
Abstract
Medulloblastoma is an invasive, high-grade (WHO grade IV) embryonal tumor defined both by histologic grade and location in the cerebellum.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Medulloblastoma
- Large cell medulloblastoma
- Anaplastic medulloblastoma
- Nodular medulloblastoma
- Desmoplastic medulloblastoma
- Extensively nodular
- Medullomyoblastoma
1 Overview
-
Medullobl astoma is an invasive, high-grade (WHO grade IV) embryonal tumor defined both by histologic grade and location in the cerebellum.
-
Even though this tumor shares histologic features with other central nervous system (CNS) embryonal tumors (primitive neuroectodermal tumors), it has been historically regarded as a distinct entity.
-
Recent molecular studies, including genomic and gene expression profiling as well as signaling pathway dysregulation and biologic studies, have now justified its historical clinical definition as a distinct clinicopathologic entity with predominant occurrence in children.
-
Most are sporadic.
-
They occur less frequently in the setting of hereditary syndromes. These include Turcot’s syndrome, with germline mutation of the adenomatous polyposis coli (APC) gene, and Gorlin’s syndrome, the nevoid basal cell carcinoma syndrome with germline mutation of the PTCH gene, seen in less than 2 % of medulloblastomas.
2 Clinical Features
-
Medulloblastomas account for 20 % of malignant CNS tumors in childhood, the second most common mali gnancy in childhood.
-
Most tumors occur in children below the age of 20, with a peak between 5 and 8 years of age. A second but smaller peak is seen at ages 35–40 years. Rarely, it may be congenital.
-
Patients present with symptoms and signs of cerebellar dysfunction, including truncal and appendicular ataxia, and raised intracranial pressure due to obstruction of the fourth ventricle and CSF flow, with headache, vomiting, and progressive lethargy.
3 Neuroimaging
-
Early onset of calcification of the falx cerebri, tentorium cerebelli, and dura, with bridging of the se lla turcica due to calcification of the diaphragma sellae is seen with CT scans in 60–80 % of patients with Gorlin’s syndrome (Fig. 8.1).
Fig. 8.1 
Axial CT scan of a patient with G orlin’s syndrome (also known as basal cell nevus syndrome) associated with medulloblastoma. Note the characteristic abnormal, heavy calcification outlining the free edge of the tentorium and the falx in this young child
-
Midline vermian mass lesions in children or lateral cerebellar hemispheric tumors in adults are typical.
-
Characteristically, MRI shows a predominantly solid mass, hypointense or isointense with gray matter, with moderate diffuse, nonhomogenous enhancement (Figs. 8.2, 8.3, 8.4, 8.5, 8.6, and 8.7).
Fig. 8.2 
Axial T2-weighted MR image (A) and apparent diffusion coefficient (ADC) maps (B) demonstrating a heterogeneously hyperintense mass extending bilaterally to the cerebellopontine angles in a 27-month-old boy. There is restricted diffusion within the tumor, which was confirmed to be a medulloblastoma on histology
Fig. 8.3 
Axial T1-weighted M R imaging before (A) and after (B) gadolinium demonstrates some central enhancement
Fig. 8.4 
Axial CT image showing hyperdense, centrally placed tumor within the posterior fossa, consistent with a highly cellular tumor such as a medulloblastoma or atypical teratoid/rhabdoid tumor (AT/RT)
Fig. 8.5 
Sagittal T1-weighted image (A) and T2-weighted image (B) demonstrates a T1-hypointense an d T2-hyperintense mass in the same patient as in Fig. 8.4
Fig. 8.6 
(A, B) Diffusion-weighted imaging in the same patient as in Fig. 8.4 shows restriction as may be seen in a med ulloblastoma, AT/RT or anaplastic ependymoma. This case was histologically proven to be a medulloblastoma
Fig. 8.7 
T1-weighted axial (A) and sagittal (B) MR images following gadolinium administration, showing moderate e nhancement, much less than would be seen with a solid pilocytic astrocytoma
-
There is often associated restricted diffusion consistent with a small-cell and densely cellular tumor (Figs. 8.2 and 8.6).
