
Abstract
Background
Previous research indicated that the benefits of expressive writing on cancer patients’ physical and psychological well-being may vary across cultures. However, it remains unknown whether the within-ethnicity cultural orientation would also moderate the efficacy of expressive writing. Immigrants are a special population who differ widely in extent of endorsing the home culture and the host culture. We examined the role of acculturation in moderating the effect of expressive writing among Chinese American breast cancer survivors in reducing different post-traumatic stress disorder (PTSD) symptom clusters: re-experiencing, avoidance, and arousal.
Method
Ninety-six Chinese American breast cancer survivors were randomly assigned to three groups to write about cancer-related topics: a self-regulation group to write about deepest feelings, stress coping, and finding benefits; an emotional disclosure group to write about deepest feelings; and a cancer-fact group to write about cancer experience objectively. The only examined moderator, acculturation, was assessed at baseline. PTSD symptoms were assessed at baseline and 1-, 3-, and 6-month follow-ups.
Results
Acculturation moderated the effect of expressive writing at 3- and 6-month follow-ups. Among participants with low acculturation, PTSD symptoms were less severe in the self-regulation and cancer-fact groups compared with the emotional disclosure group; in contrast, no group differences in PTSD were found among highly acculturated participants.
Conclusions
Our findings highlight the important role of sub-ethnic cultural orientation in the efficacy of psychosocial interventions targeting immigrant populations.
Trial Registration
ClinicalTrials.gov Identifier: NCT03546673
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Research has documented elevated levels of post-traumatic stress disorder (PTSD) among cancer survivors [1], including symptoms of re-experiencing (recurrent and intrusive thoughts about cancer and the subsequent emotional distress), arousal (heightened anxiety and irritability), and avoidance (increased efforts of avoiding situations that could trigger the memories of cancer) [2]. The PTSD symptoms could be caused by the unexpected diagnosis of cancer and the perceived uncertainty about the future [3], and these symptoms can last years after cancer diagnosis [4, 5]. Prolonged PTSD symptoms can negatively affect psychological adjustment among cancer survivors [6].
Over the recent decade, expressive writing has been increasingly studied for its effects on cancer patients’ physical and psychological well-being [7]. In a typical expressive writing intervention, participants are randomly assigned to an intervention and a control group to write about a topic. Participants in the intervention group are typically asked to write about their deepest thoughts and feelings related to their cancer experience (emotional disclosure), perceived benefits obtained from their cancer experience (cognitive reappraisal), or their stress coping experience. Participants in the control group are asked to either write objectively about the cancer diagnosis and treatment experience or write about a non-cancer topic such as daily activities. Although cultural sensitivity to psychosocial interventions has received increasing attention in the past decade [8], most expressive writing studies were conducted among non-Hispanic Whites. Although the Asian American population is increasing in the USA [9] and breast cancer incidence rates have been rapidly rising among Asian Americans [10], very limited research has been conducted to test the efficacy of expressive writing among Asian American breast cancer survivors [11]. Asian American breast cancer survivors tend to have smaller social networks and experience more difficulty in getting social support than White survivors do [12]. They are also inclined not to share their feelings related to cancer experience to prevent causing emotional burden to others and disrupting interpersonal harmony [13]. Considering the social challenges that Asian American breast cancer survivors frequently encounter, expressive writing may be an optimal intervention for this minority group.
Despite the increasing empirical attention to the benefits of expressive writing among cancer patients, few studies have examined its efficacy on PTSD symptoms. In an expressive writing intervention study for Chinese American breast cancer survivors, Gallagher and colleagues [14] found that participants in the cancer-fact group had better post-intervention outcomes of PTSD than the emotional disclosure group. This finding differed from previous studies among non-Hispanic Whites [15,16,17] that found greater benefits of emotional disclosure writing compared to cancer-fact writing. These mixed findings suggest that the therapeutic effects of expressive writing may vary depending on participants’ cultural orientation.
Compared to European culture, Asian culture tends to value collectivism and discourage emotional expression. Such negative attitudes toward emotional expression may result from the concerns that expressing emotions, especially negative ones, may damage interpersonal relationships or disrupt group harmony [18]. Thus, Asians tend to consider emotional expression as less acceptable, and may not find it comfortable to write about their emotional feelings compared to people in European culture [19,20,21,22]. As a result, Asians may engage less in the writing process, and thus may gain less psychological benefit from expressive writing compared with non-Hispanic Whites. Consistent with this suggestion, the existing studies on expressive writing indicated that writing about deepest feelings was not as beneficial to Asians as to non-Hispanic Whites. For example, Lu and Stanton [23] found that Asian American undergraduates benefited more from writing focused on cognitive reappraisal and writing that combined emotional disclosure and cognitive reappraisal compared to the neutral topic writing, but not from emotional disclosure writing. Knowles et al. [24] found that written emotional disclosure predicted fewer self-reported illness symptoms among European American undergraduates but not among Asian American undergraduates. In a study by Lu et al. [25] on Chinese American breast cancer survivors, cancer-fact writing, which facilitates cognitive reappraisal and re-integration, predicted higher quality of life compared to emotional disclosure writing and a writing condition that combined stress coping, benefit finding, and emotional disclosure.
