
Abstract
Background
Habit formation has been proposed as a way to maintain behaviour over time.
Purpose
Recent evidence suggests that constructs additional to repeated performance may predict physical automaticity, but no research has yet explored possible direct impacts of intention, planning, affect, and perceived behavioural control (PBC) on automaticity.
Method
In a prospective study over a 2-week period amongst 406 undergraduate students (M age = 21.5 years [SD = 2.59], 27.4 % males), we investigated main and interaction effects of past exercise behaviour, PBC, intention, planning, and affect on exercise automaticity.
Results
Results showed that — controlling for past behaviour — PBC, affect, and planning were significant and positive predictors of exercise automaticity. Decomposing a significant interaction between PBC and planning when to exercise revealed that planning became less predictive of exercise automaticity at higher levels of PBC.
Conclusion
Findings show that exercise automaticity is predicted by repeated performance and social–cognitive constructs. Further, interactions between social–cognitive predictors may be different for behavioural automaticity than for behavioural frequency.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Although engaging in sufficient exercise has various health benefits, the majority of people are currently insufficiently active to obtain these health benefits. Understanding modifiable determinants of exercise behaviour is a prerequisite for developing evidence-based interventions to target increased exercise adherence. Determinant studies have often been informed by a range of social–cognitive theoretical models, of which the theory of planned behaviour (TPB) [1] is most frequently utilised. The TPB models (exercise) behaviour as an endpoint of a reasoned process, in which an individual formulates an intention to act. This intention is based on the weighing of pros (e.g., enhanced health) and cons (e.g., fatigue) and considers approval or disapproval from significant others as well as facilitators (e.g., sufficient time to exercise) and barriers (e.g., bad weather) when deciding whether to engage in exercise behaviour. As a result, interventions that target increases in exercise behaviour have often sought to raise knowledge of benefits of exercise behaviour or how to cope with barriers and restraints.
Previous exercise behaviour change interventions, however, have only been modestly successful: differences between experimental and control conditions often do not exceed the small effect-size threshold. Furthermore, most of these positive intervention effects tend to be short-lived, often not exceeding a 6-month post-intervention period, when participants either drop out or continue at a suboptimal level [2]. This may be due to the effort required to initiate intentional behaviour change and the depletion of the limited cognitive control resources required to consciously sustain intentional action [3]. Recent research suggests that the development of habits may help to sustain behaviour over the long term. Habits are behaviours which, through repeated prior performance in the presence of stable contextual cues, have become automatic responses to those cues [4, 5]. Repetition in stable contexts strengthens the association between the situational cue and the behavioural action. Once this association is sufficiently strong, the mere perception of that context will automatically activate the associated habituated responses and a habit is said to have formed. Unlike intentionally driven behaviours, which require conscious effort to be enacted and maintained, habitual actions are characterised by automaticity, as expressed in uncontrollability and immediacy of enactment upon encountering associated cues [6]. For this reason, habitual responses can override intentional responses in determining actions [7, 8]. This has led commentators to suggest that the development of automaticity (i.e., habit) for newly adopted and health-enhancing behaviours is a desirable outcome for behaviour change interventions [5, 7].
Because habits are suggested to form through context-dependent repetition, social cognitive variables should impact on automaticity indirectly, by influencing the extent to which a behaviour is repeated over time. However, a recent study on automaticity development reported considerable variation in the time taken before newly initiated behaviours reached a plateau of automaticity, despite equal repetitions [9]. This effect also occurred for complex behaviours such as exercise and variables next to the mere number of behavioural repetitions may therefore determine strength of behavioural automaticity [9]. These variables may feasibly strengthen automaticity directly, independent of repetition history, or may interact with past behaviour, thus moderating the reinforcing value of each repetition on habit strength [10, 11]. For example, Gardner and Lally [10] showed that self-determined regulation had a direct effect on physical activity automaticity, independent of past behaviour, and also had a indirect effect by interacting with past behavioural frequency: repetition had a greater impact on automaticity when behaviours were regarded as more intrinsically motivating. The current body of evidence, however, is limited with regard to whether and which social cognitions outlined in popular models of human behaviour impact behavioural automaticity directly [10, 12]. Nevertheless, two constructs have consistently been shown to be strongly associated with (exercise) automaticity, namely action planning and positive affective attitudes. Both variables deserve further attention as predictors of automaticity.
