
Abstract
The Montreal Cognitive Assessment (MoCA) is a rapid screening battery, also including subtests to assess frontal functions such as set-shifting, abstraction and cognitive flexibility. MoCA seems to be useful to identify non-amnestic mild cognitive impairment (MCI) and subcortical dementia; it has high sensitivity and specificity in distinguishing MCI from mild Alzheimer’s Disease. Previous studies revealed that certain items of MoCA may be culturally biased and highlighted the need for population-based norms for the MoCA. The aim of present study was to collect normative values in a sample of Italian healthy subjects. Four hundred and fifteen Italian healthy subjects (252 women and 163 men) of different ages (age range 21–95 years) and educational level (from primary to university) underwent MoCA and Mini Mental State Examination (MMSE). Multiple linear regression analysis revealed that age and education significantly influenced performance on MoCA. No significant effect of gender was found. From the derived linear equation, a correction grid for MoCA raw scores was built. Inferential cut-off score, estimated using a non-parametric technique, is 15.5 and equivalent scores were computed. Correlation analysis showed a significant but weak correlation between MoCA adjusted scores with MMSE adjusted scores (r = 0.43, p < 0.001). The present study provided normative data for the MoCA in an Italian population useful for both clinical and research purposes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Many brief screening measures of general cognitive status have been developed in response to the need for early detection of cognitive deterioration in primary care settings. Such screening tests are expected to be relatively quick, easy to administer, score and interpret [1].
Among the cognitive screening tests, the Mini Mental State Examination (MMSE [2]) is likely the most commonly used instrument for detecting cognitive deterioration [3]. However, it has been underlined that MMSE makes a large use of verbal material, is not sensitive to subtle cognitive impairments and may fail to identify cognitive defects in frontal/executive, attention or visuospatial domains [3, 4].
On the basis of the above considerations, Nasreddine et al. [3] developed the Montreal Cognitive Assessment (MoCA) covering eight cognitive domains: short-term and delayed verbal memory, visuospatial abilities, executive functions, attention, concentration, working memory, language, orientation to time and place. With respect to MMSE, MoCA includes several tasks with visuospatial material, together with tasks and procedures specifically assessing frontal/executive functions and attention [5], and long-term memory [3]. Nasreddine et al. [3] reported that a cut-off <26 was the best balance between sensitivity and specificity for identifying cognitive deterioration in the course of mild cognitive impairment (MCI) and Alzheimer’s disease (AD). Moreover, MoCA has been reported to be a sensitive tool for screening patients with non-AD dementia such as the behavioral variant of Frontotemporal Dementia [6], dementia associated with Parkinson’s Disease [7], and vascular dementia [8].
In administering MoCA, however, it should be taken into account that several items may be culturally biased, and this implies the strong need to employ population-based norms [9]. MoCA has been translated in Italian by Pirani et al. [10], but until now no normative study has been performed in Italian population. The present study was designed to provide normative data for MoCA stratified by age, education and sex in a sample of Italian healthy subjects. According to the statistical procedures adopted for most neuropsychological tests carried out on Italian population [11], inferential cut-off scores for MoCA and for each cognitive domain were calculated and a transformation of raw scores into equivalent scores (ES) was proposed.
Materials and methods
Subjects
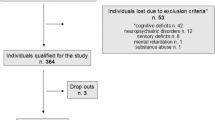
Participants were recruited in different districts of Italy (most of them in Naples, Milan and Siena) and were enrolled in the study if they had no current or past history of neurologic or psychiatric diseases (e.g., alcohol or drug abuse, depression or major psychiatric diseases, brain injury, stroke and dementia).To avoid enrolment of a “super-normal sample” that may not represent the general population, individuals with mild hypertension and well-compensated type II diabetes were not excluded. However, we excluded from analysis participants who achieved an age-and education-adjusted MMSE score below the normal cut-off [12], to reduce probability of enrolling individuals with possible diffuse cognitive impairment, as it has been done in previous normative studies on Italian neuropsychological tests [e.g., 13–15].
All participants took part in the study on a voluntary basis after having provided their written informed consent and without receiving any reward. This enrolment procedure resulted in a sample of 415 healthy Italian subjects (252 women and 163 men), covering a wide age range (21–95 years), and representing all levels of formal education (from primary school to university). Mean age of the whole sample was 56.82 years (18.8), mean formal education was 11.13 years (4.76). The distribution of the sample for age and education is reported in Table 1.
Procedure
All participants were tested individually in a quiet room. All of them first underwent the Italian version of MoCA [10], and then completed the Italian version of MMSE [12].
