
Abstract
Success of cancer chemotherapy is limited by simultaneous resistance towards many anticancer drugs making clinical combination therapy protocols less efficient. P-glycoprotein represents an efflux pump of the ABC transporter family, which recognizes and extrudes anticancer drugs of diverse chemical classes and biochemical functions. The P-glycoprotein-mediated profile of cross-resistance has been termed multidrug resistance (MDR). In our investigations, we focused on MDR of in vivo tumor lines maintained in mice. The development of in vivo resistance towards anthracyclines (doxorubicin, daunorubicin) in L1210 and S180 ascites tumor lines was accompanied with decreased uptake and increased efflux of the fluorescent dye rhodamine 123, overexpression of P-glycoprotein as well as MDR1 mRNA overexpression and MDR1 gene amplification. In addition to acquired multidrug resistance in these syngeneic mouse tumor lines, we investigated inherent drug resistance in human lung xenograft tumors transplanted to nude mice. Drug resistance in these xenografts was also associated with overexpression of P-glycoprotein and MDR1 mRNA, but without MDR1 gene amplification. Furthermore, we explored P-glycoprotein expression in clinical biopsies of diverse tumor entities (leukemia, lung cancer, breast cancer, cervical carcinoma, endometrial carcinoma. nephroblastoma, renal cell carcinoma) and found that high levels of P-glycoprotein expression correlated with pretreatment with chemotherapy, drug resistance, and failure to achieve complete remission. During the past years, a wealth of publications worldwide confirmed a role of the P-glycoprotein for clinical treatment refractoriness and as an unfavorable prognostic factor for survival time of patients.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- ABC transporter
- Anthracyclines
- Cancer
- Chemotherapy
- Drug resistance
- Prognostic factor
- Rhodamine 123
- Survival time
- Xenograft tumor
1.1 Introduction
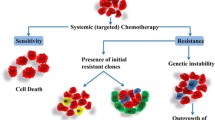
The development of resistance to anticancer drugs has dogged clinical oncology since the very early days of chemotherapy. Since the establishment of nitrogen mustard-derived compounds and methotrexate in the 1940s and 1950s, it became clear that tumors have efficient escape mechanisms preventing the cure of many cancer patients [1, 2]. A surprising observation was that over the decades until today it was not possible to develop drugs without appearance of resistance phenomena in tumors. The development of combination therapy improved the situation compared to monotherapy, but sustainable treatment success leading to reliable cure of patients could also not be reached [3–5]. A main problem is that the side effects of most cytotoxic and cytostatic drugs to proliferating normal tissues (e.g. bone marrow, gastrointestinal mucosa, hair roots, reproductive organs) are significantly such that sufficient doses of drugs cannot be applied to kill tumor cells Suboptimal drug concentrations facilitate the survival of inherently more resistant cells in a heterogeneous tumor population. Depending of the type of tumor, the clinical situation is that a fraction, but not all patients, benefits from chemotherapy leading to improved survival times. It was unexpected at that time that combination regimens were also subject to resistance development, since drugs with different cellular and molecular modes of action were used. The clinical phenomenon of unresponsiveness to multiple drugs was reproducible under cell culture conditions in the laboratory. It was David Kessel who described in 1968 that cell lines display cross-resistance to different drugs [6]. This observation was also reported in hundreds of publications in subsequent years and laid the bases for a new area of research in cancer biology. Strikingly, tumors that are initially responsive to chemotherapy can develop resistance during treatment. Resistant tumor cells can acquire cross-resistance to a wide range of compounds that have no obvious structural or functional similarities, e.g. alkaloids (colchicine, vinblastine, vincristine), anthracyclines (doxorubicin, daunorubicin), taxanes (paclitaxel, docetaxel), epipodophyllotoxins (etoposide, teniposide), and antibiotics (actinomycin D, mitomycin C) [7, 8]. This phenomenon has been designated as pleiotropic or multidrug resistance (MDR).
MDR of cancer cells is associated with decreased net cellular drug concentrations and has been attributed to alterations in the plasma membrane [9–11]. A drug efflux pump termed P-glycoprotein (P for permeability) has been unraveled as an underlying mechanism [10, 12]. The MDR1/ABCB1 gene encoding the P-glycoprotein has been cloned in 1986 and was found to be amplified in many multidrug-resistant cell lines in vitro [13]. P-glycoprotein was the first member of the ATP-binding cassette (ABC) transporter family identified in cancer. Its discovery has enormously stimulated cancer research in subsequent years and numerous in vitro cell lines were characterized to overexpress P-glycoprotein and MDR1 mRNA as well to carry amplified copy numbers of the MDR1 genes in their genomes [14].
1.2 Architecture and Function of the P-Glycoprotein
This efflux transporter belongs to a gene family of ATP-binding cassette (ABC) transporters. The human genome consists of 48 members of this gene family. About one dozen ABC transporters have been suggested to transport anticancer drugs, although the P-glycoprotein is the best understood. The P-glycoprotein consists of 1,258 amino acids which are organized as two duplicated halves. It spans the cell membrane with 123 transmembrane segments and two intracellular ATP-binding domains. The extracellular glycosylation of P-glycoprotein is not of functional relevance.
Several hypotheses have been discussed on the biochemical mode of action (Fig. 1.1):

