
Abstract
Obesity and prostate cancer are two of the most common conditions in older men and there is strong evidence that obesity influences the risk, aggressiveness and outcomes of men with prostate cancer. In addition, several comorbidities are observed with obesity, including diabetes mellitus, hypertension, hypercholesterolemia and cardiovascular disease. Separate study of these diagnoses has also identified associations with prostate cancer risk and outcomes. Whether the underlying obesity, the comorbid conditions, or both are responsible for the observed interactions with prostate cancer is not fully understood. Further, pharmacologic treatment of these comorbidities may influence prostate cancer, either by reducing the direct effect of the comorbidity, or independently through additional pharmacologic mechanisms. In this chapter, we review the relationship between common obesity related comorbidities and prostate cancer risk, progression and mortality. We also describe, when available, data on the medications used to treat these comorbidities and the influence these therapies may have on prostate cancer.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Prostate cancer
- Obesity
- Comorbidity
- Diabetes mellitus
- Metabolic syndrome
- Hypercholesterolemia
- Hypertension
- Prostate cancer-specific mortality
- Heart disease
General Overview of Obesity and Prostate CancerRisk/Incidence, Progression, Mortality
Obesity prevalence in the U.S. has risen dramatically over the past 20 years. Presently, more than one-third of adults are obese (body mass index (BMI) ≥30 kg/m2) and among older men, approximately 40% are obese [1]. Obesity is linked with an increase in cancer-specific mortality and an estimated 14% of cancer deaths in U.S. men are due to obesity [2]. The associations of obesity with prostate cancer risk are complex. Pooled/meta-analyses from prospective studies report no overall association of obesity with total PCa risk [3,4,5,6,7]; however, there is growing evidence that associations of obesity with PCa differ for aggressive and nonaggressive PCa. Numerous studies report that obesity is associated with a decreased risk of non-aggressive (low-grade and/or local stage) disease and an increased risk of aggressive (high-grade and/or advanced stage) disease [3,4,5, 7]. Furthermore, there is strong and consistent evidence for a positive association between obesity and PCa progression and PCa-specific mortality (PCSM) [1, 2, 8,9,10,11,12,13,14,15,16,17,18,19,20,21]. As shown in Table 3.1, obesity is associated with a 20–160% elevation in PCa-specific mortality. Pooled/meta analyses report that for every five-point increase in BMI, there is a corresponding 20% increase in PCSM (95% CI 0.99–1.46) and conclude that “cumulative data is compelling for a strong positive association between obesity and fatal prostate cancer” [23]. A 2011 Institute of Medicine Workshop on Obesity and Cancer Report noted: “evidence is building that obesity and weight gain are risk factors for poor outcome in prostate cancer” [24].
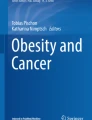
The mechanisms underlying the obesity-PCa progression relationship are unknown. However, a number of metabolic changes that occur in obese men may be responsible, including (1) impaired glucose regulation and insulin resistance; (2) altered adipokines (e.g., leptin and adiponectin); (3) sex hormones; and (4) chronic inflammation, among other potential etiologies. It is well recognized that several morbidities are associated with obesity, such that obesity is one of the leading causes of preventable disease and disability in the United States. Obese patients are at higher risk of having diabetes mellitus, hypertension, hypercholesterolemia and cardiovascular disease (Fig. 3.1) [25].

Comorbid conditions by obesity level, US 2007–2010 (Plotted from data in Saydah et al. [25])
Obesity is also associated with several other cardiovascular comorbid conditions in addition to hypertension, including coronary artery disease, heart failure, and arrhythmias. Interestingly, these diagnoses have also been associated with prostate cancer risk and outcomes. Whether it is obesity driving the relationship with prostate cancer, or if there is a separate effect of the comorbid condition is not fully understood, but there has been a great deal of research on the potential mechanisms underlying the links between the comorbidities and prostate cancer. Further, pharmacologic treatment of these conditions may impact the effects of the comorbidities on prostate cancer , either through reduction in the direct effect of the comorbidity, or separately through additional pharmacologic mechanisms.
In this chapter, we review the relationship between common obesity related comorbidities and prostate cancer . We review the literature, where available, for the association between these comorbidities and prostate cancer risk, progression and mortality. If applicable, we also describe the data on medications used to treat these comorbidities and the influence these medications may have on prostate cancer.
Metabolic Syndrome and Prostate Cancer Risk
Metabolic syndrome (MetS ) is as a cluster of several metabolic abnormalities associated with increased risk of cardiovascular disease and diabetes. Components include hypertension, glucose intolerance, obesity, hypertriglyceridemia, and low high density lipoprotein cholesterol, with insulin resistance as the underlying hallmark feature (Table 3.2) [29].
The prevalence of MetS among US adults in the 2000–2003 National Health and Nutrition Examination Survey was 34% overall [30]. However, among older men the prevalence was much higher, with 41% of men age 40–59 years and 52% of men age 60 or older meeting the criteria for metabolic syndrome [30]. Over the past decade, a growing body of literature suggests that the metabolic syndrome may be involved in the pathogenesis and progression of prostate cancer.
Data on the association between metabolic syndrome and prostate cancer risk are conflicting. Several studies have reported significant positive associations between metabolic syndrome and prostate cancer risk. Two studies from northern Europe that found an increased risk for men with three metabolic syndrome components (RR = 1.56, 95% CI, 1.21–2.00) [31] and OR = 3.36, 95% CI 1.19–9.44) [32], and one study from Finland that reported an increased risk (RR = 1.94, 95% CI 1.06–3.53) among non-diabetic men with metabolic syndrome [33]. Three additional case-control studies reported an increased risk of prostate cancer among men with metabolic syndrome [34,35,36], two of which reported positive associations among African Americans (OR = 1.76, 95% CI = 1.1–2.88 [35] and OR = 1.71, 95% CI 0.97–3.01 [36]). In contrast, a number of studies reported an inverse relationship between metabolic syndrome and prostate cancer risk. In two large cohorts, men with three or more metabolic syndrome components had a significantly lower risk of total prostate cancer than men with less than three components (RR = 0.77, 95% CI 0.60–0.98 [37] and OR = 0.69, 95% CI 0.58–0.82) [38]. In the REDUCE trial , men with one metabolic syndrome component had a lower risk of overall prostate cancer (OR = 0.87, 95% CI 0.76–0.99), although two or three to four components were not significantly related to prostate cancer risk [39]. In a large Swedish cohort, a composite score of five metabolic syndrome factors was associated with a 7% lower risk of overall prostate cancer (RR = 0.93, 95% CI = 0.89–0.97) [40]. In addition, several cohort studies have reported no significant associations between metabolic syndrome and overall prostate cancer risk [41,42,43,44,45,46]. It is likely that the inconsistencies in these associations may be due, at least in part, to differences in the populations studied, definitions of metabolic syndrome or methodologies used.
Three meta-analyses have also evaluated the association of metabolic syndrome with risk of prostate cancer; one of which reported a significant increased risk of overall prostate cancer (RR = 1.54, 95% CI 1.23–1.94) [3] and two reported no overall association [47, 48]. One meta-analysis also evaluated associations of metabolic syndrome with prostate cancer risk among by region, and reported that metabolic syndrome was associated with a reduced risk of total prostate cancer among studies conducted in U.S. (primarily white) populations (RR = 0.79, 95% CI: 0.69–0.91) [47].
Few prospective studies have examined the association of metabolic syndrome and prostate cancer severity defined by grade, stage, and/or aggressiveness. In a large Canadian cohort, metabolic syndrome was associated with a reduced risk of low-grade (RR = 0.69, 95% CI 0.52–0.82) and high-grade (RR = 0.75, 95% CI 0.60–0.94) prostate cancer [38]. Similar associations of metabolic syndrome and a reduced risk of low- and high-grade prostate cancer were reported in the REDUCE trial [39]. However, one case-control study among African Americans in the US reported a significant increased risk of organ confined prostate cancer among men with metabolic syndrome, compared to men without (OR = 1.82 95% CI 1.02–3.23), and no association with advanced prostate cancer [35]. Similarly, a case-control study from Italy reported metabolic syndrome was associated with a significant increased risk of low-grade (Gleason <7; OR = 1.48, 95% CI 1.48–3.17) and high-grade (Gleason ≥7; OR = 1.80, 95% CI 1.17–2.78) prostate cancer [34]. In addition, several cross-sectional studies of men undergoing biopsy or treatment of prostate cancer (radical prostatectomy) have reported positive associations for metabolic syndrome with the presence of higher grade/stage or more aggressive prostate cancer [49,50,51,52,53,54,55].
Lastly, four studies have also examined the association of metabolic syndrome with prostate cancer specific mortality, of which one reported an increased risk (RR = 1.86, 95% CI 1.59–2.19) [46], one reported a decreased risk (RR = 1.14, 95% CI = 1.01–1.28), and two reported no association [45, 56].
Diabetes Mellitus and Prostate Cancer Risk
Diabetes mellitus commonly co-exists with obesity, and there is a large body of epidemiologic evidence providing strong support for the notion that diabetes mellitus is associated with a decreased risk for prostate cancer. To date, three meta-analyses have reported a statistically significant inverse association of diabetes mellitus with risk of total prostate cancer [57,58,59]. The most recent of these analyses, which reviewed 45 studies (29 cohort and 16 case-control) of more than 132,000 total prostate cancer cases, reported a 15% lower risk of overall prostate cancer (95% CI 0.82–0.89) for type-2 diabetes mellitus compared to non-diabetics [57]. Although many studies did not indicate the type of diabetes mellitus, given that type-2 is far more common than type-1, the associations between diabetes mellitus and prostate cancer risk are generally interpreted in terms of type-2 [60].
The inverse association is fairly consistent across various ethnic groups within the US [61, 62]; although evidence is limited to two studies with sufficient numbers of minority participants. Data from populations outside of the US are less consistent with some studies reporting no association [63, 64] or positive associations [65, 66] between diabetes mellitus and prostate cancer. In addition, one meta-analysis reported the opposite association of diabetes mellitus with prostate cancer risk between western studies (RR = 0.81; 95% CI 0.76–0.85) and Asian studies (RR = 1.64; 95% CI 1.00–2.88) (p-interaction = 0.01) [57].
Many studies have also examined the association of diabetes mellitus and prostate cancer severity defined by grade, stage, and/or aggressiveness. Among studies reporting inverse associations between diabetes mellitus and total prostate cancer risk, most reported similar associations by prostate cancer grade, stage or aggressiveness [61, 62, 67,68,69,70,71]. One recent meta-analysis reported the risk of low-grade (RR = 0.74; 95% CI 0.64–0.86) and localized disease (RR = 0.72; 95% CI 0.67–0.76) was modestly stronger than for high grade (RR = 0.78; 95% CI 0.67–0.90) and advanced disease (RR = 0.85; 95% CI 0.75–0.97) [72]. In contrast, a small number of studies found no differences in associations between diabetes mellitus and prostate cancer aggressiveness. At least three large studies reported significant inverse associations for low-grade, localized or less-aggressive disease only [67, 73,74,75]. One study reported an increased risk for diabetes mellitus with early-stage disease (stage A), but inverse association for higher stage (stages B–D) disease [76], and one study reported a positive association between diabetes mellitus and risk of advanced prostate cancer [65]. Given the relatively small proportion of advanced tumors in many of the studies with screen-detected cases, additional epidemiologic studies are needed to more fully explore the association of diabetes mellitus with more advanced prostate cancer.