Action planning is a prospective self-regulatory strategy in which an individual mentally links distinct responses to future environments, so that when those environments are encountered, the response is initiated. By emphasising this contextual cue, it has been suggested that action planning strategies mimic automatic responses derived from repetition [13]. Through this 'strategic automatization', planning when and where to act should delegate control of action from the individual to the contextual cue [14]. Evidence from laboratory and field studies indeed suggests that planning strategies ensure that opportunities for action are more likely to be detected and, once detected, action responses are faster and more precise [14–16]. For instance, Webb and Sheeran [15] used a cue-detection paradigm in a laboratory setting and found that those forming implementation intentions to detect the selected cue (e.g., the letter F or the number 3) were not only faster to respond to those cues, but also made fewer errors. In a field study on breast self-examination (BSE), Orbell et al. [16] instructed participants to formulate plans regarding when and where to perform BSE. One month after these instructions, participants had not only performed BSE just as they had specified, but these implementation intentions also mediated the effect of past BSE on future BSE behaviour. This latter finding suggests that action planning instructions operate similarly to how habits mediate past and future behaviour relationships [17]. In summary, by increasing the likelihood that repetition will be context-dependent, it is conceivable that planning when and where to act may play a role in automaticity over and above the influence of past behaviour.
Although increased action planning has been linked to positive changes in behavioural performance in a variety of behaviours such as regular physical activity [18, 19], exercise behaviour [20, 21], alcohol consumption [22] and diet [23], correlational and experimental action planning studies to date have mostly used behaviour, rather than automaticity, as a study outcome. One notable exception is an exercise intervention conducted amongst middle-aged rehabilitation patients [21], which showed that self-regulatory strategies lead to small-sized changes in exercise habit strength. However, this research has limited applicability to the general population because it focused on patients pursuing exercise as part of a rehabilitation regime. Understanding whether self-regulatory strategies are also important for exercise automaticity in other population segments that undertake exercise behaviour for preventive, rather than therapeutic purposes, is therefore needed.
With regard to positive affective attitudes, previous research has indicated that affective attitudes have medium-to-large effect-sized correlations with exercise habits [12, 24]. This strong relationship is likely due to palatable experiences with previous exercise behaviour [25], which may act as reinforcing rewards that both stimulate repeated [exercise] behaviour and strengthen the impact of repetition on automaticity [10, 11, 26]. That is, cognitive attitudes are based on behavioural beliefs about fairly long term consequences of exercising, whereas behavioural beliefs underlying affective attitudes are usually more immediate [27]. This means that affective attitudes are regularly reinforced when an individual exercises, which is likely to produce higher levels of behavioural consistency and increased chance of automaticity development. In addition, affective considerations surrounding a behaviour have been found to influence action impulsively, bypassing conscious deliberation processes [28], in a manner similar to that in which automaticity directs behaviour [5, 29]. In addition, Gardner and Lally's [10] study demonstrated the interplay between affective rewards and action in influencing physical activity automaticity among (young) adults: physical activity behaviours that were more intrinsically regulated, so resembling more internal enjoyment and satisfaction [30], were more likely to become automatic. A similar result has recently been provided by De Bruijn et al. [11], who showed that the fruit consumption behaviour — habit link was stronger when participants reported more positive implicit associations with behaviour. Thus, it would appear that behaviours that are more enjoyable and have more affective properties are prone to become more automatic. Despite this literature, little evidence is available into the influence of affective attitudinal components as outlined in the TPB on exercise automaticity.
