
Abstract
Purpose
The purpose of this systematic review and meta-analysis was to determine the influence of graft source (allograft vs. autograft) and configuration (single-limbed vs. double-limbed) on failure rate and disease-specific patient-reported outcome (Kujala score) after medial patellofemoral ligament (MPFL) reconstruction for patellar instability.
Methods
A systematic review of PubMed, Scopus, and the Cochrane Library was performed. A total of 31 studies met inclusion/exclusion criteria and were used to extract cohorts of patients who underwent ligament reconstruction with various allograft, autograft, single-limbed, and double-limbed constructs. Failure rates and postoperative improvements in Kujala scores were compared between cohorts using inverse-variance weighting in a random-effects analysis model and appropriate comparative statistical analyses (Chi-squared and independent samples t tests).
Results
A total of 1065 MPFL reconstructions were identified in 31 studies. Autograft reconstructions were associated with greater postoperative improvements in Kujala scores when compared to allograft (32.2 vs. 22.5, p < 0.001), but there was no difference in recurrent instability (5.7 vs. 6.7 %, p = 0.74). Double-limbed reconstructions were associated with both improved postoperative Kujala scores (37.8 vs. 31.6, p < 0.001) and lower failure rate (10.6 vs. 5.5 %, p = 0.030).
Conclusion
MPFL reconstructions should be performed using double-limbed graft configurations. While autograft tendon may be associated with higher patient-reported outcomes in the absence of associated connective tissue disorders or ligamentous laxity, patient factors and allograft processing techniques should be carefully considered when selecting an MPFL graft source, as revision rates were no different between graft sources.
Level of evidence
IV.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The medial patellofemoral ligament (MPFL) is the primary stabilizing soft tissue restraint to lateral patellar translation during early knee flexion (0–30°) [16, 20]. Acute patellar dislocation can result in significant intraarticular chondral injury and concurrent MPFL disruption in a large percentage of patients [18, 21]. In appropriately indicated patients with recurrent instability, MPFL reconstruction is an effective surgical treatment [7, 8, 10, 12, 19, 38, 48, 58, 68] with re-dislocation rates reported in less than 5 % of patients in some series [22, 39, 53]. While multiple surgical techniques for MPFL reconstruction have been described in the literature, there is no current consensus as to which technique or graft source optimizes clinical outcomes [32, 50, 60].
The ideal surgical construct and graft source for MPFL reconstruction is not widely accepted, due in part to the general lack of large prospective comparative studies. Few case series directly compare the use of autograft versus allograft sources nor single versus double-limb reconstruction techniques, thereby failing to identify best practices [9, 55, 65]. The purpose of this study was therefore to perform a systematic review and meta-analysis of existing literature in order to determine the influence of graft source (allograft vs. autograft) and configuration (single-limbed vs. double-limbed) on failure rate and disease-specific patient-reported outcomes (Anterior Knee Pain Scale, or “Kujala score”) after MPFL reconstruction. We hypothesized that autograft and double-limbed constructs would each result in improved clinical outcomes (defined by Kujala scores) and lower failure rates (defined by recurrent patellar instability).
Materials and methods
The methodology for meta-analysis of observational studies used in the current study has been widely utilized in the orthopaedic surgery literature [4, 24, 36, 42, 44, 45, 49]. A systematic review of PubMed, Scopus, and the Cochrane Library was performed (search date: 15 July 2014). Search terms were “patellar instability [AND] MPFL reconstruction” and subsequently expanded to “MPFL reconstruction”, along with associated MeSH terms.
Following the primary search, a title and abstract review was performed in accordance with the standard PRISMA checklist, to identify articles that contained relevant information. [34] If relevant information was identified, articles were then assessed in order to determine compliance with the following inclusion criteria:
-
1.
A minimum of 5 subjects (i.e. no case reports or small case series)
-
2.
Recurrent patellar instability as a reported outcome measure: defined by constituent studies as subluxation or dislocation. Determination of instability was heterogeneous across studies, but included both patient-reported episodes and confirmation by examination under anaesthesia.
