
Abstract
Pediatric neurovascular diseases can profoundly affect brain development, growth, and a child’s quality of life. Appropriately managing these conditions in children requires a thorough understanding of their etiologies, diagnoses, treatment options, and prognoses. In this chapter, the authors review pediatric stroke and Moyamoya disease as well as vascular lesions such as AVMs, cavernous malformations, aneurysms, hemangiomas, vein of Galen malformations and dural sinus malformations.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Pediatric stroke
- Moyamoya
- Arteriovenous malformation
- Aneurysm
- Cavernous malformation
- Hemangioma
- Vein of Galen malformation
- Dural sinus malformation
Understanding pediatric neurovascular pathology and the how it differs specifically from the adult disease can inform management and importantly, prognosis. Management, in turn, should rely on data derived from pediatric patients specifically, rather than extrapolated from the adult literature. Unlike in adults, there aren’t well-established guidelines for management. Often associated with other genetic conditions and anomalies, understanding the underlying genetics and pathophysiology of pediatric vascular conditions will significantly advance our treatment strategies [25].
1 Pediatric Stroke
The incidence of stroke has been reported in 2–3 children per 100,000 per year, with intracerebral hemorrhage accounting for a large proportion of these cases [89]. Both vascular lesions and moyamoya disease are important and potential debilitating causes of pediatric stroke, ischemic and hemorrhagic, respectively [120].
1.1 Diagnosis
Computed tomography (CT) is the first imaging modality that should be used when a stroke is suspected, especially in an emergency setting [133]. CT has the capability to show hemorrhage, even from an underlying vascular malformation [133]. CT perfusion can also be used now with lower contrast dosing and radiation than in the past [19]. MRI perfusion and diffusion is more sensitive for diagnosing ischemic stroke, but is more difficult to obtain in children as it may require sedation [133]. In neonates, due to the lack of mature myelination and high water content, MRI sequences need to be adjusted for higher relaxation times and smaller brain structures. An increase in T2 signal and a decrease in T1 signal will lead to a “missing cortex” appearance, in which cortex and unmyelinated white matter are difficult to distinguish [19]. Ultrasound is also commonly used to detect neonatal stroke [19]. In children, DWI sequences can show ischemic areas quickly and reliably while ADC mapping can confirm areas of infarction [19]. ADC maps will normalize within a week as the ischemic area begins to contrast enhance. This contrast enhancement normalizes within several weeks [19]. MRI perfusion techniques such as arterial spin labeling (ASL) can provide additional information in the setting of acute and chronic ischemic stroke, certain ischemic conditions such as Moyamoya disease, as well as vascular malformations [21, 24, 27, 47, 96, 125, 128, 133]. Much like in adults, angiography can also detect pathology such as vascular malformations and aneurysms with great sensitivity, but is also more invasive [133].
1.2 Etiology
There are a number of causes of pediatric stroke which can be broadly categorized into arterial, venous, and hemorrhagic strokes [19] (Table 1.). In this chapter, we will focus on intracranial vascular lesions as well as the etiologies that are most likely to warrant neurosurgical intervention.
2 Pediatric Vascular Lesions
Pediatric vascular lesions often occur in the setting of other rare conditions such as genetic syndromes (such as PHACES—posterior fossa anomalies, hemangiomas of the cervical facial region, arterial cerebrovascular anomalies, cardiac anomalies, eye anomalies and sternal anomalies) and other vasculopathies [25, 76]. In this chapter we will discuss the most common pediatric vascular lesions: Arteriovenous malformations (AVMs), cavernous malformations, Moyamoya disease, and aneurysms. Other pediatric-specific vascular lesions include infantile hemangioma, vein of Galen malformation, and dural sinus malformation [25] (Table 2).
2.1 AVMs
AVMs are direct connections between arteries and veins without intermediate capillary beds [127].
2.1.1 Incidence
Despite their early development, children comprise only 3–19% of AVM patients [72, 91]. AVMs have an incidence of 1 in 100,000 in children, but are responsible for 14–57% of pediatric cerebral hemorrhages [22, 103]. Dural AVMs are even more rare in children, with only 59 reported cases [12]. It is estimated that 12–18% will present with symptoms, and therefore be detected, during childhood [22]. Children have a mean nidus size of 3.4 cm, and Spetzler-Martin grade 2 [72]. Different age groups appear to have different hemorrhage patterns [93]. AVMs can be located anywhere in the brain, though in the children they have been found most commonly in the parietal lobe, followed by the cerebellum, frontal lobe, occipital lobe, thalamus, and other regions [72]. Children have a higher incidence of posterior fossa and basal ganglia malformations than adults [72]. The majority of children have a compact type AVM, with few having diffuse AVMs [72].
2.1.2 Etiology
AVMs are congenital vascular malformations that begin to develop during the third week into the 8th week of gestation when capillary and venous vessels are forming [98]. Feeding vessels occur as a result of exogenous expression of basic fibroblast growth factor and vascular endothelial growth factor (VEGF) that is further stimulated by local ischemia and inflammation [72, 94]. Macrophages contribute to this inflammatory state by secreting cytokines such as TNF-α, IL-6, and VEGF that promote pathological angiogenesis and remodeling [94]. Inflammation and angiogenesis are present on surgically resected AVMs, suggesting that they are dynamic lesions that continue to evolve [94]. Microhemorrhages further stimulate macrophage infiltration, which in and of itself can affect vascular integrity and risk of hemorrhage [94].
Pediatric AVMs are more likely to have multiple foci of arterio-venous shunting, though this may be a manifestation of vascular immaturity, rather than a uniquely pediatric phenomenon [25]. AVMs have been described in the setting of Ras1 mutations [49]. Patients with hereditary hemorrhagic telangiectasia (HHT) have autosomal dominant mutations in growth factor-β signaling genes (ENG, ALK1, ACVRL1 or SMAD4) and often present with intracranial AVMs, in addition to other vascular abnormalities [45, 68, 109]. Children with HHT1 mutations more often present with cerebral AVMs than those with HHT2 mutations [45]. Pediatric AVMs have also been reported as de novo lesions forming during childhood [131]. Some evidence suggests that de novo AVMs may occur as a result of intractable epilepsy, with seizures triggering the release of VEGF [129].
Pediatric dural AVMs are thought to occur as abnormalities in venous sinus development with expansion and remodeling of the posterior sinuses beyond the normal time period [12]. Arteriovenous malformations have also been noted to occur after trauma, though less commonly than in the adult population [10, 100, 130].
2.1.3 Diagnosis
-
(a)
Clinical symptoms: Pediatric AVMs most commonly present with intracerebral hemorrhage (50 to greater than 80%), followed by seizures, or headaches [72]. In fact, ruptured AVMs are the leading cause of intracerebral hemorrhage in children (30–50%) [32, 89]. Children present with hemorrhage (80–85%) more often than adults (50–65%) [72]. In adults AVMs are more likely to be discovered in incidentally whereas in children they are only occasionally discovered incidentally in the setting of other screening or neurologic symptoms [25, 72]. Seizures are the most common presenting symptom in unruptured AVMs, with large AVM size as a risk factor [91]. Hemorrhage may also lead to seizures [91].
In children, AVMs with a small nidus, a periventricular nidus location, and diffuse morphology are at greater risk of rupture [39, 95]. Single draining veins and deep venous drainage are also predictive of hemorrhage [67]. Approximately a third of children with AVMs also have associated aneurysms [11]. Aneurysms within the arterial portion of AVMs may be associated with a higher risk of rupture [11].
Pediatric spinal AVMs are even more rare than intracranial ones, and are typically associated with other hereditary syndromes [63]. They are more commonly located in the thoracic spinal cord, and can present with either congestive or compressive myelopathy, back pain, or as pulsating masses [63].
Dural AVMs consist of three different subtypes, each with a unique set of presenting symptoms:
-
(1)
Infantile dural arteriovenous shunts [12]—High flow, low pressure anomalies often with direct involvement of the meningeal and occipital vessels. They consist of patent sinuses and no venous lakes. They usually present in early childhood with macrocrania, hydrocephalus, seizures, and progressive neurologic deficits.
-
(2)
Adult-type dural arteriovenous shunts [12]—Typically located in the cavernous sinus, adult-type dAVMs present with symptoms of venous hypertension, proptosis, and chemosis. Venous hypertension, if present in the cortex, may also manifest cause intracerebral hemorrhage.
-
(3)
Dural sinus malformations such as Vein of Galen malformations—these will be discussed in a later section.
-
(b)
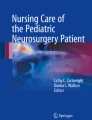
Imaging: Vessel imaging with DSA is the gold standard for diagnosing and visualizing AVMs. This is often obtained after initial imaging with CT or MRI, depending on the initial presentation. Surveillance imaging with MRA or CTA can serve as an adjunct to angiography. Ultrasmall superparamagnetic iron oxide (USPIO) nanoparticles such as ferumoxytol are quickly emerging as valuable contrast agents for visualizing vascular malformations on MRI [46]. One study found that ferumoxytol was superior to gadolinium for visualizing AVMs whereas another demonstrated uptake of ferumoxytol within the vacular wall of the AVM nidus [46] (Fig. 1).
