
Abstract
Focal segmental glomerulosclerosis (FSGS) is an important diagnostic finding in kidney biopsies from patients with proteinuric kidney diseases. Its presence often heralds a relentlessly progressive loss of kidney function over time. An effective treatment is not possible in all, or even most, cases. Advances in our understanding of the causes of this pathological lesion, thought to be based on pathology of the glomerular visceral epithelial cell (the podocyte), may eventually lead to more specific and less toxic treatment for patients having this form of renal pathology.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
Introduction
Focal segmental glomerulosclerosis (FSGS) is a finding on kidney biopsy of sclerosis of portions of some, but not all, glomeruli. FSGS is a pathological finding often seen in progressive proteinuric glomerular diseases and is ultimately the result of podocyte loss from the glomerular tuft. Thus, FSGS is a finding common to a number of podocyte-associated glomerulopathies, diseases reflecting podocyte dysfunction (causing proteinuria) and podocyte loss (causing sclerosis). Some variants (collapsing FSGS) may involve dysregulated proliferation of podocytes.
The pathological entity FSGS has a significant overlap with, but is not identical to, the clinical entity of steroid-resistant nephrotic syndrome (SRNS). Classically, FSGS has been categorized as primary FSGS or secondary FSGS, based on the presumed etiology. This distinction both obscures and somewhat undervalues our current understanding of the mechanisms of podocyte injury and should therefore be eschewed in any systematic exploration of FSGS. Instead, three broad categories of mechanisms can be considered to cover the majority of cases: genetic, immune-related signaling, and hemodynamic. All these forms share the features of podocyte dysfunction and/or loss. The particular mechanism involved may suggest the most appropriate therapy. This chapter will review the epidemiology of FSGS, highlight the clinical features and disease outcomes, explore the pathology and proposed pathogenic mechanisms, and discuss treatment regimens for SRNS.
Epidemiology of FSGS in Children
Due to its rarity, the incidence of FSGS is quite hard to establish, particularly in pediatrics. Because there are no noninvasive markers of FSGS, estimates of its prevalence in pediatric NS are based solely on biopsy findings. An early population-based study showed an incidence of “lipoid nephrosis” on biopsy of 1.5 per 100,000 per year in 10–20-year-olds (Simon et al. 1994). This presumably sets an upper limit on the incidence of FSGS, as it likely contained cases of minimal change disease as well. Studies in the 1970–1980s, including reports from the International Study of Kidney Disease in Children (ISKDC) and the Southwest Pediatric Nephrology Study Group (SPNSG), suggested that FSGS represents a small fraction of nephrotic syndrome (NS) cases. The ISKDC recruited 521 patients from 4 continents at time of presentation of NS, and kidney biopsy before treatment was initiated (ISKDC 1978). The ISKDC patients were not selected for biopsy on the basis of their failure to respond to a course of oral steroids, as is the usual practice today. The study found 7% of NS patients had FSGS compared with 77% with minimal change disease (MCD). Of note, the study included patients referred to participating sites, and thus the results are not entirely generalizable to the overall NS population. Similar to ISKDC findings, the SPNSG found a prevalence of FSGS of 7.1% in 1031 biopsies (SPNSG 1985).
There is evidence that the incidence of FSGS has been increasing over time, from ~7% of biopsied NS cases in ISKDC and SPNSG to 23% in the 1980–1990s (Srivastava et al. 1999). In another population-based study of almost 300,000 children with idiopathic NS covering 17 years (1985–2002), there was a significant rise in the percentage of those having FSGS on biopsy from the first half (10.8%) to the second half (24.7%) of the study period; both were greater than the incidence found by the 1978 ISKDC and 1985 SPNSG studies (Filler et al. 2003). An informal meta-analysis has suggested about a doubling of the incidence (based on percentage of cases of nephrotic syndrome or percentage of biopsies) over the last three decades (Borges et al. 2007). Other studies have showed no secular change in FSGS incidence, but probably a greater frequency of steroid resistance among patients with FSGS (Banaszak and Banaszak 2012; Boyer et al. 2007).
Changes in biopsy practices are hard to exclude as a factor impacting the prevalence of FSGS found on biopsy. Only the ISKDC population was biopsied without any prior treatment (thus representing a relatively unselected population) (Churg et al. 1970). Thus, any recent estimates of FSGS incidence based solely on biopsy results may demonstrate selection bias for those patients with steroid-resistant disease. For example, a study of 152 patients recruited at time of NS presentation found that 31% did not undergo biopsy given a positive response to steroids and no or few relapses; of those who underwent biopsy, 31% had FSGS (Bonilla-Felix et al. 1999). Nonetheless, adult studies have similarly found an increase in FSGS incidence over time (Haas et al. 1995). As discussed below, the risk for renal decline in FSGS underlines the significance of a rise in disease incidence for public health.
There appear to be racial differences in FSGS incidence, although these are difficult to precisely define because of differing representations of different racial groups in various studies; the risk is probably greater in African-American children, while the relative risk for Hispanic children is still unclear. The lifetime risk of FSGS overall may be only about 0.24% (Kitiyakara et al. 2004), but clearly shows racial differences. As discussed later in this chapter, the discovery of the apolipoprotein L1 (APOL1) high-risk genotype in individuals with African ancestry may explain the ethnic disparities in the disease outcomes. Additionally, the incidence of FSGS is greater in adolescents compared to younger children (Boyer et al. 2007; Hogg et al. 2007).
Statistics on end-stage kidney failure (ESRD) prevalence have been detailed by the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS), a multicenter prospective study that has been collecting data on end-stage kidney disease in children since 1987 (Alexander et al. 1990). The first report covering 761 transplants in 754 patients, published in a 1989 report, found end-stage kidney disease due to FSGS as the third most common indication for kidney transplant (Alexander et al. 1990). FSGS was the primary diagnosis in 12% of transplant recipients and was greater for older children: 12% at 13–17 years as compared to 9% at 2–5 years. The most recent report, published in 2010, now encompassed data from 11,603 kidney transplants in 10,632 patients (Smith et al. 2013). Despite 20 years of new patient additions to the registry, FSGS remained the third most common primary diagnosis for ESRD at 11.7%, behind renal dysplasia at 15.8% and obstructive uropathy at 15.3%. Similarly, FSGS as a primary diagnosis again increased with patient age. In adults, review of data from the United States Renal Data Services indicates FSGS is the most common glomerulopathy associated with ESRD (Kitiyakara et al. 2003), consistent with pediatric studies.
Clinical Presentation and Features
FSGS results in proteinuria, and many patients can present with nephrotic syndrome (NS) – the clinical presentation of heavy proteinuria, hypoalbuminemia, and edema. Patients with FSGS have substantial morbidity and mortality, including a high incidence of progression to end-stage kidney failure and a risk of disease recurrence after kidney transplantation. While FSGS is treated as a single clinical entity, there is in fact a heterogeneous collection of etiologies that eventually result in the FSGS lesion. Over the past several decades, significant research has been dedicated to discovering the molecular mechanisms underlying FSGS, and defining clinical classifications that would permit personalization of prognosis and optimization of therapeutic regimens.
As noted above, studies have revealed that children with FSGS are more likely to present later and with resistance to corticosteroids. The ISKDC found a later age of onset for FSGS, with 50% of children presenting after age 6 versus only 20% of MCD patients with disease onset after this age (ISKDC 1978). Steroid responsiveness as a metric for NS disease classification was recognized from the 1981 report of the ISKDC. The ISKDC reported that 78% of NS patients had clinical remission by 8 weeks of steroid therapy (ISKDC 1981). Seventy percent of FSGS patients did not respond to steroid therapy. Currently, it is well accepted that most FSGS falls into the subset of steroid-resistant NS (SRNS). However, it cannot be assumed that all SRNS is FSGS, as SRNS encompasses other pathological diagnoses such as MCD, membranoproliferative glomerulonephritis (MPGN), and membranous nephropathy (MN).
Outcomes
Children with FSGS can develop a progressive decline in kidney function. A review of the Toronto Glomerulonephritis registry suggested that children with FSGS (not steroid responsive) have a renal survival rate of 60% at 10 years (Cattran and Rao 1998). Additional studies of children with SRNS (either due to minimal change disease or to FSGS) from different populations have found a similar rate of renal survival (60–80%) at 10 years (Martinelli et al. 2001; Mekahli et al. 2009; Paik et al. 2007; Trautmann et al. 2017). As discussed below, other than response to therapy, which predicts outcome in multiple studies, additional factors predicting the risk of kidney functional decline are not well established.
The high morbidity associated with FSGS has prompted a search for factors predictive of disease progression. Analysis of a single cohort of children with biopsy-proven FSGS identified age, serum creatinine, hematuria, and percentage of global sclerosis as factors predicting development of chronic kidney disease (CKD) (Abrantes et al. 2006). However, the best current predictor of progression of kidney disease is remission of proteinuria, which has been confirmed as a prognostic marker in several studies. Renal survival at 3 years can be seen in up to 90% who achieve complete or partial remission, whereas 50% of those who do not achieve remission have progression of CKD (Gipson et al. 2006). Recent analysis of the PodoNet international registry showed that 10-year renal survival for SRNS was 94% for those achieving complete remission in the first year and 72% for those achieving partial remission, but 43% for those with multidrug resistance (Trautmann et al. 2017). Partial remission itself is predictive of renal survival in adults, although those who relapse may have a more rapid rate of renal decline than those without relapse (Troyanov et al. 2005). In addition to remission status, ethnicity is increasingly recognized as a risk factor for renal functional decline. African-American (AA) ethnicity, as compared with non-AA ethnicity, was demonstrated to show increased risk and worse outcome for children with FSGS (Ingulli and Tejani 1991; Sorof et al. 1998). More recently, morphometry from diagnostic biopsies in a cohort of patients with primary proteinuric glomerulopathies has been strongly associated with change in eGFR, suggesting that morphometric analysis may potentially play a future role in estimating risk of renal functional decline (Lemley et al. 2016).
Pathology
The biopsy appearance of FSGS is variable. It was first described in children (Rich 1957). Characteristic (and required for the biopsy diagnosis) is the presence of segmental sclerotic lesions including capillary obliteration and often intracapillary PAS-positive hyaline deposition. Early on, these are both focal (found in only some glomeruli) and segmental (affecting only part of the glomerular capillary tuft). Also quite typical are various changes in the podocytes (vacuolization, microvillous transformation, protein reabsorption droplets, foot process effacement, condensation of cytoskeletal filaments in the bases of the foot processes); hyperplasia of podocytes on the glomerular basement membrane (GBM), sometimes called a “cap,” or conversely patches of bare GBM without any podocyte cover (or sometimes a “halo” of detached podocytes over multilayered, new loose GBM-like material); wrinkling of the GBM; intracapillary foam cells; some degree of mesangial expansion or hypercellularity; and/or synechiae or adhesions of the tuft to the overlying parietal cell layer of Bowman’s capsule. The immunofluorescence examination is generally negative or shows (what appears to be) nonspecific or passive mesangial deposition of small amounts of IgM or C3.
Interstitial fibrosis and tubular atrophy (IFTA) may be present to varying degrees for more advanced or more severe cases of FSGS. Foam cells may be present in the interstitium. The presence of IFTA in a biopsy without obvious segmental sclerotic lesions is suggestive of “missed FSGS,” since this strongly suggests the obliteration of glomeruli with subsequent atrophy of the attached tubules. Given the segmental presence of glomerular sclerosis, with lesions making up as little at 5–10% of the capillary tuft volume (Remuzzi et al. 1990), the chances of missing involved parts of a given glomerulus with a single sampling section are quite high. The estimated incidence of segmental lesions based on single section may be one third or less of the actual incidence (Remuzzi et al. 1995). Vascular changes are usually associated with hypertension as a secondary phenomenon.
