into the shaft distal to the planned osteotomy and an external fixator was mounted. At this point, an osteotomy of the tibial tubercle followed by a proximal anterior tibial wedge osteotomy was performed according to the technique described by Dejour [3]. An anterior osteotomy wedge of 10 degrees was marked by two parallel K-wires for the proximal cut and two parallel K-wires for the distal cut. The wedge was then cut out with an oscillating saw alongside the k-wires with C-arm control. Afterwards the tibial tubercle was refixed with transosseous sutures (Fig. 1). For testing in the pre-osteotomy status, a 3D printed 10° polylactide (PLA) wedge was inserted to ensure axial compression at higher axial loads [1].

Osteotomy procedure: the X-ray shows the 10° wedge of the anterior proximal tibia, which was cut and secured with an external fixator, which enabled closing of the osteotomy while the specimen fixed in the testing machine
The specimens were then placed into the testing fixture and the CT-measured native slope was verified by a 3D-digitizer (Microscribe, Immersion, Ca, USA) detecting the angle between the proximal Steinman-pin and the horizontal plane in the sagittal axis. At the time of anterior closing of the osteotomy, the slope was checked again using the external fixator pins. This allowed controlled manipulation of the tibial slope from native (pre-osteotomy) status to the post-osteotomy status and vice versa. For the purpose of the study, the specimens were tested pre- and post-osteotomy in the ACL-deficient and -reconstructed condition. Prior to this, we ran testing of the native ACL knee as an internal control.
The ACL was transected through a small anteromedial arthrotomy while the specimens were kept in the fixture. For reconstruction of the ACL, specimens were dismounted from the testing machine. The slope was adjusted to native status. A quadruple ACL allograft (LifeNet Health, Virginia Beach, VA) made from a doubled semitendinosus tendon and a doubled gracilis tendon was sutured, giving an averaged diameter of 8 mm. This technique, according to Fritsch et al., was adapted to ensure the same length and diameter in every specimen [9, 13]. The graft was then preloaded with 80N on the working bench for 20 min. The reconstruction of the ACL was performed, using Arthrex (Arthrex Inc., Naples, FL) techniques, as follows: The tibial tunnel was placed from the tibial osteotomy in an open technique through the existing arthrotomy, while the femoral tunnel was drilled with a RetroFlip-Cutter creating a socket of 15 mm. An anatomical femoral and tibial insertion was considered to be in between the anteromedial and posterolateral bundles. An adjustable loop suspension device (ACL TightRope) with a flipped button was used at the femoral site and checked with a C-arm radiograph. The tibial side of the graft limbs were then sutured together with baseball stitches over 15 mm by two #2 FiberWire [35]. After fixing the specimen in the testing mount, these sutures were hooked onto a load cell and tensioned to 80N of preload (Fig. 2). The arthrotomy and skin were closed with FiberWire #2 to prevent desiccation.

Left knee specimen: ACL-graft was fixed in line to the tibial drilling and hooked to a load cell, which was attached to the tibial potting. This allowed pre-tensioning and measurement of change of forces on the ACL-graft
Biomechanical testing
The testing apparatus consisted of a six degrees of freedom frame for the femoral fixation, locked in 30° of knee flexion and neutral rotation (Fig. 3). On the tibial side, the mounting fixture was attached to a rocker (balance). A displacement-controlled (0.2 mm/s) electro-mechanical actuator (Bimba, Monee, IL, USA) with an attached load cell (Omega, MA, USA) applied axial loads of 200N and 400N to the tibia versus the femur. The entire axial loading device was placed on a X–Y table, which allowed centering followed by de-centering and free rotation of the tibia versus the fixed femur when axial loads were applied. Additionally, a drawer cable was attached to the anterior side of the X–Ytable and fixed to an MTS machine actuator (Model 858, MTS Inc, Eden Prairie, MI, USA). During the simulated Lachman’s test (anterior drawer), tibial rotation was locked and a displacement-controlled anterior shift was applied with 0.5 mm/s to reach 134 N of anterior load. After release of the anterior load, the joint was centered again and an anterior shift (134 N) with combined axial loading (200N) was applied [11]. All four loading conditions were randomized. All loading conditions were repeated three times while all measurements were zeroed for every repeated testing sequence. The average of three measurements was taken for outcome analysis.

