
Abstract
Over the last two decades cardiovascular calcification (CVC) evolved from a poorly understood process and largely underestimated issue to one due to complex pathophysiologic mechanisms and posing significant health threats. Many clinical conditions are associated with the development of CVC and in several cases the events leading to its growth have been elucidated. Vascular calcification is not uniformly a marker of atherosclerosis, as extensive medial calcification can occur in patients with chronic kidney disease for example. Research efforts have focused on developing therapies tailored at slowing the progression of CVC in the hope to improve the health of affected subjects. Patients with chronic kidney disease are at particularly high risk of suffering from the consequences of CVC and have therefore been targeted with various inhibitors of calcification. Other rarer disorders associated with CVC also have been the focus of research leading to novel therapeutic advances. In this chapter we review some of the most common conditions associated with CVC and some of the most recent therapeutic advances in each area.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Chronic Kidney Disease
Epidemiology of Cardiovascular Calcification in CKD
Numerous studies have shown a relationship between vascular calcification and increased risk of cardiovascular (CV) events in patients with CKD as well as increased prevalence of CV calcification (CVC) with declining renal function. In the MESA study, the prevalence and severity of coronary artery calcium (CAC) among 1284 subjects with non-dialysis dependent CKD was higher compared to 5296 subjects with normal renal function [1]. Similar results were reported in the Dallas Heart Study. Patients with CKD, defined as microalbuminuria and an estimated glomerular filtration rate (eGFR) <60 ml/min × min × 1.73 m2, had an almost three-fold increase in risk of extensive CAC compared to patients with normal renal function (odds ratio of CAC greater than100 units: 2.85; 95% confidence interval, 0.92 to 8.80 in CKD vs no-CKD subjects) [2].
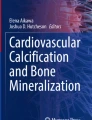
Gorriz et al. [3] showed a stepwise age-independent increase in prevalence and severity of vascular calcification in a cohort of 572 non-dialysis dependent CKD patients. Using simple imaging tools such as planar X-rays of the abdomen, hips and hands, to detect arterial calcification, the authors reported calcifications in one or more territories in 79% of the study participants; in 47% of the patients CVC was graded as severe. At dialysis inception the prevalence of CVC is about 60% and it increases to about 80% in patients on maintenance dialysis (Fig. 13.1) [4, 5]. Unlike the general population, there is no difference in markers of vasculopathy (namely thoracic aorta calcification, CAC or arterial stiffness) in patients receiving maintenance hemodialysis (HD) regardless of race or sex [6]. This suggests that dialysis is noxious for the CV system independent of clinical characteristics that may differentiate patients in the general population. Data on whether renal function restoration after kidney transplantation reduces the risk of CVC are limited and likely confounded by the concomitant use of various immunosuppressants [7].

Volume renderedimages of the (a) heart and (b) thoracic aorta in a patient receiving maintenance hemodialysis showing heavy calcification of the coronary arteries, aorta and cardiac valves. LAD left anterior descending coronary artery, LCX left circumflex coronary artery, RCA right coronary artery (image courtesy of Dr. An de Vriese, AZ Sint-Jan, Bruges, Belgium)
Studies evaluating CVC using simple imaging modalities such as vascular ultrasound and planar X-ray in the radial, femoral, iliac arteries [8,9,10,11], abdominal aorta [12, 13], and CAC on chest CTs [14, 15] have all shown CVC as a marker of risk in CKD. In both subjects with normal renal function and patients with CKD, the MESA study showed an association between CAC and CV events independent of age, sex, race and comorbid conditions [1]. In addition, CAC was a better predictor of outcome than markers of arterial stiffness (ankle-brachial index) and carotid intima media thickness. Similarly, the Chronic Renal Insufficiency Cohort study of 1541 non-dialysis patients with CKD showed that CAC predicted myocardial infarction, congestive heart failure and all-cause mortality, independent of baseline CV risk evaluated by traditional risk score algorithms [16]. Inclusion of CAC in a risk algorithm led to a small albeit significant increase in the accuracy of cardiovascular events prediction.
Vascular calcification has been shown to be an independent predictor of all-cause mortality irrespective of demographic, risk factors or comorbidities in patients with CKD receiving maintenance HD or peritoneal dialysis (PD) and after kidney transplantation [17, 18]. A simple cardiovascular calcification index (CCI) that included patient’s age, dialysis vintage, calcification of the cardiac valves, and abdominal aorta was linearly associated with risk of all-cause mortality in patients on HD, such that the unadjusted hazard risk (HR) increased by 12% for each point increase in CCI (P < 0.001) [19]. Adjustment for confounders did not substantially change the strength of the association. In contrast, as seen in the general population, the absence of CVC is a harbinger of an excellent prognosis. Block et al. showed that within a few weeks tomonths of initiating dialysis, CAC predicted mortality after adjustment for age, race, gender, and diabetes mellitus with an increase in mortality proportional to the baseline score (P = 0.002) [5]. Conversely, the mortality rate was low at 5 years in patients without CAC (3.3/100 patient years without CAC vs 14.7/100 patients years for CAC > 400). In a series of 179 patients receiving PD, in the absence of CAC, subjects had a significantly lower risk of all-cause mortality, cardiovascular mortality and cardiovascular events, even after adjustment for demographic and comorbid factors [18].
Observational studies have shown that deposition of hydroxyapatite in the arterial wall is linked to a decrease in arterial compliance and subsequently increased CV risk [20, 21]. Di Iorio et al. reported a significant association of CAC and arterial stiffness (assessed via pulse wave velocity) as well as abnormal myocardial repolarization (assessed via QT dispersion on EKG) in 132 incident hemodialysis patients [22]. In studies of patients with CKD not receiving dialysis, worsening CKD stage was associated with a stepwise increase in arterial stiffness [23, 24]. Similarly, Raggi and coworkers showed that patients on maintenance HD with evidence of valvular, thoracic and abdominal aorta calcification have reduced aortic compliance [25]. Observational data confirmed the cardiovascular risk inherent with decreasing arterial compliance.
Similar to vascular calcification, the prevalence and severity of aortic and mitral valve calcification are higher in patients with CKD compared to the general population and associated with an unfavourable outcome. Valvular calcification leads to disturbed leaflet mobility, increased transvalvular pressure gradients, left ventricular hypertrophy (for aortic stenosis) and left atrium enlargement (with mitral valve stenosis and regurgitation) leading to poor outcomes [26, 27]. The increased risk associated with valvular calcification appears independent of its reported association with coronary artery or aortic calcification [28].
The debate on whether calcium deposition is a repair mechanism versus promoter of vascular damage is still ongoing. There are data suggesting that the mineral content of a plaque is a predictor of survival along with the extent of CVC. Bellasi et al. showed that a higher CAC density was independently associated with increased all-cause mortality with and without adjustment for confounders in a series of 140 consecutive HD patients [29]. These results are in conflict with data reported in the general population. In fact, an inverse association between plaque density and survival was reported in the general population by the MESA investigators [30]. Reverse epidemiology is a plausible explanation. Since most patients with CKD die primarily and prematurely of CV related events [31], patients receiving maintenance hemodialysis may not be comparable age- and sex matches for individuals with normal renal function.
Pathophysiology of Vascular Calcification in CKD
There is a linear relationship between CV mortality and decreased eGFR and increased proteinuria [31]. The all-cause and CV mortality rates for patients on dialysis are at least 15–20 times higher than the general age- and gender-matched population [32, 33]. This burden of CV disease is evident upon the initiation of renal replacement therapy when 40% of patients already have evidence of coronary heart disease and up to 80% have abnormalities in left ventricular structure and function by echocardiographic criteria [32, 34].
It has been postulated that accelerated CVsenescence is one of the mechanisms responsible for development of CVC and CV risk in patients with impaired renal function [35]. Independent of age, CVC becomes more prevalent and severe as renal function declines [1]. A large body of evidence supports a biologically plausible, temporal [36] and dose-response [37] relationship between vascular calcification and CV risk in patients with CKD. Seminal findings by Goodman et al. demonstrated that CAC starts accumulating in young patients with end-stage renal disease (ESRD), decades before this pathology is observed in the normal population [38]. CAC scores in adult patients on HD have been reported to be over five-fold higher than age- and sex-matched individuals with established coronary artery disease, but normal kidney function [39]. A tendency for fast progression of CVC over 1 year has been reported in patients receiving HD [40]. Risk factors for greater progression of CVC in HD patients include age, diabetes mellitus, time since initiation of renal replacement therapy, and elevated levels of serum phosphorous and inflammatory markers. In addition to the extent of CVC, the rate of progression of CVC appears to be an important risk factor for CV events including mortality.
Intimal calcification is associated with the development and maturation of atherosclerotic lesions and is associated with traditional risk factors such as dyslipidemia, hypertension, diabetes and smoking and is not specific to CKD [41]. Medial calcification is more specific to CKD being associated with derangement of bone and mineral metabolism [42]. In addition, medial calcification is associated with vascular stiffening and arteriosclerosis observed with age and metabolic disorders including diabetes and ESRD. Beyond traditional risk factors, numerous non-traditional risk factors have been associated with CV aging and vascular calcification in CKD, namely inflammation, oxidative stress, metabolic derangements and accumulation of uremic toxins [35, 43].
Vascular calcification is considered an actively regulated process that may arise via a number of cellular mechanisms that include loss of calcification inhibitors, development of an osteogenic phenotype in vascular smooth muscle cells (VSMC), accumulation of protein aggregates and apoptotic bodies that serve to nucleate the development of hydroxyapatite, and disordered mineral metabolism.
In physiologic conditions, inhibitors such as pyrophosphate, matrix-GLA protein (MGP) or fetuin-A prevent transformation of amorphous calcium-phosphate complexes into insoluble crystals of hydroxyapatite and their precipitation in soft tissue including the blood vessels [42, 43]. In-vitro and in-vivo data also suggest the role of micronutrients in vascular calcification propagation [44]. Preclinical data showed that VSMC incubated with high serum levels of calcium and phosphate undergo a osteochondrogenic phenotypic switch and become capable of secreting bone matrix in the context of the arterial wall, triggering calcification deposition and progression [42]. In addition, chronically elevated serum concentration of calcium and phosphate may lead to precipitation of mineral nanocrystals and the activation of resident macrophages, pro-inflammatory cytokine secretion and cellular apoptosis in an attempt to eliminate calcium-phosphate crystals [43].
An imbalance in pro- and anti-inflammatory cytokines leads to a state of chronic subclinical inflammation in CKD. The synthesis of anti-calcifying factors such as fetuin-A and the anti-ageing α-klotho [45] is reduced due to over-expression of pro-inflammatory cytokines such as interleukin 6 (IL-6) or tumor necrosis factor alpha (TNFα). Fetuin-A is a glycoprotein synthesized in the liver and essential for the formation of the highly soluble calciproteins (a complex of fetuin-A and plasma calcium-phosphate crystals) that keep calcium and phosphorus from forming crystal in the circulation. The protein α-klotho modifies the binding of fibroblast growth factor 23 (FGF-23) to its receptor in the kidney increasing urinary phosphate wasting [43]. Downregulation of α-klotho expression has been linked with accelerated vascular ageing. Furthermore, dysregulation of the α-klotho/FGF-23 axis has been implicated in the development and progression of CVC although the exact role of this complex is not fully understood [46]. FGF-23 and α-klotho control phosphate excretion through the kidneys and may have a direct vascular protective role by modulating different signaling pathways such as FGF-receptor 1 and mTOR [43]. Further elucidation of the contribution of the FGF-23/α-klotho complex to the development of CVC in patients with CKD is needed.