Models on the function of P-glycoprotein
The partitioning model: It has been speculated that the P-glycoprotein does not transport drugs by itself but affects drug distribution indirectly by altering the pH value or membrane potential [15]. This model was supported by the fact that some anticancer drugs are positively charged and that the pH in multidrug-resistant cells differs from sensitive cells. It is now generally accepted that the P-glycoprotein is primarily not an ion channel [16].
The hydrophobic vacuum cleaner hypothesis: Many P-glycoprotein substrates are hydrophobic and are better soluble in the lipid bilayer of the cell membrane than in the extracellular aqueous phase. Anticancer drugs are thought first to interact with the cell membrane and then bind to a binding site of the P-glycoprotein leading the drug to the internal channel of P-glycoprotein and effluxes out of the cell [17, 18]. This model may not only explain the increased efflux of multidrug-resistant cells, but also the frequently observed decreased drug influx [19, 20]. Hydrophilic drugs do not enter the P-glycoprotein from the lipid bilayer but first they passively diffuse into the cytosol and then reach the P-glycoprotein from the intracellular side.
The translocase or flippase model postulates that according to the higher intracellular drug concentration gradient, drug molecules bind to the intracellular binding domains of the P-glycoprotein, which changes conformation by an energy-driven process (i.e. ATP cleavage) and flips drugs to the extracellular space [17].
1.3 Acquired Drug Resistance in Tumor Lines In Vivo
Instead of studying multidrug resistance in vitro, our own research efforts were directed to investigate drug resistance in animals to get closer to the clinical situation. One reason for that decision was that drug-resistant cell lines have been described to exhibit 1,000- to 10,000-fold resistance to drugs such as methotrexate [21–23]. These high degrees of resistance do usually not occur in the clinical situation and might be laboratory artifacts.
We established doxorubicin-resistant L1210 leukemia cells, which express the MDR phenotype. The tumor cell line was generated in vivo in mice—an approach which might be more analogous to the clinical development of drug resistance. Mice bearing L1210 ascites cells were treated with doxorubicin i.p. weekly. Doxorubicin was applied at a concentration of 2 mg/kg body weight. The pretreatment was carried out for at least 20 passages. The test for resistance was carried out by injecting groups of animals with either untreated (sensitive) or drug-pretreated (resistant) tumor cells. Then, doxorubicin was injected i.p. on the fourth and fifth days after tumor cell transplantation. The effects of doxorubicin (different concentrations) on the tumor cells were measured 2 days after the last injection. Under these conditions, tumor-bearing animals were killed, the ascites cells were removed by puncture and counted using a coulter counter. L1210 ascites tumor cells preconditioned with doxorubicin were more resistant in vivo to this drug than the parental cells (Fig. 1.2, left side).

Detection of resistance of doxorubicin-preconditioned L1210 ascites tumor cells in vivo and In vitro. Abscissa: different dose levels of doxorubicin. Closed symbols indicate parental (sensitive) ascites tumor cells and open symbols drug-pretreated (resistant) ones. Data were taken from Volm et al. [25]
An in-vitro short-term test was also used to detect the resistance of the pretreated tumor cells and to define the degree of resistance. The basic feature of this test is the measurement of inhibition of incorporation of radioactive nucleic acid precursors into tumor cells after the addition of cytostatic agents [24]. The tumor cells were incubated in vitro with doxorubicin for 3 h. The radioactive precursor was added during the third hour of incubation. Aliquots of the cell suspensions were pipetted onto filter discs, the acid-soluble radioactivity extracted, and the incorporated activity measured by scintillation counting. As shown in Fig. 1.2 (right side), the resistance of the pretreated cells found in vivo could be confirmed in vitro. The maximum degree of resistance was 45-fold for the cells preconditioned with doxorubicin. Cross-resistance of these cell lines was found to doxorubicin and daunorubicin, but not to cytosine-arabinoside and cyclophosphamide [25].
Cross-resistance of anthracyclines to the cytotoxic fluorescent dye rhodamine 123 has been described [26]. Therefore, we determined rhodamine 123 accumulation in the resistant and sensitive L1210 ascites cells by fluorescence microscopy. We found that resistant cells needed more time to accumulate rhodamine 123 than their sensitive parental cells. Sensitive cells showed a significant rhodamine 123 fluorescence, whereas daunorubicin-resistant cells did not (Fig. 1.3).

Accumulation of rhodamine 123 in sensitive and daunorubicin-resistant L1210 ascites tumor cells as measured by flow cytometry. Biparametrical histograms of cells stained with (a) rhodamine 123 (4 mg/ml, 60 min incubation) and (b) propidium iodide (35 μg/ml). At least 20,000 cells were measured per histogram. Propidium iodide was used to exclude dead cells. Time and concentration kinetics of rhodamine 123 (2, 4, and 8 μg/ml) in sensitive (c) and resistant L1210 cells (d). (e) Determination of rhodamine 123 efflux (1 h preincubation with 8 μg/ml) in sensitive (closed symbols) and resistant L1210 cells (open symbols). Data were taken from Efferth [27] and Efferth et al. [28]
For the quantification of rhodamine 123 fluorescence, we used an ORTHO 30L cytofluorescence analyzer equipped with two argon ion lasers and an INTERTECHNIQUE Plurimed spectrum analysis computer system. Figure 1.3 shows representative biparametrical fluorescence histograms of intracellular rhodamine 123 fluorescence intensity in resistant and sensitive L1210 ascites tumor cells. These flow cytometric data confirmed the microscopic observation that resistant cells accumulated less rhodamine 123.
The rhodamine 123 accumulation was measured in a time- and concentration-dependent manner. Drug-sensitive parental L12010 cells accumulated high amounts of rhodamine 123 depending on the concentration and the incubation time (Fig. 1.3c), whereas rhodamine 123 was taken up at much lower amounts in the resistant L1210 cells (Fig. 1.3d). These accumulation kinetics showed the intracellular accumulation, which was the net sum of both the uptake and the efflux. Therefore, the question remains about the relevance of drug efflux, since P-glycoprotein functions as an efflux transporter. Sensitive and resistant L1210 cells were loaded with rhodamine 123, centrifuged and transferred into rhodamine 123-free medium. As shown in Fig. 1.3e, sensitive cells retained rhodamine 123, whereas resistant cells showed a considerable efflux of this fluorescent dye. To further analyze whether rhodamine 123 is pumped out in an energy-dependent process (presumably by the P-glycoprotein), resistant cells were incubated with and without 2-deoxy-glucose. Cells use glucose for energy metabolism to generate ATP and 2-deoxy-glucose is an efficient inhibitor of ATP production. Hence, 2-deoxy-glucose is expected to inhibit the ATP-dependent efflux of P-glycoprotein. Resistant cells loaded with 2-deoxy-glucose were incubated with rhodamine 123 and then transferred into rhodamine 123-free Hanks’s balanced salt solution. 2-Deoxy-glucose-treated resistant cells did not show a considerable efflux of rhodamine 123, whereas untreated resistant cells did [27, 28]. We conclude that the ATP-dependent efflux of rhodamine 123 was blocked by 2-deoxy-glucose and that ATP is necessary for the energy-dependent efflux function of the P-glycoprotein.
1.4 Development of Resistance by Repeated Drug Treatments
To monitor the development of drug resistance during consecutively repeated doxorubicin treatments, mice bearing L1210 tumors were once weekly treated with 0.5 mg doxorubicin/kg body weight i.p. The development of doxorubicin resistance was analyzed during eight treatments in vivo by using the in vitro short term test. Sensitive (S) and established resistant L1210 ascites tumor cells (R) with a resistance factor of 45 were used as negative and positive controls respectively (Fig. 1.4). Resistance increased with the number of treatments and the level of resistance achieved after eight treatments is similar to that of the established tumor line (Fig. 1.4). This suggests that a maximum level of resistance was already reached after only eight treatments. In order to prove this result, we increased the dosage of doxorubicin in the established tumor line from 2 to 8 mg /kg body weight for ten treatments and indeed did not observe a further increase of the level of resistance.

