
Abstract
Background
Previous studies showed different dyssynchrony patterns between ischemic and normal myocardium at early post-stress using Tl-201 gated SPECT myocardial perfusion imaging (MPI). The aim of this study was to assess the relation of stress-induced dyssynchrony and the extent of angiographic coronary artery disease (CAD).
Methods and Results
The MPI images of 144 patients were retrospectively analyzed. With ≥70% stenosis as the criteria of CAD, 57 had no CAD, 32 had 1-vessel disease, 36 had 2-vessel disease, and 19 had 3-vessel disease, respectively. LV global and territorial dyssynchrony parameters were measured by the phase analysis from stress/rest Tl-201 SPECT MPI and compared between stress and rest among the patient groups. The patients with multi-vessel CAD had significantly more global dyssynchrony than the patients without ≥70% stenosis at stress. The patients with multi-vessel CAD showed significantly more global and territorial dyssynchrony on stress images than on rest. More patients with 3-vessel CAD were correctly classified as multi-vessel disease, when combining both visual interpretation and dyssynchrony assessment.
Conclusion
The patients with multi-vessel CAD had significantly more global and territorial dyssynchrony at early post-stress than at rest. Such quantitative measures of myocardial stunning may assist in the diagnosis of multi-vessel CAD.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Myocardial stunning, defined as prolonged global and/or regional myocardial dysfunction after stress-induced ischemia, has been well described on stress/rest gated myocardial perfusion imaging (MPI).1,2 It might be manifested as transient post-stress decline of left-ventricular (LV) ejection fraction (EF) or reversible regional wall motion abnormality (RWA) on gated MPI and were found to correlate with the severity of stress-induced perfusion defects. Plenty of studies further demonstrated that stress-induced stunning shown on gated MPI correlated with severe and extensive coronary artery disease (CAD).3-6 It should be noted that the observation of myocardial stunning might be different when using different kinds of radiotracers (e.g., Tl-201, Tc-99m sestamibi, or Rb-82), imaging protocols (e.g., peak-stress, early post-stress, or post-stress), or different types of stress (e.g., exercise or pharmacological stress).
Phase analysis of gated MPI was first developed by Chen et al7 for measuring LV dyssynchrony. Previous studies have shown that quantitative indices given by phase analysis, such as phase standard deviation (SD) and phase histogram bandwidth, correlated well with LV dyssynchrony parameters measured by tissue Doppler echocardiography.8-10 These studies were done using Tc-99m labeled radiotracers (sestamibi or tetrofosmin) and usually acquired data 1 hour or more post injection. Therefore, the stress images represented the late post-stress function, close to the resting function. A study using Tc-99m sestamibi MPI reported that the presence of even large reversible defects did not alter LV dyssynchrony from rest to stress.11
Chen et al first evaluated the performance of phase analysis of Tl-201 gated SPECT MPI in comparison with Tc-99m sestamibi and found a good correlation between the LV dyssynchrony parameters obtained from the images of these two tracers.12 Furthermore, the same group investigated myocardial stunning in CAD patients using phase analysis of Tl-201 gated SPECT MPI and showed that stress-induced myocardial ischemia caused dyssynchronous contraction in the ischemic region, deteriorating LV synchrony.13 On the contrary, normal myocardium had more synchronous contraction at stress than at rest.13 The different dyssynchrony pattern between ischemic and normal myocardium at early post-stress may aid diagnosis of CAD using Tl-201 gated SPECT MPI.
This study followed the above studies in phase analysis of Tl-201 gated SPECT MPI in CAD patients. It was aimed to assess the relation of stress-induced LV dyssynchrony and the extent of angiographic CAD.
Materials and Methods
Patients
The MPI images of 144 consecutive patients, who were referred for dipyridamole-stress/rest Tl-201 gated SPECT MPI for diagnosing CAD and had coronary angiography following the Tl-201 scans, were retrieved from the nuclear medicine databases in Changhua Christian Hospital. Table 1 shows the clinical characteristics of the enrolled patients. According to the coronary angiography of these patients, 57 did not have significant stenosis (≥70%) in any coronary artery, 32 had ≥70 stenosis in one of the coronary arteries, 36 had ≥70% stenosis in two of the coronary arteries, and 19 had ≥70% stenosis in all three coronary arteries, respectively. Except for more diabetes and history of myocardial infarction (MI) in patients with CAD, no significant differences were noted regarding the age, gender, hypertension, hyperlipidemia, smoking, family history of CAD, history of percutaneous transluminal coronary angioplasty (PTCA), or coronary artery bypass graft (CABG). The study protocol was approved by the Institutional Review Board of Changhua Christian Hospital.
