
Abstract
Pulmonary arterial hypertension (PAH) pathobiology involves a remodeling process in distal pulmonary arteries, as well as vasoconstriction and in situ thrombosis, leading to enhanced pulmonary vascular resistance and pressure, to right heart failure and death. The exact mechanisms accounting for PAH development remain unknown, but growing evidence demonstrate that inflammation plays a key role in triggering and maintaining pulmonary vascular remodeling. Not surprisingly, PAH is often associated with diverse inflammatory disorders. Furthermore, pathologic specimens from PAH patients reveal an accumulation of inflammatory cells in and around vascular lesions, including macrophages, T and B cells, dendritic cells, and mast cells. Circulating levels of autoantibodies, chemokines, and cytokines are also increased in PAH patients and some of these correlate with disease severity and patients’ outcome. Moreover, preclinical experiments demonstrated the key role of inflammation in PAH pathobiology. Immunosuppressive agents have also demonstrated beneficial effects in animal PAH models. In humans, observational studies suggested that immunosuppressive drugs may be effective in treating some PAH subtypes associated with marked inflammation. The present chapter reviews experimental and clinical evidence suggesting that inflammation is involved in the pathogenesis of PAH, as well the therapeutic potential of immunosuppressive agents in PAH.
Jolyane Meloche and Sébastien Renard have equally contributed to this work.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Pulmonary arterial hypertension (PAH) is a progressive life-threatening disease characterized by a progressive elevation of pulmonary vascular resistance, right ventricular (RV) failure, and ultimately death (Rubin 1997). According to current classification (Badesch et al. 2009), PAH constitutes the first category of pulmonary hypertension (PH) (Simonneau et al. 2009). This specific group of pre-capillary PH includes idiopathic PAH (iPAH), heritable PAH, and PAH related to drugs and toxins, congenital heart disease, connective tissue disease (CTD), human immunodeficiency virus (HIV) infection, portal hypertension, chronic haemolytic anemia, and schistosomiasis.
Since 1994, when Tuder et al. (1994) identified for the first time inflammatory infiltrates within PAH patients’ plexiform lesions, an increasing amount of experimental and human reports supported the crucial role of inflammation in PAH development (Dorfmuller et al. 2003; Hassoun et al. 2009; Price et al. 2012). Numerous inflammatory disorders and autoimmune processes are associated with the development of experimental and human PAH (Daley et al. 2008; Morse et al. 1997; Negi et al. 1998; Nicolls et al. 2005). Moreover, bone morphogenetic protein receptor type 2 (BMPRII), a pathway largely involved in heritable PAH (Deng et al. 2000; Lane et al. 2000; Machado et al. 2001), also modulates the inflammatory response (Hagen et al. 2007; Song et al. 2008). However, even if inflammation in PAH is well recognized to promote and/or perpetuate pulmonary vascular remodeling (Pullamsetti et al. 2011), its precise relationship with other components of the PAH pathogenesis like endothelial cells (EC) dysfunction, proliferation of pulmonary artery (PA) smooth muscle cells (PASMC) and fibroblast, and in situ thrombosis remains elusive. Furthermore, it is still unclear if inflammation really initiates vascular remodeling (“initial hit”), participates in its progression (“secondary hits”) or represents a reactive response to remodeling only (“bystander phenomenon”) (Price et al. 2012). From a therapeutic perspective, some reports have shown that immunosuppressive or anti-inflammatory drugs may improve PAH, both in animal models (Bonnet et al. 2007; Price et al. 2011; Sutendra et al. 2011; Suzuki et al. 2006; Wang et al. 2011; Zheng et al. 2010) and human cases (Jais et al. 2008; Karmochkine et al. 1996; Ogawa et al. 2011; Tanaka et al. 2002).
This chapter will review the relevance of inflammatory processes in experimental and human PAH, the implication of cells and other mediators in the inflammatory response observed in PAH, the potential targets for immunosuppressive treatment iPAH, and the updated clinical experience with available immunosuppressant agents.
2 Clinical Evidence of Inflammation in Human PAH
Over the past decades, many inflammation processes have been clearly associated with PAH development, including CTD (Asherson 1990; Cool et al. 1997; Fagan and Badesch 2002; Hachulla et al. 2005), HIV infection (Cool et al. 1997; Humbert 2008) and schistosomiasis infection (Butrous et al. 2008; Tuder 2009). PAH may also occur as an ultimate complication of exceptional autoimmune/inflammatory disorders such as POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammapathy, skin changes) (Lesprit et al. 1998) or Castelman disease (Montani et al. 2005a). Also, several reports indicate an association between Hashimoto thyroiditis and PAH (Thurnheer et al. 1997). Even in iPAH, inflammatory phenomenons are present, confirming the key role of inflammation in the global pathophysiology of PA vascular remodeling (Hall et al. 2009; Humbert et al. 1995; Perros et al. 2007; Soon et al. 2010).
2.1 Histological and Cytological Data in Human PAH
Histological data were the first to support the role of inflammation in PAH pathobiology. Tuder et al. (1994) described in 1994 perivascular inflammatory cell infiltrates composed of T cells, B cells, and macrophages in seven of ten cases of iPAH with plexogenic arteriopathy. Cool et al. (1997) reported a few years later mononuclear inflammatory cells surrounding vascular sites of plexiform growth in CTD-PAH lungs. These common features between iPAH and CTD-PAH underlined a potential role of inflammation in all PAH subtypes. Since these results, many histological and fundamental reports confirmed that immune cells abnormalities are implicated in human PAH pathogenesis (Hassoun et al. 2009; Kherbeck et al. 2011; Perros et al. 2011; Price et al. 2012), including very recent data suggesting that in iPAH, the tertiary lymphoid follicle composed of B lymphocytes, T lymphocytes, and dendritic cells have connections to remodeled PA via a stromal network supplied by lymphatic channels (Perros et al. 2012).
2.2 Inflammatory Mediators and Biomarkers in Human PAH
Increased circulating levels of interleukin (IL)-1β and IL-6 were initially reported in iPAH by Humbert et al. (1995) in the early 1990s. Elevated serum cytokines have also been observed in other PAH subtypes like CTD-PAH (Gerbino et al. 2008), HIV-PAH (Humbert et al. 1995), as well as PAH associated with sickle cell disease (Niu et al. 2009) and congenital heart disease (Diller et al. 2008). Some authors even suggested inflammatory cytokines (Soon et al. 2010) and C-reactive protein (Quarck et al. 2009) levels predicted survival in PAH, although this remains controversial (Montani et al. 2011; Soon et al. 2010). Different types of chemokines are also increased in human PAH patients’ serum, such as chemokine (C-C motif) ligand (CCL) 2 [known as monocyte chemotactic protein (MCP)-1] (Sanchez et al. 2007), CCL5 [known as regulated upon activation normal T cell expressed and secreted (RANTES)] (Dorfmuller et al. 2002), and CXC3CL1 (known as fractalkine) (Balabanian et al. 2002). In addition, PASMC from PAH patients demonstrate stronger migratory and proliferative response to CCL2 compared to controls (Sanchez et al. 2007). Thus, besides evidences of local inflammation in PAH, these data suggest PAH is associated with a systemic inflammatory state that may correlate with disease severity.
2.3 Inflammatory Conditions Associated with Human PAH
Clinical arguments have been accumulated supporting the role of inflammation in human PAH, especially in the spectrum of CTD and infectious diseases.
2.3.1 CTD and Inflammatory Diseases Associated with PAH
2.3.1.1 Systemic Scleroderma
The frequent association between two rare conditions is a strong argument for a link between them. Among CTD, scleroderma (SSc) is most commonly associated with PAH, occurring in 5–15 % of SSc patients (Hachulla et al. 2005; Mukerjee et al. 2003b). As in iPAH, EC activation and apoptosis, inflammatory cells recruitment, intimal proliferation, and advential fibrosis leading to vessel obliteration are observed in SSc-PAH (Cerinic et al. 2003; Dorfmuller et al. 2007; Le Pavec et al. 2011; Sgonc et al. 2000), supporting the concept that common features take part in the pathobiology of both iPAH and SSc-PAH (Terrier et al. 2008). SSc-PAH patients are also characterized as having an important number of autoantibodies (Fritzler et al. 1995; Grigolo et al. 2000; Morse et al. 1997; Mouthon et al. 2005; Nicolls et al. 2005; Okano et al. 1992; Tamby et al. 2006), including antifibroblast antibodies (Tamby et al. 2006) and anti-EC antibodies (Arends et al. 2010; Tamby et al. 2005), which activate fibroblasts and induce pro-inflammatory and pro-adhesive phenotype, promoting vascular remodeling (Chizzolini et al. 2002). Finally, the impact of the autoimmunity in PAH is further supported by the heterogeneous prevalence of PAH among SSc depending on the precise autoantibodies detected (Steen 2005).
2.3.1.2 Systemic Lupus Erythematosus
The prevalence of PAH in systemic lupus erythematosus (SLE) varies from 0.5 to 14 % depending on the diagnostic algorithm used to define PAH (Fois et al. 2010). As for other CTDs, the presence of antinuclear antibodies and rheumatoid factor, as well as abnormalities in immunoglobulin G, complement fractions, cytokines, and growth factors suggest a predominant role for immunological mechanisms in SLE-associated PAH (Quismorio et al. 1984). It is important to keep in mind that other mechanisms may lead to PH in SLE like chronic thromboembolism related to antiphopholipid syndrome, diffuse interstitial disease (Pope 2008; Torre and Harari 2011), or more rarely active pulmonary vasculitis (Asherson and Oakley 1986).
2.3.1.3 Others CTDs and Rare Inflammatory States
Other CTD inflammatory and/or autoimmune disorders such as mixed CTD (Fagan and Badesch 2002; Jais et al. 2008), polymyositis–dermatomyositis (Minai 2009), Sjogren’s syndrome (Launay et al. 2007), rheumatoid arthritis (Chung et al. 2010; Hassoun 2009), Hashimoto’s thyroiditis (Chu et al. 2002; Thurnheer et al. 1997), sarcoidosis (Nunes et al. 2006), and more rarely, POEMS syndrome (Jouve et al. 2007; Lesprit et al. 1998), multicentric Castleman disease (Bull et al. 2003), and systemic vasculitis (Launay et al. 2006) have been associated with PAH.
2.3.2 Infectious Diseases Associated with PAH
Evidence for inflammation in PAH infectious-related forms is also supported by histological, cytological, serological, and clinical data where the infective agent is commonly considered as a potential inflammatory trigger.
2.3.2.1 Human Immunodeficiency Virus and Human Herpes Virus 8
HIV infection is an independent risk factor for PAH (Opravil et al. 1997), occurring in 0.5 % of infected patients (Barnier et al. 2009; Sitbon et al. 2008). Histological features in HIV-PAH are similar to that in other PAH subtypes (Cool et al. 1997; Humbert 2008; Mehta et al. 2000). The mechanisms by which HIV leads to PA remodeling may involve chronic immune activation and upregulation of proinflammatory cytokines and growth factors (Humbert et al. 1998). Indeed, expression and production of platelet-derived growth factors (PDGF) and vascular endothelial growth factors (VEGF) are increased in lung tissue and HIV-infected T cells (Ascherl et al. 1999; Humbert et al. 1998). Viral proteins like Glycoproteine 120 and Tat are also associated with lung endothelial dysfunction in HIV infection mostly through endothelin-1 secretion (Ehrenreich et al. 1993; Ensoli et al. 1990). Controversial data also suggested Human herpes virus 8 (HHV-8) coinfection could account for the development of HIV-PAH (Hsue et al. 2008; Montani et al. 2005b). The effects of highly active antiretroviral therapy (HAART) on HIV-PAH are controversial as cases of PAH regression (Barnier et al. 2009; Speich et al. 2000) and worsening (Pellicelli et al. 1998) have been reported after initiation of therapy.
As described above, genes coding for the vasculotropic virus HHV-8 proteins have also been identified in plexiform lesions of iPAH patients by Cool et al. in the early 2000s (Cool et al. 2003). HHV-8 is known as Kaposi’s sarcoma-associated herpes virus and is usually associated with angioproliferative disorders. HHV-8 could thus have a pathogenetic role in PAH, triggering vascular remodeling and plexiform lesions formation. Moreover, rare case reports documented an association between reversible PAH and HHV-8/HIV-associated multicentric Castelman’s disease (Montani et al. 2005a). Although there are indirect evidences from in vitro and animal studies in favor of a link between HHV-8 and PAH pathophysiology, HHV-8 has not been detected in recent histological studies in human iPAH (Bendayan et al. 2008; Henke-Gendo et al. 2005; Valmary et al. 2011). Thus, the potential role of this virus on PA remodeling in PAH remains controversial.