-
MR spectroscopy shows marked elevation of choline with little, if any, NAA peak (Fig. 8.8A).◦
Fig. 8.8 
(A) Typical appearanc es of MR spectroscopy utilizing a long TE in the same patient as in Fig. 8.7, demonstrating a marked decrease in N-acetyl aspartase (NAA), a marker of neuronal and axonal integrity, and a significant elevation in choline, a marker of cell membrane turnover. Also present is a lipid peak consistent with the presence of necrosis. (B, C) Coronal and axial T1-weighted post-gadolinium MR images show a cerebellar mass with grapelike nodules in a patient with an extensively nodular medulloblastoma
-
Elevation of the taurine peak may also be seen in medulloblastoma.
-
-
The extensively nodular variant often seen in patients less than 1 year old may present with multiple, grapelike, enhancing nodular features (Fig. 8.8B and C).
-
Diffuse leptomeningeal enhancement and thecal sac drop metastases, when present, are consistent with CSF dissemination and poorer prognosis (Figs. 8.9, 8.10, 8.11, 8.12, and 8.13).
Fig. 8.9 
Sagittal T1- weighted, post-gadolinium imaging of the lumbosacral spine in a patient with medulloblastoma, demo nstrating evidence for abnormal leptomeningeal enhancement in the dorsal surface of the thoracic cord, as well as evidence for extensive drop metastases within the distal thecal sac
Fig. 8.10 
Unenhanced axial CT scan demonstrating a mixed solid and cystic tumor arising in the posterior fossa a nd causing obstruction to the supratentorial ventricular system. The solid portion of the tumor appears hyperdense, consistent with high cellularity. Note also the high density outlining the Sylvian fissures, suspicious for disseminated tumor
Fig. 8.11 
(A) Restricted diffusion demonstrated within the enhancing solid portion of this tumor on an ADC map suggests a medulloblastoma, AT/RT, or anaplastic ependymoma in the differential diagno sis. (B) Note the presence of abnormal leptomeningeal enhancement in the axial T1-weighted, postcontrast image
Fig. 8.12 
Sagittal (A) and coronal (B) T1-weighted images from the same patient as in Fig. 8.11, following the administration of gadolinium. Florid, abnormal leptomeningeal enhancement is observed with hydrocephalus and extension of abnormal enhancement into the spinal canal. Histology revealed a medulloblastoma in this 15-month-old boy
Fig. 8.13 
(A, B) MR images of the spine, demonstrating extensive abnormal, thick leptomeningeal enhancement surrounding the entire spinal cord at the time of presentation
-
There is often evidence of mass effect, including severe dilatation of the third and lateral ventricles, transepend ymal CSF flow, and brainstem compression (Figs. 8.10 and 8.12).













4 Pathology
-
Grossly, medul loblastoma presents commonly as a midline vermian mass (Fig. 8.14).
Fig. 8.14 
Medulloblas toma arising in the vermis, with associated necrosis and hemorrhage
-
Resection specimens or intraoperative biopsies are often soft, gray-pink, and appear necrotic. Extensively nodular or desmoplastic tumors may sometimes have a soft to slightly firm consistency with a lobulated appearance.
-
Intraoperative cytologic imprints or smears
-
◦ Moderate cellular ity is characteristic. There is a good correlation between cytologic features and histologic classification as classic or nodular, anaplastic, or large cell medulloblastomas.
-
◦ Classic and nodular medulloblastomas demonstrate monolayered sheets of relatively uniform, round to oval (occasionally elongated or carrot-shaped) molded nuclei with hyperchromasia and some chromatin clumping (Fig. 8.15A). Molded, markedly atypical cells with high nucleocytoplasmic ratio in CSF cytospin are consistent with dissemination (Fig. 8.15B). Rosette-like arrangements representing Homer Wright rosettes may be seen (Fig. 8.16).