The present study was therefore conducted with a focus on antecedents of exercise automaticity in a sample of university students. We sought to identify variables that have previously been shown to be associated with exercise habit, and may influence automaticity over and above past behaviour, or may interact with past behaviour (as a proxy for repetition) in determining exercise automaticity. Next to previous exercise behaviour, we explored the potential role of action planning and affective attitude as predictors of automaticity. It was also decided to model intention, perceived behavioural control (PBC), and exercise behaviour as potential antecedents of exercise automaticity for two reasons. First, research on intentions and habits in the exercise domain indicate that strong exercise intentions facilitate exercise habits, suggesting that habits need to be supplemented by intentions in the exercise domain [12, 31, 32]. Second, PBC reflects not only ease of (exercise) performance, but also control over behavioural performance [33] and has been found to be a strong correlate of exercise habits [12]. We also considered interactions between significant behavioural and social cognitive predictors of exercise automaticity.
Method
Participants and Procedures
Data using validated questionnaires from undergraduate students that participated for course credits were utilised in the present study. A two-wave data collection was used. At baseline, measures were taken of PBC, behaviour, intention, action planning items, and affective attitude towards engaging in sufficient exercise. At follow-up 2 weeks later, exercise automaticity was assessed. The study was announced during course meetings in which students were informed that the study would question them about (their views towards) exercise behaviour. Students were then sent an email containing a link to an online survey, which took around 10 min to complete. The link to the survey was also available on the course Blackboard website. At baseline, 586 participants (M = 21.6 years [SD = 2.28], 27.0 % males) provided data. Two weeks later, these participants were again contacted using email and via Blackboard course website. At this follow-up measurement, 406 participants (M = 21.5 years [SD = 2.59], 27.4 % males) provided follow-up data, indicating that 28.2 % dropped out. Female participants were more likely to discontinue participation (odds ratio [OR = 1.70]; 95 % confidence interval [CI], 1.10–2.64; p = 0.027), but age and study variables were unrelated to dropout (all p > 0.343). The institutional review board approved the study.
Measures
With the exception of exercise automaticity items, all items for social–cognitive constructs were worded in terms of engaging in sufficient exercise in the next 2 weeks. This was defined as meeting the international exercise guideline of ‘exercising on at least three occasions per week lasting at least 20 minutes per bout’ [34]: participants were instructed to keep this definition in their minds when answering the questions. Exercise behaviours were defined as activities that are strenuous in nature, which increase your heart rate, increases the chance of sweating and make it difficult to talk. Exercise automaticity was assessed using the Self-Report Behavioural Automaticity Index (SRBAI) [35], a subscale of four items from the Self-Report Habit Index (SRHI) [17] that has been identified to reliably measure automaticity. The SRHI has been validated against response frequency measures and indices of past behaviour [17], whilst the SRBAI was validated through a content validation task and re-analyses of previous SRHI applications [35]. Participants were requested to indicate to what extent they agreed (−3 = totally disagree, +3 = totally agree) with four statements, namely, ‘engaging in sufficient exercise is something’: (1) I do automatically, (2) I do without having to consciously remember, (3) I do without thinking, and (4) I start doing before I realise I am doing it (α = 0.91). Variables from the TPB were used following Ajzen's suggestions. Affective attitude towards sufficient exercise was assessed with three items that had different stems, namely very unpleasant (−3) or very pleasant (+3), very unenjoyable (−3) or very enjoyable (+3), and very stressful (−3) or very relaxing (+3) (α = 0.87). Intention towards sufficient exercise was assessed with two items, namely whether participants intended (−3 = no, definitely not; +3 = yes, definitely) and whether they were sure (−3 = totally disagree; +3 = totally agree) to engage in sufficient exercise (α = 0.83). Perceived behavioural control was assessed with two items that measured ease (−3 = very difficult; +3 = very easy) and controllability (−3 = definitely not under one's control; + definitely under one's control). This scale had good a internal reliability (α = 0.91). Three items assessed action planning, asking participants to indicate whether they had (−3 = no, definitely not, +3 = yes, definitely) made detailed plans of where, when, and with whom they were going to exercise. The individual planning items, rather than the mean of the three items, were modelled as predictors in order to identify whether specific types of cues — social (with whom), temporal (when) or situational (where) — would be most relevant for exercise automaticity. Finally, exercise behaviour was assessed with relevant items from the International Physical Activity Questionnaire [36], where participants were asked to indicate how many times they engaged in vigorous exercise behaviour in the previous 4 weeks and the time spent exercising on each occasion. An average amount of exercise in minutes per week was calculated.