2.3.2.2 Parasites: Schistosomiasis-Related PAH
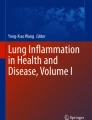
Among the estimated 200 million people infected by schistosomiasis worldwide (King 2010), between 2 and 5 % are believed to develop PAH (Graham et al. 2010), but their survival remains, in any case, better than in iPAH (dos Santos Fernandes et al. 2010). PAH occurs almost exclusively in patients with hepatosplenic infection by Schistosoma mansoni (Lapa et al. 2009) with subsequent portal hypertension. Histologically, plexiform lesions as well as concentric medial hypertrophy and thrombosis similar to those seen in iPAH are observed in schistosomiasis-related PAH (Tuder 2009). The mechanisms leading to PAH remain elusive, but may be related to mechanical impaction of pulmonary vessels by eggs, focal arteritis, and inflammation and increased pulmonary blood flow as consequence of portocaval shunts. Contribution of inflammation to vascular remodeling is not well understood but could be mediated by the modulation of regulatory T lymphocytes (Treg) activity resulting in the overexpression of a specific transforming growth factor superfamily (Freitas et al. 2007) or by the upregulated IL-13 signaling (Graham et al. 2010). In chronically infected animals without PH, increases in perivascular CD68-macrophages and CD45-lymphocytes have also been reported, suggesting an important switch from a Th1 to a Th2 immune response (Crosby et al. 2010). However, very few data allow extrapolating these experimental findings to human schistosomiasis-related PAH. Taken together, these non-exhaustive data suggest that increased levels of inflammatory mediators are common in human PAH (Fig. 1). Initial or latent inflammatory disorders may be an initial trigger for pulmonary vascular remodeling or act as a “second hit.” Although the relationship between inflammation and PAH is most obvious for PAH related to autoimmune, inflammatory, and infectious diseases, this association is not limited to a particular type of PAH.

Large amounts of inflammatory cell infiltrate pulmonary arteries in PAH. There is also vascular wall hypertrophy and presence of apoptotic endothelial cells. Cytokines (interleukins, TNF, MCP, etc.) and autoantibodies (anti-endothelial cells and antifibrolast for example) are present in the vascular wall and blood circulation. These autoantibodies can bind to endothelial cells and fibroblast and enhance cell modification (i.e., apoptosis and increase collagen production). Infiltration of T and B cells as well as macrophages, dendritic cells, mast cells, and fibroblast is observed in PAH. These inflammatory cells produce different cytokines as shown on the bottom part of this figure
3 Cells and Inflammatory Mediators Implicated in Pulmonary Vascular Remodeling
Different cell types, chemokines, cytokines, and antibodies play a role in the pathogenesis of PAH. This inflammatory process is not specific to a PAH subgroup, suggesting a central role of inflammation in PAH pathology.
3.1 Cell Types Implicated in Inflammatory Processes
3.1.1 T Lymphocytes (or T cells)
T cells are part of the adaptive immune response. They can differentiate into many subtypes according to different stimuli. Major subtypes found in lungs are T helper CD4+ (Th), Treg, and T cytotoxic CD8+ (Tc) cells. CD4+ Th cells are further divided in Th1, Th2, and Th17 according to their activation and cytokine production. Th1 play a role in cellular immunity and clearance of intracellular pathogen by producing interferon-γ. Th2 produce pro-inflammatory cytokines and are mainly implicated in humoral immunity, inflammation, and allergy. Th17 regulate tissue inflammation and autoimmunity by producing IL-17. CD4+ Th cells are important regulators of adaptive immune response since they stimulate B cell differentiation and macrophage activation, which are critical in triggering the immune response. CD8+ Tc are responsible of killing viral infected cells and tumor cells by binding to major histocompatibility complex class I molecules. Treg suppress autoreactive T cells and, thus, control self-tolerance and autoimmunity by balancing Th1 and Th2 responses. Different evidences support the role of T cells in PAH development. For instance, Treg are able to limit vascular endothelial injury and prevent PAH (Tamosiuniene et al. 2011). In animal models, athymic rats (no mature T cells) develop PAH more rapidly than rats with intact T cell production (Taraseviciene-Stewart et al. 2007), giving a protective role to T cells in PAH. Conversely, depletion of Th cells ameliorates the extent of PAH in other models (Sutendra et al. 2011). Thus, certain subtypes of T cells may confer beneficial effect in PAH, whereas others like Th2 may promote pulmonary vascular remodeling (Daley et al. 2008). Overall, infiltrated T cells within PA wall are increased in iPAH patients. Some studies have shown that Tc are decreased and Treg increased in PAH (Ulrich et al. 2008a) and others showed no difference in Treg between control and PAH patients (Huertas et al. 2012). The precise role of these T cell subtypes is not yet defined. Studies in cancer demonstrated that T cells inhibit tumor growth, but their functions are often suppressed in tumor microenvironment (Koebel et al. 2007; Zitvogel et al. 2008). A similar pattern could be observed in PAH, as leptin can modulate the hyporesponsiveness of Treg (Huertas et al. 2012). Overall, it is clear that inflammation plays an important role in PAH pathogenesis and that T cells are implicated but the exact mechanism has not yet been completely elucidated.
3.1.2 Dendritic Cells
Dendritic cells are professional antigen-presenting cells, displaying antigen to activate the adaptive immune response (T cell activation). They are responsible for the initiation of the inflammatory response. Recent studies documented the role of dendritic cells in the inflammatory process in different disorders including SLE (Palucka et al. 2005). Furthermore, these cells are present in pulmonary vascular lesions and blood of PAH patients (Wang et al. 2009). Perros et al. (2007) demonstrated that immature dendritic cells are involved in pulmonary vascular remodeling and thus could be involved in PAH immunopathology. Finally, dendritic cells have the ability to differentiate into other cell phenotypes, including EC, expanding their potential role in PAH pathogenesis (Conejo-Garcia et al. 2004).
3.1.3 Mast Cells
Mast cells are derived from bone marrow precursors and reside in tissues adjacent to blood vessels. They are major effector cells of immediate hypersensitivity reactions (allergy). They contain numerous mediator-filled granules, containing histamine and heparin, and a cross-linking of their IgE to a receptor stimulates granules release as well as synthesis and secretion of other mediators leading to hypersensitivity reaction. Accumulation of mast cells is seen in different PAH types (Hamada et al. 1999; Heath and Yacoub 1991). The exact role of mast cells in PAH pathobiology is not yet well established, but they seem to be implicated in direct vasoactive effects (Heath and Yacoub 1991) and in vascular remodeling by releasing matrix metalloproteinases (Vajner et al. 2006). Conversely, mast cells can also produce IL-10, which has important anti-inflammatory and immunosuppressive effects.
3.1.4 Macrophages
Macrophages constitute the first line of immune defense and are part of the innate immune system. In normal lungs, macrophages are mainly present in alveolar airspaces to protect against inhaled pathogens. They play a crucial role in the inflammatory and immune response: they have an antigen-presenting role and display different antigens to activate T cells. Macrophages are increased in pulmonary vascular lesions and around remodeled PA in human and experimental PAH (Tuder et al. 1994). Macrophages are also responsible for producing a large spectrum of inflammatory mediators such as tumor necrosis factor (TNF), endothelin-1, different interleukins, and chemokines (Hassoun et al. 2009; Humbert et al. 2004). Recent studies demonstrated an interaction between macrophages and T cells in PAH (Gerasimovskaya et al. 2012). Indeed, macrophage migration is suppressed by activated T cells but not quiescent T cells, whereas activated macrophages partly block T cells antitumor growth effect. Activated macrophages are also able to suppress T cell activation, thus inhibiting the anti-migratory effect of T cells on macrophages, sustaining macrophage migration, and inflammation in PAH (Gerasimovskaya et al. 2012; Zitvogel et al. 2008).
3.1.5 B Lymphocytes
B cells are responsible of generating antibodies to specific antigenic epitopes which bind to antigens and tag cells for degradation by complement cascade and phagocytosis. In addition to increased antibody production observed in PAH, B cells are increased in PAH lung vasculature and in plexiform lesions and play a critical role in cell-mediated immune regulation though cytokines production (IL-6, IL-10, TNF), antigen presentation, and lymphoid organogenesis (Ulrich et al. 2008b).
3.2 Role of Antibodies
In iPAH, antinuclear antibodies are increased up to 40 % (Rich et al. 1986), whereas antoantibodies such as anti-Scl70, anticentromere, anticardiolipin, and anti-annexin C antibodies are also observed in CTD patients. The specific role of these autoantibodies in PAH pathogenesis is not yet elucidated. More recently, other autoantibodies have been detected in PAH patients.
3.2.1 Antifibroblast Antobodies
Antifibroblast antibodies are detected in 40 % of iPAH and in 30 % of SSc-PAH patients (Tamby et al. 2006). These antibodies enhance fibroblast differentiation and adhesion molecules production. Fibroblast are implicated in collagen production, which plays an important role in both CTD and PAH. Antifibroblast antibodies target different heat shock proteins, glucose-6-phosphate dehydrogenase, PI3-kinase, calumenin, and α-enolase (Terrier et al. 2008, 2009). These targets are implicated in oxidative stress-induced apoptosis resistance (Efferth et al. 2006), cell energy metabolism, cell growth, and cytoskeleton organization (Shibasaki et al. 1994), leading to increased contractility of myofibroblasts as observed in SSc and PAH.
3.2.2 Anti-endothelial Cell Antibodies
Anti-EC antibodies are detected in over half of patients with SSc and their levels are increased in SSc-PAH compared to SSc patients without PAH (Salojin et al. 1997). Anti-EC antibodies are also present in iPAH patients’ serum. A recent study identified lamins, beta tubulins, vinculin, and calumenin as anti-EC antibody targets (Dib et al. 2011). It has been suggested that these antibodies activate EC and induce apoptosis. Further studies would be needed to fully understand their role in the pathogenesis of PAH.
3.3 Chemical Pro-inflammatory Mediators
3.3.1 Cytokines and Chemokines
A large number of cytokines and chemokines (soluble cytokines acting as chemoattractants) are elevated in PAH (Balabanian et al. 2002; Soon et al. 2010). They are mainly produced not only by the innate immune system, i.e., dendritic cells and macrophages, but also by cells which form the vascular wall and adventia (Nathan 2002). Increased IL-1 and IL-6 levels are found in severe PAH (Humbert et al. 1995). Other cytokines such as IL-2, IL-4, IL-8, IL-12p70, and TNF-α are also increased in PAH patients’ serum (Fig. 1). Some of these cytokines, like IL-1b, IL-8, and TNF-α, predict outcome in PAH patients (Soon et al. 2010). The implication of these cytokines in PAH development has also been shown in animal models. For example, knock-out mice for IL-6 are resistant to hypoxia-induced PAH (Savale et al. 2009) and mice overexpressing IL-6 develop severe PH (Steiner et al. 2009), suggesting a central role of IL-6 in PAH. Furthermore, circulating IL-6 levels are predictive for the presence of associated PAH among SSc patients (Gourh et al. 2009). IL-6 is known to have many effects on inflammatory and vascular cells (Steiner et al. 2009). In fact, IL-6 stimulates T lymphocytes accumulation, chemokine production (such as CXCL3) by EC (Imaizumi et al. 2004), as well as PASMC and EC proliferation (Savale et al. 2009; Steiner et al. 2009). C-reactive protein is a marker of inflammation and tissue damage and is an active player in vascular wall damage and atherosclerosis (Scirica and Morrow 2006). C-reactive protein levels predict cardiovascular events (Labarrere and Zaloga 2004). Recently, Quarck et al. (2009) demonstrated that C-reactive protein levels are also increased in PAH patients and correlate with long-term outcomes. Moreover, normalization of its levels with therapy is associated with improved functional capacity and survival in PAH (Quarck et al. 2009; Sztrymf et al. 2010).
An important chemokine potentially involved in PAH pathogenesis is fractalkine (CX3CL1 for C-X3-C motif ligand 1). Fractalkine, which can be detected as a soluble form, is anchored in EC membrane and is overexpressed in severe PAH (Balabanian et al. 2002). This chemokine may be responsible for leukocyte capture from the blood and recruitment (if they express C-X3-C motif receptor) (Balabanian et al. 2002). Circulating levels of monocyte chemoattractant protein-1 (MCP-1, also known as CCL2) are also increased in PAH. MCP-1 is secreted by EC, macrophages, and fibroblasts and stimulates leukocytes and monocytes migration. As described earlier, cytokines can also act as chemokines. Thus IL-8, which is produced by hematopoietic cell and part of the C-X-C class, is chemoattractant for T cells and neutrophils (Schall et al. 1990). Macrophage inflammatory protein-la (MlP-lα, also known as CCL3) promotes migration of monocytes and T and B cells through the endothelial junctions and underlying tissue (Schall et al. 1993). MlP-lα mRNA expression is increased in PAH lung biopsy specimens compared to control (Fartoukh et al. 1998). RANTES is another important chemoattractant for T cells and monocytes and is increased in PAH (Dorfmuller et al. 2002; Luster 1998; Schall et al. 1990). Dorfmüller et al. (2002) demonstrated that RANTES mRNA levels are increased in EC from small remodeled PA and in plexiform lesions, thus increasing the amount of inflammatory cells in remodeled arteries of PAH patients.
