
Abstract
Objectives
Technology is increasingly being used to help practise mindfulness. Immersive virtual reality-enhanced mindfulness may prove especially effective for a wide range of clinical interventions where traditional mindfulness is currently proving valuable. The current paper provides a preliminary survey of research on this topic, aimed at verifying scientific evidence that VR technology improves the practice of mindfulness and its therapeutic effectiveness. A recognition on emerging technological solutions aimed at improving decentering and interoceptive awareness (IA) in mindfulness interventions is also proposed.
Methods
A systematic search was performed in ACM, Science Direct, Web of Science, Scopus, IEEE Xplore, and PubMed, using the following keywords: “mindfulness” AND “virtual reality”. Quality Assessment Tool for Quantitative Studies (QATQS) was used to assess study quality.
Results
Fifty-three papers were considered in the review involving 1652 subjects. Pain, stress, depression, anxiety, borderline personality disorder, and addictions are the addressed clinical cases. The quality analysis did not reveal any strong quality papers and over 90% were rated as weak. According to the majority of the studies, VR guarantees increasing relaxation self-efficacy, reducing mind wandering, and preserving attention resources. Interoceptive awareness and decentering are both overlooked in the literature.
Conclusions
VR exhibits potential favourable features to support mindfulness practice, especially immersive and multisensory VR. The use of bio/neurofeedback sensors allows an adaptive experience in real time. A design proposal for upcoming trends in VR-supported mindfulness was presented and the need for more rigorous, randomised controlled studies in the future was highlighted.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
In the last decade, mindfulness training has been supported by Information and Communication Technology (ICT) solutions and scientific literature has been dealing with this trend. Among the technologies, virtual reality (VR) (in particular immersive VR) exhibits particularly favourable features to improve mindfulness practice. VR is defined as a real or imaginary 3D environment simulated on the computer that allows users to experience the sensation of being present in a different physical place (Sanchez-Vives and Slater, 2005).
Immersion is the system’s capability to adequately stimulate all human perceptual channels (sensory, vestibular, proprioceptive, and interoceptive). The level of immersion offered by the VR system depends on the extension of the perceptual domains involved (multisensory integration) and on the accuracy, resolution, and reactivity in production of stimuli (Bohil et al., 2011). The psychological product of immersion is the sense of presence. The user is partially or totally unaware of the mediating role played by technology (Gorini et al., 2011). The user experiences the sensation of “being there” in the virtual space (Bowman & McMahan, 2007).
According to the predictive coding theory, the human brain, while interacting with the world, systematically makes predictions about what will happen next (Clark, 2013). The brain constantly generates an “embodied simulation”, considering both exteroceptive (sensory) and inner (interoceptive, proprioceptive, and vestibular) stimuli. Moseley et al. (2012) postulated the existence of a body matrix, as a multi-perceptive representation of the body and the surrounding space.
Immersive virtual reality shares the same basic mechanism with the brain: it is based on a model of the body and the environment, and their interaction. This model supports the prediction of the perceptive consequences of these interactions. Furthermore, VR generates the multisensory stimuli congruent with the predictions of the model. In this perspective, the sense of presence is the result of simulation coherent with the body matrix performed by the technology. The higher the fidelity of this simulation, the greater the level of presence (Riva et al., 2019).
According to Hölzel et al. (2011), mindfulness works according to a combination of fundamental mechanisms including body awareness and decentering (Fresco et al., 2007). Regarding body awareness, mindfulness pursues the balanced improvement of the interoception: the capacity of receiving, accessing, and appraising internal bodily signals (Farb et al., 2015). In this way, for example, mindfulness prevents and treats dysfunctional forms of interoceptive awareness (IA) underlying chronic pain, anxiety, and disordered eating (Hanley et al., 2017). Regarding decentering, mindfulness fosters the overcoming of the impression that the self is a constant and immutable entity. Therefore, it leads the subject to identify with the phenomenon of “experiencing” itself rather than with a static self (Hölzel et al., 2011). This decentering process is a key factor of the non-judgmental awareness.
Immersive VR proposes experiences not only at an exteroceptive level, but also at an interoceptive one, by means of neuro/biofeedback. Interoceptive feedback can be mapped onto a sensory channel (e.g., acoustic, visual), by conveying symbolically internal information (e.g., heartbeat and hunger stimulus). On the other hand, the feedback can also be returned directly as a physiological stimulus, through suitable acoustic and vibrotactile actuators (Riva et al., 2017). VR can correct dysfunctional representations of the body by determining a controlled mismatch between the model predicted by the brain (body matrix) and the actual stimuli offered to the user (Riva et al., 2017). In this way, immersive VR actually promotes an alteration of the body matrix. In particular, it contributes to build a new vision of oneself (decentering), by generating the sensation of a presence in a virtual body and in the digital space around it, and by introducing an experience that alters previous perceptions (Riva et al., 2019).
The isolation of the participant from external distractors is a further enhancement provided by VR to mindfulness training. Focusing and keeping a continuous attention on a certain object are a challenging skill to achieve, especially for novices (Lutz et al., 2008). VR (in particular immersive VR) transports the practitioner to a new scenario without distracting stimuli (Costa et al., 2019).
VR allows the practitioner to experience multisensory contacts with natural environments without leaving home: the more the user feels “away from the spaces of everyday stress”, the deeper the meditation (Costa et al., 2019). According to attention restoration theory (ART), the immersion in natural environments can lead to a rehabilitation of attentional resources often exhausted due to stress (Kaplan, 1995). Also, the possibility of personalising environments offered by VR can improve mindfulness: satisfying user preferences in terms of attentional anchors can improve engagement and adherence to the mindfulness practice. Indeed, as discussed by Anderson and Farb (2018), individuals have personal preferences about the most suitable stimulus to capture their attention. Finally, a sense of community can be fostered by the presence of social interactions between users, facilitating feelings of unity (Sliwinski et al., 2017). Networked and multi-user VR sessions allow for the sharing of mindfulness experiences without limits of spatial distance.
In the therapeutic field, there is growing evidence of the effectiveness of VR exposure therapy (VRET) for the treatment of phobias, anxiety disorders and post-traumatic stress disorder (Garcia-Palacios et al., 2002), and specifically in the field of cognitive rehabilitation, also taking advantage of serious games (Barba et al., 2019; Nunnari et al., 2019). In the case of virtual mindfulness, the idea is to minimise the likelihood that the mind wanders in the form of distracting thoughts. Although immersive VR applied to mindfulness skills training is not yet well documented, some studies explored its potential, showing encouraging results (Chandrasiri et al., 2020; Flores et al., 2018; Gomez et al., 2017; Navarro-Haro et al., 2016, 2017). The use of bio- and neurofeedback may have remarkable results to support mindfulness practice. Moreover, the multisensory feedback can be returned in real time by means of a gradual evolution of the virtual environment, taking advantage of gamification dynamics (Choo & May, 2014).
More than 10 years after the first research, a survey on studies concerning VR-supported mindfulness was never carried out. Some reviews focused on mindfulness supported by interactive technologies. However, in Sliwinski et al. (2017), virtual reality is not covered in an exhaustive way (only 5 papers). In other recent reviews (Choo & Burton, 2018; Lyzwinski et al., 2018; Plaza et al., 2013), only mobile app-based solutions were considered. There are also many surveys reviewing whether VR is an effective tool in clinical application (Lindner et al., 2019; Stănică et al., 2016), but none specifically concerning mindfulness. Furthermore, a framework-background is needed in order to position new studies on VR-supported mindfulness evaluating the scientific relevance more appropriately (Kitchenham, 2004).
The research questions of this review are as follows: Is there scientific evidence that VR technology improves the practice of mindfulness? Is there scientific evidence that VR technology improves the therapeutic effectiveness of mindfulness? Are there any experimental studies focusing on the specific support given by VR to mindfulness in order to increase interoceptive awareness and decentering? Are there innovative design solutions emerging in the VR-supported mindfulness field and, if so, for what specific purposes?