Development of resistance to doxorubicin in L1210 ascites tumor cells in vivo. Dose–response curves of doxorubicin after treatments (2–8×) with 0.5 mg/kg doxorubicin. S, sensitive (parental) tumor line; R, doxorubicin-resistant line after more than 20 treatments with 2 mg/kg body weight doxorubicin. Each point represents mean of four measurements. Data were taken from Volm et al. [32]
In order to find out whether the P-glycoprotein increases according to both the number of treatments and the increase of doxorubicin resistance, we investigated MDR1 gene amplification and mRNA expression as well as P-glycoprotein expression. After four treatments many tumor cells expressed P-glycoprotein and after eight treatments nearly all tumor cells showed increased expression of the P-glycoprotein as shown by immunohistochemistry (Fig. 1.5). Southern-blot analysis during eight treatments with doxorubicin showed that the development of resistance was associated with MDR1 gene amplification and correlated with the degree of drug resistance. A comparison of the intensity of the bands in the established line (L1210/Dox) with that in the tumors with eight treatments indicated similar degrees of amplification. Slot-blots probing MDR1 mRNA expression confirmed these results (Fig. 1.5). The gene amplification did not increase by further treatments with a higher concentration of doxorubicin.

Development of doxorubicin resistance, MDR1 gene amplification, MDR1 and P-glycoprotein overexpression in L1210 tumor cells after treatment (2–8×) with 0.5 mg/kg doxorubicin in vivo. S, sensitive (parental) tumor line; R, doxorubicin-resistant cell line after more than 20 treatments with 2 mg/kg body weight doxorubicin. Figure was taken from Volm [33]
1.5 Reversal of Resistance After Cessation of Chemotherapy
The question arises as to whether or not the resistance that developed over 20 passages would persist after cessation of doxorubicin treatment. Remarkably, resistance decreased over time and disappeared after 20 passages without treatment (Fig. 1.6). This decrease in resistance was accompanied by a loss of P-glycoprotein as well as by a loss of MDR1 mRNA expression and gene amplification (Fig. 1.7; [32]). These results in mouse tumors fit to the clinical situation. It has been observed clinically that the longer the duration of the disease free intervals following chemotherapy, the more likely is the response of the tumors to the same chemotherapy.

Dose response curves of doxorubicin after cessation of doxorubicin treatment (5–25 passages). S, sensitive (parental) tumor line; R, doxorubicin-resistant tumor line. Each point represents mean of four measurements. Data were taken from Volm et al. [32]

Reversion of doxorubicin resistance, P-glycoprotein and MDR1 overexpression and MDR1 gene amplification in L1210 tumor cells after cessation of treatment for 20 passages in vivo. Each point represents mean of four measurements. Data were taken from Volm [33]
Corresponding to the development of resistant L1210 leukemia ascites cell lines, we developed doxorubicin- or daunorubicin-resistant sarcoma S180 ascites cell lines. These resistant S180 cell lines also displayed cross-resistance to various other drugs [29, 30]. As shown in Fig. 1.8, these two resistant S180 ascites tumor lines also displayed decreased uptake of rhodamine 123 (as shown by flow cytometry), amplification of the MDR1 gene (as shown by Southern blot), as well as overexpression of MDR1 mRNA (as shown by Northern blot) and protein overexpression (as shown by Western blot, immunofluorescence and immunohistochemistry). Hence, multidrug resistance in these S180 tumor lines can also be explained by the P-glycoprotein in a comparable fashion as observed in the multidrug-resistant L1210 tumor lines.

Different methods for detecting multidrug resistance. Shown are results in sensitive parental cells (S) and multidrug-resistant cell lines (R1, R2). Resistance was developed in response to doxorubicin (R1) and daunorubicin (R2). (a) In vitro short-term test to determine the degree of resistance. (b) Flow cytometry to measure accumulation of rhodamine 123. (c) Southern blotting to detect gene amplification of the MDR1 gene. The hybridization was performed with the pcDR 1.5 cDNA probe. (d) Northern blotting to detect mRNA overexpression of the MDR1 gene (Hybridization with pcDR 1.5). (e) Western blotting to detect overexpression of P-glycoprotein (with mAb C219). (f) Immunofluorescence and (g) immunohistochemistry to detect overexpression of P-glycoprotein (with mAb C219). Taken from Volm et al. [31]
1.6 Inherent Drug Resistance in Human Lung Tumor Xenografts In Vivo
Transplantable murine tumors have the advantage that they can be maintained in mice with an intact immune system. Chemotherapy depresses the immune functions of the body—a process that takes place both in mice and men. In this respect, syngeneic mouse tumors reflect the situation in human cancer patients. Another animal model utilizes human xenograft tumors. These tumors grow in nude mice with a deficient immune system and do, therefore, not reject human cells. The advantage of this animal model is that the human tumors can be investigated in living mouse models without performing experiments in patients. Hence, this is an attractive model to analyze the chemotherapy effects in human tumors.
In addition to the development of resistance during repeated treatments with anticancer drugs (termed acquired or secondary drug resistance), resistance can also occur in untreated tumors. This form of resistance is characterized by unresponsiveness to anticancer drugs even if the tumors had never been challenged with chemotherapy. This form is termed inherent or primary resistance. Clinically, both forms lead to the failure of chemotherapy and the question arises, whether the P-glycoprotein/MDR1 is also of relevance for the inherent drug resistance. Lung cancer is frequently characterized by inherent drug resistance, which is one reason for the observed survival times of lung cancer patients.
We investigated the intrinsic resistance of a panel of eight human epidermoid lung cancer xenografts to vincristine and daunorubicin and tested the cross-resistance pattern to a variety of other agents. Our results demonstrated that xenograft lines derived from human lung tumors, not previously treated with chemotherapy exhibited a comparable pattern of cross-resistance as observed in the multidrug-resistant L1210 or S180 cell lines [34, 35]. By means of fluorescence microscopy, we found that drug-resistant epidermoid lung carcinoma xenograft tumors showed an intensive immunostaining for P-glycoprotein, whereas no immunoreactivity could be seen in drug-sensitive xenografts (Fig. 1.9). Northern and Southern blot analyses revealed that the MDR1 mRNA expression was increased according to P-glycoprotein expression and the degree of drug resistance, whereas MDR1 gene amplification was not detectable (Fig. 1.9).