Analyses
Basic data description was done by calculating mean scores and standard deviations for study variables and their bivariate associations. To study predictors of follow-up exercise automaticity, a sequential linear regression model was computed with baseline exercise behaviour entered in the first block, affective attitude, PBC, intention, and action planning items entered in the second block. Interactions with exercise behaviour were entered in the third step and interactions between social–cognitive variables were entered in the fourth step. Interactions were computed from mean-centred variables and were only entered in the regression equation where the interacting variables had significant main effects. Significant interactions were decomposed by means of simple slope analyses following standard procedures [37]. Because the predictor variables have previously been shown to be highly correlated [31, 38], variance inflation factors (VIF) were computed to assess potential multicollinearity among main effects, where VIF >5 was regarded as indicative of multicollinearity [39].There were no missing data and we controlled for the influence of age and gender in the regression model.
Results
Descriptives and Bivariate Correlations
Of the participants who provided data at both time-points, 34.5 % (n = 140) reported engaging in sufficient exercise at baseline. Eighty-three participants (20.3 %) reported no engagement in exercise behaviour and 183 participants (45.1 %) had engaged in insufficient exercise in the 4 weeks prior to the data collection. Table 1 shows that, with the exception of affective attitudes, mean scores for study variables were around midscale value and that mean exercise behaviour in minutes per week was M = 21.45 (SD = 22.57). Large-sized correlations (r > 0.50) with follow-up exercise automaticity were found for intention, PBC, and exercise behaviour, whilst medium-sized correlations (r between 0.30 and 0.50) with follow-up automaticity were found for affective attitude and the action planning items.
Regression Analysis
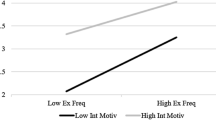
No VIF scores >5 were observed, so indicating stability of regression coefficients in the regression model. Table 2 reports the regression coefficients, standard errors and standardised regression coefficients for this model. Step 1 showed that exercise behaviour alone explained 33.8 % of the variance in exercise automaticity (β = 0.58, p < 0.001). In the second step, PBC (β = 0.32, p < 0.001), affective attitude (β = 0.12, p = 017), and the action plan referring to when (β = 0.16, p = 0.009) and where (β = 0.23, p < 0.001) were additional significant predictors of exercise automaticity, next to exercise behaviour (β = 0.25, p = 0.002). Intention did not significantly predict exercise automaticity (β = 0.09, p = 0.256). The addition of these variables significantly increased (F change = 16.62, df = 6, p < 0.001) the amount of explained variance to 46.1 %. The third step did not significantly increase the amount of explained variance (F change = 0.15, df = 4, p = 0.965) and revealed nonsignificant interactions between significant social–cognitive variables and exercise behaviour (all p > 0.635). Adding the interactions between the significant social–cognitive variables in the fourth step of the regression model significantly (F change = 2.93, df = 2, p = 0.008) increased the amount of explained variance to 47.2 %. This final step revealed nonsignificant interactions for all of the computed interactions terms (all p > 0.251), with the exception of the interaction between PBC and the action plan referring to when to exercise (β = 0.22, p = 0.006).Footnote 1 The decomposition of this significant interaction revealed that planning was a significant predictor of exercise automaticity at low levels of PBC (β = 0.18, p = 0.002), but weaker at mean levels of PBC (β = 0.10, p = 0.019) and nonsignificant at high levels of PBC (β = 0.06, p = 0.298).