Method
Search Strategy
This study implemented the guidelines for systematic literature reviews presented by Kitchenham (2004), also following PRISMA recommendations to ensure a transparent and complete reporting of the paper extraction process (Moher et al., 2011). A literature search was performed covering the period between January 2010 and January 2021, by using the following databases: Association of Computing Machinery (ACM), Science Direct, Web of Science, Scopus, IEEE (Institute of Electrical and Electronics Engineers) Xplore, and PubMed.
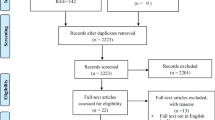
The following search terms were used in combination for the research in all the databases considering titles and abstracts: (VR OR Virtual Reality) AND Mindfulness. In Fig. 1, the PRISMA flow diagram of VR-supported mindfulness systematic review process is depicted. In the Identification phase, we searched the databases by applying the search terms. Regarding the eligibility criteria, the papers had to be peer-reviewed, published in journals/conference proceedings, and written in English. Then, the screening process was carried out, by combining the results of each sources and excluding all the duplicates. Manual screening based on titles and abstracts was performed in order to eliminate papers according to further eligibility criteria. Specifically, papers were excluded if the word mindfulness was merely used as a reference to a dispositional state or trait (i.e. awareness) rather than a meditation protocol/technique. In the final step (eligibility phase), all the survived full-text papers (a) focused not specifically on mindfulness meditation or (b) that proposed non-immersive VR solutions (i.e. not based on 3D computer graphics and first-person perspective (Gorisse et al., 2017)) were kept out. All papers that passed this last phase were included in the review analysis in order to answer the research questions.

PRISMA flow diagram (Moher et al., 2011) of VR-supported mindfulness systematic review process
Quality Assessment Strategy
A quality assessment was realised on the collected papers. First of all, the papers were clustered according to their goals. The labels for the clusters were borrowed from the Food and Drug Administration Guidance Document concerning the early feasibility study for Medical Devices (U.S. Food and Drug Administration, 2013). The Design and Prototyping studies (DS) focus on the innovation of their proposal and are not oriented to its experimental validation. The Early Feasibility studies (EFS) are interested in testing how the technological solution is safe, ergonomic, and user-friendly. The Feasibility studies (FS) experimentally validate the outputs of a VR-supported mindfulness sessions in terms of improvement in the therapy application (for example in terms of therapy adherence). For these studies, the clinical context is not strictly necessary. The Pivotal studies (PS) are focused on the assessment of a VR-supported mindfulness therapy outcomes. Therefore, they define a therapeutic need, and experimentally measure the effectiveness of the interventions in the medium and long term.
All the collected papers, excluding those belonging to the Design and Prototyping cluster, were classified according to Quality Assessment Tool for Quantitative Studies (QATQS) (Thomas et al., 2008). Even though Early Feasibility and Feasibility studies do not concern clinical trials, they were included in the quality assessment because they are all based on experimental campaigns. The papers were evaluated according to the six components of the QATQS: (1) selection bias, (2) study design, (3) confounders, (4) blinding, (5) data collection methods, and (6) withdrawal and drop outs. As proposed in Kriakous et al. (2021), each component was rated on a quality score of 1 to 3. The papers were labelled according to their overall score based on the following criteria: if no component obtained a score of 3, the paper is labelled as strong; if only one component has a score of 3, the paper is labelled as a medium; if at least two components have a score of 3, the papers are labelled as weak.
Firstly, the evaluation was implemented by the second author, by following the QATQS protocol guidelines. Then, the fourth author independently evaluated the papers for the second time. Finally, in case of disagreement, all authors were involved to discuss further and seek convergence. A QATQS dictionary was used to keep standardised and homogeneous results. Following further discussion, the authors did not note any deviations in the interpretation of the results.
Results
The search conducted through ACM Digital Library, Science Direct, Web of Science, Scopus, IEEE Xplore, and PubMed revealed one hundred and fifty-eight papers duplicates excluded. During the abstract screening, sixty papers were excluded because they did not meet the inclusion criteria. Forty-seven more studies were excluded after the full-text screening. For each paper passed through the eligibility phase, the included references were analysed. This led to include three additional relevant documents not returned in the initial search. Overall, fifty-three papers concerning VR-supported mindfulness solutions were included in the review analysis. The paper distribution per year is reported in Fig. 2.

Number of papers per years on VR-supported mindfulness published since 2007
No strong paper resulted from the quality analysis. Furthermore, only three studies reached the medium level (Goldenhersch et al., 2020; Igna et al., 2014; Navarro-Haro et al., 2019). All the others (more than 90%) were classified as weak (Table 1). The QATQS component most impacting on the bad quality performances was the blinding. Except for one, not all papers implemented a blinding strategy. The only exception is Tinga et al. (2019), where the sources of the biofeedback were randomly connected to the patient body or to a signal generator. As regards the types of clinical studies, the percentages of their occurrences are reported in Table 1. Only 27% of the experimental studies used a control group: nine Randomised Control Studies (RCS), and two Control Clinical Studies (CCS). The remaining 63% adopted a before-after strategy in twenty-nine cases, and an after-only strategy in three cases (see Table 1). In Fig. 3, the occurrences of Clinical study types and relative quality levels are reported. The median value of the experimental samples is 23. Even when the number of participants is higher the number of experimental sessions often appears to be limited. The collected clinical use cases are (Fig. 4) chronic and acute pain (Botella et al., 2013; Darnall et al., 2020; Garrett et al., 2017; Gromala et al., 2011, 2015; Haisley et al., 2020; Louw et al., 2019; Tong et al., 2016), stress syndromes (Botella et al., 2013; Chavez et al., 2020; Costa et al., 2018; Flores et al., 2018; Gomez et al., 2017), depression (Botella et al., 2013; Flores et al., 2018), anxiety (Botella et al., 2013; Chavez et al., 2020; Flores et al., 2018; Gomez et al., 2017; Navarro-Haro et al., 2019; Seol et al., 2017; Tarrant et al., 2018), borderline personality disorder (Navarro-Haro et al., 2016), and substance dependence (Chen et al., 2018; Goldenhersch et al., 2020).

Occurrences of Clinical study types and relative quality levels. Weak = red, medium = yellow

Papers on VR-supported mindfulness: numbers with respect to clinical use cases
Table 2 presents the collected fifty-three papers, distinguished by application field (therapeutic and educational). Furthermore, the eventual use of bio/neurofeedback is reported and, in the case of immersive applications, the display model is specified. The type of the study (i.e. Design and Prototyping, Early Feasibility, Feasibility, and Pivotal) is reported in the last column, according to the labels presented in the “Method” section. In the column Quality Assessment, (i) the design of the experiment, (ii) the sample size and the number of sessions, and (iii) the quality score are reported. Randomised controlled trial, controlled clinical trial, before-after study, and only-after study resulted to be the different types of experiment designs.