Fig. 8.15 
Intraoperative cytology preparation of a classic medulloblastoma, showing “small blue cells” with limited cytoplasm, moderate cellular pleomorphism, and nuclei with chromatin condensation and micronucleoli (A). Note the lack of a fibrillary background and an occasional apoptotic body. CSF from a patient with medulloblastoma (B) shows a cluster of disseminated malignant cells, cellular molding, irregular nuclear contour, and high nucleocytoplasmic ratio
Fig. 8.16 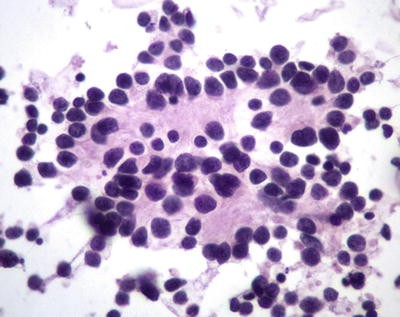
Cytology prepara tion showing Homer Wright rosettes
-
◦ Anaplastic medulloblastomas demonstrate a significant component of large, pleomorphic cells with prominent chromatin clumping and visible nucleoli. “Cell wrapping” or “cannibalism” (the nucleus of one cell wrapped around the nucleus of another) and apoptotic nuclei are frequent (Fig. 8.17). Occasional multinucleated cells may sometimes be seen.
Fig. 8.17 
Cytology prepa ration of an anaplastic medulloblastoma showing carrot-shaped cells, moderate cellular pleomorphism, “cell wrapping” (arrowhead), “cannibalism” (arrow), and hyperchromatic nuclei with chromatin condensation and micronucleoli
-
◦ Large cell medulloblastoma, when present or predominant, often shows a discohesive, monotonous population of large cells with open chromatin and visible nucleoli, sometimes mimicking the cytologic monotony of large cell lymphomas (Fig. 8.18).
Fig. 8.18 
Cytology preparation of a large cell medulloblastoma showing a monomorphic cytology, nucle i with open chromatin, and slightly prominent micronucleoli
-
◦ Endothelial proliferation and mitosis may be present in all cytologic types.
-
◦ Rare evidence of cytologic differentiation with astrocytic, ganglionic, or melanocytic differentiation (with melanin pigments), or rhabdomyoblastic differentiation (strap cells) may be seen.
-
-
Histology: Varied histol ogic features may be seen between and within tumors.
-
◦ Classic medulloblastomas are com posed of monotonous sheets of small cells (Fig. 8.19).
Fig. 8.19 
Classic medu lloblastoma with high cellularity and o verlapping nuclei, some of which are carrot-shaped. A few “dark” apoptotic bodies are present
-
Slight nuclear irregularity is often present.
-
Mitoses are present but often variable.
-
Necrosis may be present, with or without pseudopalisading.
-
Apoptosis is often present.
-
Endothelial proliferation is present and sometimes can be florid.
-
Neuroblastic differentiation is seen as the Homer Wright rosette (Fig. 8.20).
Fig. 8.20 
Classic medu lloblasto ma with Homer Wright rosettes
-
Mature neuronal differentiation as ganglion or “ganglioid” cells may be seen but must be distinguished from entrapped neurons.
-
A spindle or fascicular pattern, when present, is usually focal (Fig. 8.21)
Fig. 8.21 
Spindled an d fascicular pattern of growth in a classic medulloblastoma
-
Prominent nuclear irregularity with nucleoli and pleomorphism suggests the presence of anaplastic features, which may be focal; a transition from classic to anaplastic may be appreciable (Fig. 8.22). Extensive anaplasia may justify designation as an anaplastic subtype.
Fig. 8.22 
Transi tion fro m classic medulloblastoma (left bottom) to low-grade anaplastic features (right top)
-
Anaplasia may vary from slight to moderate to severe (Figs. 8.23 and 8.24).