Discussion
The main purpose of the present study was to identify whether relevant social–cognitive variables were predictive of exercise automaticity in a sample of young adult undergraduate students, next to previous exercise behaviour. A focus on these social–cognitive variables was deemed appropriate because previous research has proved their relevance for repeated exercise behaviour. In line with earlier empirical evidence and theoretical postulations [4], results showed that exercise behaviour was an important predictor of exercise automaticity, accounting for about a third of the variance in exercise automaticity. In their earlier meta-analysis on habits, Ouellette and Wood [4] reported a summary r of 0.59 between past behaviour and future behaviour in stable contexts. Our results demonstrate that past exercise behaviour has a similar relationship with exercise automaticity, highlighting the relevance of behavioural repetition in automaticity development [5, 29]. Perhaps more importantly, various social–cognitive variables were also predictive of exercise automaticity, over and above the influence of past behaviour. In particular, planning when and where to exercise, as well as PBC and affect, added significantly to the regression model and explained some 12 % of additional variance in exercise automaticity.
Despite the fact that intention was a large effect-sized correlate of exercise behaviour in the bivariate model, intention did not predict exercise automaticity in the multivariate model. Although socio-cognitive models postulate that an intention construct is the most important determinant of (exercise) behaviour, empirical evidence from meta-analytical work has provided more limited support for this postulate regarding exercise behaviours [40, 41]. For instance, Rhodes and De Bruijn [40] reported that nearly half of those with positive physical activity intentions are unable to follow-up on these intentions. Perhaps more importantly, Rhodes and Dickau [41] found that medium-effect sized changes in exercise intention led to only trivial changes in exercise behaviour. Although the intention construct as assessed in contemporary models may fail to capture resolve to proceed with exercise decisions in the face of constraints or other demands [42], there is also evidence that intention may become less relevant for behaviours that have been maintained for a longer period [43] and therefore likely to have become habitual [4].
Reflecting previous evidence on the relevance of PBC for the initiation and maintenance of exercise behaviour [12, 44, 45], PBC was the strongest predictor of exercise automaticity, where the decision to engage in exercise behaviour requires minimum deliberation. Development of behavioural automaticity depends on situational consistency [4] and because PBC typically reflects situational control over behaviour [33], exercise performance in situations that are easily accessible may thus be more likely to be conducive to becoming automatic. Likewise, our findings also demonstrate that individuals that plan to enact exercise behaviour in response to specific cues end up with more automatic exercise behaviours. Our findings are in line with habit formation models and studies [4, 46] and suggest that temporal (e.g., Tuesday evening at 8 o'clock) and situational (e.g., local gym) cues, rather than social cues, may be most relevant cues for strengthening exercise automaticity.
Although these results suggest that simultaneously emphasising controllability and planning may be a fruitful intervention priority when targeting exercise automaticity, the decomposition of the significant interaction between planning when to exercise and PBC showed that planning became less predictive of exercise automaticity when people were more confident in their ability to engage in sufficient exercise. This counters evidence from studies on other behaviours such as dental hygiene [47] and diet [48], where higher levels of planning were more strongly related to behaviour when matched by higher levels of PBC. It should be noted, however, that these latter studies focused on frequency of behaviour, rather than the automaticity with which the behaviour was performed. As noted, automaticity of behaviour is conceptually distinct from frequency of behaviour [49]. Potentially, constructs such as planning and PBC may operate and interact differently across various phases of behaviour change, such as initiation, maintenance, and automaticity [45].
Despite their correlational nature, the results of the present and other recent studies point to a temporal conceptual model through which motivation, behaviour and socio-cognitive factors interrelate in a temporal order to lead to exercise habits [45]. That is, exercise habit formation may be reliant on motivation and specific self-regulation instructions in the initial exercise adoption phase, where preparatory and action planning foster initial behavioural changes, but then an emphasis shift to self-efficacy considerations and coping planning strategies would be needed for maintenance and habituation [45]. Indeed, our findings suggest that, when exercise has become automatic, experiencing a sense of exercise controllability may knock an individual out of self-regulatory action planning mode. As a result, action planning strategies may be misplaced in individuals who engage in exercise automatically and who have a strong perception of exercise control.