Eighty-nine percent make use of immersive VR interfaces (Table 3), by means of a head-mounted display (HMD), preferring commercial models such as the Oculus Rift (36%), followed by Oculus Go (15%), and low-cost mobile solutions such as Samsung Gear VR (13%), HTC Vive (11%), Google Cardboard (4%), and Google Daydream (4%) (Table 3). The transition from non-immersive solutions, usable via screens or projectors, to immersive interfaces appears to be growing rapidly in recent years. Forty-five percent propose adaptive systems based on biosignals’ processing (Table 3). Forty-five of examined studies focused on the educational field, the remaining 55% focused on clinical interventions (Table 3). Compared to non-immersive VR, using traditional input and output tools (screen, keyboard, mouse), with respect to the interaction and navigation of the user in the scene (Botella et al., 2013), most of the reviewed solutions are oriented towards immersive virtual reality, employing a head-mounted display. Several papers collected in this survey propose a tool for the mindfulness skills training (Chandrasiri et al., 2020; Choo & May, 2014; Costa et al., 2019; Kosunen et al., 2016; Roo et al., 2017; Shaw et al., 2011). For example, the system in Chandrasiri et al. (2020) immerses users in relaxing scenarios consisting of 360° videos experienced by wearing the Oculus Rift HMD. In Fig. 5, a standard architecture of an immersive VR-supported approach is shown. Many papers exploit immersive VR in order to immerse the user in natural scenarios (Blum et al., 2019; Costa et al., 2019; Kosunen et al., 2016; Navarro-Haro et al., 2016), in accordance with attention restoration theory (ART) and with design principles focused on Biophilia. Moreover, immersive VR is adopted in cognitive psychology interventions. Encouraging results are reported for the treatment of borderline personality disorder, in the context of dialectical behavior therapy (DBT) (Navarro-Haro et al., 2016, 2017), by using a nature-inspired virtual scenario. The authors pointed out the short-term benefits in patients, due to the increasing of their level of acceptance. The potential of the solution to improve the therapeutic outcome is also highlighted. Navarro-Haro et al. (2016) pointed out that VR can be particularly valuable for clinical psychology applications because many patients with psychological problems also have trouble concentrating and find mindfulness too difficult.

Standard architecture of an immersive VR-supported approach: mindfulness audiovisual contents are enjoyed by the user through a head-mounted display (Navarro-Haro et al., 2017)
Biofeedback may represent a promising upgrade for a VR-supported mindfulness intervention. In Gromala et al. (2015), the non-immersive virtual meditative walking (VMW) is proposed, in order to treat patients with chronic pain. The system simulates a meditative walk in a forest, adapting the weather conditions of the environment according to the subject’s skin conductance (and his/her state of arousal). If the user is relaxed, the weather appears clear, while as the levels of anxiety increase, the scenario changes, increasing the fog level. The system is based on a DeepStream3D immersive desktop display, a specific display used to transform a PC desktop into a wide-screen 3D theatre. Therefore, the user can look around but use the mouse to control the gaze direction. Shaw et al. (2011) inaugurated the use of biofeedback in immersive VR-based mindfulness. By means of meditation and biofeedback, users are able to achieve awareness of physiological states that are not usually directly perceptible. They propose the meditation chamber, an immersive virtual reality adaptive to the inputs produced by a biofeedback system (respiration rate, heart rate, and galvanic skin response). The system pursues to (i) reduce stress levels mainly through muscle relaxation and other meditation exercise, and (ii) allow users with limited meditation skills to perceive the change in physiological states. In Seol et al. (2017), the heart rate information is fed back to the user through a haptic interface, which is a simulacrum of the user’s heart beating in his hand. The system architecture is highlighted in Fig. 6. The use of a tangible haptic feedback is an example of an augmented virtuality strategy to improve concentration on the present. In Blum et al. (2019), the advantages of implementing heart rate variability (HRV) biofeedback in a virtual scenario are shown. Although the weak quality of the study (14-scored QATQS), the results suggest that a virtual reality-based implementation proves to be more effective than the standard one in several respects, including increasing relaxation self-efficacy, reducing mind wandering, and preserving attention resources.

Architecture of a biofeedback based VR-haptic system: a simulacrum of the user’s heart beats in his hand synchronized to the heart rate signal (Seol et al., 2017)
Neurofeedback is a peculiar type of biofeedback theoretically aimed at applying the principles of biofeedback at a neurocognitive level, for the self-modulation of some functions of the central nervous system. This self-check is made easier through the information deriving from the electroencephalogram (EEG) processed by a computer and displayed with a delay of a few milliseconds. In Gil et al. (2018), the effectiveness of neurofeedback for improving mindfulness-related capacities in healthy individuals was demonstrated. Fifty volunteers were asked to focus on increasing the upper alpha power. EEG signals were averaged over parieto-occipital locations. In Sas and Chopra (2015), the benefits of EEG-based binaural feedback in deepening meditative states were found, particularly for novice meditators. The brain activity modulation appears to be induced directly on a physiological level without conscious involvement of the user (Birbaumer et al., 2013; Cho et al., 2008). Electroencephalographic signals may be also used for a quantitative assessment of mindfulness effectiveness. A systematic review on 56 papers (Lomas et al., 2015), collecting experiments on 1715 subjects (21% with psychiatric diagnoses), highlighted the enhancement of alpha and theta power as the most frequent mindfulness effect. High alpha and theta levels, in both healthy individuals and in patient groups, may signify a state of relaxed alertness, which is a condition valuable to mental health. In Balconi et al. (2017), the preliminary evidence on the effect of an intensive technology-mediated meditation protocol, based on mindfulness practices and supported by a brain-sensing wearable device, was presented. The outcome indices included instrumental measures (resting-state and task-related electroencephalographic markers—EEG-ERPs).
SOLAR (Prpa et al., 2015) is an example of VR-supported mindfulness solution based on EEG signals. The system recreates a non-immersive virtual environment (available on screen), modelled by means of abstract objects, in a consistent way with the user’s breathing rate and also with brain activity (recorded using an EEG Emotiv Epoc headset). The prototype is based on non-invasive and non-distracting audio-visual stimuli, used to catch the user’s attention. The gamification module is based on rewarding practices and natural scenarios. In Choo and May (2014), the authors proposed Serenity that is a game for mindfulness skills development based on the use of virtual reality and assisted by neurofeedback (Emotiv EPOC). A rewarding mechanism is used to incentivise the player consciously meditate with the software. A reward is guaranteed for each lesson completed each completed lesson, no matter how poorly or well the participant performed. This helps prevent performance anxiety among users, who should feel free to focus on learning mindfulness at their own pace. In Kosunen et al. (2016), the authors proposed the RelaWorld system whose goal is to implement two mindfulness techniques, through virtual reality and neurofeedback (Fig. 7) which are point focus meditation (PFM) and body scan meditation (BSM). The former is achieved by focusing the user’ s attention on a specific point, the latter by offering an interface in which the user is sequentially invited to focus on a specific region of the body. The immersive VR interface (available on the Oculus Rift HMD) is based on a relaxing scenario, depicting a natural tropical paradise. Neurofeedback was used to detect alpha and theta waves’ activity, both involved during meditation and related to relaxation and concentration respectively. The results of this before-after study (15-scored QATQS) indicate better performance for the neuro-adaptive VR session, compared to the session without neurofeedback and the session without VR or neurofeedback. The analysis is based on the output of the meditation depth questionnaire (MEDEQ).

A neurofeedback-based immersive VR solution. A 3D virtual reality environment is designed for meditation practices in RelaWorld (Kosunen et al., 2016). The Oculus Rift DK2 headmounted display is used together with the EEG recored QuickAmp (BrainProducts GmbH., Germany)
Discussion
The general quality weakness characterising the literature does not allow to point out evidences about the relationship between VR and mindfulness. Nevertheless, research questions related to the effect of VR on adherence and effectiveness in mindfulness practice can be answered by borrowing the conclusions of a few better rated papers. Papers from FS cluster address the adherence issue, and among them, Tarrant et al. (2018) presented a 13-scored CCT study based on the use of electroencephalography. Twenty-one participants in a single experimental session validated the hypothesis that a VR-supported solution provides better results than the traditional mindfulness treatment (control group). The measurement system was based on electrophysiological markers of anxiety. Miller et al. (2020) proposed a 13-scored before-after study with forty-eight subjects and one experimental session. VR-supported meditation resulted more effective than typical (non-VR) one for inducing positive affective experiences.