-
3.
Minimum 1-year clinical follow-up
-
4.
Study published in either English or Mandarin language
Articles meeting these inclusion criteria were then manually reviewed in their entirety. Exclusion criteria were:
-
1.
Use of a synthetic ligament
-
2.
Concomitant surgical procedure (i.e. same surgical setting) including: tibial tubercle osteotomy, trochleoplasty, total knee arthroplasty. Concomitant soft tissue procedures were not excluded (e.g. lateral retinacular release).
-
3.
A cadaveric study
-
4.
Article solely describing a new surgical technique
-
5.
Failure to specify graft source material: allograft or autograft
-
6.
Insufficient data reporting. Corresponding authors were contacted on three separate attempts to ascertain missing data. Studies were excluded if missing data were not available.
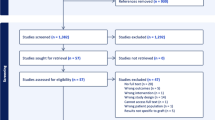
A PRISMA flow chart (Fig. 1) outlines the application of meta-analysis inclusion and exclusion criteria to the 216 articles that were identified for potential inclusion. A total of 31 studies met inclusion/exclusion criteria and were used to extract cohorts of patients who underwent ligament reconstruction with allograft, autograft, single-limbed, and double-limbed constructs (Table 1). Relevant patient demographics (age, sex), length of follow-up, incidence of postoperative patellar dislocations, and improvements in Kujala scores were recorded.

PRISMA diagram outlining the application of the inclusion and exclusion criteria of this systematic review [41]
Subject cohorts were extracted from the studies that met inclusion/exclusion criteria and subsequently combined using Comprehensive Meta-Analysis Software Package (Biostat Inc., Englewood, NJ, USA). A meta-analysis utilizing inverse-variance weighting in a DerSimonian–Laird random-effects model was then created [15, 33, 34]. Study heterogeneity was quantitatively assessed using I 2 statistic and indicated the potential for heterogeneity of the included studies (range 0–96 %). A random-effects model was chosen because it is the most appropriate and conservative method for assessment in the setting of study heterogeneity. It also accounts for both within-study and between-study variance. Furthermore, random-effects modelling is considered to be more appropriate in medical decision making contexts [1, 15]. Weighted failure rates and postoperative improvements in Kujala scores were compared between cohorts using Chi-squared and independent samples Student’s t tests. Funnel plots were generated, and the Egger intercept method was used to assess for publication bias [17].
Results
Study selection
A total of 1065 MPFL reconstructions were performed in 31 studies. Patient demographics and weighted results for each study are displayed in Table 1. Cohort size across graft source and configuration is detailed in Table 2.
The weighted mean follow-up across all studies was 35.0 months. Mean patient age at the time of operation was 23.4 years. Twelve studies exclusively used semitendinosus tendon autograft. Other autograft tissue sources included gracilis, patellar tendon, adductor magnus, quadriceps, and unspecified hamstring tendon. The allograft tendon sources that were utilized included semitendinosus, tibialis anterior, patellar tendon, and unspecified hamstring. Two studies did not specify the allograft source used [37, 72].
Preoperative and postoperative collection of the Kujala score was completed for 75 of 128 (58.6 %) reconstructions in the single-limbed group and 451 of 937 (48.1 %) in the double-limbed group. Similarly, 47 of 132 (35.6 %) Kujala scores were assessed in the allograft cohort and 445 of 933 (47.7 %) were provided in the autograft cohort. Overall, 4 of the 31 studies (13 %) did not utilize the Kujala score as an outcome measure [6, 12, 37, 62]. Twelve of the remaining studies reported incomplete data with regard to the Kujala scores (e.g. point estimates only without data distribution such as standard deviation, postoperative Kujala score only), and the corresponding authors did not respond to inquiries for original data or compliant descriptive statistics. These Kujala scores were therefore not included in the final analyses.
