
Abstract
Background
Dravet syndrome (DS) is one of the most severe forms of drug-resistant epilepsy and available interventions fail to control seizures in most patients. Cannabidiol (CBD) is the first in a new class of antiepileptic drugs with a distinctive chemical structure and mechanism of action.
Objective
The aim of this systematic review was to evaluate the efficacy and safety of CBD as adjunctive treatment for seizures in patients with DS using meta-analytical techniques.
Methods
We searched for randomized, placebo-controlled, single- or double-blinded trials. Main outcomes included ≥ 50% reduction in baseline convulsive seizure frequency and the incidence of treatment withdrawal and adverse events (AEs). Risk ratios (RRs) with 95% confidence intervals (95% CIs) were estimated through the inverse variance method.
Results
Three trials were included involving 359 participants, 228 for CBD and 131 for placebo groups. In all trials, the active treatment was a plant-derived pharmaceutical formulation of purified CBD oral solution. The pooled RR for 50% response during the treatment was 1.69 (95% CI 1.21–2.36; p = 0.002). Across the trials, treatment was discontinued in 20 (9.0%) and 3 (2.3%) cases in the add-on CBD and placebo groups, respectively; the RR for CBD withdrawal was 3.12 (95% CI 1.07–9.10; p = 0.037). The RR to develop any AE during add-on CBD treatment was 1.06 (95% CI 0.87–1.28; p = 0.561). AEs significantly associated with adjunctive CBD were somnolence, decreased appetite, diarrhea, and increased serum aminotransferases.
Conclusions
Adjunctive CBD resulted in a greater reduction in convulsive seizure frequency than placebo and a higher rate of AEs in patients with DS presenting with seizures uncontrolled by concomitant antiepileptic therapy.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Adjunctive cannabidiol (CBD) can reduce convulsive seizure frequency in patients with Dravet syndrome. |
The most common adverse events are somnolence, decreased appetite, diarrhea, and increased serum aminotransferases. |
Drug–drug interactions can influence the efficacy and safety profile of CBD. |
1 Introduction
Epilepsies are a heterogeneous group of most often severe brain disorders and treatment is mainly symptomatic [1, 2]. The majority of patients can achieve control of their seizures through antiepileptic therapy, whereas one-third are resistant to treatment [3,4,5], causing significant morbidity [6], increased mortality [7, 8], and decreased life expectancy [9].
Dravet syndrome (DS) is one of the most severe forms of drug-resistant epilepsy. Approximately two-thirds of the patients with DS carry loss-of-function mutations in the voltage-gated sodium channel α1 subunit gene (SCN1A), and mutations in other genes have been reported in SCN1A-negative patients. Most mutations arise de novo, but inheritance from a mildly affected parent can also occur [10]. The onset of DS is typically during the first year of life in previously healthy infants with prolonged convulsive seizures, which are often triggered by fever and can evolve into status epilepticus [11]. Delay in psychomotor development becomes apparent from the second year onwards and behavioral disturbances are common. Long-term seizure outcome is poor, with many patients still having seizures in adulthood, and moderate to severe intellectual impairment and disabilities characterize nearly all the affected individuals [12].
Valproic acid (VPA) and clobazam (CLB) are widely used in DS. VPA is often chosen to prevent the initial recurrence of convulsive seizures, and benzodiazepines are frequently co-administered to reduce the duration of long-lasting seizures. Second-line and later options typically include stiripentol (STP), topiramate, levetiracetam, ketogenic diet, bromides, and vagus nerve stimulation [12].
Antiepileptic polytherapy is common, but it fails to control seizures in most patients and there remains an unmet clinical need to identify new effective therapeutic strategies.
Cannabidiol (CBD) is a major chemical component of the resin of Cannabis sativa plant. In contrast to tetra-hydrocannabinol, CBD lacks psychoactive effects and is devoid of abuse liability [13]. Compared with conventional antiepileptic drugs (AEDs), CBD has a distinctive chemical structure and mechanism of action. CBD has negligible affinity or activity at the cannabinoid receptors at clinically meaningful concentrations and its anti-seizure properties are mainly mediated by the modulation of intracellular Ca2+ levels, through both the inhibition of the G-protein coupled receptor GPR55 and activation of the transient receptor channel TRPV1, and the inhibition of adenosine re-uptake [14].
A plant-derived pharmaceutical formulation of purified CBD oral solution (Epidiolex®) was approved in June 2018 by the US Food and Drug Administration as treatment and in July 2019 by the European Medicines Agency as adjunctive therapy in conjunction with CLB for seizures associated with DS or Lennox-Gastaut syndrome (LGS) for patients aged 2 years and older.