Biomechanical test setup: Specimen fixed with the tibia on a X–Ytable; axial compression device; MTS machine cable for anterior drawer; attached load-cell to the ACL-graft; 3D motion tracking cameras
Tibiofemoral kinematics were evaluated with an optical motion capture system (Vicon, Co, USA) using four digitizing cameras to evaluate the 3D movement (anterior tibial translation (ATT), internal tibial rotation (ITR)). Calibration (accuracy 0.01 mm for distance and 0.1° for degrees) was done before testing of each specimen with X–Y–Z vectors assigned according to the potted tibia on the X–Y table. Reflecting tripods were mounted on a Steinman pin at the anterior distal femur and at the proximal tibia. ATT and ITR were calculated as differences between start and end of every loading condition versus the femur using Vicon motion analysis software (ProCalc, Vicon, CO, USA).
A load cell (FUTEK, Irvine, CA) attached to the tibial sutures of the ACL graft measured load (N, accuracy 0.0001N) throughout testing in the reconstructed status. Prior to every loading condition, the preload of 80N on the ACL graft was maintained manually with a screw thread. When the osteotomy was closed, tension on the ACL graft was manually applied to reach again 80N of preload. (Fig. 4). For clinical relevance, all outcome measurements were given to one decimal.

Flow-chart of the testing procedure showing the different knee specimen status, different testing conditions, and outcome measurements
Statistical analysis
An a priori power analysis was conducted using load on ACL-graft values from repeated testing on two pilot specimens. The smallest difference observed was 11N difference in axial loading (200N) on ACL-graft tension at 10 degrees of osteotomy change. Assuming a standard deviation of 10 N, a sample size of at least 9 knees will provide 80% power to detect a 11-N difference at an alpha level of 0.05. A Shapiro–Wilk test was used to confirm normality of the data. Descriptive statistics were reported using mean, standard deviation (SD), and 95% Confidence Intervals (CI) when appropriate to characterize the study groups. To account for repeated measures, differences in ACL force, tibial translation, and rotation amplitude were examined using mixed linear regression. Pairwise comparisons of the pre- and post-osteotomy mean values were carried out for each condition (the ACL-deficient, and ACL-reconstructed knee) to determine the effect decreasing tibial slope on ACL force, tibial translation, and rotation amplitude. A comparison of the amount of change from pre- to post-osteotomy across the different ACL status (interaction) was carried out to determine whether decreasing tibial slope created a differential amount of change in tibial translation and rotation amplitude. Bonferroni adjusted p values were obtained to account for multiple comparisons. A p value less than 0.05 was considered statistically significant. All analyses were conducted with Stata 15 software (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
Results
Axial loading
ATT was significantly decreased after slope reduction in the ACL-deficient knee by (mean ± SD) 4.3 mm ± 3.6 (p < 0.001) at 200N and 6.2 mm ± 4.3 (p < 0.001) at 400N of axial load (Table 1). In the ACL-reconstructed knee, ATT decreased slightly, but not significantly, by 0.7mmm ± 0.7 mm (p = not significant (n.s.)) at 200N and by 1.4 mm ± 1.4 (n.s.) at 400N after the osteotomy. In the ACL-deficient status an increase of ITR of 2.3°± 2.8 at 200N (p < 0.001) and by 4.0° ± 4.1 at 400 N (p < 0.001) was observed after the osteotomy (Table 2). Furthermore, ITR was significantly increased by 1.9° ± 1.1 under sequential axial loading of 200N versus 400N (p < 0.001) in the ACL-deficient post-osteotomy status. After reconstruction of the ACL, ITR was not significantly affected due to the osteotomy by 0.1° ± 0.9 (n.s.) at 200N and 0.1° ± 1.6 (n.s.) at 400N of axial load. ACL-graft forces decreased after slope reduction osteotomy by a mean of 14.7 N ± 9.8 (p < 0.001) at 200N and 33.8 N ± 16.3 (p < 0.001) at 400 N axial load (Fig. 5). The relative changes of the resulting ACL graft forces decreased by a mean of 17.0% (SD ± 9.8%) and 33.1% (SD ± 18.1%), respectively, under axial load after slope correction.