The most commonly used classification system for FSGS is the Columbia classification (D’Agati 2003; D’Agati et al. 2004). In this scheme, five different morphological variants are distinguished: cellular, perihilar, tip, collapsing, and not-otherwise-specified (NOS). There is a general association of morphologic type with outcome (with respect to remission on therapy and loss of renal function), with tip lesions (more common among white patients) having the best overall outcomes and collapsing lesions (more common among African-American patients) having the worst outcomes.
The five Columbia variants are partly defined by exclusion among each other. The most common variant is the not-otherwise-specified (NOS) variant, also known as classical FSGS; it shows the required features of a segmentally sclerotic lesion, but lacks the defining characteristics of the other variants. It is thought that several of the other forms may “evolve” toward the NOS variant with time. The perihilar variant requires perihilar sclerosis or hyalinosis in >50% of the involved glomeruli. It excludes findings of the remaining variants. Glomerulomegaly and adhesions are common. This variant is commonly associated with hemodynamic (secondary) forms of FSGS. The cellular variant involves segmental, endocapillary hypercellularity (involving >25% of the tuft and leading to capillary occlusion). It excludes findings of the tip and collapsing variants. There may be infiltrating monocytes, lymphocytes, and neutrophils. The podocytes may be swollen and hyperplastic, leading to the appearance of a pseudocrescent (an extracapillary cellular aggregate not attached to Bowman’s capsule). Patients with this form may be more nephrotic and have a more rapid rate of disease development. The tip lesion variant has at least one glomerulus with either an adhesion or a confluence of podocytes near or protruding into the opening of the proximal tubule. Collapsing or perihilar lesions must be absent. The most aggressive variant is the collapsing lesion. It requires at least one glomerulus with segmental or global obliteration of the capillary lumina with wrinkling or collapse of the GBM, as well as podocyte hypertrophy and/or hyperplasia. A single glomerulus with such features of collapse pre-empts the diagnosis of the other variants. The form often has a malignant course to ESRD with severe NS, although recent evidence suggests that – after controlling for baseline clinical characteristics and immunotherapy exposure – the chances of remission and the risks of renal failure are similar to NOS (Laurin et al. 2016). Podocytes may be de-differentiated and stain for Ki67, a marker of cell proliferation. Generally, there is a loss of endocapillary cells. Whether the collapsing variant results from dysregulated proliferation of podocytes or – as with other forms of FSGS – there is net loss of podocytes is still unclear. No study using stereologically valid methods to estimate podocyte number in this variant has been reported; in the setting of a shrinking “reference volume” (the glomerular tuft), the subjective impression of crowding of podocytes on the tuft cannot be automatically interpreted as representing an increased number of these cells. The presence of tubuloreticular inclusions in this variant suggests HIV-associated nephropathy (HIVAN).
The pathological form of C1q nephropathy is a form of FSGS with variable mesangial hypercellularity with paramesangial C1q deposits (usually also containing IgG, IgM, and/or C3). Most patients with this lesion show NS and some amount of CKD. The lesion of diffuse mesangial sclerosis (DMS) will not be specifically addressed (see section on Genetics). This form of podocytopathy is substantially different from most forms of FSGS and very likely results from some unique pathobiological features. This histopathology lesion is often seen in infants with congenital NS.
There is some debate as to whether or not the segmental sclerotic lesions of FSGS are reversible (Benigni et al. 2011; Remuzzi et al. 2006), specifically under renin-angiotensin blockade. Such a question is not easily addressed experimentally (even in animal models of FSGS) since one cannot sample the same tissue twice.
The reported higher propensity of glomeruli in FSGS to be in the juxtamedullary region may be an important feature (Rich 1957), although the basis of this reported preferential involvement is not understood. The significance of glomerular hypertrophy in the propensity for FSGS in this region is also not clear, as stereological autopsy studies in adult men showed equivalent or smaller glomerular volumes in juxtamedullary glomeruli (Samuel et al. 2005). It is also possible that hypertrophic glomeruli may reflect preceding glomerular loss (compensatory hypertrophy of remnant glomeruli) or congenital glomerulopenia, both leading to increased susceptibility to subsequent glomerular injury. Children with MCD who have larger glomeruli on their initial biopsy are more likely to “evolve” to FSGS over time (Fogo et al. 1990). The concept of a “morphological transition” from minimal change disease to FSGS has been proposed (Tejani 1985). This relates to the concept of MCD and FSGS lying on a common (connected) spectrum of disease. The difficulties with such a proposal include the potential selection bias of patients receiving follow-up biopsies (suggesting more severe or treatment-resistant disease) and the substantial risk of “missed” FSGS in the early biopsies, especially if the number of glomerular tufts sampled is inadequate (Corwin et al. 1988).
Taxonomy of FSGS
A taxonomy is an organizational principle based on hierarchical relationships resulting from structural similarities. The goal of a taxonomy of FSGS is to predict prognosis and response to therapy. A better molecular understanding of podocyte pathobiology together with advances in histological analysis holds the promise for the development of a taxonomic classification of FSGS that integrates gene expression, cell biology, and histological and clinical manifestations (Barisoni et al. 2007; Kretzler and Sedor 2015). The “new taxonomy” is intended to be mechanistic rather than purely descriptive; it supports the development of targeted treatments (precision medicine). It is based on two axes: an axis of histology (MCN, FSGS, DMS, CG) and one of etiology (idiopathic, genetic, reactive). It is likely that with advances in understanding the underlying unifying mechanisms at work in the NS, additional axes (transcriptomic, biomarker-related) will be added to an expanded taxonomy (Gadegbeku et al. 2013).
Pathogenesis
Three broad categories of mechanisms can be considered to cover the majority of cases: genetic, immune-related signaling, and hemodynamic. Of these, the first category encompasses pathogenic variants of podocyte-expressed genes leading to dysfunction of distinct cellular mechanisms, such as calcium signaling, the actin cytoskeleton, or structural proteins regulating the filtration slit diaphragm. The second has traditionally been considered to be due to the effects of various circulating proteins of the immune system (e.g., products of T lymphocytes) largely based on the salutary effects of immune-modulating agents, such as steroids and cyclosporine. Recent cell biological studies, however, have shown this association to be more complex than a purely immune phenomenon, as several effective immunosuppressive therapeutic agents have been shown to have direct, nonimmune-mediated effects on various components of the podocyte considered to be pivotal to normal function. Various malignancies (Hodgkin lymphoma, adenomas, mesotheliomas) may also release circulating factors that adversely influence the podocyte. Finally, the third broad category reflects structural and functional adaptations to renal mass reduction triggering compensatory hyperfunction (and hypertrophy) at the single glomerulus level. Other stimuli may also lead to intracapillary hypertension with similar results, such as obesity or sickle cell disease. Aside from the three major categories, less frequent causes are podocytopathies associated with infectious agents, specific medications/drugs, and pre-eclampsia, among others (see Table 1).
Primary pathogenic causes of FSGS (genetic, hemodynamic, circulating factors, etc.) must be distinguished from disease modifying factors, which may influence the rate of progression of CKD in the setting of FSGS. Such factors include congenital glomerulopenia (probably represented by glomerulomegaly, as in oligomeganephronia, but also in certain at-risk populations), genetic variants (such as risk alleles in APOL1), and obesity, among others. At least some of these factors seem to be related to a relative insufficiency of podocytes.
Genetic Disease
The past two decades have seen a virtual explosion in our understanding of the genetics underlying NS. Initial genetic studies using the time- and labor-intensive method of positional cloning in kindreds with familial FSGS/SRNS discovered causal mutations in several genes (NPHS1, NPHS2, ACTN4, TRPC6, INF2). Recent advances in sequencing technology have facilitated whole-exome sequencing in affected families, resulting in a rapid increase in the discovery of causative genes. Over 30 genes have now been implicated in the pathogenesis of FSGS/SRNS, and most of the gene products localize to the podocyte (Hall and Gbadegesin 2015). These genetic discoveries have provided novel insights into the molecular mechanisms underlying the structure and regulation of the slit diaphragm, the role of the actin cytoskeleton, and the importance of energetics and mitochondrial metabolism in podocytes. Additionally, early studies have suggested that those patients with a monogenic cause of NS may represent a unique subset of NS, with greater resistance to immunosuppressive therapy and lower likelihood of posttransplant recurrence compared with nonmonogenic disease (Benoit et al. 2010; Buscher et al. 2016; Buscher et al. 2010; Ruf et al. 2004; Weber et al. 2004) (see Table 2).
NPHS1: An early discovery of a monogenic form of NS emerged from the study of congenital NS of the Finnish type (CNF), a distinct entity characterized by massive proteinuria, often starting in utero, with early progression to end-stage kidney disease (Hallman and Hjelt 1959). Mutations in NPHS1, which encodes the protein nephrin, a 1241 amino acid Ig-like transmembrane protein, was identified as the monogenic cause of CNF (Kestila et al. 1998). Nephrin localizes to the slit diaphragm, the narrow region between interdigitating foot processes of podocytes (Holthofer et al. 1999; Holzman et al. 1999; Ruotsalainen et al. 1999). Using electron microscopy, nephrin has been shown to form strands that resemble the “zipper-like” structure of the healthy slit diaphragm (Wartiovaara et al. 2004). The extracellular domains of nephrin have been demonstrated to form homophilic interactions, suggesting nephrin molecules may form cell-cell adhesions between podocytes (Khoshnoodi et al. 2003). However, more recent experimental evidence suggests that nephrin may have different role in a multilayered protein scaffold that maintains the interpodocyte filtration slit (Grahammer et al. 2016). Aside from a structural role, nephrin expression seems to underlie a signaling pathway (Huber et al. 2003a). For example, nephrin has been shown to bind Nck, an adaptor protein that controls the podocyte actin cytoskeleton, and the nephrin-Nck interaction is needed for actin reorganization (Jones et al. 2006). These studies suggest nephrin may serve as a signaling platform, acquiring information from the slit diaphragm and translating it to the podocyte actin cytoskeleton.
NPHS1-related NS has been classified as having an autosomal recessive Mendelian inheritance pattern. Two NPHS1 variants (Fin-major and Fin-minor) were the most common variants initially identified (Kestila et al. 1998). In the homozygous state, these particular variants lead to a clinically severe phenotype of CNF with early progression to end-stage kidney disease (ESKD) (Patrakka et al. 2000). In addition to early-onset disease, a growing body of evidence has implicated NPHS1 in the development of FSGS later in life. Santin and colleagues reported 4 children and 1 adult with FSGS-associated NPHS1 variants (Santin et al. 2009b). In all five of these individuals, there was compound heterozygosity for NPHS1. Likewise, Philippe and colleagues reported one familial case and nine sporadic case of NPHS1 compound heterozygosity (Philippe et al. 2008). Of these, three (all sporadic) had FSGS; of these, all had steroid resistance and two had progression to ESKD in the second decade of life. Given the importance of nephrin to maintaining the slit diaphragm, it is not surprising to see a phenotypic spectrum, with milder variants postulated to result in later onset of disease (Kitamura et al. 2007; Wong et al. 2013).
NPHS2: Positional cloning identified NPHS2 , which encodes the protein podocin, as a causative gene in familial FSGS (Boute et al. 2000). Podocin is a 383 amino acid transmembrane protein that is localized to the podocyte foot process at the slit diaphragm (Roselli et al. 2002). Podocin may form oligomers in lipid raft microdomains, potentially acting as a protein scaffold (Schwarz et al. 2001). Indeed, podocin has been shown to interact with nephrin at the slit diaphragm, and podocin mutations can disrupt nephrin targeting to lipid rafts, and thus nephrin-dependent signaling (Huber et al. 2001; Huber et al. 2003b). These findings highlight a putative mechanistic role for podocin at the glomerular filtration barrier.