MoCA consists of 12 subtasks exploring the following cognitive domains: (1) memory (score range 0–5), assessed by means of delayed recall of five nouns, after two verbal presentations; (2) visuospatial abilities (score range 0–4), assessed by a clock-drawing task (3 points) and by copying of a cube (1 point); (3) executive functions (score range 0–4), assessed by means of a brief version of the Trail Making B task (1 point), a phonemic fluency task (1 point), and a two-item verbal abstraction task (2 points); (4) attention, concentration and working memory (score range 0–6), assessed by means of a sustained attention task (target detection using tapping; 1 point), a serial subtraction task (3 points), and forward and backward span tasks for digits (1 point each); (5) language (score range 0–6), assessed by a naming task with low-familiarity animals (3 points), repetition of two syntactically complex sentences (2 points) and the abovementioned phonemic fluency task; (6) temporal and spatial orientation (score range 0–6), assessed by means of structured queries (i.e., “Tell me the year, month, exact date, and day of the week; Tell me the name of this place, and which city it is in”) (6 points).
MoCA total score ranges from 0 (worst performance) to 30 (best performance).
Statistical analysis
Statistical analysis was performed following the procedure adopted by Capitani et al. [16]. Several multiple regression analyses were performed to assess the relative influence of demographic variables (i.e., gender, age, educational level) on the participants’ total MoCA score and domain subscores. The effects of age and educational level (expressed as years of schooling) were explored after several transformations (e.g., logarithmic, quadratic). Gender, age and education were entered into a multiple linear regression analysis to partial out their possible overlapping effect. The results of the multiple regression analyses were entered into a regression equation to calculate a correction factor for each subject of the sample. Adjusted scores were obtained by adding or subtracting the contribution of concomitant variables from the original scores. After correcting all the raw scores, the adjusted scores were ranked from the worst to the best and a non-parametric procedure [17], with a set of confidence at 95 %, has been used to estimate unidirectional limits of tolerance that discriminate a score as normal or abnormal according to falling within the highest 95 % or within the lowest 5 % of the normal population [16, 18].
Cut-off value was defined the score at which or below which the probability that an individual belongs to the normal population is less than 0.05 [18].
Adjusted scores were then converted to a five-point interval scale, from 0 to 4 equivalent scores [11]. The five-point interval scale was divided as follows: 0 = scores equal or lower than the outer tolerance limit (5 %); 4 = scores higher than the median value of the whole sample; 1, 2 and 3 were obtained by dividing into three equal parts the area of distribution between 0 and 4 [11].
The same procedure was used to estimate the outer tolerance limits for the different cognitive domains assessed by the MoCA.
To allow adjustment of the raw scores of newly tested individuals according to demographic variables, a correction grid was built for any combination of age level (by 10-year steps) and educational level (according to the Italian schooling system).
Results
Table 2 shows descriptive statistics of demographic aspects, MMSE, total MoCA score and MoCA domain subscores. Mean MoCA total score was lower in older and less educated subjects (Table 3).
The square root of education years and the logarithmic transformation of the age [log(100 − age)] were used for the total score and for all cognitive domain subscores, but for the domain orientation where age was not transformed. After such transformations, the final regression model for the total MoCA score included age and education but not gender, accounting for 48 % of the total variance. The linear regression analyses for the domain subscores revealed that gender significantly affected memory and attention only, whereas education significantly affected all six cognitive domains, and age significantly affected all cognitive domains but attention (Table 4).
For a sample of 415 subjects and using non-parametric procedure, outer and inner tolerance limits are defined by values corresponding to the 14th and 29th worst observations. The outer tolerance limit obtained, or cut-off point, for the total MoCA score was 15.5; while inner tolerance limit was 17.54. Adjusted MoCA scores lower than or equal to 15.5 can be considered abnormal because the region of tolerance includes also the value of the 14th worst observation [16]. Adjusted MoCA scores higher than 17.54 indicate a normal performance, while intermediate scores (15.5–17.54) indicate a borderline performance, which in our study was obtained by 3.6 % of the sample.
We applied the abovementioned procedure to estimate outer tolerance limits for each domain subscore. The ES, the number of subjects included within each ES (density) and the cumulative frequency of subjects comprised from 0 to 1, 2, 3 and 4 are shown in Table 5. It is important to note that the outer tolerance limit for the memory subscore was negative, thus not allowing to apply any correction for this cognitive domain. Moreover, several adjustment factors computed for the domain subscores of visuospatial abilities and executive functions were larger than the respective outer tolerance limits, thus hindering applicability of these domain subscores to some combinations of age and education.