Oxidative stress and advanced glycation end products (AGEs) generation, for which oxidative stress is partly responsible, have been implicated in the pathogenesis of CVC [43]. AGEs promote RANKL activation in osteoblasts and calcium/phosphate removal from the bone. In addition, experimental data suggest that AGEs may induce VSMC osteogenic differentiation through p38/mitogen-activated protein kinase (MAPK) and Wnt/β catenin signaling. Finally, AGEs together with other uremic toxins synergistically trigger inflammation by inducing the synthesis of pro-inflammatory cytokines (IL-1, IL-6, TNFα) linked to endothelial dysfunction and vascular calcification [43].
As renal function declines, uremic toxins such as indoxyl sulfate (IS) accumulate and may directly affect the vasculature [43]. IS triggers the expression of the sodium-phosphate co-transporter Pit-1 that leads to the osteogenic differentiation of VSMCs induced by calcium and phosphorus. In addition, IS suppresses liver synthesis of fetuin-A further predisposing CKD patients to vascular calcification development. Finally, epidemiological observations suggest that patients with CKD are deficient in vitamin K (cofactor for MGP carboxylation and activation), and pyrophosphate (a major endogenous inhibitor of calcium-phosphate crystals formation), and are thus further predisposed to the crystallization of calcium-phosphorus in soft tissues [47].
Therapeutic Approaches
Several treatments have been implemented to target various steps in the deranged metabolism of bone and minerals in CKD. The primary ones consisted of normalizing Ca, P, and parathyroid hormone serum levels, minimizing Vitamin D use or considering calcium sensing receptor activating drugs (“calcimimetics”) to control secondary hyperparathyroidism (see section on secondary hyperparathyroidism). Other approaches included administration of pyrophosphate (inhibitor of calcification), bisphosphates (inhibitors of bone osteoclastic activity), and Vitamin K (to favour the formation of active MGP) in patients with known CVC [48]. Only a few of these agents have demonstrated effectiveness in slowing progression of CVC.
Statins, primarily lipophilic, appear to accelerate rather than inhibit calcification progression probably due to the inhibition of vitamin K synthesis [49]. MGP is a potent inhibitor of calcification and requires activation through a Vitamin K-dependent pathway. One trial comparing Vitamin K antagonists vs direct oral anticoagulants has been reported, while two more ongoing trials are evaluating the effect of vitamin K supplementation on CVC progression. De Vriese et al. [50] randomized 132 maintenance hemodialysis patients to coumadin vs rivaroxaban or rivaroxaban plusVitamin K supplementation. Despite a reduction in the serum level of decarboxylated MGP (i.e. inactive MGP) with rivaroxaban or rivaroxaban plus Vitamin K2 supplementation, there was no significant slowing of progression of coronary artery, valvular and aortic calcification. The VitaVasK study of 348 patients on maintenance HD will evaluate the impact of Vitamin K1 on progression of thoracic aortic calcification and CAC compared to placebo [51]. The IRIVASC-Trial will evaluate the impact of rivaroxaban compared to coumadin/phenprocoumon on coronary and aortic valve calcification in 190 patients with an eGFR >15 mL/min/1.73 m2, and either atrial fibrillation or pulmonary embolism. (https://clinicaltrials.gov/ct2/show/NCT02066662?term=IRIVASC&draw=2&rank=1; last verified April 6, 2020).
Phosphate and its associated effects on FGF23 and PTH have been linked to CVC [5, 52], and inhibitors of intestinal phosphate absorption, either calcium-containing or calcium-free, are commonly used to correct hyperphosphatemia in patients with advanced CKD [53]. Several studies showed that calcium-based binders in CKD [54,55,56] and calcium supplements in patients without renal dysfunction [57, 58] promote formation of CVC, while inhibiting bone formation [59, 60]. These results were accompanied by an increase in mortality in randomized clinical trials of patients with CKD stage 3 to dialysis [61,62,63], and in a meta-analysis of randomized trials comparing calcium-based binders to the non-calcium based binders lanthanum and sevelamer [64]. Calcium-based binders had a detrimental effect on CAC progression and were associated with a significant increase in mortality in patients receiving HD compared to non-calcium phosphate binders [64]. Thus, current guidelines on bone and mineral metabolism management in patients with CKD suggest limiting the dose of calcium-based phosphate binders for all patients with renal impairment [65].
Animal and laboratory experiments suggested that magnesium modulates the development of phosphate-induced calcification in a dose-dependent manner [66,67,68,69]. Small clinical studies showed that magnesium either directly slowed CAC progression or indirectly reduced the propensity for calcification in patients with moderate to end-stage CKD [70,71,72]. An open label randomized trial in 120 patients with stage 3–4 CKD showed that magnesium significantly slowed progression of CAC compared to standard of care (median change: 11.3%, IQR 0–30.8 vs 39.5%, IQR 19.0–81.3; p < 0.001) in patients [73].
There are a few new compounds under investigation that might impact development and progression of CVC. Sotatercept, an anti-anemia compound that inhibits the Activin A receptor, in preclinical data showed an increase in bone mineralization and reduction in deposition of hydroxyapatite in the vasculature [74]. The immunosuppressant everolimus appears to increase the synthesis of Klotho by inhibiting mTOR, while the chemotherapeutic agent bortezomib may exert some protective effect against CVC progression by increasing Wnt/B-catenin signaling [74]. Finally, several Wnt inhibitor antagonists (sclerostin, DKK1-secreted frizzeled related proteins) are in early stage of preclinical development [74]. SNF472 targetsa novel pathway by selectively inhibiting the formation and growth of hydroxyapatite crystals, which are thought to be the final pathway in the development of vascular calcification. In the recently completed CaLIPSO, a double-blind, placebo-controlled phase 2b trial, SNF472 significantly attenuated the progression of CAC volume score (11% vs 20%, p = 0.016) compared to placebo in patients with ESRD receiving HD [75].
The pharmacological and surgical therapy of hyperparathyroidism are discussed in the next section.
Disorders of the Parathyroid Glands and Mineral Metabolism
The parathyroid hormone (PTH) is secreted by 4 small parathyroid glands located behind the thyroid gland. Until recently PTH was believed to be the primary regulator of phosphorus and calcium metabolism. However, a family of proteins known as phosphatonins described in the mid 1990s [76] is now thought to contribute very closely to the control of phosphorus metabolism along with PTH. The main actions of PTH include stimulating bone resorption, promoting phosphaturia, hydroxylation of 25-hydroxy vitamin D2 to its active form 1–25 dihydroxy vitamin D (Vit D3) in the kidney, as well as inducing calcium reabsorption from the distal renal tubule. Vit D3, in turn, promotes absorption of phosphorus and calcium from the gut and reabsorption of calcium from the distal tubule. The parathyroid glands are especially sensitive to calcium serum levels through the action of a cell membrane receptor known as calcium sensing receptor [77]. Of interest, this receptor is present in numerous other tissues and organs throughout the body. A low calcium level is rapidly detected at the parathyroid level by the calcium sensing receptor and it induces a powerful release of PTH. Several feedback mechanisms are operative between serum calcium and phosphorus levels, PTH, Vit D3, calcitonin (produced in the medulla of the thyroid gland) and fibroblast growth factor 23 (FGF-23) such that the serum levels of calcium and phosphorus are tightly controlled (Fig. 13.2a) [79].


(a) Physiologicalmaintenance of serum calcium and phosphorus levels through the interaction of parathyroid hormone, vitamin D3 and FGF-23. (b) As kidney injury occurs and chronic kidney disease progresses several feed-back mechanisms are ignited. This results in hyperplasia of the parathyroid glands, reduced production of active vitamin D3 and α-Klotho with increased production of FGF-23 and parathyroid hormone. This cascade of events eventually leads to progressive bone resorption and weakening along with increasing soft-tissue calcification (reproduced with permission from Komaba H [78])
FGF-23 is produced by osteoblasts and osteocytes and it is the best-known member of the phosphatonin family. Its primary functions are inactivation of the enzyme 1-α hydroxylase in the kidney to slow the formation of active Vit D3, induction of the 24-hydroxylase enzyme (that results in the formation of inactive 1-24-25(OH)3 vitamin D3), and induction of phosphaturia in the kidney proximal tubule. Essential to the functions of FGF-23 is its soluble protein α-Klotho. This protein binds to the FGF-23 receptor increasing the affinity of the receptor for FGF-23 and rendering the latter more efficient. PTH and FGF-23 levels rise very soon after renal function declines below a glomerular filtration rate of 60 ml/min/1.73 m2[80], and are part of a complex cascade of events involved in the development of the mineral-bone-and vascular disorder typical of advanced stagesof chronic kidney disease (Fig. 13.2b).
Hyperparathyroidism
Primary hyperparathyroidism (PHPT) is characterized by high parathyroid hormone (PTH) and calcium serum levels with low serum phosphorus. It is usually due to an adenoma (80% of the times) or hyperplasia of a parathyroid gland, although it can also rarely be due to a carcinoma of one of the glands or be part of a hereditary multiple endocrine neoplasia syndrome [81]. More frequently encountered is secondary hyperparathyroidism (SHPT) that typically develops in patients with advanced CKD. Other rare causes of SHPT include osteomalacia, rickets, and malabsorption. In CKD the high serum levels of parathyroid hormone (PTH) is due to hyperplasia of one or more parathyroid glands in response to the progressive retention of phosphate as renal failure declines, along with reduced activation of 25-hydroxycholecalciferol to VitD3. The loss of VitD3 eliminates an important negative feed-back on PTH suppression and causes reduced calcium absorption from the intestine along with reduced calcium retention at the level of the distal tubule. The declining serum calcium levels are detected by the calcium sensing receptor in the parathyroid glands chief cells and ignite a powerful release of PTH to restore balance. High PTH levels promote the maturation of osteoblasts into osteoclasts that act by removing calcium and phosphorus from the bone. Simultaneously, and likely preceding the rise in PTH, FGF-23 is released in a counter regulatory feed-back (Fig. 13.2b) [78]. Eventually the bone of patients with advanced CKD becomes resistant to the effects of minerals and hormones responsible for bone remodelling, while the parathyroid glands become progressively less responsive to the inhibitory effects of FGF-23. The end result is a progressive weakening of the bone architecture and loss of tensile strength leading to repetitive fractures. As manyas 20–30% of patients with SHPT develop tertiary HPT most commonly in the setting of renal transplant, where patients continue to have elevated PTH levels even after receiving a renal allograft [82]. It is believed that prolonged hypocalcemia may induce parathyroid gland hyperplasia that does not regress despite the renal transplant. Although tertiary HPT is usually caused by hyperplasia of all four glands, in some cases the disorder can be caused by adenomas of one or more parathyroid glands [83, 84]. Serum levels of minerals and hormones involved in the metabolism and remodeling of bone have been associated with subclinical cardiovascular disease and cardiovascular morbidity and mortality as well as all-cause death both in the general population and in patients with CKD. Onufrak et al. [85] showed an association between serum levels of phosphorus and thickness of the carotid intima-media layer in the general population. Adeney et al. [86] demonstrated that patients with moderate kidney dysfunctionwith higher serum phosphate levels, albeit still in the normal range, had more extensive vascular and valvular calcification than those with lower phosphate levels. High-normal serum phosphate levels were associated with a greater incidence of cardiovascular morbidity and mortality and/or all cause death in several population studies [87,88,89,90] Similarly, associations have been reported between PTH levels and subclinical and clinical cardiovascular disease [91, 92] all-cause death [93], heart failure [94, 95] and even vascular dementia [96] in the general population. FGF-23 levels have been associated with cardiac events [97,98,99] and ischemic stroke [100, 101], in subjects with normal renal function. Older studies reported an association between serum calcium levels and risk of myocardial infarction [102], cardiovascular and non-cardiovascular death in the community [103, 104] as well as valvular calcification [105].