Fig. 1 
Ferumoxytol enhanced MRI (a), KTOF (b), ASL (c) and DSA (d) demonstrating a pediatric arteriovenous malformation

2.1.4 Treatment
For pediatric patients, the main goal of treatment is complete elimination of the AVM since children are thought to have a higher annual bleeding risk (1–3% vs. 2–4% in adults) [54, 72]. While children have a lower risk of initial hemorrhage in untreated AVMs, they have a higher cumulative lifetime risk [35]. The treatment modalities for pediatric AVMs are similar to that in adults, and include surgical resection, radiation therapy, embolization, or a combination of these treatments [76]. Multimodality therapy may improve obliteration rates and decrease hemorrhage rates substantially [32]. Lower grade AVMs have a faster obliteration time (1.8 compared to 6.4 years) and require fewer procedures (2.2 compared to 6.1) for obliteration than higher grade ones [32].
Microsurgical resection can offer complete obliteration (87–94%) and is therefore the preferred mode of treatment, especially for low grade, accessible lesions [32, 44, 72]. Perioperative angiography can allow for higher rates of post-operative obliteration [51, 77]. The rate of complications is typically low, but can include neurologic deficit, stroke, or infection [51]. A laminectomy with microsurgical resection either with or without embolization is also the treatment for spinal AVMs with good outcomes [63].
Alternatively stereotactic radiosurgery (SRS) can be used as primary treatment but is usually reserved for cases that would carry a high operative morbidity such as AVMs with located in deep or eloquent regions, or as adjuvant therapy [32, 35, 65, 72]. SRS can offer a cure rate of 81% with a 5% risk of complications [32]. In a dose response analysis, 16 Gy was the dose needed to obliterate 70% of an AVM and efficacy improved with margin doses of at least 18–22 Gy to the nidus [35, 54, 121]. Reduced doses are used for larger AVMs or those in eloquent regions [65]. It is difficult to predict the precise time for complete obliteration but it can take up to 3 years [32]. The use of SRS for unruptured pediatric AVMs allows for obliteration rates at 3, 5, and 10 years of 29%, 54%, and 72%, respectively [35]. Across all AVMs, even those previously ruptured or treated, obliteration rates with SRS are slightly higher at 45%, 64%, 67%, and 72% at 3, 4, 5, and 10 years, respectively [65]. If patients do not have complete obliteration at interval follow-up, there may be benefit to repeating radiation treatment [65]. Long-term follow-up of pediatric patients who received SRS demonstrated that smaller nidus size, fewer draining veins and higher doses of radiation led to a higher obliteration rate [35, 54, 65]. Patients with a lower Virginia Radiosurgery AVM score which takes into account AVM volume, location, and history of hemorrhage correlated with greater chances of obliteration [22, 35]. Similar to other forms of radiosurgery, large doses, single fraction therapy, and modified AVM scores are associated with higher rates of obliteration [127]. It is unclear whether prior embolization affects the efficacy of radiosurgery but it can help reduce the AVM size, theoretically increasing the cure rate [32, 35, 65]. Potential complications of SRS include post-treatment hemorrhage, edema, hematomas, radiation necrosis, radiation induced white matter changes and radiation induced neoplasms [35, 54, 65, 121, 127]. Patients are at particular risk for hemorrhage during the latency interval prior to obliteration [32, 65]. Lower doses of radiation lower the risk of post-procedure neurologic deficit, but increase the risk of post-radiation hemorrhage [114]. Larger target volumes also lead to a greater risk of hemorrhage [65]. Proton-beam SRS, which minimizes radiation delivery to normal tissue beyond the lesion, has reported obliteration rates from 35–94%.
Pre-operative embolization can be an important adjunct to AVM treatment with the goals of reducing bleeding risk as well as, in some cases, treating cardiac failure and venous hypertension [8, 72]. AVMs are embolized either with n-BCA or Onyx [8]. Whether transarterial or transvenous, endovascular embolization is the primary treatment for dural AVMs, though embolization can often lead to the recruitment of secondary arterial feeders [12]. One group described transvenous onyx embolization to treat pediatric AVMs with unfavorable arterial anatomy [99]. Some of the patients had tranvenous embolization alone whereas the other had a combined transarterial-transvenous approach. The average follow-up was just under 2 years, and all patients were noted to have angiographic cure [99]. Endovascular treatment can also be used exclusively for spinal AVMs [63] (Fig. 2).

Pre-operative (a) and 6-month post-operative (b) DSA showing collateralization of the R MCA territory after EC-IC bypass
Following treatment, angiography (1 year post-treatment for resection, 2 years for stereotactic radiosurgery, and 5 years for diffuse AVMs) is recommended to assess for cure, followed by repeat MRI/MRA every 5 years to check for recurrence [72, 76]. In a retrospective study Morgenstern et al. report that conventional angiography was more sensitive than MRI/MRA since the latter failed to detect any recurrences [105]. They suggest DSA at regularly scheduled intervals to assess for recurrence while minimizing associated risks [105]. CTA can also be used as an adjunct to angiography for post-treatment follow-up. Diffuse-type AVMs, named for their appearance on angiogram, are more difficult to treat and are therefore more likely to recur [72]. Patients with residual nidus can typically undergo additional treatment of their AVM, depending on the lesion’s location [72] (Fig. 3).

Axial CTA demonstaing basilar tip aneurysm
2.1.5 Prognosis
Children have a higher morbidity and mortality related to AVM rupture and have a higher cumulative lifetime risk of rupture than adults [35, 39, 72]. Especially in lesions that have already ruptured, treatment is preferred over observation [103]. Pediatric AVMs with a single draining vein or deep drainage are more likely to rupture, or rerupture [20, 35]. Those that present with hemorrhage or risk factors for hemorrhage also have a worse prognosis [39, 67]. Patients with a higher Glasgow coma score (GCS) on admission were found to have a better functional outcome at discharge and conversely those with a lower baseline modified Rankin score have a worse clinical outcome [67]. One study found that patients with a worse clinical outcome had a higher age at presentation [93]. Higher AVM grade is also associated with a worse clinical outcome [32]. Partial treatment may worsen the natural history of AVMs [20, 32]. Pediatric AVMs with associated aneurysms are at greater risk for rerupture [20]. Pediatric dural AVMs, in particular, are more aggressive than their adult counterparts with a mortality rate of 25% [12]. Some have argued that children with HHT mutations, who are at higher risk for AVM development and have a slightly higher presence of cerebral AVMs (~16% in one screening study compared to 11% in the general population), should undergo routine screening [45].
Children comprise the majority of reported AVM recurrences (69%), perhaps related to the immaturity and plasticity of pediatric vasculature [72]. One study reported recurrence an average recurrence at 33.6 months after surgery [105]. Recurrences have been reported as late as 16 years from treatment and can also present with hemorrhage, seizures or neurologic symptoms [72, 98]. AVM compactness is predictive of recurrence with less compact AVMs having a higher risk of recurrence after surgery [40]. Particularly in young patients, deep venous drainage is associated with a higher rate of recurrence [104]. Multiple theories have been proposed to explain why angiographically “cured” AVMs recur including the “hidden nidus” or “reserve nidus” theory in which angiographically negative areas that are contiguous with the AVM are responsible for regrowth [72]. Alternatively, other authors suggest that immature vasculature makes AVM formation an active process that is maintained throughout childhood and that ceases with AVM maturity [72]. Given the risk of recurrence, even at over a decade after angiographic cure, long-term follow-up with vessel imaging is recommended [98]. At Stanford, serials MRI’s are obtained at 6 months, 1 year, 3 years and every 2 years after surgical intervention until the age of 18. After endovascular therapy or radiosurgery, interval MRI’s are also obtained to demonstrate whether complete obliteration of the nidus has occurred in addition to a post-procedure DSA to confirm obliteration. Serial imaging is obtained at regular intervals during adulthood (Fig. 4).

DSA (a) and 3D DSA (b) demonstrating a basilar tip aneurysm
2.2 Cavernous Malformations
Cerebral cavernous malformations (CCMs) are clusters of vessels without intervening brain tissue [73]. The thin vessel walls lack smooth muscle [73]. These malformations are prone to hemorrhage and hemosiderin is often visible in the surrounding brain [73].
2.2.1 Incidence
Cavernous malformations comprise 2–20% of intracranial vascular malformations in children [59, 73]. In turn, the pediatric population comprises 25% of all patients with cavernous malformations [59, 73]. They tend to present either around 3 years or between 11 and 17 years of age and occur equally in boys and girls [73]. Familial CCMs are more common in Hispanic populations, and about half of Hispanic patients with CCMs have the familial form [73].
CCMs have a reported size of 0.1 to 9 cm but tend to be larger in children (average size of 6.7 cm compared to 2–3 cm in adults) [73]. This may be due to the more cystic nature of pediatric CCMs [73].
Similar to adults, in children the majority of CCMs are supratentorial (80%), more specifically in the cortex or subcortical white matter [73]. In the children they are found in the brainstem more than in adults, most commonly in the pons (14.7%) [73]. CCMs of the basal ganglia, hypothalamus, and spinal cord are all relatively rare in children [73]. Spinal CCMs comprise only 3–16% of pediatric spinal vascular malformations [73].
