
Abstract
The identification of microscopic toxicologic changes in eyes is influenced by many factors. Important factors include in vivo procedures, such as route of administration to the eye, and procedures involved in preparation of the microscopic ocular sections. A wide variety of toxins may affect all parts of the eye and ocular adnexa and must be differentiated from iatrogenic and spontaneous changes. Both toxic and spontaneous changes may occur in certain species of animals, certain strains of animals, or at certain ages; therefore, a good understanding of potential changes, as well as knowledge of the normal ocular anatomy, physiology, and function, is essential. This chapter focuses on the histologic preparation of ocular tissues and findings involving the anterior segment, uvea, and ocular adnexa and is followed by a chapter focusing on the lens and posterior segment of the eye.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
5.1 Introduction
The detection and identification of microscopic toxicologic changes is influenced by many factors. For example, one needs to have an understanding of comparative ocular anatomy in order to differentiate variations in normal anatomical structures of different species from treatment-related changes in these structures. Smith et al. [1] and Prince [2] provide a review of the ocular anatomy of the mouse and rabbit, respectively, and others provide broader discussions of comparative ocular anatomy [3–5].
The detection of microscopic findings requires an awareness of clinical ocular findings observed via direct ophthalmoscopy, indirect ophthalmoscopy, and often slit lamp biomicroscopy [6–8]. These methods, along with additional techniques used in ophthalmology, can detect the exact location of findings and thus challenge the pathologist to provide a microscopic correlate. Detection of microscopic changes requires preparation of good quality histologic sections that have proper orientation and minimal tissue artifacts. Ocular findings need to be accurately classified as spontaneous, iatrogenic, or treatment-related and labeled with the proper diagnostic term.
Toxicologic pathologic evaluation begins with a review of the protocol. In addition to typical features of a study protocol, procedures used in the collection, fixation, trimming, processing, embedding, and ocular section preparation should be reviewed [9]. With oral administration, the globe will most likely be evaluated in a standard manner. However, direct dosing to the eye may result in ocular changes in specific locations that will require customized sampling of ocular tissue. Examples include localized superficial findings in the cornea following topical administration of a drug and findings in the vitreous or retina following intravitreal injections. Pathology laboratory personnel should be familiar with all ocular procedures used in studies and if not, should conduct a methods development study prior to the toxicity study to ensure that good quality sections will be prepared.
Development of the eye and ocular teratogenesis have been discussed in the literature including several comprehensive reviews [10–16]. Although ocular development is similar for humans and animals, the timing of events varies among humans and animals [12, 17]. Ocular findings occurring in neonatal or young animals are often characterized as developmental and are often identified during prestudy examinations. When using mice, especially genetically engineered mice, it is advantageous to know the anticipated effects on the eye of the induced genetic mutation [1].
5.2 Preparation for Microscopic Ocular Examination
Toxicologic ophthalmic pathology involves the detection and accurate characterization of macroscopic and microscopic toxicologic ocular findings. Macroscopic findings are often detected by use of the clinical ophthalmic examination; therefore, clinical ocular findings should be available at the time of necropsy, trimming, and microscopic examination. Microscopic correlates to ophthalmic findings should be determined, when possible.
The detection of ocular findings is not possible unless the histologic ocular sections are of good quality with the proper orientation and minimal tissue artifacts [9, 18, 19]. Obtaining ocular sections of good quality requires good communication between the pathologist and those involved in the clinical examination, postmortem procedures, and preparation of sections. Pathology laboratory personnel handling ocular tissue need to be familiar with all procedures (i.e., enucleation, fixation, trimming, processing, embedding, sectioning, and staining) required for good section quality. In general, if fewer individuals are involved in the process (enucleation through section preparation), there are fewer artifacts.
Enucleation begins with a review of the ophthalmic findings which may be in the form of descriptions, diagrams, or images [20]. All globes should be enucleated as soon as possible after death (i.e., the beginning of the postmortem examination) to minimize postmortem autolysis, especially of the retina [18, 21]. Globes and the optic nerve should always be handled as gently as possible with minimal tension to avoid artifacts, such as retinal detachment, myelin in the subretinal space, and artifacts (i.e., spherical to irregularly shaped hyaline bodies) in the optic nerve [22–24]. At least 0.5 cm of the retrobulbar optic nerve should remain attached to the globe so that a cross section of the optic nerve can be prepared. For most studies, the extraocular muscles, orbital glands, and other orbital tissues should be carefully removed from around the globe prior to fixation for the following reasons: (1) allows for a gross examination of the globe, (2) exposes natural landmarks used for trimming (e.g., long posterior ciliary artery), and (3) facilitates fixation of intraocular structures (e.g., retina). For rodents, removal of the harderian gland will allow visualization and collection of the retrobulbar optic nerve for cross sectioning. If needed, extraocular tissues may be fixed separately and processed. If globes are being collected for an ocular irritation study, then bulbar conjunctiva should be retained with the globe. For sub-Tenon’s depot injections, extraocular tissue may need to be left intact to evaluate the injection site.
Prior to fixation, globes (especially those of albino rodents) may need to be marked with tattoo ink, an indelible dye, or a suture as a landmark for trimming. By convention, the mark is usually placed at the 12 o’clock position [1]. In addition, both globes should be identified as right (oculus dexter [OD]) or left (oculus sinister [OS]) at the time of enucleation, and the identification should be maintained throughout the process of section preparation.
The purpose of fixation is to preserve ocular tissues with minimal artifacts. There are many different fixatives used for fixation of the eye, but none are ideal. All fixatives have advantages and disadvantages which are important to understand in order to choose the most appropriate one for a given situation. Since there is variability in results among histotechnology laboratories using the same fixative, a pilot study is necessary to develop the method for each fixative in each laboratory to ensure that good quality ocular sections are obtained. The appearance of the ocular tissue is partially determined by the ingredients in the fixative used [25–27]. Depending on the fixative, immersion fixation (i.e., fixatives containing glacial acetic acid) should be sufficient for obtaining good sections of globes. In addition to immersion, optimal fixation with glutaraldehyde-based fixatives requires an intraocular injection of the fixative or the creation of a small window through which the fixative can diffuse. Systemic perfusion of the head is not necessary unless ocular tissues are going to be processed for plastic embedding and examination of sections at a thickness of 1 μm or examined by transmission electron microscopy. Systemic perfusion may cause inconsistent results or artifacts, especially if the perfusion pressure is too high (e.g., spaces beneath the retinal pigment epithelium) or if the fixative is too cold.
Fixatives containing glutaraldehyde (1–6%, buffered with monobasic and dibasic sodium phosphate) have proven to be an acceptable fixative for rodent globes (24-h immersion) and nonrodent globes (injection or window techniques followed by 48-h immersion). After initial fixation, globes are then stored in 10% neutral buffered formalin (NBF) [28, 29]. Glutaraldehyde is often combined with 10% NBF for light microscopy and is combined with paraformaldehyde for transmission electron microscopy [30, 31]. Generally, advantages of glutaraldehyde fixation of globes include (1) no vacuolation of the corneal epithelium and endothelium, (2) visible outlines of lenticular fibers, and (3) visible outlines of photoreceptor outer segments [28]. Possible artifacts of glutaraldehyde fixation include (1) a few spaces in the corneal stroma, (2) lenticular cracks, (3) distorted shape of cornea and lens of rodents due to altered tissue osmolarity, (4) cellular vacuolation in the inner nuclear layer, and (5) vacuolation in the inner and outer segments [28].
Other fixatives that are commonly used (i.e., Davidson’s, modified Davidson’s, Bouin’s, and Zenker’s solutions) contain glacial acetic acid and appear to penetrate relatively quickly for good fixation, especially the retina [1, 25, 32]. Glacial acetic acid provides good preservation of nuclei and helps prevent hardening of tissues (especially the lens) but causes cells to swell which may result in artifacts. Davidson’s or a modified Davidson’s solution contains a combination of buffered formalin, ethanol, glacial acetic acid, and distilled water. These fixatives are frequently used for fixation of rodent globes [33, 34]. Fixation times vary depending on the size of the globe and include 6–24 h for rodent globes and 24–48 h for rabbit, monkey, or dog. Prolonged exposure to glacial acetic acid should be avoided because of artifacts. After initial fixation, the globes should be rinsed and placed in 10% NBF for at least 24 h before trimming. The main advantage of these fixatives is the general good fixation of rodent globes and retinas of all species. In addition, tissues fixed in Davidson’s fixative may also be used for immunohistochemistry. The main disadvantages of Davidson’s solution include an opaque gross appearance of the globe and the occurrence of artifacts after prolonged fixation which include (1) corneal epithelial vacuolation, (2) clefts in the corneal stroma, (3) corneal endothelial cell vacuolation, (4) shattering of the lens, (5) liquefaction and globule formation in the lens of monkeys resembling cataract, (6) lens swelling which may result in rupture of the lens capsule in rodents, and (7) indistinct appearance of rods and cones. Tissues fixed with Davidson’s are not suitable for electron microscopy.
Bouin’s solution and Zenker’s solution are fixatives that have been widely used in the past for fixation of the retina but have been largely replaced by other fixatives because of disposal issues [25–27]. Bouin’s solution contains picric acid and is also potentially explosive in the dried state. Zenker’s solution, as well as some other fixatives, contains mercuric chloride [22, 25, 26, 28, 35].
Regardless of the type of fixative used, the ratio of the volume of the globe to the fixative should be at least one part globe to at least ten parts fixative. Gauze may be placed on top of the globe to ensure it stays submerged, and wide-mouth containers should be used. The container should be at least a couple of centimeters wider than the globe to allow for complete exposure of the globe to the fixative.
As mentioned, immersion fixation of nonrodent globes with glutaraldehyde needs to be enhanced by increasing the exposure of internal ocular structures, especially the retina. This may be accomplished by injecting fixative into the vitreous chamber or creating a small window in the globe after some initial fixation. Intravitreal injection of a fixative is accomplished by the insertion of a small (25–27 ga) needle into the vitreous chamber through the sclera at a point just posterior to equator (thickest part of globe and parallel to the limbus). The needle should be directed posteriorly to avoid contacting the lens, and the injection should not be in the desired plane of section for microscopic examination. For most species, the needle should be inserted (with syringe attached) along the nasal or temporal aspect of the plane of the long posterior ciliary artery. For nonhuman primates, the point of insertion of the needle is 90° superior or inferior to the long posterior ciliary artery. The fixative should be slowly injected into the vitreous body until the globe feels turgid (volumes of 0.15–0.3 ml are common). If done correctly, compression artifacts are usually not observed. After injecting the fixative, the globe should be submerged in the same fixative.
A globe should not be incised prior to fixation because it causes the globe to be distorted, but a small (∼5 mm) window may be created in a globe that has undergone immersion fixation for 5–30 min without distortion. As with the injection technique, the window should not be located in the desired plane of section. To make a window, the globe should be positioned with the cornea down, and the position of the long posterior ciliary artery should be noted. A cut with a sharp tissue slicer blade through the sclera is made to create a small (∼5 mm diameter) window along a peripheral parasagittal plane. This window will usually be at the nasal or temporal position for nonprimates and a superior or inferior position for primates.
After initial fixation, the globe may be transferred into 10% NBF to ensure that it will be firm for trimming. At the time of trimming, the globe may be examined for any abnormalities or for the location of medical devices [36]. Findings observed should be recorded along with any other comments pertaining to the preparation of the ocular tissue. The grossing process may be enhanced by transillumination.
Trimming begins by being aware of clinical ocular findings. Generally, standard sections of the globe will be adequate for evaluation, but trimming may need to be modified depending on ophthalmic findings or ocular conditions (e.g., injection site or globe with an implanted medical device). The proper standard plane of section should be one that is uniform for all globes of a certain species, unless otherwise specified [18]. For nonprimates, the uniform section should be a vertical midsagittal plane that is through the pupil and includes the optic disc [20]. This will result in a superior portion and an inferior portion. For canine globes, the tapetum lucidum will be in the superior portion, and for globes of rabbits, the inferior aspect of the globe is larger (optic nerve to limbus) than the superior aspect. For primates, the standard ocular section for systemic studies should include the macula. This area contains a central depression, the fovea, but it is generally not necessary for this structure to be present in the histologic section. By trimming along this plane of section, the temporal aspect (optic nerve to limbus) of the primate globe is longer than the nasal aspect. Primate globes may be trimmed vertically in intravitreal studies, but it would be necessary to obtain multiple sections in order to evaluate the macula and the optic disc. For all species, a cross section of retrobulbar optic nerve should be obtained for examination.
Generally, globes are trimmed in a posterior-anterior direction to ensure that the optic nerve will be in the section. When trimming, the globe should be placed on a block of paraffin or other trimming board. The long posterior ciliary artery extending from the optic nerve along a horizontal plane toward the temporal limbus and medial limbus should be located. The blade (i.e., long tissue slicer blade or other very sharp blade, such as a disposable microtome blade) is positioned perpendicular to the posterior ciliary artery for vertical planes of section and parallel for horizontal planes of section. The end of the blade initiates the cut which is smooth, downward, and forward cutting into the globe. A sawing motion should be avoided to avoid artifacts (e.g., lens luxation and retinal detachment). The blade will meet some resistance at the lens, so put hands on each side of the blade and push down through the lens and cornea. The vitreous body should stay as a gel and helps to keep the lens and retina in place. Some histotechnologists advocate the removal of the vitreous to avoid retinal detachment, especially for primate eyes, but this is not necessary and will make the vitreous unavailable for examination. The trimmed globe should be put into a megacassette because standard cassettes are too thin except for rodent globes. Trimming globes thinly in order to fit into a standard cassette results in retinal detachment and other artifacts. A window should be created in the upper domed portion of the globe in the cassette to prevent the formation of bubbles during embedding. The window should not be any larger than necessary to avoid hitting the lens, if possible, but large enough so the trimmed globe will not project above the edges of the megacassette. For trimming a globe that has a window created at the time of fixation, the window can be covered with a finger to “seal” it. Since a window already exists in the globe, additional trimming may not be needed.
An alternative method for trimming globes of animals is one that is similar to a method used for human globes [21, 37]. This method avoids hitting the lens but requires a lot more facing of the paraffin block and is generally not used for safety studies.
Globes of rodents need minor or no trimming. For globes of rats, a parasagittal cut is made through the globe removing a small (1–2 mm thick) calotte. This will leave the optic nerve, lens, and most of the cornea in the larger section. The globes of mice are small enough that they do not need to be trimmed and can be embedded whole.
The globes of albino rodents are small and diffusely white which may make it difficult to get uniform sections, especially when fixed in certain fixatives (i.e., Davidson’s fixative). Applying a dot of pasty tattoo ink or tissue dye to the superior aspect of the globe at the time of enucleation may be helpful. This mark should be along a superior-inferior midline plane. With a uniform plane of section, measurements of certain ocular structures, such as the outer nuclear layer of the sensory retina (i.e., nuclei of the rods and cones) may be obtained, thus creating a “spider graph” [38].
Generally, globes of animals in toxicity studies are processed along with nonocular tissues, but separate processors with separate processing procedures may be used [18, 21, 32, 37, 39]. To aid in sectioning the lens, cedarwood oil may be used in the processor prior to xylene, and low-melting-point paraffins with plastic polymers may be used for processing and embedding.
Embedding is an important phase in the process that can contribute to artifacts [18]. The window created at fixation or trimming is useful in removing air bubbles and for making sure that the lens is in complete contact with the bottom of the embedding mold. Not having a complete section of lens may be a problem especially for larger globes with relatively large lenses (e.g., dog).
Sectioning of the blocks may be troublesome for the histotechnologist [18, 32, 37]. Techniques may vary depending upon the species of animal, but the main problems consist of not getting good sections of the lens [39]. Removing the lens and embedding it separately should be avoided. Chilling the paraffin blocks gradually from room temperature to freezer temperature helps to avoid cracking and crumbling, especially of the lens. Softening of the lens by turning the block face down on gauze located on ice and applying 10% ammonium hydroxide, glycerin, or soap to the block may help improve section quality [39–41]. Another troublesome issue is getting sections of optic disc or optic nerve of albino rodents. For these animals, a dye or tattoo ink may be applied to the optic nerve at the time of enucleation, and candling the block to observe the location of the optic nerve may be another option.
After the sections are obtained from the block, ribbons are placed on a water bath. The water bath should be cleaned of tissue debris between ribbons to avoid extraneous tissue from getting into ocular sections. Generally, low-temperature paraffin is used, so the temperature of the water bath does not need to be excessively hot. Heat causes the globe to expand, but overexpansion causes the tissue not to adhere to the glass slides (e.g., glaucomatous globes) and causes artifacts (e.g., spaces within ocular tissues). The temperature of the water bath is generally 2° above the melting point of the paraffin. To help in the adherence of the ocular tissue to the glass slide, poly-L-lysine, extra gelatin, or other material may be placed in the water bath [37]. Some histotechnologists use two water baths. One is at room temperature for initial contact of the ribbon with the water to remove wrinkles and the second at a higher temperature to allow for expansion. After the sections are adhered to the glass slides, they are slowly dried in a horizontal position in a warm (60°) oven overnight. Generally, for most toxicity studies, the ocular sections are stained with hematoxylin and eosin, but specific ocular structures may be enhanced with special stains or immunohistochemistry [18, 20]. For example, periodic acid-Schiff stain is used to stain basement membranes (e.g., Descemet’s membrane, lenticular capsule, basal lamina of ciliary epithelium) and the mucin in conjunctival goblet cells.
5.3 Descriptive Terminology
Good quality ocular sections should help in the identification of ocular changes. Terms used to describe gross and microscopic ocular changes should be specific as to the location within the eye and specific as to the type of ocular change. By knowing the plane of section, terms, such as anterior, posterior, superior, inferior, temporal, nasal, inner, outer, central, and peripheral, may be used along with the specific structure of the eye that has a finding. The type of ocular finding should also be as specific as possible. For example, a gross loss of transparency of the lens should be referred to as a lenticular opacity, since the finding may be reversible (i.e., cold cataract) or irreversible (i.e., cataract) [42–44]. Microscopically, features, such as liquefaction and globule formation in the lenticular cortex, are considered to represent lenticular cortical degeneration, and the combination of clinical and microscopic findings indicates that the lenticular change is a permanent change (i.e., cataract). In addition, since the retina is composed of many different types of cells, the use of retinal degeneration may be too vague. For one study, retinal degeneration might represent loss of ganglion cells, and in another study, retinal degeneration might represent changes associated with photoreceptors. Use of precise diagnostic terms for ocular findings helps to eliminate confusion.
5.4 Extraocular Tissues (Ocular Adnexa)
The extraocular tissues include the eyelids and the contents of the orbit. The orbit is a bony fossa that contains the globe, optic nerve, extraocular muscles, orbital fascia, adipose tissue, various types of glands, and the third eyelid, in some species [2–4, 7, 32, 45].
5.4.1 Eyelids
Each eyelid is composed of an outer cutaneous surface and an inner surface lined by palpebral conjunctiva. Mucin from goblet cells in the conjunctiva forms the inner layer of the tear film. At the palpebral margin are the sebaceous meibomian glands. Secretions of the meibomian glands form the outer layer of the tear film.
Eyelid alterations may be spontaneous or due to toxicity. Spontaneous alterations may be congenital, inflammatory, hyperplastic, or neoplastic. For example, entropion (i.e., inward folding of the eyelids) can occur as congenital defects in rabbits and as a sequel to inflammation in any animal. Entropion can damage the conjunctiva and cornea with affected rabbits exhibiting blepharospasm, conjunctivitis, epiphora, and corneal ulceration. Another example of a spontaneous finding is the incomplete formation of the palpebral fissure described in 4–5-week-old Swiss mice Crl:CD1(ICR)BR [46].
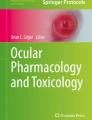
Inflammation of the eyelid may involve several structures (e.g., blepharitis in Göttingen minipig) or just specific structures, such as the meibomian gland (i.e., meibomian adenitis) [47]. Inflammation of the meibomian glands includes the presence of lymphocytes, neutrophils, and macrophages and may result in glandular dysfunction (i.e., decreased secretion). Meibomian gland dysfunction can lead to a decreased tear film and keratoconjunctivitis sicca (KCS) (i.e., dry eye) [48]. Similar effects may be expected in humans. Inflammation of the eyelids also includes spontaneous, nonspecific dermal mononuclear cell infiltrates (Fig. 5.1).