The aim of this systematic review and meta-analysis was to assess the efficacy and safety of adjunctive CBD for the treatment of seizures in patients with DS.
2 Methods
2.1 Search Strategy
This systematic review and meta-analysis was reported according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [15]. We systematically searched (October week 3, 2019) MEDLINE (accessed by PubMed), the Cochrane Central Register of Controlled Trials (CENTRAL) and the US National Institutes of Health Clinical Trials Registry (http://www.clinicaltrials.gov) (search strategies are outlined in Electronic Supplementary Material). Additional data were sought in the Assessment Report and Drug Approval Package of CBD by the European Medicines Agency/Committee for Medicinal Products for Human Use and the US Food and Drug Administration [16, 17]. The manufacturer of CBD was contacted for information about any unpublished or ongoing studies. There were no date limitations or language restrictions. The reference lists of retrieved studies were reviewed to identify additional reports of relevant trials. The protocol was not registered previously.
2.2 Eligibility Criteria
Studies were selected when they met the following entry criteria: randomized, double or single blinded, placebo-controlled, parallel group studies with active and control groups receiving CBD and matched placebo, respectively, in addition to an existing AED treatment. Participants had to meet the following criteria: any sex, any ethnicity, pediatric and/or adult age, diagnosis of DS and seizures uncontrolled by concomitant AEDs.
2.3 Outcome Measures
The primary efficacy outcome was the proportion of patients who achieved ≥ 50% reduction from baseline in convulsive seizure frequency during the treatment period. A convulsive seizure was defined as a tonic, clonic, tonic-clonic, or atonic seizure. Secondary efficacy outcomes were the percentage change in convulsive seizure frequency during the treatment period compared with baseline and the proportion of patients who achieved 100% reduction in baseline convulsive seizure frequency.
Safety outcomes were the proportions of patients withdrawing from the treatment for any reason; withdrawing from the treatment for adverse events (AEs); experiencing any AE; experiencing any serious adverse event (SAE); and experiencing any of the AEs found to be commonly related to CBD on the basis of previous evidence [18] (i.e., somnolence, decreased appetite, diarrhea, pyrexia, vomiting, fatigue, upper respiratory infections, increase of serum aminotransferases concentrations by threefold or greater the upper limit of the normal range).
Changes from baseline to the end of treatment in measures of global functioning, including Patient or Caregiver Global Impression of Change (P/CGIC), sleep disruption, daytime sleepiness, quality of life, and behavioral adaptation, as assessed by validated scales, were also reviewed.
2.4 Study Selection, Data Extraction and Assessment of the Risk of Bias
Two review authors (S. L. and F. B.) independently assessed trials for inclusion and extracted the following information from included studies: main study author and year of publication, methods of randomization, allocation concealment and blinding, duration of baseline and treatment periods, dose/s of CBD tested, number and demographics of participants, number of participants experiencing each outcome, and change in baseline convulsive seizure frequency during treatment per randomized group. Any disagreement was resolved by discussion with a third review author (M. S.). The risk of bias of the identified studies was assessed in accordance with the recommendations of the Cochrane Collaboration [19].
2.5 Statistical Analysis
Heterogeneity among the trials was assessed by the Chi squared test and the I2 statistics for heterogeneity [19, 20]. Provided no significant heterogeneity was present (p > 0.05), results were synthesized using a fixed-effects model. If the probability value was ≤ 0.05, the heterogeneity was interpreted according to the I2 statistic: a fixed-effects model was adopted for I2 < 40% and a random-effects model was adopted for I2 ≥ 40% [21,22,23,24,25]. We presented heterogeneity statistics for all analyses unless only one trial contributed data and heterogeneity was not applicable. The risk ratio (RR) and mean difference (MD) with 95% confidence intervals (CIs) were the measures of associations between treatment and dichotomous or continuous outcomes. The intent-to-treat (ITT) population data were used for the efficacy analyses. The subgroup analysis of primary efficacy outcome by concomitant use of CLB (CLB-On for patients taking concomitant CLB and CLB-Off for patients not taking concomitant CLB) was planned. Results were presented according to CBD daily dose, where sufficient data were available. Reported probability values were two-sided, with significance set at < 0.05. Data analysis was performed using STATA/IC 13.1 statistical package (StataCorp LP, College Station, TX, USA).