Several limitations need to be acknowledged. The first limitation is the reliance on self-report data, which may be influenced by memory biases. For instance, we assessed exercise behaviour using the International Physical Activity Questionnaire (IPAQ), which has been found to correlate quite well with energy expenditure derived from doubly labelled water techniques, but also has a systematic bias towards underreporting of physical activity, particularly at vigorous levels [36]. Likewise, exercise automaticity was measured using participants' retrospective reflections on the automaticity of exercise behaviour [35], but concerns have been raised about the validity of self-reporting automaticity [50] and mixing automaticity of action with automaticity of initiation [51]. For instance, it is unlikely for people to engage in long bouts of exercise behaviour without actually being aware of doing so. Likewise, both the SRBAI and the SRHI do not include contextual cueing of behaviour, thereby potentially reflecting behavioural action across contexts [50]. Although these habit scales are useful for large-sized population studies [35], it would be desirable to see if our results are invariant to other ways of measuring habit. A second limitation relates to the current sample of the study, an undergraduate student sample that was predominantly female. Notably, a meta-analysis of self-regulatory strategies in the physical activity domain showed that these strategies are more likely to be effective in undergraduate student samples [19] and so the influence of action planning strategies on exercise automaticity may operate differently in other age groups. Replication of our findings in other samples is thus warranted. Third, the present study used correlational data and, although we employed a prospective design, such designs cannot be relied upon to demonstrate causality of relationship for established and ongoing behaviours, where behavioural frequency, habit and motivation are likely to be stable over time [52]. For instance, the direct effect of the two planning items and PBC on exercise automaticity may also indicate methodological issues, in which past behaviour alone is potentially an inadequate proxy for context-dependent repetition. The present results should therefore be viewed as initial efforts that should inform more rigorous experimental tests of these relationships using longitudinal habit formation designs [52]. Finally, past exercise behaviour was assessed at baseline regarding the previous 4 weeks, which may not adequately have captured longer-term repetition history. Despite these limitations, this study is one of the first to detail social–cognitive predictors of exercise automaticity above and beyond repetition of behaviour. Whereas the main effects on automaticity were generally in line with studies on frequency and duration of behaviour, the trade-off between PBC and action planning in determining exercise automaticity may point to the fact that social–cognitive variables in part interact differently from automaticity of behaviour than for mere frequency of behaviour.
Notes
When adding interactions for nonsignificant main effects to the regression equation, there were no additional significant interactions in the regression equation (all p-values for these interactions >0.21).
References
Ajzen I. The theory of planned behaviour. Organ Behav Hum Decis Process. 1991;50:179–211.
Hillsdon M, Foster C, Thorogood M. Interventions for promoting physical activity. Cochrane Database Syst Rev. 2005;1:CD003180.
Baumeister RF, Bratslavsky E, Muraven M, Tice DM. Ego depletion: is the active self a limited resource? J Pers Soc Psychol. 1998;74:1252–65.
Ouellette J, Wood W. Habit in every day life: the multiple processes by which past behavior predicts future behavior. Psychol Bull. 1998;124:54–74.
Wood W, Neal DT. A new look at habits and the habit–goal interface. Psychol Rev. 2007;114:843–63.
Bargh JA. The four horsemen of automaticity: awareness, efficiency, intention, and control in social cognition. In: Wyer Jr R, Srull T, editors. Handbook of social cognition. Hillsdale: Erlbaum; 1994. p. 1–40.
Gardner B, De Bruijn GJ, Lally P. A systematic review and meta-analysis of the self-report habit index to nutrition and physical activity behaviors. Ann Behav Med. 2011;42:174–87.