The upper eyelid from a control rabbit has diffuse infiltrates of lymphocytes and plasma cells in the dermis as a spontaneous change. H&E. 5× objective
Neoplasms may arise from any of the structures in the eyelid, including the skin. Neoplasms reported in rats include squamous papilloma, squamous cell carcinoma, schwannoma, melanoma, granular cell tumor, basal cell tumor, sebaceous adenoma, malignant fibrous histiocytoma, and sarcoma [49].
Several drugs and chemicals can cause alterations involving the eyelids [50]. Edema of the eyelid can occur from systemic administration of iminodipropionitrile to monkeys.
Polychlorinated biphenyl (PCB) poisoning produces a chloracne condition in humans and affects sebaceous glands including the meibomian gland [51]. In monkeys, PCBs and similar compounds cause swelling of eyelids with meibomian gland hypersecretion and abnormal pigmentation of the conjunctiva. Microscopically, meibomian glands often contain keratin cysts with atrophy of the glands, increased numbers of layers of epithelial cells in the ducts, dilated ducts, and increased mitotic figures in basal cells [52–56].
Chronic application of topical epinephrine [57] to rabbit eyes results in a syndrome that has been called meibomian gland dysfunction. Features include plugging of the orifice of glands, microcysts, and opacification and enlargement of the gland. Ducts have increased stratification and keratinization, while the lumen is dilated with retention of desquamated epithelium.
Retinoids have been recognized to have effects on the meibomian gland. Isotretinoin (13-cis-retinoic acid), a therapy for acne vulgaris and keratinizing dermatoses, has been associated with side effects of blepharoconjunctivitis in 20–45% of human patients [58]. Systemic treatment of adult New Zealand white rabbits produces mild conjunctival erythema and crusting of the eyelid margins [58, 59]. These correlate microscopically with thickened meibomian gland ducts and ductal epithelium. The amount of acinar tissue is decreased due to degeneration and necrosis of acinar cells and accompanied by periacinar fibrosis. Additional changes include accentuation of the basal cells and decreases in basaloid cells lining acini with a lack of inflammation [58, 59].
Toxaphene administered orally to cynomolgus monkeys has been reported to produce local effects in the meibomian gland. Affected monkeys had inflammation, enlargement, or both, of the meibomian gland due to impacted diverticula in both the upper and lower lids causing accumulations of glandular secretions [60].
Systemic administration of small molecule inhibitors of epidermal growth factor receptor (EGFR) may produce granulomatous inflammation of the meibomian gland. This is suspected to be a pharmacologic effect due to a failure to secrete glandular content and continued production leading to subsequent glandular rupture. Release of glandular lipids into the surrounding tissue causes a granulomatous response.
Prostaglandin analogs (latanoprost, travoprost, and bimatoprost) are topically applied drugs that decrease intraocular pressure. In addition, there is lengthening of eyelashes (hypertrichosis) [61–64].
5.4.2 Extraocular Muscles
The extraocular muscles consist of six muscles (four rectus muscles and two oblique muscles) and, in species such as the dog and rabbit, the retractor bulbi [4, 7, 65]. The dorsal, ventral, and medial rectus muscles and the ventral oblique muscle are innervated by the oculomotor (III) nerve. The lateral rectus and retractor bulbi muscles are innervated by the abducens (VI) nerve. The dorsal oblique muscle is innervated by the trochlear (IV) nerve.
Extraocular muscles may be affected by light exposure and retrobulbar injections [66]. After 24 h of light exposure, extraocular muscles of rats were infiltrated with numerous neutrophils and mononuclear cells with myofiber degeneration. With time, neutrophilic infiltrates decreased and mononuclear cells persisted. Myoblasts formed to replace fragmented myofibers. Extraocular muscles may develop areas of inflammation (e.g., granulomas) associated with periorbital or retrobulbar injections and should be examined following these injections (Fig. 5.2).

Granuloma adjacent to an extraocular muscle in a rabbit given an injection into the periorbital soft tissues. Granuloma consists of numerous large, foamy, and eosinophilic macrophages, some of which are multinucleate. H&E. 5× objective
5.4.3 Orbital Glands
Except for the rodent’s harderian gland, most of the glands of the lacrimal system are not examined in routine toxicology studies but will often be examined in ocular toxicology studies. Since lacrimal glands and lacrimal structures may vary among different species, such as some species having the gland of the third eyelid and dogs having orbital glands that are not lacrimal glands (i.e., zygomatic salivary gland in the dog), it is important to be aware of these differences so that personnel involved in the collection of lacrimal structures can locate the intended structures [2–4, 7, 67–71].
Rodents have intraorbital and extraorbital lacrimal glands and a harderian gland [7, 68]. Cytomegaly and karyomegaly, along with nuclear pseudoinclusions, are features identified in the glands with males having a greater degree of these features than females. These differences may be explained by differences in gene expression in males versus females that may be associated with sex steroids [72].
Harderian glands are tubuloalveolar, merocrine glands without an intraglandular duct system [69, 70]. Harderian glands are usually larger in females than males and lymphoid cells may be present. The lipid-containing secretion contains porphyrins, mainly protoporphyrin IX, which may be a potential photosensitizer when activated by ultraviolet and blue components of daylight. The lumina may contain brown accretions which accumulate with age and may be associated with atrophy, granulomatous inflammation, and sclerosis. The amount of porphyrin in the gland is affected by castration, administration of androgens or estrogens, and nutritional deficiencies of riboflavin or vitamin A [69, 73, 74].
In the rabbit, the Harder’s gland may be referred to as a harderian gland but is different in gross and microscopic appearance than the harderian gland of rodents and does not produce porphyrins. The Harder’s gland is grossly composed of a white lobe and a pink lobe. The white lobe has smaller lumina and the cytoplasm contains larger lipid droplets. The pink lobe has larger lumina and stains more intensely with hematoxylin and eosin stain (Fig. 5.3). Small foci of lymphocytes are found sporadically in the lacrimal and Harder’s glands in rabbits [68].

Normal rabbit Harder’s gland. The adjacent pink (left) and white (right) lobes are readily distinguishable based on morphology. H&E. 10× objective
The main effect resulting from alterations in lacrimal glands is increased secretion (i.e., dacryorrhea) or decreased secretion leading to KCS. The morphologic changes that may be observed in lacrimal glands following injury are relatively limited. These include degeneration, necrosis (either oncotic or apoptotic), hypertrophy, atrophy, inflammation, and pigment accumulations. Focal lacrimal glandular hyperplasia, diffuse hyperplasia, or squamous metaplasia of ductal epithelium in rats may occur as a regenerative response to glandular damage [75]. Squamous metaplasia may be observed infrequently in the nictitating gland in dogs (Fig. 5.4).

Gland of the third eyelid from a control dog. The gland has focal squamous metaplasia. H&E. 10× objective
Harderian gland alteration (i.e., metaplasia), or harderianization, of the lacrimal gland is characterized as normal-appearing harderian acini in an otherwise normal lacrimal gland. Harderianization occurs as early as 3 weeks and increases with age and in the glands of both sexes, but males tend to have a greater incidence and extent of the change than females. The relative occurrence has been shown to be decreased with castration [76, 77]. Lacrimal gland alteration also occurs in rabbits and is characterized as normal lacrimal gland acini in the Harder’s gland (Fig. 5.5).

Harder’s gland from a rabbit. Lacrimal gland alteration consisting of a cluster of basophilic acini morphologically similar to lacrimal gland acini located within the pink lobe of the Harder’s gland. H&E. 20× objective
Alterations of the lacrimal gland include minimal lymphoplasmacytic cell infiltration, especially in the rabbit, and focal glandular hyperplasia and squamous hyperplasia of ductal epithelium in rats [75, 76]. Hyperplasia generally occurs as a regenerative response to degeneration or inflammation [75]. Experimentally, diffuse acinar hyperplasia occurs in rats infused with recombinant human growth factor and is characterized by an increased number of cells per acinus, cell hypertrophy, anisokaryosis, accumulation of cell debris, and brown pigmentation [78].
Hyperplasia of the lacrimal gland may occur in aged rodents and appears to be more common in mice than aged rats or hamsters [49, 75, 79–81]. Hyperplasia of the lacrimal glands may be associated with degeneration and inflammation with squamous metaplasia of ducts [75].
In contrast to other periorbital tissues, lacrimal glands are sensitive to radiation injury. Radiation injury of ocular adnexa initially manifests acutely within 48 h of irradiation of the lacrimal glands. Degeneration and apoptosis or necrosis of the acinar cells occurs as a dose-dependent phenomenon. Ionizing radiation that exceeds 35Gy fractionated at 1.8–2.0 Gy (180–200 rad) per fraction increases the risk of lacrimal damage [82]. The ductular epithelium is also susceptible, but to a lesser degree than the acinar epithelium. Degenerating cells may have enlarged nuclei. Necrosis leads to a neutrophilic inflammatory response, and with time, there are decreased numbers of serous acini and atrophy of remaining serous acini. Periocular tissues will likely be edematous and diffusely infiltrated with neutrophils. However, this periocular tissue reaction may be due to vascular endothelial injury and not to glandular injury per se, as blood vessels are dilated and have hypertrophic endothelium [83, 84].
Drugs may affect lacrimal glands by decreasing lacrimal secretion resulting in KCS, but species susceptibility may vary [85]. For example, practolol, a ß-adrenergic receptor blocker, induces adverse ocular effects in humans, but not in animal models [86].
Lacrimal glands of dogs are affected by treatment with sulfonamide and 5-aminosalicylic acid [85, 87]. Sulfonamides have been reported to produce decreased tear production and subsequent KCS in dogs. The glands have chronic inflammation with atrophy and replacement by fibrous connective tissue, plasma cells, and lymphocytes. Atrophy of the lacrimal glands may occur in dogs following administration of 5-aminosalicylic acid for 1 year [88]. Atrophy and lymphoid cell infiltration occurs in the lacrimal glands, the glands of the nictitating membrane, and the parotid salivary glands. These dogs develop KCS with flattening and desquamation of superficial corneal epithelial cells, stunting and loss of cell surface microplicae, decreased density of cell cytoplasm, and disruption of anterior cell membranes. Corneal changes include inflammation, vascularization, and proliferation of fibroblasts. However, KCS does not appear to have been reported in human patients chronically treated with 5-aminosalicylic acid.
Inflammatory reactions in lacrimal glands can also be stimulated by various cytokines. These experiments have largely been for the purpose of developing models of autoimmune dacryoadenitis. Interleukin-1 injected into the lacrimal gland inhibits neural- and agonist-induced protein secretion with decreased tear output [89]. Associated with this is a severe inflammatory response that is reversible within 7–13 days after injection. The inflammation leads to destruction of lacrimal gland acinar epithelium. During resolution, there is increased proliferation of acinar and ductal epithelium with ultimate recovery to normal tear production. Interleukin-12 and interleukin-18 will also result in injury to the lacrimal gland, but without infiltrates of inflammatory cells [90]. Injection of these cytokines together via the intraperitoneal route results in apoptosis of serous acinar cells. Administration of either cytokine alone had no effects on these glands.
Another change in lacrimal glands is discoloration due to an accumulation of pigments. 7-Acetyl-1,1,3,4,4,6-hexamethyl-1,2,3,4-tetrahydronaphthalene (AHTN) is a fragrance material in consumer products that resulted in a green discoloration of lacrimal gland in female rats, but not male rats [91]. Discoloration was also noted in the liver and lymph nodes with reversal of the discoloration occurring in the liver, but not lacrimal gland. No microscopic correlate to the green discoloration of the lacrimal gland was observed.
Practolol administration to dogs results in a macroscopic dark brown to black discoloration of the lacrimal glands [92]. Microscopically, fine, dark brown pigment granules are present in the apical or supranuclear cytoplasm of the serous acinar lacrimal epithelial cells. Ultrastructurally, these correspond to membrane-bound dense bodies. In another study, practolol administration to dogs resulted in decreased tear flow and lymphocytic infiltrates into the lacrimal gland, but changes did not occur when a related compound (carteolol) was administered [85]. Phenazopyridine accumulates selectively in the lacrimal glands, nictitating glands, and glands of Moll, resulting in pigmentation [93]. Clinical effects include blepharospasm, photophobia, purulent conjunctivitis, and corneal ulceration, presumably from decreased tear production. Grossly, within 48 h of oral administration, phenazopyridine causes dark brown to black pigmentation of the lacrimal gland and gland of the third eyelid. Microscopically, brown to black pigment is visible in glandular acini within 48 h and accumulated with time. Neutrophilic infiltrates occur within 3–6 days of administration, and ultrastructurally, immature secretory granules containing phenazopyridine occur within 24 h as an osmiophilic material interspersed with normal granule constituents. With time, granules in acinar cells become pleomorphic or fuse.
Botulinum toxin B, a treatment for hypersecretion of lacrimal glands, blocks muscarinic receptors and when injected directly into the lacrimal gland suppresses lacrimation for 4–5 months in human patients. In mice, a similar physiologic effect can be produced, resulting in KCS, but without histologic changes in lacrimal glands [94, 95]. Similarly, administration of a muscarinic receptor agonist in rats results in corneal opacity with neovascularization [96]. Both lacrimal glands and harderian glands undergo hypertrophy which is suspected to be an adaptive response to the blockade. Diminution of lacrimal secretions is also observed with administration of other antispasmodic agents [97].
Common spontaneous microscopic findings of the Harder’s gland in rabbits include variability in the size of the lumina with scattered aggregates of dilated acini, minimal lymphoplasmacytic cell infiltrates, and focal areas of atrophy. Spontaneous findings involving the rodent harderian gland are common and include degeneration, especially in older animals, which may be characterized by atrophy of glandular acini, mineralization, fibrosis, and cyst formation. Additional spontaneous findings in harderian glands include inflammatory cell (neutrophils, lymphocytes, plasma cells) infiltrates, inflammation (dacryoadenitis), and excessive secretion of porphyrin (chromodacryorrhea).
Chromodacryorrhea may be caused by stress, necrosis or inflammation of the harderian gland, or administration of cholinergic drugs [98, 99]. Inflammation and necrosis may be caused by a viral disease (i.e., sialodacryoadenitis virus [SDV]) that occurs in young rats and mice [100]. The infection involves salivary glands, lacrimal glands, and harderian glands. The necrosis and edema of the harderian gland results in orbital swelling and proptosis of the globe which leads to corneal ulceration and keratitis. Other causes of necrosis, edema, and inflammation of the harderian gland include retro-orbital trauma from venipuncture, exposure to certain drugs (e.g., 4-chloronitrobenzene in rats), and exposure of albino rats to high-intensity light for 12–24 h (Fig. 5.6) [101–104]. Exposure of albino mice to constant light for as little as 24 h results in exophthalmos. Microscopically, the harderian gland has swollen secretory cells with an obliteration of glandular lumina. With time, glandular lumina contain lipid and cellular debris, and lining cells vary in appearance from columnar to squamous. Mitotic figures, leukocytes, and macrophages are present, along with necrosis of glandular cells and edema [102]. With cessation of the exposure, harderian gland changes regress within about a week.

Globe and adjacent tissues from a rat with iatrogenic trauma from retro-orbital blood collection. Multiple changes include necrosis, hemorrhage, and inflammation of periorbital tissues and intraocular exudation with serous retinal detachment. H&E. 2.5× objective
Inflammation of the harderian gland may also occur following exposure to exogenous chemicals.
Several agents, such as albuterol, have been shown to produce enlargement of the harderian gland [105]. Chronic aflatoxin administration to the Syrian hamster will result in hyperplasia and epithelial atypia of the harderian gland [106]. With time, some of these changes progress to papillary cystadenomas and solid adenomas. Recombinant human epidermal growth factor administered systemically has resulted in changes in the harderian gland of rats that include an increased numbers of epithelial cells per acinus, increased cell size, accumulation of cell debris in acinar lumina, and occasional areas of degenerating cells with pyknotic nuclei [78].
Atropine sulfate, a mydriatic often used in nonrodent species during ophthalmic examinations, causes a suppression of expulsion of secretory material [107]. Changes include dilation of acinar lumina and accumulations of brownish pigment. The increased brown pigment correlated with increased levels of porphyrin pigments in these glands. Glandular epithelial degeneration occurred in some animals which may have been associated with the prolonged accumulation of the porphyrin. The degeneration was characterized by thinning of the epithelium with formation of larger cytoplasmic vacuoles.
Many different agents and conditions cause effects in the harderian gland. Administration of the neuroleptic timipirone causes increases in the number of accretions of porphyrin in mice [108]. In rats, accumulation of porphyrin occurs with dietary pantothenic acid deficiency and results in hypertrophy of the harderian gland [109]. Atrophy of the harderian gland occurs following exposure to xenobiotics, and administration of retinoids causes a decrease in the weights of harderian glands due to a decrease in acini and small nuclei, indicating inactivity [110].
Since the harderian gland develops to a significant degree after birth, prenatal exposure to an agent (e.g., the herbicide 2,4-dichorophenyl-p-nitrophenyl ether) may result in degeneration after birth [111].
Spontaneous hyperplasia of the harderian gland may occur in aged rodents and appears to be more common in mice than aged rats or hamsters [49, 75, 79–81]. At times, hyperplasia of the harderian gland of the rat (i.e., Fischer 344) may be associated with degeneration, inflammation, and ductular squamous metaplasia [75].
5.4.4 Nictitating Membrane
The third eyelid (i.e., nictitating membrane, membrane nictitans) is a fold of conjunctiva that contains a cartilaginous plate surrounded ventromedially by a lacrimal gland (i.e., gland of the third eyelid, nictitans gland) which contributes to the production of tears [4, 112]. The inner conjunctival covering (i.e., bulbar conjunctiva) of the third eyelid contains numerous lymphoid nodules which can undergo lymphoid hyperplasia. The third eyelid is present in many laboratory animals (e.g., rabbits, dogs, minipigs) but is absent in rodents and primates. Retraction of the globe into the orbit by the retractor bulbi muscle or sinking of the globe into the orbit because of bulbar pain or a small size (e.g., microphthalmia or phthisis bulbi) allows the third eyelid to passively cover the cornea. Large red masses protruding from the third eyelid at the medial canthus may be the result of swelling and protrusion of the nictitating membrane [113, 114].
5.4.5 Lacrimal and Lymphoid Drainage
The products of the lacrimal glands flow over the cornea and are drained away via puncta in the eyelid margins that open into canaliculi and lacrimal sacs. The canaliculi travel a short distance vertically in the lid margin, then horizontally before connecting with the lacrimal sac. The canaliculi are lined by nonkeratinizing, stratified squamous epithelium. The lacrimal sac is located in the lacrimal fossa, a depression in the medial wall of the orbit. The lacrimal sac is lined by stratified columnar epithelium containing goblet cells. From the lacrimal sac, the nasolacrimal duct forms as a downward extension and can be histologically evaluated in appropriate nasal sections. The lymphatic drainage for the lacrimal glands and harderian glands is via periauricular and submandibular nodes in humans. Sampling of similar nodes in laboratory animal species should be considered when dosing via a topical route.
Treatment-related findings occur in the nasolacrimal duct. Hyperplasia of the lining epithelium of the nasolacrimal duct of rats has been noted following systemic treatment with recombinant human epidermal growth factor (EGF) [78]. Findings include a duct with an increased mucosal thickness, loss of cilia, and occasional pyknotic nuclei. EGF is secreted and cleared by the harderian gland and is eventually drained into the nasolacrimal duct. Interestingly, there was no corneal change, but corneal healing has been noted to be enhanced in cats and rabbits treated with EGF [115, 116].
Inflammation of the nasolacrimal duct is associated with chronic administration of antihistamines to rats and has been associated with the presence of stents [117, 118].
Hydrophilic coatings of the stents appear to decrease foreign body reactions and increase patency. Blockage of the nasolacrimal duct from inflammation or implanting a stent may result in epiphora (i.e., excessive tearing). Administration of docetaxel has been associated with this finding [119]. Cyalume, a chemiluminescent material, has been used to clinically evaluate the nasolacrimal system in human patients and does not injure the nasolacrimal duct but has resulted in findings in other locations [120].
5.4.6 Orbital Fascia and Other Orbital Contents
Orbital fascia consists of periorbita, Tenon’s capsule (i.e., fascia bulbi), and fascial sheaths of extraocular muscles [4, 7, 45]. Other structures include the retro-orbital sinus in mice and retro-orbital plexus in rats which are used for venipuncture.
An increase in the size of intraorbital contents results in an anterior protrusion of the globe (i.e., proptosis or exophthalmos). The cause is often the result of inflammation but could potentially be due to orbital neoplasia or the result of toxicity. In animals, orbital edema may be due to systemic administration of p-phenylenediamine and exophthalmos may be due to systemic administration of acetonitrile, aminocaproic acid, organic cyanides, or vitamin A [50].
5.4.7 Neoplasia of Lacrimal and Harderian Glands
Neoplasia of the harderian gland and lacrimal gland may occur in aged rodents and appears to be more common in mice than rats or hamsters [49, 75, 79–81]. Most tumors in rats are adenomas, with papillary, or cystic acinar differentiation, but orbital schwannoma has been reported [76]. The incidence depends on strain (e.g., Fischer 344, Osborne-Mendel and Wistar rats) but may be as much as 0.5–15% [81]. Harderian gland adenomas are frequently well-demarcated masses that compress the adjacent parenchyma, but usually do not have a well-defined capsule. They are papillary, cystic, or a combination and are composed of pseudoglandular structures and form arborizing and folded fingerlike fronds. Fronds are composed of a delicate fibrovascular core lined by cells that are usually tall columnar with foamy amphiphilic cytoplasm. The cells usually form a single layer, but areas are frequently present that give the appearance of having a basal layer of normal-appearing cells “capped” by smaller cells adjacent to the lumen. Harderian gland adenocarcinomas are usually well differentiated, differing from adenomas by greater atypia, invasion, and metastasis. Undifferentiated adenocarcinomas often contain a single large cytoplasmic vacuole, and mitotic figures are uncommon [121–123]. Harderian gland adenocarcinomas can metastasize to the eye and spread systemically [49, 76, 123]. Harderian gland tumors in mice may be induced by various agents, including ionizing radiation and genotoxic carcinogens [50, 81]. Harderian adenocarcinoma has been induced experimentally in rats by repeated injections with 10% urethane or when fed a low-fat diet containing 0.03% 2-acetylaminofluorene [49].
5.5 Cornea
The cornea is composed of several transparent layers that include (1) the precorneal tear film; (2) an outer, nonpigmented, nonkeratinized, and stratified squamous epithelial layer; (3) the anterior limiting membrane (i.e., Bowman’s layer) in primates; (4) an avascular stromal layer; (5) Descemet’s membrane; and (6) the corneal endothelium [4, 7, 124]. The function of the cornea is to transmit and refract light.
The results of iatrogenic intervention may result in various degrees of corneal opacity and should be distinguished from alterations due to toxicity. Some procedures such as surgery or an injection of a test article may affect all layers of the cornea. It is important to be aware of iatrogenic causes of corneal lesions that may be observed in the course of a toxicology study. Although most pathologists microscopically examine the eye in toxicology studies of systemically administered compounds, there are times when the test article is administered locally to the eye. In these studies, the pathologist needs to be aware of the route of administration and the alterations that may be present due to that route of administration. These effects are most notable when there is a surgical procedure or injection of the test article. Complications, or the lack thereof, should be documented. Corneal alterations that may be observed include an incision site and suture material as well as needle tracks from an injection. If the cornea is incised, complications may include inflammatory reactions to infected incision sites, down growth of corneal epithelium into the incision site, islands of corneal epithelium within the cornea that may become epithelial inclusion cysts (Fig. 5.7), corneal epithelial growth on the endothelial surface of the cornea, loss of corneal endothelium, deposition of foreign material into the eye or incision site or needle track (Fig. 5.8), and entrapment of the iris in the incision site (Fig. 5.9) [20]. For both incisions and needle tracks captured in histologic sections, the corneal stroma may be focally disorganized, which may or may not be sufficient to be observed as corneal opacity on ophthalmic or gross examination.