Despite the above empirical evidence of macro cultural differences in the therapeutic effect of expressive writing, no research has investigated whether the efficacy of expressive writing is moderated by differential cultural values within the same ethnicity. Immigrants with the same cultural origin can vary in their engagement to the host culture [26]. For example, Chinese immigrants who reside near Chinatowns may be more isolated in their cultural enclaves and thus tend to have fewer opportunities to acculturate to American mainstream culture, compared with Chinese who live in predominately White communities. In addition, Chinese immigrants who have lived in the USA longer may be more receptive to American mainstream culture than those who came to the USA recently. These within-ethnicity differences in acculturation level may lead to differential values in regard to emotional expression [22]. In particular, Chinese immigrants who are better acculturated to the American mainstream culture may hold greater values about emotional expression, and thus may feel more comfortable and more engaged in writings about their inner feelings. In contrast, less acculturated Chinese immigrants tend to endorse emotional suppression to a greater extent, and may be less comfortable and less engaged in writing about their emotions [20, 27]. In addition, our previously published work [14, 25] found better quality of life and overall PTSD score in the cancer-fact writing condition relative to the emotional disclosure and self-regulation writing for Chinese American breast cancer survivors, suggesting that cognitive processing may be more beneficial than emotional disclosure for this population. Based on these findings, it is likely that since low acculturated Chinese American breast cancer survivors tend be restraint and uncomfortable expressing their emotions, they may benefit less from writings that focus on emotional disclosure alone. Indeed, previous research found that ambivalence over emotional expression (desiring to express emotions but fearing the consequence of doing so) predicted lower quality of life and higher depression for highly acculturated participants but not for lowly acculturated participants, suggesting that lowly acculturated Chinese Americans may benefit less from emotional disclosure compared to highly acculturated counterparts [28].
The Present Study
A previous study using the same data has examined the overall longitudinal effects of expressive writing on the total PTSD symptom score among Chinese American breast cancer survivors [14]. The present study expanded this work by investigating how the efficacy of expressive writing on different PTSD symptom clusters (re-experiencing, avoidance, and arousal) would vary depending on participants’ within-ethnicity cultural orientation. We hypothesized that acculturation would moderate the effect of expressive writing on PTSD symptoms. Specifically, for highly acculturated Chinese American breast cancer survivors, who tend to desire emotional expression, emotional disclosure writing and self-regulation writing (a condition that combined emotional disclosure, benefit finding, and stress coping) would deliver more benefits than cancer-fact writing in reducing PTSD symptoms. In contrast, for lowly acculturated participants, who tend to restrain emotions, the cancer-fact writing would be more beneficial than emotional disclosure writing. For the effect of self-regulation among lowly acculturated participants, we envision two possibilities. On the one hand, because the self-regulation writing contained a component of emotional disclosure, it may be less beneficial than the cancer-fact writing for lowly acculturated participants. On the other hand, because the self-regulation writing also involved cognitive reappraisal, it may produce more benefits than emotional disclosure writing. We tested these hypotheses based on data from a published trial examining the effects of expressive writing on quality of life among Chinese American breast cancer survivors [25].
Methods
Participants and Procedure
The details about the recruitment process, the experimental design, and a study flow chart were reported in the previously published trial [25]. The present study has been approved by the appropriate institutional research ethics committee and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Ninety-six female Chinese American breast cancer survivors were recruited from local communities in the USA. Inclusion requirements were as follows: (1) a diagnosis of stage 0–III breast cancer; (2) completion of primary medical treatment within 4 years at the time of baseline; and (3) being comfortable with writing and speaking in Chinese. Table 1 presents the demographic and medical characteristics of the participants.