Triandis H. Interpersonal behavior. Montery: Brook/Cole; 1977.
Lally P, van Jaarsveld CHM, Potts HWW, Wardle J. How are habits formed: modelling habit formation in the real world. Eur J Soc Psychol. 2010;40:998–1009.
Gardner B, Lally P. Does intrinsic motivation strengthen physical activity habit? Modelling relationships between self-determination, past behaviour, and habit strength. J Behav Med. 2013;36(5):488–97.
De Bruijn GJ, Keer M, Conner M, Rhodes RE. Using implicit associations towards fruit consumption to understand fruit consumption behaviour and habit strength relationships. J Health Psychol. 2012;17:479–89.
De Bruijn GJ. Exercise habit strength, planning and the theory of planned behaviour: an action control approach. Psychol Sport Exerc. 2011;12:106–14.
Gollwitzer PM. Implementation intentions: strong effects of simple plans. Am Psychol. 1999;54:493–503.
Gollwitzer P, Schaal B. Metacognition in action: the importance of implementation intentions. Personal Soc Psychol Rev. 1998;2:124–36.
Webb TL, Sheeran P. Identifying good opportunities to act: implementation intentions and cue discrimination. Eur J Soc Psychol. 2004;34:407–19.
Orbell S, Hogdkins S, Sheeran P. Implementation intentions and the theory of planned behavior. Personal Soc Psychol Bull. 1997;25:945–54.
Verplanken B, Orbell S. Reflections on past behavior: a self-report index of habit strength. J Appl Soc Psychol. 2003;33:1313–30.
Rhodes RE, Naylor PJ, McKay HA. Pilot study of a family physical activity planning intervention among parents and their children. J Behav Med. 2010;33:91–100.
Bélanger-Gravel A, Godin G, Amireault S. A meta-analytic review of the effect of implementation intentions on physical activity. Health Psychol Rev. 2013;7:1–32.
Conner M, Sandberg T, Norman P. Using action planning to promote exercise behavior. Ann Behav Med. 2010;40:65–76.
Fleig L, Lippke S, Pomp S, Schwarzer R. Intervention effects of exercise self-regulation on physical exercise and eating fruits and vegetables: a longitudinal study in orthopedic and cardiac rehabilitation. Prev Med. 2011;53:182–7.
Armitage CJ. Effectiveness of experimenter-provided and self-generated implementation intentions to reduce alcohol consumption in a sample of the general population: a randomized exploratory trial. Health Psychol. 2009;28:545–53.
Adriaanse MA, Vinkers CD, De Ridder DT, Hox JJ, De Wit JB. Do implementation intentions help to eat a healthy diet? A systematic review and meta-analysis of the empirical evidence. Appetite. 2011;56:183–93.
Rhodes RE, de Bruijn GJ, Matheson DH. Habit in the physical activity domain: integration with intention temporal stability and action control. J Sport Exerc Psychol. 2010;32:84–98.
Reed J, Buck S. The effect of regular aerobic exercise on positive-activated affect: a meta- analysis. Psychol Sport Exerc. 2009;10:581–94.
Hull C. Principles of behavior: an introduction to behavior theory. New York: Appleton- Century-Crofts; 1943.
Ekkekakis P, Hargreaves EA, Parfitt G. Invited guest editorial: envisioning the next fifty years of research on the exercise–affect relationship. Psychol Sport Exerc. 2013;14(5),751–758.
Conner M, Rhodes RE, Morris B, McEachan R, Lawton R. Changing exercise through targeting affective or cognitive attitudes. Psychol Health. 2011;26:1–17.
Lally P, Gardner B. Promoting habit formation. Health Psychol Rev. 2013;7:S137–58.
Ryan R, Deci E. Active human nature: self-determination theory and the promotion and maintenance of sport, exercise, and health. In: Hagger MS, Chatzisarantis NL, editors. Intrinsic motivation and self-determination in exercise and sport. Human Kinetics Europe Ltd: Champaign, IL; 2007. pp. 1–19.