Effect of a single dose of 2 mg/kg vincristine on tumor size (top), MDR1 gene amplification and mRNA expression (middle) and P-glycoprotein expression (bottom) of eight different epidermoid lung cancer xenografts. MDR1 hybridization was performed with the genomic pcDr 1.5 DNA probe. P-glycoprotein was detected by immunofluorescence and mAb 265/F4. Data are taken from [33, 35]
1.7 P-Glycoprotein in Clinical Tumor Biopsies
After studying transplantable tumors with either acquired or inherent drug resistance in animals, we were interested to explore the relevance of P-glycoprotein in human tumors. Patients with previously untreated non-small cell lung carcinomas (NSCLC) were surgically treated and specimens of the tumors for resistance testing (in vitro-short-term test) and detection of P-glycoprotein (immunohistochemistry) were used.
Of the 91 lung tumors, 43 were P-glycoprotein positive and 48 were negative. There was a significant correlation between the resistance and P-glycoprotein expression (Fig. 1.10) Of the 64 resistant tumors 39 were P-glycoprotein positive (61 %), whereas of the 27 sensitive tumors only four were P-glycoprotein positive (15 %) [38]. Furthermore, a significant correlation between the oncoproteins c-Fos and c-Jun and the P-glycoprotein was found [36, 37]. Both proteins form a protein complex, which functions as transcription factor (AP-1). These results and the fact that the MDR1 gene promoter carries AP-1 binding motifs may be taken as a clue that the P-glycoprotein may be regulated by the transcription factor AP-1.

Relationship between the response to doxorubicin as determined by the in vitro short-term test (ordinate) and immunohistochemical detection of P-glycoprotein (abscissa) in human lung cancer biopsies [38]
Investigations by us and others on liver carcinogenesis revealed a connection between P-glycoprotein expression and resistance to liver-carcinogenic compounds [39–41]. As smoking is widely accepted to cause lung cancer, we hypothesized an association between smoking habits, resistance to doxorubicin, and expression of P-glycoprotein. Biopsies of 94 non-small cell lung cancers were analyzed for their doxorubicin resistance using an in vitro short-term assay as well as their P-glycoprotein expression by immunohistochemistry. These results have been correlated to the smoking habits of the patients [42]. As shown in Fig. 1.11, lung tumors from smokers were more frequently resistant to doxorubicin and expressed higher levels of P-glycoprotein than lung tumors from nonsmokers (p = 0.007 and p = 0.0001, respectively). These data may be taken as a hint that smoking contributes not only to lung carcinogenesis but also to drug resistance of lung tumors. This is an interesting result, since non-small cell lung cancer is a tumor entity well known for its unresponsiveness to chemotherapy and short survival times of patients.

Relationship between smoking habits of patients and response to doxorubicin as determined by the in vitro short-term test and immunohistochemical detection of P-glycoprotein in 94 human non-small cell lung cancer biopsies [42]
Another question raised was whether chemotherapy of tumors may induce P-glycoprotein expression. Accordingly, we analyzed a total number of 162 tumor biopsies by means of immunohistochemistry [43–54]. The tumors were divided into three groups according to their treatment. The first group consisted of untreated tumors and the second group of tumors was treated with anticancer drugs not inducing MDR. The third group consisted of tumors, which were pretreated with drugs known to cause MDR (e.g. doxorubicin, vincristine). Biopsies from leukemia, breast cancer, ovarian carcinoma, or nephroblastoma which have not been pretreated displayed P-glycoprotein expression in a few cases (3 of 49 = 6 %). Among the tumors treated with non-MDR-drugs only one out of nine was P-glycoprotein positive (=11 %). By contrast, biopsies from 44 tumors treated with MDR-inducing drugs exhibited P-glycoprotein in 22 cases (=50 %) (Table 1.1). This pattern of P-glycoprotein expression speaks for the expression of P-glycoprotein during chemotherapy and indicates that P-glycoprotein is one responsible factor for the development of acquired (secondary) drug resistance (Table 1.1). Another group of tumors (renal, cervical, and endometrial carcinoma) showed a completely different profile. These tumors showed P-glycoprotein expression in a high number of biopsies, although these tumors have not been pretreated (43 out of 55 tumors = 78 %). A few tumors were nevertheless treated with MDR-relevant drugs and they were all P-glycoprotein positive (5/5 = 100 %). These three tumor types are known to be relatively unresponsive towards chemotherapy. This indicates that P-glycoprotein expression in these tumor types is tightly correlated with inherent (primary) resistance towards anticancer drugs. Exemplary immunostainings of P-glycoprotein in human tumors are depicted in Fig. 1.12.

