
Abstract
Background
Regadenoson is a pharmacologic stress agent, which was recently approved for stress myocardial perfusion imaging (MPI). Aside from the initial protocol-driven studies, clinical experience with this stress agent is limited. Furthermore, low-level treadmill testing in a large population with regadenoson has not previously been evaluated. We describe our experience in the first 6 months of routine inpatient and outpatient clinical use.
Methods
Between 7/1/08 and 12/04/08, 1263 patients underwent regadenoson stress testing (596 with low-level treadmill, 667 supine). Past medical history, clinical symptoms during stress, and changes in systolic blood pressure were prospectively recorded.
Results
Low-level treadmill testing was well tolerated in our patient population. Shortness of breath, dizziness, palpitations, transient heart block, and nausea were less frequent when patients were able to exercise. In our population, 51% experienced a drop in systolic blood pressure greater than 10 mmHg, with 9% experiencing a decrease in more than 30 mmHg. This decrease in blood pressure was more common in patients who underwent low-level treadmill testing vs those that were supine (56% vs 47%, P-value < 0.001). The frequency of symptoms in our entire population was as follows: chest pain 35%, dizziness/lightheadedness 16%, shortness of breath 27%, headache 1.4%, nausea 2.3%, and palpitations 5%. There were no major hemodynamic or conduction abnormalities. In the 16% of patients, a history of COPD/Asthma Regadenoson MPI was well tolerated. There were no procedural deaths.
Conclusion
Regadenoson and Regadenoson combined with low level exercise MPI appear to be safe and well tolerated. An asymptomatic fall in systolic blood pressure seems to be more common in patients who undergo low-level treadmill testing.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
As the United States population is aging and becoming more obese, the percentage of patients who cannot undergo exercise stress testing due to age or age-related musculoskeletal disabilities, impaired functional capacity, and/or respiratory limitations is rising. At our institution alone, over 5000 patients underwent pharmacologic stress testing in 2007, which comprised almost two-third of our total patient stress population. Traditionally, adenosine and dipyridamole have been the pharmacologic stress agents of choice; however, adverse effects such as adenosine-induced bronchoconstriction and varying degrees of heart block often occur.1 Adenosine-induced bronchoconstriction is an important limitation as many as 30% of patients referred for adenosine myocardial perfusion imaging (MPI) also carry the diagnosis of COPD and knowledge of broncho-reactivity to adenosine is often not known prior to adenosine administration.2
The selective A2A receptor agonist, regadenoson, has been studied in several clinical trials and has demonstrated non-inferiority for the detection of ischemia in comparison to adenosine and has less severe adverse side effects.1,3-8 However, these trials did not utilized low-level treadmill exercise and the patients included in these clinical trials usually do not represent the “typical” patients that are referred for myocardial MPI. Therefore, the experience and outcomes of clinical trials may not necessarily reflect what occurs in the clinical settings at large. Clinical trials often recruit relatively healthy patients, without significant co-morbidities. In these trials, there was <50% history of myocardial infarction, <35% history of arrhythmia, <20% history of CHF, and <10% history of COPD or asthma.1,3,4,7,8 The aim of this study is to report our real-world clinical experience in 1263 consecutive inpatients and outpatients using regadenoson alone or in combination with low-level treadmill exercise.
Methods
Between 7/1/08 and 12/04/08, 1263 consecutive patients underwent clinically indicated regadenoson stress testing (596 with low-level treadmill, 667 supine). Past medical history, clinical symptoms during stress, ECG changes, and changes in systolic blood pressure were prospectively recorded using a standardized form. In 201 patients (16%) there was a history of reactive airway disease (asthma/COPD). Lung exams were performed to confirm lack of active wheezing prior to regadenoson administration. The patients’ regadenoson MPI was canceled if active bronchoconstriction was detected upon lung auscultation. As per standard clinical practice, patients with second or third degree atrioventricular heart block without functional pacemakers were excluded from drug administration.
Imaging Protocols
All images were acquired according to the American Society of Nuclear Cardiology guidelines using Gated SPECT single-day or 2-day (depending on body weight) technetium 99m tracer (tetrofosmin) protocols.