Egger’s intercept method revealed an intercept of −4.41 (P = 0.046) for Kujala score (indicating borderline potential for publication bias). Subsequent inspection of the funnel plot (Fig. 2a) indicated an equally wide variation in results for studies with low standard error (e.g. larger studies), rather than true publication bias. With regard to failure rate, Egger’s intercept method revealed an intercept of −1.78 (P = 0.01), indicating there was some evidence of publication bias in the included studies. Inspection of the funnel plot (Fig. 2b) indicated a “file drawer effect”, or a likely preferential publication of studies with more favourable (lower) failure rates. Subsequent analysis of subgroup funnel plots for failure rate revealed an identical effect for all subgroups: single-limbed (Egger’s intercept −2.01, p < 0.01); double-limbed (Egger’s intercept −1.60, p < 0.01); autograft (Egger’s intercept −1.78, p < 0.01); allograft (Egger’s intercept −1.77, p = 0.01).

Funnel plots testing for publication bias in the reporting of Kujala score and failure rate. Analysis of Kujala score (a) indicated an equally wide variation in results for studies with low standard error (e.g. larger studies), rather than true publication bias. Analysis of failure rate (b) indicated a “file drawer effect”, or a likely preferential underreporting of failure rates across the orthopaedic surgical literature
Graft configuration
Double-limbed reconstructions were associated with both improved postoperative Kujala scores and a lower failure rate. Chi-squared analysis of postoperative failure, as defined by recurrent patellar instability, favoured double-limbed configurations (5.5 vs. 10.6 %, p = 0.03). Furthermore, autograft reconstructions were associated with greater postoperative improvements in Kujala scores when compared to allograft using independent samples t test (37.8 ± 0.4 vs. 31.6 ± 1.1, p < 0.001). This finding (difference in improvement of 6.2 points between groups) approached clinical importance based on a minimal clinical important difference (MCID) of the Kujala score of 7 points [54].
Graft source
Chi-squared analysis revealed that failure rate was no different between autograft and allograft reconstructions (5.70 vs. 6.70 %, respectively, p = 0.74). However, autograft reconstructions were associated with greater postoperative improvements in Kujala scores when compared to allograft using independent samples t test (32.2 ± 2.5 vs. 22.5 ± 2.0, p < 0.001). Moreover, this difference (9.7 points) was clinically important, as it exceeded the MCID of the Kujala score (7 points).
Discussion
The most important findings of the present study were that the rate of recurrent patellar instability postoperatively as well as improvements in Kujala score were superior for the double-limb graft configuration. Similarly, improvements in Kujala scores were superior in the autograft cohort; however, rates of recurrent instability were no different. Similar concepts in the ACL literature have garnered increased attention. ACL reconstruction has demonstrated a higher rate of graft failure in young active patients when allograft sources are utilized. [26, 30, 67] Furthermore, some authors have proposed functional and biomechanical benefits of double-bundle reconstruction; however, it has not been shown to be wholly superior to single-bundle ACL reconstruction. [23, 29, 63] The MPFL has a broad, fan-shaped patellar insertion, and cadaveric studies demonstrate a mean patellar insertion width of 27.9 mm, which may be more precisely replicated with double-limbed grafts [3]. Despite these apparent conceptual similarities, it is important to note that the ACL and MPFL may not be comparable due to their differing anatomy and function. While the ACL is a stout intraarticular structure that provides stability in all ranges of knee flexion, the MPFL is a thin, extraarticular structure which acts as a checkrein in early knee flexion only. The 208-N tensile strength of the MPFL is significantly less than the 2160-N tensile strength of the native ACL, so extrapolations of ACL reconstruction theory may not be appropriate and the MPFL literature must be examined independently, further underscoring the importance of the current study [43, 70].
A study by Wang et al. [65] retrospectively compared double-limbed reconstruction (n = 44) with single-limbed reconstruction (n = 26) [65]. The authors observed a 4.3 % recurrent dislocation rate (3/70) in the study population, all in the single-limb group. The Kujala score also favoured use of the double-limb technique. Kujala scores continued to improve from 12 months to 48 months postoperatively, indicating long-term stability and graft longevity following MPFL reconstruction may be associated with the use of a double-limbed graft. Anatomic studies by Aragåo et al. [3] and Steensen et al. [57] defined the anatomic dimensions of the patellar attachment of the MPFL as fan-shaped, thereby facilitating distribution of ligament tension along the superior and middle portions of the patella [3, 57]. These observations provide an anatomic basis for double-limb constructs’ best approximation of the anatomic configuration of the MPFL, thereby resulting in improved stability compared to single-limb reconstructions.