Immunohistochemical detection of P-glycoprotein in human tumors by mAb C219. (a) Renal cell carcinoma, (b) endometrial carcinoma, (c) multiple myeloma, (d) ovarian carcinoma, (e) breast carcinoma, and (f) control tumor (daunorubicin-resistant solid carcinoma 180 of the mouse). Taken from Volm et al. [31]
The results of our own investigations were compared with data from the literature. In a previous meta-analysis, a total number of 6.248 tumors were investigated for their P-glycoprotein and MDR1 mRNA expression as well as MDR1 gene amplification [55]. While MDR1 gene amplification is a very rare event in clinical tumor samples, overexpression of MDR1 mRNA frequently occurred even in untreated tumors (Fig. 1.13). Comparable results were found for the expression of P-glycoprotein in untreated tumors (Fig. 1.14). These results in a large number of clinical tumors indicate that MDR1 gene expression does not account for multidrug resistance in the clinic. Nevertheless, overexpression of MDR1 mRNA and P-glycoprotein represent a frequent event. Their occurrence even in untreated tumors point to the relevance of P-glycoprotein/MDR1 for inherent or primary drug resistance.

Expression of MDR1 mRNA in untreated human tumors as determined by Northern blotting, slot blotting, in situ hybridization, RNAse protection assay or RT-PCR. Taken from Efferth and Osieka [55]

Expression of P-glycoprotein in untreated human tumors. P-glycoprotein was detected either by Western blotting, immunohistochemistry, immunofluorescence, or flow cytometry. Taken from Efferth and Osieka [55]
The next question raised was whether the increase of P-glycoprotein/MDR1 in animal tumors in vivo after treatment with anticancer drugs could also be observed in a clinical setting. Therefore, it was evaluated whether the expression of P-glycoprotein/MDR1 in human tumors was higher after chemotherapy as compared to untreated tumors before chemotherapy. As shown in Fig. 1.15, the mRNA and protein expression levels considerably increased after chemotherapy. This indicates that P-glycoprotein/MDR1 also plays a role for acquired or secondary drug resistance.

Increase of P-glycoprotein/MDR1 expression in treated as compared to untreated tumors. Taken from Efferth and Osieka [55]
1.8 Prognostic Relevance of P-Glycoprotein for Treatment Outcome
To address the question whether P-glycoprotein expression is of prognostic relevance for the survival of patients, a total number of 104 pediatric patients with untreated non-B-type acute lymphoblastic leukemia are analyzed using immunohistochemistry for the expression of P-glycoprotein in relationship to their therapy outcome. As response criteria, we used the relapse rate and the relapse-free interval. P-glycoprotein expression was detected in 36 out of 104 leukemia (35 %). We found a significant lower probability of remaining in first continuous complete remission (CCR) (p = 0.05) and a tendency for an increased relapse rate in patients with P-glycoprotein-positive blast cells (Fig. 1.16; [56]).