NPHS2-associated FSGS was initially characterized by an autosomal recessive Mendelian inheritance pattern, childhood onset, and early progression to ESKD (Boute et al. 2000). Further studies demonstrated progression to ESKD often within the first decade of life (Hinkes et al. 2008). In addition to familial cases, causal NPHS2 variants have been identified in sporadic FSGS cases as well (Caridi et al. 2001; Karle et al. 2002). To date, over 100 variants have been identified, extending across NPHS2’s entire coding region (Bouchireb et al. 2014). The common R229Q NPHS2 missense variant is found in about 3% of European individuals (Tsukaguchi et al. 2002). While common, it can cause NS in the setting of compound heterozygosity with other specific NPHS2 mutations (Machuca et al. 2009; Santin et al. 2011). In these situations, it appears disease-causing variants resulting in C-terminal substitutions exert a dominant negative effect on R229Q podocin’s ability to heterodimerize and localize to the slit region (Tory et al. 2014).
WT-1: The WT-1 gene was initially mapped given its association with Wilms’ tumor – one of the most common types of malignancy in children (Call et al. 1990). WT-1 was identified as a zinc-finger containing transcription factor expressed in the kidney, which acts a tumor suppressor, as haploinsufficiency resulted in development of Wilms’ tumor (Haber et al. 1990). Further studies of WT-1 identified an association with glomerular diseases, with different phenotypes based on specific patterns of genetic variation. Denys-Drash syndrome involves the constellation of DMS and associated renal functional decline, pseudohermaphroditism, and Wilms’ tumor and has been associated with mutations in exons 8 and 9 (Pelletier et al. 1991). Frasier syndrome involves male pseudohermaphroditism, streak gonads, and FSGS, and involves alternative splicing of intron 9 resulting in inclusion of 3 additional amino acids (KTS isoform) (Barbaux et al. 1997).
TRPC6: Variants in TRPC6 were first identified in familial FSGS with autosomal dominant inheritance, characterized by development of heavy proteinuria in the third or fourth decade of life and progression to end stage in around 10 years (Winn et al. 2005). Subsequently, nonfamilial cases and childhood-onset presentation have been demonstrated (Santin et al. 2009a). TRPC6 encodes TRPC6, a member of the transient receptor potential (TRP) family of cation channels, which seem to act as cellular sensors via calcium currents (Clapham 2003). Indeed, some TRPC6 variants result in altered calcium influx (Reiser et al. 2005; Winn et al. 2005). TRPC6 is located at the slit diaphragm in association with nephrin and podocin (Reiser et al. 2005). Thus, TRPC6 may act to communicate between the slit diaphragm and the intracellular networks of the podocyte and has been highlighted as a potential therapeutic target.
ACTN4: Variants in ACTN4 were first identified in familial FSGS with autosomal dominant inheritance, characterized by development of mild proteinuria in adolescence and slow progression of renal dysfunction (Kaplan et al. 2000). Subsequently, nonfamilial cases and childhood-onset presentation have been demonstrated (Choi et al. 2008; Weins et al. 2005). ACTN4 encodes alpha-actinin-4, an actin-binding and cross-linking protein (Weins et al. 2007). Identified variants have been clustered around the actin-binding domain, suggesting variants alter alpha-actinin-4’s role in regulation of the podocyte actin cytoskeleton.
INF2: Variants in INF2 were first identified in familial FSGS with autosomal dominant inheritance, characterized by development of moderate proteinuria in adolescence and early adulthood with subsequent progression to end-stage disease (Brown et al. 2010). The initial phenotype was comparable to ACTN4-associated FSGS, and interestingly, INF2 encodes an actin-binding protein with roles in accelerating actin polymerization. Additional familial cases with childhood-onset and intrafamilial phenotypic variability were subsequently identified (Lee et al. 2011).
LMX1B: A recently described genetic cause of familial FSGS has been a specific mutation in the LIM-homeodomain transcription factor, LMX1B . Like many other genes mentioned in this section, LMX1B is expressed specifically in the podocyte (in postnatal life). Mutations in this gene have long been known to cause the multisystem disorder, nail-patella syndrome (OMIM 161200). Severe renal manifestations in this disorder do not segregate with the LMX1B mutation, even within a family, suggesting that sequence variation in an LMX1B-regulated podocyte gene may be required for the severe renal phenotype (Lemley 2009). Recently, amino acid variation at a single residue (R246Q) in the homeodomain region of the protein has been shown to cause an autosomal dominant, heritable form of FSGS, without the usual skeletal and other extrarenal manifestations of nail-patella syndrome (Isojima et al. 2014). In addition to findings characteristic of FSGS, LMX1B nephropathy also may show the ectopic presence of type III collagen within the GBM. A small minority of patients with nail-patella syndrome may progress to ESRD even during childhood. These individuals will typically have a preceding phenotype including the nephrotic syndrome (Lemley 2009).
In addition to the aforementioned genes, over 20 other genes have been identified, each with important putative roles at the glomerular filtration barrier. While efforts are ongoing to identify novel FSGS-associated genes, a recent focus of research has been identifying the prevalence of monogenic disease using large NS cohorts. The PodoNet Consortium registry contains over 1500 patients with childhood-onset steroid-resistant NS, congenital NS, or subnephrotic proteinuria of potential genetic origin, recruited from over 20 countries. Sequencing of 1174 individuals has identified a genetic cause in 23.6% (Trautmann et al. 2015). In a separate cohort of 1783 unrelated, international families with steroid-resistant NS, sequencing of 27 genes identified a genetic cause for NS in 29.5% of all cases, but a bimodal distribution, with 12–14% having genetic causes among US patients, while 45% of patient from Middle Eastern countries had definable genetic causes (Sadowski et al. 2015). The incidence of sporadic NS in unselected, admixed populations has also been investigated. Sequence analysis of 312 individuals from NEPTUNE study, which enrolled North Americans with proteinuric kidney disease suspected of being MCD, FSGS, or membranous nephropathy (MN) without a known history of familial disease, and irrespective of response to therapeutics, found an incidence of monogenic disease of only 2.9% in sporadic NS (Sampson et al. 2016a). Through such large scale screening efforts, novel variants are continuously identified in these monogenic genes, and a critical goal of genetic research is appropriate attribution of causality, given the implications for genotype-phenotype correlations and subsequent prognostic and therapeutic decision-making.
Regardless whether considered as either familial or sporadic disease, monogenic disease represents only a fraction of FSGS, and it remains as yet unclear to which degree other non-Mendelian forms may contribute to the burden of genetic FSGS. Digenic inheritance of NPHS1 and NPHS2 variants (primarily the R229Q NPHS2 variant) has been reported in cases of congenital NS, suggesting that non-Mendelian genetic variation could contribute to glomerular phenotype (Koziell et al. 2002; Schultheiss et al. 2004). Sequencing of NS patients may identify causal variants, but may also incidentally identify secondary variants with unknown phenotypic contribution (Weber et al. 2016). However, recent work by Crawford et al. did not identify digenic heterozygosity or oligogenicity in 21 known monogenic NS genes as a contributor to NS in a large US cohort, suggesting that this form of inheritance is unlikely to have a large role in causing NS (Crawford et al. 2017).
In addition to rare causal variants (“mutations”), research over the past decade has highlighted the role of genetic variants that increase the risk of NS in a non-Mendelian manner, such as common variants in APOL1 in blacks with FSGS, as discussed below.
Apolipoprotein L1 (APOL1): APOL1 encodes apolipoprotein L1, a protein component of high-density lipoprotein and of the trypanosome lytic factor in human serum, which confers resistance against potentially lethal African sleeping sickness. Two coding variants in APOL1, termed G1 (a nonsynonymous coding variant) and G2 (a 6 base-pair deletion), common in individuals with recent African ancestry but absent in European populations, are highly associated with increased risk of FSGS and ESRD (Genovese et al. 2010; Tzur et al. 2010). These APOL1 variants restore trypanolytic activity, which led to its strong positive selection, and subsequent common frequency in those of recent African origin, particularly west African (Genovese et al. 2010).
APOL1 is only present in a few primate species including humans, suggesting it is not universally required for mammalian kidney development or maintenance. Although APOL1 circulates through bloodstream, plasma levels have not correlated with APOL1 genotype or CKD (Bruggeman et al. 2014; Kozlitina et al. 2016). The ways by which APOL1 variants cause kidney disease and damage are not fully understood, although diverse mechanisms have been suggested, such as potassium efflux leading to cytotoxicity (Olabisi et al. 2016). To explore the role of APOL1 variants, several transgenic mouse models have been developed. Transgenic mice with noninducible, podocyte-specific expression of APOL1 G2 variant did not demonstrate any proteinuria or histologic findings of glomerulosclerosis, as compared to mice with G0 reference allele, but did develop a pregnancy-associated phenotype (Bruggeman et al. 2016). Of note, transgenic APOL1 expression was noted to be variable in this model system. More recently, transgenic mice with podocyte-specific conditional, inducible-expression of either G1 or G2 variant developed azotemia and albuminuria and had histological findings of glomerulosclerosis, whereas mice expressing reference allele did not display this phenotype; additionally, there was a correlation between risk-variant expression levels and phenotype (Beckerman et al. 2017). At a molecular level, APOL1 variants disrupted endosomal trafficking and hence decreased autophagic flux, enhancing inflammatory-mediated cell death. Further research is needed to expand our understanding of how high-risk variants of APOL1 contribute to FSGS pathogenesis and progression of any form of CKD.
Initial reports suggested that kidney disease is associated with these APOL1 variants only in the recessive model (homozygosity or compound heterozygosity) (Genovese et al. 2010). Also known as the “high risk” (HR) genotype, those harboring two risk alleles demonstrate an earlier onset of FSGS and faster progression to ESRD as compared to African-Americans having zero or one variant, the “low risk” (LR) genotype (Kopp et al. 2011). In two cohorts of African-American NS patients with variable histopathologic findings from the NEPTUNE and FSGS Clinical Trial studies, HR genotype was associated with higher tubulointerstitial disease on histopathology (Kopp et al. 2015; Sampson et al. 2016b). Black children with NS and a HR genotype have lower eGFR on presentation, faster decline in eGFR over time, and increased odds of having been born preterm (Ng et al. 2016).
APOL1 variants are common, with 13% of African-Americans having the high-risk genotype, with an associated estimated lifetime FSGS risk of 4% (Kopp et al. 2011). Given this high prevalence, there has been interest in ascertaining the clinical utility of APOL1 genotyping. One area of prime interest is in regards to kidney transplantation. Recipient APOL1 genotype status has not been shown to affect 5-year survival of deceased donor grafts (Lee et al. 2012). However, several reports have demonstrated that HR APOL1 genotype in the deceased donor kidney is associated with earlier allograft failure, controlling for other factors affecting allograft such as cold-ischemic time, HLA match, and various recipient characteristics (Freedman et al. 2015; Freedman et al. 2016; Reeves-Daniel et al. 2011). These studies have introduced the question of whether APOL1 genotyping should play a role in deceased donor kidney allocation. Some authors have argued that rapid APOL1 genotyping should become routine for deceased donor kidneys, although others have argued against it (Freedman and Julian 2015; Ross and Thistlethwaite 2016). As donor kidneys are in short supply, further research is needed to define the role of APOL1 genotyping in organ allocation.