In the quest for a potential mechanism of action to explain these findings, associations have been reported between traditional cardiovascular risk factors and higher serum levels of phosphorus [88] FGF-23 [106, 107] and calcium [102, 108]. In animal experiments, PTH has been shown to be independently able to induce extensive cardiovascular calcifications [109, 110]. Therefore, it should come as no surprise that patients affected by PHPT tend to suffer a higher than expected incidence of cardiovascular events compared to the general population [111, 112]. This is likely due to a combination of endothelial dysfunction [113], systemic hypertension [114, 115], left ventricular hypertrophy and dysfunction [115,116,118], cardiac arrhythmias and cardiac calcification. Calcium deposition is particularly frequent on the cardiac valves and in the myocardium of patients with PHPT [119, 120]. However, there does not appear to be an increased prevalence and severity of CAC especially in patients with mild hypercalcemia [120,121,123]. Surgical treatment for PHPT caused by adenomas restores endothelial and coronary microvascular dysfunction [124, 125]. Additionally, halted progression of cardiac and valvular calcification was reported both at one year and after 3.5 years from surgical intervention [126, 127]. Although a significant correlation between LVH and valvular calcification has been reported [119], as well as between LVH and myocardial calcifications [126], data on the effectiveness of parathyroidectomy in reversing structural and functional left ventricular changes are inconclusive [128].
An extensive body of literature documented an association between abnormalities of mineral metabolism and adverse events in ESRD [129]. For patients with moderate CKD, PTH levels have been associated with all-cause death but not cardiovascular events [130]. An association has been reported between FGF-23 and development of congestive heart failure but not atherosclerotic events in one study [131], and both types of events in another [132]. In a prospective cohort study, FGF-23 was not predictive of cardiovascular events or death in patients with CKD stage 3, while low VitD3 and elevated PTH levels were [133]. Finally, a recent meta-analysis concluded that the association between FGF-23 levels and cardiovascular outcomes may be non-causal, and therefore FGF-23 may be a bystander rather than a causative factor [134]. The inconsistent epidemiological evidence surrounding FGF-23 may be due to the heterogeneity of studies included in the analyses as well as the small number of subjects and events in some of the studies. Nonetheless, there is an undoubtful connection between the extensive vascular and valvular calcification of patients with advanced CKD and untoward outcomes [3, 21, 29, 134,135,137]. As described in the section dedicated to CKD, multiple trials directed at slowing the progression of calcification have been conducted. The compounds used to slow progression tested so far include: calcium-based and non calcium-based phosphate binders such as sevelamer, lanthanum and magnesium; molecules capable of stimulating the calcium sensing receptor (calcimimetics) such as cinacalcet and etelcalcetide to reduce the release of PTH from the parathyroid glands; and direct inhibitors of the formation of crystals of hydroxyapatite. Numerous publications have demonstrated the ability of non-calcium-based phosphate binders to slow the progression of cardiovascular calcification, and one meta-analysis showed that these compounds may also reduce mortality [64]. A randomized clinical trial compared the effectiveness of cinacalcet plus low dose VitD3 versus liberal doses of VitD3 to control SHPT in patients receiving hemodialysis [138]. The primary study results showed a borderline effectiveness of the calcimimetic to slow cardiovascular calcification progression. However, in the per-protocol analyses cinacalcet and low dose VitD3 were very effective at slowing progression of CAC, and valvular calcification [139]. The related outcome trial failed to show a reduction in all-cause mortality and major cardiovascular events [140], although a subanalysis showed a potential role of cinacalcet in reducing non-atherosclerotic cardiovascular events [141]. In a subanalysis of the INDEPENDENT trial, patients with ESRD who received the non-calcium based phosphate binder sevelamer along with cinacalcet showed a lower mortality rate than those receiving calcium-based binders with cinacalcet or patients receiving VitD3 with any binder [142]. These results highlighted the importance of phosphorus control while avoiding imbalances of calcium metabolism. The most recent trial directed at slowing progression of cardiovascular calcification in ESRD explored the potential of a direct inhibitor of hydroxyapatite [75]. The drug reduced further expansion of CAC by 45–75% in the intention to treat and per-protocol analyses. No outcome data are yet available related to this compound. Parathyroidectomy has a role in SHPT when medical therapy fails to control the biochemical alterations of this conditions often associated with severe bone and vascular abnormalities. In observational studies parathyroidectomy has been associated with slowing of CAC progression [143] and reduction in cardiovascular mortality [143,144,146]. However, no randomized controlled study has been conducted to compare medical therapy versus surgical intervention for SHPT [147], often leaving the choice of treatment to the preference of thetreating physician.
Hypoparathyroidism
Sporadic idiopathic hypoparathyroidism (SIH), either due to an autoimmune disease or caused by complex genetic abnormalities, is a rare endocrinological disorder characterized by low serum levels of parathyroid hormone and calcium, and elevation in serum phosphate [148]. The disease can manifest with a variety of neuromuscular and sensory symptoms such tetany, muscle cramping, airway obstruction, laryngospasm, chronic fatiguability, peri-oral numbness and generalized paresthesia, but also seizures, parkinsonism, depression, irritability and cognitive impairment. Ectopic deposition of crystals of calcium and phosphorus has been reported to involve several tissues. Calcification of the cerebral basal ganglia has been classically associated with this disorder (Fig. 13.3) [149]. Although its true pathogenesis remains unclear, it is probably related to prolonged hypocalcemia and simultaneous hyperphosphatemia [150]. Calcification of the eyes and kidneys is also frequent and associated with cataract formation and progressive renal function decline [151]. Peripheral vascular calcification and coronary artery calcification have been reported, but with a much lower prevalence [152]. Therefore, the impact of CAC on the incidence of cardiovascular events in patients affected by hypoparathyroidism is unknown. Nonetheless, other types of cardiovascular complications have been reported such as supraventricular and ventricular cardiac arrhythmias, the latter probably secondary to prolonged QT, and left ventricular systolic dysfunction.

Head computedtomography scan showing extensive calcification of the basal ganglia (horizontal arrows in section a and solid vertical arrow in section b), and cerebellum (open vertical arrow in section b) (reproduced with permission from Harada K [149])
A form of relative hypoparathyroidism, known as low turnover bone disease, has been described in patients with ESRD. In this condition serum levels of PTH are relatively lower than needed to induce periodic bone remodeling, and this causes progressive bone weakening and worsening cardiovascular calcification. As in the case of very high PTH levels, low levels of PTH have also been associated with increased mortality in patients undergoing hemodialysis [153, 154]. The use of high calcium concentrations in the dialysate fluid, large doses of calcium-based phosphate binders and VitD3 appear to be the most frequent mechanisms inducing suppression of pulsatile release of PTH that is necessary for its activity on bone remodeling and mineral metabolism. In a subanalysis of a randomized clinical trial in ESRD, the authors showed that the progression of CAC was more pronounced in patients with diabetes mellitus, particularly in those receiving calcium-based phosphate binders compared to those receiving a calcium free binder [155]. Confirming the significance of this observation, in a longitudinal study of over 53,500 Japanese patients receiving dialysis, the highest incidence of myocardial infarction was observed in patients with high dialysate calcium and lowserum PTH levels [156].
Human Immunodeficiency Syndrome
After the introduction of highly active antiretroviral therapy (HAART)patients living with human immunodeficiency virus (PLWH) have had a significant increase in life expectancy [157, 158]. As a result, cardiovascular diseases (CVD) have become a leading cause of mortality and morbidity in PLWH [159, 160]. An intense debate has revolved around the pathophysiology of CVD development, spurred by the observation that traditional risk factors are highly prevalent in PLWH but do not appear to justify the entire risk [161]. The consensus appears to be that a combination of traditional and non-traditional risk factors is contributory [162]. Several investigators have raised the possibility that some HAART, especially abacavir and those in the protease inhibitor family, may raise the risk of cardiovascular events [162,163,165]. Additionally, smoldering inflammation and a state of ongoing immune activation due to chronic HIV infection, enhanced permeability of the gastrointestinal barrier to bacteria, and co-infection with other viruses are likely sources of ongoing vascular damage [166]. As a result PLWH are believed to experience an accelerated ageing process in the context of a highly inflamed environment (inflamageing of HIV). In fact, several publications have demonstrated an increased inflammatory arterial burden in PLWH [167, 168].
Despite the increased risk, most of the tools utilized to predict atherosclerotic cardiovascular events in the general population perform poorly in PLWH [169]. Therefore, imaging of sub-clinical atherosclerosis has received mounting attention in this population for early detection of disease, enhanced risk prediction and -ultimately- improved prognosis.
Subclinical Atherosclerosis in HIV
Early publications remarked on the increased carotid intima-media thickness (IMT) as an indirect marker of atherosclerosis in PLWH. Hsue et al. reported that PLWH had a thicker IMT than matched controls; HIV infection was an independent predictor of carotid IMT after adjustment for age, sex, smoking, hypertension, dyslipidemia and diabetes mellitus [170]. Additionally, a nadir CD4 count <200 cells/mL was a predictor of IMT progression in these patients. Similarly, Salmazo et al. reported that PLWH had a thicker carotid IMT than controls [171]. Furthermore, carotid plaques were detected with ultrasound imaging in 37% of PLWH and 4% of controls (p < 0.001). PLWH with carotid plaques had higher serum lipid levels and poorer glycemic control. Infection with HIV increased the odds of having a carotid plaque by five fold after adjustment for obesity, smoking and age. Chest computed tomography has provided valuable insight into the prevalence and development ofatherosclerotic disease in PLWH. Post et al. reported a higher prevalence of non-calcified coronary artery plaques detected by means of computed tomography angiography (CTA) in PLWH compared to controls, although they did not observe an increased prevalence or extent of coronary artery calcium (CAC) [172]. On the contrary, Guaraldi et al. remarked on the utility of CAC as a marker of ageing and cardiovascular risk in PLWH [173]. Using previously validated CAC equations, they showedthat as many as 40% of PLWH have a vascular age on average 15-year older than age and sex matched controls. Cardiometabolic risk factors such as elevated serum triglycerides and cholesterol lipoproteins were associated with increased vascular age in univariate analyses, although the only multivariable predictor of older vascular age was the current CD4 cell count. Additional indirect evidence of accelerated ageing and atherosclerosis accrual in PLWH was provided by the observation that high CAC scores are associated with a lower bone mineral density of the femoral head [174].
