
Abstract
Background
Models of cognitive reserve in aging suggest that individual’s life experience (education, working activity, and leisure) can exert a neuroprotective effect against cognitive decline and may represent an important contribution to successful aging.
Aim
The objective of the present study is to investigate the role of cognitive reserve, pre-morbid intelligence, age, and education level, in predicting cognitive efficiency in a sample of healthy aged individuals and with probable mild cognitive impairment.
Methods
Two hundred and eight aging participants recruited from the provincial region of Bari (Apulia, Italy) took part in the study. A battery of standardized tests was administered to them to measure cognitive reserve, pre-morbid intelligence, and cognitive efficiency. Protocols for 10 participants were excluded since they did not meet inclusion criteria, and statistical analyses were conducted on data from the remaining 198 participants. A path analysis was used to test the following model: age, education level, and intelligence directly influence cognitive reserve and cognitive efficiency; cognitive reserve mediates the influence of age, education level, and intelligence on cognitive efficiency.
Results
Cognitive reserve fully mediates the relationship between pre-morbid intelligence and education level and cognitive efficiency, while age maintains a direct effect on cognitive efficiency.
Discussion
Cognitive reserve appears to exert a protective effect regarding cognitive decline in normal and pathological populations, thus masking, at least in the early phases of neurodegeneration, the decline of memory, orientation, attention, language, and reasoning skills.
Conclusions
The assessment of cognitive reserve may represent a useful evaluation supplement in neuropsychological screening protocols of cognitive decline.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In recent years, we have witnessed a steady increase in the number of diagnoses related to neurodegenerative diseases, especially dementia. These diagnoses come with increasing costs for public health and social assistance systems struggling to develop effective responses and solutions for the chronic and debilitating pathologies that can accompany aging [1, 2].
Biomedical and psychosocial research increasingly concentrates on the prodromal and early phases of neurodegenerative diseases as well as risk and prevention factors, seeking to identify variables that make the largest impact on cognitive decline. An aging individual with cognitive deficits that do not yet impact daily-life functioning meets the criteria for mild cognitive impairment (MCI) [3], together with an increased risk of developing Alzheimer’s disease. Brain changes with advancing age, such as diminution of cerebral weight and volume, formation of amyloid plaques, and changes in protein synthesis, are the organic substrates of cognitive deterioration and can have a significant negative impact on daily life.
Recent debates in the literature aim to establish which cognitive function is first implicated in cognitive decline, in order to define a model of MCI specific to each type of dementia [4]. It is noteworthy, however, that individuals with cognitive decline may present with widely varying types of cognitive dysfunction and differ considerably in terms of the severity of their symptoms. This is in accordance with the hypothesis of cognitive reserve (CR) [5], which posits that certain brain functions can mitigate the effects of neurodegeneration and reduce vulnerability to neural damage [6, 7]. According to this model, individuals differ in terms of innate variables such as intelligence, and diverse experiences due to lifestyle, cultural and educational background, work-related activities, and personal habits [8]. The strong assumption underlying the model of CR is that flexible and high-performing neural circuitry should be less vulnerable to degeneration processes. The CR model also posits that individuals can develop neural resources which reduce the risk of a cognitive decline to come and can thus sustain a greater degree of neural damage before crossing the threshold of clinically recognized cognitive impairment. This threshold can therefore be understood as representing an interaction between the level of organic damage sustained and the capacity of an individual to dynamically compensate for such damage, by using pre-existent neural circuitry or recruiting alternative networks that maintain the stability of their cognitive skills across time [9].
Numerous studies have identified three main sources of CR, which correspond to the three main aspects of an individual’s life experience: (a) education level [10–12], (b) work-related activities [13, 14], and (c) leisure time [15–17]. It is these factors that contribute to the development of neurological reserve, which protects the brain from neuropathology and plays an important role in promoting successful aging. In the Italian context, the CRI-q [18, 19], an instrument that measures cognitive reserve by probing an individual’s experience in these three areas, was recently developed.