3 Results
3.1 Results of the Search
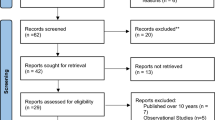
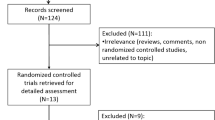
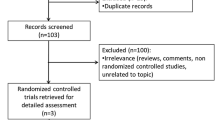
Two hundred and fifty-eight records were identified by database and trial registers searching. Four randomized controlled trials (RCTs) were retrieved for detailed assessment; one of them was withdrawn by the sponsor before participants were enrolled (ClinicalTrials.gov number NCT02318563). Accordingly, three studies [26,27,28] were considered in the review and included in the meta-analysis (Fig. 1).

Flow diagram of study selection process. CENTRAL Cochrane Central Register of Controlled Trials
3.2 Characteristics and Risk of Bias of Included Studies
The included studies were multicenter, randomized, double-blind, placebo-controlled, parallel group trials. They enrolled 359 participants according to the ITT, 228 for CBD and 131 for placebo groups, respectively. In all trials, the active treatment was a plant-derived pharmaceutical formulation of purified CBD oral solution (100 mg/mL) (Epidiolex®), which was administered as add-on therapy to the preexisting antiepileptic regimen. One study aimed to investigate the dose-ranging safety [26] and two trials assessed both the efficacy and safety [27, 28] of adjunctive CBD in patients with DS. Characteristics of the studies and participants are summarized in Tables 1 and 2, respectively. In the GWPCARE2, two patients assigned to CBD 10 mg/kg/day temporarily received a dose above the target and were included in the CBD 20 mg/kg/day group for the safety analysis.
All trials used adequate methods of sequence generation and allocation concealment. We judged the included trials at low risk of performance and detection bias since blinding was ensured by matching placebo, and neither the investigators nor the patients knew the identity of the treatment being administered. The risks of attrition and selective reporting bias were rated to be low since all patients lost to follow-up and withdrawals were documented, and there was no suspicion of selective outcome reporting. All trials were sponsored by the manufacturer of CBD (GW Pharmaceuticals).
3.3 Fifty Percent or Greater Reduction in Convulsive Seizure Frequency
The percentages of patients who had at least 50% reduction in convulsive seizure frequency during the treatment period were 45.4% with add-on CBD and 26.6% with placebo, respectively [27, 28]. The overall pooled RR for 50% response across the trials [27, 28] was 1.69 (95% CI 1.21–2.36; p = 0.002) (Chi squared = 0.13, df = 1, p = 0.716; I2 = 0.0%) (Fig. 2a). During the treatment period, the estimated RRs for ≥ 50% convulsive seizure frequency reduction were 1.68 (95% CI 1.03–2.75; p = 0.038) for adjunctive CBD at the dose of 10 mg/kg/day [28] (Fig. 2b) and 1.73 (95% CI 1.22–2.45; p = 0.002) (Chi squared = 0.26, df = 1, p = 0.611; I2 = 0.0%) at the dose of 20 mg/kg/day in comparison with placebo [27, 28] (Fig. 2c).

Fifty percent or greater reduction in monthly seizure convulsive frequency from baseline during the treatment period. Risk ratios from fixed-effects model are shown. CBD cannabidiol, CI confidence interval
Across the trials [27, 28], the responder rates in convulsive seizure frequency were 27.5% in the add-on CBD arm and 20.0% in the placebo group among patients not taking CBL and the estimated RR was 1.34 (95% CI 0.65–2.79; p = 0.431) (Chi squared = 1.70, df = 1, p = 0.193; I2 = 41.1%); among CBL-On patients, the ≥ 50% reduction in convulsive seizure frequency was achieved by 55.2% and 30.4% in the adjunctive CBD and placebo groups, respectively, and the corresponding RR was 1.72 (95% CI 1.19–2.48; p = 0.004) (Chi squared = 0.30, df = 1, p = 0.584; I2 = 0.0%] (Fig. 3a). The RRs to achieve ≥ 50% convulsive seizure frequency reduction with add-on CBD treatment at 10 mg/kg/day were 2.29 (95% CI 0.46–11.24; p = 0.309) in CLB-Off and 1.52 (95% CI 0.94–2.45; p = 0.088) in CLB-On subgroups of patients [28] (Fig. 3b). The estimated RRs for a 50% or greater reduction in frequency of convulsive seizures for patients assigned to 20 mg/kg/day in comparison with placebo were 1.39 (95% CI 0.66–2.90; p = 0.383) (Chi squared = 2.18, df = 1, p = 0.139; I2 = 54.2%) and 1.80 (95% CI 1.23–2.64; p = 0.002) (Chi squared = 0.15, df = 1, p = 0.697; I2 = 0.0%) in CLB-Off and CLB-On subgroups, respectively [27, 28] (Fig. 3c).