Imaging Protocol
Patients fasted at least 4 hours and were asked to abstain from caffeine-containing foods, beverages, and medications containing methylxanthine for 24 hours. Dipyridamole was administered intravenously at a rate of 0.14 mg·kg−1·minute−1 for 4 minutes. 111 MBq of Tl-201 was then injected 3 minutes after the end of the dipyridamole infusion. Blood pressure and heart rate were recorded every minute. Aminophylline was given for patients suffering from severe adverse effects after dipyridamole stress, such as chest pain, dyspnea, nausea, vomiting, severe bradycardia (heart rate less than 40 bpm), 2nd or 3rd degree atrioventricular block, ST depression, or frequent premature ventricular contractions. As shown in Table 1, 16%-32% of patients suffered from severe adverse effects needing aminophylline for relieving the discomfort in different CAD groups, but there was no significant difference regarding the frequency or the dose of used aminophylline between the groups.
Stress and rest acquisitions started 5-10 minutes and 4 hours after Tl-201 injection in a supine position. No rest re-injection of Tl-201 was done. A dual-head gamma camera (Millennium MG, GE, Haifa, Israel) equipped with a low-energy general-purpose collimator was used. Thirty-two projections, with 70 seconds of data collection per projection, were obtained over a 180° arc extending from the 45° right anterior oblique to the 45° left posterior oblique position. A 20% window was centered over the 72 and 167 keV Tl-201 photopeaks. The acquisition was synchronized with ECG with an acceptance window of 100%, and each projection was divided into eight images per cardiac cycle. The projection images were acquired into 64 × 64 matrices with a 1.45 acquisition zoom and were reconstructed by filtered back projection with a Butterworth filter (order = 10 and cut-off frequency = 0.4 cycle·pixel−1).
Image Analysis
The perfusion images were displayed in the short-axis, vertical long-axis, and horizontal long-axis views. The LV was divided into 17 segments and all segments were scored with a 5-point scale (0 = normal, 1 = mildly reduced, 2 = moderately reduced, 3 = severely reduced, and 4 = absent uptake) by two experienced observers in consensus. The summed stress score (SSS) and summed rest score (SRS) were obtained by the sum of the scores of 17 segments on stress and rest images. The summed difference score (SDS) was defined as the difference of SSS and SRS. The patients were then divided into normal group, infarct group, and ischemia group as previously described.13 The 17 segments were classified into three vascular territories: left anterior descending artery (LAD) for apex and anterior wall, left circumflex artery (LCX) for lateral wall, and right coronary artery (RCA) for inferior wall. The perfusion of an individual territory was classified as abnormal when at least 1 point of abnormality on consecutive 2 or more segments on stress images.
The gated data were processed with completely automated software (QGS 3.0; Cedars-Sinai Medical Center, Los Angeles, CA) to calculate LVEF and LV volumes. Our previous work assessed the repeatability of LVEF measurements by Tl-201 gated SPECT,14 and an increase or decrease of 6% or greater between the post-stress and rest gated SPECT studies was considered significant. For regional wall motion analysis, SSS, SRS, and SDS for RWA were calculated as our previous study.15 SDS for RWA greater than 2 was considered to indicate the presence of reversible RWAs (RRWA).
For dyssynchrony assessment, all of the SPECT images were transferred to Emory University by phase analysis,7 which was done blinded from the angiographic results. The phase analysis technique calculated a phase value for each sampled region (>600 sampled regions for the entire LV), which represented the onset of mechanical contraction of the region. The SD of all phase values and bandwidth of the phase histogram characterized LV global dyssynchrony.7 Furthermore, phase SD was calculated for the three coronary territories, respectively, as demonstrated in Figure 1. The global and territorial dyssynchrony parameters were then compared between the stress and rest images in the four patient groups classified according to the angiographic results (no significant stenosis, 1-vessel disease, 2-vessel disease, and 3-vessel disease), respectively.