To allow adjustment of the raw scores of newly tested individuals according to demographic variables, a correction grid was built for the most frequent combinations of age (by 10-year steps) and educational level (according to the Italian schooling system). When the correction grid does not allow to make adjustments because individuals have demographic characteristics not included in the grid, it is useful to use the regression equations to estimate the adjusted scores (Table 6).
Analysis of the correlation coefficient between adjusted total MoCA score and MMSE adjusted scores revealed a statistically significant, but moderate, positive correlation (r = 0.43, p < 0.001).
Discussion
The present study is the first to provide age-, education- and sex-stratified normative data for the Italian version of MoCA, obtained from a large sample of healthy subjects recruited in different regions.
The mean total MoCA score of 21.98 points found in our study was lower than the mean score for the normal control in the original study (27.4) [3], but close to that reported in a Japanese population study on older subjects (21.8) [19], and to that reported in a Portuguese study (24.7) [20]. Moreover, in the present study, a cut-off of 15.5 points is suggestive for presence of cognitive decline, and this value is far from the cut-off reported in the original study (26) [3]. These discrepancies may depend on possible selection bias for the non-population-based samples in the original study and/or on cultural and linguistic artifacts when the original MoCA has been translated into the Italian version.
Notwithstanding the relatively lower scores observed in the present sample, our findings are consistent with the previous studies in several ethnic groups [9, 19, 20], as they show that the total MoCA score is significantly affected by age and schooling. The lack of the effect of gender on the total MoCA score was also consistent with previous Portuguese [20] and Japanese [19] normative studies.
Since MoCA allows to evaluate different cognitive domains, for the purpose of detecting cognitive impairments related to both cortical and subcortical dementias [3], here we provided normative data for all cognitive domain subscores and evaluated the possible effects of socio-demographic variables on them. Previous normative studies did not provide such data, so possible comparison data are not available at the moment. We observed that educational level influenced performance on all cognitive domains, while age influenced the performance in all subdomains but attention. The influence of age and education on cognitive performances is consistent with the previous reports [16]. Most normative studies, indeed, demonstrate that age and education must be taken into account when evaluating raw scores obtained by old and/or less educated individuals. This is particularly exemplified by the huge effect of illiteracy on performance on neuropsychological tasks [21], some of which cannot be administered to people without any formal education. In the present study, we did not enroll individuals without any formal education since they are very few in Italian samples, and would likely require different administration and scoring procedures [21].
Gender was found to influence the attention and the memory domain subscores. In the former domain, females performed poorer than males; whereas in the latter, females achieved higher scores than males. The findings about a female advantage in the memory subscore appear to be consistent with Italian normative data for the serial position curve test [11] and with other studies reporting a female advantage in verbal memory tasks, such as recall of word lists, paired-associate learning [22], story recall [23] and Rey’s word list learning test [24, 25]. However, it should be remembered that we did not provide the correction grid for memory domain because all demographic variables entered in the final regression model did not explain data variability sufficiently.
As for the attention domain, the present data appear to be consistent with those reported in the Italian normative study on a paper-and-pencil digit cancelation test (attentional matrices [11]), but in general, there are limited and divergent empirical evidences about gender differences on attentional tests (e.g., [26, 27]).
Our findings about correlation between MoCA and MMSE scores indicated a significant but moderate correlation between the two instruments, consistent with the idea that they evaluate partially different aspects of cognitive functioning [3].
In conclusion, the present study provided normative data for MoCA and cut-off values to identify possible cognitive decline. For this purpose, it is important to underline that demographic (i.e., age and education) aspects significantly influence performance on MoCA and domain subscores, and that specific reference values must be applied when using MoCA in research and clinical contexts. The total MoCA scores seem to be suitable for screening MCI in community health care [3], but use of memory domain subscore appears to be hampered by the limited score distribution observed in our sample, at least on the present Italian version of the test.