3.3.2 Other Growth Factors Implicated in Inflammation
Growth factors including PDGF, epidermal growth factor, VEGF, and fibroblast growth factor 2 are implicated in the proliferative and apoptosis-resistant phenotype contributing to pulmonary vascular remodeling in PAH. There is an overlap between certain cytokines and growth factors. For example, IL-6 stimulates PASMC proliferation through an increase in VEGF and its receptor VEGFR2 (Steiner et al. 2009). PDGF-like molecules are secreted by many cell types, including PASMC, EC, and macrophages (Heldin 1992) and their expression is increased in PAH patients (Humbert et al. 1998). It has been shown that PDGF is able to induce smooth muscle cell proliferation and migration, which explains its implication in various fibroproliferative disorders such as hypoxic PH (Katayose et al. 1993; Schermuly et al. 2005).
4 Inflammation in PAH: Beyond the Pulmonary Vasculature
Right ventricular failure is an important component of the PAH pathophysiology. Indeed, RV failure is the leading cause of death in PAH. Not surprisingly, many circulating biomarkers currently used in PAH prognosis assessment are in fact cardiac-derived biomarkers (Barrier et al. 2012), such as brain natriuretic peptides (Blyth et al. 2007; Gan et al. 2006; Nagaya et al. 2000), troponins (Hoeper et al. 2004; Torbicki et al. 2003), and osteopontin (Lorenzen et al. 2011). The RV capacity to adapt to increased afterload is highly heterogeneous among PAH patients: some are adaptive remodelers with RV hypertrophy and preserved RV function, whereas others are maladaptive remodelers and rapidly develop RV failure (Sztrymf et al. 2010). Some studies have suggested the implication of inflammation in RV remodeling and hypertrophy (Overbeek et al. 2008). However, very little is known about the molecular and cellular mechanisms involved in RV adaptation.
Part of the answer could be found through the analysis of SSc-PAH patients, which have a worse prognosis than iPAH patients (Condliffe et al. 2009; Kawut et al. 2003). This difference may be partly explained by the older age of SSc patients and their comorbidities. Nevertheless, recent data suggest that their RV adapts differently compared to iPAH patients (Chung et al. 2010), including higher N-terminal BNP levels and increased neurohormonal activation found in SSc-PAH compared to iPAH despite of less severe hemodynamic abnormalities (Mathai et al. 2009; Overbeek et al. 2008). Indirect evidence of increased RV inflammation in SSc-PAH has been suggested. For instance, an increased signal intensity in T2-weighted sequence (abnormalities commonly associated with inflammatory myocarditis in the absence of coronary artery disease) is documented on cardiac magnetic resonance imaging studies in SSc-PAH patients compared to SSc-patients without PAH (Hachulla et al. 2009). Recently, Overbeek et al. (2008) confirmed that RV from SSc-PAH (n = 5) had more neutrophilic granulocytes, macrophages, and lymphocytes than in iPAH (n = 9) or controls (n = 4), whereas RV interstitial fibrosis was similar in all groups. However, the participation of inflammation to RV failure is also suspected in all PAH types except, perhaps, for patients with left-to-right shunt and Eisenmenger physiology. In this setting, cardiomyocyte contractions may produce a trigger for autocrine, paracrine, and neuroendocrine signaling pathways leading to a vicious circle of RV inflammation and ischemia, leading to cardiomyocytes apoptosis and RV failure (Bogaard et al. 2009a). Nonetheless, observed RV recovery after lung transplantation supports the idea that RV failure is not irreversible and may be amenable to specific interventions in PAH. Interestingly, Bogaard et al. (2009a) recently demonstrated that a mechanical model of chronic progressive RV pressure overload using PA banding did not lead to fatal RV failure. In contrast, the Sugen model, an established model of angioproliferative PAH, showed myocardial apoptosis, fibrosis, decreased RV capillary density, and VEGF expression despite increased nuclear stabilization of Hypoxia Inducible Factor-1 (HIF-1), ultimately leading to RV dilation and failure. A more recent animal study from this group assessed a potential RV failure molecular signature (Bogaard et al. 2009b). Their results suggest that RV hypertrophy and/or failure phenotypes in Sugen rats are characterized by distinct patterns of gene expression (mRNA and microRNA) related to cell growth, angiogenesis, and energy metabolism (Drake et al. 2011). Additionally, using PA banding and monocrotaline (MCT) rat models, Piao et al. (2010a, b) demonstrated that in RV hypertrophy, there was a mitochondrial metabolic switch from glucose oxidation to glycolysis. This increase in glucose uptake by the RV can be seen on PET scan, compared to a normal RV that is usually invisible (Bokhari et al. 2011; Can et al. 2011). The increase in glycolysis may temporarily preserve the energetic balance, but ultimately becomes maladaptive (Piao et al. 2010a, b). The reversibility of mitochondrial dysfunction in animals with RV hypertrophy, by a oxidative phosphorylation restoration using a prototypic pyruvate dehydrogenase kinase inhibitor (dichloroacetate), may offer selective strategies for improving RV function; this is in addition to known positive effects of dichloroacetate on PA remodeling in multiple experimental PAH models (Guignabert et al. 2009; McMurtry et al. 2004; Michelakis et al. 2002). These data suggest that complex molecular, cellular, and hemodynamic heart–lung interactions may be involved in the transition from compensated RV hypertrophy to failure in PAH. New therapeutic approaches based, among others, on RV inflammation and abnormal glycolytic metabolism may thus be of interest in PAH.
5 Available Immunosuppressive Agents: Mode of Action and Use in Human Diseases Predisposing to PAH
The mechanisms of action of common immunosuppressive agents are summarized in Table 1 and schematized in Fig. 2.

Mode of action of different immunosuppressive agents as described in text. Cyclophosphamide targets bone marrow stem cells and inhibits their differentiation into B and T cells. Glucocorticoids target B and T cell differentiation and activation. Ciclosporin has a more T cell-specific mode of action as it inhibits differentiation of T cells into Th1, Th2, and Th17. Other molecules such as methotrexate and mycophenolate mofetil target DNA and RNA synthesis, thus blocking proliferation
5.1 Glucocorticoids
Glucocorticoids are small lipophilic compounds affecting B cell and T cell development, differentiation, and function. Their major mechanism for immune suppression is through NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) inhibition. NF-κB is involved in many cytokines and/or chemokines synthesis. Inhibition of this transcription factor, therefore, blunts the immune system capacity to mount a response (Rhen and Cidlowski 2005). Glucocorticoids also suppress cell-mediated immunity by inhibiting genes coding for different cytokines such as IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, IL-8, and interferon-γ. They can also stimulate T cell apoptosis by triggering the transcription of different genes (Leung and Bloom 2003). Finally, glucocorticoids not only suppress immune response but also inhibit the two main products of inflammation: prostaglandins synthesis at the phospholipase A2 level as well as leukotrienes synthesis at the cyclooxygenase/PGE isomerase level (Goppelt-Struebe et al. 1989). Glucocorticoids are thus potent anti-inflammatory agents, regardless of the inflammation’s cause. Therefore, glucocorticoids are often recommended by experts for the treatment of inflammatory manifestations of CTD (Bertsias et al. 2008; Kowal-Bielecka et al. 2009) as well as other inflammatory disorders like POEMS syndrome (Dispenzieri 2011) and sarcoidosis (Coker 2007). Some experimental data also support that glucocorticoids (prednisolone) have an antiproliferative effect on cultured PASMC from patients with iPAH (Ogawa et al. 2005).
5.2 Cyclophosphamide
Cyclophosphamide (CYC) is an alkylating agent used in chemotherapy to slow or stop cell growth. It alkylates or binds to DNA, cross-linking DNA, and RNA strands, thus inhibiting protein synthesis. These actions are neither cell cycle specific nor cell type specific. CYC also exerts its anti-inflammatory function through direct cytoxicity of bone marrow precursors and mature lymphocytes (Fig. 2), leading to a reduction of T and B cells as well as the CD4:CD8 T cell ratio (Manno and Boin 2010; Marder and McCune 2007; McCune et al. 1988), but depending on the dose used, it can also act on Treg and in this case stimulate the immune system (Brode and Cooke 2008). CYC is currently used, most commonly with concomitant corticosteroids, to treat some severe manifestations of CTD, including in interstitial lung disease related to SSc (Hoyles et al. 2006; Marder and McCune 2007; Nadashkevich et al. 2006; Nannini et al. 2008; Tashkin et al. 2006) and neuropsychiatric involvement related to lupus (Barile-Fabris et al. 2005; Stojanovich et al. 2003). Because of many side effects of CYC, however, other immunosuppressive agents are generally preferred for less severe complications of CTD or for maintaining remission.
5.3 Mycophenolate Mofetil
Mycophenolate mofetil (MMF) is an immunosuppressive drug with antiproliferative effects on inflammatory cells through the inhibition of the 5′-monophosphate dehydrogenase. This enzyme is involved in purines synthesis, an essential step for DNA synthesis in lymphocytes (Fig. 2). This agent is mainly used following organ transplantation. MMF has also been shown to be as effective and better tolerated than CYC for the treatment of lupus nephritis (Bertsias et al. 2008; Contreras et al. 2004). In addition, small series have suggested moderate benefit for interstitial lung disease (Gerbino et al. 2008; Zamora et al. 2008) and skin score (Derk et al. 2009) in SSc.
5.4 Methotrexate
Methotrexate (MTX) is a folic acid analogue and a potent competitive inhibitor of dihydrofolate reductase. It inhibits both DNA and RNA synthesis (Fig. 2). MTX is frequently used in SSc to treat inflammatory arthritis and myositis. Its efficiency for skin disease and interstitial lung disease is however limited (Pope et al. 2001; van den Hoogen et al. 1996). Similarly, MTX has an uncontested role in the management of arthritis and skin manifestations of SLE (Yildirim-Toruner and Diamond 2011), although it has no role for major organ involvement related to SLE (Carneiro and Sato 1999).
5.5 Ciclosporin
Ciclosporin A (CsA) is frequently used for Th1-, Th2-, and Th17-related disorders. It exerts its immunosuppressive function by interfering with T-cell production as well as Th differentiation and function (Grinyo et al. 2004; Kobayashi et al. 2007) (Fig. 2). CsA inhibits calcium synergic action and suppresses the calcineurin pathway, although the precise pharmacological mechanisms of CsA have not yet been fully elucidated (Tsuda et al. 2012). Calcineurin is a key molecule for the nuclear factor for activated T cells (NFAT) activation, which is the main transcription factor for IL-2. Additional anti-fibrotic effects as well as efficiency in chronic graft-versus-host disease have prompted consideration for SSc treatment. In a small open-label study, CsA was associated with a 36 % decrease in skin scores (Clements et al. 1993). Similar improvements were demonstrated in a small randomized trial testing CsA in combination with iloprost (Filaci et al. 1999). However, side effects like systemic hypertension and renal toxicity (Denton et al. 1994) have limited the clinical development of this calcineurin inhibitor in the spectrum of SSc, and this molecule is not currently recommended as first line immunosuppressive agent in SSc (Kowal-Bielecka et al. 2009). Similarly, CsA is not recommended for the management of SLE whatever its manifestations (Bertsias et al. 2008).
5.6 Anti-infectious Agents
5.6.1 Highly Active Antiretroviral Therapy in HIV-Related PAH
Considering on one hand the absence of apparent correlation between the stage of HIV infection, the degree of immunodeficiency, the CD4+ T lymphocytes counts, and the occurrence or severity of HIV-PAH (Mehta et al. 2000; Nunes et al. 2003) and, on the other hand, the heterogeneous evolution of HIV-PAH following antiretroviral therapy initiation, experts do not recommend systematic HAART initiation in case of HIV-PAH (Galie et al. 2009; Hammer et al. 2008). In fact, a large majority of patients are diagnosed for HIV-PAH while already on HAART. Nevertheless, a stable prevalence of HIV-PAH overtime despite HIV patients live much longer than in the 1980s suggest HAART may be associated with a lower incidence of PAH among HIV-infected patients (Opravil and Sereni 2008; Sitbon et al. 2008).