2.2.2 Etiology
The majority of cavernous malformations occur sporadically (50–80%) though they can also form as an inherited condition [73]. Familial CCM is characterized by the occurrence of CCMs in at least two family members, the presence of multiple CCMs, or a disease-causing mutation in one of the CCM loci. CCM genes have three different loci, deemed CCMI (7q12.2), CCM2 (7p15-p13), and CCM3 (3q25.2-q27) that encode for the K-Rev interaction trapped 1(Krit 1), MGC4607, and programmed cell death 10 (PGCD) proteins, respectively [73]. These proteins are involved in endothelial cell adhesion [73]. Disease-causing mutations at the CCM loci occur according to the two-hit hypothesis [73]. Familial CCM has an autosomal dominant inheritance pattern with incomplete penetrance and variable expressivity [73].
The appearance of cavernous malformations has also been reported after radiation therapy, though it is unclear whether radiation caused them to appear or rather become symptomatic [73].
While CCMs are not intrinsically epileptogenic, they can induce seizures via their effect on the adjacent brain tissue [73]. Feric ions released during microhemorrhages are highly epileptogenic, and overtime the surrounding brain parenchyma can become an epileptogenic focus [73]. Repetitive seizure activity may even cause secondary epileptogenic foci away from the site of the lesion [73].
2.2.3 Diagnosis
-
(a)
Clinical symptoms. Up to 70% of children with cavernous malformations present with seizures [73]. They may also present as intracerebral hemorrhage (~30%), though less commonly than AVMs in this setting [73, 89]. Pediatric patients have a higher rate of bleeding than adults—27.3–78% compared to 8–37%, respectively [73]. Hemorrhage can occur in the brain parenchyma, the ventricles or the subarachnoid space, and symptomatology may be based on lesion location. Patients may have headache, seizures or other neurologic symptoms as a result of hemorrhage [73].
-
(b)
Imaging. The presence of hemorrhage may obscure vascular anatomy and can visualization on imaging somewhat difficult [73]. On non-contrast CT, CCMs are well-circumscribed hyperdense lesions with minimal surrounding mass effect. CCMs may demonstrate blood or calcifications, as well as a capsular rim defining the hemorrhagic portion of the CCM [73]. Pediatric CCMs are more likely to have large hypodense cysts than their adult counterparts [73]. MRI is sensitive and specific for CCMs [73]. On T2-weighted MRI, CCMs demonstrate a characteristic “popcorn” like appearance with mixed signal, surrounded by a ring of decreased signal caused by the presence of hemosiderin [73]. GRE and SWI images are extremely sensitive for detected CCMs and may show enlarged areas of hypointensity [73]. Contrast administration will show whether a DVA is present. CCMs are not well demonstrated on DSA.
2.2.4 Treatment
Treatment of pediatric cavernous malformations must consider the lifetime risk of hemorrhage and potential for the development of seizures [73]. Surgical resection, when feasible, can offer a cure and is generally recommended in the pediatric population setting of acute hemorrhage, focal neurologic deficits, or radiographic enlargement [73]. Resection may be delayed up to a month following hemorrhage to allow edema and symptoms to resolve [73]. CCMs present in eloquent cortex are generally observed and the risk of surgical resection must be weighed carefully against that of recurrent hemorrhage [73]. Epilepsy may be difficult to cure following resection of the CCM depending on the chronicity of seizure activity [73]. Patients with seizures may therefore benefit from early resection of the offending CCMs [73]. Surgery is generally effective either alone or with antiepileptic medication and 50–90% of patients are reported to be seizure-free following surgery [59, 73]. The evidence for surgery is less well established for incidentally discovered asymptomatic lesions, or with multiple CCMs [73]. In particular there may be significant morbidity associated with the resection of brainstem cavernous malformations [2, 84]. Brainstem cavernous malformations also have a higher rate of recurrence after surgical resection in children compared to adults [2].
Laser ablation as an adjunct to surgical resection has allowed for safe resection of CCMs in precarious regions such as the brain stem, thalamus, and spinal cord [73]. It can help minimize bleeding and thermal damage but cannot penetrate blood or calcium [73].
Unlike in AVMs, radiosurgery is generally not recommended for CCMs because it can cause edema and exacerbate symptoms, as well as temporarily increase the risk of hemorrhage up to 22.4% per year [73]. Based on the adult literature, it takes 2–4 years following radiosurgery treatment for the hemorrhage risk to decrease, reducing the frequency of hemorrhage by 4.5–17.3% per year [73]. The rate of permanent deficit and mortality reported from brainstem studies is high at 1.7–22.7% and 12%, respectively.
2.2.5 Prognosis
The morbidity associated with CCMs depends on the location of the lesion. CCMs, located in the basal ganglia, cerebellum or brainstem, are more likely to cause symptoms. The annual risk of hemorrhage is approximately 3% per patient-year (0.25–6.4%) across all patients, including those with familial CCMs which have a higher tendency to bleed [73]. Children have a bleeding incidence of 27, 3–78% compared to 8–37% in the adult population [73]. Brainstem cavernous malformations also have a greater tendency to bleed at 5% per patient per year [73]. Worsened functional status can occur in the setting of recurrent hemorrhage, more so for infratentorial compared to supratentorial lesions [73]. Children with CCMs should undergo MRI surveillance to assess for interval growth of their CCMs, as well as the presence of microhemorrhages [73]. Individuals who have relatives with known CCMs should undergo genetic screening so that they can undergo appropriate surveillance [73].
CCMs grow as a result of repetitive microhemorrhages that cause release of angiogenic factors [73]. Partial resection of CCMs can also lead to a recurrence [73].
Patients with longstanding seizures are at an increased risk for intractable epilepsy and lifelong disability [73]. Microhemorrhages can also lead to the development of epilepsy, therefore repetitive hemorrhages on surveillance imaging may warrant surgical removal [73]. A more extensive resection, including the surrounding hemosiderin ring, and a CCM size < 1 cm are associated with a better chance of being seizure-free after surgery [73]. Patients who do not undergo surgical resection should be monitored clinically for seizures [73].
2.3 Moya Moya
Moyamoya is a disease that involves the progressive occlusion of intracranial blood vessels without evidence of intra-arterial plaques [28].
2.3.1 Incidence
Moyamoya disease is typically diagnosed either between the ages of 5 to 10, or after 40 [43, 52]. The disease appears to present equally in boys and girls but the age of presentation may affect this ratio [17, 28]. It is most prevalent among Asians and is conversely the most common pediatric cerebrovascular disease in Asia [17]. Moyamoya disease accounts for approximately 10% of transient ischemic attacks in the pediatric population [3].
This differs from transient cerebral arteriopathy, which may also present with stroke but is a focal inflammatory process that is limited to several months [132].
2.3.2 Etiology
Similar to in adults, the etiology of pediatric moyamoya disease is unclear [113]. Similar to adults, hypoperfusion and ischemia rather than vaso-occlusion appears to be the predominant mechanism [115]. The process of new blood vessel growth may even precede any overt impairment in blood flow [69]. An anastomosis network of collateral vessels may grow from both the anterior and posterior circulations [15, 16]. However, a number of variants have been identified in association with moya moya including those in the RNF213, ACTA2, BRCC3, GUCY and other genes [26, 31, 60, 61, 83, 92, 120]. In turn, moyamoya has been reported in association with a number of genetic syndromes such as trisomy 21, sickle cell disease, and neurofibromatosis type I [14, 53, 61, 120]. One study found a familial occurrence of 9.4% [17].
Moyamoya syndrome, on the other hand, occurs secondary to another underlying condition such as sickle cell anemia, neurofibromatosis type-1, neurocutaneous syndromes, smooth muscle disorders, Down’s syndrome, thyroid disease and following radiation [9, 41, 101, 112].
2.3.3 Diagnosis
-
(a)
Clinical symptoms: Unlike in adults, children with Moyamoya disease more often present with ischemic symptoms rather than cerebral hemorrhage [48, 52, 82, 113]. The onset of ischemic events can be triggered by hyperventilation in the setting of fever, dehydration, crying or increased activity [52]. In turn, hyperventilation may cause vasoconstriction, which can worsen cerebral perfusion [52]. Cortical ischemia can also secondarily cause epilepsy [52]. Pediatric patients are more likely to have epilepsy than adult patients [28]. Chronic ischemia can cause intellectual disability unrelated to, but often correlated with a history of strokes [52]. Silent microbleeds are more common in the adult moyamoya population and are a predictor of subsequent hemorrhagic stroke [75]. Hypertrophy of the collateral vessels within the basal ganglia can also lead to chorea as a presenting symptom [4]. Although extremely rare, children with moyamoya may also have concurrent intracranial aneurysms, which in turn, may cause mass effect or rupture [90].
Pediatric moyamoya can present with different radiographic findings that vary by developmental stage [62]. Blood flow to the brain is related to metabolic demand, which decreases with age and a reduction in neuronal mass [82]. Also, other comorbidities in the adult population may also affect cerebral blood flow [82]. In the pediatric moyamoya population, cerebral blood flow is decreased across imaging modalities compared to normal controls [82]. In an acetazolamide or CO2 challenge, cerebrovascular reserve is also significantly lower in children with moyamoya [82].
-
(b)
Imaging: Cerebral angiography, due to its invasiveness, is used less liberally in the management of pediatric moyamoya [134]. Less invasive imaging techniques such as PET, single photon emission computed tomography (SPECT), xenon-enhanced CT, dynamic perfusion CT, MR imaging with dynamic susceptibility contrast and with arterial spin labeling have a large role to play in the pediatric population [74]. At Stanford, patients also receive MRI perfusion imaging with an acetazolamide (ACZ) challenge: Patients with Moyamoya demonstrate an exhaustion of cerebrovascular reserve and therefore decreased cerebral blood flow after ACZ administration [124]. Perfusion magnetic resonance imaging is often favored for post-operative follow-up. More specifically, regional time to peak and regional cerebral blood volume measurements can help determine whether sufficient collateralization has occurred [134].