Dyssynchrony assessment for the entire LV (phase standard deviation [SD] and histogram bandwidth) and coronary territories (phase SD in the territories). This patient had a 100% stenosis in the mid left anterior descending artery (LAD) according to the coronary angiography. The global dyssynchrony parameters (phase SD and histogram bandwidth) and LAD phase SD deteriorated from rest to early post-stress. Such deterioration was due to the delayed contraction in the ischemic region
According to a previous study that measured the repeatability of the phase analysis technique,16 the SD of phase SD between two serial scans was 2.6°. With a z score of 1.65, a difference of 4.3° in phase SD was considered statistically significant between two scans. Using this criterion, in this study an increase in phase SD in the coronary territories from rest to stress was considered a significant deterioration of territorial synchrony and used as an indication of significant stenosis in the corresponding coronary artery. The incremental diagnostic value of the territorial dyssynchrony assessment over the visual interpretation was evaluated in the patients with 3-vessel disease.
Statistical Analysis
Phase SD was compared among stress and rest images using paired t test. Unpaired t test with unequal variance was used to compare phase SD among the groups. χ 2 test was used to compare the proportions of the patients with 3-vessel angiographic CAD, who were detected using various methods in Figure 4. P < .05 was considered statistically significant.
Results
Table 2 shows the global dyssynchrony parameters in the patient groups. In general, the patient groups with more severe angiographic CAD had more dyssynchrony than the patient groups with less angiographic CAD. However, only the patient groups with 2-vessel disease and with 3-vessel disease had significantly more global dyssynchrony than the patient group without ≥70% stenosis at stress. When comparing the stress and rest dyssynchrony, two opposite trends were observed. In the patient group without ≥70% stenosis, stress images showed significantly less dyssynchrony than the rest images. On the contrary, in the patient groups with 2-vessel disease and with 3-vessel disease the stress images showed significantly more dyssynchrony than the rest images. This finding demonstrated myocardial stunning in the patients with severe and extensive CAD.
Table 3 shows the global and territorial dyssynchrony parameters in the patient group with 2-vessel disease. Subgroup analysis showed that the patients with LAD ≥70% stenosis had significant more dyssynchrony (both globally and territorially in LAD) at stress than at rest. Such finding was not observed in the patients without LAD ≥70% stenosis. This finding indicated that LAD stenosis had higher impact on dyssynchrony than the stenosis in other coronary arteries.
Table 4 shows the global and territorial dyssynchrony parameters in the patient group with 3-vessel angiographic CAD. The stress images showed significantly more dyssynchrony for the entire LV and for the coronary territories than the rest images.
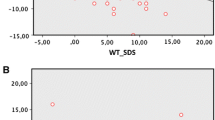
Figure 2 shows phase SD in the patients with normal perfusion (N = 71), infarct (N = 31), and ischemia (N = 42). From rest to stress, phase SD significantly reduced in the patients with normal perfusion, but significantly increased in the patients with ischemia. This result also demonstrated myocardial stunning in the CAD patients and confirmed the finding of our previous study.13 However, a weak correlation was found between phase SD change from stress to rest and SDS (r = 0.2475, P = .0028), as shown in Figure 3.

Stress and rest phase standard deviation (SD) in the patients with normal perfusion, infarct, and ischemia

The correlations of phase standard deviation (SD) change from stress to rest and summed difference score (SDS)
Figure 4 shows the diagnostic results in the patients with 3-vessel angiographic CAD by the visual interpretation noted in the nuclear medicine databases, visual interpretation plus LVEF changes, visual interpretation plus regional wall motion assessment, territorial dyssynchrony assessment, and visual interpretation plus territorial dyssynchrony assessment, respectively. Significantly more patients with 3-vessel angiographic CAD were correctly classified as 3-vessel disease when combining both visual interpretation and territorial dyssynchrony assessment than visual interpretation alone (P < .001). Figure 4 also shows a promising trend that the incremental value of the territorial dyssynchrony assessment in the diagnosis of 3-vessel angiographic CAD over visual interpretation was higher than both LVEF changes and regional wall motion assessment.