Resulting ACL-graft force in N when joint was axially loaded at 200N and 400N was performed, pre- versus post-osteotomy, after ACL-graft pre-tensioning of 80N
Anterior drawer
ATT was significantly increased by 2.7 mm ± 3.6 (p < 0.001) after the osteotomy in the ACL-deficient status (Table 3). The ACL-reconstructed knee showed a slight increase of ATT by 1.1 mm ± 0.9 (n.s.) after the osteotomy. When adding an axial load to the anterior drawer, the change on ATT due to the osteotomy was 5.2 mm ± 1.2 (p < 0.001) in the ACL-deficient status. The reconstructed ACL did not show a significant change after the osteotomy when drawer and axial loading was combined, 1.4 mm ± 1.0 (n.s.). Force on the ACL-graft was significantly increased by 13.0 N ± 8.3 (p < 0.001) after the osteotomy when a simulated Lachman test was applied. When axial load was combined with anterior drawer, this effect was no longer significant, 5.3 N ± 12.6 (n.s.), (Fig. 6).

Resulting ACL-graft force (N) when anterior drawer (134N) with and without axial loading (200N) was performed, pre- versus post-osteotomy, after ACL-graft pre-tensioning of 80N
Discussion
The most important findings of the study were that a slope-reducing osteotomy by 10° significantly reduces ATT in the ACL-deficient, and slightly in the ACL-reconstructed knee. Furthermore, the slope reduction significantly reduced forces on the ACL-graft under axial joint loading. This proved our primary and secondary hypothesis and is consistent with recent literature [37]. On the other hand, when anterior drawer without axial loading was performed, an increase of force on the ACL-graft and an increased ATT after the osteotomy were observed. This was contrary to our third hypothesis.
In clinical studies, an increased PTS has been associated with an increased risk of non-contact ACL injury [32, 38], mucoid degeneration of the native ACL [15], higher pivot-shift grades in ACL-injured patients [25], increased incidence of tunnel widening after ACL reconstruction [26], and increased ATT in patients with intact grafts after ACL reconstruction [18]. Furthermore, there is growing evidence that an increased PTS is an important risk factor for graft failure after ACL reconstruction [2, 17, 27, 33]. Lee et al. found significantly greater PTS in patients with ACL-graft rupture compared to a matched control group of patients with intact ACL-grafts. The odds ratio of ACL-graft rupture in knees with a PTS greater than 12° was 4.52 [17]. For the purpose of our study specimens with an increased native slope were selected based on standardized CT measurements. The slope-reducing osteotomy of 10°, therefore, resulted in a hypothetically averaged slope of 0°.
The surgical technique used in this study represents a standard procedure performed through an anterior approach with additional tibia tunnel drilling. This technique did not affect the osteotomy [3]. In our study, we used an external fixator to change slopes pre- versus post-osteotomy when testing the three specimen conditions. However, in a clinical setting, this technique can easily be performed with one of the current locking plate systems. Several authors have suggested to combine revision ACL reconstruction with an anterior closing wedge tibial osteotomy to reduce the PTS and potentially decrease forces in the ACL-graft [3, 4, 29]. The theory of altering femoro-tibial kinematics through the change of slope has been proven in several biomechanical studies and mathematical models [1, 11, 23, 28, 37]. However, most studies focused on the effects of an increased tibial slope [1, 6, 10, 22]. Only few studies have investigated the effects of a slope-reducing osteotomy [31, 37].
The results of the study provide a biomechanical justification for a comprehensive approach to ACL reconstruction with a slope-reducing osteotomy. Especially in cases of a re-ruptured ACL, the indication for performing an osteotomy can be biomechanically underscored, even without concomitant reconstruction of the ACL. We demonstrated that a slope reduction leads to significantly lower forces on the ACL-graft and lower anterior tibial translation. This is in accordance with a recent study from Yamaguchi et al. They studied the effect of a 10° anterior closing wedge osteotomy in 11 fresh-frozen human knees between 0° and 50° of knee flexion in a robotic setup [37]. They found that the slope-reducing osteotomy resulted in significantly decreased native ACL force and significantly reduced anterior tibial translation under tibiofemoral compression alone and when combined with anterior force or valgus moment. This concept was described by Feucht et al. as an anteriorly directed shear force resulting in anterior translation of the tibia relative to the femur [7]. Several authors have demonstrated increased ACL strain or ACL rupture after axial tibiofemoral compression [8, 20, 24]. We used two different axial loading forces (200 N, 400 N), and our results suggest an equal linearity on femoro-tibial translation pre- versus post-osteotomy.