Cornea from a rabbit two weeks following a surgical procedure. The incision site has a nest of corneal epithelium entrapped in the stroma, which, given sufficient time, may develop into a cyst. The endothelial surface has a focal area of retrocorneal membrane development. H&E. 10× objective

Injection site in the cornea from a dog. There is a linear area of deposition of crystalline material from the injection remaining in the corneal stroma. H&E. 10× objective

Iridal entrapment in a rabbit. The iris is entrapped in a healing corneal incision. Note the suture cross sections near the corneal surface. H&E. 5× objective
In addition to iatrogenic findings, there are various alterations that occur spontaneously or in response to toxicity. Some changes may be localized to specific layers of the cornea, but more often than not, multiple layers of the cornea are affected. Toxic effects of the cornea have a tendency to affect either the outer cornea or the inner cornea. Toxic effects may be the result of a topical application or may be associated with systemic effects. Systemically administered drugs can also affect the cornea by secretion into the tear film (and therefore iritate the cornea directly), by injury of the lacrimal gland which removes the protective tear film which results in damage, or by inhibiting the protective corneal reflexes through depression of the central nervous system.
5.5.1 Macroscopic Corneal Opacities
Corneal opacities are noted on ophthalmic or macroscopic examination and refer to loss of transparency of the cornea. These are often due to mineralization, especially in rodents. Corneal opacities in rats may be diffuse or punctate and reversible or permanent. Diffuse corneal opacities occur in rats, especially males, and increase in incidence with age [125]. They may be punctate, focal lesions that give the cornea the dimpled gross appearance of an orange peel. Diffuse or focal opacities may be associated with or accompanied by conjunctivitis, keratitis, and corneal ulceration [126]. As such, corneal opacity is a nonspecific term that may correlate with multiple microscopic alterations.
In rats, corneal opacity as a spontaneous change may be unilateral or bilateral and tends to occur in males greater than or equal to 18 weeks of age. They correspond with multiple deposits of fine, white granules on the corneal surface grossly or deposits of basophilic fine granules or basophilic laminated plaques in the corneal basement membrane microscopically [127]. Corneal degeneration with superficial punctate opacities has been reported in Sprague-Dawley and Wistar rats of various ages and of both sexes [128]. Corneal opacities generally occur with an increased incidence with increased age in Sprague-Dawley rats [126, 127]. Others have reported reflective opacities in rats to be corneal crystalline deposits, with a higher incidence in males, that are usually bilateral, multifocal, and punctate, and usually in nasal locations oriented horizontally along the palpebral fissure [129].
Corneal abnormalities as spontaneous occurrences in mice on ophthalmic or gross examination have been reported in various strains [122, 126, 128, 130, 131]. Diffuse corneal opacities are infrequent in mice but increase in incidence with age and are due to mineralization of the anterior stroma [126]. Hubert reported corneal abnormalities in 4–5-week-old Swiss mice Crl:CD1(ICR)BR [46]. MRL mice with features of hyperparathyroidism have been described with corneal changes [132, 133]. Opacities in mice may be due to infrequent cage cleaning or cage environment, where urease-positive bacteria may increase ambient cage ammonia levels [130]. It has been suggested that some strains of mice may have a genetic predisposition. Therapeutic agents such as azathioprine and meticorten have been described as causing corneal opacities as well. In spontaneous diabetic KK mice, calcium is present as extracellular deposits of fine basophilic granules or as dense strips at the junction between the epithelium and the stroma, with older lesions tending to have neovascularization and minimal cellular infiltrates of neutrophils and mononuclear cells [132, 134].
5.5.2 Superficial Corneal Alterations
Changes in the corneal epithelium to superficial injury or toxicity include edema, erosions or abrasions, and ulcers from necrosis [135]. Grant characterizes the corneal changes from chemical burns from contact with liquids and solids; contact with gases, vapors, and dusts; or changes from systemic substances [50]. Chemical burns may cause immediate caustic injuries. Examples include alkalis and acids which not only affect the epithelium but also the stroma with edema and loss of mucopolysaccharides leading to opacification. The opacification is often accompanied by vascularization. Gases, vapors, and dusts may include a stinging sensation and result in tearing. Most substances that induce lacrimation can injure the cornea if the concentration is high enough. Findings include epithelial edema, vacuolation, delayed healing, or inflammation. Corneal epithelial edema is initially intracellular and appears as perinuclear pallor. With progression, there is pericellular fluid accumulation with the potential for bulla formation. An erosion (i.e., abrasion) is the partial desquamation of corneal epithelium and is usually due to focal mechanical trauma of a foreign body, such as dust particles. Since the defect does not extend past the corneal epithelial basement membrane, it may not be discernible on ophthalmic examination. With extension through the epithelial basement membrane (i.e., ulcer), the stroma will retain fluorescein. Ulceration may occur as a result of an initial abrasion with a bacterial infection. Abrasions are occasionally observed in the corneal epithelium in large animals [136]. Although in histologic section abrasions appear like small “craters” in the epithelium, they are likely instead linear. Microscopically, abrasions containing crowded cells in the basal layer are indicative of healing. Generally, the corneal epithelium heals quickly [137].
Hypertyrosinemia has been demonstrated to produce corneal opacities in laboratory animals [138–140]. Excessive tyrosine fed in the diet to rats produces initially an edema of the corneal epithelium with subsequent infiltrate of neutrophils into the superficial epithelial layers [139]. This progresses to neutrophilic infiltrates throughout the epithelium and eventually to infiltrates and edema of the corneal stroma. In rabbits, similar changes have been described with hypertyrosinemia with ophthalmic observations of pinpoint opacities and “glittering pre-endothelial structures” on slit lamp [138]. Microscopically, the corneal epithelium had focal proliferations with vacuolation of basal epithelial layers. Scattered epithelial cells underwent necrosis. Hypertyrosinemia induced by 2-(2-nitro-4-trifluoromethylbenzoyl)-cyclohexane-1,3-dione (NTBC), which is a potent inhibitor of 4-hydroxyphenylpyruvate dehydrogenase, produced corneal opacities in dogs, but not rats or rhesus monkeys [140]. All three species had elevations of serum tyrosine and aqueous tyrosine, indicating that there are some species-specific differences that lead to the corneal opacity with hypertyrosinemia.
Keratitis in various animal species is occasionally observed. These have been suspected to be due to environmental irritants such as ammonia and dusts from the bedding and feed, reduced lacrimal secretion, trauma, or exophthalmos [68, 130, 141]. Several strains of mice have had corneal opacities with histologic correlates of chronic inflammation of the corneal epithelium and anterior corneal stroma that included such features as ulcers and erosions, acute keratitis, neovascularization, and mineralization of the basement membrane [130]. These may be considered iatrogenic in the sense that they are an artifact of the test system, although animal colony management should reduce or eliminate these as a common occurrence.
5.5.3 Corneal Irritation or Local Toxicity
Adverse effects of drugs or ocular medical devices (i.e., contact lenses) on the outer cornea can be determined by use of the Draize ocular irritation scoring method and its various modifications [17, 142–146]. Currently, some of the features of a clinical adverse reaction are being predicted by use of in vitro or ex vivo assays such as the bovine corneal opacity and permeability assay (BCOP) [147, 148]. The BCOP will largely mirror in vivo responses, except for the absence of an inflammatory response or neovascularization in these in vitro and ex vivo assays.
The various responses to irritating substances such as alkalis, acids, and surfactants from direct contact to the cornea have been studied to better understand the pathology as well as to serve as benchmarks in the development of in vitro and ex vivo substitutes to in vivo testing [135, 149–154]. Alkali burns are caused by saponification of cell membranes, allowing greater penetration of the injurious chemical, making alkali burns usually the most severe injury. Acid burns are caused by coagulation and precipitation of cellular proteins, and the natural buffering of tissues tends to limit the injury of acids as compared to alkalis [151]. Surfactants generally produce a milder injury than acids or alkalis. Surfactants are broadly classified as cationic, anionic, or nonanionic based on their chemical structure, but cationic surfactants tend to produce the greatest injury due to the precipitation of cellular proteins [17]. Anionic surfactants are intermediate and tend to cause cell lysis, while nonionic surfactants do not produce protein precipitation or cell lysis [150]. Regardless of the nature of the chemical, they all can produce erosion, denudation, and necrosis of the corneal epithelium [135]. Greater irritant capacity generally corresponds with greater extent and depth of injury. Mild irritants are therefore confined to the epithelium, while moderate irritants will injure the corneal stroma, and severe irritants will affect the deep stroma and possibly the corneal endothelium. Affected corneal stroma will be edematous and have necrosis and lysis of keratocytes. The corneal endothelium may be lost. With time, the cornea will respond with keratocyte regeneration, neovascularization, conjunctivalization, or epidermalization of the corneal epithelium. The degree of response will reflect the initial depth and area of injury. It should be noted that although the corneal epithelium is first and often most greatly affected, this may not always be the case. For bleaching agents, it was noted that the corneal stromal injury was greater than the corneal epithelial injury [153]. Severe or perforating keratitis may lead to inflammation of the iris (i.e., iritis), anterior uvea (i.e., anterior uveitis), inner aspect of the globe (i.e., endophthalmitis), or the whole globe (i.e., panophthalmitis). With chronic inflammation affecting most or all of the globe, then shrinkage and distortion of the globe (i.e., phthisis bulbi) can occur.
The outer cornea may be injured due to desiccation from an acute or chronic loss of tear film. The tear film may be compromised by a lack of production or a lack of covering of the corneal surface. A lack of production may be due to inflammation of the lacrimal gland or administration of certain pharmacological compounds, including local anesthetics, anticholinergic compounds, or anticholinesterases, which decrease lacrimal secretions. Compounds that affect the lacrimal gland or meibomian glands may result in a minimal, reversible changes in the cornea (e.g., keratinization) or, if more severe, a chronic condition involving the cornea, KCS. Changes in the cornea associated with KCS include keratinization, epidermalization, pigmentation, fibrosis, and neovascularization of the superficial stroma and possibly mononuclear or mixed inflammatory cell infiltration.
Acute corneal desiccation may occur following general anesthesia as an iatrogenic cause of corneal changes [155, 156]. Desiccation in the interpalpebral area leading to keratoconjunctivitis sicca and associated secondary uveitis is reported in rats following general anesthesia with a combination of xylazine and ketamine [157]. Animals undergoing general anesthesia will often have incomplete closure of the eyes (lagophthalmos). Even if the anesthesia is not prolonged, desiccation of the areas of cornea not covered by the eyelids will occur by evaporation following breakup of the precorneal tear film, which can happen in seconds to minutes. In humans, the time required for injury is longer than in rodents, with no changes reported in human eyes up to approximately 100 min. In addition to lagophthalmos, general anesthesia may also reduce the production and the stability of tears [155]. Microscopically, corneal desiccation may result in changes of degeneration or erosion and thinning and ulceration of the corneal epithelium. Changes generally will be acute to subacute, and the changes of chronic KCS would not be anticipated as iatrogenic changes in laboratory animals. Several authors have described drug-induced corneal opacities related to narcotic analgesics or prolonged anesthesia [157–159]. For example, a single administration of the long-acting narcotic analgesic 1-alpha-acetylmethadol to male Sprague-Dawley rats resulted in localized corneal opacities mainly in central, nasal, or inferior-nasal regions after 3–5 days [159]. Microscopically, these animals had thickened corneal epithelium, loss of cellular polarity, hyalinization of the basement membrane, stromal vascularization, spindle cell proliferation, inflammation, and frank perforation. It was considered likely that this was due to adverse effects on corneal sensory innervation, blinking, or tear formation, instead of direct chemical effect on the corneal epithelium.
Although not due to lagophthalmos and drying, other anesthetic agents have been associated with corneal epithelial changes. These include administration of agents such as cocaine, tetracaine, and proparacaine. Chronic use of these anesthetics may alter the plasma membrane integrity of corneal epithelial cells, cause release of enzymes such as lactate dehydrogenase, and cause decreases in mitochondrial dehydrogenase activity [160]. Corneal opacities have been reported in rats following administration of morphine and narcotic analgesics [159]. Microscopically, there may be thinning of the corneal epithelium, and generally, these are acute or subacute and do not progress to the changes of chronic keratoconjunctivitis sicca.
Chronic desiccation of the cornea leading to KCS may also be the result of anterior displacement of the cornea. This may occur as the result of an enlarged globe (e.g., glaucoma) or from anterior displacement of the entire globe (exophthalmos, proptosis) secondary to orbital swelling. Inflammation of the harderian gland with chromodacryorrhea from repeated orbital bleeding or from a viral infection (e.g., sialodacryoadenitis) may also be causes [100]. Anterior displacement of the cornea appears to affect males more than females. Treatment with clonidine induces exophthalmos and a reduction in tear flow in mice and rats resulting in flattening and desquamation of corneal epithelium and vacuolation of basal cells. These changes may progress to keratoconjunctivitis and anterior uveitis [141].
In addition to irritants and loss of tear film, corneal epithelial lesions may be produced by drugs that inhibit mitosis and reduce the proliferative capacity of the corneal basal epithelium. A variety of antineoplastic agents are known to affect the cornea, and these often present clinically in patients as punctate keratitis [161]. For example, the antineoplastic drug, capecitabine, is converted to 5-fluorouracil in vivo and is concentrated in tears. Clinical signs in dogs include multiple erosions of the cornea with superficial corneal epithelial pigmentation and neovascularization [162]. Microscopically, the corneal epithelial basal cells were disorganized and had an abnormal morphology resulting in a thinned corneal epithelium. Thinning (i.e., atrophy) of the corneal epithelium with progression to ulceration and inflammation also occurred in dogs given inhibitors of oxidosqualene cyclase [163]. Atrophy has also been described in human patients treated with triparanol, a late stage blocker of cholesterol synthesis [164, 165]. Decreases or alterations in tear production may occur with oxidosqualene inhibitors related to reductions in the lipid-rich glands such as the meibomian glands [166].
Hyperplasia of the corneal epithelium may occur as a nonspecific response to injury such as to topical chemical injury as described above. Conjunctivalization is a metaplastic response where the corneal epithelium transforms into the appearance of conjunctiva, with goblet cell differentiation and irregular thickness. A chronic change observed in the corneal epithelium of mice is goblet cell metaplasia [167]. Hyperplasia has also been observed with systemically administered compounds, a notable example being EGF [168]. High doses of systemically administered recombinant EGF produced diffuse, uniform thickening of the corneal epithelium due to an increased number of layers of corneal epithelial cells overlying basal cells that were hypertrophic and hyperplastic.
Although uncommon, localized corneal proliferation may occur, especially in chronic studies. Corneal hyperplasia may be observed as a focal, diffuse, or nodular thickening of the corneal epithelial layer and is not considered to be preneoplastic [167]. Hyperplasia may be accompanied by keratinization. Corneal proliferation may include squamous cell hyperplasia, epithelial hyperplasia, squamous cell papilloma, and squamous cell carcinoma as chronic changes in rats. Squamous cell carcinoma is not known as a spontaneous finding in mice [169]. The corneal surface epithelium may be focally thickened due to congenital findings such as corneal dermoids. A corneal dermoid is the localized presence of tissue appearing as skin within the cornea. The finding may be unilateral or bilateral and will be discovered on prestudy ophthalmic examinations. These have been described in the rat, hairless and haired guinea pig, rabbit, and dog [170–174].
Squamous cell hyperplasia and acute keratitis have been induced in female HRA/Skh mice treated with 8-methoxypsoralen combined with UV radiation [175].
5.5.4 Superficial Corneal Stromal Alterations
Alterations in Bowman’s layer in primates include edema, spheroidal degeneration, or interruptions and may or may not be noted as corneal opacities. Edema of Bowman’s layer is usually associated with edema in the overlying epithelium or the underlying stroma and is manifested by decreased eosinophilia of this layer microscopically. Spheroidal degeneration of Bowman’s layer is considered collagen deposition and appears as extracellular spherical deposits. This change occurs as a sequela of chronic actinic exposure in humans. Interruptions in Bowman’s layer are often traumatic or related to surgery. Since Bowman’s layer does not regenerate, these interruptions will be filled in either with overlying corneal epithelium or with fibrous connective tissue from the underlying stroma.
5.5.4.1 Subepithelial Corneal Mineralization
Corneal mineralization can be due to multiple causes. Corneal dystrophy is a term commonly used in veterinary ophthalmic pathology to encompass many of these changes. However, corneal dystrophies are defined as spontaneously occurring, noninflammatory changes bilaterally affecting the central cornea with no associated systemic disease, when narrowly defined by the definitions used in human ophthalmology. Thus, narrowly defined, true corneal dystrophies as a primary disease appear to be rare in animals, while the more nonspecific calcific band keratopathies are relatively common. Calcific band keratopathy occurs in human patients in association with a variety of ocular and systemic diseases including chemical and physical injury, chronic glaucoma, and phthisis bulbi. It may also accompany hyperparathyroidism or vitamin D poisoning [176]. Hypercalcemia produces bilateral findings and may extend to include calcification of the bulbar conjunctiva [177]. In humans, it also usually involves Bowman’s layer.
Calcific band keratopathies, which as previously mentioned are also commonly referred to as corneal dystrophies in laboratory animals, are mineralized or calcified deposits presenting microscopically as basophilic granularity along the corneal epithelial basement membrane [178]. The extent and severity of secondary changes varies with animal strain, age, and experimental conditions [125]. The macroscopic lesion is often characterized by a central, bilateral, and elliptical band in the area underlying the palpebral fissure [179]. More advanced findings may consist of epithelial necrosis, foreign body reaction, and scarring. Often, experimental corneal calcification is the result of trauma, which causes edema and proliferation of fibroblasts. These cells synthesize and release glycosaminoglycans into damaged regions, where the calcification develops; the free anionic groups of glycosaminoglycans tend to bind calcium [180].
Drying of the cornea is an important mechanism of mineralization because evaporation of the tear film from the cornea results in supersaturation and precipitation of calcium in the superficial corneal stroma. Band keratopathy may develop due to inability to cover the underlying cornea with the lids, as well as high ammonia levels from urease-positive bacteria in the bedding [130]. In mice, it may be due to harderian gland adenoma leading to proptosis and keratitis.
A true corneal dystrophy has been described in the American Dutch belted rabbit and the New Zealand white rabbit. The American Dutch belted rabbit develops opacities involving the corneal epithelium, basement membrane, and superficial stroma that are noted clinically with the use of a slit lamp. Microscopically, the basement membrane is thickened, and the overlying epithelium is thinned and disorganized. The underlying corneal stroma is also often disorganized [181]. The corneal dystrophy reported in the New Zealand white rabbits is characterized by a normal basement membrane, but the overlying epithelium is irregular with both thickened and thinned areas [182]. Calcification or mineralization of the cornea independent of these corneal dystrophies has been reported in rabbits due to local trauma, hypervitaminosis D, and administration of dihydrotachysterol [158, 183–185]. Corneal injury potentiates the corneal calcification produced by the hypercalcemia of dihydrotachysterol in rabbits. Calcification also occurs in the rabbit cornea in response to immunogenic uveitis combined with hypercalcemia [186].
Experimental corneal calcification in the rabbit has been produced by mild irritation with carbon dioxide laser [183]. Ultrastructurally, numerous spherules of fine crystals were within the basement membrane of the corneal epithelium. Some calcific spherules were also present in membrane-bound vesicles within the cytoplasm of keratocytes. These deposits stained black with von Kossa silver stain and red with alizarin red S stain, indicating the presence of calcium. Additionally in rabbits, ––morphine appears to cause drying of the cornea [158] with development of exophthalmos in treated rabbits.
In rats, corneal mineralization, often referred to as corneal dystrophy, is a condition where calcium and phosphorus is deposited in the superficial cornea in a diffuse or punctate distribution along the palpebral fissure [179]. It is postulated that changes in the corneal microenvironment (e.g., pH or ion concentration) can cause calcium to precipitate [128, 177]. Strains of rats involved include Wistar, Sprague-Dawley, and Fischer 344 [122, 126, 128, 130, 178]. In Sprague-Dawley, Fischer 344, and Wistar rats, mineralization occurs more in males than females [129]. A syndrome called spontaneous corneal dystrophy has been described in Fischer 344 rats that have extracellular electron-dense deposits of calcium and phosphorus in basement membranes of corneal epithelial cells and other tissues (e.g., renal tubular basement) such that the condition is not strictly limited to the cornea and therefore does not fit the strict definition of corneal dystrophy used in human ophthalmology [178, 187]. Band keratopathy can occur in rats due to the increased dietary content of vitamin D3, local ocular disease, or systemic abnormalities in calcium-phosphate metabolism [131]. Excess vitamin D causes similar findings in the corneas of albino and pigmented guinea pigs. However, the guinea pig cornea appears to be much less susceptible to experimental corneal calcification than the rat or the rabbit.
In the rat, de-epithelialization of the central or entire cornea is effective in inducing corneal calcification. Other treatments in the rat, including isoproterenol, alloxan [188, 189], increased dietary vitamin D3 [185], subcutaneous administration of morphine sulfate, and suturing the eyelids open, all can be associated with corneal calcification.
Meador et al. described corneal mineralization associated with epicardial mineralization in SCID mice with deposition of mineralized material in the corneal basement membrane or in thin clefts at the epithelial/stromal junction [192]. In more severe instances, deposits were surrounded by macrophages. The corneal epithelium was variably thinned and dystrophic.
5.5.4.2 Corneal Pigmentation
There are many different causes of corneal pigmentation. Brown, hemosiderin-laden macrophages may be present in the anterior chamber and adherent to the endothelium or in the corneal stroma following hemorrhage; yellow particles in the anterior layers of the cornea have been reported in the human cornea following administration of compounds containing gold [191]; and pigmentation occurs following administration of minocycline, amiodarone, phenothiazines, antimalarials, and salts containing silver [192–194]. Pigmentation may also be a consequence of migration of melanocytes from the conjunctiva associated with neovascularization and reparative responses from previous ulceration.
5.5.4.3 Corneal Stromal Edema
Nonspecific alterations in the stroma include edema and inflammation. Stromal edema is characterized by increased thickness of the stroma due to increased interstitial fluid. Inflammatory cells may infiltrate as part of the edema process. Expansion of the stroma by edema disrupts the regular arrangement of the collagen bundles of the stroma, producing opacity. Proper histologic processing is important to appreciate corneal edema, as artifacts can lead to notable differences in corneal thickness as observed on histologic slides.
5.5.4.4 Corneal Inflammation
Corneal inflammation is almost always accompanied by edema. Inflammation first presents grossly as perilimbal hyperemia. With time, cells migrate into the corneal epithelium and stroma. When inflammation is severe, cells will migrate from the iris into the anterior chamber (hypopyon) and then into the cornea. Nonulcerative inflammation, such as superficial keratopathy, if minor, can heal without any residual opacity. Stromal keratopathy involves the stromal layer and will likely be vascularized. Ulcerative corneal inflammation usually has a bacterial component that follows the initial injury. Sequelae to keratopathy include scars, which microscopically appear as fibrosis and will be clinically opaque. Keratectasia (i.e., ectatic cicatrix), descemetocele, and adherent leukoma may form. Pterygium is conjunctival growth onto the cornea and should be distinguished from pseudopterygium which is the extension of a conjunctival flap over the cornea. Keratectasia (ectatic cicatrix), descemetocele, adherent leukoma, and corneal staphyloma are the more serious consequences of ulceration.
Keratitis and sequelae are often related to injury and increase with age, with the rat having a greater incidence of keratitis than the mouse [125, 126]. Keratitis has been associated with SDV and coagulase-positive Staphylococci [100, 125, 129]. Corneal scars, with superficial vascularization, may be attributed to prior trauma [129]. Large animals such as the dog and monkey tend to have only infrequent keratitis, and the incidence in the dog has been report to be as low as 0.5%. In dogs, this has been attributed to dust and bedding and may be exacerbated when ocular defense mechanisms are depressed following administration of pharmacological agents.
Keratitis may be a manifestation of photosensitization after exposure to phenothiazine, methoxsalen, or other photosensitizing compounds [17, 50]. Ultraviolet radiation exposure and phototoxicity have been demonstrated to occur in humans and a variety of animal species with the cornea being one site of injury [161]. UV radiation has been associated with marked loss of keratocytes in mice [195]. Phototoxicity following exposure to Penicillium viridicatum culture material includes epithelial changes in the cornea, such as ballooning degeneration, proliferation and thickening of the corneal epithelium, and thinning of the corneal stroma [196]. Changes in the corneal stroma include corneal vascularization, fibrosis, and inflammation that may lead to keratoconus and rupture of the globe. The observed thinning of the cornea with UV light and the thickening demonstrated with some photosensitizers suggest that there may be effects related to differences in the physical energy injury.
5.5.4.5 Corneal Neovascularization
Neovascularization is the vascularization of a normally avascular corneal stroma (Fig. 5.10). It is a common response to corneal injury and is often associated with inflammatory mediators [197, 198]. Corneal neovascularization may be observed in nude or hairless mice [167, 199]. Blood vessels interfere with transparency by their physical presence and participate in inflammation. Vascularization of the cornea is a beneficial repair response to inflammation, although, as a sequela, it may produce opacities due to the persistence of nonperfused ghost vessels visible on ophthalmic examination as linear opacities. Vascularization will be confined only to the injured cornea and does not generally involve healthy cornea. Findings often associated with corneal neovascularization include conjunctival congestion, corneal stromal edema, and inflammation.