The incremental value of the territorial dyssynchrony assessment over the visual interpretation of the perfusion images in the diagnosis of 3-vessel angiographic coronary artery disease (CAD). *The proportions of the patients with 3-vessel angiographic CAD, who were detected by the methods. The P values were calculated by comparing against perfusion alone using χ 2 test
Discussion
This study was the first study to demonstrate the relation between early post-stress dyssynchrony and angiographic CAD using Tl-201 gated SPECT MPI. The main finding of this study was that the patients with severe multi-vessel CAD had significantly more global and territorial dyssynchrony at stress than at rest. On the contrary, the patients without significant stenosis in any coronary arteries had significantly less dyssynchrony at stress than at rest. Such different dyssynchrony pattern clearly demonstrated myocardial stunning in the patients with severe multi-vessel CAD. In addition, regional phase analysis was used in two previous studies to measure the site of latest mechanical activation as the optimal LV lead positions for cardiac resynchronization therapy (CRT) in heart failure patients.17,18 Those two studies showed that CRT response improved when pacing the regions with delayed contraction as measured by regional phase analysis of gated SPECT MPI images. This study was the first study to use regional phase analysis to measure delayed contraction in coronary territories in CAD patients.
The conventional stress/rest MPI provided relative perfusion information of different vascular territories of the LV, thus might underestimate the extent and severity of ischemia for patients with relatively balanced perfusion abnormality in multi-vessel disease. According to the study of Berman et al,19 MPI might underestimate the extent of ischemia in about 20-50% of multi-vessel CAD patients. Therefore, the measurement of myocardial stunning can assist in the diagnosis of multi-vessel CAD patients, especially the ones with balanced ischemia in 3-vessel disease.
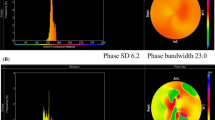
Figure 4 showed that the territorial dyssynchrony assessment had an incremental value over the visual interpretation of the conventional stress/rest perfusion images in the diagnosis of 3-vessel angiographic CAD. Figure 5 shows a patient example to demonstrate such incremental diagnostic value of the territorial dyssynchrony assessment in balanced 3-vessel disease. The perfusion images of this patient showed balanced perfusion distribution at both stress and rest, which resulted in small perfusion defects (SSS = 6, SRS = 4). The SDS in the LAD, LCX, and RCA territories were 1, 0, and 1, respectively. Visual interpretation noted only mild grade of perfusion abnormality in the apex and inferior wall. For Tl-201 images, such an abnormality was not uncommon due to attenuation artifact,20 thus the perfusion images were considered as an equivocal finding of CAD. The post-stress and rest LVEF was 53% and 54%, respectively, and the transient ischemic dilation (TID) ratio was 1.01. Based on our previous study, the case should be considered to have severe CAD only when TID ratio ≥ 1.1914 or stress-induced worsening of LVEF ≥ 6%.15 Noteworthy, this patient had remarkable deterioration in global and territorial synchrony from rest to stress. According to the coronary angiography this patient had LAD stenosis 70%, LCX stenosis 80%, RCA stenosis 70%, respectively.

An example patient with a balanced 3-vessel disease. (A) The perfusion images revealed only mild grade of perfusion abnormality with partial reversibility in apex and inferior. (B) Perfusion polar map (left column), phase polar map (middle column) and phase histogram (right column). The phase analysis revealed remarkable deterioration in global and territorial synchrony from rest to stress.
Another finding of this study was that LAD stenosis had higher impact on dyssynchrony than the stenosis in other coronary arteries, as shown in the patient group with 2-vessel disease (Table 3). The reason might be that LAD generally supplies blood to a larger LV territory than other vessels. However, the number of patients in Table 3 was small, so such finding needs to be confirmed in a larger population.
In this study, patients underwent dipyridamole stress instead of exercise stress. Although perfusion abnormalities during dipyridamole stress reflect heterogeneity of coronary reserve, which may not be considered as true ischemia. Nevertheless, ischemia sometimes does occur under dipyridamole stress and results in ischemic stunning. Our previous studies of Tl-201 gated SPECT MPI found that dipyridamole-induced stunning, manifested as LVEF worsening during dipyridamole stress, was a highly specific marker of significant CAD.14,15,21 In a study by Lee et al,22 dipyridamole-induced reversible regional wall-motion abnormalities were present in one half of the patients with CAD on 1-hour post-stress Tc-99m sestamibi gated SPECT images. With Rb-82 PET and dipyridamole or adenosine stress, Dorbala et al23 also showed reduced LVEF greater than 5% in patients with multi-vessel CAD.