Another factor that appears to be involved in building CR is intelligence, innate and pre-morbid [20]. Intelligence quotient (IQ) is usually measured using standardized tests that provide detailed information on an individual’s intellectual performance in a specific cognitive domain, with respect to a normative sample. In contrast, measures of pre-morbid intelligence aim to quantify the extent to which a neurological damage has impacted the intellectual capacity of patients. Pre-morbid intelligence is usually measured using a performance test that provides an estimate of pre-morbid IQ [21]. One of the most widely used tests of this type for English native speakers is the National Adult Reading Test (NART) [22], which assesses pronunciation of irregular, low-frequency words. These words are likely to be pronounced incorrectly using common phonetic interpretation rules if an individual does not already possess this linguistic knowledge. The theoretical assumption is that reading ability is retained across time despite deterioration in other cognitive domains. Since reading ability is highly correlated with general intelligence, it can be used to estimate the IQ that preceded neural damage or deterioration. Colombo and colleagues [23] have proposed a similar test for Italian native speakers, the Test di Intelligenza Breve (TIB, i.e., Brief Intelligence Test).
Some studies use pre-morbid IQ as a component in the estimation of CR [14]. However, Nucci and colleagues [18] discourage the use of IQ as an index of CR, arguing that the latter should be (a) considered an autonomous construct referring to the accumulation or storehouse of potential resources, (b) evaluated in a manner which does not depend on tests that measure performance, (c) suitable for the very elderly or to persons with diagnoses that are not specifically neurodegenerative (e.g., those who present with psychiatric syndromes or physical disabilities), and (d) measured by a test readily administrable to family members or caregivers.
The general objective of the present study was to investigate the causal role of CR, pre-morbid intelligence, age, and education level in predicting the cognitive efficiency in a sample of healthy aged and with probable mild cognitive impairment people. A further objective was to evaluate the construct of CR as a possible mediator for the effects of other predictors, namely pre-morbid intelligence, age, and education level, on cognitive efficiency.
Materials and methods
Participants
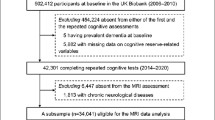
Two hundred and eight participants, Apulia residents largely recruited from the metropolitan area of Bari, took part in the study on a voluntary basis from March to May 2015. Inclusion criteria were: (a) absence of any diagnosis of dementia or overt signs of other neurodegenerative diseases, (b) absence of psychiatric diseases that might affect cognitive functioning, (c) absence of neurological or chronic systemic disorders not pharmacologically compensated that might affect cognitive functioning, (d) no history of stroke, brain lesion, or cranial trauma, and (e) autonomy in daily life. Ten participants were excluded for the following reasons: Four participants received a score equal to above one on the Clinical Dementia Rating (CDR) scale, presumably indicating cognitive deterioration of a light/moderate to severe nature, three participants obtained a score below cutoff for autonomous functioning in daily life, one participant had been diagnosed as bipolar, and two participants suffered from epilepsy. The final sample whose data were included in statistical analyses was composed of 198 participants.
Procedure
All participants recruited for the study were given the following battery of tests:
-
Mini-mental state examination—MMSE [24];
-
Montreal Cognitive Assessment—MoCA [25]: The MoCA is a measure with a similar scope as the MMSE, which also allows for a rapid screening of global cognitive functioning;
-
Test di Intelligenza Breve (i.e., Brief Intelligence Test)—TIB [23]: The TIB is a measure that serves as an estimate of IQ preceding a traumatic or morbid event, using an algorithm based on the theory of neural networks. The TIB consists of 54 words including 34 “test words,” some with irregular (proparoxytone) and others with regular (even) stress, and 20 high-frequency words not considered in the performance score. The test consists in reading the words aloud. These words are divided into “easy” and “difficult” categories, based on the difficulty of pronouncing them correctly. On the basis of the number of errors computed, the age of the subject, her/his education level, and gender, it is possible to quantify the individual’s pre-existing cognitive level, providing three distinct scores (i.e., verbal, performance, and total score);
Cognitive Reserve Index Questionnaire—CRI-q [18]: The CRI-q is a measure based on the principal indices of CR reported in the literature. The questionnaire collects information related to the three sources constituting CR, which are thought to have both independent and additive effects: education, working activity, and leisure time. The three resulting scores (CRI Education—CRI WorkingA.—CRI Leisure T.) are combined in a single score called the “Cognitive Reserve Index” (CRI). The final score for the CRI-q questionnaire and its three sub-indices are computed on a scale with a mean of 100 and a standard deviation of 15;
-
Clinical Dementia Rating—CDR [26];
-
Activities of Daily Living—ADL [27];
-
Instrumental Activities of Daily Living—IADL [28];
-
Structured Interview: A brief structured interview with an associated checklist was constructed ad hoc, in order to probe and exclude the following pathologies with possible detrimental impact on cognition: known neurodegenerative diseases other than dementia, psychiatric syndromes, neurological and chronic systemic disorders not compensated by pharmacological treatment, strokes, brain lesions, and cranial traumas.