Fifty percent or greater reduction in monthly seizure convulsive frequency from baseline during the treatment period according to clobazam status. Risk ratios from fixed-effects model are shown. CBD cannabidiol, CI confidence interval
3.4 Percentage Change and 100% Reduction in Convulsive Seizure Frequency
The overall MD in convulsive seizure frequency during the treatment period between adjunctive CBD and placebo was 20.3 (95% CI 8.2–32.4; p = 0.001) (Chi squared = 0.06, df = 1, p = 0.808; I2 = 0.0%) in favor of CBD [28]. The MD in the reduction of convulsive seizure frequency resulted in 21.8 (95% CI 4.9–38.7; p = 0.012) percentage points between the 10-mg CBD and placebo groups [28] and 18.8 (95% CI 1.5–36.1; p = 0.033) percentage points between the 20-mg CBD and placebo arms [28] in favor of add-on CBD. Freedom from convulsive seizures was achieved by 4.9% of the patients assigned to adjunctive CBD and none of the participants receiving placebo [RR 6.77 (95% CI 0.36–128.38); p = 0.202] [27].
3.5 Treatment Withdrawal and Adverse Events
Across the trials, treatment was discontinued in 20 (9.0%) and 3 (2.3%) cases in the add-on CBD and placebo groups, respectively; the overall RR for withdrawal for any reason was 3.12 (95% CI 1.07–9.10; p = 0.037) (Chi squared = 0.86, df = 2, p = 0.649; I2 = 0.0%) [26,27,28]. The RRs for treatment withdrawal were 4.37 (95% CI 0.52–36.36; p = 0.173) (Chi squared = 0.19, df = 1, p = 0.661; I2 = 0.0%) for adjunctive CBD at the dose of 10 mg/kg/day [26, 28] and 3.49 (95% CI 1.19–10.25; p = 0.023) (Chi squared = 0.92, df = 2, p = 0.632; I2 = 0.0%) for CBD at the dose of 20 mg/kg/day [26,27,28], in comparison with placebo. Drug discontinuation due to AEs occurred in 15 (6.8%) and 1 (0.8%) participants in the active and control groups, respectively [RR 4.68 (95% CI 1.10–19.95); p = 0.037] (Chi squared = 0.87, df = 2, p = 0.647; I2 = 0.0%) [26,27,28]. The RRs for treatment discontinuation due to AEs were 2.67 (95% CI 0.13–56.63; p = 0.529) for adjunctive CBD at the 10-mg/kg daily dose [26, 28] and 6.44 (95% CI 1.49–27.85; p = 0.013) (Chi squared = 0.55, df = 2, p = 0.760; I2 = 0.0%) for adjunctive CBD at the 20-mg/kg daily dose [26,27,28] (Table 3).
AEs were reported by 195 (88.2%) and 108 (82.4%) patients treated with adjunctive CBD and placebo, respectively [RR 1.06 (95% CI 0.87–1.28); p = 0.561] (Chi squared = 6.59, df = 2, p = 0.037; I2 = 69.7%) [26,27,28]; SAEs were reported by 44 (19.9%) and 14 (10.7%) patients treated with adjunctive CBD and placebo [RR 1.67 (95% CI 0.96–2.91); p = 0.069] (Chi squared = 1.45, df = 2, p = 0.485; I2 = 0.0%) [26,27,28] (Table 4). The incidence rates of the selected AEs in the add-on CBD-versus placebo-treated participants were as follows: somnolence 26.7% versus 12.2%, decreased appetite 24.0% versus 10.7%, diarrhea 21.7% versus 11.5%, pyrexia 20.4% versus 12.2%, vomiting 12.2% versus 5.3%, fatigue 14.9% versus 8.4%, upper respiratory tract infection 6.8% versus 6.1%, increased alanine or aspartate aminotransferases more than 3 times the upper normal limit 15.4% versus 0.8% (Table 4). The analysis per daily dose is summarized in Table 5.
3.6 Global Functioning Measures
An improvement from baseline in overall condition (slightly improved, much improved, or very much improved) according to the CGIC at the last visit was reported in 122 out of 192 patients (63.5%) in the adjunctive CBD group and in 47 out of 123 patients (38.2%) in the placebo arm [RR 1.64 (95% CI 1.28–2.10); p < 0.001] (Chi squared = 0.30, df = 1, p = 0.586; I2 = 0.0%). The RRs for improvement at the CGIC were 1.64 (95% CI 1.18–2.29; p = 0.003) for CBD at the dose of 10 mg/kg/day and 1.59 (95% CI 1.22–2.07; p = 0.001) (Chi squared = 0.56, df = 1, p = 0.456; I2 = 0.0%) for CBD at the dose of 20 mg/kg/day in comparison with placebo. One trial provided data on changes from baseline to the end of treatment in scores evaluating sleep disruption, daytime sleepiness, quality of life, and behavioral adaption [27]; no significant differences emerged between the treatments (Table 6).