The importance of altered cardiometabolism as a predisposing factor to the development of subclinical atherosclerosis in PLWH was addressed in several publications. Guaraldi et al. described an association of CAC with the presence of lipodystrophy in long-term users of HAART [175]. Epicardial adipose tissue (EAT) is visceral adipose tissue layered directly over the coronary arteries and is a source of adipocytokines that can stimulate the development of atherosclerosis both via paracrine and endocrine mechanisms [176]. EAT volume is increased in PLWH [177], and is associated with high CAC scores as well as lipodystrophy, serum lipoprotein levels, markers of HIV infection such as CD4 cell count and duration of HAART use [178]. The increase of EAT over time was shown to parallel progression of CAC and to be associated with male sex and CD4 cell count [179]. Finally, both EAT and CAC were shown to be predictive of incident myocardial infarction and death in an observational study of 843 PLWH followed for a median of 2.8 years [180]. Not only is CAC more abundant and prevalent in PLWH, marking the presence of more extensive atherosclerosis, but it also progresses more rapidly than in the general population [181]. Its progression is associated with age, LDL cholesterol serum level, abdominal visceral adipose tissue and CD4 cell count [182]. As noted, there are recurrent factors involved in the development and progression of CAC in PLWH, supporting the notion that traditional and non-traditionalrisk factors are involved. Nuclear-based molecular imaging provides a more sophisticated approach to detecting subclinical atherosclerosis and accrual of vascular calcification.18F-sodium fluoride (NaF) is a tracer used in positron emission tomography imaging with high affinity for growing microcrystals of hydroxyapatite [183]. Its primary use is for the detection of bone metastases. However, recent evidence suggests that it avidly adheres on the surface of microcrystals in the context of unstable atherosclerotic plaques [184, 185]. In a recent experiment, areas of high uptake of NaF were detected in 50% of 300 arterial territories in metabolically stable PLWH receiving long-term HAART (Fig. 13.4) [186]. Furthermore, coronary artery uptake of NaF was significantly more frequent than FDG uptake in PLWH [187]. The high prevalence of NaF uptake in PLWH contrasted with a much lower prevalence than in ambulatory patients with diabetes mellitus, consideredat equally increased cardiovascular risk [188]. Using molecular imaging another interesting observation was made by Zanni et al. [189] In a proof of concept study in 12 HAART naïve patients, the author compared baseline vascular and systemic (i.e. axillary and mediastinal lymph nodes) inflammation assessed with FDG, as well as biomarkers of immune activation prior to and after initiation of HAART. Patients were treated with a combination HAART and followed for a median of 7 months before imaging and serological markers were repeated. Although systemic inflammation and markers of immune activation decreased, there was parallel increase in vascular inflammation. Therefore, based on these preliminary results, there seems to be a disconnect between the cardiovascular and systemic effects of HAART, supporting the notion that HAART may be responsible for part of the increased risk reportedin PLWH.

Positron emissiontomography/computed tomography merged images on the carotid arteries of a patient living with HIV. The crosshair and white arrows point at an area along the right carotid artery where a calcified lesion shows a high uptake of18F-sodium-fluoride. (reproduced with permission from Raggi P [186]. under the Creative Commons Attribution 4.0 International License; http://creativecommons.org/licenses/by/4.0/)
Pseudoxanthoma Elasticum
This autosomal recessive disease affects 1:100.000 to 1:25.000 live births and it is due to a defect in the ATP binding cassette-6 (ABCC6) gene [190, 191]. The hallmark of the disease is a yellowish discoloration and loss of elasticity of the skin, especially in the neck, nape and axillary areas, visual impairment and vascular calcification [192]. The actual pathophysiology of calcification is unclear, but the defective ABCC6gene is likely associated with a low level of the naturally occurring inhibitor of calcification pyrophosphate [193]. Other inhibitors of systemic calcification, such as MGA and fetuin-A, as also seen in patients with CKD [194], may be defective or reduced. The resulting imbalance between inhibitors of calcification and serum phosphate and calcium levels leads to the creation of an environment favouring the development of systemic calcification. Crystals of amorphous calcification (calcium, hydrogen and phosphate), as well as true hydroxyapatite are found in the context of disrupted elastic fibers in the mid dermis, and in the intima and media of small to mid-size arteries (Fig. 13.5). Calcifications can also be found amid disrupted collagen fibers in the myocardium and pericardium of affected patients. The typical eye lesions are known as angioid streaks of the fundus; despite looking like proliferating vessels they are due to disruption of the Bruch’s membrane by fibrocalcific deposits. Eventually the retina is invaded by proliferating neo-vessels that can lead to severe macular damage and blindness [195]. The most frequent cardiovascular manifestations of pseudoxanthoma elasticum (PXE) are claudication of the upper and lower extremities and transient ischemic attacks and stroke [196, 197], while the risk of myocardial infarction does not appear to be significantly increased above that of the general population. However, an increased risk of ischemicheart disease and vascular calcification has been reported in heterozygous carriers of ABBC6 mutations [198]. Aortic aneurysms, stenosis of the radial and carotid arteries have also been reported, along with asymptomatic calcification of kidneys, spleen, pancreas, breast, testicles and liver. Progressive loss of kidney function has been reported as well as frequent gastrointestinal bleeding. Eventually, increased peripheral resistance and pulse pressure due to medial calcification may also induce brain damage and cognitive impairment leading to another highly undesirable cardiovascular complication [199, 200].

Histological findings in a patient with pseudoxantoma elasticum, showing disrupted (a) and calcified (b) elastic fibers in the dermis; (c) the electronmicroscopy image shows high resolution details of the calcified elastic fibers. (reproduced with permission from Germain DP [191] under the Creative Commons Attribution 4.0 International License; http://creativecommons.org/licenses/by/4.0/)
A recent trial demonstrated that slowing of peripheral arterial calcification in PXE can be obtained with etidronate, a bisphosphonate with a mechanism of action similar to that of pyrophosphate normally used for the treatment of osteoporosis [201]. Other potentially effective new therapies are the newly developed direct inhibitors of hydroxyapatite crystals formation [202]. These derivatives of the naturally occurring inhibitor of vascular calcification, myo-inositol hexakisphosphate, have been shown to inhibit inception and growth of cardiovascular calcification in animal experiments independent of the underlying pathophysiologic mechanism [203]. These drugs hold great promise for the treatment of systemic calcification not only in rare diseases, but for patients with advanced CKD [75] and the general population as well.
References
Matsushita K, Sang Y, Ballew SH, et al. Subclinical atherosclerosis measures for cardiovascular prediction in CKD. J Am Soc Nephrol. 2015;26:439–47.
Kramer H, Toto R, Peshock R, et al. Association between chronic kidney disease and coronary artery calcification: the Dallas Heart Study. J Am Soc Nephrol. 2005;16:507–13.
Gorriz JL, Molina P, Cerveron MJ, et al. Vascular calcification in patients with nondialysis CKD over 3 years. Clin J Am Soc Nephrol. 2015;10:654–66.
Chertow GM, Burke SK, Raggi P. Sevelamer attenuates the progression of coronary and aortic calcification in hemodialysis patients. Kidney Int. 2002;62:245–52.
Raggi P, Boulay A, Chasan-Taber S, et al. Cardiac calcification in adult hemodialysis patients. A link between end-stage renal disease and cardiovascular disease? J Am Coll Cardiol. 2002;39:695–701.
Bellasi A, Veledar E, Ferramosca E, et al. Markers of vascular disease do not differ in black and white hemodialysis patients despite a different risk profile. Atherosclerosis. 2008;197:242–9.
D’Marco L, Bellasi A, Mazzaferro S, et al. Vascular calcification, bone and mineral metabolism after kidney transplantation. World J Transplant. 2015;5:222–30.
London GM, Guerin AP, Marchais SJ, et al. Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18:1731–40.
Safar ME, Blacher J, Pannier B, et al. Central pulse pressure and mortality in end-stage renal disease. Hypertension. 2002;39:735–8.
Adragao T, Pires A, Lucas C, et al. A simple vascular calcification score predicts cardiovascular risk in haemodialysis patients. Nephrol Dial Transplant. 2004;19:1480–8.
Bellasi A, Ferramosca E, Muntner P, et al. Correlation of simple imaging tests and coronary artery calcium measured by computed tomography in hemodialysis patients. Kidney Int. 2006;70:1623–8.
Okuno S, Ishimura E, Kitatani K, et al. Presence of abdominal aortic calcification is significantly associated with all-cause and cardiovascular mortality in maintenance hemodialysis patients. Am J Kidney Dis. 2007;49:417–25.
Verbeke F, Van Biesen W, Honkanen E, et al. Prognostic value of aortic stiffness and calcification for cardiovascular events and mortality in dialysis patients: outcome of the Calcification Outcome in Renal Disease (CORD) Study. Clin J Am Soc Nephrol. 2010;6:153–6.
Shantouf R, Budoff MJ, Ahmadi N, et al. Effects of sevelamer and calcium-based phosphate binders on lipid and inflammatory markers in hemodialysis patients. Am J Nephrol. 2008;28:275–9.
Block GA, Raggi P, Bellasi A, et al. Mortality effect of coronary calcification and phosphate binder choice in incident HD patients. Kidney Int. 2007;71:438–41.
Chen J, Budoff MJ, Reilly MP, et al. Coronary artery calcification and risk of cardiovascular disease and death among patients with chronic kidney disease. JAMA Cardiol. 2017;2:635–43.
Bellasi A, Raggi P. Vascular calcification in chronic kidney disease: usefulness of a marker of vascular damage. J Nephrol. 2011;24(Suppl 18):S11–5.
Xie Q, Ge X, Shang D, et al. Coronary artery calcification score as a predictor of all-cause mortality and cardiovascular outcome in peritoneal dialysis patients. Perit Dial Int. 2016;36:163–70.
Bellasi A, Block GA, Ferramosca E, Ratti C, Raggi P. Integration of clinical and imaging data to predict death in hemodialysis patients. Hemodial Int. 2013;17:12–8.
Blacher J, Guerin AP, Pannier B, et al. Impact of aortic stiffness on survival in end-stage renal disease. Circulation. 1999;99:2434–9.
Blacher J, Guerin AP, Pannier B, et al. Arterial calcifications, arterial stiffness, and cardiovascular risk in end-stage renal disease. Hypertension. 2001;38:938–42.
Di Iorio B, Nargi O, Cucciniello E, et al. Coronary artery calcification progression is associated with arterial stiffness and cardiac repolarization deterioration in hemodialysis patients. Kidney Blood Press Res. 2011;34:180–7.
Wang MC, Tsai WC, Chen JY, et al. Stepwise increase in arterial stiffness corresponding with the stages of chronic kidney disease. Am J Kidney Dis. 2005;45:494–501.
Kim CS, Bae EH, Ma SK, et al. Chronic kidney disease-mineral bone disorder in korean patients: a report from the KoreaN Cohort Study for Outcomes in Patients With Chronic Kidney Disease (KNOW-CKD). J Korean Med Sci. 2017;32:240–8.
Raggi P, Bellasi A, Ferramosca E, et al. Association of pulse wave velocity with vascular and valvular calcification in hemodialysis patients. Kidney Int. 2007;71:802–7.
Pressman GS, Movva R, Topilsky Y, et al. Mitral annular dynamics in mitral annular calcification: a three-dimensional imaging study. J Am Soc Echocardiogr. 2015;28:786–94.