Informed consent was obtained from all individual participants included in the study. Participants were randomly assigned to three writing conditions and completed the writing tasks once a week in three consecutive weeks. At each weekly writing session, participants were asked to follow the assigned writing instructions for that week and write continuously for up to 30 min, or until they completed one page of essay. The emotional disclosure group wrote about their deepest thoughts and feelings related to their breast cancer experience for 3 weeks. The self-regulation group wrote about deepest thoughts and feelings in Week 1, their most stressful experience and coping strategies in Week 2, and the positive thoughts and feelings they experienced since cancer diagnosis in Week 3. The cancer-fact group wrote about the details of their cancer diagnosis and treatment experience objectively for 3 weeks. PTSD symptoms were measured at baseline and at 1-, 3-, and 6-month follow-ups after the intervention. Acculturation was measured at baseline, as the only moderator investigated in the present study. All 96 participants completed the baseline questionnaire, with 74 completing the writing task (nself-regulation = 25, nemotional-disclosure = 26, ncancer-fact = 23). A total of 72 participants completed the 1-month follow-up assessment (nself-regulation = 24, nemotional-disclosure = 25, ncancer-fact = 23), 71 participants completed the 3-month follow-up assessment (nself-regulation = 24, nemotional-disclosure = 24, ncancer-fact = 23), and 70 participants completed the 6-month follow-up assessment (nself-regulation = 24, nemotional-disclosure = 23, ncancer-fact = 23). Post-hoc power analysis indicated that based on a sample size of 70 at the 6-month follow-up session, we had 52% power to detect a small effect (f2 = .06) and had 89% power to detect a medium effect (f2 = .15).
Measures
PTSD Symptoms
PTSD symptoms were measured using the PTSD Symptom Scale—Self report (PSS-SR) [29], which consists of three subscales that measure re-experiencing, avoidance, and arousal. Participants rated the severity of the symptoms described in each item on a four-point scale from (0) not at all to (3) almost always. Sum scores were computed for each symptom cluster, with a higher score indicating more severe symptom. As recommended by Foa et al. (1993), a specific PTSD symptom may be present if the item corresponding to the symptom is scored 1 or greater. Based on DSM-IV-TR criteria [3], an individual may have PTSD when at least 1 re-experiencing, 3 avoidance, and 2 arousal symptoms are reported. In the current study, the Cronbach’s α values at all measurement sessions ranged from .864 to .871 (re-experiencing), .794 to .875 (avoidance), and .805 to .857 (arousal), suggesting adequate internal reliability.
Acculturation
The Stephenson Multigroup Acculturation Scale—Dominant Society Immersion subscale [30] was used to measure acculturation. To reduce participants’ burden, five items with top loadings on the Dominant Society Immersion factor were selected, including “I attend social functions with (Anglo) American people,” “I have many (Anglo) American acquaintances,” “I speak English at home,” “I think in English,” and “I know how to prepare American food.” Participants rated their agreement on each item on a four-point scale from (0) false to (3) true. A higher average score indicates higher acculturation to American mainstream culture. The scale had adequate reliability in the present study (Cronbach’s α = .844).
Manipulation Check
After completing the last writing session, participants were asked three manipulation check questions, including how personal the writings were, how much they revealed emotion in the writings, and how much the writings increased their understanding about the disease. Participants rated the degree of each item on a seven-point likert scale from 0 (not at all) to 6 (a great deal).
Analysis Strategy
We began by conducting manipulation check and attrition analysis to compare potential baseline differences between completers and dropouts. Second, we described the descriptive statistics of the main variables. For hypothesis testing, a series of linear regressions were conducted using SPSS 24.0 with each PTSD symptom cluster as a dependent variable at each follow-up session. The predictors included acculturation, writing group, and the interaction between acculturation and writing group. The baseline score of each PTSD symptom cluster was added as a covariate. To identify potential demographic or medical covariates, bivariate correlations were tested between the dependent variables and demographic and medical information. All predictors and covariates were centered to reduce multicollinearity. The writing groups were dummy coded. For each dependent variable, the demographic and medical covariates, as well as baseline PTSD symptoms were entered in Step 1, acculturation and writing group dummy codes were entered in Step 2, and the interaction between group and acculturation was entered in Step 3. Regression models were first run with the cancer-fact group as the reference group, and then run again with the self-regulation group as the reference group.
Results
Manipulation Check
We conducted ANOVA to examine the group difference in participants’ ratings on the extent to which their writing essays were personal, emotion revealing, and improved their understanding about the disease. As was also reported in Lu et al. [25], there were significant group differences in only the rating on emotion revealing. The cancer-fact group (M = 1.55, SD = .91) revealed less emotion than the self-regulation group (M = 4.04, SD = 1.17) and the emotional disclosure group (M = 4.71, SD = 1.31), all p < .001. There was no difference between the self-regulation group and the emotional disclosure group, p = .112.