Cornea from a rabbit. The cornea is infiltrate by numerous inflammatory cells, and a relatively large vessel extends laterally through the corneal stroma. H&E. 20× objective
Neovascularization has also been associated with deficiencies of tryptophan, riboflavin, vitamin A, and zinc [200, 201]. Some compounds can induce neovascularization, such as EP4-prostaglandin E2 agonists. When this compound was administered topically, corneal neovascularization was induced as if either through a pharmacologic or inflammatory mechanism [202]. The induction of neovascularization may be inhibited by administration of compounds such as anti-vascular endothelial growth factor (VEGF) antibodies [203].
Not all corneal stromal vascularization is neovascularization. Limbal vessels can occasionally extend a short distance into the peripheral cornea. This finding is observed in the corneas of rabbits with no other corneal or limbal changes and is considered to represent normal finding. Careful examination of multiple sections of the eye from control animals can help differentiate normal variability from abnormality. In addition, corneal nerves may occasionally be observed within sections and should not be confused with neovascularization (Fig. 5.11).

Cornea from a rabbit. A nerve traverses laterally through the corneal stroma and is occasionally observed as a normal structure. H&E. 20× objective
5.5.4.6 Lipid Keratopathy and Corneal Phospholipidosis
Corneal lipidosis can be observed on occasion as either a spontaneous or induced change. Lipid deposition in the cornea of rabbits and dogs has been observed in animal colonies. Rabbits with altered lipid metabolism, notably the Watanabe WHHL rabbit or rabbits on high-fat diets, are susceptible to corneal lipidosis [204–207]. The eyes have grossly visible corneal opacities, initially as clouding of the medial ventral cornea, which will progress to pearly corneal opacities extending to the central and lateral cornea. Microscopically, the anterior corneal stroma has infiltrates of cells with necrosis and cellular infiltrates. Infiltrates consisted of large, pale, and foamy macrophages. Foci of necrosis contained Sudan black-positive materials. Corneal lipidosis may also be drug induced, with birefringent crystals in outer stroma that are visible with polarized light and stain with Sudan black. The guinea pig also may present with lipid deposition as part of a disease process including conjunctivitis, keratitis, and keratoconjunctivitis sicca [208].
In dogs, corneal lipidosis is a rare spontaneous change but when it occurs may present as marginal, zonal, or epithelial forms [209]. In beagle dogs on life span toxicology studies of radionuclides, similar corneal opacities have been observed with microscopic changes of amorphous to crystalline lipid deposits in the anterior cornea [209]. These appeared to be a spontaneous change in aged dogs, as no evidence of a systemic hypercholesterolemia was detected. However, deposits were determined to be neutral fats, phospholipids, and cholesterol [210].
Cationic amphiphilic drugs are recognized to produce phospholipidosis of the cornea. Chloroquine, tamoxifen, and other drugs in humans produce corneal deposits characterized by lipid in lysosomes of the corneal epithelium and keratocytes [161, 211–213]. In humans, the phospholipidosis is reversible and associated with little or no visual impairment [191]. Corneal phospholipidosis is also described in rats and dogs [214–216] and could occur in any species dosed with cationic amphiphilic compounds. Histologically, phospholipidosis in the cornea appears as clear lipidosis-like alterations in the corneal epithelial cells and keratocytes with bluish granules with hematoxylin and eosin staining. Semithin sections demonstrate densely staining toluidine blue positive, irregular cytoplasmic inclusions [215]. Transmission electron microscopy shows the typical lamellar and crystalline-like inclusions. Tilorone, an immunostimulatory agent that causes increased production of interferon, has been shown to produce both phospholipidosis and mucopolysaccharidosis in rats. The phospholipidosis is typical and reversible, while the mucopolysaccharidosis occurs as deposits of glycosaminoglycans in lysosomes of the corneal epithelium and keratocytes which persist for long periods [217, 218].
5.5.5 Deep Corneal Alterations
Descemet’s membrane undergoes changes secondary to changes in the overlying corneal stroma or underlying corneal endothelium. With expansion of the corneal stroma, such as with edema, Descemet’s membrane may develop tears (i.e., stria), and the edges of large tears in Descemet’s membrane often coil when examined microscopically (Fig. 5.12). Deep ulceration of the corneal stroma may result in anterior displacement of Descemet’s membrane into the stromal defect forming a descemetocele. Since Descemet’s membrane is continuously produced by corneal endothelium, it will become thickened with age or can undergo duplication [219]. Degenerative changes in Descemet’s membrane will manifest as irregular or diffuse thickening and are generally due to disease of the subjacent corneal endothelium. Descemet’s membrane may extend onto structures of the filtration angle (i.e., descemetization), and cellular material may be embedded within it as a result of transcorneal injections.

Cornea from a rabbit 1 day following a surgical procedure. The incision site (left) has coiling of Descemet’s membrane (right). H&E. 20× objective
Degeneration or loss of the corneal endothelium, with sufficient time, will result in irregular thickening of Descemet’s membrane. Since Descemet’s membrane is continuously laid down during the life of an animal, where the endothelium is healthy and active, Descemet’s membrane will continue to be expanded. In those areas where the endothelium is not actively laying down Descemet’s membrane, it gives the impression of local thinning, which is only a relative change.
The corneal endothelium is important in maintaining fluid balance within the corneal stroma, so a morphologic or functional loss of corneal endothelial cells results in diffuse corneal edema and opacification. When the inhibition is the result of a compound, the resulting opacity is often diffuse in comparison to localized injury. Intracameral implantation of medical devices can lead to a physical loss of the endothelium and may demonstrate this localized opacity. Compounds that are known to injure the corneal endothelium include 5-fluorouracil, local anesthetics, methylene blue, and tobramycin. Compounds such as methylhydrazine, 1,2-dichloroethane, 1,2-dibromoethane, and 1,2-dichloroethylene have been reported to cause corneal endothelial cell injury in animal studies, but not in humans [50]. With sufficient time, loss of the corneal endothelial cells causes irregular thinning of Descemet’s membrane from a lack of continuous deposition and normal thickening.
The corneal endothelium has limited regenerative capacity which does vary some by species. For example, endothelial cells of nonhuman primates, dogs, and cats enlarge and migrate instead of proliferating, but in the rabbit, endothelial cells proliferate but may not provide a functional barrier [220–222]. In humans, the endothelium is thought not to proliferate at all or, if it does, not at a rate sufficient to replace lost cells since there is decreased corneal endothelial density with age. Therefore, injury to the corneal endothelium in a toxicology study is generally not an acceptable result. Human corneal endothelium has been shown in vitro to have proliferative capacity, even from aged patients, but that capacity requires a strong mitogenic signal [223]. Similar observations have been made with corneas of other species, in that there is proliferative capacity when cultured in vitro, but there is still a tendency for decreased corneal endothelial density with age for rhesus macaques, rats, mice, and rabbits. At times, some limited endothelial proliferation can be observed in laboratory animals (Fig. 5.13).

Cornea from a dog that had a device implanted in the anterior chamber. The posterior surface of the cornea has a focal area of endothelial hyperplasia. H&E. 20× objective
With the limited regenerative capacity of the corneal endothelium, the loss of corneal endothelium is repaired by spreading and decreased density of the existing endothelium (Fig. 5.14). This can manifest as attenuation microscopically, where corneal endothelial nuclei are fewer and spaced farther apart. Detection of such a change requires detailed comparison with concurrent controls and consistent orientation of the eye, since there are differences in endothelial density dorsally as compared to ventrally. However, this is probably better assessed with specular microscopy, described elsewhere in this book. With a greater degree of endothelial loss, where the remaining endothelium cannot migrate and spread over the defect, a fibrous membrane (i.e., retrocorneal membrane) may form [224] (Fig. 5.15). The origin of the retrocorneal membrane is thought to be from keratocytes or from corneal endothelial cells that have undergone a metaplastic change to fibrocytes [225]. A retrocorneal membrane would be expected to result in permanent corneal opacity in affected areas. Loss of endothelium may also result in adherence of the iris to the posterior corneal surface which is anterior synechia.

Cornea from a monkey that had a device implanted in the anterior chamber. The inferior cornea (a) has a paucity of endothelial cells as compared to the superior cornea (b). The corneal endothelium is attenuated and widely spaced. H&E. 20× objective