Each testing administration was jointly accomplished by two research assistants expert in neuropsychology and lasted about 90 min, with breaks provided as requested by participants. Testing took place in the homes of the participants, was administered in spacious and well-lit rooms, and did not conflict with the regular schedules of the participants. All participants signed a consent form declaring their voluntary participation in the research.
Statistical analyses
The data were analyzed using R software. Path analysis was employed to analyze data. It is a technique used to describe relations between variables and constitutes a special case of structural equation modeling [29, 30], in which only a single indicator is used to specify for each variable in the causal model. It may be viewed as a structural model that lacks measurement model (i.e., the hypothesized relation between observed and latent variables). Path analysis is an appropriate technique of investigation if the hypotheses proposed by the researcher are consistent with already established hypotheses and well-attested results reported in the relevant literature, indicating that the hypothesized relations between variables are corroborated by empirical findings. In the present study, we tested the following model: age, education level and intelligence directly influence CR and cognitive efficiency; CR mediates the influence of age, education level, and intelligence on cognitive efficiency. Furthermore, age, education level, and intelligence are significantly correlated with each other, as are the two measures of cognitive efficiency.
Results
Table 1 shows the means, standard deviations, and correlation coefficients for the variables employed in this study. As already specified in the Methods section, CDR was measured in order to exclude individuals with light/moderate to severe cognitive deterioration (CDR ≥ 1). It was also used to distinguish between healthy participants with no evidence of cognitive impairment (CDR = 0) and those with probable mild cognitive impairment (CDR = 0.5). It was preferable to use this measure as the criterion for classification since the MMSE and MoCA scores were used in the statistical model as outcome variables. Furthermore, with respect to MoCA, there is an ongoing debate concerning which score might be considered the best cutoff in determining a diagnosis of mild cognitive impairment for the Italian population [31–33]. Out of 198 participants (111 female), 164 were shown to be cognitively healthy (83 females), and 34 showed a probable mild cognitive impairment (28 females).
All correlations between predictors, and between the predictors and the two measures of cognitive efficiency, were significant with p < 0.001. The effect sizes varied between 0.29 (correlation between age and CR) and 0.71 (correlation between pre-morbid intelligence and CR). No correlation coefficient between age, education level, and pre-morbid intelligence was higher than 0.75, suggesting that there were no issues of multicollinearity among the predictors. Consequently, all the variables were included in the path analysis.
Table 2 shows the standardized estimates for the effects of each predictor on each outcome variable, with the related standard errors, Z scores, and p values. R-squared values for each outcome variable are also shown. The predictors explain 35 % of the variance in MMSE scores, 36 % of the variance in the MoCA scores, and 64 % of the variance in CR scores. Figure 1 illustrates significant effects in the path analysis model; non-significant effects have been removed but are reported in Table 2. With respect to the effects of the predictors on the measures of cognitive efficiency, significant results were found for the effect of age on the MMSE (β = −0.23, p < 0.001) and on the MoCA (β = −0.16, p < 0.001), and for the effect of CR on the MMSE (β = 0.48, p < 0.001) and on the MoCA (β = 0.52, p < 0.001). As for the effects of the predictors on CR, significant results were obtained for the coefficients of pre-morbid intelligence (β = 0.48, p < 0.001) and education level (β = 0.42, p < 0.001). Also significant (p < 0.001) was the covariance between age, education level, and pre-morbid intelligence (age and education level Cov = −0.34; age and pre-morbid intelligence Cov = −0.30; and pre-morbid intelligence and education level Cov = 0.54), and the covariance between the MMSE and MoCA (Cov = 0.65).

Graphical representation of the model tested. The solid lines represent statistically significant coefficients: the solid-dotted lines indicate the variance explained by the outcome and mediation variables
Table 3 shows the direct, indirect, and total effects of the predictors on the MoCA and on the MMSE. There were no direct effects of pre-morbid intelligence and education level on cognitive efficiency. On the other hand, these same variables demonstrated rather important indirect effects on cognitive efficiency (pre-morbid intelligence on the MoCA β = 0.25, p < 0.001; pre-morbid intelligence on the MMSE β = 0.23, p < 0.001; education level on the MoCA β = 0.22, p < 0.001; and education level on the MMSE β = 0.20, p < 0.001). These relationships were completely mediated by CR, which absorbed most of the variance due to these two predictors. By contrast, no significant indirect effects were observed for age.