Attrition Analysis Between the Completers and the Dropouts
Independent-samples t test and chi-square test were conducted to compare participants who completed the follow-up assessments and those who did not. The two groups did not differ significantly in demographic variables (age, education, employment status, and marital status), medical variables (cancer stage, time since diagnosis, and treatment completed), acculturation score, and baseline scores of PTSD symptom clusters (all p > .07).
Descriptive Statistics and Correlation of Main Variables
Table 1 presents demographic and clinical characteristics of the study sample. The average age of the participants was 54.54 years. A majority of the participants (62.5%) were immigrants from China mainland and were married (71.9%). Education level was quite high, with 33.3% of the sample having a high school education and 47.9% having college education. Many participants had either stage I (30.1%) or stage II (41.7%) disease. Table 2 presents the means and standard deviations (SDs) of each PTSD symptom cluster at each measurement session, and acculturation at baseline. The SDs and the ranges of PTSD symptom clusters and acculturation suggest adequate variability of PTSD symptoms and acculturation of the study sample.
Based on DSM-IV-TR criteria [3], 59 (61.5%) participants were above the threshold for a likely diagnosis of PTSD. Based on the criteria for the presence of PTSD symptoms as recommended by Foa et al. [29], 84.4% of participants had at least one re-experiencing symptom, 87.5% of participants had at least one avoidance symptom, and 90.6% of participants had at least one arousal symptom. These findings suggest that PTSD was highly prevalent among this sample.
Table 3 presents the correlation matrix of major variables. Results of bivariate correlations indicated that cancer stage was positively related with re-experiencing at baseline and the 1- and 3-month follow-ups (rs = .25–.30, ps < .05), and arousal at baseline (r = .22, p < .05); household income was negatively related with re-experiencing at the 3-month follow-up (r = − .27, p < .05); and education was negatively related with re-experiencing (r = − .279, p < .01) and arousal (r = − .264, p < .05) at baseline. Based on the correlation results, cancer stage was added as a covariate for re-experiencing (at baseline and all follow-up sessions) and arousal (at baseline); household income was added as a covariate for re-experiencing (at 3-month follow-up); and education was included as a covariate for re-experiencing and arousal (at baseline).
Moderation of Acculturation on the Efficacy of Expressive Writing
Results of bivariate correlations indicated that cancer stage was positively related with re-experiencing at baseline and the 1- and 3-month follow-ups (rs = .25–.30, ps < .05), and arousal at baseline (r = .22, p < .05); household income was negatively related with re-experiencing at the 3-month follow-up (r = − .27, p < .05); and education was negatively related with re-experiencing (r = − .28, p < .01) and arousal (r = − .26, p < .05) at baseline. Based on the correlation results, cancer stage was added as a covariate for re-experiencing (at baseline and all follow-up sessions) and arousal (at baseline); household income was added as a covariate for re-experiencing (at 3-month follow-up); and education was included as a covariate for re-experiencing and arousal (at baseline).
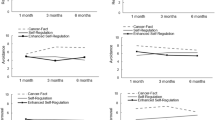
Figure 1 presents the results of moderation of acculturation on the effect of writing group in influencing re-experiencing, avoidance, and arousal symptoms at the 6-month follow-up. There were no main effects of acculturation on any PTSD symptom cluster at any measurement session (ps > .100). For interaction effects, as recommended by Aiken and West [31], simple slope tests were conducted to examine the group difference in PTSD symptoms at each follow-up based on high vs. low acculturation (1 SD above vs. below the mean, respectively). For re-experiencing, acculturation moderated the writing effect (emotional disclosure vs. self-regulation) at the 6-month follow-up (β = − 0.23, p = .041). Simple slope tests indicated that for low acculturated participants, the self-regulation group had lower re-experiencing than the emotional disclosure group (p = .038); in contrast, for highly acculturated participants, there was no difference between the two groups (p = .432). For avoidance, acculturation moderated the writing effect (emotional disclosure vs. cancer-fact) at the 6-month follow-up (β = − .38, p = .012). For low acculturated participants, the cancer-fact group had lower avoidance than the emotional disclosure group (p = .010); in contrast, for highly acculturated participants, there was no difference between the two groups (p = .239). For arousal, acculturation moderated the writing effect (emotional disclosure vs. cancer-fact) at both the 3-month (β = − .31, p = .030) and 6-month follow-ups (β = − .35, p = .014) and the writing effect (emotional disclosure vs. self-regulation) at the 6-month follow-up (β = − 0.30, p = .02). At the 3-month follow-up, for low acculturated participants, the cancer-fact group had lower arousal than the emotional disclosure group (p = .023); for highly acculturated participants, there was no difference between the emotional disclosure group and the cancer-fact group. Similarly, at the 6-month follow-up, for low acculturated participants, both the cancer-fact group (p = .001) and the self-regulation group (p = .016) had lower arousal than the emotional disclosure group; in contrast, for highly acculturated participants, there were no group differences (ps > .10). No other interaction effects were found (ps > .05).