4 Discussion
Cannabidiol was more effective than placebo in reducing the frequency of convulsive seizures when added to existing AEDs at both the daily doses of 10 and 20 mg/kg in children and adolescents with DS. The higher perception of improvement from baseline in overall condition held by caregivers in the active group than in the placebo arm supported the favorable effect of therapy with CBD. Remarkably, the improvement in seizure control was achieved by patients with severe epilepsy who had previously failed a median of four AEDs, were taking an average of three anti-epileptic treatments, and had a high frequency of seizures at baseline.
A larger magnitude of treatment effect was found in patients taking CLB compared with patients not on CLB, with the confidence intervals for the CLB-Off subgroups overlapping unity. This finding may be, at least partly, ascribed to the bi-directional pharmacokinetic interaction between CBD and CLB. CBD can inhibit the catalytic activity of the cytochrome P450 (CYP) 2C19 and determine a 2- to 4-fold increase in plasma concentrations of N-desmethylclobazam (N-CLB), the biologically active metabolite of CLB [26, 29]. In parallel, CLB leads to an approximate 1.5-fold increase in 7-hydroxy-CBD, the CBD active metabolite, likely via inhibition of CYP2D6 and glucuronidation [29]. Recently, a pre-clinical study aimed at addressing the nature of the interaction between CBD and CLB identified both pharmacodynamic and pharmacokinetic mechanisms [30]. Indeed, combined treatment with CBD and CLB resulted in greater anticonvulsant efficacy in a Scn1a+/− mouse model of DS only when an anticonvulsant dose of CBD was used, whereas a sub-anticonvulsant dose of CBD did not promote greater antiseizure effects despite increasing plasma CLB levels [30]. Further, a novel pharmacodynamic mechanism where CBD and CLB together enhanced inhibitory GABAA receptor activation was identified [30]. Heterogeneity in baseline characteristics between CLB-On and CLB-Off patients might also account for the differential treatment response; as most of the patients not taking CLB had previously tried CLB without success, had failed more AEDs during their lifetime, and had higher seizure frequency at baseline, they may be considered a group more difficult to treat [16].
The limited sample size did not allow us to draw definitive conclusions about the therapeutic effect of CBD in patients not taking CLB. with regard to this critical concern, patients enrolled in the pivotal GWPCARE1 Part B trial who were taking CLB and STP at baseline did not show a further increase in N-CLB concentrations following the initiation of CBD, but they had improved seizure control [17]. As STP is a strong CYP2C19 inhibitor like CBD, it can be assumed that CLB and N-CLB levels were already maximally increased by STP-induced metabolic inhibition and CBD did not cause additional inhibition. In this subset of patients, reduction in seizures occurred in 80% and 50% of the cases assigned to CBD and placebo, respectively [17]. This observation may suggest that the rise in N-CLB levels is not sufficient to explain the antiseizure activity of CBD, but does not exclude the possibility of a meaningful synergic pharmacodynamic interaction between CBD and CLB. The pooled analyses of treatment estimates of primary seizure count and responders for CLB-Off patients with DS and LGS who participated in four completed RCTs also supports the presence of a CLB-independent effect of CBD [16]. The combination of data inherent to two different epileptic conditions and types of seizures may represent one limit of this approach.
Across the phase III trials, there were more treatment withdrawals for any reason and for AEs in the add-on CBD group than in the placebo arm. The overall rates of CBD discontinuation were similar to those associated with other AEDs in DS [31], and a statistically meaningful difference with placebo was observed with the highest CBD daily dose.
The most frequently reported AEs were somnolence, decreased appetite, diarrhea, and elevation in transaminases. They were mostly mild to moderate in severity, dose-related, and substantially overlapped the tolerability profile reported in patients with LGS enrolled in RCTs and in patients with severe refractory epilepsies who were administered CBD in an open-label program [32, 33]. Somnolence was the most common AE encountered with CBD and it was more likely to occur when CBD was co-administered with CLB, suggesting the need to strictly monitor CLB-On patients and adjust doses as necessary.