5.6.2 Antihelmintic Treatment in Schistosomiasis-Related PAH
Prazicantel is the most widely used antihelmintic drug to treat schistosomiasis in humans. It is a pyrazinoisoquinoline derivative only active against the adult worms (Ross et al. 2002). In mice, hepatic fibrosis and lung granuloma formation has been shown to be partly reversed by prazicantel and other antihelmintic treatment (de Almeida and Andrade 1983). In a murine model, prazicantel also reversed pulmonary vascular remodeling and prevented the development of schistosomiasis-related PAH in association with a reduction of lung mRNA expression of cytokines IL-13, IL-8, and IL-4 (Crosby et al. 2011). In humans, prazicantel is usually given to prevent further progression of the disease, even if pulmonary embolism composed of dead worms may follow this specific treatment and lead to a superimposed acute cor pulmonale (Lambertucci et al. 2000). However, antischistosomal therapy has not demonstrated any effect on pulmonary hemodynamics in schistosomiasis-related PAH, despite one case report documenting remission of PAH after prazicantel treatment (Bouree et al. 1990). New therapeutic strategies potentially targeting the inflammatory component of the disease (e.g., IL-13 antagonists) are thus needed for schistosomiasis-related PAH (Fernandes et al. 2011).
6 Immunosuppressive Agents in Experimental PH
6.1 Presence of Inflammation in Different PH Experimental Models
To study PH pathobiology, three different models are commonly used: hypoxia model, monocrotaline-induced model (MCT) and the newly developed Sugen-induced model (SU5416, a VEGF receptor inhibitor associated to chronic hypoxia) (Ryan et al. 2011). Other models [e.g., transgenic mice overexpressing 5-HTT specifically in PASMC and fawn-hooded rat are also used but at lesser extent (Guignabert et al. 2006)]. The hypoxia model develops mild to moderate PH with modest inflammation. Conversely, the MCT model develops significant inflammation with higher cytokine levels and marked inflammatory cells infiltrates in remodeled vascular wall, with inflammatory cells displaying a strong IL-6 expression (Bhargava et al. 1999; Price et al. 2011). In addition to these changes, the Sugen model shows plexiform-like lesions and, as in humans, many inflammatory cells are present in these vascular lesions. All these models show an increase in T and B cells, macrophages, mast cells, monocytes, and dendritic cells.
In these experimental models, inflammatory cells are not only innocent bystanders of the pulmonary vascular remodeling but also influence its development. For instance, absence of T cells increases vascular remodeling and worsens PH in the Sugen model (Taraseviciene-Stewart et al. 2007). Similarly, euthymic rat develop severe PH when submitted to both SU5416 injection and chronic hypoxia, whereas athymic rat develop severe vascular remodeling even in normoxia. In athymic rats, pulmonary arterioles become occluded by proliferating EC and are surrounded by mast cells, B cells, and macrophages. IL-4, proliferating cell nuclear antigen, and collagen type I levels are also markedly increased. These studies demonstrate the complex interactions between the immune system, the VEGF receptor signaling pathway, and the pulmonary vascular remodeling process. As a result, different immunosuppressive treatments have been tested in experimental PH.
6.2 Glucocorticoids
Some experimental data support that glucocorticoid treatments (with prednisolone) have an antiproliferative effect on PASMC isolated from iPAH patients (Ogawa et al. 2005). While PDGF induces iPAH-PASMC proliferation and migration, prednisolone reverses this effect in a dose-dependent manner (Ogawa et al. 2005). Very high dose of prednisolone thus caused cell cycle arrest of PASMCs with subsequent suppression of proliferation, whereas prednisolone has no effect on PASMC from controls.
Dexamethasone treatment (5 mg/kg/day) also significantly improved survival in a rat model of in MCT-induced PH (Price et al. 2011; Wang et al. 2011). Furthermore, Price et al. (2011) demonstrated that dexamethasone not only prevented but also normalized hemodynamics and right ventricular hypertrophy in a dose-dependent manner in established PH. At the vascular level, dexamethasone reversed medial and adventicial thickening, reduced MCT-induced adventitial infiltration of IL-6-expressing inflammatory cells (Price et al. 2011), inhibited pulmonary IL-6 overexpression, reduced CX3CR1 expression (Wang et al. 2011), suppressed perivascular CD8+ T cells, and restored the EC integrity (Wang et al. 2011).
6.3 Cyclophosphamide
No animal data was found.
6.4 Mycophenolate Mofetil
In the past decade, different groups demonstrated the beneficial effects of MMF (20–40 mg/kg/day), a prodrug of mycophenolic acid, on MCT-induced PH (Suzuki et al. 2006; Zheng et al. 2010). MMF decreased PASMC proliferation in both MCT-induced PH and in vitro (with fibroblasts to stimulate proliferation) in a dose-dependent manner (Zheng et al. 2010). MMF was also associated with a decrease in macrophages and IL-6 production in the pulmonary vasculature (Suzuki et al. 2006), whereas T cells or mast cells were unchanged (Zheng et al. 2010). From a hemodynamic point of view, MMF decreased RV systolic pressure and hypertrophy. These beneficial effects were seen with MMF concentrations within clinical applicable range, suggesting potentiality of MMF in the treatment of human PAH (Zheng et al. 2010).
6.5 Methotrexate
No animal data was found.
6.6 Ciclosporin
Koulmann et al. (2006) suggested that CsA treatment inhibits PH and RV hypertrophy either by inhibiting HIF-1 transcriptional activity in lung, by decreasing calcineurin activity in lung and heart, by direct effects of CsA, or by a combination of these factors. The CsA dose used in this study (25 mg/kg/day) is much higher than in more recent studies. The exact mechanism by which CsA inhibits PH has been determined more recently. Indeed, Bonnet et al. (2007) demonstrated that NFAT was overexpressed both in human and experimental PH and was largely involved in the PH pathobiology. NFATc2 was in fact mostly activated in iPAH PASMC (Bonnet et al. 2007). By different techniques, they provided evidence that the inhibition of NFAT using a specific [VIVIT (Aramburu et al. 1999)] or an indirect inhibitor (CsA) had beneficial effect on experimental (in vitro and in vivo) PH (Bonnet et al. 2007). Both CsA and VIVIT decreased PASMC proliferation and restored apoptosis levels in vitro. In established MCT-induced PH, CsA (1 mg/kg, similar to doses used clinically) conferred beneficial effects on hemodynamics, RV hypertrophy, and vascular remodeling (Bonnet et al. 2007). In a PH model of mice overexpressing 5-HTT (Guignabert et al. 2006), CsA decreased the pulmonary expression of NFAT and increased Kv1.5 protein levels but did not affect PH itself (mean PA pressure for example) (Guignabert et al. 2006). These results may be explained by the fact that inflammation is not an important component of SM22-5-HTT+ PH mice model (Macian 2005). Whether NFAT inhibition using indirect (e.g., CsA) or specific (e.g., VIVIT) inhibitors is effective in human PH or RV hypertrophy and failure remains unknown (McKinsey and Olson 2005).
6.7 Dehydroepiandrosterone
Our team demonstrated that dehydroepiandrosterone (DHEA) confers beneficial effects on PH not only due to its vasodilator effects but also by disrupting the IL-6/STAT3/NFAT axis known to potentiate PH (Paulin et al. 2011). In vitro data demonstrated that DHEA treatment inhibits IL-6-induced PASMC proliferation. By doing so, it confers anti-inflammatory effects. In MCT-induced PH, DHEA therapy also reverses PH, as assessed by mean pulmonary arterial pressure, right ventricular hypertrophy, and vascular wall thickness.
6.8 Etanercept
Tumor necrosis factor alpha (TNF-α) is a key proinflammatory cytokine that is increased in human and experimental PH (Stojanovich et al. 2003). Furthermore, TNF transgenic rats overexpressing TNF-α develop PH demonstrating its implication in PH pathogenesis (Fujita et al. 2001). Etanercept is a recombinant TNF-α receptor which binds to circulating TNF-α and functionally inhibits its action by blocking binding to cell membrane receptors, thus weakening its pro-inflammatory action (Zhou 2005). In MCT-induced PH, etanercept administered at clinically relevant doses (Lovell et al. 2000) at the same time as MCT injection (in prevention) or 3 weeks later of when PH was established (as a reversal therapy) decreased PH severity and RV hypertrophy (Sutendra et al. 2011). Since TNF-α expression is driven by NFAT in T cells, they confirmed that NFAT activation led to increased levels of TNF-α in an autocrine manner in PASMC. Furthermore, NFAT activation (and its downstream target Kv1.5) was similarly decreased by etanercept and VIVIT, a specific NFAT inhibitor. MCT-PH rats treated with etanercept also demonstrated lower TNF-α and IL-6 levels (another NFAT target) and decreased CD8+ T cells (Sutendra et al. 2011). Etanercept also reduced PH in a late endotoxin-induced model in pigs (Mutschler et al. 2006). Conversely, etanercept at a significantly lower dose had a nonsignificant effect on RV systolic pressure in MCT-induced PH (Henriques-Coelho et al. 2008).
6.9 Sirolimus
Sirolimus (or rapamycin) is an immunosuppressive drug preventing T cells and B cells activation by blocking their response to IL-2. It also blocks the VEGF pathway. Unlike tacrolimus and CsA, sirolimus is not a calcineurin inhibitor but has similar effects on the immune system. While sirolimus may prevent the development of MCT-induced PH, it is ineffective in reversing established PH (McMurtry et al. 2007; Nishimura et al. 2001).
7 Immunosuppressive Agents in Human PAH
Even if preclinical data show some beneficial effects, therapies targeting inflammation have not been formally tested in human PAH. Nevertheless, anti-inflammatory/immunosuppressive therapies are sometimes cautionary recommended by experts in exceptional circumstances. These pharmacological agents, their reported effects on inflammatory disorders and PAH, as well as their potential adverse effects and drug interactions with current PAH therapies are summarized Table 1.
7.1 Updated Experiment of Immunosuppressive Agents in Human PAH
7.1.1 Idiopathic PAH
Rare case reports suggested immunosuppressive therapy could be effective in iPAH. In 1999, Bellotto et al. described the case of an iPAH patient with sustained clinical and hemodynamic improvement following the initiation of prednisone and MTX (Bellotto et al. 1999). Recently, Ogawa et al. (2011) reported the case of a 34-year-old female with iPAH treated with epoprostenol for 3 years, who significantly improved after prednisolone was prescribed for concomitant idiopathic thrombocytopenia. Importantly, both cases of presumed iPAH were characterized by concomitant inflammatory disorders. Apart from these rare cases, no data support the use of immunosuppressive therapy in iPAH.
7.1.2 PAH Related to CTD
According to the EULAR Scleroderma Trials and Research database, PAH is a leading cause of SSc-related deaths even in the era of modern PAH therapies (Mathai and Hassoun 2011; Tyndall et al. 2010). Current guidelines recommend SSc-PAH should follow the same treatment algorithm as in iPAH (Galie et al. 2009). To date, the efficacy of immunosuppressive therapy in SSc-PAH is not supported by observational studies. Indeed, Sanchez et al. (2006) reported that, among a retrospective cohort of 28 CTD-PAH patients, none of the six SSc-PAH responded (defined as patients remaining in New York Heart Association functional class I or II with sustained hemodynamic improvement after at least 1 year without the addition of PAH specific therapy) to monthly cyclophosphamide and glucocorticoids alone. More pronounced fibrotic vascular disease and presence of major comorbidities are proposed reasons to explain the absence of response to immunotherapy in SSc-PAH (Le Pavec et al. 2011). Conversely, cases reported before the advent of specific therapies suggested a positive impact of immunosuppressive therapy on the SLE-PAH course (Groen et al. 1993; Kawaguchi et al. 1998; Morelli et al. 1993; Pines et al. 1982). In the same retrospective study from Sanchez et al. (2006), 5 of the 12 (42 %) SLE-PAH were considered as responder under immunosuppressive therapy alone. Later and from the same group, Jais et al. (2008) reported similar findings, with half of the SLE-PAH patients responding clinically and hemodynamically to immunosuppressive therapy. Patients with less severe PAH at the time of diagnosis were more likely to benefit from immunosuppressive therapy. Normalization of hemodynamic parameters was even observed in some patients with SLE-PAH who received immunosuppressive therapy either alone or in combination with PAH-specific treatment (Heresi and Minai 2007; Jais et al. 2008; Ribeiro et al. 2001). Clinical and hemodynamic improvements have also been observed, although less frequently, in patients with PAH associated with mixed CTD (Sanchez et al. 2006). More recently, immunosuppression added to specific PAH therapy has been reported effective in a heterogeneous cohort of 13 CTD-PAH as compared to a historical group of 8 CTD-PAH receiving specific PAH therapy alone (Minai 2009). Unfortunately, repartition of CTD subtypes was different between the two groups (more SLE and less SSc in the “combination” group) limiting the interpretation of these results. Despite the limited data supporting the efficacy of immunosuppressive therapy, current guidelines suggest immunosuppression, most commonly in combination with PAH-specific agents, may be considered in SLE-PAH or mixed CTD-PAH (Jais et al. 2008; Ribeiro et al. 2001).
