
Abstract
Study Objective
Assessment of safety and feasibility of total laparoscopic hysterectomy in a high-volume tertiary care centre.
Design
Retrospective study design.
Setting
Tertiary care centre: Galaxy care Hospital, Pune, India.
Materials and Methods
This is a retrospective observational study conducted in a tertiary care resident training hospital in Pune which is a high-volume teaching hospital. 1200 total laparoscopic hysterectomy patients between July 2013 and June 2019 operated by a group of trained surgeons were analysed, and parameters, namely demography, indication of surgery, surgical time, intra-operative blood loss, post-operative complications, duration of hospital stay, discharge and follow-up, were studied.
Result(s)
A total of 1200 women who underwent total laparoscopic hysterectomy for various indications were included in the study. TLH was successfully performed in all women. Mean age of women was 45 years. 72.00% had a BMI between 18.5 and 24.9, 16.08% had a BMI between 25 and 29.9, 3.92% had a BMI of > 29.9 while 8% had a BMI < 18.5. Indications for surgery included uterine fibroid (33.08%), adenomyosis (22.25%), endometrial hyperplasia (14.33%), endometrial polyp (7%), endometriosis (3.33%), postmenopausal bleeding (9.25%), chronic PID (5.25%), prolapse (4.25%) and risk reduction surgery in 1.25%. 2.00% had intra-operative complications while 7.58% had post-operative complications which were identified and managed successfully.
Conclusion(s)
Advances and innovation in equipment, energy sources and surgical training have made TLH a well-tolerated and efficient surgery. Irrespective of the previous morbidity, pathology and uterine size, TLH is a duplicable and safe in a well-trained high-volume centre.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hysterectomy is one of the most common surgical procedures performed on women all over the world. The incidence of hysterectomy in India is about 4–6%; ninety percent of these are performed for benign indications [1].
Route of hysterectomy was earlier based on the size and mobility of the uterus, patient’s body mass index (BMI), past history of abdominal surgery, nulliparity, age and a history of a complex disease [2].
Hysterectomy may be done through an abdominal, laparoscopic, vaginal or robot-assisted approach. However, there are controversies related to the optimal route of surgery [3].
Optimal route of hysterectomy always remains a matter of discussion till date [4].
Studies prove that laparoscopic hysterectomy is associated with shorter hospital stay and faster recovery than abdominal route of hysterectomy [5].
Laparoscopic hysterectomy has made way for several modifications including laparoscopic-assisted vaginal hysterectomy (LAVH), laparoscopic-assisted supracervical hysterectomy (LSCH) and total laparoscopic hysterectomy (TLH) [6].
Laparoscopic hysterectomy (LH) includes laparoscopic ligation of the major vessels supplying the uterus by electrosurgery desiccation, suture ligature, or staples [7].
In 1989, Dr. Harry Reich described first total laparoscopic hysterectomy using bipolar desiccation and published the same [8].
However, even after 20 years of its inception, unavailability of training and volumes deters many surgeons from venturing into laparoscopy.
Fear of complications, namely bowel or ureteric injuries coupled with inadequate training in minimal access surgery, often leads to some patients still being subjected to open surgery even at high-volume centres.
Laparoscopic hysterectomy is technically demanding and a surgery still performed infrequently by many gynaecologists.
Indications for a hysterectomy are usually not life-threatening but cause discomfort and inconvenience; hence, most women who undergo this surgery do so in order to improve their quality of life. Thus, minimally invasive techniques are sought for this procedure [9].
Laparoscopic hysterectomy offers several advantages over abdominal and vaginal hysterectomy which include shorter recovery times, lower blood loss, early return to daily activity and decreased infectious morbidity [2].
One of the most important surgeon and system characteristics is surgical volume [2].
Depth and advances in gynaecological surgery are rising owing to surgical innovation and increasing inclination towards minimally invasive surgical approaches.
Outcome of surgical procedures is influenced by patient characteristics, operating surgeon and management at the hospital [10].
Data suggest that patients treated by high-volume surgeons and in high-volume centres have superior outcomes compared to those operated on by lower-volume surgeons [11].
Sparsity of data analysing large case volumes and outcomes of laparoscopic hysterectomy has led to this study aimed at analysing the safety of total laparoscopic hysterectomy in a high-volume tertiary care centre.