Circulating Factors and Biomarkers
The high recurrence rate of FSGS following renal transplantation and the beneficial effect of plasmapheresis on disease recurrence have led many to hypothesize that a circulating “permeability” factor may contribute to disease pathogenesis in some cases (Hickson et al. 2009; Mahesh et al. 2008). The loss of renal allografts to disease recurrence in pediatric patients is not negligible. Review of the 2001 NAPRTCS registry indicated that 15% of graft failure in patients transplanted for FSGS was due to disease recurrence (Baum et al. 2002). Numerous investigators have sought to identify the putative circulating factor causing disease to better assess risk and suggest effective interventions. Several candidates (e.g., soluble urokinase plasminogen activator receptor [suPAR], hemapexin, cardiotrophin-like cytokine-1 [CLC-1]) have been suggested. However, at this time, the identity of the responsible circulating factor(s) remains unclear.
suPAR was experimentally shown to lead to foot process effacement via activation of αvβ3 integrin, which attaches podocytes to the glomerular basement membrane; integrin activation has been shown to promote cellular motility (Wei et al. 2008). In initial cohort comparisons, patients with FSGS had higher suPAR levels than healthy controls or patients with other glomerular diseases (Wei et al. 2011; Wei et al. 2012). This initial experimental evidence raised the possibility that integrin blockade could prevent downstream effects that lead to podocyte disruption and proteinuria; however, integrin blockade has not thus far been substantiated as a useful therapeutic target. In addition, subsequent studies have failed to demonstrate that higher suPAR levels are specifically associated with FSGS (Bock et al. 2013; Franco Palacios et al. 2013; Spinale et al. 2015).
Biochemical purification methods have been used to attempt isolating the focal sclerosis permeability factor (FSPF) from plasma of FSGS patients (Sharma et al. 2004). Given the potential for a circulating factor to interact with the glycocalyx, galactose-affinity chromatography was applied to plasma from FSGS patients, and identified circulating cardiotrophin-like cytokine factor 1 (CLC-1) as the putative factor (McCarthy et al. 2010). Galactose therapy was then tried in a case report, as galactose bound the permeability factor (Savin et al. 2008). Use of oral galactose in a series of children did show decreases in bioassayable FSPF, but no change in proteinuria (Sgambat et al. 2013). The FONT trial (Novel Therapies for Resistant Focal Segmental Glomerulosclerosis) attempted to test the efficacy of galactose as a therapy for FSGS, but fell short of patient recruitment goals (Trachtman et al. 2015a). Thus, the role for galactose as a treatment for FSGS remains unclear.
Some biomarkers have been identified that may help to differentiate between MCD and FSGS. CD80 (also known as B7-1), which is present on antigen-presenting cells, is a membrane protein involved in providing a costimulatory signal for T cell activation. CD80 is also in found on the podocyte, where it is upregulated in experimental models of NS, potentially acting as a modifier of glomerular permselectivity and a component of cellular danger signaling machinery (Reiser et al. 2004). Urinary CD80 levels have been found to be elevated in patients with relapsed MCD, but not in patients with MCD in remission or in FSGS patients (Garin et al. 2009; Garin et al. 2010). Thus, urinary CD80 may be useful to discriminate between MCD and FSGS, although studies on larger patient populations are necessary. An inhibitor of B7-1 (CD80), abatacept (cytotoxic T-lymphocyte-associated antigen 4-immunoglobulin fusion protein [CTLA-4—Ig]), which has been approved for treatment of rheumatoid arthritis, has also been investigated as a treatment for FSGS. In a small cohort of 5 patients with either primary or recurrent FSGS, abatacept resulted in partial or complete remission (Yu et al. 2013). In in vitro experiments, abatacept restored β1 integrin activation and blocked podocyte migration, suggesting a biological mechanism in glomerular disease whereby B7-1 promotes podocyte migration through β1 integrin inactivation (Yu et al. 2013). Based only on a small collection of case studies, the role for podocyte CD80 targeted inhibition with abatacept remains interesting and is being evaluated in an ongoing randomized clinical trial (Mundel and Greka 2015).
An older biomarker – both of histology and of steroid responsiveness – is the selectivity of proteinuria (Cameron 1968; Ellis and Buffone 1981; Lines 1969). This biomarker seems to have been forgotten, rather than disproved or supplanted by a superior alternative. Selectivity refers to the relationship of specific proteins’ urinary clearances to their molecular weights (MW), traditionally, the slope of the fit line for several proteins’ clearances to their MW, ranging from orosomucoid (MW 40 kD) or albumin (MW 68 kD) to α2-macroglobulin (MW 840 kD), plotted on a log-log scale; more simply as the relative clearances of IgG (MW 160 kD) and transferrin (MW 90 kD). A more negative slope (or lower ratio) is considered to represent greater selectivity. The predictive ability of the selectivity index to distinguish MCD from FSGS (or steroid-resistant NS) was greater in some studies (absolute, for example, in (Lines 1969)) than in others (Cameron 1968; Ellis and Buffone 1981). Protein selectivity has biological plausibility as a possible index of different forms of podocyte dysfunction, e.g., disruption of normal slit diaphragm function (high selectivity) versus podocyte detachment (low selectivity). Whether a reconsideration of this biomarker (using easier ELISA technology) in comparison to urinary CD80 levels, for example, is worthwhile remains to be seen.
Hemodynamic
FSGS due to hemodynamic derangements would be classically considered as a secondary form of FSGS. Hyperfunction injury is the paradigm case. This results from compensatory hypertrophy and hyperfunction of remnant nephrons attendant to a significant loss of functional renal mass, as occurs following subtotal nephrectomy. Particularly exuberant responses to the hypertrophic stimulus (as seen after unilateral nephrectomy in rapidly growing young rats (Nagata et al. 1992)) result in excessive compensatory glomerular hypertrophy, which may lead to relative podocyte insufficiency, even if no podocytes are lost initially. It is tempting to posit that another example of such imbalanced, exuberant growth may occur in children with premature birth or low birth weight (leading to lower glomerular number (Manalich et al. 2000)), especially if coupled with subsequent excessive catch-up growth during childhood leading to excessive glomerular hypertrophy (Barker et al. 2005). This class of FSGS often shows less foot process effacement and greater variability of foot process morphology even among the foot processes of a single podocyte, suggesting the influence of local mechanical (rheological) forces on foot process geometry (Kriz and Lemley 2016).
There seems to be a convergence of various initial etiologies of disease to a final pathomechanism of progression based on podocyte “insufficiency,” viz., an inadequate number of podocytes to assure the stability of an enlarged glomerular tuft (Fries et al. 1989). Why this is relentlessly progressive (despite the undeniable beneficial effects of angiotensin blockade) is subject to debate. It has been suggested that “podocyte damage damages [other] podocytes” (Ichikawa et al. 2005)), presumably based on loss of protective autocrine factors. Progression from segmental scarring to global glomerular sclerosis may depend on the role of the RAAS in adapting to the loss of ultrafiltration capacity and compensatory functional effects activated by tubuloglomerular feedback (Lemley 2012). Alternatively, the loss of lateral stabilization against shear forces by slit diaphragms between neighboring podocyte foot processes may explain the fact that after a certain degree of podocyte loss, the further loss of podocytes is autonomously progressive (Fukuda et al. 2012; Kriz and Lemley 2016).
What seems to be indisputable is that for many podocytes, detachment from the glomerular tuft occurs as viable cells (Vogelmann et al. 2003). This has been suggested to result from a very specific mechanism of podocyte detachment in which elevated shear stresses on the filtration slits (from sustained hyperfiltration) result in shearing forces that may strip otherwise viable podocytes off of the GBM, often still attached by intercellular junctions to their neighboring, equally viable podocytes (see Fig. 1) (Kriz and Lemley 2016; Lemley 2016). That shear stress, rather than increased intracapillary hydrostatic pressure, is the major influence on podocyte detachment is suggested by the fact that the typical morphological variant for this type of FSGS is the perihilar one. Local filtration rates and shear stresses in the filtration slits are highest at the beginning of the capillary branching at the afferent arteriole, near the hilum, and fall steadily as ultrafiltration raises the oncotic pressure of the capillary plasma, countering the net hydrostatic driving pressure for filtration and possibly reaching a point where no further filtrate crosses the filtration slits (Fig. 2).

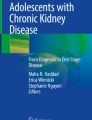
FSGS features and Columbia classification variants. (a) Adhesions or synechiae, a very early sclerosing lesion, may form between the sclerosing segment and Bowman’s capsule as podocytes become depleted through detachment or cell death. An open capillary loop connects to Bowman’s capsule via minimal matrix deposition (blue arrow) (Jones methenamine silver, x400). (b) NOS, not otherwise specified, is the usual (classic) histologic pattern of FSGS. It is defined by segmental obliteration of the glomerular capillary lumina by increased extracellular matrix and/or hyalinosis that does not meet defining criteria for any other variant. It is the most common variant and can present with either nephrotic syndrome or subnephrotic proteinuria. NOS can occur in patients with primary FSGS or diverse secondary forms, including genetic FSGS (Jones methenamine silver, x400). (c) Perihilar variant is defined as perihilar hyalinosis and sclerosis at the vascular pole involving the majority (>50%) of glomeruli with segmental lesions. It may be found in primary FSGS but is particularly common in adaptive FSGS, where it is usually accompanied by glomerular hypertrophy (glomerulomegaly). Patients with adaptive FSGS and perihilar variant are more likely to present with subnephrotic proteinuria and normal serum albumin levels (Periodic acid-Schiff, x400). (d) Tip variant is defined by the presence of at least one segmental lesion involving the tip domain, next to the origin of the proximal tubule, with either extracellular matrix adhesion to the tubular outlet or confluence of visceral cells with parietal or tubular epithelial cells (blue arrow). Intracapillary foam cells are frequently seen. It is more common in Caucasians and typically presents with abrupt onset of full nephrotic syndrome. Most cases are primary. It has the most favorable outcome with the highest rate of steroid responsiveness, the best preservation of renal function, and the least tubulointerstitial injury at biopsy (Periodic acid-Schiff, x400). (e) Cellular variant is defined by at least one glomerulus with an expansile segmental lesion featuring endocapillary hypercellularity, often including foam cells and infiltrating leukocytes (blue arrow). Segmental sclerosis is not required. This is the least common variant. It usually presents with nephrotic syndrome, and most cases are primary (Periodic acid-Schiff, x400). (f) Collapsing variant is defined by the presence of at least one glomerulus with either segmental or global implosive glomerular capillary wall collapse with hypertrophy and hyperplasia of the overlying glomerular epithelial cells. This is the most aggressive variant with worst renal function at presentation, severe markers of nephrotic syndrome, the strongest black racial association, the lowest rate of therapy response, and the most rapid progression to renal failure. It can occur in primary FSGS as well as secondary forms related to interferon therapy, pamidronate therapy, HIV infection, parvovirus B19 infection, acute ischemia, and rare genetic forms (Jones methenamine silver, x400). (g) Transmission electron microscopic view of the normal glomerular capillary wall showing intact podocyte foot processes above the glomerular basement membrane (x10,000). (h) Transmission electron microscopic view of a glomerular capillary in FSGS showing podocyte foot process effacement above the glomerular basement membrane (x10,000)

Detachment of viable podocytes from the GBM (yellow). Lumens of capillaries are highlighted in green and the space between podocytes and GBM in pink. (a) Three podocytes are detaching (1–3). Podocytes 1 and 3 have extensive foot process effacement. Podocyte 2 is widely detached from the GBM, although still connected to its neighboring podocytes by intercellular junctions (arrows). (b) A similar situation of detachment of three podocytes. Cell nuclei of all podocytes have normal chromatin patterns (no apoptosis). Both a and b from rats with Masugi nephritis (days 28 and 7, respectively). Bar, 5 μm (Reprinted from Kriz et al., Am J Physiol Renal Physiol., 304:F333–47, 2013)
Angiotensin blockade is particularly protective in the setting of hemodynamic glomerular injury. By almost doubling the ultrafiltration coefficient (possibly by capillary remodeling), enalapril likely led to halving the net driving forces for glomerular filtration along the entire length of the glomerular capillaries after subtotal nephrectomy in rats (Lemley 2016).