Immersive VR makes gamification strategies easily applicable. Gamification can help increase retention, affection, and motivation to practise and, therefore, address adherence. Among all technology-assisted mindfulness interventions, immersive VR solutions are more effective from the engagement (assisted by the gamification dimension) and user motivation perspectives. More in general, the practice of video games captures players’ attention and improves it (Green & Bavelier, 2003); when an immersive multimodal channel is used, the sense of absorption, which is the ability to involve attentional capacity continuously over time, increases. It is complex to consider mindfulness like a game from the point of view of a practitioner, because games, by definition, lead to encourage external attention, whereas mindfulness tends towards introspection and focuses on the inner self (Choo & May, 2014). Furthermore, putting gamification mechanics based on challenges and rewards together with mindfulness seems antithetical, as meditation is far from stimulating competition and achievement (Shapiro et al., 2018). The reviewed studies focus on the use of gamification dynamics in a smart way, in order to avoid generating side effects. Rewarding practices should always reward the player for continued practice and never discourage poor performance and “failures”. Specifically, the more time the user spends practising, the newer stages should be unlocked in the experience (e.g. new meditation scenarios, new exercises). The meditation score, based on the psychophysiological data collected, must also be returned through non-distracting environmental storytelling elements, contextual to the experience. Several studies offer a series of design best practices to consider in the future development of gamification experiences to support mindfulness (Sliwinski et al., 2015, 2017). Ultimately, the use of motivational design sounds crucial for a good virtual mindfulness experience (Amores et al., 2016; Choo & May, 2014; Kosuru et al., 2019; Prpa et al., 2015).
The PS cluster papers refers to the effectiveness of VR-based mindfulness on specific therapeutic outcomes. Among them, Goldenhersch et al. (2020) presented a 10-scored RCT study on an immersive VR smartphone-based intervention implemented to support smoking cessation through mindfulness meditation. One hundred and fifty participants were involved in twenty-one experimental sessions, and the system showed great potential in relation to participant adherence and initial efficacy of therapy. Igna et al. (2014) presented an 11-scored CCT study with sixty-eight participants on six experimental sessions. The study gathered results related to the beneficial impact of mindfulness treatments with and without VR for the reduction of chronic back pain. The results pointed out how pain levels tended to be lower in the mindfulness-based protocol group (MBCT) than in the control one. In this context, no differences were revealed between the VR-based solution and the traditional treatment. Finally, Navarro-Haro et al. (2019) presented an 11-scored RCT study, with thirty-nine participants over seven experimental sessions, geared towards the treatment of general anxiety disorder (GAD) in primary care. Their results confirmed the hypothesis that the group receiving a VR-mindfulness training protocol (DBT) tends to be more adherent to the intervention than to the traditional intervention alone.
The study proposed by Navarro-Haro et al. (2019) is the only one focusing on the interoceptive awareness. By processing data from the Multidimensional Assessment of Interoceptive Awareness (MAIA) questionnaire (Mehling et al., 2012), the study proved an increase of IA in both experimental and control groups. Nevertheless, the study did not use any biofeedback. Tinga et al. (2019), based on a blinded RCT, showed that respiratory biofeedback has low effectiveness in reducing objective arousal (assessed through EEG and heart rate variability) compared to placebo control feedback. However, the potential of biofeedback in supporting IA is not considered. In general, the literature shows a lack of attention to the role of biofeedback in IA.
With regard to decentering, almost 50% of the reviewed studies use cutting-edge VR technologies (Oculus Rift and HTC Vive HMDs) ensuring high accuracy, resolution, and reactivity in the production of stimuli. In these cases, the high level of immersion is compatible with effective interventions on the body matrix. However, no study exploits the immersive potential of VR in altering previous perceptions and in contributing to build a new vision of oneself.
The reviewed papers provide several contributes addressing innovative design solutions emerging in the VR-supported mindfulness field. The use of bio/neurofeedback data in the immersive VR environment allows the customization of a scenario according to the subject. In this way, it is possible to offer an experience closer to the cultural sensitivity of the patient. Furthermore, individuals belonging to the same culture react in different ways to certain stimuli or scenarios. Partiality (Anderson & Farb, 2018) is defined as a predisposition that an individual exhibits towards a particular practice. Therefore, considering his partiality is possible to evaluate and choose the most useful and effective practice for a given user, and this can help to maintain engagement in the activity. Somatosensory attention-oriented anchors are the most frequently considered (i.e. popular techniques focused on breathing). Moreover, auditory and visual anchors are also investigated, although there is a lack of comparisons of their effectiveness with respect to partiality (Anderson & Farb, 2018).
Bio/neurofeedback data allow the introduction of specific gamification strategies, linked to the enhancement of neurophysiological performance. These data are returned in the virtual environment as elements of environmental storytelling (Kosunen et al., 2017) offered through real-time gamification dynamics (e.g. levitation modulated by concentration levels in RelaWorld (Kosunen et al., 2016) or the flowers blooming in Serenity game (Choo & May, 2014)). Thus, a series of events can occur in the virtual space as a consequence of the variation of certain psychophysiological states. In this way, the possibility for the practitioner to feel and perceive his own body is increased.
The use of psychophysiological data allows the promotion of collaborative experiences in which the avatars of other participants are animated based on the user’s psychological state. Direct observation of the virtual avatars of other users practising the same activity could induce in the practitioner a greater state of relaxation, due to the mirror neurons’ mechanism (Rizzolatti et al., 2009). From a clinical perspective, gathering biometric data in virtual immersive environments can improve diagnosis by evaluating specific individual reactions to certain environmental stimuli and for medium- and long-term effectiveness evaluations.
Ultimately, the auditory and visual (but potentially also haptic, olfactory, and gustatory) features of the environment can be precisely controlled. Therefore, multisensory immersive adaptive VR offers a unique and flexible tool to manage and customise both content and stimuli, according to the needs, reactions, attitudes, and socio-cultural background and sensitivity of the practitioner. This promptly responds to the needs of the clinician (but also of the facilitator in non-therapeutic/educational contexts), with reference to the possibility of monitoring the system and tuning the environmental setting parameters in real time according to the user profile.
Limitations and Future Research
There are some limitations to the current review. First of all, a comparison among different tools (e.g. questionnaires, biosignal-based measurement systems) for the assessment of VR effectiveness in supporting mindfulness is marginally addressed. Moreover, strategies to transfer and adapt traditional mindfulness content to the VR medium were not discussed. For example, it might be interesting to evaluate the most effective symbolic mediation for internal bodily signals in supporting interoceptive awareness.
Finally, this review did not focus on the relationship between levels of immersion and the effectiveness of VR in supporting mindfulness, particularly with regard to altering the body matrix. Future researchers could distinguish VR systems considering (i) the type of perceptual domains (sensorial, proprioceptive, interoceptive, and vestibular input) and (ii) the accuracy, resolution, and responsiveness of the stimuli in each domain.
The reviewed literature exhibits a general statistical quality and the relationship between VR and mindfulness seems to be still unclear. Therefore, more rigorous, blind, and randomized controlled studies are needed in the future. Furthermore, literature shows a lack of attention to the role of biofeedback in IA and the potential of VR to improve the decentering.
To better summarise the features of VR-supported mindfulness 2.0, the general architecture of a multisensory immersive VR system that gathers real-time information from the body and brain is depicted in Fig. 8. Consistent with the reviewed literature, the convergence of various input and output information channels may be particularly promising in order to effectively support mindfulness interventions. All the biosignals (the bio/neurofeedback raw data collected by the relative transducers) are fed as input to a processing unit. Here, they will be processed and then transformed into adaptive stimuli by the adaptivity manager. These stimuli will be presented to the user by means of the immersive VR interface through all perceptual domains (sensorial, proprioceptive, interoceptive, and vestibular). A Sessions Memory module takes into account the diachronic dimension of the experience, as well as its dynamic component and its progressive evolution. This is crucial from the point of view of “gamification”, where content adapts dynamically to the evolution of the user experience. A communication unit module enables the transfer of information within and outside the system. The communication channels guarantee data exchange with (i) the VR-immersive unit, where adaptive content can transit in one direction, and user tracking data in the other; (ii) other users, to foster a collaborative experience and to bring tangible benefits of group practice; and (iii) the user therapist (e.g. via web interface as is the case in RecoVR (Cikajlo et al., 2016)), where both biosignals and mindfulness score can transit (the therapist can consult, evaluate, and collect this data mainly offline, and then make diagnostic and therapeutic decisions).