Moderation of acculturation on the effect of writing group in influencing re-experiencing, avoidance, and arousal symptoms at 6-month follow-up session
Discussion
The present study took the first step in investigating the moderation of acculturation on the effect of expressive writing on PTSD symptoms among Chinese American breast cancer survivors. The findings suggest that acculturation moderates the effect of expressive writing among this underserved population. As expected, among lowly acculturated participants, the cancer-fact and self-regulation groups showed less severe PTSD symptoms than the emotional disclosure group at the 3-month and 6-month follow-up sessions; in contrast, our hypothesis regarding highly acculturated participants was not supported. No condition differences in PTSD symptoms were found among highly acculturated participants.
Previous research suggests that the therapeutic effect of expressive writing depends on participants’ cultural background. Although writing about deepest feelings related to the traumatic cancer experience benefited European Americans in physical and psychological well-being, these benefits were not observed among Asian Americans [23, 24]. This cultural difference in responsiveness to emotional disclosure may result from the cultural difference in values about emotional expression. Specifically, European culture values individualism and self-assertion and encourages emotional expression in social interactions [32, 33]. In contrast, Asian culture values collectivism and group congruence and encourages suppressing emotions (especially negative ones) to avoid the risk of disrupting group harmony [19, 22]. Due to these cultural differences in attitudes toward emotional expression, Asian Americans may feel less comfortable in writing about innermost feelings and thus may restrict the potential benefits of emotional disclosure writing, compared with European Americans.
Our findings add to the current literature about cultural difference and suggest that differential cultural values within the same ethnicity background also moderate the efficacy of expressive writing. In the present study, participants had lived in the USA for various time periods and may have varied in degree of engagement with American mainstream culture. Thus, they may hold different values toward emotional expression, which may moderate the effect of expressive writing that involves emotional disclosure.
For lowly acculturated participants, our hypothesis was supported that the cancer-fact writing group displayed less severe PTSD symptoms than the emotional disclosure group for avoidance at 6-month follow-up, and for arousal at both 3-month and 6-month follow-ups. These findings were in line with previous studies that found more adaptive psychological outcomes in the cancer-fact condition than emotional disclosure condition for Chinese American breast cancer survivors [14, 25].
Among the lowly acculturated, better outcome in the self-regulation condition was also observed compared to the emotional disclosure condition for re-experiencing and arousal at 6-month follow-up. Given that both the self-regulation writing and the cancer-fact writing involve cognitive processing, our finding suggests that expressive writings that involve cognitive processing are more beneficial than emotional expression alone for lowly acculturated Chinese American breast cancer survivors. This finding is also in line with the cross-cultural studies that found cognitive reappraisal-based writing was more beneficial for Asians than European Americans [23]. The process of finding benefits, ruminating the stress coping experience, and confiding the cancer facts may provide an opportunity for lowly acculturated Chinese American breast cancer survivors to make sense of the cause of cancer, to reappraise the cancer experience and themselves in a more positive way, and thus develop new perspective and new goals to adapt to a new life.
Contrary to our hypothesis, we did not find significant group differences in PTSD symptoms for highly acculturated participants. One plausible explanation for the absence of benefits of emotional disclosure and self-regulation writing for highly acculturated participants may be that the relative receptiveness to American main stream culture may not suffice to offset the strong collectivist background in which the participants were raised. The youngest immigration age for our sample was 15 years old. Thus, it is reasonable to believe that although the highly acculturated participants endorse American main stream culture to a greater extent than their lowly acculturated counterparts, they may still hold relatively strong collectivist beliefs and may be more restraint of emotional disclosure compared to non-Hispanic Whites; these factors may restrict the potential benefit of writing conditions that involve emotional disclosure. It is also possible that the lack of group differences among highly acculturated participants might be due to the insufficient power. As is indicated by the post-hoc analysis, the sample at the 6-month follow-up session may be underpowered to detect very small effects. Future research is needed to confirm our findings using a larger study sample. Together, our findings shed light on the important role of within-ethnicity cultural orientation in evaluating psychosocial intervention programs targeting immigrants.