Hemodynamic factors are probably also drivers of glomerular pathology in obesity-related FSGS (which has also been described in children), low congenital nephron number, polycythemia, sleep hypoxia, sickle cell disease, and cyanotic congenital heart disease (Adelman et al. 2001; Falk et al. 1992; Hida et al. 2002; Hodgin et al. 2009; Kambham et al. 2001; Tejani et al. 1985).
Treatment
Treatment of FSGS is aimed at reducing proteinuria with the overall goal of preserving kidney function. As noted above, achieving partial or complete remission is prognostic for renal survival. Current treatment options to achieve this goal include steroids, immune-based therapies (calcineurin inhibitors, or CNIs), antimetabolites, biologics), as well as other strategies, such as renin-angiotensin-aldosterone system blockade. FSGS treatment has been reviewed recently (Hodson et al. 2010; Sethna and Gipson 2014). Therapeutic decisions are based on responsiveness to initial treatment with steroids (sensitive or resistant).
In younger children, following the presentation of NS, corticosteroids are empirically started, based upon the findings of the ISKDC study suggesting a high likelihood of favorable histology (MCD) and positive disease response to treatment (ISKDC 1981). Thus, biopsy is often deferred at initial presentation, unless atypical signs (e.g., renal insufficiency, gross hematuria, hypertension) necessitate a histologic diagnosis. In the ISKDC, the majority (70%) of children with FSGS did not respond to steroids, although the sample size was small. Likewise, the SPNSG found that 40 of 56 patients (71%) with FSGS did not respond (SPNSG 1985). A lack of steroid response is often the motivating factor for a kidney biopsy, which can then identify FSGS as the histopathologic diagnosis. In addition, given the importance of achieving remission of proteinuria to renal survival, a lack of steroid response often necessitates administration of other agents to attempt to control proteinuria. In addition, even when FSGS does respond to steroids, the benefits of achieving remission are often balanced with the side effects of prolonged steroid use (growth delay, hypertension, weight gain, and Cushingoid appearance, amongothers). Thus, despite steroid sensitivity, alternate agents are often needed to reduce overall steroid exposure.
As the majority of cases of FSGS represent steroid-resistant NS (SRNS), the following treatment discussion will focus on SRNS. For SRNS, the Kidney Disease: Improving Global Outcomes (KDIGO) organization recommends CNIs – cyclosporine or tacrolimus – as a first-line treatment (KDIGO 2012). Several early randomized trials demonstrated that cyclosporine, as compared to placebo, is better able to achieve remission (Lieberman and Tejani 1996; Ponticelli et al. 1993)). However, cyclosporine does have significant cosmetic side effects, such as hypertrichosis (excess hair growth) and gingival hyperplasia as well as nephrotoxicity, hyperlipidemia, and hypertension (El-Husseini et al. 2005). Thus, tacrolimus, another CNI, has emerged as a treatment with comparable efficacy as cyclosporine but less cosmetic side effects and a better cardiovascular risk profile (Choudhry et al. 2009). CNIs are commonly used for immune suppression following solid organ transplantation, and their successful use in NS has suggested that these agents alter immunological mechanisms underlying NS. However, cyclosporine has been shown to directly stabilize the actin cytoskeleton in podocytes, highlighting a novel mechanism for its antiproteinuric effect (Faul et al. 2008). Nonetheless, since both cyclosporine and tacrolimus can cause hypertension and nephrotoxicity, often prompting the need for surveillance biopsies to assist with risk and benefit analysis of ongoing CNI use, alternative therapies have been sought.
In addition to CNIs, KDIGO recommends use of either angiotensin-converting enzyme inhibitors (ACEi) or angiotensin receptor blockers (ARBs), agents that alter the renin-angiotensin-aldosterone system (RAAS). Addition of fosinopril to steroid therapy was more effective than steroid only therapy in reducing proteinuria (Yi et al. 2006). Alongside tapering steroid therapy, higher dose enalapril was more effective in reducing proteinuria than lower dose (Bagga et al. 2004). These agents act to decrease GFR and can lead to azotemia and hyperkalemia, necessitating laboratory monitoring; caution should be used in those with significantly decreased kidney function, given the potential for hyperkalemia. Lastly, RAAS inhibition can result in fetal malformations; thus, the use of ACE inhibitors or ARBs is contraindicated during pregnancy.
When the combination of CNIs and corticosteroids fail to achieve remission, KDIGO recommends consideration of the antimetabolite mycophenolate mofetil (MMF) or high-dose corticosteroids therapy. MMF has been shown to be effective in achieving remission in a single-center prospective study (Li et al. 2010). Another observational study that compared MMF alone or MMF following cyclosporine treatment showed no difference in steroid/cyclophosphamide-resistant NS patients (de Mello et al. 2010). Recently, a randomized trial that compared patients with FSGS receiving oral pulse dexamethasone and mycophenolate versus patients receiving cyclosporine did not find a difference in rates of proteinuria remission, although the study was underpowered to detect moderate effect differences (Gipson et al. 2011). A retrospective study has suggested a role for MMF as “maintenance” therapy following combined cyclosporine/MMF therapy (Gellermann et al. 2012). The exact role for MMF in SRNS/FSGS management remains unclear, and further research is necessary.
The cytotoxic agent, cyclophosphamide, has been used in steroid-dependent and/or frequently relapsing NS. Early case series suggested that cyclophosphamide could potentially be used for steroid-resistant NS, including FSGS (Bajpai et al. 2003; Rennert et al. 1999). While these reports appeared promising, cyclophosphamide does carry small but significant risks associated with its use, including hemorrhagic cystitis, infection, infertility, and late-onset malignancy. Analysis of a small, randomized trial of FSGS patients receiving either steroid therapy or steroid therapy plus oral cyclophosphamide demonstrated no difference in remission rates or adverse outcomes (Tarshish et al. 1996). A randomized trial comparing SRNS patients with various histologies (including a third with FSGS) demonstrated addition of tacrolimus to steroids achieved higher rate of remission than those treated with intravenous cyclophosphamide (Gulati et al. 2012). Based upon review of available data, however, KDIGO currently recommends against use of cyclophosphamide for SRNS. The combination of pulse intravenous methylprednisolone alongside oral prednisone, known as the “Tune-Mendoza protocol,” had demonstrated high efficacy in achieving remission (Mendoza and Tune 1992). In this protocol, oral alkylating agents (e.g., cyclophosphamide) were used as an adjunct. Currently, the Tune-Mendoza protocol has fallen out of favor. Rituximab, an anti-CD20 antibody, has demonstrated efficacy in management of steroid-dependent NS; however, results in SRNS have not been promising (Magnasco et al. 2012).
Recurrence of FSGS following renal transplantation poses a significant threat to the kidney allograft, necessitating prompt treatment. Management of recurrent FSGS differs from management of primary disease and has recently been reviewed (Trachtman et al. 2015b). Particularly, plasmapheresis has been highlighted as an important tool for management, with many patients experiencing lasting remission.
Conclusion
FSGS is a histological lesion that can be seen in glomerular proteinuric disease resulting from a variety of pathophysiologic mechanisms. In the past two decades, remarkable progress has been made in understanding the mechanisms leading to FSGS, such as molecular underpinnings of podocytopathies or the hemodynamic mechanical forces leading to podocyte depletion. In addition, the discovery of the APOL1 risk allele has elucidated a partial explanation for the racial disparity in disease prevalence. Nonetheless, further research is needed to better predict treatment response and prognosis in patients with FSGS. Given the correlation between FSGS and ESKD, research is underway to develop new treatments to mitigate the progression of CKD. The rarity of proteinuric glomerular diseases, such as FSGS-associated disease, necessitates the continued engagement of the pediatric nephrology community in research studies and clinical trials.
References
Abrantes MM, Cardoso LS, Lima EM, Penido Silva JM, Diniz JS, Bambirra EA, Oliveira EA (2006) Predictive factors of chronic kidney disease in primary focal segmental glomerulosclerosis. Pediatr Nephrol 21:1003–1012. https://doi.org/10.1007/s00467-006-0138-y
Adelman RD, Restaino IG, Alon US, Blowey DL (2001) Proteinuria and focal segmental glomerulosclerosis in severely obese adolescents. J Pediatr 138:481–485. https://doi.org/10.1067/mpd.2001.113006
Alexander SR et al (1990) The 1989 report of the north American Pediatric renal transplant cooperative study. Pediatr Nephrol 4:542–553
Bagga A, Mudigoudar BD, Hari P, Vasudev V (2004) Enalapril dosage in steroid-resistant nephrotic syndrome. Pediatr Nephrol 19:45–50. https://doi.org/10.1007/s00467-003-1314-y
Bajpai A, Bagga A, Hari P, Dinda A, Srivastava RN (2003) Intravenous cyclophosphamide in steroid-resistant nephrotic syndrome. Pediatr Nephrol 18:351–356. https://doi.org/10.1007/s00467-003-1095-3
Banaszak B, Banaszak P (2012) The increasing incidence of initial steroid resistance in childhood nephrotic syndrome. Pediatr Nephrol 27:927–932. https://doi.org/10.1007/s00467-011-2083-7
Barbaux S et al (1997) Donor splice-site mutations in WT1 are responsible for Frasier syndrome. Nat Genet 17:467–470. https://doi.org/10.1038/ng1297-467
Barisoni L, Schnaper HW, Kopp JB (2007) A proposed taxonomy for the podocytopathies: a reassessment of the primary nephrotic diseases. Clin J Am Soc Nephrol 2:529–542. https://doi.org/10.2215/cjn.04121206
Barker DJ, Osmond C, Forsen TJ, Kajantie E, Eriksson JG (2005) Trajectories of growth among children who have coronary events as adults. N Engl J Med 353:1802–1809. https://doi.org/10.1056/NEJMoa044160
Baum MA, Ho M, Stablein D, Alexander SR (2002) Outcome of renal transplantation in adolescents with focal segmental glomerulosclerosis. Pediatr Transplant 6:488–492
Beckerman P et al (2017) Transgenic expression of human APOL1 risk variants in podocytes induces kidney disease in mice. Nat Med 23:429–438. https://doi.org/10.1038/nm.4287