Slenker et al. [55] compared recurrence of instability and Kujala scores by graft source following MPFL reconstruction in a small retrospective series, for patients who received hamstring autograft (n = 12) and soft tissue allograft (n = 23) [55]. The authors found no statistically significant difference in postoperative Kujala score, likely due to limited sample size and statistical power. While no patellar dislocations were reported after surgery, three patients (3/35; 8.6 %) reported episodes of patellar subluxation, all in the allograft cohort. This observation lends minimal support to the use of autograft; however, in the light of the results of the current study autograft may result in better patient-reported outcomes but not significantly lower risk of recurrent instability.
Limitations of the current meta-analysis reflect those of the constituent studies. Specifically, the reliance on retrospective observational studies makes selection bias unavoidable. Some studies evaluating Kujala score did not offer preoperative scores and had to be excluded from this portion of the analysis. Furthermore, most studies that utilized allograft tissue did not specify the tissue source or processing procedures, despite the understanding that graft irradiation can lead to structural compromise. [13] An additional limitation of the constituent studies included in this meta-analysis is that graft configuration and tissue source are unable to be analysed concurrently, because subjects have been extracted from observational cohort studies and analyses performed independently. Therefore, conclusions cannot be combined to indicate a superior combination of graft source and configuration. However, we are able to draw conclusions regarding superiority of graft configuration (single- vs. double-limbed) and tissue source (autograft vs. allograft) independently. Finally, most of these studies did not aim to evaluate graft source or configuration as the primary independent variable. As a result, authors did not specify age or sex within study populations. Therefore, we were unable to further stratify our cohorts and thus cannot definitively conclude one graft source or configuration is superior across patient populations. Nonetheless, despite some of the methodological flaws of the constituent studies, we believe the aggregation of multiple study cohorts provides the best available evidence for this topic to date. The underreporting of surgical failure rates likely lead to publication bias; however, there was no evidence of differential reporting bias between cohorts, indicating that the comparative results from the current study remain valid.
Few studies have directly compared allograft with autograft or single-limb versus double-limb constructs, and to our knowledge, no studies have assessed both graft source and configuration simultaneously. Strengths of the current study lie in the increased statistical power gained through cohort extraction and meta-analysis. Based upon failure rate and Kujala scores, clinicians should strongly consider restoring the anatomy of the MPFL with a double-limb graft configuration for recurrent patellar instability. In addition, clinicians should remain mindful that Kujala scores favour the selection of autograft tissue (in the absence of ligamentous laxity or a connective tissue disorder); however, there was no difference in revision rate between autograft and allograft sources and allograft processing techniques were not elucidated in the constituent studies.
Conclusion
Both the rate of recurrent postoperative patellar instability and Kujala scores were superior in the double-limb graft configuration cohort, and Kujala scores were superior with the use of autograft tendon. MPFL reconstructions should be performed using double-limbed configurations. While autograft tendon may be associated with higher patient-reported outcomes in the absence of associated connective tissue disorders or ligamentous laxity, patient factors and allograft processing techniques should be carefully considered when selecting an MPFL graft source, as revision rates were no different between graft sources.