In contrast to the relatively consistent inverse associations reported between diabetes mellitus and risk of total and low-risk prostate cancer, multiple studies have reported that diabetes mellitus is associated with an increased risk of both all-cause and prostate cancer-specific mortality in men with prostate cancer. A recent meta-analysis of these data concluded that diabetes mellitus was associated with a 29% increase in risk of prostate cancer-specific mortality (RR = 1.29; 95% CI 1.22–1.38) and a 37% (RR = 1.37, 95% CI 1.29–1.45) increase in all-cause mortality [77]. Although individual findings are consistent across the majority of studies, many did not account for potentially important confounders such as prostate cancer characteristics (grade and stage), prostate specific antigen (PSA), prostate cancer treatment(s) or the possible impact of competing risks from other diabetes mellitus-related co-morbidities on the association of diabetes mellitus with prostate cancer-specific mortality . Few studies have evaluated the association of diabetes mellitus prostate cancer mortality among men without prostate cancer at baseline. In a study of almost 18,000 men in London, UK, with 40 years of follow-up, neither impaired glucose tolerance nor diabetes mellitus were associated with prostate cancer-specific mortality [78]. In a study of approximately 2000 male American Indians, diabetes mellitus was associated with an increased risk of prostate cancer mortality; however, among men without diabetes mellitus, a higher level of insulin resistance (measured by homeostasis model assessment to quantify insulin resistance (HOMA-IR)) was associated with a lower risk of prostate-cancer specific mortality [79].
Timing of Diabetes Mellitus and Prostate Cancer Risk
There is growing evidence to suggest that the association of diabetes mellitus with prostate cancer risk may differ by duration of diabetes mellitus. The early stage of type 2 diabetes mellitus is characterized by hyperinsulinemia, which is accompanied by increased levels of circulating insulin like growth factor 1 (IGF-1) and testosterone, and decreased levels of insulin-like growth factor binding protein 3 (IGF-BP3) and serum hormone binding globulin (SHBG) [80]. In contrast, as diabetes mellitus progresses, insulin levels decline and IGF-1 and testosterone levels decrease, and IGF-BP3 and SHBG levels increase [81, 82]. Numerous studies have reported data on duration of diabetes mellitus and risk of prostate cancer, the majority of which report stronger inverse associations of diabetes mellitus and prostate cancer risk with an increasing number of years elapsed since diabetes mellitus diagnosis [68,69,70,71, 76, 80]. Others have reported no meaningful differences [74, 75, 83] and two studies have reported positive associations of PCa risk with increasing duration of diabetes mellitus [84, 85]. Many of the studies reporting stronger inverse associations with increasing duration of diabetes mellitus have also reported a positive association between prostate cancer and recently diagnosed diabetes mellitus [63, 68, 70, 86], which is likely attributable to increased surveillance and health care utilization around the time of diabetes mellitus diagnosis. Larger studies have also examined associations of diabetes mellitus duration and different prostate cancer stage, grade or aggressiveness. All have reported similar associations between diabetes mellitus duration and prostate cancer severity [69, 71, 83]. Notably, few of the studies evaluating diabetes mellitus duration and prostate cancer risk directly assessed diabetes mellitus duration (as opposed to evaluating length of follow-up during the study) [68, 71, 74,75,76, 87], although the findings of these studies do not differ substantively from the overall literature.
Diabetes Mellitus Treatment and Prostate Cancer Risk and Outcomes
It is unknown whether the observed findings above between diabetes and prostate cancer are due to the diabetes, or due to the pharmacologic treatment of diabetes mellitus. Metformin is the most commonly used medication for diabetes mellitus and a great deal of interest exists on its potential anti-cancer properties. Metformin has several potential mechanisms that may influence cancer, including increased AMP-activated protein kinase (AMPK) activation , decreased hepatic gluconeogenesis (with resultant decrease in hyperinsulinemia), and improved insulin sensitivity [88, 89]. AMPK is activated in response to cellular stress [90] leading to a reduction of mammalian target of rapamycin (mTOR) activation, protein synthesis and cellular proliferation [91, 92]. Hyperglycemia and hyperinsulinemia have been associated with multiple malignancies [93,94,95,96,97,98,99]. As metformin use results in lower serum insulin levels [89, 93, 100, 101] the result may produce decreased downstream activation of these mitogenic pathways and potentially, a decrease in PCa growth (Fig. 3.2 [92]).

Mechanism of action of metformin in cancer
Several studies of metformin and prostate cancer risk have been performed with some finding a reduction in prostate cancer risk [102,103,104,105] and others finding no effect [40, 106,107,108,109]. Two meta-analyses [110, 111] found no evidence for an effect of metformin on prostate cancer risk with similar odds ratios (OR 0.96, 95% CI 0.87–1.05; and OR 0.93, 95% CI 0.82–1.05, respectively). It should be noted that the main indication for metformin is the treatment of diabetes mellitus, so comparing metformin users to non-users may just be comparing diabetics to nondiabetics, which makes interpreting results for use of any diabetes medication difficult.
There are stronger data for an effect of metformin on prostate cancer outcomes, and several meta-analyses have been performed with evidence of metformin leading to a reduction in the risk of biochemical recurrence after primary therapy and also a reduction in both prostate cancer-specific and overall mortality [112,113,114,115,116]. In the meta analysis by Coyle et al., the reduction in risk of recurrence after primary treatment was seen following radiation therapy (HR 0.45, 95% CI 0.29–0.70) but not following radical prostatectomy (0.94, 0.77–1.15) [115].
Small clinical trials of metformin and prostate cancer outcomes have been completed and several studies are ongoing. One trial of 40 men starting ADT randomized men to either ADT alone or ADT in combination with metformin and a lifestyle intervention (diet and exercise) [117]. After 6 months, men in the intervention arm had significant improvements in weight, BMI, abdominal girth and blood pressure [117]. Metformin is being studied in various stages of prostate cancer (pre-prostatectomy, active surveillance, adjuvant for high risk localized disease, biochemical recurrence, at time of salvage radiation, castrate resistant prostate cancer, advanced hormone sensitive) (https://www.clinicaltrials.gov/).
Use of other medications for diabetes mellitus has also been studied with regards to prostate cancer. Several studies have investigated insulin and prostate cancer risk. A meta-analysis of 11 non-randomized studies from 2007 to 2013 and found that compared to use other glucose lowering agents, insulin was not associated with a reduction in risk of prostate cancer [118]. Sulfonylurea, which is an insulin-secretagogue, has also been studied with most showing no effect on prostate cancer risk compared to patients with diabetes mellitus taking metformin [119, 120], non-sulfonylurea therapy [121] or non-diabetes mellitus patients [122]. Recently, a study from Sweden found that those subjects with >1 year of diabetes mellitus and taking insulin/sulfonureas for >1 year had a reduction in the risk of prostate cancer compared to those not taking diabetes medications (OR 0.73, 95% CI 0.55–0.98) [40]. However, a study from the Finnish Randomized Study of Screening for Prostate Cancer found that use of sulphonylureas was associated with an increase in the risk of metastatic prostate cancer compared to other oral medications for diabetes mellitus (HR 2.04, 95% CI 1.11–3.77) [123]. Further research is needed to define the role of sulfonylurea and prostate cancer. Another class of diabetes medications, thiazolidinediones , are PPAR gamma ligands which can have anti-cancer properties and several preclinical studies have shown these agents to be active against prostate cancer cells [124]. Interestingly, higher levels of Peroxisome proliferator-activated receptor gamma (PPAR-γ)receptors have been identified on prostate cancer cells as opposed to benign prostate cells [125]. With prostate cancer, the data has suggested an increased risk [126, 127] or no effect [128, 129].
Hyperlipidemia and Prostate Cancer Risk
Hyperlipidemia is a well-established consequence of obesity, and there is growing evidence to suggest that men with hypercholesterolemia are at increased risk of high-grade or advanced prostate cancer. Several large prospective studies from various populations have reported that increasing cholesterol concentrations are associated with a greater risk of high-grade [130,131,132,133,134] and aggressive [135,136,137] prostate cancer. Two of these studies reported that the positive association between cholesterol level and high-risk prostate cancer was limited to overweight/obese men [133, 134]; although other studies have not reported differences in associations by obesity status [130, 131]. In an attempt to evaluate whether the use of cholesterol-lowering medications could explain associations between cholesterol concentrations and high-risk prostate cancer, three studies conducted analyses excluding men who reported use of these medications [130, 134, 136]. Associations were similar after excluding men who reported use of these medications, although no longer statistically significant in one study [130]. Few prospective studies have evaluated the relationship of cholesterol concentration with prostate cancer mortality. The majority report no association [45, 138]; however, one reported a significant increased risk for increasing total cholesterol concentrations [78].
The relationship between circulating cholesterol concentrations and total prostate cancer, however, is less clear. Initial studies of the association of cholesterol with risk of total prostate cancer , many of which were based on a small number of prostate cancer cases, reported no association [78, 139,140,141,142] or an inverse association [143, 144]. Since then, several prospective studies based on much larger sample sizes have confirmed findings from early studies [45, 130, 131, 133, 134, 145,146,147,148]; however, several recent studies have reported a significant increase in risk of total prostate cancer with increasing total cholesterol concentrations [132, 135,136,137].
Few prospective studies have evaluated associations of other lipids , such as high-density lipoprotein (HDL) and low-density lipoprotein (LDL) , with risk of prostate cancer. Studies evaluating the relationship between HDL concentrations and risk of prostate cancer have been inconsistent. Some have reported a reduced risk of total prostate cancer [135, 148], while other report no association [45, 145] or an increased risk of total [132], high-risk [132] or low-risk [136] prostate cancer. Studies of the relationship between LDL concentrations and prostate cancer risk are also conflicting, with some studies reporting no association [45, 145, 148], and others reporting increased risks for total [132] and high-grade prostate cancer [132, 136]. The relationship of triglyceride concentrations with risk of prostate cancer has only been evaluated by three studies, all of which reported no association [45, 136, 147]. Only one study evaluated associations of apolipoproteins with risk of prostate cancer, and found a slight inverse association of apolipoprotein A-1 with risk of total cancer, but no association for apolipoprotein-B [148].
Hyperlipidemia Treatment and Prostate Cancer Risk
Statins use for high cholesterol has risen to almost 30% of US adults [149]. The potential mechanisms by which statins may reduce prostate cancer development and progression are multiple and can be divided into cholesterol-mediated pathways (e.g., reducing intra-tumor level of cholesterol precursor to androgens; altering cell membrane signaling) or non-cholesterol-mediated pathways (e.g., pro-apoptosis; lowering mevalonate levels and subsequent production of farnesyl and geranyl pyrophosphate which would block cellular proliferation and survival) (Fig. 3.3) [151].

Mechanism of action of statins in prostate cancer (from [150])
Several studies have explored the relationship between statin use and primary prevention of incident prostate cancer. A meta analysis published in 2012 of 27 studies found that use of statins reduced incident prostate cancer (RR 0.93, 95% CI 0.87–0.99) and had a greater effect on reducing the risk of advanced prostate cancer (RR 0.80, 95% CI 0.70–0.98) [152]. Studies published since this meta analysis have been mixed with some showing a reduced risk of prostate cancer [153, 154] but several showing no protective effect [106, 155,156,157,158].
Tertiary prevention of prostate cancer recurrence and studies of prostate cancer specific mortality have also been performed. In a recent meta-analysis [159] of 22 studies of biochemical recurrence, use of statins was associated with a reduced risk of prostate cancer recurrence (HR 0.88, 95% CI 0.77–1.00). Interestingly, the effects were limited to treatment with radiation (HR 0.67, 95% CI 0.48–0.86; 7 studies) with no effect seen in those undergoing prostatectomy (HR 0.96, 95% CI 0.83–1.09). Whether statins (1) act as a radiosensitizer, or (2) if statins influence the effects of concomitant androgen deprivation therapy (ADT) use with radiation (ADT was used in 6 of 7 radiation studies with the proportion of men in those studies receiving ADT along with their radiation therapy ranging from 26 to 67%), or (3) if the statins association is due to unmeasured confounding is unknown. In a separate meta-analysis of mortality from 13 studies, use of statins reduced both overall (HR 0.56, 95% CI 0.38–0.83) and prostate cancer specific mortality (0.53, 95% CI 0.36–0.77) [160], with the effect observed for both pre and post-treatment use of statins.