Although the cancer-fact writing condition was treated as the control group in the present study and some previous studies among non-Hispanic White breast cancer patients [17, 34,35,36], it may produce therapeutic effects among Chinese American breast cancer survivors. Pennebaker [37] posited that writing about trauma-related thoughts and feelings provides an opportunity to make sense and gain insights from the traumatic event and helps integrate the upsetting experience into self-schema. Due to cultural and language barriers, Chinese American cancer survivors tend to experience more difficulties in communicating with health care providers about their questions and concerns of cancer diagnosis and treatment [12]. These obstacles in communication may result in ambiguous and fragmented perceptions about their disease and health condition. Writing privately about the detailed diagnosis and treatment experience provides Chinese American cancer survivors an opportunity to organize and integrate the traumatic experience into their self-schema, make sense of the cancer experience, and gain insights from the cancer experience. As a result, this cognitive integration process may help to reduce the feelings of self-constraint, increase self-acceptance of the traumatic event, and eventually reduce distress. Supporting this explanation, our previous study on the same population [25] found significantly more insight- and causation-related words in the writing essays of the cancer-fact group than the emotional disclosure group. In sum, our findings, together with the existing literature, suggest that for low acculturated Chinese American breast cancer survivors, expressive writing that involves cognitive integration and cognitive reappraisal may be more optimal in reducing PTSD symptoms than writing that focuses on disclosing deepest emotions related to cancer.
Our findings suggest that the better outcomes produced by self-regulation writing and cancer-fact writing in comparison to emotional disclosure were most prominent at the 6-month follow-up, rather than at the shorter-term follow-ups. One plausible explanation may pertain to the cognitive pathways through which the expressive writing improves psychological well-being, including re-evaluating the cause of cancer, reappraising the impact of cancer, and employing cognitive coping strategies. It can often take time for individuals to integrate these cognitive processes into one’s existing schema and develop alternative perspectives to reduce distress. Such cognitive integration and coping processes may be more effortful and time consuming for Chinese American breast cancer survivors than non-Hispanic Whites as they have less access to social support and mental health resources due to cultural and language barriers [38,39,40]. As such, future research should consider incorporating culturally sensitive social resources into expressive writing to maximize the intervention effect, such as social support groups and trainings of emotion regulation and stress coping.
Conclusions
Study Limitations
The present study has several limitations. First, due to attrition, the sample size was relatively small at the follow-up sessions. The small sample size at the follow-up sessions may restrict the power to detect small effects, which may account for the lack of writing effects for highly acculturated participants. Future research is needed to replicate the results among a larger sample of this population. Second, due to the dropouts at follow-up sessions, the analysis results may be biased if data were not missing at random. Third, the observed benefits of cancer-fact writing suggest that it has therapeutic effects for Chinese American breast cancer survivors and thus should not be a true control condition for this sample [25]. Future research will profit from adding a neutral control condition, such as writing about daily activities. Fourth, we did not assess participants’ comfort or willingness in disclosing emotions. Therefore, it remains a question whether the observed difference in the writing effect between high- and low-acculturated participants were accounted for by participants’ willingness to express emotions. For future research, adding participants’ willingness or comfort in writing about emotions as a covariate to test the residual effects of acculturation should be considered. Fifth, one must be cautious when attempting to generalize the findings to other Asian immigrants, such as Japanese and Koreans, or Chinese who reside in China. Participants in the present study had lived in the USA for various time periods, and thus may differ from their non-immigrant Chinese counterparts in multiple aspects, such as socioeconomic status and cultural values. These factors are likely to influence the efficacy of expressive writing.
Clinical Implications
Notwithstanding these limitations, the present study is the first attempt to investigate acculturation as a moderator for expressive writing. The findings advance our understanding about the role of culture in influencing the efficacy of psychosocial interventions such as expressive writing. Our findings suggest that not only the macro cultural background but also the within-ethnicity cultural orientation could moderate the efficacy of expressive writing on PTSD symptoms among Chinese American breast cancer survivors. Our study highlights the need for researchers’ attention to cultural sensitivity when designing and evaluating psychosocial intervention programs among clinical immigrant populations.
References
Kangas M, Henry JL, Bryant RA. Posttraumatic stress disorder following cancer: a conceptual and empirical review. Clin Psychol Rev. 2002;22(4):499–524. https://doi.org/10.1016/S0272-7358(01)00118-0.
Wu X, Wang JR, Cofie R, Kaminga AC, Liu AZ. Prevalence of posttraumatic stress disorder among breast cancer patients: a meta-analysis. Iran J Public Health. 2016;45(12):1533–44.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: Text Revision; 2000.