Discussion
The main result of the present study, obtained through a path analysis model, was that cognitive efficiency was significantly predicted by age and by CR, which was, in turn, robustly correlated with pre-morbid intelligence and education level. There was an inverse relation between age and cognitive efficiency: The greater the age of participants, the lower their cognitive efficiency. CR wholly mediated the relation between pre-morbid intelligence and education level, on the one hand, and MMSE and MoCA scores, on the other hand. This was a direct relationship: Greater pre-morbid IQ and education levels lead to a larger accumulation of resources that older adults can use to cope with cognitive decline, which in turn leads to better cognitive efficiency. The ties between intelligence, which can be considered an innate individual factor, and education level, which can be considered as a complex product of innate factors such as intelligence and environmental factors, with CR are aligned with theoretical models which understand reserve in the sense of an “accumulation” or “storehouse” of experiences taken from various aspects of life [18, 19, 34]. This storehouse, which an individual begins to build from a young age when neuronal growth and neural plasticity are maximal, and which carries forward through the entire life span, contributes to sustaining cognitive capacity even in later stages when neuronal circuits begin to deteriorate. CR can thus be seen as a protective factor against normal and pathological cognitive decline which might mitigate, at least in the early stages of neural degeneration, deficits in memory, orientation, attention, language, and reasoning [4, 35–41].
It is noticeable that CR has been nearly always represented by means of indicators such as education level, socio-economic status (i.e., SES), occupational attainment, and measures of intelligence (in most cases a measure of pre-morbid intelligence). In some cases, a composite score derived from a linear combination of these factors has been employed [42]. Nonetheless, in more recent theoretical advancements [43], CR has been conceptualized as a hypothetical construct that may be better represented by a multiple indicator model, including also other components such as lifestyle factors, engagement in cognitively stimulating behaviors, and social activities [44, 45]. This way of thinking at CR suggests that: a) There are multiple sources which contribute to CR, and b) CR may be viewed not as a fixed entity, but rather as a changing phenomenon across the life span, which can gain or lose its protective potential depending on exposures and behaviors acted throughout an individual’s entire life span. Thus, CR can be considered as a measure per se rather than being represented singly by education level, work attainment, or pre-morbid intelligence. Furthermore, the latter are not supposed to progress or to change significantly from a certain stage of life, while other life experiences (i.e., lifestyle factors, cognitively stimulating behaviors, and social activities) can occur in every stage of life, even in those where individuals are not supposed to raise their education level or to improve their IQ anymore [7].
The assessment of CR in elderly people could provide a useful supplementary measure to integrate with existing protocols in the neuropsychological assessment of cognitive decline, which is usually conducted using performance-based tests. Regarding the diagnostic process of cognitive decline due to neurodegenerative processes, obtaining information about CR may be critical, since individuals showing different degrees of CR will demonstrate disease-related clinical symptoms at different times. In this case, it would be useful for the clinician to predispose more challenging and more pathology-specific diagnostic tests for people with high degrees of CR [7]. Moreover, including measures which account for an individual’s life experiences could help in formulating a clinical assessment of the likely progress of neurodegenerative processes and could provide indications for recommending possible interventions based on restorative or compensatory strategies in elderly people with a diagnosis of mild cognitive impairment [46–48].
This work took an exploratory approach in examining possible theoretical models relating CR and pre-morbid intelligence to cognitive efficiency as one of the life outcome in elderly [49]. The most important suggestion of the present study was that the influence of pre-morbid intelligence on cognitive efficiency seemed to be mediated by the educational, professional, and social/leisure experiences across the life span. In other terms, the intelligence measured throughout special tests—as NART [11, 14] or TIB [18, 19]—seemed predictive of personal choices/opportunities and, in turns, of cognitive efficiency.
In conclusion, although intelligence, sketchily detected in the present study according to a pre-morbid IQ measure, undoubtedly gives a paramount contribution to individuals’ choices and experiences along the life span, the variability of life trajectories cannot be caught only by the contribution of this factor. Crucially, the effect of pre-morbid intelligence on cognitive efficiency seems to be mediated by a composite measure of experiences occurring during life span, rather than having a direct impact. If the latter suggestion will be confirmed by future research, improving life span experiences, also involving people in leisure activities and in life-long learning programs, should mitigate the effects of lower pre-morbid IQ and education level on cognitive efficiency.