An interesting interaction has recently been identified in steroid transport, statins and prostate cancer. The organic anion transporter, SLCO2B1, is involved in cellular uptake of several substrates, including steroid hormones such as dehydroepiandrosterone (DHEA) that prostate cancer cells can use as a precursor to dihydrotestosterone (DHT). Castrate resistant prostate cancer metastases have increased expression of SLCO genes compared to primary prostate cancer and genetic variants of SLCO transporters have been found to be associated with prostate cancer-specific mortality [161,162,163]. Statins are also a substrate for SLCO2B1 and act as a competitive inhibitor to DHEA for transport into prostate cancer cells [164]. In a study of 926 men starting ADT for advanced disease, use of statins (31% of cohort) had a longer time to progression compared to those not taking statins (adjusted HR 0.83, 95% CI 0.69–0.99) [164]. However, in castrate resistant disease, a common medication utilized is abiraterone, which is a CYP17A1 inhibitor that results in blocking all androgen production including DHEA. In this scenario, if adrenal DHEA is acting as an androgen source for prostate cancer cells in the setting of ADT, and abiraterone is blocking the production of DHEA, one would expect to not see a benefit to statin use if SLCO2B1 transport inhibition is the mechanism of statin effect on prostate cancer. In a study of 108 men receiving abiraterone, there was no difference in the percent experiencing >50% decline in PSA or in progression-free survival or overall survival between those with (n = 21) or without (n = 87) statin use [165]. Further study is needed to confirm these findings.
Hypertension and Prostate Cancer
Epidemiologic studies have reported inconsistent findings regarding the association of high blood pressure with risk of prostate cancer. The majority of studies have reported no significant association with incident [31, 32, 37, 166,167,168,169,170] or fatal [169, 171] prostate cancer, although some studies have reported an increased risk of total [32, 172, 173] or advanced prostate cancer [172], and at least one study reported an inverse association for total and non-aggressive prostate cancer [174].
Treatment for Hypertension and Prostate Cancer
Several classes of drugs are commonly used individually or in combination as pharmacological treatment for high blood pressure, including diuretics, beta-blockers (BBs) , calcium channel (CC) blockers , angiotensin-converting enzyme (ACE) inhibitors , and angiotensin II-receptor (AR) blockers. Many of these medications have been shown to either suppress prostate cancer cell growth and proliferation, angiogenesis in vitro, and inhibit migration of PC-3 human prostate carcinoma in vivo [175]. Thus, numerous studies have evaluated the association of antihypertensive medication use with prostate cancer risk. For overall antihypertensive medication use, four large prospective studies found no evidence of an association with risk of prostate cancer [166, 172, 173, 176]. However, in one large population-based cohort, current use of any antihypertensive medication was associated with a slight decreased risk of total (RR = 0.90, 95% CI 0.83–0.98) and organ-confined low-grade prostate cancer (RR = 0.89, 95% CI 0.81–0.99) [177].
Studies on individual classes of antihypertensive medications and prostate cancer risk have also produced mixed results. Among studies evaluating the association of ACE inhibitor use and prostate cancer incidence, most have found no association [166, 167, 178,179,180,181,182], two found an inverse association [176, 177], although the inverse association was limited to one individual ACE inhibitor (captopril) in one study [176] and in the second one was no longer statistically significant after adjustment for other antihypertensive use [177], and two study reported a significant positive association for total prostate cancer only [183, 184]. A recent meta-analysis of the prospective studies found that use of ACE inhibitors or AR blockers was associated with a significant decreased risk of overall prostate cancer (RR = 0.88, 95% CI 0.80–0.97), [185] although two additional meta-analyses of data from clinical trials did not find an association with risk of prostate cancer for ACE inhibitor use [186, 187]. For calcium channel blockers, several large population-based cohort studies and a case-control study have reported no association with risk of total [167, 177, 183, 184, 188, 189], low-grade [177] or aggressive/fatal prostate cancer [177, 190]. Only one study reported a significant inverse association for CC blocker use with total prostate cancer risk (OR = 0.55; 95% CI, 0.31–0.97) [191]. The majority of studies evaluating the association of BB use and prostate cancer risk have also found no association [166, 167, 176, 177, 191]. However, in two observational studies, BB use was associated with lower overall prostate cancer risk (OR = 0.80; 95% CI, 0.70–1.0) [183], and in one was associated with a slight increased risk (OR = 1.16; 95% CI, 1.12–1.21) [184].
Heart Disease and Prostate Cancer Risk
An additional comorbidity that occurs with, or as a result of obesity, is heart disease. There are some data that a history of coronary artery disease (CAD) is associated with an increased risk of prostate cancer. In a secondary analysis of the REDUCE trial (a randomized controlled trial of dutasteride versus placebo for reducing the risk of prostate cancer in men with a prior negative biopsy), 9% of men had a history of CAD and this was associated with a 35% increased risk of prostate cancer in the multivariate model [192]. Men with CAD also were more likely to be obese, have diabetes mellitus, hypertension and hypercholesterolemia.
Treatment of Heart Disease and Prostate Cancer Risk
The cardiac glycosides (e.g., digoxin ) are used in the treatment of congestive heart failure and cardiac arrhythmias. Cardiac glycosides also have been found to alter serum androgen levels [193, 194], inhibiting tumor growth and development, [195] and have inhibitory effects on prostate cancer cell lines [196,197,198,199]. In a study that screened a medication library for growth inhibition in prostate cancer cell lines, cardiac glycosides were among the most potent [199]. Although an analysis of the Health Professionals Follow-up Study found a significant reduction in the risk of prostate cancer for digoxin users (HR 0.76, 95% CI 0.60–0.95) [199], other studies have not shown a statistically significant reduction in prostate cancer risk [200, 201]. With regards to prostate cancer-specific mortality , the literature does not support a protective role for digoxin, with two of the studies showing non-significant increases in prostate cancer-specific mortality among users [202, 203]. Sotalol , a BB and potassium-channel inhibitor used for arrhythmias has commonly been studied along with glycosides, with one study finding a reduction in the risk of advanced prostate cancer associated with sotalol use [204].
Individuals with heart disease are often recommended to take aspirin daily to prevent to reduce the risk of vascular events (heart attack, stroke) [205]. There are several studies on aspirin use and cancer risk and mortality, with the strongest data present for colorectal cancer risk. The anti-cancer mechanisms for aspirin are hypothesized to include induction of apoptosis, reduced prostaglandin production with effects on angiogenesis, proliferation and host immunity [206, 207]. A meta analysis of the effects of aspirin on prostate cancer risk and mortality was published in 2014 [208]. Overall, use of aspirin was associated with a reduction in the incidence of total prostate cancer (OR 0.92, 95% CI 0.87–0.97) and advanced prostate cancer (OR 0.81, 95% CI 0.73–0.89). In a recent study with TMPRSS2:ERG fusion status available, aspirin users had a 37% reduction in the risk of TMPRSS2:ERG fusion positive tumors (95% CI 0.43–0.93) with dose effect present, whereas no association was seen with TMPRSS2:ERG fusion negative tumors and aspirin use (OR 0.99, 0.69–1.42) [209]. TMPRSS2:ERG fusion is the most common gene rearrangement in prostate cancer, present in approximately 50% of cases. As aspirin reduces the level of reactive oxygen species in a cell (which can create dsDNA breaks), use of aspirin may protect against DNA strand breaks required for TMPRSS2:ERG fusion. In a recent meta-analysis, use of aspirin was associated with a modest reduction in the risk of prostate cancer specific mortality (OR 0.86, 95% CI 0.78–0.96 for total prostate cancer; OR = 0.81, 95% CI 0.71–0.92 for advanced prostate cancer) [208].
Potential Biases of Associations of Obesity-Related Metabolic Conditions and Risk of Prostate Cancer
When considering the potential mechanisms that underlie the inverse association between comorbid conditions and prostate cancer, non-causal explanations should also be considered. Many obesity-related metabolic conditions have been associated with lower prostate-specific antigen (PSA) levels . For example, PSA has been shown to be lower in diabetics and lowest in individuals with a long duration of disease [62, 70, 210,211,212,213,214,215]. Similarly, obesity, which commonly coexists with diabetes, is believed to lowers PSA due to hemodilution [216,217,218,219]. Furthermore, some medications, such as statins and 5-alpha reductase inhibitors have been associated with lower PSA levels [220,221,222]. Because PSA drives biopsy recommendations and subsequent PCa detection in clinical practice, lower PSA in men with obesity-related medical conditions could lead to fewer biopsies and consequently to less diagnoses of cancer. Thus, it is possible that the observed associations between obesity-related metabolic conditions and prostate cancer risk are attributable, at least in part, to the effects of these conditions and/or their treatments on PSA values.
Conclusions
Obesity and prostate cancer are two common conditions in men over the age of 50 today and there appears to be a relationship between the two, with obesity potentially influencing the risk, aggressiveness and outcomes of men with prostate cancer. As our understanding of the mechanisms between these conditions grows, the appreciation of the complexity of the relationship and the likely contribution from multiple factors also increases. With obesity, a number of comorbid conditions also become more common. The observed associations between these diagnoses or their treatments and prostate cancer could be explained by confounding by the obesity:prostate cancer relationship. Or, these diagnoses and treatments may influence prostate cancer development and progression independent of obesity. Further research will help define the complex interplay. Until then, care of men at risk for, or with prostate cancer, should also include attention to weight management, glucose and lipid control, to promote both overall and prostate-cancer specific health.
References
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003;348(17):1625–38. doi:10.1056/NEJMoa021423.
Wright ME, Chang SC, Schatzkin A, Albanes D, Kipnis V, Mouw T, Hurwitz P, Hollenbeck A, Leitzmann MF. Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality. Cancer. 2007;109(4):675–84. doi:10.1002/cncr.22443.
Hsing AW, Sakoda LC, Chua S Jr. Obesity, metabolic syndrome, and prostate cancer. Am J Clin Nutr. 2007;86(3):s843–57.
Allott EH, Masko EM, Freedland SJ. Obesity and prostate cancer: weighing the evidence. Eur Urol. 2013;63(5):800–9. doi:10.1016/j.eururo.2012.11.013.
MacInnis RJ, English DR. Body size and composition and prostate cancer risk: systematic review and meta-regression analysis. Cancer Causes Control. 2006;17(8):989–1003. doi:10.1007/s10552-006-0049-z.
Discacciati A, Orsini N, Wolk A. Body mass index and incidence of localized and advanced prostate cancer—a dose-response meta-analysis of prospective studies. Ann Oncol. 2012;23(7):1665–71. doi:10.1093/annonc/mdr603.
Zhang X, Zhou G, Sun B, Zhao G, Liu D, Sun J, Liu C, Guo H. Impact of obesity upon prostate cancer-associated mortality: a meta-analysis of 17 cohort studies. Oncol Lett. 2015;9(3):1307–12. doi:10.3892/ol.2014.2841.
Gong Z, Agalliu I, Lin DW, Stanford JL, Kristal AR. Obesity is associated with increased risks of prostate cancer metastasis and death after initial cancer diagnosis in middle-aged men. Cancer. 2007;109(6):1192–202. doi:10.1002/cncr.22534.
Snowdon DA, Phillips RL, Choi W. Diet, obesity, and risk of fatal prostate cancer. Am J Epidemiol. 1984;120(2):244–50.
Rodriguez C, Patel AV, Calle EE, Jacobs EJ, Chao A, Thun MJ. Body mass index, height, and prostate cancer mortality in two large cohorts of adult men in the United States. Cancer Epidemiol Biomark Prev. 2001;10(4):345–53.
Siddiqui SA, Inman BA, Sengupta S, Slezak JM, Bergstralh EJ, Leibovich BC, Zincke H, Blute ML. Obesity and survival after radical prostatectomy: a 10-year prospective cohort study. Cancer. 2006;107(3):521–9. doi:10.1002/cncr.22030.