On EEG, children with moyamoya have characteristic high amplitude slow waves as well as the “rebuild-up” phenomenon, which is the reappearance of these waves a minute after hyperventilation [29]. These findings correlate with abnormal perfusion and post-operatively is thought to predict worse clinical outcomes [29].
2.3.4 Treatment
In pediatric moya moya, there is a high risk for complications after surgery [88]. Given the small diameter of pediatric vessels, the most common surgical treatments in children are forms indirect bypass, in which the STA is sutured to the dura, arachnoid, or pia, or alternatively the temporalis muscle is placed on the surface of the brain [30, 71]. Unlike in adults, some authors advocate for indirect procedures as first line treatment [1]. Indirect methods depends on angiogenesis and the gradual revascularization of vulnerable vascular territories, a process which appears to normalize at 6 months after surgery [71]. In patients for whom initial surgical treatment is ineffective (meaning, there are insufficient collaterals and the patient continues to be symptomatic), repeat or a combination of revascularization procedures may be necessary [111]. One study found that encephaloduroarteriosynangiosis (EDAS), in which the STA is sutured to an incised dural margin, allows for greater clinical improvement in children who first present with seizures rather an ischemic symptoms [30]. The authors suggest that children with ischemic symptoms may require even better perfusion than indirect methods allow in order to see clinical benefit [30]. There is also some evidence that EDAS, by decreasing the hemodynamic stress on collateral vessels, may indirectly allow for the disappearance of associated aneurysms and decrease the risk of recurrent hemorrhage from these aneurysms [90].
Other indirect procedures used in children include multiple burr holes, as well as omental-cranial transposition, a technique which can be performed laparoscopically, and used when children have progressive disease despite previous surgical interventions [108]. Children who have undergone omental-cranial transposition show good collateralization on post-operative angiogram and improved perfusion on MRI [108].
Though often limited to older children, those who are able to have a direct bypass of the STA to MCA may have better growth of collaterals and clinical outcomes compared to children who undergo EDAS [97]. Direct bypass may be technically challenging in small children, but also has the advantage of an immediate increase in blood flow [48]. Using a combination of direct and indirect or several indirect procedures can also allow for better revascularization as well as clinical outcomes [38, 48, 70].
Following surgery, repeat imaging and angiography (usually at 12 months) are recommended to assess perfusion and revascularization [76].
2.3.5 Prognosis
Of patients with moya moya, patients that are younger at symptom onset are more likely to have worsening of their disease as well as repeated ischemic strokes [17, 41]. Those with younger symptom onset are especially prone to cognitive impairments in memory and processing [57]. Even with seemingly normal intellectual function, children with moyamoya can have varying levels of cognitive impairments with put through rigorous neuropsychological testing [57]. Children, overall, present with a more severe form of the disease that more often progresses from unilateral to bilateral, though this may reflect some level of detection bias [52, 113]. Cerebral autoregulation may be even more impaired in pediatric patients than in adults, making children at greater risk for perioperative ischemic events [80].
Pediatric patients can also have delayed involvement of the posterior circulation, but show improvement of symptoms with indirect revascularization [81]. Children can present with posterior circulation involvement at less advanced stages of internal carotid artery disease than adults [56]. Those children with posterior circulation involvement are more likely to present with a stroke [56]. Involvement of the posterior circulation has been shown to be a risk factor for difficulty attending in school and maintaining regular employment [42].
Even after direct revascularization procedures, children remain at risk for ischemic stroke or hemorrhage with an incidence of approximately 0.41% per year [43].
2.4 Aneurysms
2.4.1 Incidence
The incidence of aneurysms in the pediatric population is extremely low [33, 34]. Children comprise 0.5–4.6% of the patients with aneurysms, with <1% under the 15 years of age [34]. Pediatric aneurysms may have a male predominance [23, 58, 85]. In the youngest pediatric population, saccular aneurysms are more commonly found in girls compared to fusiform or dissecting aneurysms, which were more prevalent among boys [50]. Some studies have shown a higher proportion of posterior circulation aneurysms in children compared to adults [18, 58]. Pediatric aneurysms occur at the ICA terminus more often than their adult counterparts [58, 122]. Aneurysms in adolescents are primarily in the anterior circulation, with a high prevalence of MCA aneurysms [18, 23, 50, 86]. Small aneurysms occur more often in the anterior circulation [18]. Patients <1 yr-old have an average aneurysm size of ~1.8 cm [50]. Giant aneurysms are found in equal to greater proportions in children than in adults, and more often found in the posterior circulation [50, 85, 123]. In children, saccular aneurysms are less common than giant aneurysms [118]. Saccular aneurysms are more common in the anterior circulation whereas dissecting aneurysms occur more often in the posterior circulation [78]. Children overall have a lower rate of multiple aneurysms than adults (8.7%), with an average of 2.17 aneurysms per patient [18].
2.4.2 Etiology
In the pediatric population, aneurysms form as a result of predisposing congenital conditions or environmental factors such as trauma or infection [33]. Aneurysms are more likely to be associated with comorbid conditions compared to adults, who develop aneurysms in conjunction with modifiable risk factors [18]. Aneurysms do not manifest as commonly in the setting of familial syndromes, suggesting that these develop later on in life [18].
Aneurysms have been associated with a number of genes, including TNFRSF1A, PKD1, and COL3A1 [7, 18]. MAPKs are also elevated in aneurysms [7]. Aneurysms have been associated with a number of genetic conditions such as Marfan’s syndrome, Ehler-Danlos syndrome, Moyamoya disease, Kawasaki’s disease, polycystic kidney disease, fibromuscular hyperplasia, pseudoxanthoma elasticum, sickle cell disease, tuberous sclerosis, multiple scelerosis, and childhood AIDs [5, 7, 37, 66, 85, 90, 106, 110]. Approximately 30% of children with aneurysms also have comorbid conditions [122]. Children with sickle cell are at particular risk for developing multiple intracranial aneurysms, and may do so in a slightly different distribution than the average population [106, 117]. While coarctation of the aorta had previously been associated with an increased risk of intracranial aneurysms, one study found that aneurysms were not present in pediatric patients with coarctation [36]. This suggests that early treatment can help prevent later aneurysm formation [36]. Trauma can cause vessel dissection and infection can weaken vessel wall integrity leading to mycotic aneurysms [50].
The pathophysiology of aneurysm formation in children, similar to adults, is thought to be related to one of two etiologies: (1) hemodynamic and shear stress at particularly vulnerable sites such as vessel bifurcations or (2) a weakening of the vessel wall due to either congenital or environmental factors [18]. The contribution of these factors leading to aneurysm formation may differ slightly between adults and children [18]. Children without associated conditions are found, on histopathologic analysis, to have inflammation within the vessel wall [18]. Further histopathologic and genetic studies will provide further insights into the mechanism of aneurysm formation in children [18].
2.4.3 Diagnosis
-
(a)
Clinical symptoms: In children, 30% aneurysms present with symptoms associated with mass effect on surrounding structures [33, 86]. Approximately 62% of unruptured aneurysms are symptomatic [13]. Forty-six to 80% of pediatric patients with aneurysms present with subarachnoid hemorrhage [18, 50, 58, 85]. Much like in adults, ruptured aneurysms and subarachnoid hemorrhage may cause sudden-onset headache, nausea, vomiting, inconsolable crying, bulging fontanel, Parinaud’s sign, or seizures [33]. Children, on average, present with better Hunt-Hess grades than their adult counterparts [58, 85, 86]. Patients presenting with hemorrhage are, on average, younger and have smaller sized aneurysms [23]. Ruptured aneurysms occurred most commonly in the anterior communicating artery [18]. Approximately 15% of children present with non-specific symptoms, such as headache, without associated subarachnoid hemorrhage [18].
-
(b)
Imaging: Vessel imaging with CTA or MRA can be used to diagnose aneurysms, though DSA remains the gold standard for visualization [33].
2.4.4 Treatment
Treatment options for pediatric aneurysms include surgical, endovascular, and combined treatment approaches [64, 85]. Pediatric patients have a better therapeutic outcome from aneurysm treatment than their adult counterparts [85]. The different etiologies of aneurysm formation in children makes treatment stratification important [78]. Due to a higher risk of recurrence, dissecting aneurysms with SAH and without associated thrombosis require more aggressive management than those with partial thrombosis [78]. In pediatric patients, aneurysms smaller than 7 mm in the anterior circulation have been documented to rupture [122]. The presence of nonsaccular aneurysms in very young children poses particular treatment challenges [50]. One study found that microsurgical clipping led to higher obliteration rates than endovascular treatment [118]. Initially surgical intervention had a particularly high mortality rate in the pediatric population but has since improved to be comparable with adult rates [33]. One study reported in-hospital mortality rates of 6.09% compared to 1.65% after microsurgical clipping compared to endovascular coiling, respectively [6]. There is no difference in post-procedure stroke or hemorrhage, though surgery has higher rates of infection and pulmonary complications [6]. Hospital stays are generally shorter following endovascular treatment compared to open surgery [13].