Fig. 8.23 
Progre ssive transformation of internodular areas with increasing anaplasia is sometimes seen i n desmoplastic medulloblastoma. A residual pale nodule area is shown partially at the top of the image (arrow)
Fig. 8.24 
(A–C) A naplastic m edulloblastoma with severe anaplasia. Note variable patterns of marked cellular pleomorphism, florid apoptosis, karyorrhexis, and frequent cell wrapping and cannibalism
-
-
◦ Regions with monomorphic, discohesive, large round cells with prominent nucleoli are suggestive of the presence of a large cell component (Fig. 8.25).
Fig. 8.25 
Larg e cell medullobl astoma showing cellular monomorphism, vesicular nuclei, and distinct nucleoli. Note the similarity of this morphology to that of a diffuse large cell lymphoma
-
Predomin ance of large cells or severe anaplasia represents the large cell or anaplastic subtype and accounts for about 4 % of medulloblastoma.
-
Severe anaplasia is often associated with increased apoptosis, increased frequency of mitotic activity, and cell wrapping or cannibalism.
-
-
◦ Nodular (desmoplastic) medulloblastoma is characterized by the presence of multiple reticulin-fre e, pale nodules of neurocytic cells within a neuropil-like background, which are rarely mitotic with increased apoptosis (Figs. 8.26, 8.27, and 8.28).
Fig. 8.26 
Lo w-magn ification (A) and higher-magnification (B) views of a desmoplastic (nodular) medulloblastoma, showing the characteristic pale nodules
Fig. 8.27 
Desmo plastic (n odular) medulloblastoma showing pale nodules (left), which are composed of neurocytes in a more differentiated, fibrillary, neuropil-like background. Contrast with the less-differentiated neuroblastic internodular region (right)
Fig. 8.28 
Desm oplastic ( nodular) medulloblastoma showing reticulin-free pale nodules and reticulin-positive internodular areas
-
Leptomeningeal invasion with florid, reactive desmoplasia (collagenous fibrosis), often demonstrating medium- to large-sized leptomeningeal vessels, may occur but does not constitute a desmoplastic medulloblastoma (Fig. 8.29).
Fig. 8.29 
Fibros is following lep tomeningeal invasion in a medulloblastoma. This should not be equated with a desmoplastic (nodular) medulloblastoma
-
Internodular areas are reticulin-rich and are composed of cells similar to those of classic medulloblastoma.
-
◦ These areas tend to exhibit more brisk mitotic activity than is seen within the pale nodules.
-
-
Internodular areas may sometimes show varying degrees of anaplasia (see Fig. 8.23).
-
-
◦ The extensively nodular medulloblastoma (previously termed cerebellar neuroblastoma) is a variant showing florid nodularity and neurocytic differentiation with an absent or minimal undifferentiated internodular component.
-
Cells are often arranged in a streaming pattern within a fibrillary matrix (Figs. 8.30 and 8.31).
Fig. 8.30 
Extensively nod ular medulloblastoma composed of interlacing fascicles of differentiated neurocytes in a “fibrillary” neuropil-like matrix with limited internodular areas
Fig. 8.31 
Extensively nodular medulloblastoma with neurocytes arranged in rows reminiscent of an “Indian file” pattern
-
Ganglion cell differentiation (forming cerebellar ganglioneuroblastoma) also may be present (Fig. 8.32).
Fig. 8.32 
Neuronal/ganglion ic (arrow) differentiation in a medulloblastoma
-
-
◦ Biphasic medulloblastoma rep resents a tumor with mixed classic and nodular components, in which the nodular component is not surrounded by desmoplasia; that is, the internodular areas are reticulin-free. This distinction from the nodular/desmoplastic medulloblastoma is important.
-
◦ Infrequent patterns of differentiation include:
-
Astrocytic differentiation, which must be distinguished from entrapped reactive astrocytes (Figs. 8.33 and 8.34).