References
Lezak MD, Howieson DB, Bigler ED, Tranel D (2012) Neuropsychological Assessment. Oxford University Press, Oxford
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H (2005) The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53:695–699
Mitchell AJ (2009) A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J Psychiatr Res 43:411–431
Smith T, Gildeh N, Holmes C (2007) The Montreal Cognitive Assessment: validity and utility in a memory clinic setting. Can J Psychiatry 52:329–332
Freitas S, Simões MR, Alves L, Duro D, Santana I (2012) Montreal Cognitive Assessment (MoCA): validation study for frontotemporal dementia. J Geriatr Psychiatry Neurol 25:146–154. doi:10.1177/0891988712455235
Hoops S, Nazem S, Siderowf AD, Duda JE, Xie SX, Stern MB, Weintraub D (2009) Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology 73:1738–1745
Freitas S, Simões MR, Alves L, Vicente M, Santana I (2012) Montreal Cognitive Assessment (MoCA): validation study for vascular dementia. J Int Neuropsychol Soc 18:1031–1040
Rossetti HC, Lacritz LH, Cullum CM, Weiner MF (2011) Normative data for the Montreal Cognitive Assessment (MoCA) in a population-based sample. Neurology 77:1272–1275. doi:10.1212/WNL.0b013e318230208a
Pirani A, Tulipani C, Neri M (2006) Montreal Cognitive Assessment, Italian version. http://mocatest.org/pdf_files/test/MoCA-Test-Italian.pdf
Spinnler H, Tognoni G (1987) Standardizzazione e taratura italiana di test neuropsicologici. Ital J Neurol Sci 6(Suppl 8):8–120
Measso G, Cavarzeran F, Zappalà G et al (1993) The Mini-Mental State Examination: normative study of an Italian random sample. Dev Neuropsychol 9:77–85
Appollonio I, Leone M, Isella V et al (2005) The Frontal Assessment Battery (FAB): normative values in an Italian population sample. Neurol Sci 26:108–116
Caffarra P, Vezzadini G, Dieci F, Zonato F, Venneri A (2002) Rey-Osterrieth complex figure: normative values in an Italian population sample. Neurol Sci 22:443–447
Caffarra P, Vezzadini G, Zonato F, Copelli S, Venneri A (2003) A normative study of a shorter version of Raven’s Progressive Matrices 1938. Neurol Sci 24:336–339
Capitani E (1997) Normative data and neuropsychological assessment. Common problems in clinical practice and research. Neuropsychol Rehab 7:295–309
Ackermann H (1985) Mehrdimensionale nicht-parametrische Normbereiche. Methodologische und medizinische Aspekte. Springer, Berlin
Cattelani R, Dal Sasso F, Corsini D, Posteraro L (2011) The modified five-point test: normative data for a sample of Italian healthy adults aged 16–60. Neurol Sci 32:595–601. doi:10.1007/s10072-011-0489-4
Narazaki K, Nofuji Y, Honda T, Matsuo E, Yonemoto K, Kumagai S (2013) Normative data for the Montreal Cognitive Assessment in a Japanese community-dwelling older population. Neuroepidemiology 40:23–29. doi:10.1159/000339753
Freitas S, Simões MR, Alves L, Santana I (2011) Montreal Cognitive Assessment (MoCA): normative study for the Portuguese population. J Clin Exp Neuropsychol 33:989–996. doi:10.1080/13803395.2011.589374
Ardila A, Bertolucci PH, Braga LW, Castro-Caldas A, Judd T, Kosmidis MH, Matute E, Nitrini R, Ostrosky-Solis F, Rosselli M (2010) Illiteracy: the neuropsychology of cognition without reading. Arch of Clin Neuropsychol 25:689–712
Youngjohn JR, Larrabee GJ, Crook TH (1991) First-Last Names and the Grocery List Selective Reminding Test: two computerized measures of everyday verbal learning. Arch Clin Neuropsychol 6:287–300
Zelinski EM, Gilewski MJ, Schaie KW (1993) Individual differences in cross-sectional and 3-year longitudinal memory performance across the adult life span. Psychol Aging 8:176–186
Bolla-Wilson K, Bleecker ML (1986) Influence of verbal intelligence, sex, age, and education on the Rey Auditory Verbal Learning Test. Dev Neuropsychol 2:203–211
Bleecker ML, Bolla-Wilson K, Agnew J, Meyers DA (1988) Age-related sex differences in verbal memory. J Clin Psychol 44:403–411
Merritt P, Hirshman E, Wharton W, Stangl B, Devlin J, Lenz A (2007) Evidence for gender differences in visual selective attention. Pers Indiv Differ 43:597–609
Teleb AA, Al Awamleh AA (2012) Gender differences in cognitive abilities. Curr Res Psychol 3:33–39
Acknowledgments
The authors thank dr. Angela Villani and dr. Maria Grazia Angrisano for their contribution in collecting data in Naples. Moreover, the authors thank dr. Irene Pirali and Sonia Rossi for their contribution in collecting data in Milan.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Santangelo, G., Siciliano, M., Pedone, R. et al. Normative data for the Montreal Cognitive Assessment in an Italian population sample. Neurol Sci 36, 585–591 (2015). https://doi.org/10.1007/s10072-014-1995-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-014-1995-y