Materials and Methods
A retrospective evaluation was done, of all patients (n = 1200) who underwent TLH for benign uterine pathologies from July 2013 to June 2019 at the Galaxy Laparoscopy Institute, Pune, India.
All surgeries were performed by a group of surgeons who were given structured training with standardized replicable steps.
Pre-operative Workup
Patients were evaluated with relevant pre-operative work up, and anaesthesia risks were assessed.
Pre-operative preparation included a written informed consent, counselling of the patient.
Single dose of intravenous antibiotic was given before the surgery.
Bowel preparation was done one night prior to surgery.
Patient’s Position
Patient was placed in modified Lloyd-Davis position with a bolster under the buttocks at the level of the anterior superior iliac spine (Fig. 1a).

a Patient position. b Port position
A surgical glove filled with a sterile pad was inserted into the vagina to avoid the leakage of the abdominal CO2 following colpotomy.
We used the technique of introducing Visi-port parallel to the Veress needle which was introduced at the Palmer’s point (area in the left upper quadrant 3 cm below the costal margin in the mid-clavicular line) in all the cases.
Primary port insertion was done under vision by accessing the umbilical tube and was supra-umbilical/infra-umbilical depending on the uterine size (Fig. 1b).
Procedure of Operation
The Veress needle was inserted at the Palmer’s point.
After CO2 insufflation, a 5-mm trocar (Xcel visiport) was inserted in the left upper quadrant lateral to the Veress needle.
A 5-mm telescope was introduced through this port, and the uterus with the adnexa was evaluated.
The 10-mm port was inserted under vision at the infra-umbilical site or higher depending on the size of the uterus and used as camera port followed by three 5 mm accessory ports as shown.
After inserting a 10 mm ‘0’ degree telescope, the pelvis and upper abdomen were evaluated thoroughly. Uterine manipulation was done using a myoma screw.
The right round ligament, ovarian ligament and the fallopian tube were coagulated and cut. The anterior leaf of the broad ligament was opened and an anterior ‘U’ incision taken through the utero-vesical fold. The urinary bladder was dissected over the cervix by sharp and blunt dissection.
Following uterine retraction to the right, the left tube and ligament complex were cut and the anterior U cut completed.
The posterior peritoneum behind the uterine vessels was kept intact at this stage. The left hand working forceps was placed at the level of the uterosacral ligaments to lift the cervix anteriorly and away from the sigmoid colon. The left uterine vessels were identified, coagulated and cut.
The clamps were then applied parallel to the cervix and medial to the uterine artery.
Similar dissection was done on the right side. Under continuous traction on the uterus, posterior peritoneum and parametrial tissue on the lateral aspect of the cervix was coagulated and cut ensuring dissection was always above the level of the uterosacral attachment.
Parametrial tissue at the vaginal angle was gradually separated with coagulation, and colpotomy was performed from the right vaginal angle towards the left, always staying very close to the cervix, as if the cervix was circumcised off its uppermost vaginal attachment.
Oophorectomy when indicated was performed at this stage by coagulating and cutting the infundibulo-pelvic ligaments and the specimen was removed per vaginum.
When necessary, a manual morcellation was carried out vaginally (circular wedge resection of the uterus by scalpel).
Sometimes when the uterus was large, it was morcellated and removed through the right lower 10 mm port.
The vagina was sutured by ipsilateral suturing with 2–0 vicryl continuous locking intra-corporeal suturing technique. Bowel and bladder was checked after every surgery.
Energy Sources
Majority of the time, TLH was performed with bipolar cautery and scissors. But we have also used a combination of bipolar, Ligasure and the Harmonic scalpel. We did not use monopolar current. The technique remained the same irrespective of the energy source used.
In patients having large myomas and endometriosis, identification and dissection of the ureters were undertaken as the first step.
During difficult posterior dissection, the dictum followed was that ‘fat always belongs to the rectum’, and so dissection was kept anterior to the fat and during bladder dissection, the rule followed was that ‘fat always belongs to the bladder’, and dissection was done posterior to this fat.
Catheter was removed after 6 h, and liquids were started few hours after the surgery.
The patient was discharged in the next 3 days depending upon the post-operative course and was called for follow-up after 7 days.
Results
A total of 1200 women undergoing total laparoscopic hysterectomy for various indications were included in the study. TLH was successfully performed in all women. Mean age of women was 45 years (Table 1).