Given these encouraging results, future implementations of the model presented here could include several precautions and improvements in terms of theoretical and methodological aspects. First, it would be helpful to increase the sample size, making possible a more complex model that could include new variables and allow for a structural equation model instead of a path analysis [30]. The larger the sample size, the greater the reliability of the correlation estimates which inform the model. Second, including a short battery of standardized psychological instruments alongside the CDR could improve overall diagnostic success in identifying individuals with mild cognitive impairment, with a view to including, with a reasonable degree of diagnostic certainty, only cognitively healthy individuals or in the earliest stages of cognitive deterioration [50].
References
Ferri CP, Prince M, Brayne C et al (2005) Global prevalence of dementia: a Delphi consensus study. Lancet 366:2112–2117
Carnazzo G, Santangelo A, Maugeri D et al (2011) Elderly boom. Future health care crisis: analysis and proposals. G Gerontol 59:63–70
Petersen RC, Smith GE, Waring SC et al (1999) Mild cognitive impairment: clinical characterization and outcome. Arch Neurol 56:303–308
Petersen RC, Morris JC (2005) Mild cognitive impairment as a clinical entity and treatment target. Arch Neurol 62:1160–1163
Stern Y (2002) What is cognitive reserve? Theory and research application of the reserve concept. J Int Neuropsychol Soc 8:448–460
Stern Y (2009) Cognitive reserve. Neuropsychologia 47:2015–2028
Stern Y (2012) Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol 11(1006):1012
Richards M, Deary IJ (2005) A life course approach to cognitive reserve: a model for cognitive aging and development? Ann Neurol 58:617–622
Chicherio C, Ludwig C, Borella E (2012) La capacità di riserva cognitiva e cerebrale nell’invecchiamento cognitivo. Giornale Italiano di Psicologia 39:315–339
Katzman R (1993) Education and the prevalence of dementia and Alzheimer’s disease. Neurology 43:13–20
Garrett DD, Grady CL, Hasher L (2010) Everyday memory compensation: the impact of cognitive reserve, subjective memory, and stress. Psychol Aging 25:74–83
Schmand B, Smith JH, Geerlings MI et al (1997) The effects of intelligence and education on the development of dementia. A test of the brain reserve hypothesis. Psychol Med 27:1337–1344
Salthouse TA (2006) Mental exercise and mental aging: evaluating the validity of the «use it or lose it» hypothesis. Perspect Psychol Sci 1:68–87
Scarmeas N, Zarahn E, Anderson K et al (2003) Association of life activities with cerebral blood flow in Alzheimer Disease. Implications for the cognitive reserve hypothesis. Arch Neurol 60:359–365
Schooler C, Mulatu MS (2001) The reciprocal effects of leisure time activities and intellectual functioning in older people: a longitudinal analysis. Psychol Aging 16:466–482
Wilson RS, Scherr PA, Schneider JA et al (2007) Relation of cognitive activity to risk of developing Alzheimer disease. Neurology 69:1911–1920
Helzner EP, Scarmeas N, Cosentino S et al (2007) Leisure activity and cognitive decline in incident Alzheimer disease. Arch Neurol 64:1749–1754
Nucci M, Mondini S, Mapelli D (2012) Cognitive Reserve Index (CRI). Un questionario per la valutazione della riserva cognitiva. Giornale Italiano di Psicologia 1:155–174
Nucci M, Mapelli D, Mondini S (2012) The Cognitive Reserve Questionnaire (CRIq): a new instrument for measuring the cognitive reserve. Aging Clin Exp Res 24:218–226
Alexander GE, Furey ML, Grady CL et al (1997) Association of premorbid intellectual function with cerebral metabolism in Alzheimer’s Disease: implications for the cognitive reserve hypothesis. Am J Psychiatry 154:165–172
Green RE, Melo B, Christensen B et al (2008) Measuring premorbid IQ in traumatic brain injury: an examination of the validity of the Wechsler Test of Adult Reading (WTAR). J Clin Exp Neuropsychol 30:163–172
Nelson HE, O’Connell A (1978) Dementia: the estimation of premorbid intelligence levels using the New Adult Reading Test. Cortex 14:234–244
Colombo L, Sartori G, Brivio C (2002) Stima del quoziente intellettivo tramite l’applicazione del TIB (Test Breve di Intelligenza). Giornale Italiano di Psicologia 3:613–638
Magni E, Binetti G, Bianchetti A et al (1996) Mini-Mental State Examination: a normative study in Italian elderly population. Eur J Neurol 3:198–202