Banez LL, Sun L, Trock BJ, Han M, Partin AW, Aronson WJ, Terris MK, Presti JC Jr, Kane CJ, Amling CL, Moul JW, Freedland SJ. Body mass index and prostate specific antigen as predictors of adverse pathology and biochemical recurrence after prostatectomy. J Urol. 2009;182(2):491–496. discussion 6–8. doi:10.1016/j.juro.2009.04.007.
Efstathiou JA, Bae K, Shipley WU, Hanks GE, Pilepich MV, Sandler HM, Smith MR. Obesity and mortality in men with locally advanced prostate cancer: analysis of RTOG 85-31. Cancer. 2007;110(12):2691–9. doi:10.1002/cncr.23093.
Freedland SJ, Grubb KA, Yiu SK, Humphreys EB, Nielsen ME, Mangold LA, Isaacs WB, Partin AW. Obesity and risk of biochemical progression following radical prostatectomy at a tertiary care referral center. J Urol. 2005;174(3):919–22. doi:10.1097/01.ju.0000169459.78982.d7.
Freedland SJ, Terris MK, Presti JC Jr, Amling CL, Kane CJ, Trock B, Aronson WJ. Search Database Study G. Obesity and biochemical outcome following radical prostatectomy for organ confined disease with negative surgical margins. J Urol. 2004;172(2):520–4. doi:10.1097/01.ju.0000135302.58378.ae.
Jayachandran J, Banez LL, Aronson WJ, Terris MK, Presti JC Jr, Amling CL, Kane CJ, Freedland SJ, Group SDS. Obesity as a predictor of adverse outcome across black and white race: results from the Shared Equal Access Regional Cancer Hospital (SEARCH) Database. Cancer. 2009;115(22):5263–71. doi:10.1002/cncr.24571.
Kane CJ, Im R, Amling CL, Presti JC Jr, Aronson WJ, Terris MK, Freedland SJ, Group SDS. Outcomes after radical prostatectomy among men who are candidates for active surveillance: results from the SEARCH database. Urology. 2010;76(3):695–700. doi:10.1016/j.urology.2009.12.073.
Major JM, Klonoff-Cohen HS, Pierce JP, Slymen DJ, Saltzstein SL, Macera CA, Mercola D, Kattan MW. Prostate cancer postoperative nomogram scores and obesity. PLoS One. 2011;6(2):e17382. doi:10.1371/journal.pone.0017382.
Strom SS, Wang X, Pettaway CA, Logothetis CJ, Yamamura Y, Do KA, Babaian RJ, Troncoso P. Obesity, weight gain, and risk of biochemical failure among prostate cancer patients following prostatectomy. Clin Cancer Res. 2005;11(19 Pt 1):6889–94. doi:10.1158/1078-0432.CCR-04-1977.
Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2004;4(8):579–91. doi:10.1038/nrc1408.
Andersson SO, Wolk A, Bergstrom R, Adami HO, Engholm G, Englund A, Nyren O. Body size and prostate cancer: a 20-year follow-up study among 135006 Swedish construction workers. J Natl Cancer Inst. 1997;89(5):385–9.
Ma J, Li H, Giovannucci E, Mucci L, Qiu W, Nguyen PL, Gaziano JM, Pollak M, Stampfer MJ. Prediagnostic body-mass index, plasma C-peptide concentration, and prostate cancer-specific mortality in men with prostate cancer: a long-term survival analysis. Lancet Oncol. 2008;9(11):1039–47. doi:10.1016/S1470-2045(08)70235-3.
Cao Y, Ma J. Body mass index, prostate cancer-specific mortality, and biochemical recurrence: a systematic review and meta-analysis. Cancer Prev Res (Phila). 2011;4(4):486–501. doi:10.1158/1940-6207.CAPR-10-0229.
Demark-Wahnefried W, Platz EA, Ligibel JA, Blair CK, Courneya KS, Meyerhardt JA, Ganz PA, Rock CL, Schmitz KH, Wadden T, Philip EJ, Wolfe B, Gapstur SM, Ballard-Barbash R, McTiernan A, Minasian L, Nebeling L, Goodwin PJ. The role of obesity in cancer survival and recurrence. Cancer Epidemiol Biomark Prev. 2012;21(8):1244–59. doi:10.1158/1055-9965.EPI-12-0485.
Saydah S, Bullard KM, Cheng Y, Ali MK, Gregg EW, Geiss L, Imperatore G. Trends in cardiovascular disease risk factors by obesity level in adults in the United States, NHANES 1999–2010. Obesity (Silver Spring). 2014;22(8):1888–95. doi:10.1002/oby.20761.
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC Jr, Spertus JA, Costa F, American Heart A, National Heart L, Blood I. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–52. doi:10.1161/CIRCULATIONAHA.105.169404.
Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–53. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S.
Zimmet P, Magliano D, Matsuzawa Y, Alberti G, Shaw J. The metabolic syndrome: a global public health problem and a new definition. J Atheroscler Thromb. 2005;12(6):295–300.
Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595–607.
Ervin RB. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race and ethnicity, and body mass index: United States, 2003–2006. Natl Health Stat Rep. 2009(13):1–7.
Lund Haheim L, Wisloff TF, Holme I, Nafstad P. Metabolic syndrome predicts prostate cancer in a cohort of middle-aged Norwegian men followed for 27 years. Am J Epidemiol. 2006;164(8):769–74. doi:10.1093/aje/kwj284.
Tuohimaa P, Tenkanen L, Syvala H, Lumme S, Hakulinen T, Dillner J, Hakama M. Interaction of factors related to the metabolic syndrome and vitamin D on risk of prostate cancer. Cancer Epidemiol Biomark Prev. 2007;16(2):302–7. doi:10.1158/1055-9965.EPI-06-0777.
Laukkanen JA, Laaksonen DE, Niskanen L, Pukkala E, Hakkarainen A, Salonen JT. Metabolic syndrome and the risk of prostate cancer in Finnish men: a population-based study. Cancer Epidemiol Biomark Prev. 2004;13(10):1646–50.
Pelucchi C, Serraino D, Negri E, Montella M, Dellanoce C, Talamini R, La Vecchia C. The metabolic syndrome and risk of prostate cancer in Italy. Ann Epidemiol. 2011;21(11):835–41. doi:10.1016/j.annepidem.2011.07.007.
Beebe-Dimmer JL, Dunn RL, Sarma AV, Montie JE, Cooney KA. Features of the metabolic syndrome and prostate cancer in African-American men. Cancer. 2007;109(5):875–81. doi:10.1002/cncr.22461.
Beebe-Dimmer JL, Nock NL, Neslund-Dudas C, Rundle A, Bock CH, Tang D, Jankowski M, Rybicki BA. Racial differences in risk of prostate cancer associated with metabolic syndrome. Urology. 2009;74(1):185–90. doi:10.1016/j.urology.2009.03.013.
Tande AJ, Platz EA, Folsom AR. The metabolic syndrome is associated with reduced risk of prostate cancer. Am J Epidemiol. 2006;164(11):1094–102. doi:10.1093/aje/kwj320.
Blanc-Lapierre A, Spence A, Karakiewicz PI, Aprikian A, Saad F, Parent ME. Metabolic syndrome and prostate cancer risk in a population-based case-control study in Montreal, Canada. BMC Public Health. 2015;15:913. doi:10.1186/s12889-015-2260-x.
Sourbeer KN, Howard LE, Andriole GL, Moreira DM, Castro-Santamaria R, Freedland SJ, Vidal AC. Metabolic syndrome-like components and prostate cancer risk: results from the Reduction by Dutasteride of Prostate Cancer Events (REDUCE) study. BJU Int. 2015;115(5):736–43. doi:10.1111/bju.12843.
Haggstrom C, Van Hemelrijck M, Zethelius B, Robinson D, Grundmark B, Holmberg L, Gudbjornsdottir S, Garmo H, Stattin P. Prospective study of Type 2 diabetes mellitus, anti-diabetic drugs and risk of prostate cancer. Int J Cancer. 2017;140(3):611–7. doi:10.1002/ijc.30480.
Lawrence YR, Morag O, Benderly M, Boyko V, Novikov I, Dicker AP, Goldbourt U, Behar S, Barchana M, Wolf I. Association between metabolic syndrome, diabetes mellitus and prostate cancer risk. Prostate Cancer Prostatic Dis. 2013;16(2):181–6. doi:10.1038/pcan.2012.54.
Wallner LP, Morgenstern H, McGree ME, Jacobson DJ, St Sauver JL, Jacobsen SJ, Sarma AV. The effects of metabolic conditions on prostate cancer incidence over 15 years of follow-up: results from the Olmsted County Study. BJU Int. 2011;107(6):929–35. doi:10.1111/j.1464-410X.2010.09703.x.
Russo A, Autelitano M, Bisanti L. Metabolic syndrome and cancer risk. Eur J Cancer. 2008;44(2):293–7. doi:10.1016/j.ejca.2007.11.005.
Inoue M, Noda M, Kurahashi N, Iwasaki M, Sasazuki S, Iso H, Tsugane S, Japan Public Health Center-based Prospective Study G. Impact of metabolic factors on subsequent cancer risk: results from a large-scale population-based cohort study in Japan. Eur J Cancer Prev. 2009;18(3):240–7. doi:10.1097/CEJ.0b013e3283240460.
Martin RM, Vatten L, Gunnell D, Romundstad P, Nilsen TI. Components of the metabolic syndrome and risk of prostate cancer: the HUNT 2 cohort, Norway. Cancer Causes Control. 2009;20(7):1181–92. doi:10.1007/s10552-009-9319-x.
Grundmark B, Garmo H, Loda M, Busch C, Holmberg L, Zethelius B. The metabolic syndrome and the risk of prostate cancer under competing risks of death from other causes. Cancer Epidemiol Biomark Prev. 2010;19(8):2088–96. doi:10.1158/1055-9965.EPI-10-0112.
Esposito K, Chiodini P, Colao A, Lenzi A, Giugliano D. Metabolic syndrome and risk of cancer: a systematic review and meta-analysis. Diabetes Care. 2012;35(11):2402–11. doi:10.2337/dc12-0336.
Xiang YZ, Xiong H, Cui ZL, Jiang SB, Xia QH, Zhao Y, Li GB, Jin XB. The association between metabolic syndrome and the risk of prostate cancer, high-grade prostate cancer, advanced prostate cancer, prostate cancer-specific mortality and biochemical recurrence. J Exp Clin Cancer Res. 2013;32:9. doi:10.1186/1756-9966-32-9.
De Nunzio C, Freedland SJ, Miano R, Trucchi A, Cantiani A, Carluccini A, Tubaro A. Metabolic syndrome is associated with high grade Gleason score when prostate cancer is diagnosed on biopsy. Prostate. 2011;71(14):1492–8. doi:10.1002/pros.21364.
De Nunzio C, Simone G, Brassetti A, Mastroianni R, Collura D, Muto G, Gallucci M, Tubaro A. Metabolic syndrome is associated with advanced prostate cancer in patients treated with radical retropubic prostatectomy: results from a multicentre prospective study. BMC Cancer. 2016;16:407. doi:10.1186/s12885-016-2442-7.
Morote J, Ropero J, Planas J, Bastaros JM, Delgado G, Placer J, Celma A, de Torres IM, Carles J, Reventos J, Doll A. Metabolic syndrome increases the risk of aggressive prostate cancer detection. BJU Int. 2013;111(7):1031–6. doi:10.1111/j.1464-410X.2012.11406.x.
Bhindi B, Locke J, Alibhai SM, Kulkarni GS, Margel DS, Hamilton RJ, Finelli A, Trachtenberg J, Zlotta AR, Toi A, Hersey KM, Evans A, van der Kwast TH, Fleshner NE. Dissecting the association between metabolic syndrome and prostate cancer risk: analysis of a large clinical cohort. Eur Urol. 2015;67(1):64–70. doi:10.1016/j.eururo.2014.01.040.