72.00% (n = 864) had a BMI between 18.5 and 24.9, 16.08% (n = 193) had a BMI between 25 and 29.9, 3.92% (n = 47) had a BMI of > 29.9 and 8% (n = 96) had a BMI of < 18.5.
Majority (n = 721)) of women undergoing TLH had a uterine size of 12–16 weeks. Maximum size of uterus operated upon was 20–24 weeks (n = 9) (Fig. 2).

Hysterectomy and size of uterus
Indications for surgery were uterine fibroid (33.08%), adenomyosis (22.25%), endometrial hyperplasia (14.33%), endometrial polyp (7%), endometriosis (3.33%), postmenopausal bleeding (9.25%), chronic PID (5.25%), prolapse (4.24%) and risk reduction surgery in 1.25% (Table 2).
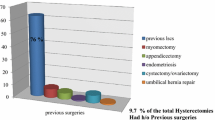
22% (n = 264) had undergone at least one surgery. Of these, 75.38% (n = 199) had undergone LSCS, 14.39% (n = 38) had undergone myomectomy, 4.17% (n = 11) had undergone cystectomy/oophorectomy, 3.41% (n = 9) had undergone surgery for endometriosis and 2.65% (n = 7) had undergone appendicectomy (Fig. 3).

Hysterectomies in patients with previous surgeries
58.5% had a blood loss of < 50 ml (n = 702), blood loss was 51–100 ml in 41.17% (n = 494) and 101–150 ml in 0.33% (n = 4).
58.3% (n = 700) of the patients were allowed orals 6 h following surgery, 31.92% (n = 383) on POD 1, 8% (n = 96) on the 2nd post-operative day and 1.75% (n = 21) on the 3rd post-operative day.
47.92% (n = 575) were discharged on the first post-operative day, 40.08% (n = 481) were discharged on the 2nd post-operative day, 9.25% (n = 111) on the 3rd post-operative day and 2.75% (n = 33) had a hospital stay of more than 3 days (Table 3).
88.25% of surgeries were completed within 60 min (n = 1059). Among these, 31.92% were done for the indication of fibroid (n = 383). Endometriosis was the indication in 3.33% (n = 40) of surgeries which were done in 91–120 min (Fig. 4).

Surgical time for TLH for various indications
1.5% (n = 18) with dense bladder adhesions had bladder injury which was detected intra-operatively and sutured laparoscopically. Among these, 61.1% (n = 11) had undergone previous LSCS, 16.67% (n = 3) had a myomectomy, 5.56% (n = 1) had an appendicectomy and 16.67% (n = 3) had endometriosis previously. TLH was done for multiple uterine fibroids in 77.78% (n = 14), adenomyosis in 5.56% (n = 1) and grade IV endometriosis in 16.67% (n = 3). Urinary catheter was kept for two to three weeks and woman recovered uneventfully.
0.5% (n = 6) with ureteric adhesions had a serosal ureteric tear for which bilateral stenting was done and urinary catheter was kept for a week and women recovered uneventfully. Of these, 66.67% (n = 4) had undergone LSCS and adhesiolysis for endometriosis previously and was undergoing TLH for endometriosis. Surgical time was 91–120 min. 33.33% (n = 2) had undergone cystectomy previously and chronic PID was the indication. Surgical time was 61–90 min (Table 4).
None of the patients had post-operative haemorrhage. Thirty-four women developed reactionary fever which was managed with antipyretics.
Nine women developed paralytic ileus, and seven women had urinary retention which was managed conservatively.
Eight women had minimal pelvic collection which was drained under ultra-sonographic guidance and all of them recovered uneventfully.
Eighteen women had urinary tract infection and fifteen developed port site infection which was managed with antibiotics and alternate day dressing for a week (port site infection) (Table 4).
Discussion
After 20 years of the first total laparoscopic hysterectomy performed by Harvey Reich, efforts to improve the technique and outcomes, reducing iatrogenic injuries, intra-operative blood loss, hospitalization time, and recovery time have been made [12].
Consensus among researchers at present has shown that this procedure is a safe procedure and is preferred to be the first line of treatment for hysterectomy in many countries [13].
According to a study done by Garry et al. [14], surgeons needed to perform 25 cases to complete the learning curve and gain adequate experience.
In our study, all the surgeries were done using the same technique which has remained the same in the past 10 years which makes it easy for everybody to duplicate the same.
The average surgical time was less than 60 min in 88.25% patients and 58.5% (n = 702) had a blood loss of less than 50 ml in our study.