Emerging architecture of a mindfulness computer supported solution based on integration of AR-immersive, biofeedback and neurofeedback
In the near future, adaptation strategies to the VR scenario will be increasingly necessary, in a health 4.0 perspective. An interesting line of research considers this issue from the perspective of artificial intelligence and physiological computing, with the aim of monitoring, measuring, analysing, and translating human psychophysiological parameters in real time to communicate the user’s state to an adaptive system (Fairclough, 2009). Artificial intelligence is used for a real-time proactive and automatic system adaptation, by transforming psychophysiological data into control signals (biocybernetic loop). A self-adaptive solution would have the advantage of being focused on the moment the subject is experiencing.
Immersive VR continues to explore multi-perceptual domains and additional modalities such as new sensory (e.g., haptics and olfactory), interoceptive (biofeedback-based), proprioceptive, and vestibular (e.g., Sonoception) channels will soon be considered (Riva et al., 2017). In this way, the sense of presence and effectiveness of the virtual experience will increase (Ramsamy et al., 2006), in particular in the decentering perspective. Finally, another interesting possibility is to consider precognitive stimuli of a multi-perceptual domain, which have a direct effect at a physiological level, not requiring symbolic mediation. These include the binaural tones, which directly modulate brain waves (adaptively) to elicit favourable conditions for meditation (Sas & Chopra, 2015).
References
All studies included in this review are marked by an *.
*Amores, J., Benavides, X., & Maes, P. (2016, May). Psychicvr: increasing mindfulness by using virtual reality and brain computer interfaces. In Kaye, J. (Ed.) Proceedings of the 2016 CHI Conference Extended Abstracts on Human Factors in Computing Systems (pp. 2–2). https://doi.org/10.1145/2851581.2889442
Anderson, T., & Farb, N. A. (2018). Personalising practice using preferences for meditation anchor modality. Frontiers in Psychology, 9, 2521. https://doi.org/10.3389/fpsyg.2018.02521
Balconi, M., Fronda, G., Venturella, I., & Crivelli, D. (2017). Conscious pre-conscious and unconscious mechanisms in emotional behaviour Some applications to the mindfulness approach with wearable devices. Applied Sciences, 7(12), 1280. https://doi.org/10.3390/app7121280
Barba, M. C., Covino, A., De Luca, V., De Paolis, L. T., D’Errico, G., Di Bitonto, P., Di Gestore, S., Magliaro, S., Nunnari, F., Paladini, G.I., Potenza, A., & Schena, A. (2019). Bravo: a gaming environment for the treatment of adhd. In: De Paolis L., Bourdot P. (Eds.) International conference on augmented reality, virtual reality and computer graphics (pp. 394–407). Springer, Cham. https://doi.org/10.1007/978-3-030-25965-5_30
Birbaumer, N., Ruiz, S., & Sitaram, R. (2013). Learned regulation of brain metabolism. Trends in Cognitive Sciences, 17(6), 295–302.
Blum, J., Rockstroh, C., Göritz, A. S. (2019). Heart rate variability biofeedback based on slow-paced breathing with immersive virtual reality nature scenery. Frontiers in Psychology, 10, 2172. https://doi.org/10.3389/fpsyg.2019.02172
Bohil, C. J., Alicea, B., & Biocca, F. A. (2011). Virtual reality in neuroscience research and therapy. Nature Reviews Neuroscience, 12(12), 752–762.
*Botella, C., Garcia-Palacios, A., Vizcaíno, Y., Herrero, R., Baños, R. M., Belmonte, M. A. (2013). Virtual reality in the treatment of fibromyalgia: a pilot study. Cyberpsychology, Behavior, and Social Networking, 16 (3), 215-223
Bowman, D. A., & McMahan, R. P. (2007). Virtual reality: How much immersion is enough? Computer, 40(7), 36–43.
*Bruggeman, K. J., & Wurster, S. W. (2018). The Hiatus system: virtual healing spaces: low dose mindfulness based stress reduction virtual reality application. In Jang, J. & Bednarz, T. (Eds.) ACM SIGGRAPH 2018 Appy Hour (pp. 1–2).
*Cebolla, A., Herrero, R., Ventura, S., Miragall, M., Bellosta-Batalla, M., Llorens, R., Baños, R. M. (2019). Putting oneself in the body of others: a pilot study on the efficacy of an embodied virtual reality system to generate self-compassion. Frontiers in Psychology, 10, 1521. https://doi.org/10.3389/fpsyg.2019.01521
*Chandrasiri, A., Collett, J., Fassbender, E., De Foe, A. (2020). A virtual reality approach to mindfulness skills training. Virtual Reality, 24 (1), 143-149
*Chavez, L. J., Kelleher, K., Slesnick, N., Holowacz, E., Luthy, E., Moore, L., & Ford, J. (2020). Virtual reality meditation among youth experiencing homelessness: pilot randomized controlled trial of feasibility. JMIR Mental Health, 7(9), https://doi.org/10.2196/18244
*Chen, X. J., Wang, D. M., Zhou, L. D., Winkler, M., Pauli, P., Sui, N., Li, Y. H. (2018). Mindfulness-based relapse prevention combined with virtual reality cue exposure for methamphetamine use disorder: Study protocol for a randomized controlled trial. Contemporary Clinical Trials, 70, 99-105
Cho, M. K., Jang, H. S., Jeong, S. H., Jang, I. S., Choi, B. J., & Lee, M. G. T. (2008). Alpha neurofeedback improves the maintaining ability of alpha activity. NeuroReport, 19(3), 315–317.
*Choo, A., & May, A. (2014, October). Virtual mindfulness meditation: Virtual reality and electroencephalography for health gamification. In Khan, Z. & Kapralos, B. (Eds.) 2014 IEEE Games Media Entertainment (pp. 1–3). IEEE.
Choo, C. C., & Burton, A. A. (2018). Smartphone apps for mindfulness interventions for suicidality in Asian youths: Literature review. JMIR mHealth and uHealth, 6(6), e139. https://doi.org/10.2196/mhealth.8304
*Cikajlo, I., Čižman-Štaba, U., Vrhovac, S., Larkin, F., & Roddy, M. (2016, October). RecoVR: Realising collaborative virtual reality for wellbeing and self-healing. In Hamza, M., H. (Ed.) Proceedings of the 3rd IASTED International Conference Telehealth Assistive Technology TAT (pp. 11–17).
Clark, A. (2013). Whatever next? Predictive brains, situated agents, and the future of cognitive science. Behavioral and Brain Sciences, 36(3), 181–204.