7.1.3 POEMS Syndrome-Related PAH
POEMS syndrome has been occasionally associated with PAH. Recently, Jouve et al. (2007) described two cases of PAH related to POEMS syndrome, including one case ascribed to PAH and one case of post-capillary/high cardiac output PAH. In any case, clinical symptoms disappear and hemodynamic study showed a significant improvement in both patients (Jouve et al. 2007). Mukerjee et al. (2003a) also reported a single case of reversible POEMS-PAH after sequential therapy including initial iloprost therapy followed by immunosuppressive therapy. Finally, among 20 cases of POEMS syndrome, 5 cases of PAH were reported during the follow-up (Lesprit et al. 1998). Of note, however, PAH was confirmed by catheterization in only two of these patients. Overproduction IL-1β, IL6, TNF-α, and VEGF was found in all cases, suggesting that cytokines may mediate the development of PAH in the POEMS syndrome. However, only two of these five patients presented a sustained improvement under immunosuppressive therapy (Lesprit et al. 1998). Results about the benefit of anti-VEGF were also conflicting (Dispenzieri 2011).
7.2 Side Effects and Drug–Drug Interactions of Immunosuppressive Agents with PAH-Targeted Therapies
Potential side effects and drug–drug interactions were detected using the side effect and drug interactions checker within http://www.drugs.com database (2010). Few data are currently available about the safety profile of immunosuppressive drugs in the setting of PAH. Nevertheless, among the usual side effects of immunosuppressive therapies (Table 1), some are particularly of concern in the setting of PAH. For example, glucocorticoids promote hypokalemia, which may be aggravated by diuretics and may be associated with an increased risk of arrhythmias. CYC and MMF may reduce red blood cells and platelet production. Anemia may be poorly tolerated, especially in PAH patients with low cardiac output. Patients treated with warfarin may also be at increased risk of bleeding in case of thrombocytopenia or CYC-related hemorrhagic cystitis. MMF may also worsen the gastrointestinal disturbance associated with prostanoid therapy. More widely, it is important to keep in mind that all immunosuppressive therapy increases risk of infection. This additional issue should be taken into consideration in the management of PAH patients, especially in those with a central venous line for epoprostenol infusion.
The main concern about drug–drug interaction relates to the cytochrome P450 metabolite pathway. Indeed, both bosentan and CsA are metabolized through the CYP450 3A4 isoenzyme. Coadministration of CsA and bosentan is contraindicated due to significant increased bosentan exposure and decreased CsA exposure (Pharmaceuticals 2011; Venitz et al. 2012). Clinicians should also be cautious if tacrolimus (another calcineurin inhibitor) and bosentan are used together. Conversely, coadministration of ambrisentan and CsA or tacrolimus is not contraindicated, although it is recommended to limit the ambrisentan dose to 5 mg once daily (Spence et al. 2010). Limited data are available for phosphodiesterase 5 inhibitors, which are also primarily metabolized by the CYP450 3A4 pathway (Schwartz and Kloner 2010). Therefore, coadministration with inhibitors of CYP450 3A4 may increase plasma concentrations of sildenafil or tadalafil, and possibility of prolonged and/or increased pharmacologic effects of these drugs should be considered. A Spanish renal transplant study was reassuring as sildenafil therapy was safe for the treatment of erectile dysfunction and did not modify CsA and tacrolimus blood levels (Cofan et al. 2002). MMF is not expected to compete with ambrisentan metabolism (Mandagere et al. 2010). Similarly, CYC is not expected to interact with specific PAH treatments because of its multiple metabolic pathways. Finally, no specific data are available concerning immunosuppressive therapy interactions with prostanoids agents.
8 Conclusion
Inflammation is undoubtedly part of the PAH pathobiology. Giving the poor outcomes in PAH despite recently developed treatments, there is an urgent need for new therapies targeting novel pathophysiological pathways. In many animal models of PAH, targeting the inflammation by current or new immunosuppressive agents improves PAH and pulmonary vascular remodeling. Treating the underlying inflammatory condition in human PAH associated with inflammatory disorders such as SLE, mixed CTD, and POEMS syndrome also led, in some cases, to marked clinical and hemodynamic improvements. Nevertheless, further studies are needed to characterize the elusive mechanisms by which inflammation triggers and sustains vascular remodeling and likely RV failure. More importantly, the poor safety profile of existing immunosuppressive drugs and the potential for drug–drug interactions with current PAH therapies mandate that appropriate large-scaled randomized trials are performed before immunosuppression becomes standard of care in any PAH type.
Abbreviations
- BMPRII:
-
Bone morphogenetic protein receptor 2
- CCL:
-
C-C motif ligand
- CsA:
-
Ciclosporin A
- CTD:
-
Connective tissue disease
- CYC:
-
Cyclophosphamide
- DHEA:
-
Dehydroepiandrosterone
- EC:
-
Endothelial cells
- HAART:
-
Highly active antiretroviral therapy
- HHV-8:
-
Human herpes virus 8
- HIF-1α:
-
Hypoxia inducible factor 1 alpha
- HIV:
-
Human immunodeficiency virus
- IL:
-
Interleukin (i.e., IL-6, IL-2)
- iPAH:
-
Idiopatic pulmonary arterial hypertension
- MCP-1:
-
Monocyte chemotactic protein 1
- MCT:
-
Monocrotaline (induced PAH)
- MIP-1α:
-
Macrophage inflammatory protein 1 alpha
- MMF:
-
Mycophenolate mofetil
- MTX:
-
Methotrexate
- NFAT:
-
Nuclear factor for activated T cells
- NF-κB:
-
Nuclear factor kappa-light-chain-enhancer of activated B cells
- PA:
-
Pulmonary artery
- PAH:
-
Pulmonary arterial hypertension
- PASMC:
-
Pulmonary artery smooth muscle cells
- PDGF:
-
Platelet-derived growth factor
- PH:
-
Pulmonary hypertension
- RANTES:
-
Regulated upon activation normal T cell expressed and secreted
- RV:
-
Right ventricle/ventricular
- SLE:
-
Systemic lupus erythematosus
- SSc:
-
Systemic scleroderma
- Tc:
-
Cytotoxic T lymphocytes
- Th:
-
Helper T lymphocytes
- TNF-α:
-
Tumor necrosis factor alpha
- Treg:
-
Regulatory T lymphocytes
- VEGF:
-
Vascular endothelial growth factor
References
Actelion Pharmaceuticals (2011) Tracleer [package insert]. Actelion Pharmaceuticals US, Inc., South San Francisco, CA
Aramburu J, Yaffe MB, Lopez-Rodriguez C et al (1999) Affinity-driven peptide selection of an NFAT inhibitor more selective than cyclosporin A. Science 285:2129–2133
Arends SJ, Damoiseaux J, Duijvestijn A et al (2010) Prevalence of anti-endothelial cell antibodies in idiopathic pulmonary arterial hypertension. Eur Respir J 35:923–925
Ascherl G, Hohenadl C, Schatz O et al (1999) Infection with human immunodeficiency virus-1 increases expression of vascular endothelial cell growth factor in T cells: implications for acquired immunodeficiency syndrome-associated vasculopathy. Blood 93:4232–4241
Asherson RA (1990) Pulmonary hypertension in systemic lupus erythematosus. J Rheumatol 17:414–415
Asherson RA, Oakley CM (1986) Pulmonary hypertension and systemic lupus erythematosus. J Rheumatol 13:1–5
Badesch DB, Champion HC, Sanchez MA et al (2009) Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol 54:S55–S66
Balabanian K, Foussat A, Dorfmuller P et al (2002) CX(3)C chemokine fractalkine in pulmonary arterial hypertension. Am J Respir Crit Care Med 165:1419–1425
Barile-Fabris L, Ariza-Andraca R, Olguin-Ortega L et al (2005) Controlled clinical trial of IV cyclophosphamide versus IV methylprednisolone in severe neurological manifestations in systemic lupus erythematosus. Ann Rheum Dis 64:620–625
Barnier A, Frachon I, Dewilde J et al (2009) Improvement of HIV-related pulmonary hypertension after the introduction of an antiretroviral therapy. Eur Respir J 34:277–278
Barrier M, Meloche J, Jacob MH et al (2012) Today’s and tomorrow’s imaging and circulating biomarkers for pulmonary arterial hypertension. Cell Mol Life Sci 69(17):2805–2831
Bellotto F, Chiavacci P, Laveder F et al (1999) Effective immunosuppressive therapy in a patient with primary pulmonary hypertension. Thorax 54:372–374
Bendayan D, Sarid R, Cohen A et al (2008) Absence of human herpesvirus 8 DNA sequences in lung biopsies from Israeli patients with pulmonary arterial hypertension. Respiration 75:155–157
Bertsias G, Ioannidis JP, Boletis J et al (2008) EULAR recommendations for the management of systemic lupus erythematosus. Report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics. Ann Rheum Dis 67:195–205
Bhargava A, Kumar A, Yuan N et al (1999) Monocrotaline induces interleukin-6 mRNA expression in rat lungs. Heart Dis 1:126–132
Blyth KG, Groenning BA, Mark PB et al (2007) NT-proBNP can be used to detect right ventricular systolic dysfunction in pulmonary hypertension. Eur Respir J 29:737–744
Bogaard HJ, Abe K, Vonk Noordegraaf A et al (2009a) The right ventricle under pressure: cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest 135:794–804
Bogaard HJ, Natarajan R, Henderson SC et al (2009b) Chronic pulmonary artery pressure elevation is insufficient to explain right heart failure. Circulation 120:1951–1960
Bokhari S, Raina A, Rosenweig EB et al (2011) PET imaging may provide a novel biomarker and understanding of right ventricular dysfunction in patients with idiopathic pulmonary arterial hypertension. Circ Cardiovasc Imaging 4:641–647
Bonnet S, Rochefort G, Sutendra G et al (2007) The nuclear factor of activated T cells in pulmonary arterial hypertension can be therapeutically targeted. Proc Natl Acad Sci USA 104:11418–11423
Bouree P, Piveteau J, Gerbal JL et al (1990) Pulmonary arterial hypertension due to bilharziasis. Apropos of a case due to Schistosoma haematobium having been cured by praziquantel. Bull Soc Pathol Exot 83:66–71
Brode S, Cooke A (2008) Immune-potentiating effects of the chemotherapeutic drug cyclophosphamide. Crit Rev Immunol 28:109–126
Bull TM, Cool CD, Serls AE et al (2003) Primary pulmonary hypertension, Castleman’s disease and human herpesvirus-8. Eur Respir J 22:403–407
Butrous G, Ghofrani HA, Grimminger F (2008) Pulmonary vascular disease in the developing world. Circulation 118:1758–1766
Can MM, Kaymaz C, Tanboga IH et al (2011) Increased right ventricular glucose metabolism in patients with pulmonary arterial hypertension. Clin Nucl Med 36:743–748
Carneiro JR, Sato EI (1999) Double blind, randomized, placebo controlled clinical trial of methotrexate in systemic lupus erythematosus. J Rheumatol 26:1275–1279
Cerinic MM, Valentini G, Sorano GG et al (2003) Blood coagulation, fibrinolysis, and markers of endothelial dysfunction in systemic sclerosis. Semin Arthritis Rheum 32:285–295
Chizzolini C, Raschi E, Rezzonico R et al (2002) Autoantibodies to fibroblasts induce a proadhesive and proinflammatory fibroblast phenotype in patients with systemic sclerosis. Arthritis Rheum 46:1602–1613
Chu JW, Kao PN, Faul JL et al (2002) High prevalence of autoimmune thyroid disease in pulmonary arterial hypertension. Chest 122:1668–1673
Chung L, Liu J, Parsons L et al (2010) Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest 138:1383–1394
Clements PJ, Lachenbruch PA, Sterz M et al (1993) Cyclosporine in systemic sclerosis. Results of a forty-eight-week open safety study in ten patients. Arthritis Rheum 36:75–83