References
Ades AE, Higgins JPT (2005) The interpretation of random-effects meta-analysis in decision models. Med Decis Mak 25:646–654
Ahmad CS, Brown GD, Stein BS (2009) The docking technique for medial patellofemoral ligament reconstruction: surgical technique and clinical outcome. Am J Sports Med 37(10):2021–2027
Aragão JA, Reis FP, de Vasconcelos DP, Feitosa VL, Nunes MA (2008) Metric measurements and attachments levels of the medial patellofemoral ligament: an anatomical study in cadavers. Clinics 63(4):541–544
Baldwin K, Morrison MJ 3rd, Tomlinson LA, Ramirez R, Flynn JM (2014) Both bone forearm fractures in children and adolescents, which fixation strategy is superior—plates or nails? A systematic review and meta-analysis of observational studies. J Orthop Trauma 28(1):e8–e14
Becher C, Kley K, Lobenhoffer P, Ezechieli M, Smith T, Ostermeier S (2014) Dynamic versus static reconstruction of the medial patellofemoral ligament for recurrent lateral patellar dislocation. Knee Surg Sports Traumatol Arthrosc 22(10):2452–2457
Berard JB, Magnussen RA, Bonjean G, Ozcan S, Lustig S, Neyret P, Servien E (2014) Femoral tunnel enlargement after medial patellofemoral ligament reconstruction: prevalence, risk factors, and clinical effect. Am J Sports Med 42(2):297–301
Bitar AC, Demange MK, D’Elia CO, Camanho GL (2012) Traumatic patellar dislocation: nonoperative treatment compared with MPFL reconstruction using patellar tendon. Am J Sports Med 40(1):114–122
Buckens CF, Saris DB (2010) Reconstruction of the medial patellofemoral ligament for treatment of patellofemoral instability: a systematic review. Am J Sports Med 38(1):181–188
Calvo Rodríguez R, Figueroa Poblete D, Anastasiadis Le Roy Z, Etchegaray Bascur F, Vaisman Burucker A, Calvo Mena R (2015) Reconstruction of the medial patellofemoral ligament: evaluation of the clinical results of autografts versus allografts. Rev Esp Cir Ortop Traumatol 59(5):348–353
Christiansen SE, Jakobsen BW, Lund B, Lind M (2008) Isolated repair of the medial patellofemoral ligament in primary dislocation of the patella: a prospective randomized study. Arthroscopy 24(8):881–887
Christiansen SE, Jacobsen BW, Lund B, Lind M (2008) Reconstruction of the medial patellofemoral ligament with gracilis tendon autograft in transverse patellar drill holes. Arthroscopy 24(1):82–87
Csintalan RP, Latt LD, Fornalski S, Raiszadeh K, Inacio MC, Fithian DC (2014) Medial patellofemoral ligament (MPFL) reconstruction for the treatment of patellofemoral instability. J Knee Surg 27(2):139–146
Curran AR, Adams DJ, Gill JL, Steiner ME, Scheller AD (2004) The biomechanical effects of low-dose irradiation on bone-patellar tendon-bone allografts. Am J Sports Med 32(5):1131–1135
Deie M, Ochi M, Adachi N, Shibuya H, Nakamae A (2011) Medial patellofemoral ligament reconstruction fixed with a cylindrical bone plug and a grafted semitendinosus tendon at the original femoral site for recurrent patellar dislocation. Am J Sports Med 39(1):140–145
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7(3):177–188
Desio SM, Burks RT, Bachus KN (1998) Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 26(1):59–65
Egger M, Smith GD, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. Br Med J 315:629–634
Elias DA, White LM, Fithian DC (2002) Acute lateral patellar dislocation at MR imaging: injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 225(3):736–743
Fabricant PD, Ladenhauf HN, Salvati EA, Green DW (2014) Medial patellofemoral ligament (MPFL) reconstruction improves radiographic measures of patella alta in children. Knee 21(6):1180–1184
Feller JA, Amis AA, Andrish JT, Arendt EA, Erasmus PJ, Powers CM (2007) Surgical biomechanics of the patellofemoral joint. Arthroscopy 23(5):542–553