*Costa, M. R., Bergen-Cico, D., Hererro, R., Navarro, J., Razza, R., Wang, Q. (2018). XR-based systems for mindfulness based training in clinical settings. In Chen, J. Y. C. & Fragomeni, G. (Eds.) International Conference on Virtual, Augmented and Mixed Reality (pp. 31-39). Springer, Cham
*Costa, M. R., Bergen-Cico, D., Grant, T., Herrero, R., Navarro, J., Razza, R., Wang, Q. (2019). Nature inspired scenes for guided mindfulness training: presence, perceived restorativeness and meditation depth. In Lamas, D., Loizides, F., Nacke, L., Petrie, H., Winckler, M., & Zaphiris, P. (Eds.) International Conference on Human-Computer Interaction (pp. 517-532). Springer, Cham
*Costa, M. R., Bergen-Cico, D., Razza, R., Hirshfield, L., Wang, Q. (2020). Perceived restorativeness and meditation depth for virtual reality supported mindfulness interventions. In Antona, M. & Stephanidis, C. (Eds.) International Conference on Human-Computer Interaction (pp. 176-189). Springer, Cham
*Crosswell, L., Yun, G. W. (2020). Examining virtual meditation as a stress management strategy on college campuses through longitudinal, quasi-experimental research. Behaviour & Information Technology, 1-15. https://doi.org/10.1080/0144929X.2020.1838609
*Damen, K. H., Van der Spek, E. D. (2018). Virtual reality as e-mental health to support starting with mindfulness-based cognitive therapy. In Clua, E., Roque, L., Lugmayr, A., & Tuomi, P. (eds.) International Conference on Entertainment Computing (pp. 241-247). Springer, Cham
*Darnall, B. D., Krishnamurthy, P., Tsuei, J., Minor, J. D. (2020). Self-administered skills-based virtual reality intervention for chronic pain: randomized controlled pilot study. JMIR Formative Research, 4 (7), e17293. https://doi.org/10.2196/17293
*Edirisooriya, Y. L., Rathnayake, N. A., Ariyasena, T. D., Thelijjagoda, S. S., Jayawickrama, N. D., Chamindi, D. I. (2019). Smartphone-based approach to enhance mindfulness among undergraduates with stress. In Shanaz, A., Lathif F., & Ragel, R. G. (Eds.) 2019 14th Conference on Industrial and Information Systems (ICIIS) (pp. 464-469). IEEE
Fairclough, S. H. (2009). Fundamentals of physiological computing. Interacting with Computers, 21(1–2), 133–145.
Farb, N., Daubenmier, J., Price, C. J., Gard, T., Kerr, C., Dunn, B. D., Klein, A. C., Paulus, M. P., & Mehling, W. E. (2015). Interoception, contemplative practice, and health. Frontiers in Psychology, 6, 763. https://doi.org/10.3389/fpsyg.2015.00763
Fresco, D. M., Moore, M. T., van Dulmen, M. H., Segal, Z. V., Ma, S. H., Teasdale, J. D., & Williams, J. M. G. (2007). Initial psychometric properties of the experiences questionnaire: Validation of a self-report measure of decentering. Behavior Therapy, 38(3), 234–246.
*Flores, A., Linehan, M. M., Todd, S. R., Hoffman, H. G. (2018). The use of virtual reality to facilitate mindfulness skills training in dialectical behavioral therapy for spinal cord injury: a case study. Frontiers in Psychology, 9, 531. https://doi.org/10.3389/fpsyg.2018.00531
Garcia-Palacios, A., Hoffman, H., Carlin, A., Furness, T. A., III., & Botella, C. (2002). Virtual reality in the treatment of spider phobia: A controlled study. Behaviour Research and Therapy, 40(9), 983–993.
*Garrett, B., Taverner, T., McDade, P. (2017). Virtual reality as an adjunct home therapy in chronic pain management: an exploratory study. JMIR Medical Informatics, 5(2), e11. https://doi.org/10.2196/medinform.7271
*Gatto, C., D’Errico, G., Nuccetelli, F., De Luca, V., Paladini, G. I., & De Paolis, L. T. (2020,). XR-based mindfulness and art therapy: facing the psychological impact of covid-19 emergency. In De Paolis, L. T. & Bourdot, P. (Eds.) International Conference on Augmented Reality, Virtual Reality and Computer Graphics (pp. 147–155). Springer, Cham.
Gil, M. N., Marco, C. E., Montero-Marín, J., Zafra, J. M., Shonin, E., & Campayo, J. G. (2018). Efficacy of neurofeedback on the increase of mindfulness-related capacities in healthy individuals: A controlled trial. Mindfulness, 9(1), 303–311.
*Goldenhersch, E., Thrul, J., Ungaretti, J., Rosencovich, N., Waitman, C., & Ceberio, M. R. (2020). Virtual reality smartphone-based intervention for smoking cessation: pilot randomized controlled trial on initial clinical efficacy and adherence. Journal of Medical Internet Research, 22(7), e17571. https://doi.org/10.2196/17571
*Gomez, J., Hoffman, H. G., Bistricky, S. L., Gonzalez, M., Rosenberg, L., Sampaio, M., Garcia-Palacios, A., Navarro-Haro, M.V., Alhalabi, W., Rosenberg, M., Meyer III, W.J. Linehan, M. M. (2017). The use of Virtual Reality Facilitates Dialectical Behavior Therapy® “Observing Sounds and Visuals” mindfulness skills training exercises for a Latino patient with severe burns: a case study. Frontiers in Psychology, 8, 1611. https://doi.org/10.3389/fpsyg.2017.01611
Gorini, A., Capideville, C. S., De Leo, G., Mantovani, F., & Riva, G. (2011). The role of immersion and narrative in mediated presence: The virtual hospital experience. Cyberpsychology, Behavior, and Social Networking, 14(3), 99–105.
Gorisse, G., Christmann, O., Amato, E. A., & Richir, S. (2017). First-and third-person perspectives in immersive virtual environments: Presence and performance analysis of embodied users. Frontiers in Robotics and AI, 4, 33. https://doi.org/10.3389/frobt.2017.00033
Green, C. S., & Bavelier, D. (2003). Action video game modifies visual selective attention. Nature, 423(6939), 534–537.
*Gromala, D., Song, M., Yim, J. D., Fox, T., Barnes, S. J., Nazemi, M., Shaw, C., Squire, P. (2011). Immersive VR: a non-pharmacological analgesic for chronic pain?. In Begole, B. & Kellogg, W. (Eds.) CHI’11 Extended Abstracts on Human Factors in Computing Systems (pp. 1171–1176).
*Gromala, D., Tong, X., Choo, A., Karamnejad, M., Shaw, C. D. (2015). The virtual meditative walk: virtual reality therapy for chronic pain management. In Begole, B. (Ed.) Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems (pp. 521–524).
*Haisley, K. R., Straw, O. J., Müller, D. T., Antiporda, M. A., Zihni, A. M., Reavis, K. M., Bradley, D.D., & Dunst, C. M. (2020). Feasibility of implementing a virtual reality program as an adjuvant tool for peri-operative pain control; results of a randomized controlled trial in minimally invasive foregut surgery. Complementary Therapies in Medicine, 49, 102356. https://doi.org/10.1016/j.ctim.2020.102356
Hanley, A. W., Mehling, W. E., & Garland, E. L. (2017). Holding the body in mind: Interoceptive awareness, dispositional mindfulness and psychological well-being. Journal of Psychosomatic Research, 99, 13–20.
Hölzel, B. K., Lazar, S. W., Gard, T., Schuman-Olivier, Z., Vago, D. R., & Ott, U. (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6(6), 537–559.
*Igna, R., Ştefan, S., Onac, I., Onac, I., Ungur, R. A., & Tatar, A. S. (2014). Mindfulness-based Cognitive-Behavior Therapy (MCBT) versus Virtual Reality (VR) enhanced CBT, versus treatment as usual for chronic back pain. A Clinical Trial. Journal of Evidence-Based Psychotherapies, 14(2). 229–247.
Kaplan, S. (1995). The restorative benefits of nature: Toward an integrative framework. Journal of Environmental Psychology, 15(3), 169–182.
Kitchenham, B. (2004). Procedures for performing systematic reviews. Keele, UK, Keele University, 33(2004), 1–26.
*Kosunen, I., Salminen, M., Järvelä, S., Ruonala, A., Ravaja, N., & Jacucci, G. (2016). RelaWorld: neuroadaptive and immersive virtual reality meditation system. In Nichols, J., Mahmud, J., & O'Donovan, J. Proceedings of the 21st International Conference on Intelligent User Interfaces (pp. 208–217).