Fig. 8.33 
Astrocyt ic differentiation in a medulloblastoma demonstrated by reactivity with antibody for glial fibrillary acidic protein (GFAP) in a subpopulation of tumor cells
Fig. 8.34 
Nonneopl astic reactive astrocytes within a medull oblastoma showing immunoreactivity for GFAP
-
Skeletal muscle or rhabdomyoblastic differentiation may rarely be seen as strap cells with or without striations; this pattern constitutes the medulloblastoma with myogenic differentiation (synonym: medullomyoblastoma) (Fig. 8.35).
Fig. 8.35 
Medullomyoblastoma with florid skeletal muscle differentiation (arrow) (A), demon strable strap cells with cross-striations (B), and desmin immunoreactivity in tumor cells (C)
-
Melanocytic di fferentiation with melanin pigment production constitutes the rare medulloblastoma with melanotic differentiation (synonym: melanotic medulloblastoma) (Fig. 8.36).
Fig. 8.36 
Melanoti c differentiation in a medulloblastoma
-
Premelanosomes and melanosomes are demonstrable by electron microscopy.
-
-
-























5 Immunohistochemistry
-
Medulloblastomas show diffuse immunopositivity for synaptophysin (Fig. 8.37) and varia ble immunopositivity for chromogranin, neurofilament protein, and the neuronal marker NeuN.
Fig. 8.37 
Immunorea ctivity for synaptophysin is consistent with neuroblastic differentiation in this poorly differentiated embryonal tumor
-
Glial fibrillary acidic protein (GFAP) often highlights trapped reactive astrocytes. Rare positivity of tumor cells is seen (see Figs. 8.33 and 8.34).
-
Immunopositivity for retinal S-antigen and rhodopsin may be rarely seen in tumors with photoreceptor differentiation.
-
Epithelial membrane antigen (EMA) is usually negative.
-
p53 immunopositivity is seen in a subset of medulloblastomas. An increased proportion of positive cells often correlates with increasing anaplasia and poorer survival (Fig. 8.38).
Fig. 8.38 
A subpopulation of tum or cells exhibit immunoreactivity of p53 protein, consistent with dysregulation of p53 in this tumor and implication of a poor prognosis
-
The MIB-1 (proliferation) index is variable, often very high (30–80 %) (Fig. 8.39).
Fig. 8.39 
Ki-67 immunoreactivity showing a high proliferation index



6 Electron Microscopy
-
Electron microscopy shows tumor cells (often paucicellular) in organelles but with demonstrable neurose cretory granules.
-
Cellular processes are frequent and contain microtubules.
-
Synaptic-type junctions may be seen.
7 Molecular Pathology
-
Medulloblastomas are presumed to arise from precursor stem cells in the external granular layer for lateral hemispheric nodular or desmoplastic medulloblastomas, and from dysplastic precursor cells arrested during migration for other vermian variants.
-
Using gene expression profiling, medulloblastomas are molecularly classified into four groups:
-
◦ Group A with wnt pathway activation
-
◦ Group B with SHH pathway activation
-
◦ Groups C and D, collectively referred to as non A/non B. Non A/non B classification is often associated with aggressive histology, MYC amplification, and poor prognosis.
-
-
Activation of the wnt signaling pathway through mutation of the APC gene has been associated with Turcot syndrome and only 3–4 % of sporadic medulloblastoma.
-
Wnt pathway–activated tumors account for about 10 % of medulloblastomas and show demonstrable nuclear localization for beta catenin and/or monosomy 6. DDX3X gene mutation is also seen in 50 % of wnt pathway tumors.
-
PTCH gene loss of function mutation, as well as mutations of SMO, SUFU, and Gli2 result in the activation of the sonic hedgehog (SHH) signaling pathway in 30 % of medulloblastomas.