Fithian DC, Paxton EW, Stone ML, Silva P, Davis DK, Elias DA, White LM (2004) Epidemiology and natural history of acute patellar dislocation. Am J Sports Med 32(5):1114–1121
Frosch S, Balcarek P, Walde TA, Schüttrumpf JP, Wachowski MM, Ferleman KG, Stürmer KM, Frosch KH (2011) The treatment of patellar dislocation: a systematic review. Z Orthop Unfall 149(6):630–645
Fu FH, Shen W, Starman JS, Okeke N, Irrgang JJ (2008) Primary anatomic double-bundle anterior cruciate ligament reconstruction: a preliminary 2-year prospective study. Am J Sports Med 36(7):1263–1274
Gans I, Baldwin KD, Ganley TJ (2013) Treatment and management outcomes of tibial eminence fractures in pediatric patients: a systematic review. Am J Sports Med 42(7):1743–1750
Han H, Xia Y, Yun X, Wu M (2011) Anatomical transverse patella double tunnel reconstruction of medial patellofemoral ligament with a hamstring tendon autograft for recurrent patellar dislocation. Arch Orthop Trauma Surg 131(3):343–351
Hettrich CM, Dunn WR, Reinke EK, MOON Group, Spindler KP (2013) The rate of subsequent surgery and predictors after anterior cruciate ligament reconstruction: two- and 6-year follow-up results from a multicenter cohort. Am J Sports Med 41(7):1534–1540
Hinterwimmer S, Imhoff AB, Minzlaff P, Saier T, Rosenstiel N, Hawe W, Feucht MJ (2013) Anatomical two-bundle medial patellofemoral ligament reconstruction with hardware-free patellar graft fixation: technical note and preliminary results. Knee Surg Sports Traumatol Arthrosc 21(9):2147–2154
Hopper GP, Leach WJ, Rooney BP, Walker CR, Blyth MJ (2014) Does degree of trochlear dysplasia and position of femoral tunnel influence outcome after medial patellofemoral ligament reconstruction? Am J Sports Med 42(3):716–722
Järvelä T (2007) Double-bundle versus single-bundle anterior cruciate ligament reconstruction: a prospective, randomize clinical study. Knee Surg Sports Traumatol Arthrosc 15(5):500–507
Kaeding CC, Pedroza AD, Reinke EK, Huston LJ, MOON Consortium, Spindler KP (2015) Risk factors and predictors of subsequent ACL injury in either knee after ACL reconstruction: prospective analysis of 2488 primary ACL reconstructions from the MOON cohort. Am J Sports Med 43(7):1583–1590
Kang HJ, Cao JH, Pan S, Wang XJ, da Yu H, Zheng ZM (2014) The horizontal Y-shaped graft with respective graft tension angles in anatomical two-bundle medial patellofemoral ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 22(10):2445–2451
Kang H, Cao J, Yu D, Zheng Z, Wang F (2013) Comparison of 2 different techniques for anatomic reconstruction of the medial patellofemoral ligament: a prospective randomized study. Am J Sports Med 41(5):1013–1021
Kontopantelis E, Reeves D (2012) Performance of statistical methods for meta-analysis when true study effects are non-normally distributed: a comparison between DerSimonian-Laird and restricted maximum likelihood. Stat Methods Med Res 21(6):657–659
Kontopantelis E, Reeves D (2012) Performance of statistical methods for meta-analysis when true study effects are non-normally distributed: a simulation study. Stat Methods Med Res 21(4):409–426
Kumahashi N, Kuwata S, Tadenuma T, Kadowaki M, Uchio Y (2012) A “sandwich” method of reconstruction of the medial patellofemoral ligament using a titanium interference screw for patellar instability in skeletally immature patients. Arch Orthop Trauma Surg 132(8):1077–1083
Lee EK, Namdari S, Hosalkar HS, Keenan MA, Baldwin KD (2013) Clinical results of the excision of heterotopic bone around the elbow: a systematic review. J Shoulder Elbow Surg 22(5):716–722
Li G, Sun XB, Ni JT, Cao L, Zhang KY (2011) Treatment of instability of patellofemoral joint through arthroscopic repair of medial patellofemoral ligament for adolescents with epiphyseal non-closure by allogenic tendon. Zhonghua Yi Xue Za Zhi 91(35):2468–2471