Bhindi B, Xie WY, Kulkarni GS, Hamilton RJ, Nesbitt M, Finelli A, Zlotta AR, Evans A, van der Kwast TH, Alibhai SM, Trachtenberg J, Fleshner NE. Influence of metabolic syndrome on prostate cancer stage, grade, and overall recurrence risk in men undergoing radical prostatectomy. Urology. 2016;93:77–85. doi:10.1016/j.urology.2016.01.041.
Kheterpal E, Sammon JD, Diaz M, Bhandari A, Trinh QD, Pokala N, Sharma P, Menon M, Agarwal PK. Effect of metabolic syndrome on pathologic features of prostate cancer. Urol Oncol. 2013;31(7):1054–9. doi:10.1016/j.urolonc.2011.12.012.
Macleod LC, Chery LJ, Hu EY, Zeliadt SB, Holt SK, Lin DW, Porter MP, Gore JL, Wright JL. Metabolic syndrome, dyslipidemia and prostate cancer recurrence after primary surgery or radiation in a veterans cohort. Prostate Cancer Prostatic Dis. 2015;18(2):190–5. doi:10.1038/pcan.2015.12.
Jaggers JR, Sui X, Hooker SP, LaMonte MJ, Matthews CE, Hand GA, Blair SN. Metabolic syndrome and risk of cancer mortality in men. Eur J Cancer. 2009;45(10):1831–8. doi:10.1016/j.ejca.2009.01.031.
Bansal D, Bhansali A, Kapil G, Undela K, Tiwari P. Type 2 diabetes and risk of prostate cancer: a meta-analysis of observational studies. Prostate Cancer Prostatic Dis. 2013;16(2):151–58. S1. doi:10.1038/pcan.2012.40.
Bonovas S, Filioussi K, Tsantes A. Diabetes mellitus and risk of prostate cancer: a meta-analysis. Diabetologia. 2004;47(6):1071–8. doi:10.1007/s00125-004-1415-6.
Kasper JS, Giovannucci E. A meta-analysis of diabetes mellitus and the risk of prostate cancer. Cancer Epidemiol Biomark Prev. 2006;15(11):2056–62. doi:10.1158/1055-9965.EPI-06-0410.
Cowie CC, Rust KF, Byrd-Holt DD, Eberhardt MS, Flegal KM, Engelgau MM, Saydah SH, Williams DE, Geiss LS, Gregg EW. Prevalence of diabetes and impaired fasting glucose in adults in the U.S. population: National Health And Nutrition Examination Survey 1999–2002. Diabetes Care. 2006;29(6):1263–8. doi:10.2337/dc06-0062.
Calton BA, Chang SC, Wright ME, Kipnis V, Lawson K, Thompson FE, Subar AF, Mouw T, Campbell DS, Hurwitz P, Hollenbeck A, Schatzkin A, Leitzmann MF. History of diabetes mellitus and subsequent prostate cancer risk in the NIH-AARP Diet and Health Study. Cancer Causes Control. 2007;18(5):493–503. doi:10.1007/s10552-007-0126-y.
Waters KM, Henderson BE, Stram DO, Wan P, Kolonel LN, Haiman CA. Association of diabetes with prostate cancer risk in the multiethnic cohort. Am J Epidemiol. 2009;169(8):937–45. doi:10.1093/aje/kwp003.
Adami HO, McLaughlin J, Ekbom A, Berne C, Silverman D, Hacker D, Persson I. Cancer risk in patients with diabetes mellitus. Cancer Causes Control. 1991;2(5):307–14.
Tavani A, Gallus S, Bertuzzi M, Dal Maso L, Zucchetto A, Negri E, Franceschi S, Ramazzotti V, Montella M, La Vecchia C. Diabetes mellitus and the risk of prostate cancer in Italy. Eur Urol. 2005;47(3):313–317.; discussion 7. doi:10.1016/j.eururo.2004.10.027.
Li Q, Kuriyama S, Kakizaki M, Yan H, Sone T, Nagai M, Sugawara Y, Ohmori-Matsuda K, Hozawa A, Nishino Y, Tsuji I. History of diabetes mellitus and the risk of prostate cancer: The Ohsaki Cohort Study. Cancer Causes Control. 2010;21(7):1025–32. doi:10.1007/s10552-010-9530-9.
Rousseau MC, Parent ME, Pollak MN, Siemiatycki J. Diabetes mellitus and cancer risk in a population-based case-control study among men from Montreal, Canada. Int J Cancer. 2006;118(8):2105–9. doi:10.1002/ijc.21600.
Gong Z, Neuhouser ML, Goodman PJ, Albanes D, Chi C, Hsing AW, Lippman SM, Platz EA, Pollak MN, Thompson IM, Kristal AR. Obesity, diabetes, and risk of prostate cancer: results from the prostate cancer prevention trial. Cancer Epidemiol Biomark Prev. 2006;15(10):1977–83. doi:10.1158/1055-9965.EPI-06-0477.
Rodriguez C, Patel AV, Mondul AM, Jacobs EJ, Thun MJ, Calle EE. Diabetes and risk of prostate cancer in a prospective cohort of US men. Am J Epidemiol. 2005;161(2):147–52. doi:10.1093/aje/kwh334.
Kasper JS, Liu Y, Giovannucci E. Diabetes mellitus and risk of prostate cancer in the health professionals follow-up study. Int J Cancer. 2009;124(6):1398–403. doi:10.1002/ijc.24044.
Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Willett WC. Diabetes mellitus and risk of prostate cancer (United States). Cancer Causes Control. 1998;9(1):3–9.
Fall K, Garmo H, Gudbjornsdottir S, Stattin P, Zethelius B. Diabetes mellitus and prostate cancer risk; a nationwide case-control study within PCBaSe Sweden. Cancer Epidemiol Biomark Prev. 2013;22(6):1102–9. doi:10.1158/1055-9965.EPI-12-1046.
Xu H, Jiang HW, Ding GX, Zhang H, Zhang LM, Mao SH, Ding Q. Diabetes mellitus and prostate cancer risk of different grade or stage: a systematic review and meta-analysis. Diabetes Res Clin Pract. 2013;99(3):241–9. doi:10.1016/j.diabres.2012.12.003.
Leitzmann MF, Ahn J, Albanes D, Hsing AW, Schatzkin A, Chang SC, Huang WY, Weiss JM, Danforth KN, Grubb RL 3rd, Andriole GL, Prostate LC. Ovarian Trial Project T. Diabetes mellitus and prostate cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Cancer Causes Control. 2008;19(10):1267–76. doi:10.1007/s10552-008-9198-6.
Tsilidis KK, Allen NE, Appleby PN, Rohrmann S, Nothlings U, Arriola L, Gunter MJ, Chajes V, Rinaldi S, Romieu I, Murphy N, Riboli E, Tzoulaki I, Kaaks R, Lukanova A, Boeing H, Pischon T, Dahm CC, Overvad K, Quiros JR, Fonseca-Nunes A, Molina-Montes E, Gavrila Chervase D, Ardanaz E, Khaw KT, Wareham NJ, Roswall N, Tjonneland A, Lagiou P, Trichopoulos D, Trichopoulou A, Palli D, Pala V, Tumino R, Vineis P, Bueno-de-Mesquita HB, Malm J, Orho-Melander M, Johansson M, Stattin P, Travis RC, Key TJ. Diabetes mellitus and risk of prostate cancer in the European Prospective Investigation into Cancer and Nutrition. Int J Cancer. 2015;136(2):372–81. doi:10.1002/ijc.28989.
Turner EL, Lane JA, Donovan JL, Davis MJ, Metcalfe C, Neal DE, Hamdy FC, Martin RM. Association of diabetes mellitus with prostate cancer: nested case-control study (Prostate testing for cancer and treatment study). Int J Cancer. 2011;128(2):440–6. doi:10.1002/ijc.25360.
Zhu K, Lee IM, Sesso HD, Buring JE, Levine RS, Gaziano JM. History of diabetes mellitus and risk of prostate cancer in physicians. Am J Epidemiol. 2004;159(10):978–82.
Lee J, Giovannucci E, Jeon JY. Diabetes and mortality in patients with prostate cancer: a meta-analysis. Springerplus. 2016;5(1):1548. doi:10.1186/s40064-016-3233-y.
Batty GD, Kivimaki M, Clarke R, Davey Smith G, Shipley MJ. Modifiable risk factors for prostate cancer mortality in London: forty years of follow-up in the Whitehall study. Cancer Causes Control. 2011;22(2):311–8. doi:10.1007/s10552-010-9691-6.
Best LG, Garcia-Esquinas E, Yeh JL, Yeh F, Zhang Y, Lee ET, Howard BV, Farley JH, Welty TK, Rhoades DA, Rhoades ER, Umans JG, Navas-Acien A. Association of diabetes and cancer mortality in American Indians: the Strong Heart Study. Cancer Causes Control. 2015;26(11):1551–60. doi:10.1007/s10552-015-0648-7.
Baradaran N, Ahmadi H, Salem S, Lotfi M, Jahani Y, Baradaran N, Mehrsai AR, Pourmand G. The protective effect of diabetes mellitus against prostate cancer: role of sex hormones. Prostate. 2009;69(16):1744–50. doi:10.1002/pros.21023.
Giovannucci E, Michaud D. The role of obesity and related metabolic disturbances in cancers of the colon, prostate, and pancreas. Gastroenterology. 2007;132(6):2208–25. doi:10.1053/j.gastro.2007.03.050.
Weir GC, Bonner-Weir S. Five stages of evolving beta-cell dysfunction during progression to diabetes. Diabetes. 2004;53(Suppl 3):S16–21.
Wu C, Moreira DM, Gerber L, Rittmaster RS, Andriole GL, Freedland SJ. Diabetes and prostate cancer risk in the REDUCE trial. Prostate Cancer Prostatic Dis. 2011;14(4):326–31. doi:10.1038/pcan.2011.28.
Will JC, Vinicor F, Calle EE. Is diabetes mellitus associated with prostate cancer incidence and survival? Epidemiology. 1999;10(3):313–8.
Tseng CH. Diabetes and risk of prostate cancer: a study using the National Health Insurance. Diabetes Care. 2011;34(3):616–21. doi:10.2337/dc10-1640.
Tavani A, Gallus S, Bosetti C, Tzonou A, Lagiou P, Negri E, Trichopoulos D, La Vecchia C. Diabetes and the risk of prostate cancer. Eur J Cancer Prev. 2002;11(2):125–8.
Atchison EA, Gridley G, Carreon JD, Leitzmann MF, McGlynn KA. Risk of cancer in a large cohort of U.S. veterans with diabetes. Int J Cancer. 2011;128(3):635–43. doi:10.1002/ijc.25362.
Joshua AM, Zannella VE, Downes MR, Bowes B, Hersey K, Koritzinsky M, Schwab M, Hofmann U, Evans A, van der Kwast T, Trachtenberg J, Finelli A, Fleshner N, Sweet J, Pollak M. A pilot ‘window of opportunity’ neoadjuvant study of metformin in localised prostate cancer. Prostate Cancer Prostatic Dis. 2014;17(3):252–8. doi:10.1038/pcan.2014.20.
Pernicova I, Korbonits M. Metformin—mode of action and clinical implications for diabetes and cancer. Nat Rev Endocrinol. 2014;10(3):143–56. doi:10.1038/nrendo.2013.256.
Hardie DG. Minireview: the AMP-activated protein kinase cascade: the key sensor of cellular energy status. Endocrinology. 2003;144(12):5179–83. doi:10.1210/en.2003-0982.
Hadad SM, Fleming S, Thompson AM. Targeting AMPK: a new therapeutic opportunity in breast cancer. Crit Rev Oncol Hematol. 2008;67(1):1–7. doi:10.1016/j.critrevonc.2008.01.007.
Dowling RJ, Niraula S, Stambolic V, Goodwin PJ. Metformin in cancer: translational challenges. J Mol Endocrinol. 2012;48(3):R31–43. doi:10.1530/JME-12-0007.
Pollak M. Insulin and insulin-like growth factor signalling in neoplasia. Nat Rev Cancer. 2008;8(12):915–28. doi:10.1038/nrc2536.