-
SHH pathway activation is seen classically in nodular or desmoplastic medulloblastoma. Gli1 and Gli2, representing downstream effectors of SHH pathway activation, are also often demonstrable in up to 85 % of medulloblastomas. The proportion of tumors classified as SHH molecular subgroup drops significantly when classified based on the expression of GAB1, filamin A, and/or YAP1. SHH-activated tumors with p53 mutation carry a significantly poor prognosis.
-
Amplification of MYCC and less commonly MYCN is a common finding in large cell/anaplastic medulloblastoma (Figs. 8.40 and 8.41); MYCC amplification is frequently associated with Group C, and MYCN amplification, with group D.
Fig. 8.40 
Fluorescence in situ h ybridization (FISH) using an MYCN–specific probe demonstrates gene amplification (green) in an anaplastic medulloblastoma. The chromosome 2 centromeric reference probe is red
Fig. 8.41 
FISH using a c-myc–sp ecific probe demonstrates gene amplification (red) in an anaplastic medulloblastoma. The chromosome 8 centromeric reference probe is green
-
Gains of CDK6 (7q21), hTERT (5p15), OTX2 (14q22) (more frequently seen in group C), and FoxG1 (14q12) have been reported.
-
17p deletion with isochromosome 17q is the commonest cytogenetic abnormality in medulloblastoma, present in 30–40 % of tumors (Fig. 8.42); it is seen particularly in group D tumors. Potential target genes in the 17p deletion include HIC1 (17p13.3), frequently hypermethylated in medulloblastoma, and REN (17p13.2), a negative regulator of the SHH signaling pathway.
Fig. 8.42 
(A) Conventional comp arative genomic hybridization (CGH) analysis demonstrating loss of 17p and gain of 17q. (B) FISH analysis showing one copy of 17p (red probe signal) and three copies of 17q (green probe signal), consistent with cytogenetic findings of isochromosome 17q
-
Losses of 16q, 10q, and 11q are present in a subset of the tumors.
-
Increased activation of the Notch signal ing pathway; overexpression of PAX5, PAX6 and SOX4; and overexpression of repressors of neural differentiation REST and FoxG1 have all been reported in medulloblastoma.



8 Differential Diagnosis
-
Medulloblastomas may have areas with prominent perivascular pseudorosettes, thus raising anaplastic ependymoma as a major differential diagnosis.
-
◦ Ependymomas tend to show variation in cellularity, however, including regions of well-differentiated ependymoma.
-
◦ EMA is often positive in ependymomas and negative in medulloblastoma.
-
◦ Synaptophysin is positive in perivascular pseudorosettes of medulloblastoma, whereas GFAP staining is more characteristic of ependymoma.
-
◦ Nuclear positivity for NeuN is not helpful, as it may be positive in both tumor types.
-
-
Atypical teratoid /rhabdoid tumor (AT/RT) may have a prominent PNET-like small round cell component, whereas large cell or anaplastic medulloblastoma may mimic AT/RT.
-
◦ FISH with INI-1 locus-specific probe shows no demonstrable allelic deletion in medulloblastoma.
-
◦ Similarly, immunostain with BAF-47 (anti-INI1) antibody shows positive nuclear staining in the neoplastic cells in medulloblastoma but negative staining in AT/RT.
-
-
Medulloblastoma needs to also be differentiated from small cell glioblastoma.
-
◦ Small cell glioblastoma will characteristically show widespread GFAP positivity and lack evidence of neural differentiation (presence of Homer Wright rosettes or neuronal immunohistochemical markers typical of medulloblastoma).
-
-
Other small round blue cell tumors of children metastatic to the CNS (rhabdomyosarcoma, Ewing sarcoma, leukemia/lymphoma, etc.) can all be effectively differentiated from medulloblastoma by immunohistochemistry.
-
◦ Metastatic neuroblastoma may closely mimic medulloblastoma, but it would be unlikely for neuroblastoma to present solely as a CNS metastasis without the primary peripheral lesion having been identified by imaging studies or a previous biopsy.