Cofan F, Gutierrez R, Beardo P et al (2002) Interaction between sildenafil and calcineurin inhibitors in renal transplant recipients with erectile dysfunction. Nefrologia 22:470–476
Coker RK (2007) Guidelines for the use of corticosteroids in the treatment of pulmonary sarcoidosis. Drugs 67:1139–1147
Condliffe R, Kiely DG, Peacock AJ et al (2009) Connective tissue disease-associated pulmonary arterial hypertension in the modern treatment era. Am J Respir Crit Care Med 179:151–157
Conejo-Garcia JR, Benencia F, Courreges MC et al (2004) Tumor-infiltrating dendritic cell precursors recruited by a beta-defensin contribute to vasculogenesis under the influence of Vegf-A. Nat Med 10:950–958
Contreras G, Pardo V, Leclercq B et al (2004) Sequential therapies for proliferative lupus nephritis. N Engl J Med 350:971–980
Cool CD, Kennedy D, Voelkel NF et al (1997) Pathogenesis and evolution of plexiform lesions in pulmonary hypertension associated with scleroderma and human immunodeficiency virus infection. Hum Pathol 28:434–442
Cool CD, Rai PR, Yeager ME et al (2003) Expression of human herpesvirus 8 in primary pulmonary hypertension. N Engl J Med 349:1113–1122
Crosby A, Jones FM, Southwood M et al (2010) Pulmonary vascular remodeling correlates with lung eggs and cytokines in murine schistosomiasis. Am J Respir Crit Care Med 181:279–288
Crosby A, Jones FM, Kolosionek E et al (2011) Praziquantel reverses pulmonary hypertension and vascular remodeling in murine schistosomiasis. Am J Respir Crit Care Med 184:467–473
Daley E, Emson C, Guignabert C et al (2008) Pulmonary arterial remodeling induced by a Th2 immune response. J Exp Med 205:361–372
de Almeida MA, Andrade ZA (1983) Effect of chemotherapy on experimental pulmonary schistosomiasis. Am J Trop Med Hyg 32:1049–1054
Deng Z, Morse JH, Slager SL et al (2000) Familial primary pulmonary hypertension (gene PPH1) is caused by mutations in the bone morphogenetic protein receptor-II gene. Am J Hum Genet 67:737–744
Denton CP, Sweny P, Abdulla A et al (1994) Acute renal failure occurring in scleroderma treated with cyclosporin A: a report of three cases. Br J Rheumatol 33:90–92
Derk CT, Grace E, Shenin M et al (2009) A prospective open-label study of mycophenolate mofetil for the treatment of diffuse systemic sclerosis. Rheumatology (Oxford) 48:1595–1599
Dib H, Tamby MC, Bussone G et al (2011) Targets of anti-endothelial cell antibodies in pulmonary hypertension and scleroderma. Eur Respir J 39(6):1405–1414
Diller GP, van Eijl S, Okonko DO et al (2008) Circulating endothelial progenitor cells in patients with Eisenmenger syndrome and idiopathic pulmonary arterial hypertension. Circulation 117:3020–3030
Dispenzieri A (2011) POEMS syndrome: 2011 update on diagnosis, risk-stratification, and management. Am J Hematol 86:591–601
Dorfmuller P, Zarka V, Durand-Gasselin I et al (2002) Chemokine RANTES in severe pulmonary arterial hypertension. Am J Respir Crit Care Med 165:534–539
Dorfmuller P, Perros F, Balabanian K et al (2003) Inflammation in pulmonary arterial hypertension. Eur Respir J 22:358–363
Dorfmuller P, Humbert M, Perros F et al (2007) Fibrous remodeling of the pulmonary venous system in pulmonary arterial hypertension associated with connective tissue diseases. Hum Pathol 38:893–902
dos Santos Fernandes CJ, Jardim CV, Hovnanian A et al (2010) Survival in schistosomiasis-associated pulmonary arterial hypertension. J Am Coll Cardiol 56:715–720
Drake JI, Bogaard HJ, Mizuno S et al (2011) Molecular signature of a right heart failure program in chronic severe pulmonary hypertension. Am J Respir Cell Mol Biol 45:1239–1247
Drugs.com (2010) Side effects and drug-drug interaction. Denver, CO. http://www.drugs.com, Updated: 2010
Efferth T, Schwarzl SM, Smith J et al (2006) Role of glucose-6-phosphate dehydrogenase for oxidative stress and apoptosis. Cell Death Differ 13:527–528, author reply 529–530
Ehrenreich H, Rieckmann P, Sinowatz F et al (1993) Potent stimulation of monocytic endothelin-1 production by HIV-1 glycoprotein 120. J Immunol 150:4601–4609
Ensoli B, Barillari G, Salahuddin SZ et al (1990) Tat protein of HIV-1 stimulates growth of cells derived from Kaposi’s sarcoma lesions of AIDS patients. Nature 345:84–86
Fagan KA, Badesch DB (2002) Pulmonary hypertension associated with connective tissue disease. Prog Cardiovasc Dis 45:225–234
Fartoukh M, Emilie D, Le Gall C et al (1998) Chemokine macrophage inflammatory protein-1alpha mRNA expression in lung biopsy specimens of primary pulmonary hypertension. Chest 114:50S–51S
Fernandes CJ, Jardim CV, Hovnanian A et al (2011) Schistosomiasis and pulmonary hypertension. Expert Rev Respir Med 5:675–681
Filaci G, Cutolo M, Scudeletti M et al (1999) Cyclosporin A and iloprost treatment of systemic sclerosis: clinical results and interleukin-6 serum changes after 12 months of therapy. Rheumatology (Oxford) 38:992–996
Fois E, Le Guern V, Dupuy A et al (2010) Noninvasive assessment of systolic pulmonary artery pressure in systemic lupus erythematosus: retrospective analysis of 93 patients. Clin Exp Rheumatol 28:836–841
Freitas TC, Jung E, Pearce EJ (2007) TGF-beta signaling controls embryo development in the parasitic flatworm Schistosoma mansoni. PLoS Pathog 3:e52
Fritzler MJ, Hart DA, Wilson D et al (1995) Antibodies to fibrin bound tissue type plasminogen activator in systemic sclerosis. J Rheumatol 22:1688–1693
Fujita M, Shannon JM, Irvin CG et al (2001) Overexpression of tumor necrosis factor-alpha produces an increase in lung volumes and pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 280:L39–L49
Galie N, Hoeper MM, Humbert M et al (2009) Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 30:2493–2537
Gan CT, McCann GP, Marcus JT et al (2006) NT-proBNP reflects right ventricular structure and function in pulmonary hypertension. Eur Respir J 28:1190–1194
Gerasimovskaya EV, Kratzer A, Sidiakova A et al (2012) Interplay of macrophages and T cells in the lung vasculature. Am J Physiol Lung Cell Mol Physiol 302(10):L1014–L1022
Gerbino AJ, Goss CH, Molitor JA (2008) Effect of mycophenolate mofetil on pulmonary function in scleroderma-associated interstitial lung disease. Chest 133:455–460
Goppelt-Struebe M, Wolter D, Resch K (1989) Glucocorticoids inhibit prostaglandin synthesis not only at the level of phospholipase A2 but also at the level of cyclo-oxygenase/PGE isomerase. Br J Pharmacol 98:1287–1295
Gourh P, Arnett FC, Assassi S et al (2009) Plasma cytokine profiles in systemic sclerosis: associations with autoantibody subsets and clinical manifestations. Arthritis Res Ther 11:R147
Graham BB, Bandeira AP, Morrell NW et al 2010) Schistosomiasis-associated pulmonary hypertension: pulmonary vascular disease: the global perspective. Chest 137:20S–29S
Grigolo B, Mazzetti I, Meliconi R et al (2000) Anti-topoisomerase II alpha autoantibodies in systemic sclerosis-association with pulmonary hypertension and HLA-B35. Clin Exp Immunol 121:539–543
Grinyo JM, Cruzado JM, Millan O et al (2004) Low-dose cyclosporine with mycophenolate mofetil induces similar calcineurin activity and cytokine inhibition as does standard-dose cyclosporine in stable renal allografts. Transplantation 78:1400–1403
Groen H, Bootsma H, Postma DS et al (1993) Primary pulmonary hypertension in a patient with systemic lupus erythematosus: partial improvement with cyclophosphamide. J Rheumatol 20:1055–1057
Guignabert C, Izikki M, Tu LI et al (2006) Transgenic mice overexpressing the 5-hydroxytryptamine transporter gene in smooth muscle develop pulmonary hypertension. Circ Res 98:1323–1330
Guignabert C, Tu L, Izikki M et al (2009) Dichloroacetate treatment partially regresses established pulmonary hypertension in mice with SM22alpha-targeted overexpression of the serotonin transporter. FASEB J 23:4135–4147
Hachulla E, Gressin V, Guillevin L et al (2005) Early detection of pulmonary arterial hypertension in systemic sclerosis: a French nationwide prospective multicenter study. Arthritis Rheum 52:3792–3800
Hachulla AL, Launay D, Gaxotte V et al (2009) Cardiac magnetic resonance imaging in systemic sclerosis: a cross-sectional observational study of 52 patients. Ann Rheum Dis 68:1878–1884
Hagen M, Fagan K, Steudel W et al (2007) Interaction of interleukin-6 and the BMP pathway in pulmonary smooth muscle. Am J Physiol Lung Cell Mol Physiol 292:L1473–L1479
Hall S, Brogan P, Haworth SG et al (2009) Contribution of inflammation to the pathology of idiopathic pulmonary arterial hypertension in children. Thorax 64:778–783
Hamada H, Terai M, Kimura H et al (1999) Increased expression of mast cell chymase in the lungs of patients with congenital heart disease associated with early pulmonary vascular disease. Am J Respir Crit Care Med 160:1303–1308
Hammer SM, Eron JJ Jr, Reiss P et al (2008) Antiretroviral treatment of adult HIV infection: 2008 recommendations of the International AIDS Society-USA panel. JAMA 300:555–570
Hassoun PM (2009) Pulmonary arterial hypertension complicating connective tissue diseases. Semin Respir Crit Care Med 30:429–439
Hassoun PM, Mouthon L, Barbera JA et al (2009) Inflammation, growth factors, and pulmonary vascular remodeling. J Am Coll Cardiol 54:S10–S19
Heath D, Yacoub M (1991) Lung mast cells in plexogenic pulmonary arteriopathy. J Clin Pathol 44:1003–1006
Heldin CH (1992) Structural and functional studies on platelet-derived growth factor. EMBO J 11:4251–4259
Henke-Gendo C, Mengel M, Hoeper MM et al (2005) Absence of Kaposi’s sarcoma-associated herpesvirus in patients with pulmonary arterial hypertension. Am J Respir Crit Care Med 172:1581–1585
Henriques-Coelho T, Brandao-Nogueira A, Moreira-Goncalves D et al (2008) Effects of TNF-alpha blockade in monocrotaline-induced pulmonary hypertension. Rev Port Cardiol 27:341–348
Heresi GA, Minai OA (2007) Lupus-associated pulmonary hypertension: long-term response to vasoactive therapy. Respir Med 101:2099–2107
Hoeper MM, Oudiz RJ, Peacock A et al (2004) End points and clinical trial designs in pulmonary arterial hypertension: clinical and regulatory perspectives. J Am Coll Cardiol 43:48S–55S
Hoyles RK, Ellis RW, Wellsbury J et al (2006) A multicenter, prospective, randomized, double-blind, placebo-controlled trial of corticosteroids and intravenous cyclophosphamide followed by oral azathioprine for the treatment of pulmonary fibrosis in scleroderma. Arthritis Rheum 54:3962–3970
Hsue PY, Deeks SG, Farah HH et al (2008) Role of HIV and human herpesvirus-8 infection in pulmonary arterial hypertension. AIDS 22:825–833
Huertas A, Tu L, Gambaryan N et al (2012) Leptin and regulatory T lymphocytes in idiopathic pulmonary arterial hypertension. Eur Respir J 40(4):895–904
Humbert M (2008) Mediators involved in HIV-related pulmonary arterial hypertension. AIDS 22(Suppl 3):S41–S47
Humbert M, Monti G, Brenot F et al (1995) Increased interleukin-1 and interleukin-6 serum concentrations in severe primary pulmonary hypertension. Am J Respir Crit Care Med 151:1628–1631
Humbert M, Monti G, Fartoukh M et al (1998) Platelet-derived growth factor expression in primary pulmonary hypertension: comparison of HIV seropositive and HIV seronegative patients. Eur Respir J 11:554–559
Humbert M, Morrell NW, Archer SL et al (2004) Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol 43:13S–24S
Imaizumi T, Yoshida H, Satoh K (2004) Regulation of CX3CL1/fractalkine expression in endothelial cells. J Atheroscler Thromb 11:15–21
Jais X, Launay D, Yaici A et al (2008) Immunosuppressive therapy in lupus- and mixed connective tissue disease-associated pulmonary arterial hypertension: a retrospective analysis of twenty-three cases. Arthritis Rheum 58:521–531