Pollak MN. Investigating metformin for cancer prevention and treatment: the end of the beginning. Cancer Discov. 2012;2(9):778–90. doi:10.1158/2159-8290.CD-12-0263.
Belfiore A. The role of insulin receptor isoforms and hybrid insulin/IGF-I receptors in human cancer. Curr Pharm Des. 2007;13(7):671–86.
Wright JL, Plymate SR, Porter MP, Gore JL, Lin DW, Hu E, Zeliadt SB. Hyperglycemia and prostate cancer recurrence in men treated for localized prostate cancer. Prostate Cancer Prostatic Dis. 2013;16(2):204–8. doi:10.1038/pcan.2013.5.
Goodwin PJ, Ennis M, Pritchard KI, Trudeau ME, Koo J, Madarnas Y, Hartwick W, Hoffman B, Hood N. Fasting insulin and outcome in early-stage breast cancer: results of a prospective cohort study. J Clin Oncol. 2002;20(1):42–51. doi:10.1200/JCO.2002.20.1.42.
Hammarsten J, Hogstedt B. Hyperinsulinaemia: a prospective risk factor for lethal clinical prostate cancer. Eur J Cancer. 2005;41(18):2887–95. doi:10.1016/j.ejca.2005.09.003.
Heni M, Hennenlotter J, Scharpf M, Lutz SZ, Schwentner C, Todenhofer T, Schilling D, Kuhs U, Gerber V, Machicao F, Staiger H, Haring HU, Stenzl A. Insulin receptor isoforms A and B as well as insulin receptor substrates-1 and -2 are differentially expressed in prostate cancer. PLoS One. 2012;7(12):e50953. doi:10.1371/journal.pone.0050953.
Anwar MA, Kheir WA, Eid S, Fares J, Liu X, Eid AH, Eid AA. Colorectal and prostate cancer risk in diabetes: metformin, an actor behind the scene. J Cancer. 2014;5(9):736–44. doi:10.7150/jca.9726.
Bailey CJ, Turner RC. Metformin. N Engl J Med. 1996;334(9):574–9. doi:10.1056/NEJM199602293340906.
Wright JL, Stanford JL. Metformin use and prostate cancer in Caucasian men: results from a population-based case-control study. Cancer Causes Control. 2009;20(9):1617–22. doi:10.1007/s10552-009-9407-y.
Murtola TJ, Tammela TL, Lahtela J, Auvinen A. Antidiabetic medication and prostate cancer risk: a population-based case-control study. Am J Epidemiol. 2008;168(8):925–31. doi:10.1093/aje/kwn190.
Preston MA, Riis AH, Ehrenstein V, Breau RH, Batista JL, Olumi AF, Mucci LA, Adami HO, Sorensen HT. Metformin use and prostate cancer risk. Eur Urol. 2014;66(6):1012–20. doi:10.1016/j.eururo.2014.04.027.
Evans JM, Donnelly LA, Emslie-Smith AM, Alessi DR, Morris AD. Metformin and reduced risk of cancer in diabetic patients. BMJ. 2005;330(7503):1304–5. doi:10.1136/bmj.38415.708634.F7.
Nordstrom T, Clements M, Karlsson R, Adolfsson J, Gronberg H. The risk of prostate cancer for men on aspirin, statin or antidiabetic medications. Eur J Cancer. 2015;51(6):725–33. doi:10.1016/j.ejca.2015.02.003.
Feng T, Sun X, Howard LE, Vidal AC, Gaines AR, Moreira DM, Castro-Santamaria R, Andriole GL, Freedland SJ. Metformin use and risk of prostate cancer: results from the REDUCE study. Cancer Prev Res (Phila). 2015;8(11):1055–60. doi:10.1158/1940-6207.CAPR-15-0141.
Azoulay L, Dell’Aniello S, Gagnon B, Pollak M, Suissa S. Metformin and the incidence of prostate cancer in patients with type 2 diabetes. Cancer Epidemiol Biomark Prev. 2011;20(2):337–44. doi:10.1158/1055-9965.EPI-10-0940.
Kowall B, Stang A, Rathmann W, Kostev K. No reduced risk of overall, colorectal, lung, breast, and prostate cancer with metformin therapy in diabetic patients: database analyses from Germany and the UK. Pharmacoepidemiol Drug Saf. 2015;24(8):865–74. doi:10.1002/pds.3823.
Franciosi M, Lucisano G, Lapice E, Strippoli GF, Pellegrini F, Nicolucci A. Metformin therapy and risk of cancer in patients with type 2 diabetes: systematic review. PLoS One. 2013;8(8):e71583. doi:10.1371/journal.pone.0071583.
Zhang P, Li H, Tan X, Chen L, Wang S. Association of metformin use with cancer incidence and mortality: a meta-analysis. Cancer Epidemiol. 2013;37(3):207–18. doi:10.1016/j.canep.2012.12.009.
Yu H, Yin L, Jiang X, Sun X, Wu J, Tian H, Gao X, He X. Effect of metformin on cancer risk and treatment outcome of prostate cancer: a meta-analysis of epidemiological observational studies. PLoS One. 2014;9(12):e116327. doi:10.1371/journal.pone.0116327.
Stopsack KH, Ziehr DR, Rider JR, Giovannucci EL. Metformin and prostate cancer mortality: a meta-analysis. Cancer Causes Control. 2016;27(1):105–13. doi:10.1007/s10552-015-0687-0.
Raval AD, Thakker D, Vyas A, Salkini M, Madhavan S, Sambamoorthi U. Impact of metformin on clinical outcomes among men with prostate cancer: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2015;18(2):110–21. doi:10.1038/pcan.2014.52.
Coyle C, Cafferty FH, Vale C, Langley RE. Metformin as an adjuvant treatment for cancer: a systematic review and meta-analysis. Ann Oncol. 2016;27(12):2184–95. doi:10.1093/annonc/mdw410.
Deng D, Yang Y, Tang X, Skrip L, Qiu J, Wang Y, Zhang F. Association between metformin therapy and incidence, recurrence and mortality of prostate cancer: evidence from a meta-analysis. Diabetes Metab Res Rev. 2015;31(6):595–602. doi:10.1002/dmrr.2645.
Nobes JP, Langley SE, Klopper T, Russell-Jones D, Laing RW. A prospective, randomized pilot study evaluating the effects of metformin and lifestyle intervention on patients with prostate cancer receiving androgen deprivation therapy. BJU Int. 2012;109(10):1495–502. doi:10.1111/j.1464-410X.2011.10555.x.
Chen YB, Chen Q, Wang Z, Zhou J. Insulin therapy and risk of prostate cancer: a systematic review and meta-analysis of observational studies. PLoS One. 2013;8(11):e81594. doi:10.1371/journal.pone.0081594.
Hsieh MC, Lee TC, Cheng SM, Tu ST, Yen MH, Tseng CH. The influence of type 2 diabetes and glucose-lowering therapies on cancer risk in the Taiwanese. Exp Diabetes Res. 2012;2012:413782. doi:10.1155/2012/413782.
Qiu H, Rhoads GG, Berlin JA, Marcella SW, Demissie K. Initial metformin or sulphonylurea exposure and cancer occurrence among patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2013;15(4):349–57. doi:10.1111/dom.12036.
Onitilo AA, Stankowski RV, Berg RL, Engel JM, Glurich I, Williams GM, Doi SA. Type 2 diabetes mellitus, glycemic control, and cancer risk. Eur J Cancer Prev. 2014;23(2):134–40. doi:10.1097/CEJ.0b013e3283656394.
Hitron A, Adams V, Talbert J, Steinke D. The influence of antidiabetic medications on the development and progression of prostate cancer. Cancer Epidemiol. 2012;36(4):e243–50. doi:10.1016/j.canep.2012.02.005.
Haring A, Murtola TJ, Talala K, Taari K, Tammela TL, Auvinen A. Antidiabetic drug use and prostate cancer risk in the Finnish Randomized Study of Screening for Prostate Cancer. Scand J Urol. 2017;51(1):5–12. doi:10.1080/21681805.2016.1271353.
Frohlich E, Wahl R. Chemotherapy and chemoprevention by thiazolidinediones. Biomed Res Int. 2015;2015:845340. doi:10.1155/2015/845340.
Matsuyama M, Yoshimura R. Peroxisome proliferator-activated receptor-gamma is a potent target for prevention and treatment in human prostate and testicular cancer. PPAR Res. 2008;2008:249849. doi:10.1155/2008/249849.
Erdmann E, Harding S, Lam H, Perez A. Ten-year observational follow-up of PROactive: a randomized cardiovascular outcomes trial evaluating pioglitazone in type 2 diabetes. Diabetes Obes Metab. 2016;18(3):266–73. doi:10.1111/dom.12608.
Lewis JD, Habel LA, Quesenberry CP, Strom BL, Peng T, Hedderson MM, Ehrlich SF, Mamtani R, Bilker W, Vaughn DJ, Nessel L, Van Den Eeden SK, Ferrara A. Pioglitazone use and risk of bladder cancer and other common cancers in persons with diabetes. JAMA. 2015;314(3):265–77. doi:10.1001/jama.2015.7996.
Boxall N, Bennett D, Hunger M, Dolin P, Thompson PL. Evaluation of exposure to pioglitazone and risk of prostate cancer: a nested case-control study. BMJ Open Diabetes Res Care. 2016;4(1):e000303. doi:10.1136/bmjdrc-2016-000303.
Kernan WN, Viscoli CM, Furie KL, Young LH, Inzucchi SE, Gorman M, Guarino PD, Lovejoy AM, Peduzzi PN, Conwit R, Brass LM, Schwartz GG, Adams HP Jr, Berger L, Carolei A, Clark W, Coull B, Ford GA, Kleindorfer D, O'Leary JR, Parsons MW, Ringleb P, Sen S, Spence JD, Tanne D, Wang D, Winder TR, Investigators IT. Pioglitazone after ischemic stroke or transient ischemic attack. N Engl J Med. 2016;374(14):1321–31. doi:10.1056/NEJMoa1506930.
Platz EA, Clinton SK, Giovannucci E. Association between plasma cholesterol and prostate cancer in the PSA era. Int J Cancer. 2008;123(7):1693–8. doi:10.1002/ijc.23715.
Platz EA, Till C, Goodman PJ, Parnes HL, Figg WD, Albanes D, Neuhouser ML, Klein EA, Thompson IM Jr, Kristal AR. Men with low serum cholesterol have a lower risk of high-grade prostate cancer in the placebo arm of the prostate cancer prevention trial. Cancer Epidemiol Biomark Prev. 2009;18(11):2807–13. doi:10.1158/1055-9965.EPI-09-0472.
Farwell WR, D’Avolio LW, Scranton RE, Lawler EV, Gaziano JM. Statins and prostate cancer diagnosis and grade in a veterans population. J Natl Cancer Inst. 2011;103(11):885–92. doi:10.1093/jnci/djr108.
Shafique K, McLoone P, Qureshi K, Leung H, Hart C, Morrison DS. Cholesterol and the risk of grade-specific prostate cancer incidence: evidence from two large prospective cohort studies with up to 37 years’ follow up. BMC Cancer. 2012;12:25. doi:10.1186/1471-2407-12-25.
Mondul AM, Clipp SL, Helzlsouer KJ, Platz EA. Association between plasma total cholesterol concentration and incident prostate cancer in the CLUE II cohort. Cancer Causes Control. 2010;21(1):61–8. doi:10.1007/s10552-009-9434-8.
Mondul AM, Weinstein SJ, Virtamo J, Albanes D. Serum total and HDL cholesterol and risk of prostate cancer. Cancer Causes Control. 2011;22(11):1545–52. doi:10.1007/s10552-011-9831-7.
Kok DE, van Roermund JG, Aben KK, den Heijer M, Swinkels DW, Kampman E, Kiemeney LA. Blood lipid levels and prostate cancer risk; a cohort study. Prostate Cancer Prostatic Dis. 2011;14(4):340–5. doi:10.1038/pcan.2011.30.