The main limitation of this study was the use of Tl-201 tracer. Tl-201 SPECT MPI usually has higher noise and poorer image quality than Tc-99m SPECT MPI. Therefore, this study used a prolonged acquisition protocol (70 second·projection−1) to increase the count density in the images. Tl-201 SPECT MPI started the acquisition within 10-minutes post injection, representing early post-stress. Therefore, it can measure myocardial stunning better than the Tc-99m SPECT, which usually acquires images late post-stress. Noteworthy, Rb-82 PET acquires peak-stress images and has better image quality than Tl-201 SPECT; therefore, the findings of this study may become more prominent if using Rb-82 PET. Finally, the image analysis in this study was done in the images retrieved from the nuclear medicine databases, not prospectively enrolled patients. Therefore, the findings of this study need to be validated prospectively, especially for the purpose of establishing the incremental diagnostic value of the dyssynchrony assessment over the perfusion assessment in multi-vessel CAD.
In conclusion, the patients with severe multi-vessel angiographic CAD had significantly more global and territorial dyssynchrony at early post-stress than at rest, as assessed by Tl-201 gated SPECT MPI. Such quantitative measures of myocardial stunning showed an incremental value over the visual interpretation of the conventional perfusion images in the diagnosis of 3-vessel disease.
New Knowledge Gained
Early post-stress dyssynchrony, as measured by phase analysis of Tl-201 gated SPECT MPI, characterizes ischemia-induced myocardial stunning and is related to the extent of angiographic CAD.
References
Johnson LL, Verdesca SA, Aude WY, Xavier RC, Nott LT, Campanella MW, et al. Postischemic stunning can affect left ventricular ejection fraction and regional wall motion on poststress gated sestamibi tomograms. J Am Coll Cardiol 1997;30:1641-8.
Hashimoto J, Kubo A, Iwasaki R, Iwanaga S, Mitamura H, Ogawa S, et al. Gated single-photon emission tomography imaging protocol to evaluate myocardial stunning after exercise. Eur J Nucl Med 1999;26:1541-6.
Emmett L, Iwanochko RM, Freeman MR, Barolet A, Lee DS, Husain M. Reversible regional wall motion abnormalities on exercise technetium-99 m-gated cardiac single photon emission computed tomography predict high-grade angiographic stenoses. J Am Coll Cardiol 2002;39:991-8.
Yamagishi H, Shirai N, Yoshiyama M, Teragaki M, Akioka K, Takeuchi K, et al. Incremental value of left ventricular ejection fraction for detection of multivessel coronary artery disease in exercise (201)Tl gated myocardial perfusion imaging. J Nucl Med 2002;43:131-9.
Shirai N, Yamagishi H, Yoshiyama M, Teragaki M, Akioka K, Takeuchi K, et al. Incremental value of assessment of regional wall motion for detection of multivessel coronary artery disease in exercise (201)Tl gated myocardial perfusion imaging. J Nucl Med 2002;43:443-50.
Sharir T, Bacher-Stier C, Dhar S, Lewin HC, Miranda R, Friedman JD, et al. Identification of severe and extensive coronary artery disease by postexercise regional wall motion abnormalities in Tc-99m sestamibi gated single-photon emission computed tomography. Am J Cardiol 2000;86:1171-5.
Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by Phase analysis of ECG-gated myocardial Perfusion SPECT imaging: Development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol 2005;12:687-95.
Henneman MM, Chen J, Ypenburg C, Dibbets P, Stokkel M, van der Wall EE, et al. Phase analysis of gated myocardial Perfusion SPECT compared to tissue Doppler imaging for the assessment of left ventricular dyssynchrony. J Am Coll Cardiol 2007;49:1708-14.
Marsan NA, Henneman MM, Chen J, Ypenburg C, Dibbets P, Ghio S, et al. Real-time 3-dimensional echocardiography as a novel approach to quantify left ventricular dyssynchrony: A comparison study with phase analysis of gated myocardial perfusion single photon emission computed tomography. J Am Soc Echocardiogr 2008;21:801-7.
Marsan NA, Henneman MM, Chen J, Ypenburg C, Dibbets P, Ghio S, et al. Left ventricular dyssynchrony assessed by two 3-dimensional imaging modalities: Phase analysis of gated myocardial perfusion SPECT and tri-plane tissue Doppler imaging. Eur J Nucl Med Mol Imaging 2008;35:166-73.
Aljaroudi W, Koneru J, Heo J, Iskandrian AE. Impact of ischemia on left ventricular dyssynchrony by phase analysis of gated single photon emission computed tomography myocardial perfusion imaging. J Nucl Cardiol 2011;18:36-42.