An increase in serum alanine or aspartate aminotransferase concentrations by ≥ 3-fold the upper limit of the normal range was reported in approximately 15% of the patients randomized to CBD and represented the main reason for treatment withdrawal [26,27,28]. The risk of hepatotoxicity was increased by concomitant treatment with VPA and elevated transaminases at baseline [26,27,28]. Although most transaminase elevations occurred within the first 30 days of use, there were also cases commencing as late as after 6 months; notably, the risk window was longer for patients taking concomitant VPA [16]. In all cases, laboratory abnormalities reversed either spontaneously during the treatment period or open-label extension trial, or after the dose of a concomitant AED—mainly VPA or CLB—was reduced, or after CBD was tapered or discontinued [26,27,28]. Slow up-titration and close monitoring of serum transaminases and signs suggestive of hepatic toxicity, above all during the initial phases of treatment and in patients concomitantly taking VPA, are recommended. Besides the hepatotoxic profile of CBD alone, additive toxicity can develop when CBD and VPA are combined. As CBD has no meaningful effects on VPA concentrations [26, 34], the nature of this interaction is thought to be mostly pharmacodynamic rather than pharmacokinetic: the interaction observed in vitro at the level of hepatic mitochondria could be the mechanism at the basis of the clinical findings [35]. The co-administration of CBD with CLB or felbamate has also been associated with slightly increased risk of transaminase elevations, which may be driven by concomitant VPA [35].
The overall better tolerability of CBD when administered at 10 mg/kg/day jointly with the efficacy profile supports the recommended starting daily dose of 5 mg/kg, the up-titration to a target maintenance dose of 10 mg/kg/day after 1 week, and the increase up to a maximum maintenance daily dosage of 20 mg/kg, in weekly increments of 2.5 mg/kg twice daily, in patients who tolerate the 10 mg/kg/day dose but require further seizure reduction.
This systematic review with meta-analysis represents a comprehensive qualitative and quantitative synthesis of all the currently available RCTs on the use of adjunctive CBD in patients with DS and provides an updated analysis of efficacy, safety, and global functioning endpoints according to drug daily dosages. Nonetheless, some shortcomings need to be considered. Only three trials met the eligibility criteria and all of them were funded by one single pharmaceutical company. The ethnic heterogeneity across the trials was low and likely to mirror the demographics on the site of recruiting centers, with more than two-thirds of the patients being Caucasian. Due to the short double-blind treatment phase of the studies, this meta-analysis cannot inform about the long-term efficacy and safety of CBD. In this respect, the interim analysis of the open-label extension of the RCTs (GWPCARE5; ClinicalTrials.gov number NCT02224573) showed that CBD in patients with treatment-resistant DS had an acceptable safety profile, which was consistent with that which emerged in the pivotal trials, and led to sustained clinically meaningful reductions in seizure frequency and improvement in the patients’ overall condition for up to 48 weeks [36]. Findings from the Expanded Access Program, which included 58 patients with DS out of 607 participants with treatment-resistant epilepsies, provided further evidence in support of the therapeutic potential of add-on CBD; the treatment was generally well tolerated and was associated with a reduction in convulsive seizure frequency of around 50% at 3 months that remained stable for 96 weeks [37]. However, additional real-world data and post-marketing surveillance will be needed to estimate the incidence of rare AEs, evaluate the occurrence of habituation and tolerance phenomena, and assess the effects of continuous CBD exposure on growth, childbearing potential, brain development, and learning.
5 Conclusion
CBD belongs to a new class of AEDs and represents the first product made directly from the cannabis plant to receive marketing authorization. Overall, adjunctive CBD was shown to be efficacious in reducing the burden of convulsive seizures in patients with DS and was associated with a higher rate of AEs than placebo, with most events being mild to moderate in intensity. Importantly, interactions with other antiseizure drugs, mainly CLB and VPA, can significantly influence the efficacy and safety profiles of CBD and should be carefully considered in everyday clinical practice. Future efforts are warranted to clarify the effect size and clinical relevance of CBD treatment independent from CLB, estimate the effectiveness of CBD in comparison with other AEDs licensed for DS, and explore whether genetic background can influence the response to therapy.
References
Fiest KM, Sauro KM, Wiebe S, Patten SB, Kwon CS, Dykeman J, Pringsheim T, Lorenzetti DL, Jetté N. Prevalence and incidence of epilepsy: a systematic review and meta-analysis of international studies. Neurology. 2017;88:296–303.
Cagnetti C, Lattanzi S, Foschi N, Provinciali L, Silvestrini M. Seizure course during pregnancy in catamenial epilepsy. Neurology. 2014;83:339–44.
Lattanzi S, Zaccara G, Giovannelli F, Grillo E, Nardone R, Silvestrini M, Trinka E, Brigo F. Antiepileptic monotherapy in newly diagnosed focal epilepsy. A network meta-analysis. Acta Neurol Scand. 2019;139:33–41.