Kosunen, I., Ruonala, A., Salminen, M., Järvelä, S., Ravaja, N., & Jacucci, G. (2017). Neuroadaptive meditation in the real world. In Friedman, D., Brouwer, A. M., & Nijholt A. (Eds.) Proceedings of the 2017 ACM Workshop on An Application-oriented Approach to BCI out of the laboratory (pp. 29–33).
Kosuru, R. K., Lingelbach, K., Bui, M., & Vukelić, M. (2019). MindTrain: how to train your mind with interactive technologies. In Alt, F., Bulling, A., & Döring, T. (Eds.) Proceedings of Mensch und Computer 2019 (pp. 643–647).
Kriakous, S. A., Elliott, K. A., Lamers, C., & Owen, R. (2021). The effectiveness of mindfulness-based stress reduction on the psychological functioning of healthcare professionals: A systematic review. Mindfulness, 12(1), 1–28.
Lindner, P., Miloff, A., Zetterlund, E., Reuterskiöld, L., Andersson, G., & Carlbring, P. (2019). Attitudes toward and familiarity with virtual reality therapy among practicing cognitive behavior therapists: A cross-sectional survey study in the era of consumer VR platforms. Frontiers in Psychology, 10, 176. https://doi.org/10.3389/fpsyg.2019.00176
Lomas, T., Ivtzan, I., & Fu, C. H. (2015). A systematic review of the neurophysiology of mindfulness on EEG oscillations. Neuroscience & Biobehavioral Reviews, 57, 401–410.
*Louw, A., Louw, C., Flynn, T. (2019). Case report: pain neuroscience education using virtual reality. Pain and Rehabilitation-the Journal of Physiotherapy Pain Association, 2019(46), 4-7
Lutz, A., Slagter, H. A., Dunne, J. D., & Davidson, R. J. (2008). Attention regulation and monitoring in meditation. Trends in Cognitive Sciences, 12(4), 163–169.
Lyzwinski, L. N., Caffery, L., Bambling, M., & Edirippulige, S. (2018). A systematic review of electronic mindfulness-based therapeutic interventions for weight, weight-related behaviors, and psychological stress. Telemedicine and e-Health, 24(3), 173–184.
Mehling, W. E., Price, C., Daubenmier, J. J., Acree, M., Bartmess, E., & Stewart, A. (2012). The multidimensional assessment of interoceptive awareness (MAIA). PLoS ONE, 7(11), e48230. https://doi.org/10.1371/journal.pone.0048230
*Miller, M., Mistry, D., Jetly, R., & Frewen, P. (2020). Meditating in virtual reality 2: phenomenology of vividness, egocentricity and absorption-immersion. Mindfulness, 12(5), 1195-1207
*Min, S., Moon, J. G., Cho, C. H., & Kim, G. J. (2020). Effects of immersive virtual reality content type to mindfulness and physiological parameters. In Teather, R. J., Joslin, C., Stuerzlinger, W., Figueroa, P., Hu, Y., Batmaz, A., U., Lee, W., & Ortega, F. (Eds.) 26th ACM Symposium on Virtual Reality Software and Technology (pp. 1–9).
*Mistry, D., Zhu, J., Tremblay, P., Wekerle, C., Lanius, R., Jetly, R., Frewen, P. (2020). Meditating in virtual reality: Proof-of-concept intervention for posttraumatic stress. Psychological Trauma: Theory, Research, Practice, and Policy, 12(8), 847-858. https://doi.org/10.1037/tra0000959
Moher, D., Altman, D. G., Liberati, A., & Tetzlaff, J. (2011). PRISMA statement. Epidemiology, 22(1), 128. https://doi.org/10.1097/EDE.0b013e3181fe7825
*Moller, H. J., Saynor, L., Chignell, M., Waterworth, J. (2019). Nature and nurturance across the ages: modest means for modern times. In Lo, D., Apel S., & Khurshid, S. (Eds.) Interactivity, Game Creation, Design, Learning, and Innovation (pp. 539-558). Springer, Cham
Moseley, G. L., Gallace, A., & Spence, C. (2012). Bodily illusions in health and disease: Physiological and clinical perspectives and the concept of a cortical ‘body matrix.’ Neuroscience & Biobehavioral Reviews, 36(1), 34–46.
*Moseley, R. (2016). Immersive brain entrainment in virtual worlds: actualizing meditative states. In Chen, L., Kapoor, S., & Bhatia, R. (Eds.) Emerging Trends and Advanced Technologies for Computational Intelligence (pp. 315-346). Springer, Cham
*Navarro-Haro, M. V., Hoffman, H. G., Garcia-Palacios, A., Sampaio, M., Alhalabi, W., Hall, K., & Linehan, M. (2016). The use of virtual reality to facilitate mindfulness skills training in dialectical behavioral therapy for borderline personality disorder: a case study. Frontiers in Psychology, 7, 1573. https://doi.org/10.3389/fpsyg.2016.01573
*Navarro-Haro, M. V., López-del-Hoyo, Y., Campos, D., Linehan, M. M., Hoffman, H. G., García-Palacios, A., Modrego-Alarcón, M., Borao, L. & García-Campayo, J. (2017). Meditation experts try virtual reality mindfulness: a pilot study evaluation of the feasibility and acceptability of virtual reality to facilitate mindfulness practice in people attending a mindfulness conference. PloS one, 12(11), e0187777. https://doi.org/10.1371/journal.pone.0187777<span id="selectionBoundary_1635278799679_7953073646774849" class="rangySelectionBoundary" style="line-height: 0; display: none;"></span>
*Navarro-Haro, M. V., Modrego-Alarcón, M., Hoffman, H. G., López-Montoyo, A., Navarro-Gil, M., Montero-Marin, J., García-Palacios A., Borao, L. & García-Campayo, J. (2019). Evaluation of a mindfulness-based intervention with and without virtual reality dialectical behavior therapy® mindfulness skills training for the treatment of generalized anxiety disorder in primary care: a pilot study. Frontiers in Psychology, 10, 55. https://doi.org/10.3389/fpsyg.2019.00055
Nunnari, F., Magliaro, S., D’Errico, G., De Luca, V., Barba, M. C., & De Paolis, L. T. (2019, October). Designing and assessing interactive virtual characters for children affected by ADHD. In Bourdot, P., Interrante, V., Kopper, R., Olivier, A.-H., Saito, H., & Zachmann, G. (Eds.) International Conference on Virtual Reality and Augmented Reality (pp. 285–290). Springer, Cham.
*Olbrecht, V. A., T O'Conor, K., Williams, S. E., Boehmer, C. O., Marchant, G. W., Glynn, S. M., Geisler, K. J., Ding, L., Yang, G., & King, C. D. (2021). Guided relaxation-based virtual reality versus distraction-based virtual reality or passive control for postoperative pain management in children and adolescents undergoing Nuss repair of pectus excavatum: protocol for a prospective, randomised, controlled trial (FOREVR Peds trial). BMJ open, 10(12), e040295.
*Palomo, P., De Oliveira, D. R., Nunes, B. P., Campayo, J. G., Cebolla, A., Baños, R., Da Silva Victor, E., & Demarzo, M. (2018). Study Protocol for a randomized controlled trial of mindfulness training with immersive technology (virtual reality) to improve the quality of life of patients with multimorbidity in Primary Care: The Mindful-VR study. Annual Review of CyberTherapy and Telemedicine, 16, 140–147
*Paredes, P. E., Balters, S., Qian, K., Murnane, E. L., Ordóñez, F., Ju, W., Landay, J. A. (2018). Driving with the fishes: towards calming and mindful virtual reality experiences for the car. Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies, 2(4), 1-21
*Patibanda, R., Mueller, F. F., Leskovsek, M., & Duckworth, J. (2017, October). Life tree: understanding the design of breathing exercise games. In Schouten, B., Markopoulos, P., Toups, Z., Cairns, P., & Bekker, T., (Eds.) Proceedings of the annual symposium on computer-human interaction in play (pp. 19–31).