The majority of aneurysms treated microsurgically are in the anterior circulation [122]. Surgical treatment includes aneurysm neck clipping and, for large complex aneurysms with parent-artery occlusion, cerebral revascularization procedures [64, 123]. Microsurgical clipping has an obliteration rate of 94% with only one case of aneurysm recurrence [119]. Data on long-term bypass patency and efficacy is also encouraging, with 83% aneurysm obliteration and one case of aneurysm recurrence [64]. Potential complications include ischemic stroke and graft occlusion.
Endovascular treatment is often favored in the majority of pediatric aneurysms, in particular for basilar tip aneurysms [13, 78, 85]. This may also be related to parental bias against surgery [119]. Posterior circulation aneurysms are particularly difficult to treat in children, therefore many favor endovascular treatment [34, 122]. Aneurysms treated endovascularly are, on average, larger than those treated microsurgically [122]. The most common endovascular procedures are coiling and stent-assisted coiling [18]. Flow-diversion alone has also been reported [107, 126]. Endovascular treatment leads an obliteration rate of 82% [119]. The durability of endovascular treatment in the pediatric population is not well established and long-term follow-up of these patients is necessary to better understand these outcomes. Durability is especially important when considering the pediatric population. Recurrence rates have been reported between 20–40% following endovascular treatment, and 14–21% require re-treatment of the index aneurysm [13, 119]. De novo aneurysms may also occur following treatment [119]. In addition, endovascular treatment necessitates greater radiation exposure [122]. Despite differences in physiology and anatomy, children tolerate endovascular procedures with a complication rate lower than that of adults [87].
2.4.5 Prognosis
The majority of patients with ruptured and unruptured aneurysms have a favorable clinical outcome [58]. Most do well after treatment with rates of 88% and 86% for good clinical outcomes following microsurgery and endovascular treatment, respectively [18]. Children need serial vessel imaging and long-term follow-up [118]. They require close follow-up for aneurysm recurrence and de novo aneurysm formation, and may require multimodal therapy throughout their lifetimes [64, 118].
The reported rates of vasospasm are much lower than in adults [18]. Children often develop radiographic vasospasm without clinical signs or symptoms of delayed cerebral ischemia, likely due to robust collateral blood flow [18, 102]. The majority of children who developed vasospasm were male. Ruptured aneurysms in the anterior circulation led to vasospasm more often than ruptured aneurysms elsewhere [18]. Open fontanelle windows facilitate serial monitoring for vasospasm using transcranial Doppler ultrasound, however the criteria used in adults may overestimate vasospasm in children [102]. In the pediatric population, nimodipine does not appear to eliminate vasospasm and is associated with significant hypotension [55]. Treatment for vasospasm still generally includes nimodipine, hypertension, and hypervolemia [18]. The majority of children had a good clinical outcome after vasospasm, with clinical outcome correlating with clinical status on initial presentation [18].
2.5 Other Vascular Lesions
2.5.1 Infantile Hemangioma
Infantile hemangiomas are benign vascular tumors that are characterized by a “strawberry red” skin lesion [25]. The cutaneous portion of hemangiomas is often only a small subset and extension into the neuroaxis, though rare, is contiguous with the skin lesion [25]. They occur predominantly in females [25].
Hemangiomas undergo a proliferative phase within the first few weeks after birth, followed by an involutive phase from a year onwards [25]. Medical therapy, either with steroids or, in one report, propranolol, is effective for shrinking the lesion [25].
2.5.2 Vein for Galen Malformation
In the prenatal period, vein of Galen malformations will manifest as loss of brain tissue or calcifications [25]. Later on, children can present as cognitive delay, venous prominence, hydrocephalus, venous sinus stenosis or intracranial venous hypertension [25]. In adults, hemorrhage or severe headache may be the presenting symptoms, though this is extremely rare [25].
According to Raybaud et al., these malformations arise from an arteriovenous fistula between the embryonic median prosencephalic vein of Markowski, a precursor to the vein of Galen, and feeding choroidal and/or quadrigeminal arteries [116]. Vein of Galen malformations can be classified into mural and choroidal subtypes. In the former, there is a direct arterio-venous connection whereas in the latter multiple small arterial vessels form nidus-like connections with the vein, similar to an AVM [25]. They have been associated with Ras1 mutations [49].
Prior to endovascular therapy, the prognosis for vein of Galen malformations was overall poor, and open treatment for vein of Galen malformations had a high morbidity (46.3%) and mortality (37.4%) [25]. In a 2006 series of 216 patients, Pierre Lasjaunias reported a morbidity and mortality of 36% and 10.6%, respectively, with endovascular transarterial embolization [79]. His group also established a grading scheme to inform the timing of intervention: those without significant organ system failure can have embolization deferred to 6 months, those with cardiac failure but without significant brain damage should undergo urgent embolization, and finally those with either multiple organ failure or evidence of parenchymal brain loss should not undergo treatment [79]. The cutoff for treatment has since become more inclusive than the original criteria described by Lasjuanias et al. with elective treatment of asymptomatic patients occurring between 3–5 months of age [25]. Even more favorable outcomes following embolization have since been published in more recent series [25]. One challenge has been endovascular access since these patients are so young at the time of treatment [25].
2.5.3 Dural Sinus Malformation
Dural sinus malformations, one subtype of dural AVMs, are the enlargement of one of the dural venous sinuses, usually the torcular or superior sagittal sinus [25]. Sinus enlargement can occur idiopathically, or as a result of either an arteriovenous fistula or sinus thrombosis [25]. Arteriovenous fistulas form from dural feeders such the middle meningeal or occipital arteries. Dural sinus malformations have been reported in relation to Ras1 mutations [49]. They can have a clinical presentation similar to that of vein of Galen malformations, though hemorrhage is much more common [25].
Given the poor prognosis reported in the literature, parents often elect to terminate these pregnancies [25]. However, the morbidity may be lower than actually reported [25]. Favorable features include only unilateral sinus involvement away from the torcula and superior sagittal sinus as well as the presence of bilateral cavernous sinus drainage and absence of jugular bulb occlusion [12].
References
Abla AA, Gandhoke G, Clark JC, Oppenlander ME, Velat GJ, Zabramski JM, et al. Surgical outcomes for moyamoya angiopathy at barrow neurological institute with comparison of adult indirect encephaloduroarteriosynangiosis bypass, adult direct superficial temporal artery-to-middle cerebral artery bypass, and pediatric bypass: 154 revascularization surgeries in 140 affected hemispheres. Neurosurgery. 2013;73:430–9.
Abla AA, Lekovic GP, Garrett M, Wilson DA, Nakaji P, Bristol R, et al. Cavernous malformations of the brainstem presenting in childhood: surgical experience in 40 patients. Neurosurgery. 2010;67:1589–98 Discussion 1598–1589.
Adil MM, Qureshi AI, Beslow LA, Jordan LC. Transient ischemic attack requiring hospitalization of children in the United States: kids’ inpatient database 2003 to 2009. Stroke. 2014;45:887–8.
Ahn ES, Scott RM, Robertson RL Jr, Smith ER. Chorea in the clinical presentation of moyamoya disease: results of surgical revascularization and a proposed clinicopathological correlation. J Neurosurg Pediatr. 2013;11:313–9.
Ahn JH, Phi JH, Kang HS, Wang KC, Cho BK, Lee JY, et al. A ruptured middle cerebral artery aneurysm in a 13-month-old boy with Kawasaki disease. J Neurosurg Pediatr. 2010;6:150–3.
Alawi A, Edgell RC, Elbabaa SK, Callison RC, Khalili YA, Allam H, et al. Treatment of cerebral aneurysms in children: analysis of the Kids’ Inpatient Database. J Neurosurg Pediatr. 2014;14:23–30.
Albrekkan FM, Bachir S, Jumaa MA, Zaidi SF, Medhkour A. Is there a genetic correlation between multiple sclerosis and cerebral aneurysms? World Neurosurg. 2016.
Altschul D, Paramasivam S, Ortega-Gutierrez S, Fifi JT, Berenstein A. Safety and efficacy using a detachable tip microcatheter in the embolization of pediatric arteriovenous malformations. Childs Nerv Syst. 2014;30:1099–107.
Amans MR, Stout C, Fox C, Narvid J, Hetts SW, Cooke DL, et al. Cerebral arteriopathy associated with Arg179His ACTA2 mutation. BMJ Case Rep 2013. 2013.
Anami H, Aihara Y, Kawashima A, Yamaguchi K, Nagahara A, Okada Y. A case report of a pediatric traumatic aneurysm with arteriovenous (A-V) fistula CASE-BASED UPDATE. Childs Nerv Syst. 2014;30:2003–8.
Anderson RC, McDowell MM, Kellner CP, Appelboom G, Bruce SS, Kotchetkov IS, et al. Arteriovenous malformation-associated aneurysms in the pediatric population. J Neurosurg Pediatr. 2012;9:11–6.
Appaduray SP, King JA, Wray A, Lo P, Maixner W. Pediatric dural arteriovenous malformations. J Neurosurg Pediatr. 2014;14:16–22.
Asaithambi G, Adil MM, Shah KM, Jordan LC, Qureshi AI. Patterns of treatment and associated short-term outcomes of unruptured intracranial aneurysms in children. Childs Nerv Syst. 2014;30:1697–700.