Benigni A et al (2011) Inhibiting angiotensin-converting enzyme promotes renal repair by limiting progenitor cell proliferation and restoring the glomerular architecture. Am J Pathol 179:628–638. https://doi.org/10.1016/j.ajpath.2011.04.003
Benoit G, Moriniere V, Charbit M, Niaudet P, Antignac C (2010) What is the risk that I will transmit nephrotic syndrome to my children, doctor? NDT Plus 3:402–404. https://doi.org/10.1093/ndtplus/sfq095
Bock ME, Price HE, Gallon L, Langman CB (2013) Serum soluble urokinase-type plasminogen activator receptor levels and idiopathic FSGS in children: a single-center report. Clin J Am Soc Nephrol 8:1304–1311. https://doi.org/10.2215/cjn.07680712
Bonilla-Felix M, Parra C, Dajani T, Ferris M, Swinford RD, Portman RJ, Verani R (1999) Changing patterns in the histopathology of idiopathic nephrotic syndrome in children. Kidney Int 55:1885–1890. https://doi.org/10.1046/j.1523-1755.1999.00408.x
Borges FF, Shiraichi L, da Silva MP, Nishimoto EI, Nogueira PC (2007) Is focal segmental glomerulosclerosis increasing in patients with nephrotic syndrome? Pediatr Nephrol 22:1309–1313. https://doi.org/10.1007/s00467-007-0516-0
Bouchireb K et al (2014) NPHS2 mutations in steroid-resistant nephrotic syndrome: a mutation update and the associated phenotypic spectrum. Hum Mutat 35:178–186. https://doi.org/10.1002/humu.22485
Boute N et al (2000) NPHS2, encoding the glomerular protein podocin, is mutated in autosomal recessive steroid-resistant nephrotic syndrome. Nat Genet 24:349–354. https://doi.org/10.1038/74166
Boyer O, Moulder JK, Somers MJ (2007) Focal and segmental glomerulosclerosis in children: a longitudinal assessment. Pediatr Nephrol 22:1159–1166. https://doi.org/10.1007/s00467-007-0493-3
Brown EJ et al (2010) Mutations in the formin gene INF2 cause focal segmental glomerulosclerosis. Nat Genet 42:72–76. https://doi.org/10.1038/ng.505
Bruggeman LA et al (2014) Plasma apolipoprotein L1 levels do not correlate with CKD. J Am Soc Nephrol 25:634–644. https://doi.org/10.1681/asn.2013070700
Bruggeman LA et al (2016) APOL1-G0 or APOL1-G2 transgenic models develop preeclampsia but not kidney disease. J Am Soc Nephrol 27:3600–3610. https://doi.org/10.1681/asn.2015111220
Buscher AK et al (2016) Rapid response to Cyclosporin a and Favorable renal outcome in nongenetic versus genetic steroid-resistant nephrotic syndrome. Clin J Am Soc Nephrol 11:245–253. https://doi.org/10.2215/cjn.07370715
Buscher AK et al (2010) Immunosuppression and renal outcome in congenital and pediatric steroid-resistant nephrotic syndrome. Clin J Am Soc Nephrol 5:2075–2084. https://doi.org/10.2215/cjn.01190210
Call KM et al (1990) Isolation and characterization of a zinc finger polypeptide gene at the human chromosome 11 Wilms’ tumor locus. Cell 60:509–520
Cameron JS (1968) Histology, protein clearances, and response to treatment in the nephrotic syndrome. Br Med J 4:352–356
Caridi G et al (2001) Prevalence, genetics, and clinical features of patients carrying podocin mutations in steroid-resistant nonfamilial focal segmental glomerulosclerosis. J Am Soc Nephrol 12:2742–2746
Cattran DC, Rao P (1998) Long-term outcome in children and adults with classic focal segmental glomerulosclerosis. Am J Kidney Dis 32:72–79
Choi HJ et al (2008) Familial focal segmental glomerulosclerosis associated with an ACTN4 mutation and paternal germline mosaicism. Am J Kidney Dis 51:834–838. https://doi.org/10.1053/j.ajkd.2008.01.018
Choudhry S, Bagga A, Hari P, Sharma S, Kalaivani M, Dinda A (2009) Efficacy and safety of tacrolimus versus cyclosporine in children with steroid-resistant nephrotic syndrome: a randomized controlled trial. Am J Kidney Dis 53:760–769. https://doi.org/10.1053/j.ajkd.2008.11.033
Churg J, Habib R, White RH (1970) Pathology of the nephrotic syndrome in children: a report for the international study of kidney disease in children. Lancet 760:1299–1302
Clapham DE (2003) TRP channels as cellular sensors. Nature 426:517–524. https://doi.org/10.1038/nature02196
Corwin HL, Schwartz MM, Lewis EJ (1988) The importance of sample size in the interpretation of the renal biopsy. Am J Nephrol 8:85–89
Crawford BD, Gillies CE, Robertson CC, Kretzler M, Otto E, Vega-Wagner V, Sampson MG (2017) Evaluating Mendelian nephrotic syndrome genes for evidence for risk alleles or oligogenicity that explain heritability. Pediatr Nephrol 32:467–476. https://doi.org/10.1007/s00467-016-3513-3
D’Agati V (2003) Pathologic classification of focal segmental glomerulosclerosis. Semin Nephrol 23:117–134. https://doi.org/10.1053/snep.2003.50012
D’Agati VD, Fogo AB, Bruijn JA, Jennette JC (2004) Pathologic classification of focal segmental glomerulosclerosis: a working proposal. Am J Kidney Dis 43:368–382
de Mello VR et al (2010) Mycophenolate mofetil in children with steroid/cyclophosphamide-resistant nephrotic syndrome. Pediatr Nephrol 25:453–460. https://doi.org/10.1007/s00467-009-1356-x
El-Husseini A et al (2005) Long-term effects of cyclosporine in children with idiopathic nephrotic syndrome: a single-centre experience. Nephrol Dial Transplant 20:2433–2438. https://doi.org/10.1093/ndt/gfi059
Ellis D, Buffone GJ (1981) Protein clearances and selectivity determinations in childhood nephrosis: a reappraisal. Clin Chem 27:1397–1400
Falk RJ, Scheinman J, Phillips G, Orringer E, Johnson A, Jennette JC (1992) Prevalence and pathologic features of sickle cell nephropathy and response to inhibition of angiotensin-converting enzyme. N Engl J Med 326:910–915. https://doi.org/10.1056/nejm199204023261402
Faul C et al (2008) The actin cytoskeleton of kidney podocytes is a direct target of the antiproteinuric effect of cyclosporine. A Nature medicine 14:931–938. https://doi.org/10.1038/nm.1857
Filler G, Young E, Geier P, Carpenter B, Drukker A, Feber J (2003) Is there really an increase in non-minimal change nephrotic syndrome in children? Am J Kidney Dis 42:1107–1113
Fogo A, Hawkins EP, Berry PL, Glick AD, Chiang ML, MacDonell RC Jr, Ichikawa I (1990) Glomerular hypertrophy in minimal change disease predicts subsequent progression to focal glomerular sclerosis. Kidney Int 38:115–123
Franco Palacios CR et al (2013) Urine but not serum soluble urokinase receptor (suPAR) may identify cases of recurrent FSGS in kidney transplant candidates. Transplantation 96:394–399. https://doi.org/10.1097/TP.0b013e3182977ab1
Freedman BI, Julian BA (2015) Should kidney donors be genotyped for APOL1 risk alleles? Kidney Int 87:671–673. https://doi.org/10.1038/ki.2015.16
Freedman BI et al (2015) Apolipoprotein L1 gene variants in deceased organ donors are associated with renal allograft failure. Am J Transplant 15:1615–1622. https://doi.org/10.1111/ajt.13223
Freedman BI et al (2016) APOL1 genotype and kidney transplantation outcomes from deceased African American donors. Transplantation 100:194–202. https://doi.org/10.1097/tp.0000000000000969
Fries JW, Sandstrom DJ, Meyer TW, Rennke HG (1989) Glomerular hypertrophy and epithelial cell injury modulate progressive glomerulosclerosis in the rat. Lab Investig 60:205–218
Fukuda A et al (2012) Angiotensin II-dependent persistent podocyte loss from destabilized glomeruli causes progression of end stage kidney disease. Kidney Int 81:40–55. https://doi.org/10.1038/ki.2011.306
Gadegbeku CA et al (2013) Design of the Nephrotic Syndrome Study Network (NEPTUNE) to evaluate primary glomerular nephropathy by a multidisciplinary approach. Kidney Int 83:749–756. https://doi.org/10.1038/ki.2012.428
Garin EH, Diaz LN, Mu W, Wasserfall C, Araya C, Segal M, Johnson RJ (2009) Urinary CD80 excretion increases in idiopathic minimal-change disease. J Am Soc Nephrol 20:260–266. https://doi.org/10.1681/asn.2007080836
Garin EH, Mu W, Arthur JM, Rivard CJ, Araya CE, Shimada M, Johnson RJ (2010) Urinary CD80 is elevated in minimal change disease but not in focal segmental glomerulosclerosis. Kidney Int 78:296–302. https://doi.org/10.1038/ki.2010.143
Gellermann J, Ehrich JH, Querfeld U (2012) Sequential maintenance therapy with cyclosporin a and mycophenolate mofetil for sustained remission of childhood steroid-resistant nephrotic syndrome. Nephrol Dial Transplant 27:1970–1978. https://doi.org/10.1093/ndt/gfr572
Genovese G et al (2010) Association of trypanolytic ApoL1 variants with kidney disease in African Americans. Science 329:841–845. https://doi.org/10.1126/science.1193032
Gipson DS et al (2006) Differential risk of remission and ESRD in childhood FSGS. Pediatr Nephrol 21:344–349. https://doi.org/10.1007/s00467-005-2097-0
Gipson DS et al (2011) Clinical trial of focal segmental glomerulosclerosis in children and young adults. Kidney Int 80:868–878. https://doi.org/10.1038/ki.2011.195
Grahammer F et al (2016) A flexible, multilayered protein scaffold maintains the slit in between glomerular podocytes. JCI Insight 1:e86177. https://doi.org/10.1172/jci.insight.86177
Gulati A et al (2012) Treatment with tacrolimus and prednisolone is preferable to intravenous cyclophosphamide as the initial therapy for children with steroid-resistant nephrotic syndrome. Kidney Int 82:1130–1135. https://doi.org/10.1038/ki.2012.238
Haas M, Spargo BH, Coventry S (1995) Increasing incidence of focal-segmental glomerulosclerosis among adult nephropathies: a 20-year renal biopsy study. Am J Kidney Dis 26:740–750
Haber DA et al (1990) An internal deletion within an 11p13 zinc finger gene contributes to the development of Wilms’ tumor. Cell 61:1257–1269
Hall G, Gbadegesin RA (2015) Translating genetic findings in hereditary nephrotic syndrome: the missing loops. Am J Physiol Renal Physiol 309:F24–F28. https://doi.org/10.1152/ajprenal.00683.2014
Hallman N, Hjelt L (1959) Congenital nephrotic syndrome. J Pediatr 55:152–162
Hickson LJ et al (2009) Kidney transplantation for primary focal segmental glomerulosclerosis: outcomes and response to therapy for recurrence. Transplantation 87:1232–1239. https://doi.org/10.1097/TP.0b013e31819f12be
Hida K et al (2002) Cyanotic congenital heart disease associated with glomerulomegaly and focal segmental glomerulosclerosis: remission of nephrotic syndrome with angiotensin converting enzyme inhibitor. Nephrol Dial Transplant 17:144–147
Hinkes B et al (2008) Specific podocin mutations correlate with age of onset in steroid-resistant nephrotic syndrome. J Am Soc Nephrol 19:365–371. https://doi.org/10.1681/asn.2007040452
Hodgin JB, Rasoulpour M, Markowitz GS, D’Agati VD (2009) Very low birth weight is a risk factor for secondary focal segmental glomerulosclerosis. Clin J Am Soc Nephrol 4:71–76. https://doi.org/10.2215/cjn.01700408