Plaza, I., Demarzo, M. M. P., Herrera-Mercadal, P., & García-Campayo, J. (2013). Mindfulness-based mobile applications: literature review and analysis of current features. JMIR mHealth and uHealth, 1(2), e24.
*Prpa, M., Cochrane, K., & Riecke, B. E. (2015). Hacking alternatives in 21 St century: designing a bio-responsive virtual environment for stress reduction. In Serino, S., Matic, A., Giakoumis, D., Lopez, G., & Cipresso, P. (Eds.) International Symposium on Pervasive Computing Paradigms for Mental Health (pp. 34-39). Springer, Cham
*Prpa, M., Tatar, K., Francoise, J., Riecke, B., Schiphorst, T., Pasquier, P. (2018). Attending to breath: Exploring how the cues in a virtual environment guide the attention to breath and shape the quality of experience to support mindfulness. In Koskjnen, I. & Lim, Y. K. Proceedings of the 2018 Designing Interactive Systems Conference, pp. 71–84.
*Prpa, M., Schiphorst, T., Tatar, K., Pasquier, P. (2018). Respire: a Breath Away from the Experience in Virtual Environment. In Mandryk, R. L., Hancock, M., Perry, M., & Cox. A.L. (Eds.) Extended Abstracts of the 2018 CHI Conference on Human Factors in Computing Systems (pp. 1-6).
Ramsamy, P., Haffegee, A., Jamieson, R., & Alexandrov, V. (2006). Using haptics to improve immersion in virtual environments. In O. Gervasi, V. Kumar, C. J. K. Tan, D. Taniar, A. Laganà, Y. Mun, & H. Choo (Eds.), International Conference on Computational Science (pp. 603–609). Springer.
Riva, G., Serino, S., Di Lernia, D., Pavone, E. F., & Dakanalis, A. (2017). Embodied medicine: Mens sana in corpore virtuale sano. Frontiers in Human Neuroscience, 11, 120.
Riva, G., Wiederhold, B. K., & Mantovani, F. (2019). Neuroscience of virtual reality: From virtual exposure to embodied medicine. Cyberpsychology, Behavior, and Social Networking, 22(1), 82–96.
Rizzolatti, G., Fabbri-Destro, M., & Cattaneo, L. (2009). Mirror neurons and their clinical relevance. Nature Clinical Practice Neurology, 5(1), 24–34.
*Roo, J. S., Gervais, R., Frey, J., & Hachet, M. (2017). Inner garden: connecting inner states to a mixed reality sandbox for mindfulness. In Mark, G., Fussell, S., Lampe, C., Schraefel, M. C., Hourcade, J. P., Appert, C., & Wigdor, D. (Eds.) Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems (pp. 1459–1470).
Sanchez-Vives, M. V., & Slater, M. (2005). From presence to consciousness through virtual reality. Nature Reviews Neuroscience, 6(4), 332–339.
Sas, C., & Chopra, R. (2015). MeditAid: A wearable adaptive neurofeedback-based system for training mindfulness state. Personal and Ubiquitous Computing, 19(7), 1169–1182.
*Seabrook, E., Kelly, R., Foley, F., Theiler, S., Thomas, N., Wadley, G., & Nedeljkovic, M. (2020). Understanding how virtual reality can support mindfulness practice: mixed methods study. Journal of Medical Internet Research, 22(3), e16106.
*Seol, E., Min, S., Seo, S., Jung, S., Lee, Y., Lee, J., Kim. G., Cho, C., Lee, S., Cho, C., Choi, S., & Jung, D. (2017). “Drop the beat” virtual reality based mindfulness and cognitive behavioral therapy for panic disorder---a pilot study. In Fjeld, M., Fratarcangeli, M., Sjölie, D., Staadt, O., & Unger J. (Eds.) Proceedings of the 23rd ACM Symposium on Virtual Reality Software and Technology (pp. 1–3).
*Shamekhi, A., & Bickmore, T. (2015). Breathe with me: a virtual meditation coach. In Brinkman, W. P., Broekens, J., & Heylen, D. (Eds.) International Conference on Intelligent Virtual Agents (pp. 279-282). Springer, Cham
Shapiro, S., Siegel, R., & Neff, K. D. (2018). Paradoxes of Mindfulness. Mindfulness, 9(6), 1693–1701.
*Shaw, C., Gromala, D., & Song, M. (2011). The meditation chamber: towards self-modulation. In Mura, G. (Ed.) Metaplasticity in virtual worlds: Aesthetics and semantic concepts (pp. 121-133). IGI Global
Sliwinski, J., Katsikitis, M., & Jones, C. M. (2015). Mindful gaming: how digital games can improve mindfulness. In Abascal, J., Diniz Junqueira Barbosa, S., Fetter, M., Gross, T., Palanque, P., & Winckler, M. (Eds.) IFIP Conference on Human-Computer Interaction (pp. 167–184). Springer, Cham.
Sliwinski, J., Katsikitis, M., & Jones, C. M. (2017). A review of interactive technologies as support tools for the cultivation of mindfulness. Mindfulness, 8(5), 1150–1159.
Stănică, I. C., Dascalu, M. I., Moldoveanu, A., Bodea, C. N., & Hostiuc, S. (2016). A survey of virtual reality applications as psychotherapeutic tools to treat phobias. eLearning & Software for Education, (1).
*Tarrant, J., Viczko, J., Cope, H. (2018). Virtual reality for anxiety reduction demonstrated by quantitative EEG: a pilot study. Frontiers in Psychology, 9, 1280. https://doi.org/10.3389/fpsyg.2018.01280
Thomas, H., Ciliska, D., Dobbins, M., & Micucci, S. (2008). National collaborating centre of methods and tools: Quality assessment tool for quantitative studies. McMaster University.
*Tinga, A. M., Nyklíček, I., Jansen, M. P., de Back, T. T., & Louwerse, M. M. (2019). Respiratory biofeedback does not facilitate lowering arousal in meditation through virtual reality. Applied Psychophysiology and Biofeedback, 44(1), 51-59
*Tong, X., Gromala, D., Gupta, D., & Squire, P. (2016). Usability comparisons of head-mounted vs. Stereoscopic desktop displays in a virtual reality environment with pain patients. In Westwood, J.D., Vosburgh, K.G., Westwood, S.W., Senger, S., Felländer-Tsai, L., Fidopiastis, C.M., & Liu, A. (Eds.) MMVR (pp. 424–431).
US Food and Drug Administration. (2013). Investigational device exemptions (IDEs) for early feasibility medical device clinical studies, including certain first in human (FIH) studies. US Food and Drug Administration, 1–40.
*Venuturupalli, R. S., Chu, T., Vicari, M., Kumar, A., Fortune, N., & Spielberg, B. (2019). Virtual reality–based biofeedback and guided meditation in rheumatology: a pilot study. ACR Open Rheumatology, 1(10), 667-675
*Yildirim, C., & O’Grady, T. (2020). The efficacy of a virtual reality-based mindfulness intervention. In Hürst, W., Sheu, C. Y., & Tsai, J. J. P. (Eds.) 2020 IEEE International Conference on Artificial Intelligence and Virtual Reality (AIVR) (pp. 158-165). IEEE
Acknowledgements
The authors would like to thank the editor and the anonymous reviewers for their stimulating and precious suggestions and comments to the review of this paper.
Author information
Authors and Affiliations
Contributions
P.A., G.D., L.D., and N.M. conceived and designed the review; G.D. and N.M. performed the paper research, extraction, and analysis; all authors analysed the results, wrote the manuscript, and reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Arpaia, P., D’Errico, G., De Paolis, L.T. et al. A Narrative Review of Mindfulness-Based Interventions Using Virtual Reality. Mindfulness 13, 556–571 (2022). https://doi.org/10.1007/s12671-021-01783-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12671-021-01783-6