Baird LC, Smith ER, Ichord R, Piccoli DA, Bernard TJ, Spinner NB, et al. moyamoya syndrome associated with Alagille syndrome: outcome after surgical revascularization. J Pediatr. 2015;166:470–3.
Baltsavias G, Khan N, Filipce V, Valavanis A. Selective and superselective angiography of pediatric moyamoya disease angioarchitecture in the posterior circulation. Interv. Neuroradiol. 2014;20:0.
Baltsavias G, Valavanis A, Filipce V, Khan N. Selective and superselective angiography of paediatric moyamoya disease angioarchitecture: the anterior circulation. Interv. Neuroradiol. 2014;20:0.
Bao XY, Duan L, Yang WZ, Li DS, Sun WJ, Zhang ZS, et al. Clinical features, surgical treatment, and long-term outcome in pediatric patients with moyamoya disease in China. Cerebrovasc Dis. 2015;39:75–81.
Beez T, Steiger HJ, Hanggi D. Evolution of management of intracranial aneurysms in children: a systematic review of the modern literature. J Child Neurol. 2016;31:773–83.
Beitzke D, Simbrunner J, Riccabona M. MRI in paediatric hypoxic-ischemic disease, metabolic disorders and malformations-a review. Eur J Radiol. 2008;68:199–213.
Blauwblomme T, Bourgeois M, Meyer P, Puget S, Di Rocco F, Boddaert N, et al. Long-term outcome of 106 consecutive pediatric ruptured brain arteriovenous malformations after combined treatment. Stroke. 2014;45:1664–71.
Blauwblomme T, Lemaitre H, Naggara O, Calmon R, Kossorotoff M, Bourgeois M, et al. Cerebral blood flow improvement after indirect revascularization for pediatric moyamoya disease: a statistical analysis of arterial spin-labeling MRI. AJNR Am J Neuroradiol. 2016;37:706–12.
Borcek AO, Emmez H, Akkan KM, Ocal O, Kurt G, Aykol S, et al. Gamma Knife radiosurgery for arteriovenous malformations in pediatric patients. Childs Nerv Syst. 2014;30:1485–92.
Buis DR, van Ouwerkerk WJ, Takahata H, Vandertop WP. Intracranial aneurysms in children under 1 year of age: a systematic review of the literature. Childs Nerv Syst. 2006;22:1395–409.
Bulder MM, Bokkers RP, Hendrikse J, Kappelle LJ, Braun KP, Klijn CJ. Arterial spin labeling perfusion MRI in children and young adults with previous ischemic stroke and unilateral intracranial arteriopathy. Cerebrovasc Dis. 2014;37:14–21.
Burch EA, Orbach DB. Pediatric central nervous system vascular malformations. Pediatr Radiol. 2015;45(Suppl 3):S463–72.
Cecchi AC, Guo D, Ren Z, Flynn K, Santos-Cortez RL, Leal SM, et al. RNF213 rare variants in an ethnically diverse population with moyamoya disease. Stroke. 2014;45:3200–7.
Chen J, Licht DJ, Smith SE, Agner SC, Mason S, Wang S, et al. Arterial spin labeling perfusion MRI in pediatric arterial ischemic stroke: initial experiences. J Magn Reson Imaging. 2009;29:282–90.
Chen PC, Yang SH, Chien KL, Tsai IJ, Kuo MF. Epidemiology of moyamoya disease in Taiwan: a nationwide population-based study. Stroke. 2014;45:1258–63.
Cho A, Chae JH, Kim HM, Lim BC, Hwang H, Hwang YS, et al. Electroencephalography in pediatric moyamoya disease: reappraisal of clinical value. Childs Nerv Syst. 2014;30:449–59.
Choi JI, Ha SK, Lim DJ, Kim SD. Differential clinical outcomes following encephaloduroarteriosynangiosis in pediatric moyamoya disease presenting with epilepsy or ischemia. Childs Nerv Syst. 2015;31:713–20.
Chong PF, Ogata R, Kobayashi H, Koizumi A, Kira R. Early onset of moyamoya syndrome in a Down syndrome patient with the genetic variant RNF213 p.R4810K. Brain Dev. 2014.
Darsaut TE, Guzman R, Marcellus ML, Edwards, Tian L, Do HM, et al. Management of pediatric intracranial arteriovenous malformations: experience with multimodality therapy. Neurosurgery. 2011;69:540–56 Discussion 556.
Del Santo MA, Cordina SM. Infantile intracranial aneurysm of the superior cerebellar artery. BMJ Case Rep 2016. 2016.
Demartini Z, Jr., Matos LA, Dos Santos ML, Cardoso-Demartini AA. Endovascular therapeutic occlusion of the posterior cerebral artery: an option for ruptured giant aneurysm in a child. Pediatr Neurosurg. 2016.
Ding D, Xu Z, Yen CP, Starke RM, Sheehan JP. Radiosurgery for unruptured cerebral arteriovenous malformations in pediatric patients. Acta Neurochir (Wien). 2015;157:281–91.
Donti A, Spinardi L, Brighenti M, Faccioli L, Leoni C, Fabi M, et al. Frequency of intracranial aneurysms determined by magnetic resonance angiography in children (mean age 16) having operative or endovascular treatment of coarctation of the aorta (mean age 3). Am J Cardiol. 2015;116:630–3.
Dubrovsky T, Curless R, Scott G, Chaneles M, Post M, Altman N, et al. Cerebral aneurysmal arteriopathy in childhood AIDS. Neurology. 1998;51:560–5.
Esposito G, Kronenburg A, Fierstra J, Braun KP, Klijn CJ, van der Zwan A, et al. “STA-MCA bypass with encephalo-duro-myo-synangiosis combined with bifrontal encephalo-duro-periosteal-synangiosis” as a one-staged revascularization strategy for pediatric moyamoya vasculopathy. Childs Nerv Syst. 2015;31:765–72.
Fok EW, Poon WL, Tse KS, Lau HY, Chan CH, Pan NY, et al. Angiographic factors associated with haemorrhagic presentation of brain arteriovenous malformation in a Chinese paediatric population. Hong Kong Med J. 2015;21:401–6.
Frisoli FA, Lang SS, Vossough A, Cahill AM, Heuer GG, Dahmoush HM, et al. Intrarater and interrater reliability of the pediatric arteriovenous malformation compactness score in children. J Neurosurg Pediatr. 2013;11:547–51.
Funaki T, Takahashi JC, Takagi Y, Kikuchi T, Yoshida K, Mitsuhara T, et al. Unstable moyamoya disease: clinical features and impact on perioperative ischemic complications. J Neurosurg. 2015;122:400–7.
Funaki T, Takahashi JC, Takagi Y, Yoshida K, Araki Y, Kikuchi T, et al. Impact of posterior cerebral artery involvement on long-term clinical and social outcome of pediatric moyamoya disease. J Neurosurg Pediatr. 2013;12:626–32.
Funaki T, Takahashi JC, Takagi Y, Yoshida K, Araki Y, Kikuchi T, et al. Incidence of late cerebrovascular events after direct bypass among children with moyamoya disease: a descriptive longitudinal study at a single center. Acta Neurochir (Wien). 2014;156:551–9 Discussion 559.
Gaballah M, Storm PB, Rabinowitz D, Ichord RN, Hurst RW, Krishnamurthy G, et al. Intraoperative cerebral angiography in arteriovenous malformation resection in children: a single institutional experience. J Neurosurg Pediatr. 2014;13:222–8.
Giordano P, Lenato GM, Suppressa P, Lastella P, Dicuonzo F, Chiumarulo L, et al. Hereditary hemorrhagic telangiectasia: arteriovenous malformations in children. J Pediatr. 2013;163(179–186):e171–3.
Gkagkanasiou M, Ploussi A, Gazouli M, Efstathopoulos EP. USPIO-enhanced MRI neuroimaging: a review. J Neuroimaging. 2016;26:161–8.
Goetti R, Warnock G, Kuhn FP, Guggenberger R, O’Gorman R, Buck A, et al. Quantitative cerebral perfusion imaging in children and young adults with moyamoya disease: comparison of arterial spin-labeling-MRI and H(2)[(15)O]-PET. AJNR Am J Neuroradiol. 2014;35:1022–8.
Golby A, Marks M, Thompson R, Steinberg G. Direct and combined revascularization in pediatric moyamoya disease. Neurosurgery. 1999;45:50.
Grillner P, Soderman M, Holmin S, Rodesch G. A spectrum of intracranial vascular high-flow arteriovenous shunts in RASA1 mutations. Childs Nerv Syst. 2015.
Gross BA, Smith ER, Scott RM, Orbach DB. Intracranial aneurysms in the youngest patients: characteristics and treatment challenges. Pediatr Neurosurg. 2015;50:18–25.
Gross BA, Storey A, Orbach DB, Scott RM, Smith ER. Microsurgical treatment of arteriovenous malformations in pediatric patients: the Boston Children’s Hospital experience. J Neurosurg Pediatr. 2015;15:71–7.
Guey S, Tournier-Lasserve E, Herve D, Kossorotoff M. Moyamoya disease and syndromes: from genetics to clinical management. Appl Clin Genet. 2015;8:49–68.
Han C, Yang WZ, Zhang HT, Ye T, Duan L. Clinical characteristics and long-term outcomes of moyamoya syndrome associated with neurofibromatosis type 1. J Clin Neurosci. 2015;22:286–90.