Hodson EM, Willis NS, Craig JC (2010) Interventions for idiopathic steroid-resistant nephrotic syndrome in children. Cochrane Database Syst Rev CD003594. https://doi.org/10.1002/14651858.CD003594.pub4
Hogg R, Middleton J, Vehaskari VM (2007) Focal segmental glomerulosclerosis – epidemiology aspects in children and adults. Pediatr Nephrol 22:183–186 doi:https://doi.org/10.1007/s00467-006-0370-5
Holthofer H et al (1999) Nephrin localizes at the podocyte filtration slit area and is characteristically spliced in the human kidney. Am J Pathol 155:1681–1687. https://doi.org/10.1016/s0002-9440(10)65483-1
Holzman LB, St John PL, Kovari IA, Verma R, Holthofer H, Abrahamson DR (1999) Nephrin localizes to the slit pore of the glomerular epithelial cell. Kidney Int 56:1481–1491. https://doi.org/10.1046/j.1523-1755.1999.00719.x
Huber TB et al (2003a) Nephrin and CD2AP associate with phosphoinositide 3-OH kinase and stimulate AKT-dependent signaling. Mol Cell Biol 23:4917–4928
Huber TB, Kottgen M, Schilling B, Walz G, Benzing T (2001) Interaction with podocin facilitates nephrin signaling. J Biol Chem 276:41543–41546. https://doi.org/10.1074/jbc.C100452200
Huber TB et al (2003b) Molecular basis of the functional podocin-nephrin complex: mutations in the NPHS2 gene disrupt nephrin targeting to lipid raft microdomains. Hum Mol Genet 12:3397–3405. https://doi.org/10.1093/hmg/ddg360
Ichikawa I, Ma J, Motojima M, Matsusaka T (2005) Podocyte damage damages podocytes: autonomous vicious cycle that drives local spread of glomerular sclerosis. Curr Opin Nephrol Hypertens 14:205–210
Ingulli E, Tejani A (1991) Racial differences in the incidence and renal outcome of idiopathic focal segmental glomerulosclerosis in children. Pediatr Nephrol 5:393–397
ISKDC (1978) Nephrotic syndrome in children: prediction of histopathology from clinical and laboratory characteristics at time of diagnosis. A report of the international study of kidney disease in children. Kidney Int 13:159–165
ISKDC (1981) The primary nephrotic syndrome in children. Identification of patients with minimal change nephrotic syndrome from initial response to prednisone. A report of the international study of kidney disease in children. J Pediatr 98:561–564
Isojima T et al (2014) LMX1B mutation with residual transcriptional activity as a cause of isolated glomerulopathy. Nephrol Dial Transplant 29:81–88. https://doi.org/10.1093/ndt/gft359
Jones N et al (2006) Nck adaptor proteins link nephrin to the actin cytoskeleton of kidney podocytes. Nature 440:818–823. https://doi.org/10.1038/nature04662
Kambham N, Markowitz GS, Valeri AM, Lin J, D’Agati VD (2001) Obesity-related glomerulopathy: an emerging epidemic. Kidney Int 59:1498–1509. https://doi.org/10.1046/j.1523-1755.2001.0590041498.x
Kaplan JM et al (2000) Mutations in ACTN4, encoding alpha-actinin-4, cause familial focal segmental glomerulosclerosis. Nat Genet 24:251–256. https://doi.org/10.1038/73456
Karle SM, Uetz B, Ronner V, Glaeser L, Hildebrandt F, Fuchshuber A (2002) Novel mutations in NPHS2 detected in both familial and sporadic steroid-resistant nephrotic syndrome. J Am Soc Nephrol 13:388–393
KDIGO (2012) Kidney disease: improving global outcomes (KDIGO) clinical practice guideline for glomerulonephritis. Kidney Int 2:142–274. https://doi.org/10.1038/kisup.2012.12
Kestila M et al (1998) Positionally cloned gene for a novel glomerular protein–nephrin–is mutated in congenital nephrotic syndrome. Mol Cell 1:575–582
Khoshnoodi J, Sigmundsson K, Ofverstedt LG, Skoglund U, Obrink B, Wartiovaara J, Tryggvason K (2003) Nephrin promotes cell-cell adhesion through homophilic interactions. Am J Pathol 163:2337–2346. https://doi.org/10.1016/s0002-9440(10)63590-0
Kitamura A, Tsukaguchi H, Hiramoto R, Shono A, Doi T, Kagami S, Iijima K (2007) A familial childhood-onset relapsing nephrotic syndrome. Kidney Int 71:946–951. https://doi.org/10.1038/sj.ki.5002110
Kitiyakara C, Eggers P, Kopp JB (2004) Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis 44:815–825
Kitiyakara C, Kopp JB, Eggers P (2003) Trends in the epidemiology of focal segmental glomerulosclerosis. Semin Nephrol 23:172–182. https://doi.org/10.1053/snep.2003.50025
Kopp JB et al (2011) APOL1 genetic variants in focal segmental glomerulosclerosis and HIV-associated nephropathy. J Am Soc Nephrol 22:2129–2137. https://doi.org/10.1681/asn.2011040388
Kopp JB et al (2015) Clinical features and histology of apolipoprotein L1-associated nephropathy in the FSGS clinical trial. J Am Soc Nephrol 26:1443–1448. https://doi.org/10.1681/asn.2013111242
Koziell A, Grech V, Hussain S, Lee G, Lenkkeri U, Tryggvason K, Scambler P (2002) Genotype/phenotype correlations of NPHS1 and NPHS2 mutations in nephrotic syndrome advocate a functional inter-relationship in glomerular filtration. Hum Mol Genet 11:379–388
Kozlitina J et al (2016) Plasma levels of risk-variant APOL1 do not associate with renal disease in a population-based cohort. J Am Soc Nephrol 27:3204. https://doi.org/10.1681/asn.2015101121
Kretzler M, Sedor JR (2015) Introduction: precision medicine for glomerular disease: the road forward. Semin Nephrol 35:209–211. https://doi.org/10.1016/j.semnephrol.2015.04.001
Kriz W, Lemley KV (2016) Mechanical challenges to the glomerular filtration barrier: adaptations and pathway to sclerosis. Pediatr Nephrol 32:405. https://doi.org/10.1007/s00467-016-3358-9
Laurin LP et al (2016) Renal survival in patients with collapsing compared with not otherwise specified FSGS. Clin J Am Soc Nephrol 11:1752. https://doi.org/10.2215/cjn.13091215
Lee BT et al (2012) The APOL1 genotype of African American kidney transplant recipients does not impact 5-year allograft survival. Am J Transplant 12:1924–1928. https://doi.org/10.1111/j.1600-6143.2012.04033.x
Lee HK et al (2011) Variable renal phenotype in a family with an INF2 mutation. Pediatr Nephrol 26:73–76. https://doi.org/10.1007/s00467-010-1644-5
Lemley KV (2009) Kidney disease in nail-patella syndrome. Pediatr Nephrol 24:2345–2354. https://doi.org/10.1007/s00467-008-0836-8
Lemley KV (2012) Protecting podocytes: how good do we need to be? Kidney Int 81:9–11. https://doi.org/10.1038/ki.2011.329
Lemley KV (2016) Glomerular pathology and the progression of chronic kidney disease. Am J Physiol Renal Physiol 310:F1385–F1388. https://doi.org/10.1152/ajprenal.00099.2016
Lemley KV, Bagnasco SM, Nast CC, Barisoni L, Conway CM, Hewitt SM, Song PX (2016) Morphometry predicts early GFR change in primary Proteinuric Glomerulopathies: a longitudinal cohort study using generalized estimating equations. PLoS One 11:e0157148. https://doi.org/10.1371/journal.pone.0157148
Li Z, Duan C, He J, Wu T, Xun M, Zhang Y, Yin Y (2010) Mycophenolate mofetil therapy for children with steroid-resistant nephrotic syndrome. Pediatr Nephrol 25:883–888. https://doi.org/10.1007/s00467-009-1375-7
Lieberman KV, Tejani A (1996) A randomized double-blind placebo-controlled trial of cyclosporine in steroid-resistant idiopathic focal segmental glomerulosclerosis in children. J Am Soc Nephrol 7:56–63
Lines DR (1969) Selectivity of proteinuria in childhood nephrotic syndrome. Arch Dis Child 44:461–464
Machuca E et al (2009) Clinical and epidemiological assessment of steroid-resistant nephrotic syndrome associated with the NPHS2 R229Q variant. Kidney Int 75:727–735. https://doi.org/10.1038/ki.2008.650
Magnasco A et al (2012) Rituximab in children with resistant idiopathic nephrotic syndrome. J Am Soc Nephrol 23:1117–1124. https://doi.org/10.1681/asn.2011080775
Mahesh S, Del Rio M, Feuerstein D, Greenstein S, Schechner R, Tellis V, Kaskel F (2008) Demographics and response to therapeutic plasma exchange in pediatric renal transplantation for focal glomerulosclerosis: a single center experience. Pediatr Transplant 12:682–688. https://doi.org/10.1111/j.1399-3046.2007.00880.x
Manalich R, Reyes L, Herrera M, Melendi C, Fundora I (2000) Relationship between weight at birth and the number and size of renal glomeruli in humans: a histomorphometric study. Kidney Int 58:770–773. https://doi.org/10.1046/j.1523-1755.2000.00225.x
Martinelli R, Okumura AS, Pereira LJ, Rocha H (2001) Primary focal segmental glomerulosclerosis in children: prognostic factors. Pediatr Nephrol 16:658–661
McCarthy ET, Sharma M, Savin VJ (2010) Circulating permeability factors in idiopathic nephrotic syndrome and focal segmental glomerulosclerosis. Clin J Am Soc Nephrol 5:2115–2121. https://doi.org/10.2215/cjn.03800609
Mekahli D et al (2009) Long-term outcome of idiopathic steroid-resistant nephrotic syndrome: a multicenter study. Pediatr Nephrol 24:1525–1532. https://doi.org/10.1007/s00467-009-1138-5
Mendoza SA, Tune BM (1992) Treatment of childhood nephrotic syndrome. J Am Soc Nephrol 3:889–894
Mundel P, Greka A (2015) Developing therapeutic ‘arrows’ with the precision of William tell: the time has come for targeted therapies in kidney disease. Curr Opin Nephrol Hypertens 24:1–392. https://doi.org/10.1097/mnh.0000000000000137
Nagata M, Scharer K, Kriz W (1992) Glomerular damage after uninephrectomy in young rats. I. Hypertrophy and distortion of capillary architecture. Kidney Int 42:136–147
Ng DK et al (2016) APOL1-associated glomerular disease among African-American children: a collaboration of the chronic kidney disease in children (CKiD) and nephrotic syndrome study network (NEPTUNE) cohorts. Nephrol Dial Transplant. https://doi.org/10.1093/ndt/gfw061
Olabisi OA et al (2016) APOL1 kidney disease risk variants cause cytotoxicity by depleting cellular potassium and inducing stress-activated protein kinases. Proc Natl Acad Sci U S A 113:830–837. https://doi.org/10.1073/pnas.1522913113
Paik KH et al (2007) Primary focal segmental glomerular sclerosis in children: clinical course and prognosis. Pediatr Nephrol 22:389–395. https://doi.org/10.1007/s00467-006-0301-5
Patrakka J et al (2000) Congenital nephrotic syndrome (NPHS1): features resulting from different mutations in Finnish patients. Kidney Int 58:972–980. https://doi.org/10.1046/j.1523-1755.2000.00254.x
Pelletier J et al (1991) Germline mutations in the Wilms’ tumor suppressor gene are associated with abnormal urogenital development in Denys-Drash syndrome. Cell 67:437–447
Philippe A et al (2008) Nephrin mutations can cause childhood-onset steroid-resistant nephrotic syndrome. J Am Soc Nephrol 19:1871–1878. https://doi.org/10.1681/asn.2008010059
Ponticelli C et al (1993) A randomized trial of cyclosporine in steroid-resistant idiopathic nephrotic syndrome. Kidney Int 43:1377–1384
Reeves-Daniel AM et al (2011) The APOL1 gene and allograft survival after kidney transplantation. Am J Transplant 11:1025–1030. https://doi.org/10.1111/j.1600-6143.2011.03513.x