Jouve P, Humbert M, Chauveheid MP et al (2007) POEMS syndrome-related pulmonary hypertension is steroid-responsive. Respir Med 101:353–355
Karmochkine M, Wechsler B, Godeau P et al (1996) Improvement of severe pulmonary hypertension in a patient with SLE. Ann Rheum Dis 55:561–562
Katayose D, Ohe M, Yamauchi K et al (1993) Increased expression of PDGF A- and B-chain genes in rat lungs with hypoxic pulmonary hypertension. Am J Physiol 264:L100–L106
Kawaguchi Y, Hara M, Harigai M et al (1998) Corticosteroid pulse therapy in a patient with SLE and pulmonary hypertension. Clin Exp Rheumatol 16:510
Kawut SM, Taichman DB, Archer-Chicko CL et al (2003) Hemodynamics and survival in patients with pulmonary arterial hypertension related to systemic sclerosis. Chest 123:344–350
Kherbeck N, Tamby MC, Bussone G et al (2011) The role of inflammation and autoimmunity in the pathophysiology of pulmonary arterial hypertension. Clin Rev Allergy Immunol 44(1):31–38
King CH (2010) Parasites and poverty: the case of schistosomiasis. Acta Trop 113:95–104
Kobayashi T, Momoi Y, Iwasaki T (2007) Cyclosporine A inhibits the mRNA expressions of IL-2, IL-4 and IFN-gamma, but not TNF-alpha, in canine mononuclear cells. J Vet Med Sci 69:887–892
Koebel CM, Vermi W, Swann JB et al (2007) Adaptive immunity maintains occult cancer in an equilibrium state. Nature 450:903–907
Koulmann N, Novel-Chate V, Peinnequin A et al (2006) Cyclosporin A inhibits hypoxia-induced pulmonary hypertension and right ventricle hypertrophy. Am J Respir Crit Care Med 174:699–705
Kowal-Bielecka O, Landewe R, Avouac J et al (2009) EULAR recommendations for the treatment of systemic sclerosis: a report from the EULAR Scleroderma Trials and Research group (EUSTAR). Ann Rheum Dis 68:620–628
Labarrere CA, Zaloga GP (2004) C-reactive protein: from innocent bystander to pivotal mediator of atherosclerosis. Am J Med 117:499–507
Lambertucci JR, Serufo JC, Gerspacher-Lara R et al (2000) Schistosoma mansoni: assessment of morbidity before and after control. Acta Trop 77:101–109
Lane KB, Machado RD, Pauciulo MW et al (2000) Heterozygous germline mutations in BMPR2, encoding a TGF-beta receptor, cause familial primary pulmonary hypertension. Nat Genet 26:81–84
Lapa M, Dias B, Jardim C et al (2009) Cardiopulmonary manifestations of hepatosplenic schistosomiasis. Circulation 119:1518–1523
Launay D, Souza R, Guillevin L et al (2006) Pulmonary arterial hypertension in ANCA-associated vasculitis. Sarcoidosis Vasc Diffuse Lung Dis 23:223–228
Launay D, Hachulla E, Hatron PY et al (2007) Pulmonary arterial hypertension: a rare complication of primary Sjogren syndrome: report of 9 new cases and review of the literature. Medicine (Baltimore) 86:299–315
Le Pavec J, Humbert M, Mouthon L et al (2011) Systemic sclerosis-associated pulmonary arterial hypertension. Am J Respir Crit Care Med 181:1285–1293
Lesprit P, Godeau B, Authier FJ et al (1998) Pulmonary hypertension in POEMS syndrome: a new feature mediated by cytokines. Am J Respir Crit Care Med 157:907–911
Leung DY, Bloom JW (2003) Update on glucocorticoid action and resistance. J Allergy Clin Immunol 111:3–22, quiz 23
Lorenzen JM, Nickel N, Kramer R et al (2011) Osteopontin in patients with idiopathic pulmonary hypertension. Chest 139:1010–1017
Lovell DJ, Giannini EH, Reiff A et al (2000) Etanercept in children with polyarticular juvenile rheumatoid arthritis. Pediatric Rheumatology Collaborative Study Group. N Engl J Med 342:763–769
Luster AD (1998) Chemokines – chemotactic cytokines that mediate inflammation. N Engl J Med 338:436–445
Machado RD, Pauciulo MW, Thomson JR et al (2001) BMPR2 haploinsufficiency as the inherited molecular mechanism for primary pulmonary hypertension. Am J Hum Genet 68:92–102
Macian F (2005) NFAT proteins: key regulators of T-cell development and function. Nat Rev Immunol 5:472–484
Mandagere A, Core B, Bird S, Bingham J, Boinpally R (2010) Absence of a clinically relevant pharmacokinetic interaction between ambrisentan and mycophenolate mofetil. In: American Journal of Respiratory and Critical Care Medicine. American Thoracic Society International Conference, New Orleans, LA, USA
Manno R, Boin F (2010) Immunotherapy of systemic sclerosis. Immunotherapy 2:863–878
Marder W, McCune WJ (2007) Advances in immunosuppressive therapy. Semin Respir Crit Care Med 28:398–417
Mathai SC, Hassoun PM (2011) Pulmonary arterial hypertension associated with systemic sclerosis. Expert Rev Respir Med 5:267–279
Mathai SC, Hummers LK, Champion HC et al (2009) Survival in pulmonary hypertension associated with the scleroderma spectrum of diseases: impact of interstitial lung disease. Arthritis Rheum 60:569–577
McCune WJ, Golbus J, Zeldes W et al (1988) Clinical and immunologic effects of monthly administration of intravenous cyclophosphamide in severe systemic lupus erythematosus. N Engl J Med 318:1423–1431
McKinsey TA, Olson EN (2005) Toward transcriptional therapies for the failing heart: chemical screens to modulate genes. J Clin Invest 115:538–546
McMurtry MS, Bonnet S, Wu X et al (2004) Dichloroacetate prevents and reverses pulmonary hypertension by inducing pulmonary artery smooth muscle cell apoptosis. Circ Res 95:830–840
McMurtry MS, Bonnet S, Michelakis ED et al (2007) Statin therapy, alone or with rapamycin, does not reverse monocrotaline pulmonary arterial hypertension: the rapamycin-atorvastatin-simvastatin study. Am J Physiol Lung Cell Mol Physiol 293:L933–L940
Mehta NJ, Khan IA, Mehta RN et al (2000) HIV-Related pulmonary hypertension: analytic review of 131 cases. Chest 118:1133–1141
Michelakis ED, McMurtry MS, Wu XC et al (2002) Dichloroacetate, a metabolic modulator, prevents and reverses chronic hypoxic pulmonary hypertension in rats: role of increased expression and activity of voltage-gated potassium channels. Circulation 105:244–250
Minai OA (2009) Pulmonary hypertension in polymyositis-dermatomyositis: clinical and hemodynamic characteristics and response to vasoactive therapy. Lupus 18:1006–1010
Montani D, Achouh L, Marcelin AG et al (2005a) Reversibility of pulmonary arterial hypertension in HIV/HHV8-associated Castleman’s disease. Eur Respir J 26:969–972
Montani D, Marcelin AG, Sitbon O et al (2005b) Human herpes virus 8 in HIV and non-HIV infected patients with pulmonary arterial hypertension in France. AIDS 19:1239–1240
Montani D, Humbert M, Souza R (2011) Letter by Montani et al regarding article, “Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension”. Circulation 123:e614, author reply e615
Morelli S, Giordano M, De Marzio P et al (1993) Pulmonary arterial hypertension responsive to immunosuppressive therapy in systemic lupus erythematosus. Lupus 2:367–369
Morse JH, Barst RJ, Fotino M et al (1997) Primary pulmonary hypertension, tissue plasminogen activator antibodies, and HLA-DQ7. Am J Respir Crit Care Med 155:274–278
Mouthon L, Guillevin L, Humbert M (2005) Pulmonary arterial hypertension: an autoimmune disease? Eur Respir J 26:986–988
Mukerjee D, Kingdon E, Vanderpump M et al (2003a) Pathophysiological insights from a case of reversible pulmonary arterial hypertension. J R Soc Med 96:403–404
Mukerjee D, St George D, Coleiro B et al (2003b) Prevalence and outcome in systemic sclerosis associated pulmonary arterial hypertension: application of a registry approach. Ann Rheum Dis 62:1088–1093
Mutschler D, Wikstrom G, Lind L et al (2006) Etanercept reduces late endotoxin-induced pulmonary hypertension in the pig. J Interferon Cytokine Res 26:661–667
Nadashkevich O, Davis P, Fritzler M et al (2006) A randomized unblinded trial of cyclophosphamide versus azathioprine in the treatment of systemic sclerosis. Clin Rheumatol 25:205–212
Nagaya N, Nishikimi T, Uematsu M et al (2000) Plasma brain natriuretic peptide as a prognostic indicator in patients with primary pulmonary hypertension. Circulation 102:865–870
Nannini C, West CP, Erwin PJ et al (2008) Effects of cyclophosphamide on pulmonary function in patients with scleroderma and interstitial lung disease: a systematic review and meta-analysis of randomized controlled trials and observational prospective cohort studies. Arthritis Res Ther 10:R124
Nathan C (2002) Points of control in inflammation. Nature 420:846–852
Negi VS, Tripathy NK, Misra R et al (1998) Antiendothelial cell antibodies in scleroderma correlate with severe digital ischemia and pulmonary arterial hypertension. J Rheumatol 25:462–466
Nicolls MR, Taraseviciene-Stewart L, Rai PR et al (2005) Autoimmunity and pulmonary hypertension: a perspective. Eur Respir J 26:1110–1118
Nishimura T, Faul JL, Berry GJ et al (2001) 40-O-(2-hydroxyethyl)-rapamycin attenuates pulmonary arterial hypertension and neointimal formation in rats. Am J Respir Crit Care Med 163:498–502
Niu X, Nouraie M, Campbell A et al (2009) Angiogenic and inflammatory markers of cardiopulmonary changes in children and adolescents with sickle cell disease. PLoS One 4:e7956
Nunes H, Humbert M, Sitbon O et al (2003) Prognostic factors for survival in human immunodeficiency virus-associated pulmonary arterial hypertension. Am J Respir Crit Care Med 167:1433–1439
Nunes H, Humbert M, Capron F et al (2006) Pulmonary hypertension associated with sarcoidosis: mechanisms, haemodynamics and prognosis. Thorax 61:68–74
Ogawa A, Nakamura K, Matsubara H et al (2005) Prednisolone inhibits proliferation of cultured pulmonary artery smooth muscle cells of patients with idiopathic pulmonary arterial hypertension. Circulation 112:1806–1812
Ogawa A, Nakamura K, Mizoguchi H et al (2011) Prednisolone ameliorates idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 183:139–140
Okano Y, Steen VD, Medsger TA Jr (1992) Autoantibody to U3 nucleolar ribonucleoprotein (fibrillarin) in patients with systemic sclerosis. Arthritis Rheum 35:95–100
Opravil M, Sereni D (2008) Natural history of HIV-associated pulmonary arterial hypertension: trends in the HAART era. AIDS 22(Suppl 3):S35–S40
Opravil M, Pechere M, Speich R et al (1997) HIV-associated primary pulmonary hypertension. A case control study. Swiss HIV Cohort Study. Am J Respir Crit Care Med 155:990–995
Overbeek MJ, Lankhaar JW, Westerhof N et al (2008) Right ventricular contractility in systemic sclerosis-associated and idiopathic pulmonary arterial hypertension. Eur Respir J 31:1160–1166
Palucka AK, Blanck JP, Bennett L et al (2005) Cross-regulation of TNF and IFN-alpha in autoimmune diseases. Proc Natl Acad Sci USA 102:3372–3377
Paulin R, Meloche J, Jacob MH et al (2011) Dehydroepiandrosterone inhibits the Src/STAT3 constitutive activation in pulmonary arterial hypertension. Am J Physiol Heart Circ Physiol 301:H1798–H1809
Pellicelli AM, Palmieri F, D’Ambrosio C et al (1998) Role of human immunodeficiency virus in primary pulmonary hypertension – case reports. Angiology 49:1005–1011
Perros F, Dorfmuller P, Souza R et al (2007) Dendritic cell recruitment in lesions of human and experimental pulmonary hypertension. Eur Respir J 29:462–468
Perros F, Montani D, Dorfmuller P et al (2011) [Novel immunopathological approaches to pulmonary arterial hypertension]. Presse Med 40(Suppl 1):1S3–1S13
Perros F, Dorfmuller P, Montani D et al (2012) Pulmonary lymphoid neogenesis in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 185:311–321
Piao L, Fang YH, Cadete VJ et al (2010a) The inhibition of pyruvate dehydrogenase kinase improves impaired cardiac function and electrical remodeling in two models of right ventricular hypertrophy: resuscitating the hibernating right ventricle. J Mol Med (Berl) 88:47–60