Hanakita S, Koga T, Shin M, Igaki H, Saito N. The long-term outcomes of radiosurgery for arteriovenous malformations in pediatric and adolescent populations. J Neurosurg Pediatr. 2015;16:222–31.
Heffren J, McIntosh AM, Reiter PD. Nimodipine for the prevention of cerebral vasospasm after subarachnoid hemorrhage in 12 children. Pediatr Neurol. 2015;52:356–60.
Hishikawa T, Tokunaga K, Sugiu K, Date I. Assessment of the difference in posterior circulation involvement between pediatric and adult patients with moyamoya disease. J Neurosurg. 2013;119:961–5.
Hsu YH, Kuo MF, Hua MS, Yang CC. Selective neuropsychological impairments and related clinical factors in children with moyamoya disease of the transient ischemic attack type. Childs Nerv Syst. 2014;30:441–7.
Huang J, McGirt MJ, Gailloud P, Tamargo RJ. Intracranial aneurysms in the pediatric population: case series and literature review. Surg Neurol. 2005;63:424–32 Discussion 432-423.
Hugelshofer M, Acciarri N, Sure U, Georgiadis D, Baumgartner RW, Bertalanffy H, et al. Effective surgical treatment of cerebral cavernous malformations: a multicenter study of 79 pediatric patients. J Neurosurg Pediatr. 2011;8:522–5.
Ito A, Fujimura M, Niizuma K, Kanoke A, Sakata H, Morita-Fujimura Y, et al. Enhanced post-ischemic angiogenesis in mice lacking RNF213; a susceptibility gene for moyamoya disease. Brain Res. 2015;1594:310–20.
Janczar S, Fogtman A, Koblowska M, Baranska D, Pastorczak A, Wegner O, et al. Novel severe hemophilia A and moyamoya (SHAM) syndrome caused by Xq28 deletions encompassing F8 and BRCC3 genes. Blood. 2014;123:4002–4.
Jung MY, Kim YO, Yoon W, Joo SP, Woo YJ. Characteristics of brain magnetic resonance images at symptom onset in children with moyamoya disease. Brain Dev. 2015;37:299–306.
Kalani MY, Ahmed AS, Martirosyan NL, Cronk K, Moon K, Albuquerque FC, et al. Surgical and endovascular treatment of pediatric spinal arteriovenous malformations. World Neurosurg. 2012;78:348–54.
Kalani MY, Elhadi AM, Ramey W, Nakaji P, Albuquerque FC, McDougall CG, et al. Revascularization and pediatric aneurysm surgery. J Neurosurg Pediatr. 2014;13:641–6.
Kano H, Kondziolka D, Flickinger JC, Yang HC, Flannery TJ, Awan NR, et al. Stereotactic radiosurgery for arteriovenous malformations, part 2: management of pediatric patients. J Neurosurg Pediatr. 2012;9:1–10.
Kato T, Hattori H, Yorifuji T, Tashiro Y, Nakahata T. Intracranial aneurysms in Ehlers-Danlos syndrome type IV in early childhood. Pediatr Neurol. 2001;25:336–9.
Kellner CP, McDowell MM, Phan MQ, Connolly ES, Lavine SD, Meyers PM, et al. Number and location of draining veins in pediatric arteriovenous malformations: association with hemorrhage. J Neurosurg Pediatr. 2014;14:538–45.
Kim H, Nelson J, Krings T, terBrugge KG, McCulloch CE, Lawton MT, et al. Hemorrhage rates from brain arteriovenous malformation in patients with hereditary hemorrhagic telangiectasia. Stroke. 2015;46:1362–4.
Kim SJ, Son TO, Kim KH, Jeon P, Hyun SH, Lee KH, et al. Neovascularization precedes occlusion in moyamoya disease: angiographic findings in 172 pediatric patients. Eur Neurol. 2014;72:299–305.
Kim SK, Wang KC, Kim IO, Lee DS, Cho BK. Combined encephaloduroarteriosynangiosis and bifrontal encephalogaleo(periosteal)synangiosis in pediatric moyamoya disease. Neurosurgery. 2002;50:88–96.
Kim YI, Phi JH, Paeng JC, Choi H, Kim SK, Lee YS, et al. In vivo evaluation of angiogenic activity and its correlation with efficacy of indirect revascularization surgery in pediatric moyamoya disease. J Nucl Med. 2014;55:1467–72.
Klimo P Jr, Rao G, Brockmeyer D. Pediatric arteriovenous malformations: a 15-year experience with an emphasis on residual and recurrent lesions. Childs Nerv Syst. 2007;23:31–7.
Kosnik-Infinger L, Carroll C, Greiner H, Leach J, Mangano FT. Management of cerebral cavernous malformations in the pediatric population: a literature review and case illustrations. J Neurosurg Sci. 2015;59:283–94.
Kuhn FP, Warnock G, Schweingruber T, Sommerauer M, Buck A, Khan N. Quantitative H2[(15)O]-PET in Pediatric moyamoya Disease: Evaluating Perfusion before and after Cerebral Revascularization. J Stroke Cerebrovasc Dis. 2015;24:965–71.
Kuroda S, Kashiwazaki D, Ishikawa T, Nakayama N, Houkin K. Incidence, locations, and longitudinal course of silent microbleeds in moyamoya disease: a prospective T2*-weighted MRI study. Stroke. 2013;44:516–8.
Ladner TR, Mahdi J, Attia A, Froehler MT, Le TM, Lorinc AN, et al. A multispecialty pediatric neurovascular conference: a model for interdisciplinary management of complex disease. Pediatr Neurol. 2015;52:165–73.
Lang SS, Beslow LA, Bailey RL, Vossough A, Ekstrom J, Heuer GG, et al. Follow-up imaging to detect recurrence of surgically treated pediatric arteriovenous malformations. J Neurosurg Pediatr. 2012;9:497–504.
Lasjaunias P, Wuppalapati S, Alvarez H, Rodesch G, Ozanne A. Intracranial aneurysms in children aged under 15 years: review of 59 consecutive children with 75 aneurysms. Childs Nerv Syst. 2005;21:437–50.
Lasjaunias PL, Chng SM, Sachet M, Alvarez H, Rodesch G, Garcia-Monaco R. Management of vein of galen aneurysmal malformations. Neurosurgery. 2006;59:S3-184–S183-194.
Lee JK, Williams M, Jennings JM, Jamrogowicz JL, Larson AC, Jordan LC, et al. Cerebrovascular autoregulation in pediatric moyamoya disease. Paediatr Anaesth. 2013;23:547–56.
Lee JY, Choi YH, Cheon JE, Paeng JC, Ryu HW, Kim KJ, et al. Delayed posterior circulation insufficiency in pediatric moyamoya disease. J Neurol. 2014;261:2305–13.
Lee M, Zaharchuk G, Guzman R, Achrol A, Bell-Stephens T, Steinberg GK. Quantitative hemodynamic studies in moyamoya disease. Neurosurg Focus. 2009;4:1–7.
Lee MJ, Chen YF, Fan PC, Wang KC, Wang K, Wang J, et al. Mutation genotypes of RNF213 gene from moyamoya patients in Taiwan. J Neurol Sci. 2015;353:161–5.
Li D, Hao SY, Tang J, Xiao XR, Jia GJ, Wu Z, et al. Surgical management of pediatric brainstem cavernous malformations. J Neurosurg Pediatr. 2014;13:484–502.
Liang J, Bao Y, Zhang H, Wrede KH, Zhi X, Li M, et al. The clinical features and treatment of pediatric intracranial aneurysm. Childs Nerv Syst. 2009;25:317–24.
Liang JT, Huo LR, Bao YH, Zhang HQ, Wang ZY, Ling F. Intracranial aneurysms in adolescents. Childs Nerv Syst. 2011;27:1101–7.
Lin N, Smith ER, Scott RM, Orbach DB. Safety of neuroangiography and embolization in children: complication analysis of 697 consecutive procedures in 394 patients. J Neurosurg Pediatr. 2015;16:432–8.
Lin Y, Harris D, Pan IW, Luerssen TG, Lam S. Incidence and predictors of complications after bypass surgery for pediatric patients with moyamoya disease. CNS Oral Present. 2015;62:198.
Liu J, Wang D, Lei C, Xiong Y, Yuan R, Hao Z, et al. Etiology, clinical characteristics and prognosis of spontaneous intracerebral hemorrhage in children: a prospective cohort study in China. J Neurol Sci. 2015;358:367–70.
Liu P, Lv XL, Liu AH, Chen C, Ge HJ, Jin HW, et al. Intracranial aneurysms associated with moyamoya disease in children: clinical features and long-term surgical outcome. World Neurosurg. 2016.
Liu S, Chen HX, Mao Q, You C, Xu JG. Factors associated with seizure occurrence and long-term seizure control in pediatric brain arteriovenous malformation: a retrospective analysis of 89 patients. BMC Neurol. 2015;15:155.
Lo FS, Wang CJ, Wong MC, Lee NC. Moyamoya disease in two patients with Noonan-like syndrome with loose anagen hair. Am J Med Genet A. 2015;167:1285–8.
Lv X, Liu J, Hu X, Li Y. Patient age, hemorrhage patterns, and outcomes of arteriovenous malformation. World Neurosurg. 2015;84:1039–44.