Curves of relapse-free intervals in children with P-glycoprotein-positive versus -negative acute lymphoblastic leukemia (ALL) obtained by Kaplan-Meier statistics. Insert: P-glycoprotein immunostaining in ALL. Data taken from Sauerbrey et al. [56]
Since the pioneering work on the role of P-glycoprotein for multidrug resistance by us and others in the 1980s and 1990s, several hundred clinical papers appeared on the prognostic role of P-glycoprotein. It seems that the scientific fruits of the early years of P-glycoprotein fell on a fertile ground leading to flowering clinical research. It is beyond the scope of the present article to give a comprehensive overview of the prognostic role of P-glycoprotein vis-a-vis survival time of patients with all different tumor types. Nevertheless, we have focused on few tumor entities to highlight the clinical value of P-glycoprotein. For that purpose, we have chosen acute myeloic leukemia and acute lymphoblastic leukemia as hematopoietic tumors and breast cancer as example of a solid tumor.
As can be seen in Table 1.2, most but not all clinical investigations on P-glycoprotein expression in acute myeloid or acute lymphoblastic leukemia are significantly correlated with shorter survival times of patients. The prognostic significance of P-glycoprotein has also been reported in detail by Marie and Legrand [73]. While most studies used immunohistochemistry or flow cytometry, MDR1 mRNA or P-glycoprotein efflux function have been addressed in only a few studies. These investigations confirm the prognostic value of P-glycoprotein found in protein expression analyses.
Most investigations on P-glycoprotein expression in breast cancer were also performed using immunohistochemistry. Similar to acute leukemia, P-glycoprotein expression in breast cancer was significantly associated with shorter progression-free survival and overall survival of patients in most clinical studies (Table 1.2).
1.9 Conclusion and Perspectives
Analysis of the drug resistance phenomenon revealed that P-glycoprotein is not only important to explain multidrug resistance of tumors in laboratory animals, but also in cancer patients. Hence, this efflux transporter represents a determinant leading to the failure of chemotherapy and ultimately to the death of many patients.
A consequence drawn from these research efforts during the past three decades may be the development of diagnostic tools to detect P-glycoprotein in tumors before chemotherapy to predict treatment success or failure. Indeed, there have been considerable efforts to develop methods making P-glycoprotein detection possible for routine diagnostics in clinical laboratories [78, 79]. It turned out that the standardization of P-glycoprotein detection assays for routine diagnostics seems not to be trivial, but nevertheless is a reachable task. For leukemia, flow cytometric assays based on double labeling with a fluorescent-labeled anti-P-glycoprotein antibody and a fluorescent P-glycoprotein substrate such as rhodamine 123 have been reported as reliable techniques to determine even low amounts of P-glycoprotein expression and activity [80, 81]. For the detection of P-glycoprotein in solid tumors, radiolabeled substrates of P-glycoprotein (e.g. sestamibi) represent an interesting approach [82–84].
The pretherapeutic determination of P-glycoprotein expression in human tumors may be a valuable tool for personalized cancer therapy. In the case of high P-glycoprotein expression, anticancer drugs involved in the MDR phenotype may be ceased and other non-cross-resistant drugs or treatment modalities (e.g. immunotherapy) may be used. Another well-known approach is the use of inhibitors, which specifically inhibit the efflux function of P-glycoprotein, thereby, re-sensitizing tumors to standard antitumor drugs. This concept will be discussed in more detail in Chap. 7 of this book.
References
Rhoads CP. Report on a cooperative study of nitrogen mustard (HN2) therapy of neoplastic disease. Trans Assoc Am Physicians. 1947;60:110–7.
Welch AD. The problem of drug resistance in cancer chemotherapy. Cancer Res. 1959;19(4):359–71.
Shapiro DM. Combination chemotherapy of cancer based upon quantitative biochemical differences. Surg Forum. 1955;5:646–50.
Frei 3rd E, Holland JF, Schneiderman MA, Pinkel D, Selkirk G, Freireich EJ, et al. A comparative study of two regimens of combination chemotherapy in acute leukemia. Blood. 1958;13:1126–48.
DeVita Jr VT, Serpick AA, Carbone PP. Combination chemotherapy in the treatment of advanced Hodgkin’s disease. Ann Intern Med. 1970;73:881–95.
Kessel D, Botterill V, Woodinsky I. Uptake and retention of daunomycin by mouse leukemic cells as a factor in drug response. Cancer Res. 1968;28:938–41.
Biedler JL, Chang TD, Meyers MB, Peterson RH, Spengler BA. Drug resistance in Chinese hamster lung and mouse tumor cells. Cancer Treat Rep. 1983;67:859–67.
Riordan JR, Ling V. Genetic and biochemical characterization of multidrug resistance. Pharmacol Ther. 1985;28:51–75.
Dano K. Active outward transport of daunomycin in resistant Ehrlich ascites tumor cells. Biochim Biophys Acta. 1973;323:466–83.
Juliano RL, Ling V. A surface glycoprotein modulating drug permeability in Chinese hamster ovary cell mutants. Biochim Biophys Acta. 1976;455:152–62.
Skovsgaard T. Mechanisms of resistance to daunorubicin in Ehrlich ascites tumor cells. Cancer Res. 1978;38:1785–91.
Riordan JR, Ling V. Purification of P-glycoprotein from plasma membrane vesicles of Chinese hamster ovary cell mutants with reduced colchicine permeability. J Biol Chem. 1979;254:12701–5.
Roninson IB, Chin JE, Choi KG, Gros P, Housman DE, Fojo A, et al. Isolation of human mdr DNA sequences amplified in multidrug-resistant KB carcinoma cells. Proc Natl Acad Sci USA. 1986;83:4538–42.
Watson MB, Lind MJ, Cawkwell L. Establishment of in-vitro models of chemotherapy resistance. Anticancer Drugs. 2007;18:749–54.
Roepe PD. The role of the MDR protein in altered drug translocation across tumor cell membranes. Biochim Biophys Acta. 1995;1241:385–405.
Higgins CF. P-glycoprotein and cell volume-activated chloride channels. J Bioenerg Biomembr. 1995;27:63–70.
Higgins CF, Gottesman MM. Is the multidrug transporter a flippase? Trends Biochem Sci. 1992;17:18–21.
Sharom FJ. The P-glycoprotein multidrug transporter. Essays Biochem. 2011;50:161–78.
Ramu A, Glaubiger D, Magrath IT, Joshi A. Plasma membrane lipid structural order in doxorubicin-sensitive and -resistant P388 cells. Cancer Res. 1983;43:5533–7.