Cornea from a rabbit 2 weeks after a surgical procedure. A retrocorneal membrane has formed at the incision site on the posterior surface of the cornea where the endothelium was lost. Note the disorganization of the stroma at the incision site and the cross sections of suture material. H&E. 10× objective
Injury to endothelial cells can be recognized ultrastructurally as loss of surface microvilli, alterations in surface apical processes, rounding of cells, separation of cells, death, and loss of cells from the basement membrane. In response to cellular stress, endothelial cells produce excess basement membrane that accumulates between the basal surface of the endothelial cells and Descemet’s membrane. This may progress to the above-mentioned fibrous metaplasia and the formation of a retrocorneal membrane [17]. Protective mechanisms associated with glutathione are important in maintaining cell viability. Endothelial cells may be damaged directly by instillation of material into the anterior chamber during surgical procedures [17].
Chemical features in the local environment including ionic concentration, bicarbonate levels, pH, and tonicity affect the corneal endothelium. Damage to endothelial cells can generally be categorized into two major mechanisms: alterations in passive permeability or alterations in function. For example, benzalkonium chloride, a surfactant, will cause endothelial cell separation and therefore will increase permeability. Dimethyl sulfoxide has been associated with corneal opacification, and this may also reasonably be related to increased permeability of the endothelial layer. Hydrogen peroxide and other drugs or substances that inhibit catalase or glutathione activity will affect endothelial membranes and ion pumps due to the increases in free radicals. Drugs that affect the endothelium can reach the anterior chamber by direct diffusion if given topically or through filtration during the formation of aqueous fluid if given systemically. Damage to the endothelium can also be a secondary event to the administration of phototoxic chemicals such as rose bengal or chlorpromazine, which produce free radicals when exposed to ultraviolet or visible spectrum light [226–228]. Anything that may affect corneal endothelial metabolism and the function of sodium-potassium ATPase pumps may result in corneal swelling.
Fischer 344 rats have been described with endothelial dystrophy. Dense opacities are observed unilaterally or bilaterally in the deep cornea as spots of 1–2 mm in size. These may be caused by antidepressants in young F344 rats [229].
5.6 Sclera and Episclera
The sclera is composed of collagenous connective tissue and serves as a supportive frame for the globe [4, 7]. The vascularized layer between the bulbar conjunctiva and the sclera is the episclera.
5.6.1 Scleral and Episcleral Alterations
The sclera is generally not primarily involved in ocular toxicity but may be secondarily involved such as being diffusely stretched when the globe enlarges (i.e., buphthalmos) due to glaucoma or due to focal stretching (i.e., ectasia) secondary to posterior coloboma. Osseous or cartilaginous metaplasia of the sclera occurs as an aging change in rats (Fischer 344) [76]. Posteriorly, drugs may be deposited in the suprachoroidal space [230] or sub-Tenon’s space near the macula in primates.
The episclera may contain mononuclear or mixed inflammatory cells secondary to irritation or inflammation of the cornea. With the increasing development of intraocular therapies, the sclera is frequently a barrier that must be breached, such that incision sites and sutures or injection tracks may be apparent in section. Healing of the sclera is mostly by cells from the episclera. With small, uncomplicated wounds, there is ingrowth of fibroblasts and occasionally of blood vessels either from the episclera or the uvea. With larger wounds, there may be incarceration or prolapse of other ocular tissues.
The only known drug class that specifically affects the sclera is the bisphosphonates [231]. In humans, bisphosphonates, specifically pamidronate, have been shown to cause scleritis within 6–48 h post intravenous injection. Bisphosphonates in general can cause ophthalmitis, but the scleritis appears to be specific for this drug class.
5.7 Conjunctiva
The corneal epithelium abruptly becomes bulbar conjunctiva at the limbus. The bulbar conjunctiva covers the episclera and extends as palpebral conjunctiva onto the inner surface of the eyelids and over the third eyelid [4, 7, 112]. Conjunctiva is composed of a single row of epithelial cells that appear as squamous epithelium near the palpebral margins and goblet cells in areas less exposed. The density of goblet cells is not homogeneous in the palpebral conjunctiva.
The conjunctival epithelium is supported by an underlying connective tissue stroma that contains lymphoid aggregates in nonrodents referred to as conjunctiva-associated lymphoid tissue (CALT) and is generally considered to be part of the mucosa-associated lymphoid tissue (MALT) system [232–235]. Some authors have in the past identified this as chronic inflammation and if exuberant, it very well may be. Rats and mice do not normally have lymphoid follicles in the conjunctiva, such that their formation in that location should be considered an abnormality [232]. As determined by evaluating rabbits, newborns have no lymphoid follicles in the conjunctiva, while adolescents have rapidly increasing amounts of lymphoid tissue that stabilizes during young adulthood and steadily declines with advancing age [236]. The lymphoid tissue in the conjunctiva is greater in the palpebral conjunctiva than in the bulbar conjunctiva and greater in the conjunctiva of the upper lid than the lower lid [235]. The conjunctival lymphoid tissue is largely located such that it overlies the cornea when the lids are closed, which is thought to be an important part of ocular immune surveillance [234]. The lymphoid tissue exists as individual lymphocytes and plasma cells scattered in the stroma as well as well-defined follicles, some of which will have germinal centers. It is important to note the relative amounts of lymphoid tissues when examining the conjunctiva of the eye, as increases or decreases may be related to test article administration, especially when that administration is ocular. Decreases in number and size of lymphoid follicles can be observed with the topical administration of anti-inflammatory agents. The nictitating membrane is also a site where lymphoid tissue is frequently present and should be considered part of the CALT.
The limbus, which is the border between the conjunctiva and the cornea, will often have small aggregates of lymphocytes in the stroma subjacent to the epithelium. These are common findings in monkeys, dogs, and rabbits but, like CALT, do not occur in normal rats and mice.
The palpebral conjunctiva of rabbits often contains a few heterophils which may increase in number as a response to irritation or infection.
5.7.1 Conjunctival Alterations
Inflammation of the conjunctiva (i.e., conjunctivitis) is often associated with corneal inflammation or inflammation of the anterior segment. This is because the cornea is continuous with the conjunctiva and because the conjunctiva is the source of vessel for corneal vascularization and a route for ingress of inflammatory cells into the cornea and anterior chamber. On gross examination, the inflammation will be manifested as hyperemia or congestion and edema (i.e., chemosis) of the mucous membranes. If there was previous hemorrhage, gross discoloration of the conjunctiva may be visible, or hemosiderin pigment deposition may be present in histologic section. Conjunctivitis and keratoconjunctivitis are reported infrequently as spontaneous changes in laboratory animals with the majority of papers describing it in nonhuman primates more so than other species [126, 136, 237, 238]. However, the incidence reported in nonhuman primates is approximately 1% [238].
Acute conjunctivitis may present with grossly identifiable exudates, consisting of mucus, sloughed epithelial cells, exudation of serous fluid and fibrin, and inflammatory cells. If the injury is great enough, this exudate can form a pseudomembrane adhered to the conjunctiva and cornea, or if there is loss of epithelium, it can form a tightly adherent true membrane. Grossly, there will likely also be chemosis and hyperemia of conjunctival vessels. Conjunctivitis frequently occurs in rabbits and is often due to bacteria which may have gained access to the conjunctival sac via the nasolacrimal duct. Eyelids may be swollen or closed with serous, mucous, or purulent discharge [239]. If chronic, the discharge can cause a loss of hair on the face below the medial canthus. Inflammation may be associated with respiratory disease, and Pasteurella multocida is frequently cultured. However, this organism can be present in grossly normal eyes.
With chronic conjunctivitis, a spectrum of changes may occur, depending on the duration, severity, and cause of the injury. Goblet cells are often increased in number, and the epithelium is hyperplastic with crypt-like infoldings. Lymphoid follicles may be increased in number and prominence, enough so that they are readily apparent on a careful gross examination. Vessels may also have perivascular infiltrates of inflammatory cells.
Sequela of conjunctivitis may include the continued increased density of goblet cells and epithelial folds. However, if there is epidermalization, there may actually be decreases in or an absence of goblet cells, due to the transition to a stratified squamous epithelium. In some instances, this stratified squamous epithelium may be keratinizing. With stromal scarring, the eye may become dry (i.e., xerophthalmia) due to constriction and obstruction of lacrimal glands and decreases in goblet cells.
Various agents can cause conjunctivitis, and many of those mentioned causing keratitis will also produce conjunctivitis. Ricin topically applied to the eyes is an exception, where the conjunctiva and sclera will develop a necrotizing inflammatory reaction; the cornea will have only a sparse neutrophilic infiltrate limited to the most peripheral areas [240].
Miscellaneous conjunctival alterations include amyloidosis, squamous cell metaplasia, squamous papilloma, squamous cell carcinoma, mucoepidermoid carcinoma, microgranuloma, and pseudopterygium [49]. Conjunctival microgranuloma may appear in the bulbar conjunctiva of older rats. The finding consists of small accumulations of macrophages with calcific deposits beneath the conjunctival epithelium and may occur with corneal mineralization [127, 131, 187]. Pseudopterygium is characterized by a sheet-like overgrowth of bulbar conjunctiva that extends over the cornea in the rabbit. Pseudopterygium is a spontaneous change infrequently observed [20]. The flap is not associated with irritation or inflammation. Microscopically, the flap consists of a loose connective tissue stroma covered by epithelium on both sides. There are usually no adhesions between the flap and either the eyelid or the cornea, and the flap of tissue will often grow back after removal.
The conjunctiva is one site of local application of test articles. When subconjunctival injections are part of the study design, the conjunctiva should be evaluated microscopically, especially in the area of the injection. With depot injections, granulomas and other reactions may be observed (Fig. 5.16).

Conjunctiva from a rabbit given a subconjunctival depot injection. The loose connective tissue is expanded by an aggregate of foamy macrophages and multinucleate giant cells. H&E. 5× objective
5.8 Uvea
The uvea or the vascular tunic of the globe includes the iris, ciliary body, and choroid [4, 7, 32, 241]. The choroid includes the tapetum lucidum in some species.
Since the uvea is the vascular tunic of the eye, it is often involved in intraocular inflammation. Intraocular inflammation needs to be prevented or minimized quickly in order to prevent permanent damage to the specialized structures of the eye. Ocular immunity is reviewed by Biros [242] but includes features such as a blood-eye barrier, an absence of lymphatic vessels, a semiconfined microenvironment, tissue-specific antigen presenting cells, and innate immune cells [242].
5.8.1 Uveal Alterations
Drug-induced morphological changes involving the uvea of laboratory animals consist of edema, inflammation, degeneration, abnormal pigmentation, cytoplasmic vacuolation, cellular necrosis, or changes in the intraocular pressure (IOP). Colchicine, naphthol, and urethane cause edema, inflammation, or degeneration of the ciliary body [50]. Naphthalene causes degeneration of the ciliary body and the choroid, and pyrithione causes edema and degeneration of the choroid [50]. Drug-induced changes must be differentiated from spontaneous findings which may be congenital, traumatic, inflammatory, degenerative, metaplastic, and proliferative processes [46, 126, 243, 244].
5.8.1.1 Pigmentary Changes
Increased or decreased pigmentation may occur following administration of compounds [245]. Drug-induced darkening of the iris occurs in cynomolgus monkeys and humans with topical administration of the prostaglandin F2a analogs latanoprost, travoprost, and bimatoprost [246–248]. The increased pigmentation is due to an increase in melanin synthesis [249]. The sympathetic nervous system is important in the development of iris pigmentation [250].
Proliferation of melanin-containing cells in the iris may be induced in hooded rats treated neonatally with urethane [251], but was not observed when Wistar rats were used.
Depigmentation of the uvea may occur as a result of inflammation or edema.
5.8.1.2 Cytoplasmic Vacuolation
Cytoplasmic vacuolation may occur in the epithelium of the iris, ciliary body, or both and may be due to a variety of causes. A fairly common cause of vacuolation is due to phospholipids. This may be caused by many compounds and will vary by species. For example, disobutamide, a piperidine antiarrhythmic drug, causes vacuolation of the epithelial cells of the iris and other cells in dogs, but not rats [252]. Phospholipidosis may involve the pigmented iridal epithelial cells of monkeys and can cause alterations in the appearance of the tapetum lucidum in dogs. Other causes of vacuolation include dilation of the endoplasmic reticulum and cell swelling. Diffuse cytoplasmic vacuolation of the iridal and ciliary epithelium occurred in albino and pigmented rabbits treated with 6-aminonicotinamide [253]. Extensive cytoplasmic vacuolation of both pigmented and nonpigmented ciliary epithelial cells occurred in cynomolgus monkeys following administration of a novel anticancer agent [254]. The ciliary body appeared swollen and had a decreased amount of pigment.
5.8.1.3 Uveal Inflammation and Trauma
Inflammation of the uvea may be caused by an immunological or a toxicological mechanism [137, 255]. Drug-related inflammation of the anterior uvea occurs in humans and is associated with the antiviral cidovir, antituberculous drug ribafutin, palmidronic acid, sulfonamides, streptokinase, and topical metipranolol [256]. Acute inflammation occurs in the anterior uvea after injection of a compound such as an antiviral agent [257]. Inflammation of the uvea may be a manifestation of toxicity in animals, such as inflammation of the ciliary body (i.e., cyclitis) that occurs after administration of cyclophosphamide to rats [258].
Inflammation as a manifestation of toxicity must be differentiated from spontaneous inflammation occurring as a background change. Rats and aged mice may develop spontaneous inflammation of the anterior uvea (i.e., iridocyclitis) [126]. The NIH Hartley strain of guinea pig is susceptible to experimental autoimmune uveitis [259]. Mononuclear cell infiltration into the ciliary body (rabbits and monkeys), choroid (monkeys), iris (rabbit), and filtration angle (rabbit) is a nonspecific change that occurs relatively frequently [68, 260] (Fig. 5.17). In the rabbit, spontaneous anterior uveal inflammation is more common than choroidal inflammation, but unilateral uveal inflammation of undetermined cause may occur [261]. In dogs, inflammation of the choroid may cause the tapetum lucidum to have a red discoloration [261]. If intraocular inflammation persists, then secondary changes occur, such as adhesions or fibrosis [20].

Pars plana of the ciliary body of a monkey with infiltrates of lymphocytes. These are commonly observed as spontaneous changes in monkeys. H&E. 10× objective
Trauma to the globe, irritation from an intracameral (i.e., within the anterior chamber) injection, or implantation of a medical device may cause inflammation with or without secondary changes. Secondary ocular changes include adhesion of the iris to the lens (i.e., posterior synechia), adherence of the iris to the cornea (i.e., anterior synechia), ciliary edema, proteinaceous fluid in the anterior chamber (i.e., aqueous flare), neutrophils in the anterior chamber (i.e., hypopyon), or hemorrhage in the anterior chamber (i.e., hyphema). Injection of material into the vitreous cavity through the pars plana will leave an injection track. Ocular findings associated with the needle track include prolapse of the ciliary epithelium or the vitreous upon removal of the needle, or intravitreal inflammation. The iris may respond to surgical trauma or irritation by a fibroproliferative response in rabbits; a similar response may be observed in humans.
5.8.1.4 Miscellaneous Uveal Findings
Miscellaneous uveal findings may be associated with administration of a compound or may be spontaneous background changes. Iris atrophy is generally not observed in laboratory animals but may be found in (C57L X A/He) F1 mouse [167]. Initially, small holes appear that may coalesce with microscopic disorganization of the normal iridal appearance. The ciliary epithelial basement membranes of dogs may become thickened following administration of an anticholinesterase pesticide [262]. Systemic administration of silver lactate to rats results in silver grain deposition in the iris and ciliary body [263]. The deposits are located on the basement membranes and within the pigmented epithelial cells. Background findings include mineralization in the iris of rodents [264] or the presence of foci of heterotopic bone (i.e., osseous choristoma or osseous metaplasia) within the ciliary body of guinea pigs [208, 265, 266]. Fischer 344 rats, but not Sprague-Dawley rats, develop choroidal adiposity as a response to systemic PPAR-gamma agonist administration [267]. The choroidal adiposity is characterized by increased adipocytes between the choroid and the sclera.
5.8.1.5 Intraocular Pressure and Glaucoma
The IOP can be increased or decreased. Intraocular pressure may be increased by subconjunctival injections of compounds, intraocular injection of compounds, and by topical application of compounds, but other possibilities should also be considered. Drugs that dilate the pupil or limit the constriction of the pupil cause the anterior chamber to be shallow and the filtration angle to be narrow [268]. This may possibly lead to an increase in the IOP, and a prolonged increase in IOP results in structural changes (i.e., glaucoma). Obviously, glaucoma is a significant problem in human ophthalmology, and a variety of therapeutics and surgical techniques are aimed at decreasing IOP.
Features of glaucoma include increased size of the globe (i.e., buphthalmos or buphthalmia), breaks in Descemet’s membrane (i.e., stria), diffuse corneal edema, thinning of the tunics (i.e., retina, uvea, sclera), luxation of the lens, and cupping of the optic disc. Thinning of the retina begins with loss of the ganglion cells (i.e., inner retinal degeneration) followed by loss of neurons with cell bodies in the inner nuclear layer. As the globe becomes stretched, the sensory retina may become separated (i.e., retinal detachment) from the retinal pigment epithelium (RPE) leading to degeneration of photoreceptors (i.e., outer retinal degeneration).
Buphthalmos occurs as a unilateral or bilateral, autosomal recessive inherited defect in New Zealand white rabbits [269] (Fig. 5.18), and beagles may develop open-angle glaucoma as an inherited autosomal recessive disorder [270]. Glaucoma largely develops as a result of impaired drainage of aqueous humor from the anterior chamber from maldevelopment (i.e., goniodysgenesis) or secondary to other ocular findings. Abnormal development of structures of the filtration angle often involves faulty development of the pectinate ligament. When the pectinate ligament is poorly developed, the root of the iris is located adjacent to the peripheral margin of Descemet’s membrane. There may be splitting and extension of Descemet’s membrane onto structures around the pectinate ligament (i.e., descemetization). Increased production of aqueous has been suggested to be a cause of increased IOP, but demonstration of this cause is rare.