The operative time in a study by Bettaiah et al. [15] ranged from a minimum of 20 min to a maximum of 2 h.
None of our patients required blood transfusion.
According to a study by Vree F et al. the impact of surgical volume on peri-operative outcomes, surgeries performed by high-volume surgeons required a shorter operative time (155.11 min vs 199.19–203.35) and resulted in less estimated blood loss compared with low and intermediate volume surgeons (161.09 mL vs 205.58–237.96 mL) 11].
Terzi et al. reported that significant reduction in operating time was achieved after the first 75 cases which was an important parameter for junior surgeons [9].
Wattiez et al. [16] did an analysis of 1647 cases between 1989–1995 and 1996–1999 which concluded that TLH appears to be safe and effective which can be achieved despite post-inflammatory disorders, previous surgery and adhesions which was similar to our study.
Intra-operative complications noted were bladder injury (1.5%) and ureteric injury (0.5%). They were recognized intra-operatively and managed accordingly.
No conversion to laparotomy was needed.
Study by Bettaiah [15] reported conversion to laparotomy rate to be 0.93%.
Standardization of steps, pre-operative as well as post-operative checklists, high surgical volumes and a disciplined uniform approach were the sole factors which influenced the conversion rate in our study.
Wallenstein et al. [2] concluded that laparoscopic hysterectomies performed by surgeons at high-volume centres and high-volume hospitals were associated with a reduction in the morbidity.
Among our post-operative complications, 2.83% developed reactionary fever. Urinary retention and paralytic ileus were seen in 0.58% and 0.75%, respectively, and were managed conservatively. In 0.67% patients, pelvic collection was noted. Port site infection and urinary tract infection were seen in 1.25% and 1.5%, respectively, and managed.
None of the cases needed re-exploration.
Vaginal cuff suturing for all our cases was done by intra-corporeal continuous interlocking technique, and none of the patients had vaginal dehiscence following the surgery.
Main reasons we feel are that all the TLH were intra-fascial hysterectomies.
Use of cold scissors for colpotomy and full thickness vaginal vault suturing are additional factors.
According to Smith et al. [17] studies that compared vaginal dehiscence with different suturing techniques as well as suture materials did not find any significant difference between the groups.
Hysterectomy being one of the most common surgeries performed among women, one of the attempts to decrease risks associated with this procedure to impact public health may include optimizing referral to surgeons with appropriate experience and volumes of major gynaecologic cases [11].
However, long learning curve, fear of iatrogenic injuries and unavailability of systematic training are roadblocks yet to be conquered.
With improvement of surgical skills, it is being considered as a day care surgery [12].
Strengths of our study included a large sample size, retrospective study design, evaluation of patients from different age groups and decreased selection.
Our study had a few limitations namely; the study was conducted in a single centre which might not reflect the overall results among various centres of India.
Additionally, the data were obtained from clinical records and as such were dependent on clear and complete information.
Conclusion
Advances in equipment, surgical techniques and training have made TLH a well-tolerated and efficient surgery.
Standardized surgical protocols and high case volumes are the cornerstone of safe surgery.
Thus, we conclude that irrespective of the previous morbidity, pathology and uterine size, TLH is duplicable and safe in a well-trained high-volume centre.
Abbreviations
- TLH:
-
Total laparoscopic hysterectomy
- BMI:
-
Body mass index
- LSCS:
-
Lower segment caesarean section
- LH:
-
Laparoscopic hysterectomy
- LAVH:
-
Laparoscopic-assisted vaginal hysterectomy
- CO2:
-
Carbon dioxide
- POD:
-
Post-operative day
- LSCH:
-
Laparoscopic-assisted supracervical hysterectomy
- LH:
-
Laparoscopic hysterectomy
- N:
-
Number
- PID:
-
Pelvic inflammatory disease
- Fig:
-
Figure
References
Ajjammanavar V, et al. Outcome of total laparoscopic hysterectomy in relation to the size of the uterus. Int J Reprod Contracept Obstet Gynecol. 2009;8(1):74–8.
Wallenstein M, Ananth CV, Kim J. Effect of surgical volume on outcomes for laparoscopic hysterectomy for benign indications. Obstet Gynecol. 2012;119:709–16.
Kreuninger JA, Cohen SL, Meurs E, et al. Trends in readmission rate by route of hysterectomy—a single-center experience. Acta Obstet Gynecol Scand. 2018;97:285–93.