Nielsen D, Maare C, Skovsgaard T. Influx of daunorubicin in multidrug resistant Ehrlich ascites tumour cells: correlation to expression of P-glycoprotein and efflux. Influence of verapamil. Biochem Pharmacol. 1995;50:443–50.
Schimke RT, Kaufman RJ, Alt FW, Kellems RF. Gene amplification and drug resistance in cultured murine cells. Science. 1978;202:1051–5.
Haber M, Reed C, Kavallaris M, Norris MD, Stewart BW. Resistance to drugs associated with the multidrug resistance phenotype following selection with high-concentration methotrexate. J Natl Cancer Inst. 1989;81:1250–4.
Efferth T, Verdörfer I, Miyachi H, Sauerbrey A, Drexler HG, Chitambar CR, et al. Genomic imbalances in drug-resistant T-cell acute lymphoblastic CEM leukemia cell lines. Blood Cells Mol Dis. 2002;29:1–13.
Volm M, Drings P, Mattern J, Sonka J, Vogt-Moykopf I, Wayss K. Prognostic significance of DNA patterns and resistance-predictive tests in non-small cell lung carcinoma. Cancer. 1985;56:1396–403.
Volm M, Bak Jr M, Efferth T, Mattern J. Induced multidrug resistance in murine leukemia L1210 and associated changes in a surface-membrane glycoprotein. J Cancer Res Clin Oncol. 1989;115:17–24.
Tapiero H, Munck JN, Fourcade A, Lampidis TJ. Cross-resistance to rhodamine 123 in Adriamycin- and daunorubicin-resistant Friend leukemia cell variants. Cancer Res. 1984;44:5544–9.
Efferth T. Immuhistochemischer Nachweis von P-Glykoprotein und Akkumulation von Rhodamin 123 in tierischen und menschlichen Tumoren. PhD Thesis. Ruprecht Karls University, Heidelberg, Germany. 1990.
Efferth T, Klett T, Mattern J, Osswald H, Pommerenke EW, Stöhr M, et al. Reversing multidrug resistance in L1210 tumor cells by hycanthone or chlorophenoxamine in vitro and in vivo. Anticancer Res. 1991;11:1275–9.
Volm M, Efferth T, Günther A, Lathan B. Detection of murine S180 cells expressing a multidrug resistance phenotype using different in vitro test systems and a monoclonal antibody. Arzneimittelforschung/Drug Res. 1987;37:862–7.
Volm M, Bak Jr M, Efferth T, Mattern J. Induced multidrug-resistance in murine sarcoma 180 cells grown in vitro and in vivo and associated changes in expression of multidrug-resistance DNA-sequences and membrane glycoproteins. Anticancer Res. 1988;8:1169–78.
Volm M, Mattern J, Efferth T. P-Glykoprotein als Marker für Multidrug-Resistenz in Tumoren und Normalgewebe. Tumor Diagn Ther. 1990;11:189–97.
Volm M, Mattern J, Pommerenke EW. Time course of MDR gene amplification during in vivo selection for doxorubicin-resistance and during reversal in murine leukemia L1210. Anticancer Res. 1991;11:579–86.
Volm M. Multidrug Resistenz von Tumoren. Themen aus der Wissenschaft 6. Universität Kaiserslautern. ISBN 3-925 178-10-4; 1992. p 57–78.
Mattern J, Bak M, Volm M. Occurrence of a multidrug-resistant phenotype in human lung xenografts. Br J Cancer. 1987;56:407–11.
Volm M, Bak M, Mattern J. Intrinsic drug resistance in a human lung carcinoma xenograft is associated with overexpression of multidrug-resistance, DNA-sequences and of plasma membran glycoproteins. Arzneimittelforschung/Drug Res. 1988;38:1189–93.
Volm M. P-glycoprotein associated expression of c-fos and c-jun products in human lung carcinomas. Anticancer Res. 1993;13:375–8.
Volm M, Efferth T. Resistenzüberwindung bei Tumoren. Dtsch Med Wschr. 1994;119:475–9.
Volm M, Samsel B, Mattern J. Relationship between chemoresistance of lung tumours and cigarette smoking. Br J Cancer. 1990;62:255–6.
Fairchild CR, Ivy SP, Rushmore T, Lee G, Koo P, Goldsmith ME, et al. Carcinogen-induced mdr overexpression is associated with xenobiotic resistance in rat preneoplastic liver nodules and hepatocellular carcinomas. Proc Natl Acad Sci USA. 1987;84:7701–5.
Thorgeirsson SS, Huber BE, Sorrell S, Fojo A, Pastan I, Gottesman MM. Expression of the multidrug-resistant gene in hepatocarcinogenesis and regenerating rat liver. Science. 1987;236:1120–2.
Volm M, Zerban H, Mattern J, Efferth T. Overexpression of P-glycoprotein in rat hepatocellular carcinomas induced with N-nitrosomorpholine. Carcinogenesis. 1990;11:169–72.
Volm M, Mattern J, Samsel B. Overexpression of P-glycoprotein and glutathione S-transferase-pi in resistant non-small cell lung carcinomas of smokers. Br J Cancer. 1991;64:700–4.
Volm M, Efferth T, Bak M, Mattern J. Detection of drug resistance in human ovarian carcinoma. Arch Gynecol Obstet. 1989;244:123–8.
Volm M, Efferth T, Bak M, Ho AD, Mattern J. Detection of the multidrug resistant phenotype in human tumours by monoclonal antibodies and the streptavidin-biotinylated phycoerythrin complex method. Eur J Cancer Clin Oncol. 1989;25:743–9.
Volm M, Efferth T. Relationship of DNA ploidy to chemoresistance of tumors as measured by in vitro tests. Cytometry. 1990;11:406–10.
Mattern J, Efferth T, Bak M, Ho AD, Volm M. Detection of P-glycoprotein in human leukemias using monoclonal antibodies. Blut. 1989;58:215–7.
Bak Jr M, Efferth T, Mickisch G, Mattern J, Volm M. Detection of drug resistance and P-glycoprotein in human renal cell carcinomas. Eur Urol. 1990;17:72–5.
Efferth T, Löhrke H, Volm M. Correlations between natural resistance to doxorubicin, proliferative activity, and expression of P-glycoprotein 170 in human kidney tumor cell lines. Urol Res. 1990;18:309–12.
Volm M, Mattern J, Efferth T, Pommerenke EW. Expression of several resistance mechanisms in untreated human kidney and lung carcinomas. Anticancer Res. 1992;12:1063–7.
Volm M, Kästel M, Mattern J, Efferth T. Expression of resistance factors (P-glycoprotein, glutathione S-transferase-pi, and topoisomerase II) and their interrelationship to proto-oncogene products in renal cell carcinomas. Cancer. 1993;71:3981–7.
Volm M, Mattern J, Stammler G, Royer-Pokora B, Schneider S, Weirich A, et al. Expression of resistance-related proteins in nephroblastoma after chemotherapy. Int J Cancer. 1995;63:193–7.
Schneider J, Bak M, Efferth T, Kaufmann M, Mattern J, Volm M. P-glycoprotein expression in treated and untreated human breast cancer. Br J Cancer. 1989;60:815–8.
Schneider J, Efferth T, Mattern J, Rodriguez-Escudero FJ, Volm M. Immunohistochemical detection of the multi-drug-resistance marker P-glycoprotein in uterine cervical carcinomas and normal cervical tissue. Am J Obstet Gynecol. 1992;166:825–9.
Schneider J, Efferth T, Centeno MM, Mattern J, Rodríguez-Escudero FJ, Volm M. High rate of expression of multidrug resistance-associated P-glycoprotein in human endometrial carcinoma and normal endometrial tissue. Eur J Cancer. 1993;29A:554–8.
Efferth T, Osieka R. clinical relevance of the MDR-1 gene and its gene product, P-glycoprotein, for cancer chemotherapy: a meta-analysis. Tumor Diagn Ther. 1993;14:238–43.