Trabecular meshwork from rabbits. (a) Congenital goniodysgenesis. Note the narrowing of the filtration angle and absences of trabecular meshwork for aqueous fluid filtration. The animal had buphthalmos and increased intraocular pressure. (b) Normal trabecular meshwork. H&E. 5× objective
The increased IOP causes a thin-walled globe, diffuse bluish corneal opacity, and cupping of the optic disc, especially because of the poorly developed lamina cribrosa in rabbits [271]. In general, enlargement of the globe may interfere with adequate hydration of the cornea resulting in drying of the cornea with possible inflammation (i.e., keratoconjunctivitis) and possibly corneal trauma [261, 272]. With time, secondary lens luxation and ciliary atrophy may occur. In addition to the development of glaucoma from maldevelopment (primary glaucoma), glaucoma may develop as a secondary effect.
Secondary glaucoma occurs when normal aqueous filtration becomes obstructed. Glaucoma may be secondary to inflammation, neoplasia, neovascular growth, or lens luxation [20]. For example, rodents develop glaucoma after inflammation in the anterior segment, particularly if adhesions occur [273–276]. Mechanical causes of secondary glaucoma include adhesion of the iris to the peripheral cornea (i.e., anterior synechia) or infiltration of the filtration meshwork by inflammatory or neoplastic cells, to mention a few causes. Older DBA/2J (D2) mice develop glaucoma due to dispersion of ocular pigment [277]. Affected mice develop elevated IOP pigment dispersion, pigment epithelial atrophy, anterior synechia, ganglion cell loss, optic disc cupping, and optic nerve atrophy. IOP may increase following administration of intraocular materials in laboratory animals. Some substances that obstruct aqueous outflow include particulates such as calcium carbonate, cotton, talc, sanguinarine, and India ink. Viscous solutions such as methyl cellulose can also slow aqueous outflow [50]. Other substances, such as alloxan, cresol, and phenol, destroy endothelial cells, including those lining the trabecular meshwork, causing an inflammatory reaction.
IOP may be decreased in some instances. Inflammation is an important cause of decreased IOP. Cardiac glycosides, including digitoxin, digoxin, lanatoside C, and ouabain reduce the IOP by interfering with the formation of aqueous through inhibition of Na/K-ATPase in the ciliary body. Iodoacetate and quinine reduce IOP by damage to the iris and ciliary body and reduction of aqueous production [50]. Topical application of prostaglandin F2c reduces IOP and increases the uveoscleral outflow resulting in edema and dilatation of intramuscular spaces of the ciliary body of cynomolgus monkeys [278].
5.8.1.6 Tapetal Alterations
Since dogs are commonly used in toxicity studies, alterations involving the tapetum lucidum are often observed in laboratory beagles [245]. Since the tapetum lucidum is not present in humans, treatment-related findings may not be relevant to human safety assessment [279]. To help determine if treatment-related tapetal findings have relevance to humans, beagles which do not have an observable tapetum lucidum are sometimes used [280]. These dogs have tapetal cells, but they are lacking intracytoplasmic rodlets [281]. For example, administration of imidazoquinoline to normal beagles results in tapetal and retinal changes, but the use of atapetal beagles results in no retinal changes [282].
The principal toxicity-related finding involving the tapetum lucidum is a loss of tapetal cells. Since young beagles are generally used for toxicity studies, age-related loss of tapetal cells can be eliminated as a possible cause for the loss [283, 284]. Degeneration or necrosis of tapetal cells may be accompanied by inflammation which may cause the tapetum lucidum to appear red or be absent [261]. Additional findings that may accompany tapetal cell degeneration include inflammation of the retina (i.e., chorioretinitis), edema, hemorrhage, or retinal detachment.
Toxicity involving the tapetum lucidum of beagles may be subdivided into zinc chelators and nonchelators. Since tapetal cells contain a high concentration of zinc, administration of zinc chelators, such as hydroxypyridinethione or pyrithione, to dogs causes tapetal and choroidal necrosis and edema with a secondary retinopathy [254, 261, 285, 286]. Administration of the zinc chelator ethambutol causes fluffy-white discoloration of the tapetum [261]. This change is reversible and is probably due to altered refraction because of disorganization of tapetal cell rodlets. Administration of hydroxypyridinethione results in retinal edema and detachment in addition to tapetal cell necrosis [261]. Administration of the chelating agent pyrithione also causes tapetal and choroidal necrosis and edema [254, 288].
Toxicity involving the tapetum lucidum of beagles is observed with nonchelators such as enrofloxcin, CGS14796C (a potential aromatase inhibitor), 1192U90 (an antipsychotic agent), dithizone, edentate, and ethylenediamine derivatives [50, 289, 290]. Compounds that do not cause chelation may also cause tapetal edema, degeneration, retinal edema, and retinal detachment in dogs and tapetal atrophy in cats [291]. These changes were specific for the tapetum since no retinal changes were observed in primates, rats, rabbits, or atapetal beagles [50].
5.8.1.7 Developmental Uveal Findings
Findings associated with toxicity of the uvea of laboratory animals must be differentiated from spontaneous uveal findings. Many of the spontaneous findings are congenital and easily differentiated from a finding associated with toxicity by being observed during the prestudy ocular examination. Developmental anomalies involving the uvea may be unilateral or bilateral, occur in a variety of laboratory animals (rat, mice, hamster, rabbit, beagle dog), and include ectopic pupil (beagle dog), persistent pupillary membrane or strands (beagle dog, Sprague-Dawley rat, Crj:CD (SD) rat, Göttingen minipig, Yucatan micropig, mice, Syrian hamster), iridal coloboma (rat), posterior coloboma (beagle dog, rat), and alterations in iridal color [47, 100, 125, 126, 129, 261, 292–294].
5.8.1.8 Uveal Neoplasia
In general, spontaneous uveal neoplasia rarely occurs in the common laboratory animals. In mice, they are generally malignant, with the exception of iridal adenoma of the nonpigmented iridal epithelium [167]. Some neoplasms metastasize to the globe (e.g., harderian gland carcinoma) or may be induced, such as fibrosarcoma induced by intraocular implantation of a suture containing 20-methylcholanthrene [169].
Rats develop spindle cell neoplasms which include uveal malignant melanoma [295], uveal leiomyoma [296], and malignant and benign intraocular Schwannoma [297]. In guinea pigs, malignant lymphoma, including T cell lymphoma and reticulosarcoma, has been reported to involve the choroid [298, 299], and uveal malignant melanoma has been reported in rabbits [300]. In the mouse, secondary tumors, such as malignant lymphoma and harderian gland carcinoma, can spread to the globe [167, 301, 302].
Spontaneously occurring uveal melanomas have been reported in albino rat strains including Sprague-Dawley, Wistar, and F344 [49]. Uveal melanomas in the rat consist of bundles and whorls of spindle-shaped cells with a perivascular orientation, possibly containing epithelioid cells and areas of necrosis. Mitotic figures may be numerous. The neoplasm generally involves the anterior uvea but may involve the choroid and extend into adjacent ocular structures. Neoplastic cells are positive for S-100 protein and vimentin intermediate filament.
Uveal malignant melanoma is generally not a neoplasm that occurs in albino mice and is rare in pigmented mice, such as B6C3F1 mice [81, 302]. In B6C3F1/Cr1BR mice, intraocular melanomas are noninvasive, well-pigmented, epithelioid neoplasms originating in the choroid with no metastasis [302]. In these mice, malignant melanoma usually originates in a lymphoid organ and metastasizes to the choroid resulting in retinal detachment [167]. Uveal malignant melanoma in the mouse may metastasize to the lymph node, spleen, and thymus.
Uveal melanoma has been induced by intravitreal instillation of nickel subsulfide or N-methyl-N-nitrosourea and by oral administration of ethionine combined with 2-acetylaminofluorene [303, 304]. Uveal melanoma has been induced in pigmented August hooded rats by subcutaneous injection of urethane or N-hydroxyurethane during the neonatal period [49]. Metastasis to the lung has been reported.
Uveal leiomyoma in the rat consists of whorls of spindle cells, occasionally around blood vessels, that are reported to be positive for desmin [296]. The cells contain myofibrils that can be demonstrated with phosphotungstic acid hematoxylin (PTAH) stains and by transmission electron microscopy.
Intraocular schwannoma arises from the iris or ciliary body but involves adjacent ocular structures [75]. The neoplasm is composed of plump spindle-shaped cells with abundant eosinophilic cytoplasm arranged in parallel rows and palisades around blood vessels. Neoplastic cells may have positive immunoreactivity for S-100, and desmosomes may be detected, ultrastructurally. Mitotic figures may be numerous and areas of necrosis may be present.
References
Smith RS, Nishina PM, Ikeda S, Jewett P, Zabaleta A, John SWM. Interpretation of ocular pathology in genetically engineered and spontaneous mutant mice. In: Ward JM, Mahler JF, Maronpot RR, editors. Pathology of genetically engineered mice. Ames: Iowa State University Press; 2000. p. 217–31.
Prince JH. The rabbit in eye research. Springfield: Charles C Thomas Pub.; 1964.
Prince JH. Comparative anatomy of the eye. Springfield: Charles C Thomas Pub.; 1956.
Samuelson DA. Ophthalmic anatomy. In: Gelatt KN, editor. Veterinary ophthalmolgy. 4th ed. Ames: Blackwell; 2007. p. 37–148.
Kuiper B, Boeve MH, Jansen T, Roelofs-van Emden ME, Thuring JW, Wijnands MV. Ophthalmologic examination in systemic toxicity studies: an overview. Lab Anim. 1997;31(2):177–83.
Munger RJ. Veterinary ophthalmology in laboratory animal studies. Vet Ophthalmol. 2002;5(3):167–75.
Rubin LF. Comparative anatomy of the eye. In: Hockwin O, Green K, Rubin LF, editors. Manual of oculotoxicity testing of drugs. Stuttgart: Gustav Fischer Verlag; 1992. p. 12–44.
Schiavo DM. Special topics about the use of laboratory animals in toxicology – an ophthalmoscopic assessment. In: Hockwin O, Green K, Rubin LF, editors. Manual of oculotoxicity testing of drugs. Stuttgart: Gustav Fischer Verlag; 1992. p. 9–20.
Short BG. Safety evaluation of ocular drug delivery formulations: techniques and practical considerations. Toxicol Pathol. 2008;36(1):49–62.
Aguirre GD, Rubin LF, Bistner SI. Development of the canine eye. Am J Vet Res. 1972;33(12):2399–414.
Cook C, Sulik K, Wright K. Embryology. In: Wright KW, editor. Pediatric ophthalmology and strabismus. St. Louis: Mosby-Year Book; 1995. p. 3–59.
Cook CS. Ocular embryology and congenital malformations. In: Gelatt KN, editor. Veterinary ophthalmology. 4th ed. Ames: Blackwell Publishing; 2007. p. 3–36.
O’Rahilly R. The timing and sequence of events in the development of the human eye and ear during the embryonic period proper. Anat Embryol (Berl). 1983;168(1):87–99.
Stromland K, Miller M, Cook C. Ocular teratology. Surv Ophthalmol. 1991;35(6):429–46.
Smith RS, Koa WW-Y, John SWM. Ocular development. In: Smith RS, editor. Systematic evaluation of the mouse eye: anatomy, pathology, and biomethods. Boca Raton: CRC Press; 2002. p. 45–63.
Hoar RM. Embryology of the eye. Environ Health Perspect. 1982;44:31–4.
Whiteley HE, Peiffer RL. The eye. In: Haschek WM, Rousseaux CG, editors. Haschek and Rousseaux’s handbook of toxicologic pathology. Salt Lake City: Academic; 2002. p. 539–84.
Ramos M, Reilly CM, Bolon B. Toxicological pathology of the retina and optic nerve. In: Bolon B, Butt MT, editors. Fundamental neuropathology for pathologists and toxicologists: principles and techniques. Hoboken: Wiley; 2011. p. 385–412.
Somps CJ, Greene N, Render JA, Aleo MD, Fortner JH, Dykens JA, et al. A current practice for predicting ocular toxicity of systemically delivered drugs. Cutan Ocul Toxicol. 2009;28(1):1–18.
Dubielzig R, Ketring KL, McLellan GJ, Albert DM. Veterinary ocular pathology: a comparative review. Edinburgh: Saunders Elsevier; 2010.
Saunders LZ, Rubin LF. Ophthalmic pathology of animals. New York: S. Karger; 1975.
Thompson SW, Luna LG. An atlas of artifacts encountered in the preparation of microscopic tissue sections. Springfield: Charles C Thomas Pub.; 1978.
Fix AS, Garman RH. Practical aspects of neuropathology: a technical guide for working with the nervous system. Toxicol Pathol. 2000;28(1):122–31.
Smith RS, Hawes NL, Miller J, Sundberg JP, John SWM. Photography and necropsy. In: Smith RS, editor. Systematic evaluation of the mouse eye: anatomy, pathology, and biomethods. Boca Raton: CRC Press; 2002. p. 251–64.
Luna LG. Manual of histology staining methods of the Armed Forces Institute of Pathology. 3rd ed. New York: McGraw-Hill Book Co.; 1968.
Preece A. A manual for histotechnologists. 3rd ed. Boston: Little, Brown and Co.; 1972.
Sheehan DC, Hrapchak BB. Theory and practice of histotechnology. 2nd ed. Columbus: Battelle; 1980.
Saby JA, Sigler RE, Klaus S. Comparison of fixatives for histologic evaluation of the canine eye. J Histotechnol. 1991;14:251–5.
Yanoff M, Fine BS. Glutaraldehyde fixation of routine surgical eye tissue. Am J Ophthalmol. 1967;63(1):137–40.
Feeney-Burns L, Burns RP, Anderson RS. Ultrastructure and acid phosphatase activity in hereditary cataracts of deer mice. Invest Ophthalmol Vis Sci. 1980;19(7):777–88.
Anderson R, Shearer TR. Glycol methacrylate sections of the crystalline lens. Stain Technol. 1986;61(6):381–2.
Weisse I. Microscopic examination of the eye. In: Hockwin O, Green K, Rubin LF, editors. Manual of oculotoxicity testing of drugs. Stuttgart: Gustav Fischer Verlag; 1992. p. 137–63.
Latendresse JR, Warbrittion AR, Jonassen H, Creasy DM. Fixation of testes and eyes using a modified Davidson’s fluid: comparison with Bouin’s fluid and conventional Davidson’s fluid. Toxicol Pathol. 2002;30(4):524–33.
Humason GL. Histochemistry and special procedures. Animal tissue techniques. San Francisco: Freeman; 1979.
Levy MC, Covatta TJ, Morris C, Aschner HH. Technique for preparing histologic sections of dogs’ and rabbits’ eyes in paraffin. Arch Ophthalmol. 1965;73:122–3.
Georger M. Concepts in the routine preparation of eye specimens. Histo-Logic. 2002;2:34–6.
Prophet EB. Technique for processing eye specimens. Histo-Logic. 1976;1:75–6.
Lee ES, Flannery JG. Transport of truncated rhodopsin and its effects on rod function and degeneration. Invest Ophthalmol Vis Sci. 2007;48(6):2868–76.
Smith RS, Zabeleta A, John SWM, Bechtold LS, Ikeda S, Relyea MJ, et al. General and special histopathology. In: Smith RS, editor. Systematic evaluation of the mouse eye: anatomy, pathology, and biomethods. Boca Raton: CRC Press; 2002. p. 265–97.
Duncan S. Microtomy and staining of cataract lens. Histo-Logic. 1981;11:160–1.
Lewis PA. Ocular Histology. 27th Annual Symposium/Convention, National Society for Histotechnology; Sept 22-27; Charlotte, NC2001.
Bermudez MA, Vicente AF, Romero MC, Arcos MD, Abalo JM, Gonzalez F. Time course of cold cataract development in anesthetized mice. Curr Eye Res. 2011;36(3):278–84.
Delaye M, Clark JI, Benedek GB. Identification of the scattering elements responsible for lens opacification in cold cataracts. Biophys J. 1982;37(3):647–56.
Lo WK. Visualization of crystallin droplets associated with cold cataract formation in young intact rat lens. Proc Natl Acad Sci U S A. 1989;86(24):9926–30.
Eglitis I. The orbital fascia. In: Prince JH, editor. The rabbit in eye research. Springfield: Charles C. Thomas Pub.; 1964. p. 28–37.
Hubert MF, Gerin G, Durand-Cavagna G. Spontaneous ophthalmic lesions in young Swiss mice. Lab Anim Sci. 1999;49(3):232–40.
Loget O. Spontaneous ocular findings and esthesiometry/tonometry measurement in the Göttingen minipig (Conventionally and microbiologically defined). In: Weisse I, Tripathi RC, Hockwin O, editors. Ocular toxicology. New York: Springer; 1995. p. 351–62.
LeDoux MS, Zhou Q, Murphy RB, Greene ML, Ryan P. Parasympathetic innervation of the meibomian glands in rats. Invest Ophthalmol Vis Sci. 2001;42(11):2434–41.
Ackerman LJ, Yoshitomo K, Fix AS, Render JA. Proliferative lesions of the eye in rats. OSS. Guides for Toxicologic Pathology. Washington, D.C.: STP/ARP/AFIP; 1998.
Grant WM. Toxicology of the eye. 3rd ed. Springfield: Charles C. Thomas Pub.; 1986.
Fischbein A, Rizzo JN, Solomon SJ, Wolff MS. Oculodermatological findings in workers with occupational exposure to polychlorinated biphenyls (PCBs). Br J Ind Med. 1985;42(6):426–30.
Ohnishi Y, Kohno T. Polychlorinated biphenyls poisoning in monkey eye. Invest Ophthalmol Vis Sci. 1979;18(9):981–4.
Brewster DW, Elwell MR, Birnbaum LS. Toxicity and disposition of 2,3,4,7,8-pentachlorodibenzofuran (4PeCDF) in the rhesus monkey (Macaca mulatta). Toxicol Appl Pharmacol. 1988;93(2):231–46.
Arnold DL, Bryce F, Stapley R, McGuire PF, Burns D, Tanner JR, et al. Toxicological consequences of Aroclor 1254 ingestion by female rhesus (Macaca mulatta) monkeys. Part 1A. Prebreeding phase: clinical health findings. Food Chem Toxicol. 1993;31(11):799–810.
Tryphonas L, Truelove J, Zawidzka Z, Wong J, Mes J, Charbonneau S, et al. Polychlorinated biphenyl (PCB) toxicity in adult cynomolgus monkeys (M. fascicularis): a pilot study. Toxicol Pathol. 1984;12(1):10–25.
Tryphonas L, Arnold DL, Zawidzka Z, Mes J, Charbonneau S, Wong J. A pilot study in adult rhesus monkeys (M. mulatta) treated with Aroclor 1254 for two years. Toxicol Pathol. 1986;14(1):1–10.
Jester JV, Nicolaides N, Kiss-Palvolgyi I, Smith RE. Meibomian gland dysfunction. II. The role of keratinization in a rabbit model of MGD. Invest Ophthalmol Vis Sci. 1989;30(5):936–45.
Kremer I, Gaton DD, David M, Gaton E, Shapiro A. Toxic effects of systemic retinoids on meibomian glands. Ophthalmic Res. 1994;26(2):124–8.
Lambert RW, Smith RE. Pathogenesis of blepharoconjunctivitis complicating 13-cis-retinoic acid (isotretinoin) therapy in a laboratory model. Invest Ophthalmol Vis Sci. 1988;29(10):1559–64.
Bryce F, Iverson F, Andrews P, Barker M, Cherry W, Mueller R, et al. Effects elicited by toxaphene in the cynomolgus monkey (Macaca fascicularis): a pilot study. Food Chem Toxicol. 2001;39(12):1243–51.
Hejkal TW, Camras CB. Prostaglandin analogs in the treatment of glaucoma. Semin Ophthalmol. 1999;14(3):114–23.
Johnstone MA, Albert DM. Prostaglandin-induced hair growth. Surv Ophthalmol. 2002;47 Suppl 1:S185–202.