With this current biomechanical analysis, rotational stability did not significantly differ due to the osteotomy in the ACL-reconstructed knees. However, in the ACL-deficient state, the anterior closing wedge tibial osteotomy increased tibial internal rotation of the knee significantly under axial compression; however, the values were relatively low. We think this is mostly because of the changed ATT and winding of the posterior cruciate ligament in the ACL-deficient state. This is similar to prior results showing that internal tibial torque negated the benefit of a slope-reducing osteotomy in the native state [37]. Therefore, the results suggest the need to perform an osteotomy and an ACL reconstruction in a ACL-deficient knee. The osteotomy will decrease anterior tibial translation, but a reconstructed ACL or an additional antero-lateral extra-articular reconstruction such as a modified Lemaire would decrease rotational instability.
We additionally looked at the effect of slope reduction on a simulated Lachman’s test to observe any difference that could be made during a clinical evaluation. The anterior drawer without axial loading provided significantly more anterior tibial translation and significantly higher forces on ACL-graft after the osteotomy. The key to this observation is the resting/starting position of the tibia versus the femur. Slope reduction osteotomy by 10° led to a posteriorly directed movement of the proximal tibia around the femur condyles. This is because of the fixed femur shaft in 30° of flexion and the distal tibia shaft remaining in its vertical position on the table. The anterior drawer and axial loading protocol in this study was similar to Giffin et al. [11]. They investigated the effect of an increased slope and found a significant relative anterior shift of the tibial resting position throughout the range of knee motion, with a maximum anterior shift of 3.6 mm noted in full extension. This is similar to our findings regarding the resting knee position, but in the opposite direction, as they investigated increasing slope procedures. Therefore, in a clinical setup, one might find a Lachman’s test with a greater anterior translation after the osteotomy due to the altered resting/starting position of the knee.
There were several limitations to our study. The knee specimens were tested only in a static knee flexion of 30°. This value was chosen for three reasons. First, this value mostly reflects physiological gait while walking. Second, the anterior drawer is performed within this range. Third, the tibial load cell attached to the ACL-graft was mostly in line with the tibial tunnel drilling. Therefore, no distraction of the graft was observed on the tibial side. However, we cannot transfer our findings to other knee flexion angles. The specimens were tested first in the ACL-deficient status followed by the ACL-reconstructed status second. Although the slope adjustment (pre- versus post-osteotomy) was randomized within each status, the mandatory testing sequence might lead to a bias in chondral-bone surface changes and femoro-tibial sliding kinematics. Pre-tensioning of the graft (80 N) within the setup was time-consuming and elaborate. Although a standardized time-based protocol was followed, we observed differences throughout the grafts (80 N preload of ± 2 N). However, this did not affect the outcome measurement.
Since this study investigated the effect of a slope-reducing osteotomy on forces on ACL-graft and kinematics of the ACL-reconstructed and ACL-deficient knee under axial loading and anterior drawing conditions, the resulting forces on the ACL-graft could be measured directly by a tibial attached load cell. Our results show the importance of slope and axial joint compression in ACL reconstruction and underline the beneficial effect of a combined ACL reconstruction and slope-reducing osteotomy on graft forces and femoro-tibial kinematics.
Conclusions
Slope-reducing osteotomy reduced anterior tibial translation in the ACL-deficient and ACL-reconstructed knee under axial load, while internal rotation of the tibia increased in the deficient status after osteotomy. The osteotomy protected the reconstructed ACL with significantly lower forces on the graft.