Iso H, Ikeda A, Inoue M, Sato S, Tsugane S, Group JS. Serum cholesterol levels in relation to the incidence of cancer: the JPHC study cohorts. Int J Cancer. 2009;125(11):2679–86. doi:10.1002/ijc.24668.
Eichholzer M, Stahelin HB, Gutzwiller F, Ludin E, Bernasconi F. Association of low plasma cholesterol with mortality for cancer at various sites in men: 17-y follow-up of the prospective Basel study. Am J Clin Nutr. 2000;71(2):569–74.
Wallace RB, Rost C, Burmeister LF, Pomrehn PR. Cancer incidence in humans: relationship to plasma lipids and relative weight. J Natl Cancer Inst. 1982;68(6):915–8.
Chyou PH, Nomura AM, Stemmermann GN, Kato I. Prospective study of serum cholesterol and site-specific cancers. J Clin Epidemiol. 1992;45(3):287–92.
Hiatt RA, Fireman BH. Serum cholesterol and the incidence of cancer in a large cohort. J Chronic Dis. 1986;39(11):861–70.
Steenland K, Nowlin S, Palu S. Cancer incidence in the National Health and Nutrition Survey I. Follow-up data: diabetes, cholesterol, pulse and physical activity. Cancer Epidemiol Biomark Prev. 1995;4(8):807–11.
Knekt P, Reunanen A, Aromaa A, Heliovaara M, Hakulinen T, Hakama M. Serum cholesterol and risk of cancer in a cohort of 39,000 men and women. J Clin Epidemiol. 1988;41(6):519–30.
Morris DL, Borhani NO, Fitzsimons E, Hardy RJ, Hawkins CM, Kraus JF, Labarthe DR, Mastbaum L, Payne GH. Serum cholesterol and cancer in the Hypertension Detection and Follow-up Program. Cancer. 1983;52(9):1754–9.
Ahn J, Lim U, Weinstein SJ, Schatzkin A, Hayes RB, Virtamo J, Albanes D. Prediagnostic total and high-density lipoprotein cholesterol and risk of cancer. Cancer Epidemiol Biomark Prev. 2009;18(11):2814–21. doi:10.1158/1055-9965.EPI-08-1248.
Kitahara CM, Berrington de Gonzalez A, Freedman ND, Huxley R, Mok Y, Jee SH, Samet JM. Total cholesterol and cancer risk in a large prospective study in Korea. J Clin Oncol. 2011;29(12):1592–8. doi:10.1200/JCO.2010.31.5200.
Van Hemelrijck M, Garmo H, Holmberg L, Walldius G, Jungner I, Hammar N, Lambe M. Prostate cancer risk in the Swedish AMORIS study: the interplay among triglycerides, total cholesterol, and glucose. Cancer. 2011;117(10):2086–95. doi:10.1002/cncr.25758.
Van Hemelrijck M, Walldius G, Jungner I, Hammar N, Garmo H, Binda E, Hayday A, Lambe M, Holmberg L. Low levels of apolipoprotein A-I and HDL are associated with risk of prostate cancer in the Swedish AMORIS study. Cancer Causes Control. 2011;22(7):1011–9. doi:10.1007/s10552-011-9774-z.
Gu Q, Paulose-Ram R, Burt VL, Kit BK. Prescription cholesterol-lowering medication use in adults aged 40 and over: United States, 2003–2012. NCHS Data Brief. 2014;177:1–8.
Moon H, Hill MM, Roberts MJ, Gardiner RA, Brown AJ. Statins: protectors or pretenders in prostate cancer? Trends Endocrinol Metab. 2014;25(4):188–96. doi:10.1016/j.tem.2013.12.007.
Alfaqih MA, Allott EH, Hamilton RJ, Freeman MR, Freedland SJ. The current evidence on statin use and prostate cancer prevention: are we there yet? Nat Rev Urol. 2017;14(2):107–19. doi:10.1038/nrurol.2016.199.
Bansal D, Undela K, D’Cruz S, Schifano F. Statin use and risk of prostate cancer: a meta-analysis of observational studies. PLoS One. 2012;7(10):e46691. doi:10.1371/journal.pone.0046691.
Lustman A, Nakar S, Cohen AD, Vinker S. Statin use and incident prostate cancer risk: does the statin brand matter? A population-based cohort study. Prostate Cancer Prostatic Dis. 2014;17(1):6–9. doi:10.1038/pcan.2013.34.
Jespersen CG, Norgaard M, Friis S, Skriver C, Borre M. Statin use and risk of prostate cancer: a Danish population-based case-control study, 1997–2010. Cancer Epidemiol. 2014;38(1):42–7. doi:10.1016/j.canep.2013.10.010.
Kantor ED, Lipworth L, Fowke JH, Giovannucci EL, Mucci LA, Signorello LB. Statin use and risk of prostate cancer: results from the Southern Community Cohort Study. Prostate. 2015;75(13):1384–93. doi:10.1002/pros.23019.
Freedland SJ, Hamilton RJ, Gerber L, Banez LL, Moreira DM, Andriole GL, Rittmaster RS. Statin use and risk of prostate cancer and high-grade prostate cancer: results from the REDUCE study. Prostate Cancer Prostatic Dis. 2013;16(3):254–9. doi:10.1038/pcan.2013.10.
Platz EA, Tangen CM, Goodman PJ, Till C, Parnes HL, Figg WD, Albanes D, Neuhouser ML, Klein EA, Lucia MS, Thompson IM Jr, Kristal AR. Statin drug use is not associated with prostate cancer risk in men who are regularly screened. J Urol. 2014;192(2):379–84. doi:10.1016/j.juro.2014.01.095.
Chan JM, Litwack-Harrison S, Bauer SR, Daniels NA, Wilt TJ, Shannon J, Bauer DC. Statin use and risk of prostate cancer in the prospective Osteoporotic Fractures in Men (MrOS) Study. Cancer Epidemiol Biomark Prev. 2012;21(10):1886–8. doi:10.1158/1055-9965.EPI-12-0816.
Tan P, Wei S, Yang L, Tang Z, Cao D, Liu L, Lei J, Fan Y, Gao L, Wei Q. The effect of statins on prostate cancer recurrence and mortality after definitive therapy: a systematic review and meta-analysis. Sci Rep. 2016;6:29106. doi:10.1038/srep29106.
Meng Y, Liao YB, Xu P, Wei WR, Wang J. Statin use and mortality of patients with prostate cancer: a meta-analysis. Onco Targets Ther. 2016;9:1689–96. doi:10.2147/OTT.S97993.
Wright JL, Kwon EM, Ostrander EA, Montgomery RB, Lin DW, Vessella R, Stanford JL, Mostaghel EA. Expression of SLCO transport genes in castration-resistant prostate cancer and impact of genetic variation in SLCO1B3 and SLCO2B1 on prostate cancer outcomes. Cancer Epidemiol Biomark Prev. 2011;20(4):619–27. doi:10.1158/1055-9965.EPI-10-1023.
Mostaghel E, Nelson PS, Nelson C, Montgomery RB. Intraprostatic steroidogenic enzymes—letter. Cancer Res. 2010;70(20):8247–8249.; author reply 9–50. doi:10.1158/0008-5472.CAN-10-1458.
Harshman LC. Mind the gap: what is driving the survival disparity between the sexes in bladder cancer? Cancer. 2016;122(13):1966–70. doi:10.1002/cncr.30027.
Harshman LC, Wang X, Nakabayashi M, Xie W, Valenca L, Werner L, Yu Y, Kantoff AM, Sweeney CJ, Mucci LA, Pomerantz M, Lee GS, Kantoff PW. Statin use at the time of initiation of androgen deprivation therapy and time to progression in patients with hormone-sensitive prostate cancer. JAMA Oncol. 2015;1(4):495–504. doi:10.1001/jamaoncol.2015.0829.
Boegemann M, Schlack K, Fischer AK, Gerss J, Steinestel J, Semjonow A, Schrader AJ, Krabbe LM. Influence of statins on survival outcome in patients with metastatic castration resistant prostate cancer treated with abiraterone acetate. PLoS One. 2016;11(9):e0161959. doi:10.1371/journal.pone.0161959.
Fitzpatrick AL, Daling JR, Furberg CD, Kronmal RA, Weissfeld JL. Hypertension, heart rate, use of antihypertensives, and incident prostate cancer. Ann Epidemiol. 2001;11(8):534–42.
Rosenberg L, Rao RS, Palmer JR, Strom BL, Stolley PD, Zauber AG, Warshauer ME, Shapiro S. Calcium channel blockers and the risk of cancer. JAMA. 1998;279(13):1000–4.
Lindgren AM, Nissinen AM, Tuomilehto JO, Pukkala E. Cancer pattern among hypertensive patients in North Karelia. Finland J Hum Hypertens. 2005;19(5):373–9. doi:10.1038/sj.jhh.1001834.
Friedman GD. Blood pressure and heart rate: no evidence for a positive association with prostate cancer. Ann Epidemiol. 1997;7(7):486–9.
Hole DJ, Hawthorne VM, Isles CG, McGhee SM, Robertson JW, Gillis CR, Wapshaw JA,Lever AF. Incidence of and mortality from cancer in hypertensive patients. BMJ. 1993;306(6878):609–11.
Batty GD, Shipley MJ, Marmot MG, Davey Smith G, Whitehall S. Blood pressure and site-specific cancer mortality: evidence from the original Whitehall study. Br J Cancer. 2003;89(7):1243–7. doi:10.1038/sj.bjc.6601255.
Martin RM, Vatten L, Gunnell D, Romundstad P. Blood pressure and risk of prostate cancer: Cohort Norway (CONOR). Cancer Causes Control. 2010;21(3):463–72. doi:10.1007/s10552-009-9477-x.
Pai PY, Hsieh VC, Wang CB, Wu HC, Liang WM, Chang YJ, Wu TN. Long term antihypertensive drug use and prostate cancer risk: a 9-year population-based cohort analysis. Int J Cardiol. 2015;193:1–7. doi:10.1016/j.ijcard.2015.05.042.
Stocks T, Hergens MP, Englund A, Ye W, Stattin P. Blood pressure, body size and prostate cancer risk in the Swedish Construction Workers cohort. Int J Cancer. 2010;127(7):1660–8. doi:10.1002/ijc.25171.
Palm D, Lang K, Niggemann B, Drell TL, Masur K, Zaenker KS, Entschladen F. The norepinephrine-driven metastasis development of PC-3 human prostate cancer cells in BALB/c nude mice is inhibited by beta-blockers. Int J Cancer. 2006;118(11):2744–9. doi:10.1002/ijc.21723.
Ronquist G, Rodriguez LA, Ruigomez A, Johansson S, Wallander MA, Frithz G, Svardsudd K. Association between captopril, other antihypertensive drugs and risk of prostate cancer. Prostate. 2004;58(1):50–6. doi:10.1002/pros.10294.
Rodriguez C, Jacobs EJ, Deka A, Patel AV, Bain EB, Thun MJ, Calle EE. Use of blood-pressure-lowering medication and risk of prostate cancer in the Cancer Prevention Study II Nutrition Cohort. Cancer Causes Control. 2009;20(5):671–9. doi:10.1007/s10552-008-9280-0.
Friis S, Sorensen HT, Mellemkjaer L, McLaughlin JK, Nielsen GL, Blot WJ, Olsen JH. Angiotensin-converting enzyme inhibitors and the risk of cancer: a population-based cohort study in Denmark. Cancer. 2001;92(9):2462–70.
Lindholm LH, Anderson H, Ekbom T, Hansson L, Lanke J, Dahlof B, de Faire U, Forsen K, Hedner T, Linjer E, Schersten B, Wester P, Moller T. Relation between drug treatment and cancer in hypertensives in the Swedish Trial in Old Patients with Hypertension 2: a 5-year, prospective, randomised, controlled trial. Lancet. 2001;358(9281):539–44.