Al-Jazzaf AM, DeSantis L, Netland PA. Travoprost: a potent ocular hypotensive agent. Drugs Today (Barc). 2003;39(1):61–74.
Law SK. Bimatoprost in the treatment of eyelash hypotrichosis. Clin Ophthalmol. 2010;4:349–58.
Prince JH, Eglitis I. Extraocular muscles. The rabbit in eye research. Springfield: Charles C Thomas Pub.; 1964. p. 57–71.
O’Steen WK, Kraeer SL, Shear CR. Extraocular muscle and Harderian gland degeneration and regeneration after exposure of rats to continuous fluorescent illumination. Invest Ophthalmol Vis Sci. 1978;17(9):847–56.
Katsuta O, Yamaguchi-Onozawa M, Okazaki K, Itoh T, Okazaki Y, Tsuchitani M. Gross and microscopic anatomy of the extraorbital lacrimal gland of the common marmoset (Callithrix jacchus). Comp Med. 2000;50(6):609–12.
Greaves P. Histopathology of preclinical toxicity studies. 3rd ed. New York: Academic; 2007.
Sakai T. The mammalian harderian gland: morphology, biochemistry, function and phylogeny. Arch Histol Jpn. 1981;44(4):299–333.
Nagai M, Nagai T, Yamamoto M, Goto K, Bishop TR, Hayashi N, et al. Novel regulation of delta-aminolevulinate synthase in the rat harderian gland. Biochem Pharmacol. 1997;53(5):643–50.
Eglitis I. The glands. In: Prince JH, editor. The rabbit in eye research. Springfield: Charles C. Thomas Pub.; 1964. p. 38–56.
Sullivan DA, Jensen RV, Suzuki T, Richards SM. Do sex steroids exert sex-specific and/or opposite effects on gene expression in lacrimal and meibomian glands? Mol Vis. 2009;15:1553–72.
Krinke AL, Schaetti PH, Krinke GJ. Changes in the major ocular glands. In: Mohr U, Dungworth DL, Capen CC, editors. Pathobiology of the aging rat. Washington, DC: ILSI Press; 1994.
Spike RC, Johnston HS, McGadey J, Moore MR, Thompson GG, Payne AP. Quantitative studies on the effects of hormones on structure and porphyrin biosynthesis in the harderian gland of the female golden hamster: I. The effects of ovariectomy and nitrogen administration. J Anat. 1985;142:59–72.
Mohr U. Fascicle No. 7: Central Nervous System, Heart, Eye, Mesothelium. In: Mohr U, editor. International Classification of Rodent Tumours: Part 1: The Rat, IARC Publications, No 122. Lyon: World Health Organization, International Agency for Research on Cancer; 1994. p. 34-51.
Yoshitomo K, Boorman GA. Eye and associated glands. Pathology of the Fischer rat: reference and atlas. San Diego: Academic Press; 1990. p. 239–59.
Sashima M, Hatakeyama S, Satoh M, Suzuki A. Harderianization is another sexual dimorphism of rat exorbital lacrimal gland. Acta Anat (Basel). 1989;135(4):303–6.
Breider MA, Bleavins MR, Reindel JF, Gough AW, de la Iglesia FA. Cellular hyperplasia in rats following continuous intravenous infusion of recombinant human epidermal growth factor. Vet Pathol. 1996;33(2):184–94.
Haseman JK, Hailey JR, Morris RW. Spontaneous neoplasm incidences in Fischer 344 rats and B6C3F1 mice in two-year carcinogenicity studies: a national toxicology program update. Toxicol Pathol. 1998;26(3):428–41.
Goodman DG, Ward JM, Squire RA, Chu KC, Linhart MS. Neoplastic and nonneoplastic lesions in aging F344 rats. Toxicol Appl Pharmacol. 1979;48(2):237–48.
Krinke GJ, Fix AS, Jacobs M, Render JA, Weisse I. Eye and harderian gland. In: Mohr U, editor. International classification of rodent tumors the mouse. Heidelberg: Springer; 2001. p. 347–59.
Parsons JT. Radiation toxicity to the visual system. J Neuroophthalmol. 2004;24(3):193–4.
Stephens LC, Schultheiss TE, Peters LJ, Ang KK, Gray KN. Acute radiation injury of ocular adnexa. Arch Ophthalmol. 1988;106(3):389–91.
Gazda MJ, Schultheiss TE, Stephens LC, Ang KK, Peters LJ. The relationship between apoptosis and atrophy in the irradiated lacrimal gland. Int J Radiat Oncol Biol Phys. 1992;24(4):693–7.
Kaswan RL, Martin CL, Chapman Jr WL. Keratoconjunctivitis sicca: histopathologic study of nictitating membrane and lacrimal glands from 28 dogs. Am J Vet Res. 1984;45(1):112–8.
Tanaka N, Ohkawa T, Hiyama T, Nakajima A. Evaluation of ocular toxicity of two beta blocking drugs, carteolol and practolol, in beagle dogs. J Pharmacol Exp Ther. 1983;224(2):424–30.
Trepanier LA. Idiosyncratic toxicity associated with potentiated sulfonamides in the dog. J Vet Pharmacol Ther. 2004;27(3):129–38.
Barnett KC, Joseph EC. Keratoconjunctivitis sicca in the dog following 5-aminosalicylic acid administration. Hum Toxicol. 1987;6(5):377–83.
Zoukhri D, Macari E, Kublin CL. A single injection of interleukin-1 induces reversible aqueous-tear deficiency, lacrimal gland inflammation, and acinar and ductal cell proliferation. Exp Eye Res. 2007;84(5):894–904.
Kimura-Shimmyo A, Kashiwamura S, Ueda H, Ikeda T, Kanno S, Akira S, et al. Cytokine-induced injury of the lacrimal and salivary glands. J Immunother. 2002;25 Suppl 1:S42–51.
Api AM, Smith RL, Pipino S, Marczylo T, De Matteis F. Evaluation of the oral subchronic toxicity of AHTN (7-Acetyl-1,1,3,4,4,6-hexamethyl-1,2,3,4-tetrahydronaphthalene) in the rat. Food Chem Toxicol. 2004;42(5):791–801.
Tsuchitani M, Narama I, Kohda S. Accumulation of pigment granules in lacrymal gland epithelium in practolol-treated beagle dogs. J Comp Pathol. 1989;100(3):237–43.
Slatter DH, Davis WC. Toxicity of phenazopyridine. Electron microscopical studies of canine lacrimal and nictitans glands. Arch Ophthalmol. 1974;91(6):484–6.
Keegan DJ, Geerling G, Lee JP, Blake G, Collin JR, Plant GT. Botulinum toxin treatment for hyperlacrimation secondary to aberrant regenerated seventh nerve palsy or salivary gland transplantation. Br J Ophthalmol. 2002;86(1):43–6.
Suwan-apichon O, Rizen M, Rangsin R, Herretes S, Reyes JM, Lekhanont K, et al. Botulinum toxin B-induced mouse model of keratoconjunctivitis sicca. Invest Ophthalmol Vis Sci. 2006;47(1):133–9.
Dethloff LA, Wilga P, Seefeld M, Ulloa H, Hawkins K, Petrere J. Effects of sustained low-level muscarinic agonism in rats. Food Chem Toxicol. 1994;32(8):753–62.
Majeed SK, Gopinath C, Heywood R. A report on drug-induced kerato-conjunctivitis sicca in dogs. J Comp Pathol. 1987;97(4):385–91.
Mason G, Wilson D, Hampton C, Wurbel H. Non-invasively assessing disturbance and stress in laboratory rats scoring chromodacryorrhea. Alt Lab Anim. 2004;32(Supple 1):153–9.
Harkness JE, Ridgway MD. Chromodacryorrhea in laboratory rats (Rattus norvegicus): etiologic considerations. Lab Anim Sci. 1980;30(5):841–4.
Heywood R. Some clinical observations on the eyes of Sprague-Dawley rats. Lab Anim. 1973;7(1):19–27.
McGee MA, Maronpot RR. Harderian gland dacryoadenitis in rats resulting from orbital bleeding. Lab Anim Sci. 1979;29(5):639–41.
Kurisu K, Sawamoto O, Watanabe H, Ito A. Sequential changes in the harderian gland of rats exposed to high intensity light. Lab Anim Sci. 1996;46(1):71–6.
Strum JM, Shear CR. Constant light exposure induces damage and squamous metaplasia in harderian glands of albino mice. Tissue Cell. 1982;14(1):149–61.
Travlos GS, Mahler J, Ragan HA, Chou BJ, Bucher JR. Thirteen-week inhalation toxicity of 2- and 4-chloronitrobenzene in F344/N rats and B6C3F1 mice. Fundam Appl Toxicol. 1996;30(1):75–92.
Libretto SE. A review of the toxicology of salbutamol (albuterol). Arch Toxicol. 1994;68(4):213–6.
Herrold KM. Aflatoxin induced lesions in Syrian hamsters. Br J Cancer. 1969;23(3):655–60.
Iwai H, Tagawa Y, Hayasaka I, Yanai T, Masegi T. Effects of atropine sulfate on rat harderian glands: correlation between morphological changes and porphyrin levels. J Toxicol Sci. 2000;25(3):151–9.
Kajimura T, Satoh H, Nomura M. Effect of hyperprolactinemia induced by neuroleptic agent, timiperone, on porphyrin content of mouse harderian gland. J Toxicol Sci. 1997;22(3):219–29.
Eida K, Kubota N, Nishigaki T, Kikutani M. Harderian gland. V. Effect of dietary pantothenic acid deficiency on porphyrin biosynthesis in harderian gland of rats. Chem Pharm Bull(Tokyo). 1975;23(1):1–4.
da Costa JR, Iucif S, Lopes RA. Effect of hypervitaminosis A on the harderian gland in rats. A morphologic and morphometric study. Int J Vitam Nutr Res. 1978;48(2):113–22.
Gray Jr LE, Kavlock RJ, Chernoff N, Ferrell J, McLamb J, Ostby J. Prenatal exposure to the herbicide 2,4-dichlorophenyl-p-nitrophenyl ether destroys the rodent harderian gland. Science. 1982;215(4530):293–4.
Eglitis I. The eyelids. In: Prince JH, editor. The rabbit in eye research. Springfield: Charles C Thomas Pub.; 1964. p. 72–85.
Richardson VCG. Diseases of domestic guinea pigs. 2nd ed. London: Blackwell Science; 2000.
Percy D, Barthold S. Pathology of laboratory rodents and rabbits. Ames: Iowa State University Press; 2001.
Brazzell RK, Stern ME, Aquavella JV, Beuerman RW, Baird L. Human recombinant epidermal growth factor in experimental corneal wound healing. Invest Ophthalmol Vis Sci. 1991;32(2):336–40.
Rich LF, Hatfield JM, Louiselle I. The influence of epidermal growth factor on cat corneal endothelial wound healing. Curr Eye Res. 1991;10(9):823–30.
Greenman DL, Cronin GM, Dahlgren R, Allen R, Allaben W. Chronic feeding study of pyrilamine in Fischer 344 rats. Fundam Appl Toxicol. 1995;25(1):1–8.
Wilhelm KE, Grabolle B, Urbach H, Tolba R, Schild H, Paulsen F. Evaluation of polyurethane nasolacrimal duct stents: in vivo studies in New Zealand rabbits. Cardiovasc Intervent Radiol. 2006;29(5):846–53.
Kintzel PE, Michaud LB, Lange MK. Docetaxel-associated epiphora. Pharmacotherapy. 2006;26(6):853–67.
Vettese T, Hurwitz JJ. Toxicity of the chemiluminescent material Cyalume in anatomic assessment of the nasolacrimal system. Can J Ophthalmol. 1983;18(3):131–5.
Carlton WW, Render JA. Adenoma and adenocarcinoma, harderian gland, mouse, rat and hamster. In: Jones TC, Mohr U, Hunt RD, editors. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 133–7.
Tucker MJ. Special sense organs and associated tissues. In: Tucker MJ, editor. Diseases of the Wistar Rat. London: Taylor and Francis; 1997. p. 237–45.
Sheldon WG, Curtis M, Kodell RL, Weed L. Primary harderian gland neoplasms in mice. J Natl Cancer Inst. 1983;71(1):61–8.
Prince JH. Cornea, trabecular region, and sclera. In: Prince JH, editor. The rabbit in eye research. Springfield: Charles C Thomas Pub.; 1964. p. 86–139.
Taradach C, Regnier B, Perraud J. Eye lesions in Sprague-Dawley rats: type and incidence in relation to age. Lab Anim. 1981;15(3):285–7.
Taradach C, Greaves P. Spontaneous eye lesions in laboratory animals: incidence in relation to age. Crit Rev Toxicol. 1984;12(2):121–47.
Shibuya K, Satou K, Sugimoto K, Saitoh T, Ihara M, Itabashi M, et al. Background data on spontaneous ophthalmic lesions in Crj:CD(SD)IGS rats. In: Matsuzawa T, Inoue H, editors. Biological reference data on CD(SD) IGS rats – 1999. Yokohama: Best Printing Co. Ltd.; 1999. p. 60–2.
Bellhorn RW, Korte GE, Abrutyn D. Spontaneous corneal degeneration in the rat. Lab Anim Sci. 1988;38(1):46–50.
Kuno H, Usui T, Eydelloth RS, Wolf ED. Spontaneous ophthalmic lesions in young Sprague-Dawley rats. J Vet Med Sci. 1991;53(4):607–14.
Van Winkle TJ, Balk MW. Spontaneous corneal opacities in laboratory mice. Lab Anim Sci. 1986;36(3):248–55.
Carlton WW, Render JA. Calcification of the cornea. In: Jones TC, Mohr U, Hunt RD, editors. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 16–20.
Mittl R, Galin MA, Opperman W, Camerini-Davalos RA, Spiro D. Corneal calcification in spontaneously diabetic mice. Invest Ophthalmol. 1970;9(2):137–45.
Hoffman RW, Yang HK, Waggie KS, Durham JB, Burge JR, Walker SE. Band keratopathy in MRL/l and MRL/n mice. Arthritis Rheum. 1983;26(5):645–52.
Huang LH, Sery TW. Corneal degeneration in a congenitally diabetic inbred strain of mouse. Br J Ophthalmol. 1971;55(4):266–71.
Jester JV, Maurer JK, Petroll WM, Wilkie DA, Parker RD, Cavanagh HD. Application of in vivo confocal microscopy to the understanding of surfactant-induced ocular irritation. Toxicol Pathol. 1996;24(4):412–28.
Schmidt RE. Ophthalmic lesions in non-human primates. Vet Pathol. 1971;8(1):28–36.
Riley MV, Green K. Comparative physiology and biochemistry of the eye. In: Hockwin O, Green K, Rubin LF, editors. Manual of oculotoxicity testing of drugs. Stuttgart: Gustav Fischer Verlag; 1992. p. 45–80.
Weber U, Sons HU, Lenz W, Bernsmeier H. Experimental tyrosine keratopathy in rabbits. Klin Monbl Augenheilkd. 1986;188(6):587–9.
Beard ME, Burns RP, Rich LF, Squires E. Histopathology of keratopathy in the tyrosine-fed rat. Invest Ophthalmol. 1974;13(12):1037–41.
Lock EA, Gaskin P, Ellis M, Provan WM, Smith LL. Tyrosinemia produced by 2-(2-nitro-4-trifluoromethylbenzoyl)-cyclohexane-1,3-dione (NTBC) in experimental animals and its relationship to corneal injury. Toxicol Appl Pharmacol. 2006;215(1):9–16.
Kast A. Keratoconjunctivitis sicca and sequelae, mouse and rat. In: Jones TC, Mohr U, Hunt RD, editors. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 29–37.
Draize JH, Woodward G, Calvery HO. Method for the study of irritation and toxicity of substances applied topically to the skin and mucous membranes. J Pharmacol Exp Ther. 1944;82:377–90.
Gershbein LL, McDonald JE. Evaluation of the corneal irritancy of test shampoos and detergents in various animal species. Food Cosmet Toxicol. 1977;15(2):131–4.
Wilhelmus KR. The Draize eye test. Surv Ophthalmol. 2001;45(6):493–515.
Roggeband R, York M, Pericoi M, Braun W. Eye irritation responses in rabbit and man after single applications of equal volumes of undiluted model liquid detergent products. Food Chem Toxicol. 2000;38(8):727–34.
DeRosa AJ. Toxic keratopathy. Int Ophthalmol Clin. 1998;38(4):15–22.
Curren DR, Evans MG, Raabe H, Ruppalt RR, Harbell J. Correlation of histopathology, opacity, and permeability of bovine corneas exposed in vitro to known ocular irritants. Vet Pathol. 2000;37:557.
Sina JF, Galer DM, Sussman RG, Gautheron PD, Sargent EV, Leong B, et al. A collaborative evaluation of seven alternatives to the Draize eye irritation test using pharmaceutical intermediates. Fundam Appl Toxicol. 1995;26(1):20–31.
Maurer JK, Parker RD. Light microscopic comparison of surfactant-induced eye irritation in rabbits and rats at three hours and recovery/day 35. Toxicol Pathol. 1996;24(4):403–11.
Maurer JK, Parker RD, Carr GJ. Ocular irritation: microscopic changes occurring over time in the rat with surfactants of known irritancy. Toxicol Pathol. 1998;26(2):217–25.
Maurer JK, Parker RD. Microscopic changes with acetic acid and sodium hydroxide in the rabbit low-volume eye test. Toxicol Pathol. 2000;28(5):679–87.
Jester JV, Molai A, Petroll WM, Parker RD, Carr GJ, Cavanagh HD, et al. Quantitative characterization of acid- and alkali-induced corneal injury in the low-volume eye test. Toxicol Pathol. 2000;28(5):668–78.
Maurer JK, Molai A, Parker RD, Li L, Carr GJ, Petroll WM, et al. Pathology of ocular irritation with bleaching agents in the rabbit low-volume eye test. Toxicol Pathol. 2001;29(3):308–19.
Maurer JK, Molai A, Parker RD, Li LI, Carr GJ, Petroll WM, et al. Pathology of ocular irritation with acetone, cyclohexanol, parafluoroaniline, and formaldehyde in the rabbit low-volume eye test. Toxicol Pathol. 2001;29(2):187–99.
White E, Crosse MM. The aetiology and prevention of peri-operative corneal abrasions. Anaesthesia. 1998;53(2):157–61.
Guillet R, Wyatt J, Baggs RB, Kellogg CK. Anesthetic-induced corneal lesions in developmentally sensitive rats. Invest Ophthalmol Vis Sci. 1988;29(6):949–54.
Williams DL. Ocular disease in rats: a review. Vet Ophthalmol. 2002;5(3):183–91.
Fabian RJ, Bond JM, Drobeck HP. Induced corneal opacities in the rat. Br J Ophthalmol. 1967;51(2):124–9.
Roerig DL, Hasegawa AT, Harris GJ, Lynch KL, Wang RI. Occurrence of corneal opacities in rats after acute administration of l-alpha-acetylmethadol. Toxicol Appl Pharmacol. 1980;56(2):155–63.
Grant RL, Acosta D. Comparative toxicity of tetracaine, proparacaine and cocaine evaluated with primary cultures of rabbit corneal epithelial cells. Exp Eye Res. 1994;58(4):469–78.
Fraunfelder FT, Fraunfelder FW, Chambers WA. Clinical ocular toxicology. Philadelphia: Saunders Elsevier; 2008.
Zarfoss M, Bentley E, Milovancev M, Schmiedt C, Dubielzig R, McAnulty J. Histopathologic evidence of capecitabine corneal toxicity in dogs. Vet Pathol. 2007;44(5):700–2.
Pyrah IT, Kalinowski A, Jackson D, Davies W, Davis S, Aldridge A, et al. Toxicologic lesions associated with two related inhibitors of oxidosqualene cyclase in the dog and mouse. Toxicol Pathol. 2001;29(2):174–9.
Kirby TJ. Cataracts produced by triparanol. (MER-29). Trans Am Ophthalmol Soc. 1967;65:494–543.
Kirby Jr TJ, Achor RW, Perry HO, Winkelmann RK. Cataract formation after triparanol therapy. Arch Ophthalmol. 1962;68:486–9.
Funk J, Landes C. Histopathologic findings after treatment with different oxidosqualene cyclase (OSC) inhibitors in hamsters and dogs. Exp Toxicol Pathol. 2005;57(1):29–38.
Geiss V, Yoshitomo K. Eyes. In: Maronpot RR, Boorman GA, Gaul BW, editors. Pathology of the mouse. St. Louis: Cache River Press; 1999. p. 471–90.
Reindel JF, Gough AW, Pilcher GD, Bobrowski WF, Sobocinski GP, de la Iglesia FA. Systemic proliferative changes and clinical signs in cynomolgus monkeys administered a recombinant derivative of human epidermal growth factor. Toxicol Pathol. 2001;29(2):159–73.
Patz A, Wulff LB, Rogers SW. Experimental production of ocular tumors. Am J Ophthalmol. 1959;48(1, Part 2):98–117.
Gupta BN. Scleral dermoid in a guinea pig. Lab Anim Sci. 1972;22(6):919–21.
Nichols CW, Yanoff M. Dermoid of a rat cornea. Pathol Vet. 1969;6(3):214–6.
Horikiri K, Ozaki K, Maeda H, Narama I. Corneal dermoid in two laboratory beagle dogs. Jikken Dobutsu. 1994;43(3):417–20.
Otto G, Lipman NS, Murphy JC. Corneal dermoid in a hairless guinea pig. Lab Anim Sci. 1991;41(2):171–2.
Styer CM, Ferrier WT, Labelle P, Griffey SM, Kendall LV. Limbic dermoid in a New Zealand white rabbit (Oryctolagus cuniculus). Contemp Top Lab Anim Sci. 2005;44(6):46–8.
Dunnick JK, Forbes PD, Eustis SL, Hardisty JF, Goodman DG. Tumors of the skin in the HRA/Skh mouse after treatment with 8-methoxypsoralen and UVA radiation. Fundam Appl Toxicol. 1991;16(1):92–102.
Porter R, Crombie AL. Corneal calcification as a presenting and diagnostic sign in hyperparathyroidism. Br J Ophthalmol. 1973;57(9):665–8.
O’Connor GR. Calcific band keratopathy. Trans Am Ophthalmol Soc. 1972;70:58–81.
Losco PE, Troup CM. Corneal dystrophy in Fischer 344 rats. Lab Anim Sci. 1988;38(6):702–10.
Shibuya K, Sugimoto K, Satou K. Spontaneous ocular lesions in aged Crj:CD(SD)IGS rats. Anim Eye Res (Jpn). 2001;20(15–19):95–9.
Ocumpaugh DE, Obenberger J. Experimental corneal calcification: a radioautographic and histochemical study. Clin Orthop Relat Res. 1970;69:162–71.
Moore CP, Dubielzig R, Glaza SM. Anterior corneal dystrophy of American Dutch belted rabbits: biomicroscopic and histopathologic findings. Vet Pathol. 1987;24(1):28–33.