References
Agneskirchner JD, Hurschler C, Stukenborg-Colsman C, Imhoff AB, Lobenhoffer P (2004) Effect of high tibial flexion osteotomy on cartilage pressure and joint kinematics: a biomechanical study in human cadaveric knees. Winner of the AGA-DonJoy Award 2004. Arch Orthop Trauma Surg 124:575–584
Christensen JJ, Krych AJ, Engasser WM, Vanhees MK, Collins MS, Dahm DL (2015) Lateral tibial posterior slope is increased in patients with early graft failure after anterior cruciate ligament reconstruction. Am J Sports Med 43:2510–2514
Dejour D, La Barbera G, Pasqualotto S, Valoroso M, Nover L, Reynolds R et al (2017) Sagittal plane corrections around the knee. J Knee Surg 30:736–745
Dejour D, Saffarini M, Demey G, Baverel L (2015) Tibial slope correction combined with second revision ACL produces good knee stability and prevents graft rupture. Knee Surg Sports Traumatol Arthrosc 23:2846–2852
Dejour H, Bonnin M (1994) Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J Bone Joint Surg Br 76:745–749
Fening SD, Kovacic J, Kambic H, McLean S, Scott J, Miniaci A (2008) The effects of modified posterior tibial slope on anterior cruciate ligament strain and knee kinematics: a human cadaveric study. J Knee Surg 21:205–211
Feucht MJ, Mauro CS, Brucker PU, Imhoff AB, Hinterwimmer S (2013) The role of the tibial slope in sustaining and treating anterior cruciate ligament injuries. Knee Surg Sports Traumatol Arthrosc 21:134–145
Fleming BC, Renstrom PA, Beynnon BD, Engstrom B, Peura GD, Badger GJ et al (2001) The effect of weightbearing and external loading on anterior cruciate ligament strain. J Biomech 34:163–170
Fritsch B, Figueroa F, Semay B (2017) Graft preparation technique to optimize hamstring graft diameter for anterior cruciate ligament reconstruction. Arthrosc Tech 6:e2169–e2175
Giffin JR, Stabile KJ, Zantop T, Vogrin TM, Woo SL, Harner CD (2007) Importance of tibial slope for stability of the posterior cruciate ligament deficient knee. Am J Sports Med 35:1443–1449
Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD (2004) Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med 32:376–382
Gifstad T, Drogset JO, Viset A, Grontvedt T, Hortemo GS (2013) Inferior results after revision ACL reconstructions: a comparison with primary ACL reconstructions. Knee Surg Sports Traumatol Arthrosc 21:2011–2018
Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC (1999) Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Jt Surg Am 81:549–557
Hashemi J, Chandrashekar N, Gill B, Beynnon BD, Slauterbeck JR, Schutt RC Jr et al (2008) The geometry of the tibial plateau and its influence on the biomechanics of the tibiofemoral joint. J Bone Jt Surg Am 90:2724–2734
Jung KH, Cho SD, Park KB, Youm YS (2012) Relation between mucoid degeneration of the anterior cruciate ligament and posterior tibial slope. Arthroscopy 28:502–506
Kvist J, Kartus J, Karlsson J, Forssblad M (2014) Results from the Swedish national anterior cruciate ligament register. Arthroscopy 30:803–810
Lee CC, Youm YS, Cho SD, Jung SH, Bae MH, Park SJ et al (2018) Does Posterior Tibial Slope Affect Graft Rupture Following ACL Reconstruction? Arthroscopy;10.1016/j.arthro.2018.01.058
Li Y, Hong L, Feng H, Wang Q, Zhang J, Song G et al (2014) Posterior tibial slope influences static anterior tibial translation in anterior cruciate ligament reconstruction: a minimum 2-year follow-up study. Am J Sports Med 42:927–933
Lind M, Lund B, Fauno P, Said S, Miller LL, Christiansen SE (2012) Medium to long-term follow-up after ACL revision. Knee Surg Sports Traumatol Arthrosc 20:166–172
Markolf KL, Bargar WL, Shoemaker SC, Amstutz HC (1981) The role of joint load in knee stability. J Bone Joint Surg Am 63:570–585
Marouane H, Shirazi-Adl A, Hashemi J (2015) Quantification of the role of tibial posterior slope in knee joint mechanics and ACL force in simulated gait. J Biomech 48:1899–1905
Martineau PA, Fening SD, Miniaci A (2010) Anterior opening wedge high tibial osteotomy: the effect of increasing posterior tibial slope on ligament strain. Can J Surg 53:261–267
McLean SG, Oh YK, Palmer ML, Lucey SM, Lucarelli DG, Ashton-Miller JA et al (2011) The relationship between anterior tibial acceleration, tibial slope, and ACL strain during a simulated jump landing task. J Bone Jt Surg Am 93:1310–1317
Meyer EG, Haut RC (2005) Excessive compression of the human tibio-femoral joint causes ACL rupture. J Biomech 38:2311–2316