Dahl AA, Østby-Deglum M, Oldenburg J, Bremnes R, Dahl O, Klepp O, et al. Aspects of posttraumatic stress disorder in long-term testicular cancer survivors: cross-sectional and longitudinal findings. J Cancer Surviv. 2016;10(5):842–9. https://doi.org/10.1007/s11764-016-0529-4.
Jim HSL, Jacobsen PB. Posttraumatic stress and posttraumatic growth in cancer survivorship: a review. Cancer J. 2008;14(6):414–9. https://doi.org/10.1097/PPO.0b013e31818d8963.
Horowitz MJ, Field NP, Classen CC. Stress response syndromes and their treatment. In: Goldberger L, Breznitz S, Goldberger L, Breznitz S, editors. Handbook of stress: theoretical and clinical aspects. 2nd ed. New York: Free Press; 1993. p. 757–73.
Merz EL, Fox RS, Malcarne VL. Expressive writing interventions in cancer patients: a systematic review. Health Psychol Rev. 2014;8(3):339–61. https://doi.org/10.1080/17437199.2014.882007.
Sue S, Zane N, Nagayama Hall GC, Berger LK. The case for cultural competency in psychotherapeutic interventions. Annu Rev Psychol. 2008;60(1):525–48. https://doi.org/10.1146/annurev.psych.60.110707.163651.
Annual estimates of the resident population by sex, race, and Hispanic origin for the United States, states, and counties: April 1, 2010 to July 1, 2014 (2014) http://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?src. Accessed 31 Jan 2018.
Gomez SL, Von Behren J, McKinley M, Clarke CA, Shariff-Marco S, Cheng I, et al. Breast cancer in Asian Americans in California, 1988–2013: increasing incidence trends and recent data on breast cancer subtypes. Breast Cancer Res Treat. 2017;164(1):139–47. https://doi.org/10.1007/s10549-017-4229-1.
Frattaroli J. Experimental disclosure and its moderators: a meta-analysis. Psychol Bull. 2006;132(6):823–65. https://doi.org/10.1037/0033-2909.132.6.823.
Wen K-Y, Fang CY, Ma GX. Breast cancer experience and survivorship among Asian Americans: a systematic review. J Cancer Surviv. 2014;8(1):94–107. https://doi.org/10.1007/s11764-013-0320-8.
Kagawa-Singer M, Wellisch DK. Breast cancer patients’ perceptions of their husbands’ support in a cross-cultural context. Psycho-Oncology. 2003;12(1):24–37. https://doi.org/10.1002/pon.619.
Gallagher MW, Long LJ, Tsai W, Stanton AL, Lu Q. The unexpected impact of expressive writing on posttraumatic stress and growth in Chinese American breast cancer survivors. J Clin Psychol. 2018;74(10):1673–86. https://doi.org/10.1002/jclp.22636.
De Moor C, Sterner J, Hall M, Warneke C, Gilani Z, Amato R, et al. A pilot study of the effects of expressive writing on psychological and behavioral adjustment in patients enrolled in a phase II trial of vaccine therapy for metastatic renal cell carcinoma. Health Psychol. 2002;21(6):615–9. https://doi.org/10.1037//0278-6133.21.6.615.
Henry EA, Schlegel RJ, Talley AE, Molix LA, Bettencourt BA. The feasibility and effectiveness of expressive writing for rural and urban breast cancer survivors. Oncol Nurs Forum. 2010;37(6):749–57. https://doi.org/10.1188/10.ONF.749-757.
Stanton AL, Danoff-Burg S, Sworowski LA, Collins CA, Branstetter AD, Rodriguez-Hanley A, et al. Randomized, controlled trial of written emotional expression and benefit finding in breast cancer patients. J Clin Oncol. 2002;20(20):4160–8. https://doi.org/10.1200/JCO.2002.08.521.
Wierzbicka A. Emotion, language, and cultural scripts. In: Kitayama S, Markus HR, editors. Emotion and culture: Empirical studies of mutual influence. Washington DC: American Psychological Association; 1994. p. 133–196. https://doi.org/10.1037/10152-004.
Butler EA, Lee TL, Gross JJ. Emotion regulation and culture: are the social consequences of emotion suppression culture-specific? Emotion. 2007;7(1):30–48. https://doi.org/10.1037/1528-3542.7.1.30.
Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003;85(2):348–62. https://doi.org/10.1037/0022-3514.85.2.348.
Okazaki S. Self-other agreement on affective distress scales in Asian Americans and White Americans. J Couns Psychol. 2002;49(4):428–37. https://doi.org/10.1037//0022-0167.49.4.428.