Reiser J et al (2005) TRPC6 is a glomerular slit diaphragm-associated channel required for normal renal function. Nat Genet 37:739–744. https://doi.org/10.1038/ng1592
Reiser J et al (2004) Induction of B7-1 in podocytes is associated with nephrotic syndrome. J Clin Invest 113:1390–1397. https://doi.org/10.1172/jci20402
Remuzzi A, Mazerska M, Gephardt GN, Novick AC, Brenner BM, Remuzzi G (1995) Three-dimensional analysis of glomerular morphology in patients with subtotal nephrectomy. Kidney Int 48:155–162
Remuzzi A, Pergolizzi R, Mauer MS, Bertani T (1990) Three-dimensional morphometric analysis of segmental glomerulosclerosis in the rat. Kidney Int 38:851–856
Remuzzi G, Benigni A, Remuzzi A (2006) Mechanisms of progression and regression of renal lesions of chronic nephropathies and diabetes. J Clin Invest 116:288–296. https://doi.org/10.1172/jci27699
Rennert WP, Kala UK, Jacobs D, Goetsch S, Verhaart S (1999) Pulse cyclophosphamide for steroid-resistant focal segmental glomerulosclerosis. Pediatr Nephrol 13:113–116. https://doi.org/10.1007/s004670050574
Rich AR (1957) A hitherto undescribed vulnerability of the juxtamedullary glomeruli in lipoid nephrosis. Bull Johns Hopkins Hosp 100:173–186
Roselli S et al (2002) Podocin localizes in the kidney to the slit diaphragm area. Am J Pathol 160:131–139. https://doi.org/10.1016/s0002-9440(10)64357-x
Ross LF, Thistlethwaite JR Jr (2016) Introducing genetic tests with uncertain implications in living donor kidney transplantation: ApoL1 as a case study. Prog Transplant 26:203–206. https://doi.org/10.1177/1526924816654608
Ruf RG et al (2004) Patients with mutations in NPHS2 (podocin) do not respond to standard steroid treatment of nephrotic syndrome. J Am Soc Nephrol 15:722–732
Ruotsalainen V et al (1999) Nephrin is specifically located at the slit diaphragm of glomerular podocytes. Proc Natl Acad Sci U S A 96:7962–7967
Sadowski CE et al (2015) A single-gene cause in 29.5% of cases of steroid-resistant nephrotic syndrome. J Am Soc Nephrol 26:1279–1289. https://doi.org/10.1681/asn.2014050489
Sampson MG et al (2016a) Using population genetics to interrogate the monogenic nephrotic syndrome diagnosis in a case cohort. J Am Soc Nephrol 27:1970–1983. https://doi.org/10.1681/asn.2015050504
Sampson MG et al (2016b) Integrative genomics identifies novel associations with APOL1 risk genotypes in black NEPTUNE subjects. J Am Soc Nephrol 27:814–823. https://doi.org/10.1681/asn.2014111131
Samuel T, Hoy WE, Douglas-Denton R, Hughson MD, Bertram JF (2005) Determinants of glomerular volume in different cortical zones of the human kidney. J Am Soc Nephrol 16:3102–3109. https://doi.org/10.1681/asn.2005010123
Santin S et al (2009a) TRPC6 mutational analysis in a large cohort of patients with focal segmental glomerulosclerosis. Nephrol Dial Transplant 24:3089–3096. https://doi.org/10.1093/ndt/gfp229
Santin S et al (2009b) Nephrin mutations cause childhood- and adult-onset focal segmental glomerulosclerosis. Kidney Int 76:1268–1276. https://doi.org/10.1038/ki.2009.381
Santin S et al (2011) Clinical value of NPHS2 analysis in early- and adult-onset steroid-resistant nephrotic syndrome. Clin J Am Soc Nephrol 6:344–354. https://doi.org/10.2215/cjn.03770410
Savin VJ, McCarthy ET, Sharma R, Charba D, Sharma M (2008) Galactose binds to focal segmental glomerulosclerosis permeability factor and inhibits its activity. Transl Res 151:288–292. https://doi.org/10.1016/j.trsl.2008.04.001
Schultheiss M, Ruf RG, Mucha BE, Wiggins R, Fuchshuber A, Lichtenberger A, Hildebrandt F (2004) No evidence for genotype/phenotype correlation in NPHS1 and NPHS2 mutations. Pediatr Nephrol 19:1340–1348. https://doi.org/10.1007/s00467-004-1629-3
Schwarz K et al (2001) Podocin, a raft-associated component of the glomerular slit diaphragm, interacts with CD2AP and nephrin. J Clin Invest 108:1621–1629. https://doi.org/10.1172/jci12849
Sethna CB, Gipson DS (2014) Treatment of FSGS in children. Adv Chronic Kidney Dis 21:194–199. https://doi.org/10.1053/j.ackd.2014.01.010
Sgambat K, Banks M, Moudgil A (2013) Effect of galactose on glomerular permeability and proteinuria in steroid-resistant nephrotic syndrome. Pediatr Nephrol 28:2131–2135. https://doi.org/10.1007/s00467-013-2539-z
Sharma M, Sharma R, McCarthy ET, Savin VJ (2004) The focal segmental glomerulosclerosis permeability factor: biochemical characteristics and biological effects. Exp Biol Med (Maywood) 229:85–98
Simon P, Ramee MP, Autuly V, Laruelle E, Charasse C, Cam G, Ang KS (1994) Epidemiology of primary glomerular diseases in a French region. Variations according to period and age. Kidney Int 46:1192–1198
Smith JM, Martz K, Blydt-Hansen TD (2013) Pediatric kidney transplant practice patterns and outcome benchmarks, 1987–2010: a report of the north American Pediatric renal trials and collaborative studies. Pediatr Transplant 17:149–157. https://doi.org/10.1111/petr.12034
Sorof JM, Hawkins EP, Brewer ED, Boydstun KAS II, Powell DR (1998) Age and ethnicity affect the risk and outcome of focal segmental glomerulosclerosis. Pediatr Nephrol 12:764–768
Spinale JM et al (2015) A reassessment of soluble urokinase-type plasminogen activator receptor in glomerular disease. Kidney Int 87:564–574. https://doi.org/10.1038/ki.2014.346
SPNSG (1985) Focal segmental glomerulosclerosis in children with idiopathic nephrotic syndrome. A report of the southwest Pediatric nephrology study group. Kidney Int 27:442–449
Srivastava T, Simon SD, Alon US (1999) High incidence of focal segmental glomerulosclerosis in nephrotic syndrome of childhood. Pediatr Nephrol 13:13–18. https://doi.org/10.1007/s004670050555
Tarshish P, Tobin JN, Bernstein J, Edelmann CM Jr (1996) Cyclophosphamide does not benefit patients with focal segmental glomerulosclerosis. A report of the international study of kidney disease in children. Pediatr Nephrol 10:590–593
Tejani A (1985) Morphological transition in minimal change nephrotic syndrome. Nephron 39:157–159
Tejani A, Phadke K, Adamson O, Nicastri A, Chen CK, Sen D (1985) Renal lesions in sickle cell nephropathy in children. Nephron 39:352–355
Tory K et al (2014) Mutation-dependent recessive inheritance of NPHS2-associated steroid-resistant nephrotic syndrome. Nat Genet 46:299–304. https://doi.org/10.1038/ng.2898
Trachtman H et al (2015b) Efficacy of galactose and adalimumab in patients with resistant focal segmental glomerulosclerosis: report of the font clinical trial group. BMC Nephrol 16:111. https://doi.org/10.1186/s12882-015-0094-5
Trachtman R, Sran SS, Trachtman H (2015a) Recurrent focal segmental glomerulosclerosis after kidney transplantation. Pediatr Nephrol 30:1793–1802. https://doi.org/10.1007/s00467-015-3062-1
Trautmann A et al (2015) Spectrum of steroid-resistant and congenital nephrotic syndrome in children: the PodoNet registry cohort. Clin J Am Soc Nephrol 10:592–600. https://doi.org/10.2215/cjn.06260614
Trautmann A et al (2017) Long-term outcome of steroid-resistant nephrotic syndrome in children. J Am Soc Nephrol. https://doi.org/10.1681/asn.2016101121
Troyanov S, Wall CA, Miller JA, Scholey JW, Cattran DC (2005) Focal and segmental glomerulosclerosis: definition and relevance of a partial remission. J Am Soc Nephrol 16:1061–1068. https://doi.org/10.1681/asn.2004070593
Tsukaguchi H et al (2002) NPHS2 mutations in late-onset focal segmental glomerulosclerosis: R229Q is a common disease-associated allele. J Clin Invest 110:1659–1666. https://doi.org/10.1172/jci16242
Tzur S et al (2010) Missense mutations in the APOL1 gene are highly associated with end stage kidney disease risk previously attributed to the MYH9 gene. Hum Genet 128:345–350. https://doi.org/10.1007/s00439-010-0861-0
Vogelmann SU, Nelson WJ, Myers BD, Lemley KV (2003) Urinary excretion of viable podocytes in health and renal disease. Am J Physiol Renal Physiol 285:F40–F48. https://doi.org/10.1152/ajprenal.00404.2002
Wartiovaara J et al (2004) Nephrin strands contribute to a porous slit diaphragm scaffold as revealed by electron tomography. J Clin Invest 114:1475–1483. https://doi.org/10.1172/jci22562
Weber S et al (2016) Dealing with the incidental finding of secondary variants by the example of SRNS patients undergoing targeted next-generation sequencing. Pediatr Nephrol 31:73–81. https://doi.org/10.1007/s00467-015-3167-6
Weber S et al (2004) NPHS2 mutation analysis shows genetic heterogeneity of steroid-resistant nephrotic syndrome and low post-transplant recurrence. Kidney Int 66:571–579. https://doi.org/10.1111/j.1523-1755.2004.00776.x
Wei C et al (2011) Circulating urokinase receptor as a cause of focal segmental glomerulosclerosis. Nat Med 17:952–960. https://doi.org/10.1038/nm.2411
Wei C et al (2008) Modification of kidney barrier function by the urokinase receptor. Nat Med 14:55–63. https://doi.org/10.1038/nm1696
Wei C et al (2012) Circulating suPAR in two cohorts of primary FSGS. J Am Soc Nephrol 23:2051–2059. https://doi.org/10.1681/asn.2012030302
Weins A et al (2005) Mutational and biological analysis of alpha-actinin-4 in focal segmental glomerulosclerosis. J Am Soc Nephrol 16:3694–3701. https://doi.org/10.1681/asn.2005070706
Weins A, Schlondorff JS, Nakamura F, Denker BM, Hartwig JH, Stossel TP, Pollak MR (2007) Disease-associated mutant alpha-actinin-4 reveals a mechanism for regulating its F-actin-binding affinity. Proc Natl Acad Sci U S A 104:16080–16085. https://doi.org/10.1073/pnas.0702451104
Winn MP et al (2005) A mutation in the TRPC6 cation channel causes familial focal segmental glomerulosclerosis. Science 308:1801–1804. https://doi.org/10.1126/science.1106215
Wong W, Morris MC, Kara T (2013) Congenital nephrotic syndrome with prolonged renal survival without renal replacement therapy. Pediatr Nephrol 28:2313–2321. https://doi.org/10.1007/s00467-013-2584-7
Yi Z, Li Z, Wu XC, He QN, Dang XQ, He XJ (2006) Effect of fosinopril in children with steroid-resistant idiopathic nephrotic syndrome. Pediatr Nephrol 21:967–972. https://doi.org/10.1007/s00467-006-0096-4
Yu CC et al (2013) Abatacept in B7-1-positive proteinuric kidney disease. N Engl J Med 369:2416–2423. https://doi.org/10.1056/NEJMoa1304572
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this entry

Cite this entry
Crawford, B.D., Sampson, M.G., Hodgin, J.B., Lemley, K.V. (2019). Focal Segmental Glomerulosclerosis, Pediatric. In: Trachtman, H., Herlitz, L., Lerma, E., Hogan, J. (eds) Glomerulonephritis. Springer, Cham. https://doi.org/10.1007/978-3-319-49379-4_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-49379-4_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-49378-7
Online ISBN: 978-3-319-49379-4
eBook Packages: MedicineReference Module Medicine