-
9 Prognosis
-
The following clinic al characteristics define high-risk patients:
-
◦ Age less than 3 years.
-
◦ Postresection residual tumor larger than 1.5 cm.
-
◦ Metastatic disease at presentation with Chang stages M1–4.
-
-
Large cell and anaplastic histology are associated with poor survival.
-
Poor prognostic molecular markers include amplification of MYCC or MYCN and overexpression of c-erbB2 or p53.
-
The nodular/desmoplastic and the extensively nodular phenotypes are associated with favorable outcome and better survival than the classic medulloblastoma.
-
Wnt pathway activation with nuclear expression of β-catenin and/or monosomy 6 has been reported as a good prognostic marker.
Suggested Reading
Adesina AM, Veo BL, Courteau G, Mehta V, Wu X, Pang K, et al. FOXG1 expression shows correlation with neuronal differentiation in cerebellar development, aggressive phenotype in medulloblastomas, and survival in a xenograft model of medulloblastoma. Hum Pathol. 2015;46:1859–71.
Bailey P, Cushing H. Medulloblastoma cerebelli: a common type of mid-cerebellar glioma of childhood. Arch Neurol Psychiatry. 1925;14:192–224.
Ellison DW, Dalton J, Kocak M, Nicholson SL, Fraga C, Neale G, et al. Medulloblastoma: clinicopathological correlates of SHH, WNT, and non-SHH/WNT molecular subgroups. Acta Neuropathol. 2011;121:381–96.
Giangaspero F, Rigobello L, Badiali M, Loda M, Andreini L, Basso G, et al. Large cell medulloblastoma. A distinct variant with highly aggressive behavior. Am J Surg Pathol. 1992;16:687–93.
Giangaspero F, Perilongo G, Fondelli MP, Brisigotti M, Carollo C, Burnelli R, et al. Medulloblastoma with extensive nodularity: a variant with favorable prognosis. J Neurosurg. 1999;91:971–7.
Giangaspero F, Wellek S, Masuoka J, Gessi M, Kleihues P, Oghaki H. Stratification on the basis of histopathologic grading. Acta Neuropathol. 2006;112:5–12.
Helton KJ, Fouladi M, Boop FA, Perry A, Dalton J, Kun L, Fuller C. Medullomyoblastoma: a radiographic and clinicopathologic analysis of six cases and review of the literature. Cancer. 2004;101:1445–54.
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131:803–20.
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. WHO classification of tumours of the central nervous system. Lyon: International Agency for Research on Cancer (IARC); 2016.
Meyers SP, Kemp SS, Tarr RW. MR imaging features of medulloblastomas. AJR Am J Roentgenol. 1992;158:859–65.
Northcott PA, Korshunov A, Witt H, Hielscher T, Eberhart CG, Mack S, et al. Medulloblastoma comprises four distinct molecular variants. J Clin Oncol. 2011;29:1408–14.
Panigrahy A, Krieger MD, Gonzalez-Gomez I, Liu X, McComb JG, Finlay JL, et al. Quantitative short echo time 1H-MR spectroscopy of untreated pediatric brain tumors: preoperative diagnosis and characterization. AJNR Am J Neuroradiol. 2006;27:560–72.
Taylor MD, Northcott PA, Korshunov A, Remke M, Cho YJ, Clifford SC, et al. Molecular subgroups of medulloblastoma: the current consensus. Acta Neuropathol. 2012;123:465–72.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing AG
About this chapter
Cite this chapter
Adesina, A.M., Hunter, J.V. (2016). Medulloblastoma. In: Adesina, A., Tihan, T., Fuller, C., Poussaint, T. (eds) Atlas of Pediatric Brain Tumors. Springer, Cham. https://doi.org/10.1007/978-3-319-33432-5_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-33432-5_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33430-1
Online ISBN: 978-3-319-33432-5
eBook Packages: MedicineMedicine (R0)