Lattanzi S, Cagnetti C, Foschi N, Provinciali L, Silvestrini M. Lacosamide monotherapy for partial onset seizures. Seizure. 2015;27:71–4.
Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med. 2000;342:314–9.
Laxer KD, Trinka E, Hirsch LJ, Cendes F, Langfitt J, Delanty N, Resnick T, Benbadis SR. The consequences of refractory epilepsy and its treatment. Epilepsy Behav. 2014;37:59–70.
Trinka E, Bauer G, Oberaigner W, Ndayisaba JP, Seppi K, Granbichler CA. Cause-specific mortality among patients with epilepsy: results from a 30-year cohort study. Epilepsia. 2013;54:495–501.
Granbichler CA, Oberaigner W, Kuchukhidze G, Bauer G, Ndayisaba JP, Seppi K, Trinka E. Cause-specific mortality in adult epilepsy patients from Tyrol, Austria: hospital-based study. J Neurol. 2015;262:126–33.
Granbichler CA, Zimmermann G, Oberaigner W, Kuchukhidze G, Ndayisaba JP, Taylor A, Luef G, Bathke AC, Trinka E. Potential years lost and life expectancy in adults with newly diagnosed epilepsy. Epilepsia. 2017;58:1939–45.
Nabbout R, Gennaro E, Dalla Bernardina B, Dulac O, Madia F, Bertini E, Capovilla G, Chiron C, Cristofori G, Elia M, Fontana E, Gaggero R, Granata T, Guerrini R, Loi M, La Selva L, Lispi ML, Matricardi A, Romeo A, Tzolas V, Valseriati D, Veggiotti P, Vigevano F, Vallée L, Dagna Bricarelli F, Bianchi A, Zara F. Spectrum of SCN1A mutations in severe myoclonic epilepsy of infancy. Neurology. 2003;60:1961–7.
Arzimanoglou A. Dravet syndrome: from electroclinical characteristics to molecular biology. Epilepsia. 2009;50(Suppl. 8):3–9.
Dravet C, Oguni H. Dravet syndrome (severe myoclonic epilepsy in infancy). Handb Clin Neurol. 2013;111:627–33.
Devinsky O, Cilio MR, Cross H, Fernandez-Ruiz J, French J, Hill C, et al. Cannabidiol: pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders. Epilepsia. 2014;55:791–802.
Ibeas Bih C, Chen T, Nunn AV, Bazelot M, Dallas M, Whalley BJ. Molecular targets of cannabidiol in neurological disorders. Neurotherapeutics. 2015;12:699–730.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
European Medicines Agency. Assessment report: Epidiolex. International non-proprietary name: cannabidiol. https://www.ema.europa.eu/en/documents/assessment-report/epidyolex-epar-public-assessment-report_en.pdf. Accessed Oct 2019.
FDA. Drug approval package: Epidiolex (Cannabidiol), NDA 210365, FDA Center for Drug Evaluation and Research. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/210365Orig1s000TOC.cfm. Accessed Oct 2019.
Lattanzi S, Trinka E, Russo E, Striano P, Citraro R, Silvestrini M, Brigo F. Cannabidiol as adjunctive treatment of seizures associated with Lennox-Gastaut syndrome and Dravet syndrome. Drugs Today (Barc). 2019;55:177–96.
Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Higgins JPT and Green S, editors. The Cochrane Collaboration, 2011. http://handbook-5-1.cochrane.org/. Accessed Oct 2019.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
Lattanzi S, Cagnetti C, Foschi N, Provinciali L, Silvestrini M. Brivaracetam add-on for refractory focal epilepsy: a systematic review and meta-analysis. Neurology. 2016;86:1344–52.
Lattanzi S, Brigo F, Grillo E, Cagnetti C, Verrotti A, Zaccara G, Silvestrini M. Adjunctive eslicarbazepine acetate in pediatric patients with focal epilepsy: a systematic review and meta-analysis. CNS Drugs. 2018;32:189–96.
Lattanzi S, Cagnetti C, Danni M, Provinciali L, Silvestrini M. Oral and intravenous steroids for multiple sclerosis relapse: a systematic review and meta-analysis. J Neurol. 2017;264:1697–704.
Lattanzi S, Brigo F, Cagnetti C, Di Napoli M, Silvestrini M. Patent foramen ovale and cryptogenic stroke or transient ischemic attack: to close or not to close? A systematic review and meta-analysis. Cerebrovasc Dis. 2018;45:193–203.
Lattanzi S, Grillo E, Brigo F, Silvestrini M. Efficacy and safety of perampanel in Parkinson’s disease. A systematic review with meta-analysis. J Neurol. 2018;265:733–40.