Pattanaik T, Mishra SP, Das S. Total laparoscopic hysterectomy—a retrospective observational study in a teaching hospital. Ann Int Med Den Res. 2017;3(1):OG10–3.
David-Montefiore E, Rouzier R, Chapron C. Surgical routes and complications of hysterectomy for benign disorders: a prospective observational study in French university hospitals. Hum Reprod. 2007;22(1):260–5.
Puntambekar SP, Wagh GN, Puntambekar SS, et al. A novel technique of total laparoscopic hysterectomy for routine use: evaluation of 140 cases. Int J Biomed Sci. 2008;4(1):38–43.
Sinha R, Sundaram M, Lakhotia S, et al. Total laparoscopic hysterectomy for large uterus. J Gynecol Endosc Surg. 2009;1(1):34–9.
Shrirame DV, Malkar V, Modi R. Study of efficacy and safety of bipolar coagulation in total laparoscopic hysterectomy. Int J Med Res Rev. 2017;5(07):748–52.
Terzi H, Hasdemir P, Biler A. Evaluation of the surgical outcome and complications of total laparoscopic hysterectomy in patients with enlarged uteruses. Int J Surg. 2016;36:90–5.
Mikhail E, Scott L, Miladinovic B, et al. Association between fellowship training, surgical volume, and laparoscopic suturing techniques among members of the American Association of Gynecologic Laparoscopists. Minim Invasive Surg. 2016;2016:1–6.
Vree F, Cohen S, Chavan N, et al. The impact of surgeon volume on perioperative outcomes in hysterectomy. JSLS. 2014;18:174–81.
Nagar O, Sharma A, Shankar V. A comparative study of total laparoscopic hysterectomy and non-descent vaginal hysterectomy for treatment of benign diseases of uterus. Int J Clin Obstet Gynaecol. 2018;2(4):63–8.
Llarena N, Shah A, Milad M. Bowel injury in gynecologic laparoscopy. Am Coll Obstet Gynecol. 2015;125(6):1407–17.
Garry R, Fountain J, Mason S, et al. The eVALuate study: two parallel randomized trials, one comparing laparoscopic with abdominal hysterectomy, the other comparing laparoscopic with vaginal hysterectomy. BMJ. 2004;7(328):1–7.
Bettaiah R, Reddy C, Anantha R. Laparoscopic hysterectomies: our 10 years’ experience in a single laparoscopic center. J Obstet Gynecol India. 2016;66(4):274–81.
Wattiez A, Soriano D, Cohen SB, et al. The learning curve of total laparoscopic hysterectomy: comparative analysis of 1647 cases. Am Assoc Gynecol Laparosc. 2002;9(3):339–45.
Smith K, Caceres A. Vaginal cuff closure in minimally invasive hysterectomy: a review of training, techniques, and materials. Cureus. 2017;9(10):e1766. https://doi.org/10.7759/cureus.1766.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest and nothing to disclose.
Ethical Approval
The study was approved by the Institutional Ethics Committee.
Informed Consent
Informed consent was taken from all human participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Shailesh Puntambekar, MD at Galaxy Care Multispeciality Hospital, Pune, Above Ayurved Rasashala, 25-A, Karve Road, Pune, Maharashtra, India. Theertha S Shetty, MS at Galaxy Care Multispeciality Hospital, Pune, Above Ayurved Rasashala, 25-A, Karve Road, Pune, Maharashtra, India. Arjun Goel, MS at Galaxy Care Multispeciality Hospital, Pune, Above Ayurved Rasashala, 25-A, Karve Road, Pune, Maharashtra, India. Shruti Chandak, MS at Galaxy Care Multispeciality Hospital, Pune, Above Ayurved Rasashala, 25-A, Karve Road, Pune, Maharashtra, India. Shakti Panchal, DGO at Galaxy Care Multispeciality Hospital, Pune, Above Ayurved Rasashala, 25-A, Karve Road, Pune, Maharashtra, India.
Rights and permissions
About this article

Cite this article
Puntambekar, S., Shetty, T.S., Goel, A. et al. Single-Centre Experience of Doing Safe Total Laparoscopic Hysterectomy: Retrospective Analysis of 1200 Cases. J Obstet Gynecol India 70, 376–383 (2020). https://doi.org/10.1007/s13224-020-01333-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-020-01333-5