Nasreddine ZS, Phillips NA, Bédirian V et al (2005) The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53:695–699
Hughes CP, Berg L, Danziger WL (1982) A new clinical scale for the staging of dementia. Br J Psychiatry 140:566–572
Katz S (1983) Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living. J Am Geriatr Soc 31:721–727
Lawton MP, Brody EM (1969) Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 9:179–186
Barbaranelli C, Ingoglia S (2013) Modelli di Equazioni Strutturali: Temi e Prospettive. Led, Milano
Bollen KA (1989) Structural equations with latent variables. Wiley, Hoboken
Conti S, Bonazzi S, Laiacona M et al (2015) Montreal Cognitive Assessment (MoCA)—Italian version: regression based norms and equivalent scores. Neurol Sci 36:209–214
Pirrotta F, Timpano F, Bonanno L et al (2015) Italian validation of Montreal Cognitive Assessment. Eur J Psychol Assess 31:131–137
Santangelo G, Siciliano M, Pedone R (2015) Normative data for the Montreal Cognitive Assessment in an Italian population sample. Neurol Sci 36:585–591
Mondini S, Guarino R, Jarema G et al (2014) Cognitive reserve in a cross-cultural population: the case of Italian emigrants in Montreal. Aging Clin Exp Res 26:655–659
Richards M, Sacker A (2003) Lifetime antecedents of cognitive reserve. J Clin Exp Neuropsychol 25:614–624
Lancioni GE, Perilli V, O’Reilly MF et al (2013) Technology-based orientation programs to support indoor travel by persons with moderate Alzheimer’s disease: impact assessment and social validation. Res Dev Disabil 34:286–293
Caffò AO, Hoogeveen F, Groenendaal M et al (2014) Comparing two different orientation strategies for promoting indoor traveling in people with Alzheimer’s disease. Res Dev Disabil 35:572–580
Bordin A, Pazzaglia F, Busato V et al (2001) Training program for the improvement of sense of direction and spatial orientation in aged people. Giornale Di Gerontologia 59:81–88
Caffò AO, Picucci L, Di Masi MN et al (2011) Working memory components and virtual reorientation: a dual-task study. In: Levin ES (ed) Working memory: capacity, developments and improvement techniques. Nova Science Publishers, Hauppage, pp 249–266
Picucci L, Caffò AO, Bosco A (2009) Age and sex differences in a virtual version of the reorientation task. Cogn Process 10:272–275
Picucci L, Caffò AO, Bosco A (2011) Besides navigation accuracy: gender differences in strategy selection and level of spatial confidence. J Environ Psychol 31:430–438
Jones RN, Fong TG, Metzger E et al (2010) Aging, brain disease, and reserve: implications for delirium. Am J Geriatr Psychiatry 18:117–127
Jones RN, Manly J, Glymour M et al (2011) Conceptual and measurement challenges in research on cognitive reserve. J Int Neuropsychol Soc 17:593–601
Valenzuela MJ, Sachdev P (2007) Assessment of complex mental activity across the lifespan: development of the Lifetime of Experiences Questionnaire (LEQ). Psychol Med 37:1015–1025
Leon I, Garcıa-Garcıa J, Roldan-Tapia L (2014) Estimating cognitive reserve in healthy adults using the cognitive reserve scale. PLoS ONE 9:e102632
Caffò AO, Hoogeveen F, Groenendaal M et al (2014) Intervention strategies for spatial orientation disorders in dementia: a selective review. Dev Neurorehabil 17:200–209
Lancioni GE, Singh NN, O’Reilly MF et al (2014) Persons with moderate Alzheimer’s disease use simple technology aids to manage daily activities and leisure occupation. Res Dev Disabil 35:2117–2128
Maseda A, Millán-Calenti JC, Lorenzo-López L et al (2013) Efficacy of a computerized cognitive training application for older adults with and without memory impairments. Aging Clin Exp Res 25:411–419
Deary IJ, Batty GD (2007) Cognitive epidemiology. J Epidemiol Community Health 61:378–384
Caffò AO, De Caro MF, Picucci L et al (2012) Reorientation deficits are associated with amnestic mild cognitive impairment. Am J Alzheimers Dis Other Demen 27:321–330
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study. This article does not contain any studies with animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Caffò, A.O., Lopez, A., Spano, G. et al. The role of pre-morbid intelligence and cognitive reserve in predicting cognitive efficiency in a sample of Italian elderly. Aging Clin Exp Res 28, 1203–1210 (2016). https://doi.org/10.1007/s40520-016-0580-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-016-0580-z