Perron L, Bairati I, Harel F, Meyer F. Antihypertensive drug use and the risk of prostate cancer (Canada). Cancer Causes Control. 2004;15(6):535–41. doi:10.1023/B:CACO.0000036152.58271.5e.
Lever AF, Hole DJ, Gillis CR, McCallum IR, McInnes GT, MacKinnon PL, Meredith PA, Murray LS, Reid JL, Robertson JW. Do inhibitors of angiotensin-I-converting enzyme protect against risk of cancer? Lancet. 1998;352(9123):179–84. doi:10.1016/S0140-6736(98)03228-0.
Morote J, Planas J. Antihypertensive drugs and the risk of prostate cancer. Eur Urol. 2011;60(6):1309–10. doi:10.1016/j.eururo.2011.09.009.
Vezina RM, Lesko SM, Rosenberg L, Shapiro S. Calcium channel blocker use and the risk of prostate cancer. Am J Hypertens. 1998;11(12):1420–5.
Kemppainen KJ, Tammela TL, Auvinen A, Murtola TJ. The association between antihypertensive drug use and incidence of prostate cancer in Finland: a population-based case-control study. Cancer Causes Control. 2011;22(10):1445–52. doi:10.1007/s10552-011-9819-3.
Yoon C, Yang HS, Jeon I, Chang Y, Park SM. Use of angiotensin-converting-enzyme inhibitors or angiotensin-receptor blockers and cancer risk: a meta-analysis of observational studies. CMAJ. 2011;183(14):E1073–84. doi:10.1503/cmaj.101497.
Sipahi I, Debanne SM, Rowland DY, Simon DI, Fang JC. Angiotensin-receptor blockade and risk of cancer: meta-analysis of randomised controlled trials. Lancet Oncol. 2010;11(7):627–36. doi:10.1016/S1470-2045(10)70106-6.
Collaboration ARBT. Effects of telmisartan, irbesartan, valsartan, candesartan, and losartan on cancers in 15 trials enrolling 138,769 individuals. J Hypertens. 2011;29(4):623–35. doi:10.1097/HJH.0b013e328344a7de.
Pahor M, Guralnik JM, Ferrucci L, Corti MC, Salive ME, Cerhan JR, Wallace RB, Havlik RJ. Calcium-channel blockade and incidence of cancer in aged populations. Lancet. 1996;348(9026):493–7. doi:10.1016/S0140-6736(96)04277-8.
Jick H, Jick S, Derby LE, Vasilakis C, Myers MW, Meier CR. Calcium-channel blockers and risk of cancer. Lancet. 1997;349(9051):525–8. doi:10.1016/S0140-6736(97)80084-0.
Sorensen HT, Olsen JH, Mellemkjaer L, Marie A, Steffensen FH, McLaughlin JK, Baron JA. Cancer risk and mortality in users of calcium channel blockers. A cohort study. Cancer. 2000;89(1):165–70.
Debes JD, Roberts RO, Jacobson DJ, Girman CJ, Lieber MM, Tindall DJ, Jacobsen SJ. Inverse association between prostate cancer and the use of calcium channel blockers. Cancer Epidemiol Biomark Prev. 2004;13(2):255–9.
Thomas JA 2nd, Gerber L, Banez LL, Moreira DM, Rittmaster RS, Andriole GL, Freedland SJ. Prostate cancer risk in men with baseline history of coronary artery disease: results from the REDUCE Study. Cancer Epidemiol Biomark Prev. 2012;21(4):576–81. doi:10.1158/1055-9965.EPI-11-1017.
Lin H, Juang JL, Wang PS. Involvement of Cdk5/p25 in digoxin-triggered prostate cancer cell apoptosis. J Biol Chem. 2004;279(28):29302–7. doi:10.1074/jbc.M403664200.
Stoffer SS, Hynes KM, Jiang NS, Ryan RJ. Digoxin and abnormal serum hormone levels. JAMA. 1973;225(13):1643–4.
Newman RA, Yang P, Pawlus AD, Block KI. Cardiac glycosides as novel cancer therapeutic agents. Mol Interv. 2008;8(1):36–49. doi:10.1124/mi.8.1.8.
McConkey DJ, Lin Y, Nutt LK, Ozel HZ, Newman RA. Cardiac glycosides stimulate Ca2+ increases and apoptosis in androgen-independent, metastatic human prostate adenocarcinoma cells. Cancer Res. 2000;60(14):3807–12.
Yeh JY, Huang WJ, Kan SF, Wang PS. Inhibitory effects of digitalis on the proliferation of androgen dependent and independent prostate cancer cells. J Urol. 2001;166(5):1937–42.
Zhang H, Qian DZ, Tan YS, Lee K, Gao P, Ren YR, Rey S, Hammers H, Chang D, Pili R, Dang CV, Liu JO, Semenza GL. Digoxin and other cardiac glycosides inhibit HIF-1alpha synthesis and block tumor growth. Proc Natl Acad Sci USA. 2008;105(50):19579–86. doi:10.1073/pnas.0809763105.
Platz EA, Yegnasubramanian S, Liu JO, Chong CR, Shim JS, Kenfield SA, Stampfer MJ, Willett WC, Giovannucci E, Nelson WG. A novel two-stage, transdisciplinary study identifies digoxin as a possible drug for prostate cancer treatment. Cancer Discov. 2011;1(1):68–77. doi:10.1158/2159-8274.CD-10-0020.
Wright JL, Hansten PD, Stanford JL. Is digoxin use for cardiovascular disease associated with risk of prostate cancer? Prostate. 2014;74(1):97–102. doi:10.1002/pros.22733.
Kaapu KJ, Murtola TJ, Maattanen L, Talala K, Taari K, Tammela TL,Auvinen A. Prostate cancer risk among users of digoxin and other antiarrhythmic drugs in the Finnish Prostate Cancer Screening Trial. Cancer Causes Control. 2016;27(2):157–64. doi:10.1007/s10552-015-0693-2.
Karasneh RA, Murray LJ, Hughes CM, Cardwell CR. Digoxin use after diagnosis of prostate cancer and survival: a population-based cohort study. Pharmacoepidemiol Drug Saf. 2016;25(9):1099–103. doi:10.1002/pds.4018.
Flahavan EM, Sharp L, Bennett K, Barron TI. A cohort study of digoxin exposure and mortality in men with prostate cancer. BJU Int. 2014;113(2):236–45. doi:10.1111/bju.12287.
Kaapu KJ, Ahti J, Tammela TL, Auvinen A, Murtola TJ. Sotalol, but not digoxin is associated with decreased prostate cancer risk: a population-based case-control study. Int J Cancer. 2015;137(5):1187–95. doi:10.1002/ijc.29470.
Hayden M, Pignone M, Phillips C, Mulrow C. Aspirin for the primary prevention of cardiovascular events: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;136(2):161–72.
Hsu AL, Ching TT, Wang DS, Song X, Rangnekar VM, Chen CS. The cyclooxygenase-2 inhibitor celecoxib induces apoptosis by blocking Akt activation in human prostate cancer cells independently of Bcl-2. J Biol Chem. 2000;275(15):11397–403.
Kirschenbaum A, Liu X, Yao S, Levine AC. The role of cyclooxygenase-2 in prostate cancer. Urology. 2001;58(2 Suppl 1):127–31.
Liu Y, Chen JQ, Xie L, Wang J, Li T, He Y, Gao Y, Qin X, Li S. Effect of aspirin and other non-steroidal anti-inflammatory drugs on prostate cancer incidence and mortality: a systematic review and meta-analysis. BMC Med. 2014;12:55. doi:10.1186/1741-7015-12-55.
Wright JL, Chery L, Holt S, Lin DW, Luedeke M, Rinckleb AE, Maier C, Stanford JL. Aspirin and NSAID use in association with molecular subtypes of prostate cancer defined by TMPRSS2:ERG fusion status. Prostate Cancer Prostatic Dis. 2016;19(1):53–6. doi:10.1038/pcan.2015.49.
Pierce BL, Plymate S, Ostrander EA, Stanford JL. Diabetes mellitus and prostate cancer risk. Prostate. 2008;68(10):1126–32. doi:10.1002/pros.20777.
Fukui M, Tanaka M, Kadono M, Imai S, Hasegawa G, Yoshikawa T, Nakamura N. Serum prostate-specific antigen levels in men with type 2 diabetes. Diabetes Care. 2008;31(5):930–1. doi:10.2337/dc07-1962.
Muller H, Raum E, Rothenbacher D, Stegmaier C, Brenner H. Association of diabetes and body mass index with levels of prostate-specific antigen: implications for correction of prostate-specific antigen cutoff values? Cancer Epidemiol Biomark Prev. 2009;18(5):1350–6. doi:10.1158/1055-9965.EPI-08-0794.
Werny DM, Saraiya M, Gregg EW. Prostate-specific antigen values in diabetic and nondiabetic US men, 2001–2002. Am J Epidemiol. 2006;164(10):978–83. doi:10.1093/aje/kwj311.
Fowke JH, Motley SS, Cookson MS, Concepcion R, Chang SS, Wills ML, Smith JA Jr. The association between body size, prostate volume and prostate-specific antigen. Prostate Cancer Prostatic Dis. 2007;10(2):137–42. doi:10.1038/sj.pcan.4500924.
Jayalath VH, Ireland C, Fleshner NE, Hamilton RJ, Jenkins DJ. The relationship between metformin and serum prostate-specific antigen levels. Prostate. 2016;76(15):1445–53. doi:10.1002/pros.23228.
Werny DM, Thompson T, Saraiya M, Freedman D, Kottiri BJ, German RR, Wener M. Obesity is negatively associated with prostate-specific antigen in U.S. men, 2001–2004. Cancer Epidemiol Biomark Prev. 2007;16(1):70–6. doi:10.1158/1055-9965.EPI-06-0588.
Banez LL, Hamilton RJ, Partin AW, Vollmer RT, Sun L, Rodriguez C, Wang Y, Terris MK, Aronson WJ, Presti JC Jr, Kane CJ, Amling CL, Moul JW, Freedland SJ. Obesity-related plasma hemodilution and PSA concentration among men with prostate cancer. JAMA. 2007;298(19):2275–80. doi:10.1001/jama.298.19.2275.
Culp S, Porter M. The effect of obesity and lower serum prostate-specific antigen levels on prostate-cancer screening results in American men. BJU Int. 2009;104(10):1457–61. doi:10.1111/j.1464-410X.2009.08646.x.
Hekal IA, Ibrahiem EI. Obesity-PSA relationship: a new formula. Prostate Cancer Prostatic Dis. 2010;13(2):186–90. doi:10.1038/pcan.2009.53.
Hamilton RJ, Goldberg KC, Platz EA, Freedland SJ. The influence of statin medications on prostate-specific antigen levels. J Natl Cancer Inst. 2008;100(21):1511–8. doi:10.1093/jnci/djn362.
Wright JL, Lin DW, Stanford JL. The effect of demographic and clinical factors on the relationship between BMI and PSA levels. Prostate. 2011;71(15):1631–7. doi:10.1002/pros.21380.
Andriole GL, Bostwick DG, Brawley OW, Gomella LG, Marberger M, Montorsi F, Pettaway CA, Tammela TL, Teloken C, Tindall DJ, Somerville MC, Wilson TH, Fowler IL, Rittmaster RS, Group RS. Effect of dutasteride on the risk of prostate cancer. N Engl J Med. 2010;362(13):1192–202. doi:10.1056/NEJMoa0908127.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Schenk, J.M., Wright, J.L. (2018). Consequence of Energy Imbalance in Prostate Cancer and Comorbidities. In: Platz, E., Berger, N. (eds) Energy Balance and Prostate Cancer. Energy Balance and Cancer, vol 14. Springer, Cham. https://doi.org/10.1007/978-3-319-64940-5_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-64940-5_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-64939-9
Online ISBN: 978-3-319-64940-5
eBook Packages: MedicineMedicine (R0)