Chen CC, Huang WS, Hung GU, Chen WC, Kao CH, Chen J. Left ventricular dyssynchrony evaluated by Tl-201 gated SPECT myocardial perfusion imaging: A comparison with Tc-99m sestamibi. Nucl Med Commun 2013;34:229-32.
Chen CC, Shen TY, Chang MC, Hung GU, Chen WC, Kao CH, et al. Stress-induced myocardial ischemia is associated with early post-stress left ventricular mechanical dyssynchrony as assessed by phase analysis of Tl-201 gated SPECT myocardial perfusion imaging. Eur J Nucl Med Mol Imaging 2012;39:1904-9.
Hung GU, Lee KW, Chen CP, Lin WY, Yang KT. Relationship of transient ischemic dilation in dipyridamole myocardial perfusion imaging and stress-induced changes of functional parameters evaluated by Tl-201 gated SPECT. J Nucl Cardiol 2005;12:268-75.
Hung GU, Lee KW, Chen CP, Yang KT, Lin WY. Worsening of left ventricular ejection fraction induced by dipyridamole on Tl-201 gated myocardial perfusion imaging predicts significant coronary artery disease. J Nucl Cardiol 2006;13:225-32.
Zhou Y, Faber TL, Patel Z, Folks RD, Cheung AA, Garcia EV, et al. An automatic alignment tool to improve repeatability of left ventricular function and dyssynchrony parameters in serial gated myocardial perfusion SPECT studies. Nucl Med Commun 2013;34:124-9.
Boogers MJ, Chen J, van Bommel RJ, Borleffs CJ, Dibbets-Schneider P, van der Heil B, et al. Optimal left ventricular lead position assessed with phase analysis on gated myocardial perfusion SPECT. Eur J Nucl Med Mol Imaging 2011;38:230-8.
Friehling M, Chen J, Saba S, Bazaz R, Schwartzman D, Adelstein EC, et al. The relationship between acute change in LV mechanical synchrony after cardiac resynchronization therapy and patient outcome: Prospective evaluation by a novel, single-injection, gated-SPECT protocol. Circ Cardiovasc Imaging 2011;4:532-9.
Berman DS, Kang X, Slomka PJ, Gerlach J, de Yang L, Hayes SW, et al. Underestimation of extent of ischemia by gated SPECT myocardial perfusion imaging in patients with left main coronary artery disease. J Nucl Cardiol 2007;14:521-8.
Kapur A, Latus KA, Davies G, Dhawan RT, Eastick S, Jarritt PH, et al. A comparison of three radionuclide myocardial perfusion tracers in clinical practice: The ROBUST study. Eur J Nucl Med Mol Imaging 2002;29:1608-16.
Hung GU, Chen CP, Yang KT. Incremental value of ischemic stunning on the detection of severe and extensive coronary artery disease in dipyridamole Tl-201 gated myocardial perfusion imaging. Int J Cardiol 2005;105:108-10.
Lee DS, Yeo JS, Chung JK, Lee MM, Lee MC. Transient prolonged stunning induced by dipyridamole and shown on 1- and 24-hour poststress 99mTc-MIBI gated SPECT. J Nucl Med 2000;41:27-35.
Dorbala S, Vangala D, Sampson U, Limaye A, Kwong R, Di Carli MF. Value of vasodilator left ventricular ejection fraction reserve in evaluating the magnitude of myocardium at risk and the extent of angiographic coronary artery disease: A 82Rb PET/CT study. J Nucl Med 2007;48:349-58.
Acknowledgments
This study was supported in part by a research grant from Changhua Christain Hospital (102-CCH-IRP-060) and an NIH Grant (1R01HL094438, PI: Ji Chen, PhD).
Disclosure
Dr Ji Chen receives royalties from the sale of Emory Cardiac Toolbox with SyncTool. The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict-of-interest practice.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Wen-Sheng Huang and Ching-Hui Huang have contributed equally to this work.
See related editorial, doi:10.1007/s12350-014-9973-6.
Rights and permissions
About this article

Cite this article
Huang, WS., Huang, CH., Lee, CL. et al. Relation of early post-stress left ventricular dyssynchrony and the extent of angiographic coronary artery disease. J. Nucl. Cardiol. 21, 1048–1056 (2014). https://doi.org/10.1007/s12350-014-9980-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-014-9980-7