Movva R, Murthy K, Romero-Corral A, et al. Calcification of the mitral valve and annulus: systematic evaluation of effects on valve anatomy and function. J Am Soc Echocardiogr. 2013;26:1135–42.
Raggi P, Bellasi A, Gamboa C, et al. All-cause mortality in hemodialysis patients with heart valve calcification. Clin J Am Soc Nephrol. 2011;6:1990–5.
Bellasi A, Ferramosca E, Ratti C, et al. The density of calcified plaques and the volume of calcium predict mortality in hemodialysis patients. Atherosclerosis. 2016;250:166–71.
Criqui MH, Denenberg JO, Ix JH, et al. Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA. 2014;311:271–8.
Thompson S, James M, Wiebe N, et al. Cause of death in patients with reduced kidney function. J Am Soc Nephrol. 2015;26:2504–11.
US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am J Kidney Dis. 2019 Oct 31. pii: S0272-6386(19)31008-X.
Baigent C, Burbury K, Wheeler D. Premature cardiovascular disease in chronic renal failure. Lancet. 2000 Jul 8;356(9224):147–52.
Bansal N, Keane M, Delafontaine P, et al. A longitudinal study of left ventricular function and structure from CKD to ESRD: The CRIC Study. Clin J Am Soc Nephrol. 2013;8(3):355–62.
Kooman JP, Kotanko P, Schols AM, et al. Chronic kidney disease and premature ageing. Nat Rev Nephrol. 2014;10:732–42.
Sigrist M, Bungay P, Taal MW, McIntyre CW. Vascular calcification and cardiovascular function chronic kidney disease. Nephrol Dial Transplant. 2006;21:707–14.
Garland JS, Holden RM, Groome PA, et al. Prevalence and associations of coronary artery calcification in patients with stages 3 to 5 CKD without cardiovascular disease. Am J Kidney Dis. 2008;52:849–58.
Goodman WG, Goldin J, Kuizon BD, et al. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med. 2000;342:1478–83.
Moe SM, Chen NX. Pathophysiology of vascular calcification in chronic kidney Disease. Circ Res. 2004;95:560–7.
McCullough PA, Agrawal V, Danielewicz E, Abela GS. Accelerated atherosclerotic calcification and Mönckeberg’s sclerosis: a continuum of advanced vascular pathology in chronic kidney disease. Clin J Am Soc Nephrol. 2008;3(6):1585–98.
Sage AP, Tintut Y, Demer LL. Regulatory mechanisms in vascular calcification. Nat Rev Cardiol. 2010;7:528–36.
Raggi P, Giachelli C, Bellasi A. Interaction of vascular and bone disease in patients with normal renal function and patients undergoing dialysis. Nat Clin Pract Cardiovasc Med. 2007;4:26–33.
Henaut L, Chillon JM, Kamel S, et al. Updates on the mechanisms and the care of cardiovascular calcification in chronic kidney disease. Semin Nephrol. 2018;38:233–50.
Bellasi A, Di Lullo L, Raggi P. Cardiovascular calcification: the emerging role of micronutrients. Atherosclerosis. 2018;273:119–21.
Mencke R, Hillebrands JL. NIGRAM consortium. The role of the anti-ageing protein Klotho in vascular physiology and pathophysiology. Ageing Res Rev. 2017;35:124–46.
Kuro-O M. The Klotho proteins in health and disease. Nat Rev Nephrol. 2019;15:27–44.
Villa-Bellosta R, Egido J. Phosphate, pyrophosphate, and vascular calcification: a question of balance. Eur Heart J. 2017;38:1801–4.
O’Neill WC, Lomashvili KA. Recent progress in the treatment of vascular calcification. Kidney Int. 2010 Dec;78(12):1232–9.
Chen Z, Qureshi AR, Parini P, et al. Does statins promote vascular calcification in chronic kidney disease? Eur J Clin Investig. 2017;47:137–48.
De Vriese AS, Caluwé R, Pyfferoen L, De Bacquer D, De Boeck K, Delanote J, De Surgeloose D, Van Hoenacker P, Van Vlem B, Verbeke F. Multicenter randomized controlled trial of vitamin K antagonist replacement by rivaroxaban with or without vitamin K2 in hemodialysis patients with atrial fibrillation: the Valkyrie Study. J Am Soc Nephrol. 2020;31:186–96.
Krueger T, Schlieper G, Schurgers L, et al. Vitamin K1 to slow vascular calcification in haemodialysis patients (VitaVasK trial): a rationale and study protocol. Nephrol Dial Transplant. 2014;29:1633–8.
Jono S, McKee MD, Murry CE, et al. Phosphate regulation of vascular smooth muscle cell calcification. Circ Res. 2000;87:E10–7.
Isakova T, Ix JH, Sprague SM, et al. Rationale and approaches to phosphate and Fibroblast Growth Factor 23 reduction in CKD. J Am Soc Nephrol. 2015;26:2328–39.
Chertow GM, Burke SK, Raggi P, Treat to Goal Working Group. Sevelamer attenuates the progression of coronary and aortic calcification in hemodialysis patients. Kidney Int. 2002;62:245–52.
Block GB, Spiegel DM, Ehrlich J, et al. Effects of sevelamer and calcium on coronary artery calcification in patients new to HD. Kidney Int. 2005;68:1815–24.
Chertow GM, Raggi P, Chasan-Taber S, Bommer J, Holzer H, Burke SK. Determinants of progressive vascular calcification in haemodialysis patients. Nephrol Dial Transplant. 2004;19:1489–96.
Anderson JJ, Kruszka B, Delaney JA, et al. Calcium intake from diet and supplements and the risk of coronary artery calcification and its progression among older adults: 10-year follow-up of the Multi-Ethnic Study of Atherosclerosis (MESA). J Am Heart Assoc. 2016;5(10):e003815.
Hulbert M, Turner ME, Hopman WM, Anastassiades T, Adams MA, Holden RM. Changes in vascular calcification and bone mineral density in calcium supplement users from the Canadian Multi-center Osteoporosis Study (CaMOS). Atherosclerosis. 2020;296:83–90.
Raggi P, James G, Burke SK, Bommer J, Chasan-Taber S, Holzer H, Braun J, Chertow GM. Decrease in thoracic vertebral bone attenuation with calcium-based phosphate binders in hemodialysis. J Bone Miner Res. 2005;20:764–72.
Morelli MB, Santulli G, Gambardella J. Calcium supplements: good for the bone, bad for the heart? A systematic updated appraisal. Atherosclerosis. 2020;296:68–73.
Block GA, Raggi P, Bellasi A, Kooienga L, Spiegel DM. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney Int. 2007;71:438–41.
Di Iorio B, Bellasi A, Russo D. Mortality in kidney disease patients treated with phosphate binders: A Randomized Study. Clin J Am Soc Nephrol. 2012;7:487–93.
Di Iorio B, Molony D, Bell C, et al. Sevelamer versus calcium carbonate in incident hemodialysis patients: results of an open-label 24-month randomized clinical trial. Am J Kidney Dis. 2013;62:771–8.
Jamal SA, Vandermeer B, Raggi P, et al. Effect of calcium-based versus non-calcium-based phosphate binders on mortality in patients with chronic kidney disease: an updated systematic review and meta-analysis. Lancet. 2013;382:1268–77.
Ketteler M, Block GA, Evenepoel P, et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Guideline Update: what’s changed and why it matters. Kidney Int. 2017;92:26–36. Kidney Int. 2017;92:1558.
Kircelli F, Peter ME, Sevinc Ok E, et al. Magnesium reduces calcification in bovine vascular smooth muscle cells in a dose-dependent manner. Nephrol Dial Transplant. 2012;27:514–21.
Louvet L, Buchel J, Steppan S, Passlick-Deetjen J, Massy ZA. Magnesium prevents phosphate-induced calcification in human aortic vascular smooth muscle cells. Nephrol Dial Transplant. 2013;28:869–78.
Xu J, Bai Y, Jin J, et al. Magnesium modulates the expression levels of calcification-associated factors to inhibit calcification in a time-dependent manner. Exp Ther Med. 2015;9:1028–34.
Diaz-Tocados JM, Peralta-Ramirez A, Rodriguez-Ortiz ME, et al. Dietary magnesium supplementation prevents and reverses vascular and soft tissue calcifications in uremic rats. Kidney Int. 2017;92:1084–99.
Spiegel DM, Farmer B. Long-term effects of magnesium carbonate on coronary artery calcification and bone mineral density in hemodialysis patients: a pilot study. Hemodial Int. 2009;13:453–9.
Tzanakis IP, Stamataki EE, Papadaki AN, Giannakis N, Damianakis NE, Oreopoulos DG. Magnesium retards the progress of the arterial calcifications in hemodialysis patients: a pilot study. Int Urol Nephrol. 2014;46:2199–205.
Bressendorff I, Hansen D, Schou M, et al. Oral magnesium supplementation in chronic kidney disease stages 3 and 4: efficacy, safety, and effect on serum calcification propensity-a prospective randomized double-blinded placebo-controlled clinical trial. Kidney Int Rep. 2017;2:380–9.
Sakaguchi Y, Hamano T, Obi Y, et al. A randomized trial of magnesium oxide and oral carbon adsorbent for coronary artery calcification in predialysis CKD. J Am Soc Nephrol. 2019;30:1073–85.
Wu M, Rementer C, Giachelli CM. Vascular calcification: an update on mechanisms and challenges in treatment. Calcif Tissue Int. 2013;93:365–73.
Raggi P, Bellasi A, Bushinsky D, Bover J, Rodriguez M, Ketteler M, Sinha S, Salcedo C, Gillotti K, Padgett C, Garg R, Gold A, Perelló J, Chertow GM. Slowing progression of cardiovascular calcification with SNF472 in patients on hemodialysis: results of a randomized phase 2b study. Circulation. 2020;141(9):728–39.
Cai Q, Hodgson SF, Kao PC, Lennon VA, Klee GG, Zinsmiester AR, Kumar R. Brief report: inhibition of renal phosphate transport by a tumor product in a patient with oncogenic osteomalacia. N Engl J Med. 1994;330(23):1645–9.
Brown EM, Gamba G, Riccardi D, et al. Cloning and characterization of an extracellular Ca(2+)-sensing receptor from bovine parathyroid. Nature. 1993;366:575–80.
Komaba H, Fukagawa M. FGF23-parathyroid interaction: implications in chronic kidney disease. Kidney Int. 2010 Feb;77(4):292–8.
Voinescu A, Iqbal NW, Martin KJ. Pathophysiology of chronic kidney disease-mineral and bone disorder. In: Turner N, Lameire N, Goldsmith DJ, Winearls CG, Himmelfarber J, Remuzzi G, editors. Oxford textbook of clinical nephrology. 4th ed. Oxford: Oxford University Press; 2016. p. 934–8.
Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, Andress DL. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int. 2007;71(1):31–8.
Marx SJ, Simonds WF, Agarwal SK, et al. Hyperparathyroidism in hereditary syndromes: special expressions and special managements. J Bone Miner Res. 2002;17(Suppl. 2):N37–43.
Pitt SC, Sippel RS, Chen H. Secondary and tertiary hyperparathyroidism, state of the art surgical management. Surg Clin North Am. 2009;89:1227–39.
Kebebew E, Duh QY, Clark OH. Tertiary hyperparathyroidism: histologic patterns of disease and results of parathyroidectomy. Arch Surg. 2004;139:974–7.