Piao L, Marsboom G, Archer SL (2010b) Mitochondrial metabolic adaptation in right ventricular hypertrophy and failure. J Mol Med (Berl) 88:1011–1020
Pines A, Kaplinsky N, Goldhammer E et al (1982) Corticosteroid responsive pulmonary hypertension in systemic lupus erythematosus. Clin Rheumatol 1:301–304
Pope J (2008) An update in pulmonary hypertension in systemic lupus erythematosus – do we need to know about it? Lupus 17:274–277
Pope JE, Bellamy N, Seibold JR et al (2001) A randomized, controlled trial of methotrexate versus placebo in early diffuse scleroderma. Arthritis Rheum 44:1351–1358
Price LC, Montani D, Tcherakian C et al (2011) Dexamethasone reverses monocrotaline-induced pulmonary arterial hypertension in rats. Eur Respir J 37:813–822
Price LC, Wort SJ, Perros F et al (2012) Inflammation in pulmonary arterial hypertension. Chest 141:210–221
Pullamsetti SS, Savai R, Janssen W et al (2011) Inflammation, immunological reaction and role of infection in pulmonary hypertension. Clin Microbiol Infect 17:7–14
Quarck R, Nawrot T, Meyns B et al (2009) C-reactive protein: a new predictor of adverse outcome in pulmonary arterial hypertension. J Am Coll Cardiol 53:1211–1218
Quismorio FP Jr, Sharma O, Koss M et al (1984) Immunopathologic and clinical studies in pulmonary hypertension associated with systemic lupus erythematosus. Semin Arthritis Rheum 13:349–359
Rhen T, Cidlowski JA (2005) Antiinflammatory action of glucocorticoids – new mechanisms for old drugs. N Engl J Med 353:1711–1723
Ribeiro JM, Lucas M, Victorino RM (2001) Remission of precapillary pulmonary hypertension in systemic lupus erythematosus. J R Soc Med 94:32–33
Rich S, Kieras K, Hart K et al (1986) Antinuclear antibodies in primary pulmonary hypertension. J Am Coll Cardiol 8:1307–1311
Ross AG, Bartley PB, Sleigh AC et al (2002) Schistosomiasis. N Engl J Med 346:1212–1220
Rubin LJ (1997) Primary pulmonary hypertension. N Engl J Med 336:111–117
Ryan J, Bloch K, Archer SL (2011) Rodent models of pulmonary hypertension: harmonisation with the world health organisation’s categorisation of human PH. Int J Clin Pract Suppl (172):15–34
Salojin KV, Bordron A, Nassonov EL et al (1997) Anti-endothelial cell antibody, thrombomodulin, and von Willebrand factor in idiopathic inflammatory myopathies. Clin Diagn Lab Immunol 4:519–521
Sanchez O, Sitbon O, Jais X et al (2006) Immunosuppressive therapy in connective tissue diseases-associated pulmonary arterial hypertension. Chest 130:182–189
Sanchez O, Marcos E, Perros F et al (2007) Role of endothelium-derived CC chemokine ligand 2 in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 176:1041–1047
Savale L, Tu L, Rideau D et al (2009) Impact of interleukin-6 on hypoxia-induced pulmonary hypertension and lung inflammation in mice. Respir Res 10:6
Schall TJ, Bacon K, Toy KJ et al (1990) Selective attraction of monocytes and T lymphocytes of the memory phenotype by cytokine RANTES. Nature 347:669–671
Schall TJ, Bacon K, Camp RD et al (1993) Human macrophage inflammatory protein alpha (MIP-1 alpha) and MIP-1 beta chemokines attract distinct populations of lymphocytes. J Exp Med 177:1821–1826
Schermuly RT, Dony E, Ghofrani HA et al (2005) Reversal of experimental pulmonary hypertension by PDGF inhibition. J Clin Invest 115:2811–2821
Schwartz BG, Kloner RA (2010) Drug interactions with phosphodiesterase-5 inhibitors used for the treatment of erectile dysfunction or pulmonary hypertension. Circulation 122:88–95
Scirica BM, Morrow DA (2006) Is C-reactive protein an innocent bystander or proatherogenic culprit? The verdict is still out. Circulation 113:2128–2134, discussion 2151
Sgonc R, Gruschwitz MS, Boeck G et al (2000) Endothelial cell apoptosis in systemic sclerosis is induced by antibody-dependent cell-mediated cytotoxicity via CD95. Arthritis Rheum 43:2550–2562
Shibasaki F, Fukami K, Fukui Y et al (1994) Phosphatidylinositol 3-kinase binds to alpha-actinin through the p85 subunit. Biochem J 302(Pt 2):551–557
Simonneau G, Robbins IM, Beghetti M et al (2009) Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 54:S43–S54
Sitbon O, Lascoux-Combe C, Delfraissy JF et al (2008) Prevalence of HIV-related pulmonary arterial hypertension in the current antiretroviral therapy era. Am J Respir Crit Care Med 177:108–113
Song Y, Coleman L, Shi J et al (2008) Inflammation, endothelial injury, and persistent pulmonary hypertension in heterozygous BMPR2-mutant mice. Am J Physiol Heart Circ Physiol 295:H677–H690
Soon E, Holmes AM, Treacy CM et al (2010) Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension. Circulation 122:920–927
Speich R, Boehler A, Rochat T et al (2000) Cystic fibrosis: current therapy. Indications for lung transplantation. Schweiz Med Wochenschr Suppl 122:57S–58S
Spence R, Mandagere A, Richards DB et al (2010) Potential for pharmacokinetic interactions between ambrisentan and cyclosporine. Clin Pharmacol Ther 88:513–520
Steen VD (2005) Autoantibodies in systemic sclerosis. Semin Arthritis Rheum 35:35–42
Steiner MK, Syrkina OL, Kolliputi N et al (2009) Interleukin-6 overexpression induces pulmonary hypertension. Circ Res 104:236–244, 228p following 244
Stojanovich L, Stojanovich R, Kostich V et al (2003) Neuropsychiatric lupus favourable response to low dose i.v. cyclophosphamide and prednisolone (pilot study). Lupus 12:3–7
Sutendra G, Dromparis P, Bonnet S et al (2011) Pyruvate dehydrogenase inhibition by the inflammatory cytokine TNFalpha contributes to the pathogenesis of pulmonary arterial hypertension. J Mol Med (Berl) 89:771–783
Suzuki C, Takahashi M, Morimoto H et al (2006) Mycophenolate mofetil attenuates pulmonary arterial hypertension in rats. Biochem Biophys Res Commun 349:781–788
Sztrymf B, Souza R, Bertoletti L et al (2010) Prognostic factors of acute heart failure in patients with pulmonary arterial hypertension. Eur Respir J 35:1286–1293
Tamby MC, Chanseaud Y, Humbert M et al (2005) Anti-endothelial cell antibodies in idiopathic and systemic sclerosis associated pulmonary arterial hypertension. Thorax 60:765–772
Tamby MC, Humbert M, Guilpain P et al (2006) Antibodies to fibroblasts in idiopathic and scleroderma-associated pulmonary hypertension. Eur Respir J 28:799–807
Tamosiuniene R, Tian W, Dhillon G et al (2011) Regulatory T cells limit vascular endothelial injury and prevent pulmonary hypertension. Circ Res 109:867–879
Tanaka E, Harigai M, Tanaka M et al (2002) Pulmonary hypertension in systemic lupus erythematosus: evaluation of clinical characteristics and response to immunosuppressive treatment. J Rheumatol 29:282–287
Taraseviciene-Stewart L, Nicolls MR, Kraskauskas D et al (2007) Absence of T cells confers increased pulmonary arterial hypertension and vascular remodeling. Am J Respir Crit Care Med 175:1280–1289
Tashkin DP, Elashoff R, Clements PJ et al (2006) Cyclophosphamide versus placebo in scleroderma lung disease. N Engl J Med 354:2655–2666
Terrier B, Tamby MC, Camoin L et al (2008) Identification of target antigens of antifibroblast antibodies in pulmonary arterial hypertension. Am J Respir Crit Care Med 177:1128–1134
Terrier B, Tamby MC, Camoin L et al (2009) Antifibroblast antibodies from systemic sclerosis patients bind to {alpha}-enolase and are associated with interstitial lung disease. Ann Rheum Dis 69:428–433
Thurnheer R, Jenni R, Russi EW et al (1997) Hyperthyroidism and pulmonary hypertension. J Intern Med 242:185–188
Torbicki A, Kurzyna M, Kuca P et al (2003) Detectable serum cardiac troponin T as a marker of poor prognosis among patients with chronic precapillary pulmonary hypertension. Circulation 108:844–848
Torre O, Harari S (2011) Pleural and pulmonary involvement in systemic lupus erythematosus. Presse Med 40:e19–e29
Tsuda K, Yamanaka K, Kitagawa H et al (2012) Calcineurin inhibitors suppress cytokine production from memory T cells and differentiation of naive T cells into cytokine-producing mature T cells. PLoS One 7:e31465
Tuder RM (2009) Pathology of pulmonary arterial hypertension. Semin Respir Crit Care Med 30:376–385
Tuder RM, Groves B, Badesch DB et al (1994) Exuberant endothelial cell growth and elements of inflammation are present in plexiform lesions of pulmonary hypertension. Am J Pathol 144:275–285
Tyndall AJ, Bannert B, Vonk M et al (2010) Causes and risk factors for death in systemic sclerosis: a study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann Rheum Dis 69:1809–1815
Ulrich S, Nicolls MR, Taraseviciene L et al (2008a) Increased regulatory and decreased CD8+ cytotoxic T cells in the blood of patients with idiopathic pulmonary arterial hypertension. Respiration 75:272–280
Ulrich S, Taraseviciene-Stewart L, Huber LC et al (2008b) Peripheral blood B lymphocytes derived from patients with idiopathic pulmonary arterial hypertension express a different RNA pattern compared with healthy controls: a cross sectional study. Respir Res 9:20
Vajner L, Vytasek R, Lachmanova V et al (2006) Acute and chronic hypoxia as well as 7-day recovery from chronic hypoxia affects the distribution of pulmonary mast cells and their MMP-13 expression in rats. Int J Exp Pathol 87:383–391
Valmary S, Dorfmuller P, Montani D et al (2011) Human gamma-herpesviruses Epstein-Barr virus and human herpesvirus-8 are not detected in the lungs of patients with severe pulmonary arterial hypertension. Chest 139:1310–1316
van den Hoogen FH, Boerbooms AM, Swaak AJ et al (1996) Comparison of methotrexate with placebo in the treatment of systemic sclerosis: a 24 week randomized double-blind trial, followed by a 24 week observational trial. Br J Rheumatol 35:364–372
Venitz J, Zack J, Gillies H et al (2012) Clinical pharmacokinetics and drug-drug interactions of endothelin receptor antagonists in pulmonary arterial hypertension. J Clin Pharmacol 52(12):1784–1805
Wang W, Yan H, Zhu W et al (2009) Impairment of monocyte-derived dendritic cells in idiopathic pulmonary arterial hypertension. J Clin Immunol 29:705–713
Wang W, Wang YL, Chen XY et al (2011) Dexamethasone attenuates development of monocrotaline-induced pulmonary arterial hypertension. Mol Biol Rep 38:3277–3284
Yildirim-Toruner C, Diamond B (2011) Current and novel therapeutics in the treatment of systemic lupus erythematosus. J Allergy Clin Immunol 127:303–312, quiz 313–304
Zamora AC, Wolters PJ, Collard HR et al (2008) Use of mycophenolate mofetil to treat scleroderma-associated interstitial lung disease. Respir Med 102:150–155
Zheng Y, Li M, Zhang Y et al (2010) The effects and mechanisms of mycophenolate mofetil on pulmonary arterial hypertension in rats. Rheumatol Int 30:341–348
Zhou H (2005) Clinical pharmacokinetics of etanercept: a fully humanized soluble recombinant tumor necrosis factor receptor fusion protein. J Clin Pharmacol 45:490–497
Zitvogel L, Apetoh L, Ghiringhelli F et al (2008) The anticancer immune response: indispensable for therapeutic success? J Clin Invest 118:1991–2001
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Meloche, J., Renard, S., Provencher, S., Bonnet, S. (2013). Anti-inflammatory and Immunosuppressive Agents in PAH. In: Humbert, M., Evgenov, O., Stasch, JP. (eds) Pharmacotherapy of Pulmonary Hypertension. Handbook of Experimental Pharmacology, vol 218. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-38664-0_18
Download citation
DOI: https://doi.org/10.1007/978-3-642-38664-0_18
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-38663-3
Online ISBN: 978-3-642-38664-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)