Lippacher S, Dreyhaupt J, Williams SR, Reichel H, Nelitz M (2014) Reconstruction of the medial patellofemoral ligament: clinical outcomes and return to sports. Am J Sports Med 42(7):1661–1668
Matic GT, Magnussen RA, Kolovich GP, Flanigan DC (2014) Return to activity after medial patellofemoral ligament repair or reconstruction. Arthroscopy 30(8):1018–1025
Matsushita T, Kuroda R, Oka S, Matsumoto T, Takayama K, Kurosaka M (2014) Clinical outcomes of medial patellofemoral ligament reconstruction in patients with an increased tibial tuberosity-trochlear groove distance. Knee Surg Sports Traumatol Arthrosc 22(10):2438–2444
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(4):264–269
Moore RE, Baldwin K, Austin MS, Mehta S (2014) A systematic review of open reduction and internal fixation of periprosthetic femur fractures with or without allograft strut, cerclage, and locked plates. J Arthroplasty 29(5):872–876
Mountney J, Senavongse W, Amis AA, Thomas NP (2005) Tensile strength of the medial patellofemoral ligament before and after repair or reconstruction. J Bone Joint Surg Br 87(1):36–40
Namdari S, Horneff JG, Baldwin K (2013) Comparison of hemiarthroplasty and reverse arthroplasty for treatment of proximal humeral fractures: a systematic review. J Bone Joint Surg Am 95(18):1701–1708
Namdari S, Rabinovich R, Scolaro J, Baldwin K, Bhandari M, Mehta S (2013) Absorbable and non-absorbable cement augmentation in fixation of intertrochanteric femur fractures: systematic review of the literature. Arch Orthop Trauma Surg 133(4):487–494
Nelitz M, Dreyhaupt J, Reichel H, Woelfle J, Lippacher S (2013) Anatomic reconstruction of the medial patellofemoral ligament in children and adolescents with open growth plates: surgical technique and clinical outcome. Am J Sports Med 41(1):58–63
Nomura E, Inoue M (2006) Hybrid medial patellofemoral ligament reconstruction using the semitendinous tendon for recurrent patellar dislocation: minimum 3 years’ follow-up. Arthroscopy 22(7):787–793
Nomura E, Inoue M, Kobayashi S (2007) Long-term follow-up and knee osteoarthritis change after medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 35(11):1851–1858
Pahlavan S, Baldwin KD, Pandya NK, Namdari S, Hosalkar H (2011) Proximal humerus fractures in the pediatric population: a systematic review. J Child Orthop 5(3):187–194
Panagopoulos A, van Niekerk L, Triantafillopoulos IK (2008) MPFL reconstruction for recurrent patella dislocation: a new surgical technique and review of the literature. Int J Sports Med 29(5):359–365
Panni AS, Alam M, Cerciello S, Vasso M, Maffulli N (2011) Medial Patellofemoral ligament reconstruction with a divergent patellar transverse 2-tunnel technique. Am J Sports Med 39(12):2647–2655
Raghuveer RK, Mishra CB (2012) Reconstruction of medial patellofemoral ligament for chronic patellar instability. Indian J Orthop 46(4):447–454
Shah JN, Howard JS, Flanigan DC, Brophy RH, Carey JL, Lattermann C (2012) A systematic review of complications and failures associated with medial patellofemoral ligament reconstruction for recurrent patellar dislocation. Am J Sports Med 40(8):1916–1923
Singer B, Singer K (2009) Anterior knee pain scale. Aust J Physiother 55(2):140
Slenker NR, Tucker BS, Pepe MD, Marchetto PA, Cohen SB (2013) Short-/intermediate-term outcomes after medial patellofemoral ligament reconstruction in the treatment of chronic lateral patellofemoral instability. Phys Sportsmed 41(2):26–33
Song SY, Kim IS, Chang HG, Shin JH, Kim HJ, Seo YJ (2014) Anatomic medial patellofemoral ligament reconstruction using patellar suture anchor fixation for recurrent patellar instability. Knee Surg Sports Traumatol Arthrosc 22(10):2431–2437