Kerby JD, Rue LW, Blair H, Hudson S, Sellers MT, Diethelm AG. Operative treatment of tertiary hyperparathyroidism: a single-center experience. Ann Surg. 1998;227:878–86.
Onufrak SJ, Bellasi A, Shaw LJ, Herzog CA, Cardarelli F, Wilson PW, Vaccarino V, Raggi P. Phosphorus levels are associated with subclinical atherosclerosis in the general population. Atherosclerosis. 2008;199:424–31.
Adeney KL, Siscovick DS, Ix JH, Seliger SL, Shlipak MG, Jenny NS, Kestenbaum BR. Association of serum phosphate with vascular and valvular calcification in moderate CKD. J Am Soc Nephrol. 2009;20:381–7.
Hagström E, Hellman P, Larsson TE, Ingelsson E, Berglund L, Sundström J, Melhus H, Held C, Lind L, Michaëlsson K, Arnlöv J. Plasma parathyroid hormone and the risk of cardiovascular mortality in the community. Circulation. 2009;119:2765–71.
Onufrak SJ, Bellasi A, Cardarelli F, Vaccarino V, Muntner P, Shaw LJ, Raggi P. Investigation of gender heterogeneity in the associations of serum phosphorus with incident coronary artery disease and all-cause mortality. Am J Epidemiol. 2009;169:67–77.
Campos-Obando N, Lahousse L, Brusselle G, Stricker BH, Hofman A, Franco OH, Uitterlinden AG, Zillikens MC. Serum phosphate levels are related to all-cause, cardiovascular and COPD mortality in men. Eur J Epidemiol. 2018;33:859–71.
Dhingra R, Sullivan LM, Fox CS, Wang TJ, D’Agostino RB Sr, Gaziano JM, Vasan RS. Relations of serum phosphorus and calcium levels to the incidence of cardiovascular disease in the community. Arch Intern Med. 2007;167:879–85.
Hagström E, Michaëlsson K, Melhus H, Hansen T, Ahlström H, Johansson L, Ingelsson E, Sundström J, Lind L, Arnlöv J. Plasma-parathyroid hormone is associated with subclinical and clinical atherosclerotic disease in 2 community-based cohorts. Arterioscler Thromb Vasc Biol. 2014;34:1567–73.
Hagström E, Ahlström T, Ärnlöv J, Larsson A, Melhus H, Hellman P, Lind L. Parathyroid hormone and calcium are independently associated with subclinical vascular disease in a community-based cohort. Atherosclerosis. 2015;238:420–6.
Yang B, Lu C, Wu Q, Zhang J, Zhao H, Cao Y. Parathyroid hormone, cardiovascular and all-cause mortality: a meta-analysis. Clin Chim Acta. 2016;455:154–60.
Wannamethee SG, Welsh P, Papacosta O, Lennon L, Whincup PH, Sattar N. Elevated parathyroid hormone, but not vitamin D deficiency, is associated with increased risk of heart failure in older men with and without cardiovascular disease. Circ Heart Fail. 2014;7:732–9.
Bansal N, Zelnick L, Robinson-Cohen C, Hoofnagle AN, Ix JH, Lima JA, Shoben AB, Peralta CA, Siscovick DS, Kestenbaum B, de Boer IH. Serum parathyroid hormone and 25-hydroxyvitamin D concentrations and risk of incident heart failure: the Multi-Ethnic Study of Atherosclerosis. J Am Heart Assoc. 2014;3:e001278.
Hagström E, Kilander L, Nylander R, Larsson EM, Michaëlsson K, Melhus H, Ahlström H, Johansson L, Lind L, Arnlöv J. Plasma parathyroid hormone is associated with vascular dementia and cerebral hyperintensities in two community-based cohorts. J Clin Endocrinol Metab. 2014;99:4181–9.
Kestenbaum B, Sachs MC, Hoofnagle AN, Siscovick DS, Ix JH, Robinson-Cohen C, Lima JA, Polak JF, Blondon M, Ruzinski J, Rock D, de Boer IH. Fibroblast growth factor-23 and cardiovascular disease in the general population: the Multi-Ethnic Study of Atherosclerosis. Circ Heart Fail. 2014;7:409–17.
Panwar B, Judd SE, Wadley VG, Jenny NS, Howard VJ, Safford MM, Gutiérrez OM. Association of fibroblast growth factor 23 with risk of incident coronary heart disease in community-living adults. JAMA Cardiol. 2018;3:318–25.
di Giuseppe R, Kühn T, Hirche F, Buijsse B, Dierkes J, Fritsche A, Kaaks R, Boeing H, Stangl GI, Weikert C. Plasma fibroblast growth factor 23 and risk of cardiovascular disease: results from the EPIC-Germany case-cohort study. Eur J Epidemiol. 2015;30:131–41.
Panwar B, Jenny NS, Howard VJ, Wadley VG, Muntner P, Kissela BM, Judd SE, Gutiérrez OM. Fibroblast growth factor 23 and risk of incident stroke in community-living adults. Stroke. 2015;46:322–8.
Wright CB, Dong C, Stark M, Silverberg S, Rundek T, Elkind MS, Sacco RL, Mendez A, Wolf M. Plasma FGF23 and the risk of stroke: the Northern Manhattan Study (NOMAS). Neurology. 2014;82:1700–6.
Lind L, Skarfors E, Berglund L, Lithell H, Ljunghall S. Serum calcium: a new, independent, prospective risk factor for myocardial infarction in middle-aged men followed for 18 years. J Clin Epidemiol. 1997;50:967–73.
Lundgren E, Lind L, Palmer M, et al. Increased cardiovascular mortality and normalized serum calcium in patients with mild hypercalcemia followed up for 25 years. Surgery. 2001;130:978–85.
Larsson TE, Olauson H, Hagström E, Ingelsson E, Arnlöv J, Lind L, Sundström J. Conjoint effects of serum calcium and phosphate on risk of total, cardiovascular, and noncardiovascular mortality in the community. Arterioscler Thromb Vasc Biol. 2010;30:333–9.
Akat K, Kaden JJ, Schmitz F, Ewering S, Anton A, Klomfass S, Hoffmann R, Ortlepp JR. Calcium metabolism in adults with severe aortic valve stenosis and preserved renal function. Am J Cardiol. 2010;105:862–4.
Gutiérrez OM, Wolf M, Taylor EN. Fibroblast growth factor 23, cardiovascular disease risk factors, and phosphorus intake in the health professionals follow-up study. Clin J Am Soc Nephrol. 2011;6:2871–8.
di Giuseppe R, Kühn T, Hirche F, Buijsse B, Dierkes J, Fritsche A, Kaaks R, Boeing H, Stangl GI, Weikert C. Potential predictors of plasma fibroblast growth factor 23 concentrations: cross-sectional analysis in the EPIC-Germany Study. PLoS One. 2015;10(7):e0133580.
Wareham NJ, Byrne CD, Carr C, Day NE, Boucher BJ, Hales CN. Glucose intolerance is associated with altered calcium homeostasis: a possible link between increased serum calcium concentration and cardiovascular disease mortality. Metabolism. 1997;46:1171–7.
Neves KR, Graciolli FG, dos Reis LM, Graciolli RG, Neves CL, Magalhães AO, Custódio MR, Batista DG, Jorgetti V, Moysés RM. Vascular calcification: contribution of parathyroid hormone in renal failure. Kidney Int. 2007;71:1262–70.
Graciolli FG, Neves KR, dos Reis LM, Graciolli RG, Noronha IL, Moysés RM, Jorgetti V. Phosphorus overload and PTH induce aortic expression of Runx2 in experimental uraemia. Nephrol Dial Transplant. 2009;24:1416–21.
Andersson P, Rydberg E, Willenheimer R. Primary hyperparathyroidism and heart disease—a review. Eur Heart J. 2004;25:1776–87.
Walker MD, Silverberg SJ. Cardiovascular aspects of primary hyperparathyroidism. J Endocrinol Investig. 2008;31:925–31.
Baykan M, Erem C, Erdoğan T, Hacihasanoğlu A, Gedikli O, Kiriş A, Küçükosmanoğlu M, Ersöz HO, Celik S. Impairment of flow mediated vasodilatation of brachial artery in patients with primary hyperparathyroidism. Int J Cardiovasc Imaging. 2007;23:323–8.
Hulter HN, Melby JC, Peterson JC, Cooke CR. Chronic continuous PTH infusion results in hypertension in normal subjects. J Clin Hypertens. 1986;2:360–70.
Jorde R, Svartberg J, Sundsfjord J. Serum parathyroid hormone as a predictor of increase in systolic blood pressure in men. J Hypertens. 2005;23:1639–44.
Saleh FN, Schirmer H, Sundsfjord J, Jorde R. Parathyroid hormone and left ventricular hypertrophy. Eur Heart J. 2003;24:2054–60.
Ozdemir D, Kalkan GY, Bayram NA, Onal ED, Ersoy R, Bozkurt E, Cakir B. Evaluation of left ventricle functions by tissue Doppler, strain, and strain rate echocardiography in patients with primary hyperparathyroidism. Endocrine. 2014;47:609–17.
Walker MD, Fleischer JB, Di Tullio MR, Homma S, Rundek T, Stein EM, Zhang C, Taggart T, McMahon DJ, Silverberg SJ. Cardiac structure and diastolic function in mild primary hyperparathyroidism. J Clin Endocrinol Metab. 2010;95:2172–9.
Längle F, Abela C, Koller-Strametz J, et al. Primary hyperparathyroidism and the heart: cardiac abnormalities correlated to clinical and biochemical data. World J Surg. 1994;18:619–24.
Stefenelli T, Abela C, Frank H, et al. Cardiac abnormalities in patients with primary hyperparathyroidism: implications for follow up. J Clin Endocrinol Metab. 1997;82:106–12.
Mesquita PN, Dornelas Leão Leite AP, Chagas Crisóstomo SD, Veras Filho E, da Cunha Xavier L, Bandeira F. Evaluation of coronary calcium score in patients with normocalcemic primary hyperparathyroidism. Vasc Health Risk Manag. 2017;13:225–9.
Kepez A, Harmanci A, Hazirolan T, Isildak M, Kocabas U, Ates A, Ciftci O, Tokgozoglu L, Gürlek A. Evaluation of subclinical coronary atherosclerosis in mild asymptomatic primary hyperparathyroidism patients. Int J Cardiovasc Imaging. 2009;25:187–93.
Streeten EA, Munir K, Hines S, Mohamed A, Mangano C, Ryan KA, Post W. Coronary artery calcification in patients with primary hyperparathyroidism in comparison with control subjects from the multi-ethnic study of atherosclerosis. Endocr Pract. 2008;14:155–61.
Osto E, Fallo F, Pelizzo MR, Maddalozzo A, Sorgato N, Corbetti F, Montisci R, Famoso G, Bellu R, Lüscher TF, Iliceto S, Tona F. Coronary microvascular dysfunction induced by primary hyperparathyroidism is restored after parathyroidectomy. Circulation. 2012;126:1031–9.
Ekmekci A, Abaci N, Colak Ozbey N, Agayev A, Aksakal N, Oflaz H, Erginel-Unaltuna N, Erbil Y. Endothelial function and endothelial nitric oxide synthase intron 4a/b polymorphism in primary hyperparathyroidism. J Endocrinol Investig. 2009;32:611–6.