Chen SH, Zhou Q, Main A, Lee EH. Chinese American immigrant parents’ emotional expression in the family: relations with parents’ cultural orientations and children’s emotion-related regulation. Cult Divers Ethn Minor Psychol. 2014;21(4):619–29. https://doi.org/10.1037/cdp0000013.
Lu Q, Stanton AL. How benefits of expressive writing vary as a function of writing instructions, ethnicity and ambivalence over emotional expression. Psychol Health. 2010;25(6):669–84. https://doi.org/10.1080/08870440902883196.
Knowles ED, Wearing JR, Campos B. Culture and the health benefits of expressive writing. Soc Psychol Personal Sci. 2011;2(4):408–15. https://doi.org/10.1177/1948550610395780.
Lu Q, Wong CC, Gallagher MW, Tou RY, Young L, Loh A. Expressive writing among Chinese American breast cancer survivors: a randomized controlled trial. Health Psychol. 2017;36(4):370–9. https://doi.org/10.1037/hea0000449.
Miller MJ. A bilinear multidimensional measurement model of Asian American acculturation and enculturation: implications for counseling interventions. J Couns Psychol. 2007;54(2):118–31. https://doi.org/10.1037/0022-0167.54.2.118.
Wei M, Su JC, Carrera S, Lin SP, Yi F. Suppression and interpersonal harmony: a cross-cultural comparison between Chinese and European Americans. J Couns Psychol. 2013;60(4):625–33. https://doi.org/10.1037/a0033413.
Tsai W, Lu Q. Acculturation matters in the relation between ambivalence over emotional expressions and well-being among Chinese American breast cancer survivors. Qual Life Res. 2017;26(10):2755–62. https://doi.org/10.1007/s11136-017-1618-1.
Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J Trauma Stress. 1993;6(4):459–73. https://doi.org/10.1002/jts.2490060405.
Stephenson M. Development and validation of the Stephenson Multigroup Acculturation Scale (SMAS). Psychol Assess. 2000;12(1):77–88. https://doi.org/10.1037//1040-3590.12.1.77.
Aiken LS, West SG. Multiple regression: testing and interpreting interactions. Thousand Oaks: Sage Publications, Inc; 1991.
Markus HR, Kitayama S. Culture and the self: implications for cognition, emotion, and motivation. Psychol Rev. 1991;98(2):224–53. https://doi.org/10.1037/0033-295X.98.2.224.
Matsumoto D. Cultural similarities and differences in display rules. Motiv Emot. 1990;14(3):195–214. https://doi.org/10.1007/BF00995569.
Creswell JD, Suman L, Annette LS, Shelley ET, Julienne EB, David KS. Does self-affirmation, cognitive processing, or discovery of meaning explain cancer-related health benefits of expressive writing? Personal Soc Psychol Bull. 2007;33(2):238–50. https://doi.org/10.1177/0146167206294412.
Craft MA, Davis GC, Paulson RM. Expressive writing in early breast cancer survivors. J Adv Nurs. 2013;69(2):305–15. https://doi.org/10.1111/j.1365-2648.2012.06008.x.
Low CA, Stanton AL, Bower JE, Gyllenhammer L. A randomized controlled trial of emotionally expressive writing for women with metastatic breast cancer. Health Psychol. 2010;29(4):460–6. https://doi.org/10.1037/a0020153.
Pennebaker JW. Putting stress into words: health, linguistic, and therapeutic implications. Behav Res Ther. 1993;31(6):539–48. https://doi.org/10.1016/0005-7967(93)90105-4.
Leong FT, Lau AS. Barriers to providing effective mental health services to Asian Americans. Ment Health Serv Res. 2001;3(4):201–14.
Warmoth K, Cheung B, You J, Yeung NCY, Lu Q. Exploring the social needs and challenges of Chinese American immigrant breast cancer survivors: a qualitative study using an expressive writing approach. Int J Behav Med. 2017;24(6):827–35. https://doi.org/10.1007/s12529-017-9661-4.
Lee S, Chen L, Ma GX, Fang CY, Oh Y, Scully L. Challenges and needs of Chinese and Korean American breast cancer survivors: in-depth interviews. N Am J Med Sci. 2013;6(1):1–8. https://doi.org/10.7156/najms.2013.0601001.
Funding
This research was funded by the American Cancer Society (MRSGT-10-011-01-CPPB: PI Qian Lu).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chu, Q., Wong, C.C.Y. & Lu, Q. Acculturation Moderates the Effects of Expressive Writing on Post-Traumatic Stress Symptoms Among Chinese American Breast Cancer Survivors. Int.J. Behav. Med. 26, 185–194 (2019). https://doi.org/10.1007/s12529-019-09769-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-019-09769-4