Steensen RN, Dopirak RM, McDonald WG (2004) The anatomy and isometry of the medial patellofemoral ligament: implications for reconstruction: implications for reconstruction. Am J Sports Med 32:1509–1513
Stefancin JJ, Parker RD (2007) First-time traumatic patellar dislocation: a systematic review. Clin Orthop 455:93–101
Steiner TM, Torga-Spak R, Teitge RA (2006) Medial patellofemoral ligament reconstruction in patients with lateral patellar instability and trochlear dysplasia. Am J Sports Med 34(8):1254–1261
Stupay KL, Swart E, Shubin Stein BE (2015) Widespread implementation of medial patellofemoral ligament reconstruction for recurrent patellar instability maintains functional outcomes at midterm to long-term follow-up while decreasing complication rates: a systematic review. Arthroscopy 31(7):1372–1380
Toritsuka Y, Amano H, Mae T, Uchida R, Hamada M, Ohzono K, Shino K (2011) Dual tunnel medial patellofemoral ligament reconstruction for patients with patellar dislocation using a semitendinosus tendon autograft. Knee 18(4):214–219
Trentacosta NE, Vitale MA, Ahmad CS (2009) The effects of timing of pediatric knee ligament surgery on short-term academic performance in school-aged athletes. Am J Sports Med 37(9):1684–1691
Tsai AG, Wijdicks CA, Walsh MP, Laprade RF (2010) Comparative kinematic evaluation of all-inside single-bundle and double-bundle anterior cruciate ligament reconstruction: a biomechanical study. Am J Sports Med 38(2):263–272
Wagner D, Pfalzer F, Hingelbaum S, Huth J, Mauch F, Bauer G (2013) The influence of risk factors on clinical outcomes following anatomical medial Patellofemoral ligament (MPFL) reconstruction using the gracilis tendon. Knee Surg Sports Traumatol Arthrosc 21(2):318–324
Wang CH, Ma LF, Zhou JW, Ji G, Wang HY, Wang F, Wang J (2013) Double-bundle anatomical versus single-bundle isometric medial patellofemoral ligament reconstruction for patellar dislocation. Int Orthop 37(4):617–624
Wang JL, Li HP, Liu YJ, Wang N, Li ZL, Wang ZG, Wei M (2012) Reconstruction of the medial patellofemoral ligament with a suture-tie technique of patellar side fixation. Chin Med J 125(11):1884–1888
Wasserstein D, Khoshbin A, Dwyer T, Chahal J, Gandhi R, Mahomed N, Ogilvie-Harris D (2013) Risk factors for recurrent anterior cruciate ligament reconstruction: a population study in Ontario, Canada, with 5-year follow-up. Am J Sports Med 41(9):2099–2107
Weeks KD, Fabricant PD, Ladenhauf H, Green DW (2012) Surgical options for patellar stabilization in the skeletally immature patient. Sports Med Arthrosc 20(3):194–202
Witoński D, Kęska R, Synder M, Sibiński M (2013) An isolated medial Patellofemoral ligament reconstruction with patellar tendon autograft. Biomed Res Int 2013:637678
Woo SL, Hollis JM, Adams DJ, Lyon RM, Takai S (1991) Tensile properties of the human femur-anterior cruciate ligament-tibia complex. The effects of specimen age and orientation. Am J Sports Med 19(3):217–225
Zhang H, Hong L, Geng X, Wang X, Feng H (2011) Reconstruction of medial patellofemoral ligament for recurrent patellar dislocation. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 25(8):925–930
Zhang L, Li Z, Liu J, Sun J, Ma J (2010) Anatomical double bundle reconstruction of medial patellofemoral ligament with allograft tendon in patellar dislocations]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 24(1):100–103
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Weinberger, J.M., Fabricant, P.D., Taylor, S.A. et al. Influence of graft source and configuration on revision rate and patient-reported outcomes after MPFL reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 25, 2511–2519 (2017). https://doi.org/10.1007/s00167-016-4006-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-016-4006-4