Devinsky O, Patel AD, Thiele EA, Wong MH, Appleton R, Harden CL, GWPCARE1 Part A Study Group, et al. Randomized, dose-ranging safety trial of cannabidiol in Dravet syndrome. Neurology. 2018;90:e1204–11.
Devinsky O, Cross JH, Laux L, Marsh E, Miller I, Nabbout R, Cannabidiol in Dravet Syndrome Study Group, et al. Trial of cannabidiol for drug-resistant seizures in the Dravet Syndrome. N Engl J Med. 2017;376:2011–20.
ClinicalTrials.gov. GWPCARE2. A study to investigate the efficacy and safety of Cannabidiol (GWP42003-P) in children and young adults with Dravet Syndrome. https://clinicaltrials.gov/ct2/NCT02224703. Accessed Oct 2019.
Geffrey AL, Pollack SF, Bruno PL, Thiele EA. Drug–drug interaction between clobazam and cannabidiol in children with refractory epilepsy. Epilepsia. 2015;56:1246–51.
Anderson LL, Absalom NL, Abelev SV, Low IK, Doohan PT, Martin LJ, Chebib M, McGregor IS, Arnold JC. Coadministered cannabidiol and clobazam: preclinical evidence for both pharmacodynamic and pharmacokinetic interactions. Epilepsia. 2019;60:2224–34.
Wallace A, Wirrell E, Kenney-Jung DL. Pharmacotherapy for Dravet Syndrome. Paediatr Drugs. 2016;18:197–208.
Lattanzi S, Brigo F, Cagnetti C, Trinka E, Silvestrini M. Efficacy and safety of adjunctive cannabidiol in patients with Lennox-Gastaut syndrome: a systematic review and meta-analysis. CNS Drugs. 2018;32:905–16.
Devinsky O, Marsh E, Friedman D, Thiele E, Laux L, Sullivan J, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15:270–8.
Morrison G, Crockett J, Blakey G, Sommerville K. A phase 1, open-label, pharmacokinetic trial to investigate possible drug–drug interactions between clobazam, stiripentol, or valproate and cannabidiol in healthy subjects. Clin Pharmacol Drug Dev. 2019;8:1009–31.
Lattanzi S, Brigo F, Trinka E, Zaccara G, Cagnetti C, Del Giovane C, Silvestrini M. Efficacy and safety of cannabidiol in epilepsy: a systematic review and meta-analysis. Drugs. 2018;78:1791–804.
Devinsky O, Nabbout R, Miller I, Laux L, Zolnowska M, Wright S, Roberts C. Long-term cannabidiol treatment in patients with Dravet syndrome: an open-label extension trial. Epilepsia. 2019;60:294–302.
Szaflarski JP, Bebin EM, Comi AM, Patel AD, Joshi C, Checketts D, CBD EAP Study Group, et al. Long-term safety and treatment effects of cannabidiol in children and adults with treatment resistant epilepsies: expanded access program results. Epilepsia. 2018;59:1540–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding has been received for the conduct of this study.
Conflict of interest
Simona Lattanzi, Cinzia Del Giovane and Mauro Silvestrini have no conflicts of interest directly relevant to the content of this study. Francesco Brigo acted as a consultant for Eisai. Eugen Trinka has received speaker’s honoraria from UCB, Biogen, Gerot-Lannach, Bial, Eisai, Takeda, Newbridge, Sunovion Pharmaceuticals Inc., LivaNova and Novartis; consultancy funds from UCB, Biogen, Gerot-Lannach, Bial, Eisai, Takeda, Newbridge, GW Pharmaceuticals, Sunovion Pharmaceuticals Inc., and Novartis; directorship funds from Neuroconsult GmbH. E. Trinka’s Institution received grants from Biogen, Red Bull, Merck, UCB, European Union, FWF Österreichischer Fond zur Wissenschaftsförderung, and Bundesministerium für Wissenschaft und Forschung. Gaetano Zaccara has received speaker’s or consultancy fees from Eisai, Sanofi-Aventis, and UCB Pharma. Pasquale Striano has received speaker fees and participated at advisory boards for Biomarin, Zogenyx and GW Pharmaceuticals, and received research funding by ENECTA srl, GW Pharmaceuticals, Kolfarma srl. and Eisai.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lattanzi, S., Brigo, F., Trinka, E. et al. Adjunctive Cannabidiol in Patients with Dravet Syndrome: A Systematic Review and Meta-Analysis of Efficacy and Safety. CNS Drugs 34, 229–241 (2020). https://doi.org/10.1007/s40263-020-00708-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40263-020-00708-6