Stefenelli T, Mayr H, Bergler-Klein J, et al. Primary hyperparathyroidism: incidence of cardiac abnormalities and partial reversibility after successful parathyroidectomy. Am J Med. 1993;95:197–202.
Dalberg K, Brodin LAA, Juhlin-Dannfelt A, et al. Cardiac function in primary hyperparathyroidism before and after operation. An echocardiographic study. Eur J Surg. 1996;162:171–6.
Best CAE, Krishnan R, Malvankar-Mehta MS, MacNeil SD. Echocardiogram changes following parathyroidectomy for primary hyperparathyroidism: a systematic review and meta-analysis. Medicine (Baltimore). 2017;96(43):e7255.
Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol. 2004;15:2208–18.
Seiler-Mussler S, Limbach AS, Emrich IE, Pickering JW, Roth HJ, Fliser D, Heine GH. Association of nonoxidized parathyroid hormone with cardiovascular and kidney disease outcomes in chronic kidney disease. Clin J Am Soc Nephrol. 2018;13:569–76.
Seiler S, Rogacev KS, Roth HJ, Shafein P, Emrich I, Neuhaus S, Floege J, Fliser D, Heine GH. Associations of FGF-23 and sKlotho with cardiovascular outcomes among patients with CKD stages 2-4. Clin J Am Soc Nephrol. 2014;9:1049–58.
Scialla JJ, Xie H, Rahman M, Anderson AH, Isakova T, Ojo A, Zhang X, Nessel L, Hamano T, Grunwald JE, Raj DS, Yang W, He J, Lash JP, Go AS, Kusek JW, Feldman H, Wolf M, Chronic Renal Insufficiency Cohort (CRIC) Study Investigators. Fibroblast growth factor-23 and cardiovascular events in CKD. J Am Soc Nephrol. 2014;25:349–60.
Shardlow A, McIntyre NJ, Fluck RJ, McIntyre CW, Taal MW. Associations of fibroblast growth factor 23, vitamin D and parathyroid hormone with 5-year outcomes in a prospective primary care cohort of people with chronic kidney disease stage 3. BMJ Open. 2017;7(8):e016528.
Marthi A, Donovan K, Haynes R, Wheeler DC, Baigent C, Rooney CM, Landray MJ, Moe SM, Yang J, Holland L, di Giuseppe R, Bouma-de Krijger A, Mihaylova B, Herrington WG. Fibroblast growth factor-23 and risks of cardiovascular and noncardiovascular diseases: a meta-analysis. J Am Soc Nephrol. 2018;29:2015–27.
Fox CS, Larson MG, Vasan RS, Guo CY, Parise H, Levy D, Leip EP, O’Donnell CJ, D’Agostino RB Sr, Benjamin EJ. Cross-sectional association of kidney function with valvular and annular calcification: the Framingham heart study. J Am Soc Nephrol. 2006;17:521–7.
Bellasi A, Ferramosca E, Ratti C, Block G, Raggi P. Cardiac valve calcification is a marker of vascular disease in prevalent hemodialysis patients. J Nephrol. 2012;25:211–8.
Goodman WG. Vascular calcification in end-stage renal disease. J Nephrol. 2002;15(Suppl 6):S82–5.
Raggi P, Chertow GM, Torres PU, Csiky B, Naso A, Nossuli K, Moustafa M, Goodman WG, Lopez N, Downey G, Dehmel B, Floege J, ADVANCE Study Group. The ADVANCE study: a randomized study to evaluate the effects of cinacalcet plus low-dose vitamin D on vascular calcification in patients on hemodialysis. Nephrol Dial Transplant. 2011;26:1327–39.
Urena-Torres PA, Floege J, Hawley CM, et al. Protocol adherence and the progression of cardiovascular calcification in the ADVANCE study. Nephrol Dial Transplant. 2013;28:146–52.
EVOLVE Trial Investigators, Chertow GM, Block GA, Correa-Rotter R, Drüeke TB, Floege J, Goodman WG, Herzog CA, Kubo Y, London GM, Mahaffey KW, Mix TC, Moe SM, Trotman ML, Wheeler DC, Parfrey PS. Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis. N Engl J Med. 2012;367:2482–94.
Wheeler DC, London GM, Parfrey PS, Block GA, Correa-Rotter R, Dehmel B, Drüeke TB, Floege J, Kubo Y, Mahaffey KW, Goodman WG, Moe SM, Trotman ML, Abdalla S, Chertow GM, Herzog CA; EValuation Of Cinacalcet HCl Therapy to Lower CardioVascular Events (EVOLVE) Trial Investigators. Effects of cinacalcet on atherosclerotic and nonatherosclerotic cardiovascular events in patients receiving hemodialysis: the EValuation Of Cinacalcet HCl Therapy to Lower CardioVascular Events (EVOLVE) trial. J Am Heart Assoc. 2014 Nov 17;3(6):e001363. Erratum in: J Am Heart Assoc. 2015 Jan;4(1):e000570.
Bellasi A, Cozzolino M, Russo D, et al. Cinacalcet but not vitamin D use modulates the survival benefit associated with sevelamer in the INDEPENDENT study. Clin Nephrol. 2016;86:113–24.
Daniel WT, Weber C, Bailey JA, Raggi P, Sharma J. Prospective analysis of coronary calcium in patients on dialysis undergoing a near-total parathyroidectomy. Surgery. 2013;154:1315–21.
Sharma J, Raggi P, Kutner N, Bailey J, Zhang R, Huang Y, Herzog CA, Weber C. Improved long-term survival of dialysis patients after near-total parathyroidectomy. J Am Coll Surg. 2012;214:400–7.
Iwamoto N, Sato N, Nishida M, Hashimoto T, Kobayashi H, Yamasaki S, Ono T, Nishimura M, Tokoro T, Sakoda C, Murakawa M, Okino K, Okamoto Y, Imai R, Adachi N, Ninomiya K, Mabuchi H, Koyama M, Nakanouchi T, Iseki K. Total parathyroidectomy improves survival of hemodialysis patients with secondary hyperparathyroidism. J Nephrol. 2012;25:755–63.
Iwamoto N, Sato N, Nishida M, Hashimoto T, Kobayashi H, Yamazaki S, Okino K, Nishimura M, Takatani T, Okamoto Y, Nakanouchi T, Koyama M, Adachi N, Ninomiya K, Mabuchi H, Iseki K. Low parathyroid hormone levels after parathyroidectomy reduce cardiovascular mortality in chronic hemodialysis patients. Clin Exp Nephrol. 2016;20:808–14.
Apetrii M, Goldsmith D, Nistor I, Siriopol D, Voroneanu L, Scripcariu D, Vervloet M, Covic A. Impact of surgical parathyroidectomy on chronic kidney disease-mineral and bone disorder (CKD-MBD) – a systematic review and meta-analysis. PLoS One. 2017;12(11):e0187025.
Shoback D. Clinical practice. Hypoparathyroidism. N Engl J Med. 2008;359:391–403.
Harada K, Fujikawa T. Intracranial calcification due to hypoparathyroidism. Am J Med. 2018;131(6):e253–4.
Goswami R, Sharma R, Sreenivas V, Gupta N, Ganapathy A, Das S. Prevalence and progression of basal ganglia calcification and its pathogenic mechanism in patients with idiopathic hypoparathyroidism. Clin Endocrinol. 2012;77:200–6.
Mitchell DM, Regan S, Cooley MR, et al. Long-term follow-up of patients with hypoparathyroidism. J Clin Endocrinol Metab. 2012;97:4507–14.
Agarwal P, Prakash M, Singhal M, Bhadada SK, Gupta Y, Khandelwal N. To assess vascular calcification in the patients of hypoparathyroidism using multidetector computed tomography scan. Indian J Endocrinol Metab. 2015;19:785–90.
Tentori F, Wang M, Bieber BA, Karaboyas A, Li Y, Jacobson SH, Andreucci VE, Fukagawa M, Frimat L, Mendelssohn DC, Port FK, Pisoni RL, Robinson BM. Recent changes in therapeutic approaches and association with outcomes among patients with secondary hyperparathyroidism on chronic hemodialysis: the DOPPS study. Clin J Am Soc Nephrol. 2015;10:98–109.
Merle E, Roth H, London GM, Jean G, Hannedouche T, Bouchet JL, Drüeke T, Fouque D, Daugas E. French Calcium and Phosphate Observatory Low parathyroid hormone status induced by high dialysate calcium is an independent risk factor for cardiovascular death in hemodialysis patients. Kidney Int. 2016;89:666–74.
Galassi A, Spiegel DM, Bellasi A, Block GA, Raggi P. Accelerated vascular calcification and relative hypoparathyroidism in incident haemodialysis diabetic patients receiving calcium binders. Nephrol Dial Transplant. 2006;21:3215–22.
Tagawa M, Hamano T, Sueta S, Ogata S, Saito Y. Higher dialysate calcium concentration is associated with incident myocardial infarction among diabetic patients with low bone turnover: a longitudinal study. Sci Rep. 2018;8:10060.
Wada N, Jacobson LP, Cohen M, French A, Phair J, Muñoz A. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984-2008. Am J Epidemiol. 2013;177:116–25.
Van Sighem AI, Gras LAJ, Reiss P, Brinkman K, de Wolf F. Life expectancy of recently diagnosed asymptomatic HIV-infected patients approaches that of uninfected individuals. AIDS. 2010;24:1527–35.
Mocroft A, Reiss P, Gasiorowski J, Ledergerber B, Kowalska J, Chiesi A, Gatell J, Rakhmanova A, Johnson M, Kirk O, Lundgren J. Serious fatal and nonfatal non-AIDS-defining illnesses in Europe. J Acquir Immune Defic Syndr. 2010;55:262–70.
Freiberg MS, Chang C-CH, Kuller LH, Skanderson M, Lowy E, Kraemer KL, Butt AA, Bidwell Goetz M, Leaf D, Oursler KA, Rimland D, Rodriguez Barradas M, Brown S, Gibert C, McGinnis K, Crothers K, Sico J, Crane H, Warner A, Gottlieb S, Gottdiener J, Tracy RP, Budoff M, Watson C, Armah KA, Doebler D, Bryant K, Justice AC. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med. 2013;173:614–22.
Shahbaz S, Manicardi M, Guaraldi G, Raggi P. Cardiovascular disease in human immunodeficiency virus infected patients: a true or perceived risk? World J Cardiol. 2015;7:633–44.
Savès M, Chêne G, Ducimetière P, Leport C, Le Moal G, Amouyel P, Arveiler D, Ruidavets J-B, Reynes J, Bingham A, Raffi F. Risk factors for coronary heart disease in patients treated for human immunodeficiency virus infection compared with the general population. Clin Infect Dis. 2003;37:292–8.
Friis-Moller N, Reiss P, Sabin CA, et al. Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med. 2007;356:1723–35.3.
Sabin CA, Worm SW, Weber R, et al. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multicohort collaboration. Lancet. 2008;371:1417–26.
Ryom L, Lundgren JD, El-Sadr W, et al. Cardiovascular disease and use of contemporary protease inhibitors: the D:A:D international prospective multicohort study. Lancet HIV. 2018;5:e291–300.
Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a chronic disease. Lancet. 2013;382:1525–33.