Ma L, Guo Y, Zhao YL, Su H. The role of macrophage in the pathogenesis of brain arteriovenous malformation. Int J Hematol Res. 2015;1:52–6.
Ma L, Huang Z, Chen XL, Ma J, Liu XJ, Wang H, et al. Periventricular location as a risk factor for hemorrhage and severe clinical presentation in pediatric patients with untreated brain arteriovenous malformations. AJNR Am J Neuroradiol. 2015;36:1550–7.
Mamlouk MD, Hess CP. Arterial spin-labeled perfusion for vascular anomalies in the pediatric head and neck. Clin Imaging. 2016;40:1040–6.
Matsushima T, Inoue T, Suzuki S, Fujii K, Fukui M, Hasuo K. Surgical treatment of moyamoya disease in pediatric patients-comparison between the results of indirect and direct revascularization procedures. Neurosurgery. 1992;31:401–5.
McCarthy C, Kaliaperumal C, O’Sullivan M. Recurrence of a paediatric arteriovenous malformation 9 years postcomplete excision: case report and review of literature. BMJ Case Rep 2012. 2012.
Mendes GA, Iosif C, Silveira EP, Waihrich E, Saleme S, Mounayer C. Transvenous embolization in pediatric plexiform arteriovenous malformations. Neurosurgery. 2015.
Miller BA, Bass DI, Chern JJ. Development of a de novo arteriovenous malformation after severe traumatic brain injury. J Neurosurg Pediatr. 2014;14:418–20.
Mizuno Y, Kurokawa T, Numaguchi Y, Goya N. Facial hemangioma with cerebrovascular anomalies and cerebellar hypoplasia. Brain Dev. 1982;4:375–8.
Moftakhar P, Cooke DL, Fullerton HJ, Ko NU, Amans MR, Narvid JA, et al. Extent of collateralization predicting symptomatic cerebral vasospasm among pediatric patients: correlations among angiography, transcranial Doppler ultrasonography, and clinical findings. J Neurosurg Pediatr. 2015;15:282–90.
Monteith SJ, Sheehan JP. Gamma knife surgery for pediatric arteriovenous malformations: a review. Clin Neurosurg. 2011;58:126–32.
Morgan MK, Patel NJ, Simons M, Ritson EA, Heller GZ. Influence of the combination of patient age and deep venous drainage on brain arteriovenous malformation recurrence after surgery. J Neurosurg. 2012;117:934–41.
Morgenstern PF, Hoffman CE, Kocharian G, Singh R, Stieg PE, Souweidane MM. Postoperative imaging for detection of recurrent arteriovenous malformations in children. J Neurosurg Pediatr. 2015;1–7.
Nabavizadeh SA, Vossough A, Ichord RN, Kwiatkowski J, Pukenas BA, Smith MJ, et al. Intracranial aneurysms in sickle cell anemia: clinical and imaging findings. J Neurointerv Surg. 2016;8:434–40.
Navarro R, Brown BL, Beier A, Ranalli N, Aldana P, Hanel RA. Flow diversion for complex intracranial aneurysms in young children. J Neurosurg Pediatr. 2015;15:276–81.
Navarro R, Chao K, Gooderham PA, Bruzoni M, Dutta S, Steinberg GK. Less invasive pedicled omental-cranial transposition in pediatric patients with moyamoya disease and failed prior revascularization. Neurosurgery. 2014;10(Suppl 1):1–14.
Nishida T, Faughnan ME, Krings T, Chakinala M, Gossage JR, Young WL, et al. Brain arteriovenous malformations associated with hereditary hemorrhagic telangiectasia: gene-phenotype correlations. Am J Med Genet A. 2012;158A:2829–34.
O’Shaughnessy BA, Eddleman C, Bendok BR, Parkinson RJ, Awad IA, Batjer HH. Ruptured superior cerebellar artery aneurysm in a child with bilateral fibromusclar hyperplasia of the renal arteries. J Neurosurg Pediatr. 2005;3:338–41.
Pandey P, Steinberg GK. Outcome of repeat revascularization surgery for moyamoya disease after an unsuccessful indirect revascularization. Clinical article. J Neurosurg. 2011;115:328–36.
Phi JH, Wang KC, Lee JY, Kim SK. Moyamoya syndrome: a window of moyamoya disease. J Korean Neurosurg Soc. 2015;57:408–14.
Piao J, Wu W, Yang Z, Yu J. Research progress of moyamoya disease in children. Int J Med Sci. 2015;12:566–75.
Potts MB, Sheth SA, Louie J, Smyth MD, Sneed PK, McDermott MW, et al. Stereotactic radiosurgery at a low marginal dose for the treatment of pediatric arteriovenous malformations: obliteration, complications, and functional outcomes. J Neurosurg Pediatr. 2014;14:1–11.
Rafay MF, Armstrong D, Dirks P, MacGregor DL, deVeber G. Patterns of cerebral ischemia in children with moyamoya. Pediatr Neurol. 2015;52:65–72.
Raybaud C, Strother C, Hald J. Aneurysms of the vein of Galen: embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology. 1989;31:109–28.
Saini S, Speller-Brown B, Wyse E, Meier ER, Carpenter J, Fasano RM, et al. Unruptured intracranial aneurysms in children with sickle cell disease: analysis of 18 aneurysms in 5 patients. Neurosurgery. 2015;76:531–8 Discission 538-539; quiz 539.
Sanai N, Auguste KI, Lawton MT. Microsurgical management of pediatric intracranial aneurysms. Childs Nerv Syst. 2010;26:1319–27.
Sinai N, Quinones-Hinojosa A, Gupta N, Perry V, Sun PP, Wilson CB, et al. Pediatric intracranial aneurysms: durability of treatment following microsurgical and endovascular management J Neurosurg 2 Suppl Pediatr. 2006;82–89.
Smith ER. Structural causes of ischemic and hemorrhagic stroke in children: moyamoya and arteriovenous malformations. Curr Opin Pediatr. 2015;27:706–11.
Smyth MD, Sneed PK, Ciricillo SF, Edwards MS, Wara WM, Larson AC, et al. Stereotactic radiosurgery for pediatric intracranial arteriovenous malformations: the University of California at San Francisco experience. J Neurosurg. 2002;97:48–55.
Stiefel MF, Heuer GG, Basil AK, Weigele JB, Sutton LN, Hurst RW, et al. Endovascular and surgical treatment of ruptured cerebral aneurysms in pediatric patients. Neurosurgery. 2008;63:859–65 Discussion 865-856.
Strickland BA, Attenello F, Russin JJ. Extracranial to intracranial bypass for the treatment of cerebral aneurysms in the pediatric population. J Clin Neurosci. 2016.
Vagal AS, Leach JL, Fernandez-Ulloa M, Zuccarello M. The acetazolamide challenge: techniques and applications in the evaluation of chronic cerebral ischemia. AJNR Am J Neuroradiol. 2009;30:876–84.
van den Tweel XW, Nederveen AJ, Majoie CB, van der Lee JH, Wagener-Schimmel L, van Walderveen MA, et al. Cerebral blood flow measurement in children with sickle cell disease using continuous arterial spin labeling at 3.0-Tesla MRI. Stroke. 2009;40:795–800.
Vargas SA, Diaz C, Herrera DA, Dublin AB. Intracranial aneurysms in children: the role of stenting and flow-diversion. J Neuroimaging. 2016;26:41–5.
Walcott BP, Hattangadi-Gluth JA, Stapleton CJ, Ogilvy CS, Chapman PH, Loeffler JS. Proton beam stereotactic radiosurgery for pediatric cerebral arteriovenous malformations. Neurosurgery. 2014;74:367–73 Discussion 374.
Wang J, Licht DJ. Pediatric perfusion MR imaging using arterial spin labeling. Neuroimaging Clin N Am. 2006;16:149–167, ix.
Wu J, Li Y, Cao Y, Wang S. De novo cerebral arteriovenous malformations: is epileptic seizure a potential trigger? Childs Nerv Syst. 2014;30:1277–81.
Yang Y, Kapasi M, Abdeen N, Dos Santos MP, O’Connor MD. Traumatic carotid cavernous fistula in a pediatric patient. Can J Ophthalmol. 2015;50:318–21.
Yeo JJ, Low SY, Seow WT, Low DC. Pediatric de novo cerebral AVM: report of two cases and review of literature. Childs Nerv Syst. 2015;31:609–14.
Yeon JY, Shin HJ, Seol HJ, Kim JS, Hong SC. Unilateral intracranial arteriopathy in pediatric stroke: course, outcome, and prediction of reversible arteriopathy. Stroke. 2014;45:1173–6.
Yock-Corrales A, Barnett P. The role of imaging studies in evaluation of stroke in children. Pediatr Emerg Care. 2011;27:966–77.
Yun TJ, Cheon JE, Na DG, Kim WS, Kim IO, Chang KH, et al. Childhood moyamoya disease: quantitative evaluation of perfusion MR imaging - correlation with clinical outcome after revascularization surgery. Neuroradiology. 2009;251:216–23.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Quon, J.L., Grant, G. (2021). Pediatric Neurovascular Conditions. In: Agrawal, A., Britz, G. (eds) Pediatric Vascular Neurosurgery. Springer, Cham. https://doi.org/10.1007/978-3-030-74749-7_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-74749-7_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-74748-0
Online ISBN: 978-3-030-74749-7
eBook Packages: MedicineMedicine (R0)