Sauerbrey A, Zintl F, Volm M. P-glycoprotein and glutathione S-transferase pi in childhood acute lymphoblastic leukaemia. Br J Cancer. 1994;70:1144–9.
Verrelle P, Meissonnier F, Fonck Y, Feillel V, Dionet C, Kwiatkowski F, et al. Clinical relevance of immunohistochemical detection of multidrug resistance P-glycoprotein in breast carcinoma. J Natl Cancer Inst. 1991;83:111–6.
Schneider J, Romero H. Correlation of P-glycoprotein overexpression and cellular prognostic factors in formalin-fixed, paraffin-embedded tumor samples from breast cancer patients. Anticancer Res. 1995;15:1117–21.
Linn SC, Giaccone G, van Diest PJ, Blokhuis WM, van der Valk P, van Kalken CK, et al. Prognostic relevance of P-glycoprotein expression in breast cancer. Ann Oncol. 1995;6:679–85.
Atalay C, Demirkazik A, Gunduz U. Role of ABCB1 and ABCC1 gene induction on survival in locally advanced breast cancer. J Chemother. 2008;20:734–9.
Larkin A, O‘Driscoll L, Kennedy S, Purcell R, Moran E, Crown J, et al. Investigation of MRP-1 protein and MDR-1 P-glycoprotein expression in invasive breast cancer: a prognostic study. Int J Cancer. 2004;112:286–94.
Surowiak P, Materna V, Matkowski R, Szczuraszek K, Kornafel J, Wojnar A, et al. Relationship between the expression of cyclooxygenase 2 and MDR1/P-glycoprotein in invasive breast cancers and their prognostic significance. Breast Cancer Res. 2005;7:R862–70.
Tsukamoto F, Shiba E, Taguchi T, Sugimoto T, Watanabe T, Kim SJ, et al. Immunohistochemical detection of P-glycoprotein in breast cancer and its significance as a prognostic factor. Breast Cancer. 1997;4:259–63.
Del Principe MI, Del Poeta G, Maurillo L, Buccisano F, Venditti A, Tamburini A, et al. P-glycoprotein and BCL-2 levels predict outcome in adult acute lymphoblastic leukaemia. Br J Haematol. 2003;121:730–8.
Tafuri A, Gregorj C, Petrucci MT, Ricciardi MR, Mancini M, Cimino G, et al. GIMEMA Group. MDR1 protein expression is an independent predictor of complete remission in newly diagnosed adult acute lymphoblastic leukemia. Blood. 2002;100:974–81.
Dhooge C, De Moerloose B, Laureys G, Kint J, Ferster A, De Bacquer D, et al. P-glycoprotein is an independent prognostic factor predicting relapse in childhood acute lymphoblastic leukaemia: results of a 6-year prospective study. Br J Haematol. 1999;105:676–83.
Damiani D, Michelutti A, Michieli M, Masolini P, Stocchi R, Geromin A, et al. P-glycoprotein, lung resistance-related protein and multidrug resistance-associated protein in de novo adult acute lymphoblastic leukaemia. Br J Haematol. 2002;116:519–27.
Legrand O, Perrot JY, Simonin G, Baudard M, Cadiou M, Blanc C, et al. Adult biphenotypic acute leukaemia: an entity with poor prognosis which is related to unfavourable cytogenetics and P-glycoprotein over-expression. Br J Haematol. 1998;100:147–55.
Campos L, Guyotat D, Archimbaud E, Calmard-Oriol P, Tsuruo T, Troncy J, et al. Clinical significance of multidrug resistance P-glycoprotein expression on acute nonlymphoblastic leukemia cells at diagnosis. Blood. 1992;79:473–6.
Del Poeta G, Stasi R, Aronica G, Venditti A, Cox MC, Bruno A, et al. Clinical relevance of P-glycoprotein expression in de novo acute myeloid leukemia. Blood. 1996;87:1997–2004.
Goasguen JE, Dossot JM, Fardel O, Le Mee F, Le Gall E, Leblay R, et al. Expression of the multidrug resistance-associated P-glycoprotein (P-170) in 59 cases of de novo acute lymphoblastic leukemia: prognostic implications. Blood. 1993;81:2394–8.
Wuchter C, Leonid K, Ruppert V, Schrappe M, Büchner T, Schoch C, et al. Clinical significance of P-glycoprotein expression and function for response to induction chemotherapy, relapse rate and overall survival in acute leukemia. Haematologica. 2000;85:711–21.
Marie JP, Legrand O. MDR1/P-GP expression as a prognostic factor in acute leukemias. Adv Exp Med Biol. 1999;457:1–9.
Sievers EL, Smith FO, Woods WG, Lee JW, Bleyer WA, Willman CL, et al. Cell surface expression of the multidrug resistance P-glycoprotein (P-170) as detected by monoclonal antibody MRK-16 in pediatric acute myeloid leukemia fails to define a poor prognostic group: a report from the Childrens Cancer Group. Leukemia. 1995;9:2042–8.
Gsur A, Zöchbauer S, Götzl M, Kyrle PA, Lechner K, Pirker R. MDR1 RNA expression as a prognostic factor in acute myeloid leukemia: an update. Leuk Lymphoma. 1993;12:91–4.
Zöchbauer S, Gsur A, Brunner R, Kyrle PA, Lechner K, Pirker R. P-glycoprotein expression as unfavorable prognostic factor in acute myeloid leukemia. Leukemia. 1994;8:974–7.
Wood P, Burgess R, MacGregor A, Yin JA. P-glycoprotein expression on acute myeloid leukaemia blast cells at diagnosis predicts response to chemotherapy and survival. Br J Haematol. 1994;87:509–14.
Marie JP, Legrand O, Perrot JY, Chevillard S, Huet S, Robert J. Measuring multidrug resistance expression in human malignancies: elaboration of consensus recommendations. Semin Hematol. 1997;34(4 Suppl 5):63–71.
Efferth T. Testing for tumor drug resistance in the age of molecular medicine. A contribution to the debate round-table on phenotypic and genotypic analyses of multidrug resistance (MDR) in Clinical Hospital Practice. Leukemia. 1999;13(10):1627–9.
Huet S, Marie JP, Gualde N, Robert J. Reference method for detection of Pgp mediated multidrug resistance in human hematological malignancies: a method validated by the laboratories of the French Drug Resistance Network. Cytometry. 1998;34:248–56.
Huet S, Marie JP, Laurand A, Robert J. Major improvement of the reference method of the French drug resistance network for P-glycoprotein detection in human haematological malignancies. Leuk Res. 2005;29:1029–37.
Maffioli L, Steens J, Pauwels E, Bombardieri E. Applications of 99mTc-sestamibi in oncology. Tumori. 1996;82:12–21.
Sharma V. Radiopharmaceuticals for assessment of multidrug resistance P-glycoprotein-mediated drug transport activity. Bioconjug Chem. 2004;15:1464–74.
Efferth T, Langguth P. Transport processes of radiopharmaceuticals and -modulators. Radiat Oncol. 2011;6:59.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Volm, M., Efferth, T. (2015). Role of P-Glycoprotein for Resistance of Tumors to Anticancer Drugs: From Bench to Bedside. In: Efferth, T. (eds) Resistance to Targeted ABC Transporters in Cancer. Resistance to Targeted Anti-Cancer Therapeutics, vol 4. Springer, Cham. https://doi.org/10.1007/978-3-319-09801-2_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-09801-2_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-09800-5
Online ISBN: 978-3-319-09801-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)