Port CD, Dodd DC. Two cases of corneal epithelial dystrophy in rabbits. Lab Anim Sci. 1983;33(6):587–8.
Fine BS, Berkow JW, Fine S. Corneal calcification. Science. 1968;162(3849):129–30.
Muirhead JR, Tomazzoli-Gerosa L. Animal models of band keratopathy. In: Tabbara K, Cello R, editors. Animals models of band keratopathy. Springfield: Charles C. Thomas Pub.; 1984. p. 221–32.
Obenberger J, Ocumpaugh DE, Cubberly MG. Experimental corneal calcification in animals treated with dihydrotachysterol. Invest Ophthalmol. 1969;8(5):467–74.
Economon JW, Silverstein AM, Zimmerman LE. Band keratopathy in a rabbit colony. Invest Ophthalmol. 1963;2:361–8.
Bruner RH, Keller WF, Stitzel KA, Sauers LJ, Reer PJ, Long PH, et al. Spontaneous corneal dystrophy and generalized basement membrane changes in Fischer-344 rats. Toxicol Pathol. 1992;20(3 Pt 1):357–66.
Friend J, Ishii Y, Thoft RA. Corneal epithelial changes in diabetic rats. Ophthalmic Res. 1982;14(4):269–78.
Obenberger J. Calcification in corneas with alloxan-induced vascularization. Am J Ophthalmol. 1969;68(1):113–9.
Meador VP, Tyler RD, Plunkett ML. Epicardial and corneal mineralization in clinically normal severe combined immunodeficiency (SCID) mice. Vet Pathol. 1992;29(3):247–9.
Davidson SI, Rennie IG. Ocular toxicity from systemic drug therapy. An overview of clinically important adverse reactions. Med Toxicol. 1986;1(3):217–24.
Johnston AM, Memon AA. Mystery of the blue pigmentation. N Engl J Med. 1999;340(20):1597–8.
Morrow GL, Abbott RL. Minocycline-induced scleral, dental, and dermal pigmentation. Am J Ophthalmol. 1998;125(3):396–7.
Sanchez AR, Rogers 3rd RS, Sheridan PJ. Tetracycline and other tetracycline-derivative staining of the teeth and oral cavity. Int J Dermatol. 2004;43(10):709–15.
Newkirk KM, Chandler HL, Parent AE, Young DC, Colitz CM, Wilkie DA, et al. Ultraviolet radiation-induced corneal degeneration in 129 mice. Toxicol Pathol. 2007; 35(6):819–26.
Budiarso IT, Carlton WW, Tuite JF. Phototoxic syndrome induced in mice by rice cultures of Penicillium viridicatum and exposure to sunlight. Pathol Vet. 1970;7(6):531–46.
Klintworth GK, Burger PC. Neovascularization of the cornea: current concepts of its pathogenesis. Int Ophthalmol Clin. 1983;23(1):27–39.
Huang AJ, Li DQ, Li CH, Shang TY, Hernandez E. Modulation of corneal vascularization. Ocul Surf. 2005;3(4 Suppl):S190–3.
Niederkorn JY, Ubelaker JE, Martin JM. Vascularization of corneas of hairless mutant mice. Invest Ophthalmol Vis Sci. 1990;31(5):948–53.
Carter-Dawson L, Tanaka M, Kuwabara T, Bieri JG. Early corneal changes in vitamin A deficient rats. Exp Eye Res. 1980;30(3):261–9.
Leure-dupree AE. Vascularization of the rat cornea after prolonged zinc deficiency. Anat Rec. 1986;216(1):27–32.
Aguirre SA, Huang W, Prasanna G, Jessen B. Corneal neovascularization and ocular irritancy responses in dogs following topical ocular administration of an EP4-prostaglandin E2 agonist. Toxicol Pathol. 2009;37(7):911–20.
Kim TI, Chung JL, Hong JP, Min K, Seo KY, Kim EK. Bevacizumab application delays epithelial healing in rabbit cornea. Invest Ophthalmol Vis Sci. 2009;50(10):4653–9.
Garibaldi BA, Goad ME. Lipid keratopathy in the Watanabe (WHHL) rabbit. Vet Pathol. 1988;25(2):173–4.
Sebesteny A, Sheraidah GA, Trevan DJ, Alexander RA, Ahmed AI. Lipid keratopathy and atheromatosis in an SPF laboratory rabbit colony attributable to diet. Lab Anim. 1985;19(3):180–8.
Stock EL, Mendelsohn AD, Lo GG, Ghosh S, O’Grady RB. Lipid keratopathy in rabbits. An animal model system. Arch Ophthalmol. 1985;103(5):726–30.
Janes RG. Changes in the rabbit’s eye caused by cholesterol feeding. Am J Ophthalmol. 1964;58:819–28.
Williams D, Sullivan A. Ocular disease in the guinea pig (Cavia porcellus): a survey of 1000 animals. Vet Ophthalmol. 2010;13(Suppl):54–62.
Spangler WL, Waring GO, Morrin LA. Oval lipid corneal opacities in beagles. Vet Pathol. 1982;19(2):150–9.
Roth AM, Ekins MB, Waring 3rd GO, Gupta LM, Rosenblatt LS. Oval corneal opacities in beagles. III. Histochemical demonstration of stromal lipids without hyperlipidemia. Invest Ophthalmol Vis Sci. 1981;21(1 Pt 1):95–106.
D’Amico DJ, Kenyon KR, Ruskin JN. Amiodarone keratopathy: drug-induced lipid storage disease. Arch Ophthalmol. 1981;99(2):257–61.
Turdumambetova G, Bredehorn T, Duncker GI. Ocular side-effects associated with amiodarone therapy. Klin Monbl Augenheilkd. 2005;222(6):485–92.
Mantyjarvi M, Tuppurainen K, Ikaheimo K. Ocular side effects of amiodarone. Surv Ophthalmol. 1998;42(4):360–6.
Lullmann H, Lullmann-Rauch R. Tamoxifen-induced generalized lipidosis in rats subchronically treated with high doses. Toxicol Appl Pharmacol. 1981;61(1):138–46.
Drenckhahn D, Jacobi B, Lullmann-Rauch R. Corneal lipidosis in rats treated with amphiphilic cationic drugs. Arzneimittelforschung. 1983;33(6):827–31.
Bicer S, Fuller GA, Wilkie DA, Yamaguchi M, Hamlin RL. Amiodarone-induced keratopathy in healthy dogs. Vet Ophthalmol. 2002;5(1):35–8.
Lullmann-Rauch R. Mucopolysaccharidosis (MPS) in ocular tissues as induced by amphiphilic di-cationic drugs. Lens Eye Toxic Res. 1990;7(3–4):263–79.
Hein L, Lullmann-Rauch R. Mucopolysaccharidosis and lipidosis in rats treated with tilorone analogues. Toxicology. 1989;58(2):145–54.
Kafarnik C, Murphy CJ, Dubielzig RR. Canine duplication of Descemet’s membrane. Vet Pathol. 2009;46(3):464–73.
Gwin RM, Warren JK, Samuelson DA, Gum GG. Effects of phacoemulsification and extracapsular lens removal on corneal thickness and endothelial cell density in the dog. Invest Ophthalmol Vis Sci. 1983;24(2):227–36.
Yee RW, Geroski DH, Matsuda M, Champeau EJ, Meyer LA, Edelhauser HF. Correlation of corneal endothelial pump site density, barrier function, and morphology in wound repair. Invest Ophthalmol Vis Sci. 1985;26(9):1191–201.
Van Horn DL, Sendele DD, Seideman S, Buco PJ. Regenerative capacity of the corneal endothelium in rabbit and cat. Invest Ophthalmol Vis Sci. 1977;16(7):597–613.
Joyce NC. Proliferative capacity of the corneal endothelium. Prog Retin Eye Res. 2003;22(3):359–89.
Sherrard ES, Rycroft PV. Retrocorneal membranes. I. Their origin and structure. Br J Ophthalmol. 1967;51(6):379–86.
Silbert AM, Baum JL. Origin of the retrocorneal membrane in the rabbit. Arch Ophthalmol. 1979;97(6):1141–3.
Hull DS, Green K, Laughter L. Cornea endothelial rose bengal photosensitization. Effect on permeability, sodium flux, and ultrastructure. Invest Ophthalmol Vis Sci. 1984;25(4):455–60.
Bartlett JD. Ophthalmic toxicity by systemic drugs. In: Chiou GCY, editor. Ophthalmic toxicology. New York: Raven Press, Ltd.; 1992. p. 175–81.
Hull DS, Csukas S, Green K. Chlorpromazine-induced corneal endothelial phototoxicity. Invest Ophthalmol Vis Sci. 1982;22(4):502–8.
Vonvoigtlander PF, Kolaja GJ, Block EM. Corneal lesions induced by antidepressants: a selective effect upon young Fischer 344 rats. J Pharmacol Exp Ther. 1982;222(1):282–6.
Olsen TW, Feng X, Wabner K, Conston SR, Sierra DH, Folden DV, et al. Cannulation of the suprachoroidal space: a novel drug delivery methodology to the posterior segment. Am J Ophthalmol. 2006;142(5):777–87.
French DD, Margo CE. Postmarketing surveillance rates of uveitis and scleritis with bisphosphonates among a national veteran cohort. Retina. 2008;28(6):889–93.
Chodosh J, Nordquist RE, Kennedy RC. Comparative anatomy of mammalian conjunctival lymphoid tissue: a putative mucosal immune site. Dev Comp Immunol. 1998;22(5–6):621–30.
Ruskell GL. Organization and cytology of lymphoid tissue in the cynomolgus monkey conjunctiva. Anat Rec. 1995;243(2):153–64.
Knop E, Knop N. The role of eye-associated lymphoid tissue in corneal immune protection. J Anat. 2005;206(3):271–85.
Knop N, Knop E. Conjunctiva-associated lymphoid tissue in the human eye. Invest Ophthalmol Vis Sci. 2000;41(6):1270–9.
Cain C, Phillips TE. Developmental changes in conjunctiva-associated lymphoid tissue of the rabbit. Invest Ophthalmol Vis Sci. 2008;49(2):644–9.
Fujihira S, Matsumoto M, Yoshizawa K, Oishi Y, Iwanami K, Fujii T. Naturally occurring ophthalmic lesions in cynomolgus monkeys used in toxicity and pharmacological studies. Anim Eye Res Jpn. 1994;13(3–4):147–54.
Shimoi A, Kakinuma C, Kuwayama C, Watanabe M. Comparison of spontaneous minor lesions in wild-caught and laboratory-bred monkeys. J Toxicol Pathol. 1998;11:85–94.
Flatt RE. Bacterial diseases. In: Weisbroth S, Flatt RE, Kraus AL, editors. The biology of the laboratory rabbit. New York: Academic Press; 1974. p. 194–236.
Strocchi P, Dozza B, Pecorella I, Fresina M, Campos E, Stirpe F. Lesions caused by ricin applied to rabbit eyes. Invest Ophthalmol Vis Sci. 2005;46(4):1113–6.
Prince JH, Eglitis I. The uvea. In: Prince JH, editor. The rabbit in eye research. Springfield: Charles C Thomas Pub.; 1964. p. 140–71.
Biros DJ. Ocular immunity. In: Gelatt KN, editor. Veterinary ophthalmology. 4th ed. Ames: Blackwell Publishing; 2007. p. 223–35.
Park SA, Jeong SM, Yi NY, Kim MS, Jeong MB, Suh JG, et al. Study on the ophthalmic diseases in ICR mice and BALB/c mice. Exp Anim. 2006;55(2):83–90.
Jeong MB, Kim NR, Yi NY, Park SA, Kim MS, Park JH, et al. Spontaneous ophthalmic diseases in 586 New Zealand white rabbits. Exp Anim. 2005;54(5):395–403.
Rubin LF, Weisse I. Species differences relevant for ocular toxicity studies. In: Hockwin O, Green K, Rubin LF, editors. Manual of oculotoxicity testing of drugs. Stuttgart: Gustav Fischer Verlag; 1992.
Brown SM. Increased iris pigment in a child due to latanoprost. Arch Ophthalmol. 1998;116(12):1683–4.
Eisenberg DL, Camras CB. A preliminary risk-benefit assessment of latanoprost and unoprostone in open-angle glaucoma and ocular hypertension. Drug Saf. 1999;20(6):505–14.
Stjernschantz JW, Albert DM, Hu DN, Drago F, Wistrand PJ. Mechanism and clinical significance of prostaglandin-induced iris pigmentation. Surv Ophthalmol. 2002;47 Suppl 1:S162–75.
Lindquist NG, Larsson BS, Stjernschantz J. Increased pigmentation of iridial melanocytes in primates induced by a prostaglandin analogue. Exp Eye Res. 1999;69(4):431–6.
Gesundheit B, Greenberg M. Medical mystery: brown eye and blue eye–the answer. N Engl J Med. 2005;353(22):2409–10.
Roe FJ, Millican D, Mallett JM. Induction of melanotic lesions of the iris in rats by urethane given during the neonatal period. Nature. 1963;199:1201–2.
Koizumi H, Watanabe M, Numata H, Sakai T, Morishita H. Species differences in vacuolation of the choroid plexus induced by the piperidine-ring drug disobutamide in the rat, dog, and monkey. Toxicol Appl Pharmacol. 1986;84(1):125–48.
Render JA, Carlton WW. Toxic effects of 6-aminonicotinamide, uvea, rabbit. In: Jones TC, Mohr U, Hunt RD, editors. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 50–4.
Gopinath C, Prentice DE, Lewis DJ. The eye and ear. In: Gopinath C, Prentice DE, Lewis DJ, editors. Atlas of experimental toxicological pathology. Lancaster: MTP Press; 1987. p. 145–55.
Potts AM, Gonasun LM. Toxic responses of the ocular and visual system. In: Duoll J, Klaassen CD, Amdur MO, editors. Toxicology: the basic science of poisons. New York: MacMillan; 1980. p. 275–310.
Fraunfelder FW, Rosenbaum JT. Drug-induced uveitis. Incidence, prevention and treatment. Drug Saf. 1997;17(3):197–207.
Heywood R. Clinical and laboratory assessment of visual dysfunction. In: Hayes AC, editor. Toxicology of the eye, ear and other special sense organs. New York: Raven Press, Ltd; 1985. p. 61–77.
Levine S. Cyclitis induced by cyclophosphamide, rat. In: Jones TC, Mohr U, Hunt RD, editors. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 38–9.
McMaster PR, Wong VG, Owens JD. The propensity of different strains of guinea pigs to develop experimental autoimmune uveitis. Mod Probl Ophthalmol. 1976;16:62–71.
Sinha DP, Cartwright ME, Johnson RC. Incidental mononuclear cell infiltrate in the uvea of cynomolgus monkeys. Toxicol Pathol. 2006;34(2):148–51.
Rubin LF. Atlas of veterinary ophthalmoscopy. Philadelphia: Lea and Febiger; 1974.
Pleština R, Piuković-Pleština M, Roberts DV. Effect of anticholinesterase pesticides on the eye and on vision. Crit Rev Toxicol. 1978;6(1):1–23.
Rungby J. Experimental argyrosis: ultrastructural localization of silver in rat eye. Exp Mol Pathol. 1986;45(1):22–30.
Faccini JM. Mouse histopathology. Philadelphia: Elsevier Science; 1990.
Griffith JW, Sassani JW, Bowman TA, Lang CM. Osseous choristoma of the ciliary body in guinea pigs. Vet Pathol. 1988;25(1):100–2.
Brooks DE, McCracken MD, Collins BR. Heterotopic bone formation in the ciliary body of an aged guinea pig. Lab Anim Sci. 1990;40(1):88–90.
Donnelly KB, Berridge B, Long GG, Schafer KA, Reynolds VL, Sullivan JM, et al. Peroxisome proliferator activated receptor gamma (PPARg) agonist-mediated ocular choroid adiposity: Strain sensitivity differences between Fischer 344 and Sprague-Dawley rats. Toxicol Pathol. 2007;35(1):189.
Hadjikoutis S, Morgan JE, Wild JM, Smith PE. Ocular complications of neurological therapy. Eur J Neurol. 2005;12(7):499–507.
Peckman JC. The rabbit: pathology. In: Gad SC, editor. Animal models in toxicology. Boca Raton: CRC/Taylor and Francis; 2007. p. 449–74.
Gelatt KN, Gum GG, Gwin RM, Bromberg NM, Merideth RE, Samuelson DA. Primary open angle glaucoma: inherited primary open angle glaucoma in the beagle. Am J Pathol. 1981;102(2):292–5.
Lindsey JR, Fox RR. Inherited diseases and variations. In: Manning PJ, Ringler DH, Newcomer CE, editors. The biology of the laboratory rabbit. New York: Academic Press; 1994. p. 239–319.
Suckow MA, Douglas FA. The laboratory rabbit. Boca Raton: CRC Press; 1997.
McMenamin PG. Dendritic cells and macrophages in the uveal tract of the normal mouse eye. Br J Ophthalmol. 1999;83(5):598–604.
McMenamin PG. The distribution of immune cells in the uveal tract of the normal eye. Eye (Lond). 1997;11(Pt 2):183–93.
Butler TL, McMenamin PG. Resident and infiltrating immune cells in the uveal tract in the early and late stages of experimental autoimmune uveoretinitis. Invest Ophthalmol Vis Sci. 1996;37(11):2195–210.
Pras E, Neumann R, Zandman-Goddard G, Levy Y, Assia EI, Shoenfeld Y, et al. Intraocular inflammation in autoimmune diseases. Semin Arthritis Rheum. 2004;34(3):602–9.
John SW, Smith RS, Savinova OV, Hawes NL, Chang B, Turnbull D, et al. Essential iris atrophy, pigment dispersion, and glaucoma in DBA/2 J mice. Invest Ophthalmol Vis Sci. 1998;39(6):951–62.
Lutjen-Drecoll E, Tamm E. Morphological study of the anterior segment of cynomolgus monkey eyes following treatment with prostaglandin F2 alpha. Exp Eye Res. 1988;47(5):761–9.
Heywood R. Drug-induced retinopathies in the Beagle dog. Br Vet J. 1974;130(6):564–9.
Heywood R. An anomaly of the ocular fundus of the Beagle dog. J Small Anim Pract. 1972;13(4):213–5.
Bellhorn RW, Bellhorn MB, Swarm RL, Impellizzeri CW. Hereditary tapetal abnormality in the beagle. Ophthalmic Res. 1975;7:250–60.
Schiavo DM. Retinopathy from administration of an imidazoquinazoline to beagles. Toxicol Appl Pharmacol. 1972;23(4):782–3.
Haggerty GC, Peckman JC, Thomassen RW, Gad SC. The dog. In: Gad SC, editor. Animal models in toxicology. 3rd ed. Boca Raton: CRC Press; 2007. p. 563–662.
Heywood R, Hepworth PL, Van Abbe NJ. Age changes in the eyes of the Beagle dog. J Small Anim Pract. 1976;17(3):171–7.
Delahunt CS, Stebbins RB, Anderson J, Bailey J. The cause of blindness in dogs given hydroxypyridinethione. Toxicol Appl Pharmacol. 1962;4:286–91.
Moe RA, Kirpan J, Linegar CR. Toxicology of hydroxypyridinethione. Toxicol Appl Pharmacol. 1960;2:156–70.
Budinger JM. Diphenylthiocarbazone blindness in dogs. Arch Ophthalmol. 1961;71:304–10.
Snyder FH, Buehler EV, Winek CL. Safety evaluation of zinc 2-pyridinethiol 1-oxide in a shampoo formulation. Toxicol Appl Pharmacol. 1965;7:425–37.
Schiavo DM, Green JD, Traina VM, Spaet R, Zaidi I. Tapetal changes in beagle dogs following oral administration of CGS 14796 C, a potential aromatase inhibitor. Fundam Appl Toxicol. 1988;10(2):329–34.
Dillberger JE, Peiffer RL, Dykstra MJ, O’Mara M, Patel DK. The experimental antipsychotic agent 1192U90 targets tapetum lucidum in canine eyes. Toxicol Pathol. 199624(5):595–601.
Cloyd GG, Wyman M, Shadduck JA, Winrow MJ, Johnson GR. Ocular toxicity studies with zinc pyridinethione. Toxicol Appl Pharmacol. 1978;45(3):771–82.
Saint-Macary G, Berthoux C. Ophthalmologic observations in the young Yucatan micropig. Lab Anim Sci. 1994;44(4):334–7.
Hubert MF, Gillet JP, Durand-Cavagna G. Spontaneous retinal changes in Sprague Dawley rats. Lab Anim Sci. 1994;44(6):561–7.
Bellhorn RW. Survey of ocular findings in 16- to 24-week-old beagles. J Am Vet Med Assoc. 1973;162(2):139–41.
Everitt JI, Shadduck JA. Melanoma of the uvea, rat. In: Jones TC, editor. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 40–3.
Owen RA, Duprat P. Leiomyoma of the iris, Sprague-Dawley rat. In: Jones TC, Mohr U, Hunt RD, editors. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 47–9.
Yoshitomi K, Boorman GA. Intraocular and orbital malignant Schwannomas in F344 rats. Vet Pathol. 1991;28(6):457–66.
Congdon CC, Lorenz E. Leukemia in guinea-pigs. Am J Pathol. 1954;30(2):337–59.
Steinberg H. Disseminated T-cell lymphoma in a guinea pig with bilateral ocular involvement. J Vet Diagn Invest. 2000;12(5):459–62.
Peiffer RL, Pohm-Thorsen L, Corcoran K. Models in ophthalmology and vision research. In: Manning PJ, Ringler DH, Newcomer CE, editors. The biology of the laboratory rabbit. 2nd ed. New York: Academic Press; 1994. p. 410–33.
Squire RA, Goodman DG, Valerio MG, Fredrickson TN, Strandberg JD, Levitt MH, et al. Tumors. In: Benirschke K, Gamer FM, Jones TC, editors. Pathology of laboratory animals. New York: Springer; 1978. p. 1051–252.
Ernst H, Rittinghausen S, Mohr U. Melanoma of the eye, mouse. In: Jones TC, Mohr U, Hunt RD, editors. Monographs on pathology of laboratory animals: eye and ear. Berlin: Springer; 1991. p. 44–7.
Albert DM, Gonder JR, Papale J, Craft JL, Dohlman HG, Reid MC, et al. Induction of ocular neoplasms in Fischer rats by intraocular injection of nickel subsulfide. Invest Ophthalmol Vis Sci. 1982;22(6):768–82.
Albert DM, Puliafito CA, Haluska FG, Kimball GP, Robinson NL. Induction of ocular neoplasms in Wistar rat by N-methyl-N-nitrosourea. Exp Eye Res. 1986;42(1):83–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Schafer, K.A., Render, J.A. (2012). Toxicologic Pathology of the Eye: Histologic Preparation and Alterations of the Anterior Segment. In: Weir, A., Collins, M. (eds) Assessing Ocular Toxicology in Laboratory Animals. Molecular and Integrative Toxicology. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-62703-164-6_5
Download citation
DOI: https://doi.org/10.1007/978-1-62703-164-6_5
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-62703-163-9
Online ISBN: 978-1-62703-164-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)