De Bruijn GJ, Rhodes RE, Van Osch L. Does action planning moderate the intention-habit interaction in the exercise domain? A three-way interaction analysis investigation. J Behav Med. 2012;35:509–19.
Rhodes RE, de Bruijn GJ. Automatic and motivational correlates of physical activity: does intensity moderate the relationship? Behav Med. 2010;36:44–52.
Ajzen I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. J Appl Soc Psychol. 2002;32:665–83.
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American college of sports medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–59.
Gardner B, Abraham C, Lally P, De Bruijn GJ. Towards parsimony in habit measurement: testing the convergent and predictive validity of an automaticity subscale of the self-report habit index. Int J Behav Nutr Physic Act. 2012; 9:102. doi:10.1186/1479-5868-9-10.
Maddison R, Mhurchu CN, Jiang Y, Vander Hoorn S, Rodgers A, Lawes CMM, et al. International Physical Activity Questionnaire (IPAQ) and New Zealand physical activity questionnaire (NZPAQ): a doubly labelled water validation. Int J Behav Nutr Phys Act. 2007;4:62.
Aiken L, West S. Multiple regression: testing and interpreting interactions. Newbury Park: Sage; 1991.
Rhodes RE, Blanchard CM, Matheson DH, Coble J. Disentangling motivation, intention, and planning in the physical activity domain. Psychol Sport Exerc. 2006;7:15–27.
O'Brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quant. 2007;41:673–90.
Rhodes RE, De Bruijn GJ. How big is the physical activity intention–behaviour gap? A meta- analysis using the action control framework. Br J Health Psychol. 2013;18:296–309.
Rhodes RE, Dickau L. Experimental evidence for the intention–behaviour relationship in the physical activity domain: a meta-analysis. Health Psychol. 2012;31:724–7.
Rhodes RE, Horne L. Deepening the measurement of motivation in the physical activity domain: Introducing behavioural resolve. Psychol Sport Exerc. 2013;14:455–60.
Bagozzi RP, Yi Y. The degree of intention formation as a moderator of the attitude-behavior relationship. Soc Psychol Quart. 1989;52(4):266–279.
Rhodes RE, Plotnikoff RC. Understanding action control: predicting physical activity intention–behavior profiles across 6 months in a Canadian sample. Health Psychol. 2006;25:292–9.
Rhodes RE, De Bruijn G. What predicts intention–behavior discordance? A review of the action control framework. Exerc Sport Sci Rev. 2013. doi:10.1097/JES.0b013e3182a4e6ed.
Wood W, Neal DT. The habitual consumer. J Couns Psychol. 2009;19:579–92.
Pakpour AH, Sniehotta FF. Perceived behavioural control and coping planning predict dental brushing behaviour among Iranian adolescents. J Clin Periodontol. 2012;39:132–7.
Gutiérrez-Doña B, Lippke S, Renner B, Kwon S, Schwarzer R. Self-efficacy and planning predict dietary behaviors in Costa Rican and South Korean women: two moderated mediation analyses. Appl Psychol. 2009;1:91–104.
Gardner B. Habit as automaticity, not frequency. Eur Health Psychol. 2012;14:32–6.
Sniehotta FF, Presseau J. The habitual use of the self-report habit index. Ann Behav Med. 2012;43:139–40.
Ajzen I. Residual effects of past on later behaviour: habituation and reasoned action perspectives. Personal Soc Psychol Rev. 2002;6:107–22.
Weinstein ND. Misleading tests of health behavior theories. Ann Behav Med. 2007;33:1–10.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
de Bruijn, GJ., Gardner, B., van Osch, L. et al. Predicting Automaticity in Exercise Behaviour: The Role of Perceived Behavioural Control, Affect, Intention, Action Planning, and Behaviour. Int.J. Behav. Med. 21, 767–774 (2014). https://doi.org/10.1007/s12529-013-9348-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-013-9348-4