Rahnemai-Azar AA, Abebe ES, Johnson P, Labrum J, Fu FH, Irrgang JJ et al (2017) Increased lateral tibial slope predicts high-grade rotatory knee laxity pre-operatively in ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 25:1170–1176
Sabzevari S, Rahnemai-Azar AA, Shaikh HS, Arner JW, Irrgang JJ, Fu FH (2017) Increased lateral tibial posterior slope is related to tibial tunnel widening after primary ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 25:3906–3913
Salmon LJ, Heath E, Akrawi H, Roe JP, Linklater J, Pinczewski LA (2018) 20-Year outcomes of anterior cruciate ligament reconstruction with hamstring tendon autograft: the catastrophic effect of age and posterior tibial slope. Am J Sports Med 46:531–543
Shelburne KB, Kim HJ, Sterett WI, Pandy MG (2011) Effect of posterior tibial slope on knee biomechanics during functional activity. J Orthop Res 29:223–231
Sonnery-Cottet B, Mogos S, Thaunat M, Archbold P, Fayard JM, Freychet B et al (2014) Proximal tibial anterior closing wedge osteotomy in repeat revision of anterior cruciate ligament reconstruction. Am J Sports Med 42:1873–1880
Southam BR, Colosimo AJ, Grawe B (2018) Underappreciated factors to consider in revision anterior cruciate ligament reconstruction: a current concepts review. Orthop J Sports Med 6:2325967117751689
Voos JE, Suero EM, Citak M, Petrigliano FP, Bosscher MR, Citak M et al (2012) Effect of tibial slope on the stability of the anterior cruciate ligament-deficient knee. Knee Surg Sports Traumatol Arthrosc 20:1626–1631
Wang HD, Gao SJ, Zhang YZ (2018) Comparison of clinical outcomes after anterior cruciate ligament reconstruction using a hybrid graft versus a hamstring autograft. Arthroscopy 34:1508–1516
Webb JM, Salmon LJ, Leclerc E, Pinczewski LA, Roe JP (2013) Posterior tibial slope and further anterior cruciate ligament injuries in the anterior cruciate ligament-reconstructed patient. Am J Sports Med 41:2800–2804
Wegrzyn J, Chouteau J, Philippot R, Fessy MH, Moyen B (2009) Repeat revision of anterior cruciate ligament reconstruction: a retrospective review of management and outcome of 10 patients with an average 3-year follow-up. Am J Sports Med 37:776–785
Williams RJ 3rd, Hyman J, Petrigliano F, Rozental T, Wickiewicz TL (2005) Anterior cruciate ligament reconstruction with a four-strand hamstring tendon autograft. Surgical technique. J Bone Jt Surg Am 87(Suppl 1):51–66
Wright RW, Gill CS, Chen L, Brophy RH, Matava MJ, Smith MV et al (2012) Outcome of revision anterior cruciate ligament reconstruction: a systematic review. J Bone Jt Surg Am 94:531–536
Yamaguchi KT, Cheung EC, Markolf KL, Boguszewski DV, Mathew J, Lama CJ et al (2018) Effects of anterior closing wedge tibial osteotomy on anterior cruciate ligament force and knee kinematics. Am J Sports Med 46:370–377
Zeng C, Cheng L, Wei J, Gao SG, Yang TB, Luo W et al (2014) The influence of the tibial plateau slopes on injury of the anterior cruciate ligament: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 22:53–65
Funding
The University of Connecticut Health Center/UConn Musculoskeletal Institute has received direct funding and material support from Arthrex Inc. (Naples. Fl.) The company had no influence on study design, data collection or interpretation of the results or the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors Imhoff FB, Mehl J, Comer B, Obopilwe E, Cote M, Feucht MJ, Wylie JD, declare that they have no conflict of interest. Author Imhoff AB is a consultant for Arthrosurface, Arthrex, and mediBayreuth. Author Arciero RA received an educational and institutional grant from Arthrex and is a consultant for Biorez. Author Beitzel K is a consultant for Arthrex. No-one of the above-mentioned authors has received personal financial support related to this study.
Ethical approval
This study was reported to the institutional review board (IRB) of the University of Connecticut, Farmington, CT, USA (IRB Mech-18-1). It was documented that de-identified specimens do not constitute human subjects research, and no further IRB approval was required.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Imhoff, F.B., Mehl, J., Comer, B.J. et al. Slope-reducing tibial osteotomy decreases ACL-graft forces and anterior tibial translation under axial load. Knee Surg Sports Traumatol Arthrosc 27, 3381–3389 (2019). https://doi.org/10.1007/s00167-019-05360-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05360-2