Tawakol A, Lo J, Zanni MV, Marmarelis E, Ihenachor EJ, MacNabb M, Wai B, Hoffmann U, Abbara S, Grinspoon S. Increased arterial inflammation relates to high-risk coronary plaque morphology in HIV-infected patients. J Acquir Immune Defic Syndr. 2014;66:164–71.
Subramanian S, Tawakol A, Burdo TH, Abbara S, Wei J, Vijayakumar J, Corsini E, Abdelbaky A, Zanni MV, Hoffmann U, Williams KC, Lo J, Grinspoon SK. Arterial inflammation in patients with HIV. JAMA. 2012;308:379–86.
Raggi P, De Francesco D, Manicardi M, Zona S, Bellasi A, Stentarelli C, Carli F, Beghetto B, Mussini C, Malagoli A, et al. Prediction of hard cardiovascular events in HIV patients. J Antimicrob Chemother. 2016;71:3515–8.
Hsue PY, Lo JC, Franklin A, Bolger AF, Martin JN, Deeks SG, Waters DD. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation. 2004;109:1603–8.
Salmazo PS, Bazan SGZ, Shiraishi FG, Bazan R, Okoshi K, Hueb JC. Frequency of subclinical atherosclerosis in Brazilian HIV-infected patients. Arq Bras Cardiol. 2018 May;110(5):402–10.
Post WS, Budoff M, Kingsley L, Palella FJ, Witt MD, Li X, George RT, Brown TT, Jacobson LP. Associations between HIV infection and subclinical coronary atherosclerosis. Ann Intern Med. 2014;160:458–67.
Guaraldi G, Zona S, Alexopoulos N, Orlando G, Carli F, Ligabue G, Fiocchi F, Lattanzi A, Rossi R, Modena MG, Esposito R, Palella F, Raggi P. Coronary aging in HIV-infected patients. Clin Infect Dis. 2009;49:1756–62.
Bellasi A, Zona S, Orlando G, Carli F, Ligabue G, Rochira V, Santoro A, Mussini C, Guaraldi G, Raggi P. Inverse correlation between vascular calcification and bone mineral density in human immunodeficiency virus-infected patients. Calcif Tissue Int. 2013;93:413–8.
Guaraldi G, Stentarelli C, Zona S, Orlando G, Carli F, Ligabue G, Lattanzi A, Zaccherini G, Rossi R, Modena MG, Alexopoulos N, Palella F, Raggi P. Lipodystrophy and anti-retroviral therapy as predictors of sub-clinical atherosclerosis in human immunodeficiency virus infected subjects. Atherosclerosis. 2010;208:222–7.
Alexopoulos N, Katritsis D, Raggi P. Visceral adipose tissue as a source of inflammation and promoter of atherosclerosis. Atherosclerosis. 2014;233:104–12.
Lo J, Abbara S, Rocha-Filho JA, Shturman L, Wei J, Grinspoon SK. Increased epicardial adipose tissue volume in HIV-infected men and relationships to body composition and metabolic parameters. AIDS. 2010;24:2127–30.
Guaraldi G, Scaglioni R, Zona S, Orlando G, Carli F, Ligabue G, Besutti G, Bagni P, Rossi R, Modena MG, Raggi P. Epicardial adipose tissue is an independent marker of cardiovascular risk in HIV-infected patients. AIDS. 2011;25:1199–205.
Zona S, Raggi P, Bagni P, Orlando G, Carli F, Ligabue G, Scaglioni R, Rossi R, Modena MG, Guaraldi G. Parallel increase of subclinical atherosclerosis and epicardial adipose tissue in patients with HIV. Am Heart J. 2012;163:1024–30.
Raggi P, Zona S, Scaglioni R, Stentarelli C, Ligabue G, Besutti G, Menozzi M, Santoro A, Malagoli A, Bellasi A, Guaraldi G. Epicardial adipose tissue and coronary artery calcium predict incident myocardial infarction and death in HIV-infected patients. J Cardiovasc Comput Tomogr. 2015;9:553–8.
Guaraldi G, Zona S, Orlando G, Carli F, Ligabue G, Fiocchi F, Menozzi M, Rossi R, Modena MG, Raggi P. Human immunodeficiency virus infection is associated with accelerated atherosclerosis. J Antimicrob Chemother. 2011;66:1857–60.
Guaraldi G, Zona S, Orlando G, Carli F, Ligabue G, Fiocchi F, Rossi R, Modena MG, Raggi P. Progression of coronary artery calcium in men affected by human immunodeficiency virus infection. Int J Cardiovasc Imaging. 2012;28:935–41.
Blau M, Nagler W, Bender MA. Fluorine-18: a new isotope for bone scanning. J Nucl Med. 1962;3:332–4.
Lee JM, Bang JI, Koo BK, Hwang D, Park J, Zhang J, Yaliang T, Suh M, Paeng JC, Shiono Y, Kubo T, Akasaka T. Clinical relevance of (18)F-sodium fluoride positron-emission tomography in noninvasive identification of high-risk plaque in patients with coronary artery disease. Circ Cardiovasc Imaging. 2017;10:e006704.
Joshi NV, Vesey AT, Williams MC, Shah AS, Calvert PA, Craighead FH, Yeoh SE, Wallace W, Salter D, Fletcher AM, van Beek EJ, Flapan AD, Uren NG, Behan MW, Cruden NL, Mills NL, Fox KA, Rudd JH, Dweck MR. Newby DE. 18F-fluoride positron emission tomography for identification of ruptured and high-risk coronary atherosclerotic plaques: a prospective clinical trial. Lancet. 2014;383:705–13.
Raggi P, Prandini N, Ligabue G, Braglia G, Esposito F, Milic J, Malagoli A, Scaglioni R, Besutti G, Beghetto B, Nardini G, Roncaglia E, Mussini C, Guaraldi G. Molecular imaging of vascular calcification with (18)f-sodium-fluoride in patients infected with human immunodeficiency virus. Int J Mol Sci. 2019;20(5).
Guaraldi G, Milic J, Prandini N, Ligabue G, Esposito F, Ciusa G, Malagoli A, Scaglioni R, Besutti G, Beghetto B, Nardini G, Roncaglia E, Mussini C, Raggi P. (18)Fluoride-based molecular imaging of coronary atherosclerosis in HIV infected patients. Atherosclerosis. 2020;297:127–35.
Raggi P, Senior P, Shahbaz S, Kaul P, Hung R, Coulden R, Yeung R, Abele J. (18)F-sodium fluoride imaging of coronary atherosclerosis in ambulatory patients with diabetes mellitus. Arterioscler Thromb Vasc Biol. 2019;39:276–84.
Zanni MV, Toribio M, Robbins GK, Burdo TH, Lu MT, Ishai AE, Feldpausch MN, Martin A, Melbourne K, Triant VA, Suchindran S, Lee H, Hoffmann U, Williams KC, Tawakol A, Grinspoon SK. Effects of antiretroviral therapy on immune function and arterial inflammation in treatment-naive patients with human immunodeficiency virus infection. JAMA Cardiol. 2016;1:474–80.
Li Q, van de Wetering K, Uitto J. Pseudoxanthoma elasticum as a paradigm of heritable ectopic mineralization disorders: pathomechanisms and treatment development. Am J Pathol. 2019;189:216–25.
Germain DP. Pseudoxanthoma elasticum. Orphanet J Rare Dis. 2017;12(1):85.
Kranenburg G, de Jong PA, Mali WP, Attrach M, Visseren FL, Spiering W. Prevalence and severity of arterial calcifications in pseudoxanthoma elasticum (PXE) compared to hospital controls. Novel insights into the vascular phenotype of PXE. Atherosclerosis. 2017;256:7–14.
Zhao J, Kingman J, Sundberg JP, Uitto J, Li Q. Plasma PPi deficiency is the major, but not the exclusive, cause of ectopic mineralization in an Abcc6(−/−) mouse model of PXE. J Invest Dermatol. 2017;137:2336–43.
Moe SM, Reslerova M, Ketteler M, O’neill K, Duan D, Koczman J, Westenfeld R, Jahnen-Dechent W, Chen NX. Role of calcification inhibitors in the pathogenesis of vascular calcification in chronic kidney disease (CKD). Kidney Int. 2005;67:2295–304.
Georgalas I, Tservakis I, Papaconstaninou D, Kardara M, Koutsandrea C, Ladas I. Pseudoxanthoma elasticum, ocular manifestations, complications and treatment. Clin Exp Optom. 2011;94:169–80.
van den Berg JS, Hennekam RC, Cruysberg JR, Steijlen PM, Swart J, Tijmes N, Limburg M. Prevalence of symptomatic intracranial aneurysm and ischaemic stroke in pseudoxanthoma elasticum. Cerebrovasc Dis. 2000;10:315–9.
Kauw F, Kranenburg G, Kappelle LJ, Hendrikse J, Koek HL, Visseren FLJ, Mali WPT, de Jong PA, Spiering W. Cerebral disease in a nationwide Dutch pseudoxanthoma elasticum cohort with a systematic review of the literature. J Neurol Sci. 2017;373:167–72.
Trip MD, Smulders YM, Wegman JJ, Hu X, Boer JM, ten Brink JB, Zwinderman AH, Kastelein JJ, Feskens EJ, Bergen AA. Frequent mutation in the ABCC6 gene (R1141X) is associated with a strong increase in the prevalence of coronary artery disease. Circulation. 2002;106:773–5.
Mitchell GF. Effects of central arterial aging on the structure and function of the peripheral vasculature: implications for end-organ damage. J Appl Physiol (1985). 2008 Nov;105(5):1652–60.
Bartstra JW, de Jong PA, Spiering W. Accelerated peripheral vascular aging in pseudoxanthoma elasticum – proof of concept for arterial calcification-induced cardiovascular disease. Aging (Albany NY). 2019;11:1062–1064.
Kranenburg G, de Jong PA, Bartstra JW, Lagerweij SJ, Lam MG, Ossewaarde-van Norel J, Risseeuw S, van Leeuwen R, Imhof SM, Verhaar HJ, de Vries JJ, Slart RHJA, Luurtsema G, den Harder AM, Visseren FLJ, Mali WP, Spiering W. Etidronate for prevention of ectopic mineralization in patients with pseudoxanthoma elasticum. J Am Coll Cardiol. 2018;71:1117–26.
Schantl AE, Ivarsson ME, Leroux JC. Investigational pharmacological treatments for vascular calcification. Adv Ther. 2018;2:1–16.
Schantl AE, Verhulst A, Neven E, Behets GJ, D’Haese PC, Maillard M, Mordasini D, Phan O, Burnier M, Spaggiari D, Decosterd LA, MacAskill MG, Alcaide-Corral CJ, Tavares AAS, Newby DE, Beindl VC, Maj R, Labarre A, Hegde C, Castagner B, Ivarsson ME, Leroux JC. Inhibition of vascular calcification by inositol phosphates derivatized with ethylene glycol oligomers. Nat Commun. 2020;11:721.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Raggi, P., Garg, R. (2022). Cardiovascular Calcification in Systemic Diseases. In: Henein, M. (eds) Cardiovascular Calcification. Springer, Cham. https://doi.org/10.1007/978-3-030-81515-8_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-81515-8_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-81514-1
Online ISBN: 978-3-030-81515-8
eBook Packages: MedicineMedicine (R0)