Regadenoson Administration
Patients were instructed to discontinue caffeine-containing products for 24 hours before the test and to hold beta blockers and nitrates on the morning of the study. As shown in Figure 1. and in accordance with ASNC guidelines, regadenoson was administered as a single 400-μg peripheral IV rapid infusion over 10 seconds followed immediately by a 5-mL saline solution flush. Tetrofosmin was injected approximately 30 seconds after starting regadenoson and was followed immediately by a 5 mL saline flush.

Regadenoson protocol
Whenever possible, patients performed low-level treadmill exercise during the adenosine infusion using the protocol shown in Figure 2. ECGs were obtained at baseline and every 2 minutes following regadenoson infusion for a total of 6 minutes or longer in cases with hemodynamic instability. Horizontal or down-sloping ST segment depression ≥1 or up-sloping ≥1.5 mm at 80 milliseconds after the J point was considered positive.

Regadenoson excercise protocol treadmill 0° elevation at 1.7 mph
SPECT Image Analysis
Stress and rest perfusion images were scored semi-quantitatively using a 17-segment model of the left ventricle using 4DMSPECT software (Ann Arbor, Michigan).9 The global summed stress score (SSS) and the summed rest score (SRS) were calculated by adding the scores of the 17 segments in the stress and resting images, respectively. Each segment was scored by consensus of two observers using a 5-point scoring system (0—normal, 1—equivocal, 2—moderate reduction of isotope uptake, 3—severe reduction of uptake, and 4—absence of detectable tracer uptake in a segment). When a segment demonstrated a lower score on either supine or prone imaging than in the other position, the lower score was assigned to that segment. On the basis of the number and severity of segments with scores 2, the observers judged the study results as normal, probably normal, equivocal, probably abnormal, or definitely abnormal.10 To further define the study results as normal or abnormal, the SSS was considered, from the addition of the scores of the 17 segments of the stress 99mTc-sestamibi images. After automatic reorientation,9 gated short-axis images were processed using quantitative-gated SPECT software, and the EF was automatically calculated. The mitral valve plane was manually corrected when necessary.11
Statistical Analysis
Continuous data are expressed as mean ± standard deviation, with median, 15th and 85th percentile values (comparable to one standard deviation). Wilcoxon rank sum tests were used to analyze group differences for the continuous data.
Results
The baseline characteristics of the study population, as well as the population divided into those who underwent low-level treadmill exercise and those who were supine during regadenoson administration, are listed in Table 1. The mean age of the total study population was 66.5 ± 12.5 years, with a mean BMI of 30.2 ± 7.35, and 43% were female. Those who underwent low-level treadmill testing were significantly younger (64.5 ± 11.3 vs 68.3 ± 13.2, P-value < 0.0001) and less often female (37% vs 48%, P-value < 0.001). The prevalence of end stage renal disease (ESRD) was 3.6% (45/1263). There was a significantly higher prevalence of diabetes, congestive heart failure, COPD/asthma, complete heart block, atrial fibrillation, and sick sinus syndrome in the patients who underwent supine testing without exercise.
In regards to hemodynamic response, the mean maximum heart rate of the total study population was 97 ± 19.1 bpm. As expected the mean maximum heart rate in the low-level treadmill group was significantly higher in comparison to the supine group (104 ± 18.6 vs 90.8 ± 17.4, P-value < 0.001). Nearly half of the entire study population experienced a decrease in systolic blood pressure greater than 10 mmHg, with 9% experiencing a decrease in more than 30 mmHg. Furthermore, there was a significant difference in blood pressure response between the two groups. Relative hypotension was significantly more frequent in the low-level treadmill group as compared to the patients who were supine during regadenoson administration (56% vs 47%, P-value < 0.001).
The frequency of symptoms associated with regadenoson administration for the entire population was as follows: chest pain 35%, dizziness/lightheadedness 16%, shortness of breath 27%, headache 1.4%, nausea 2.3%, and palpitations 5%. Transient heart block was noted in only .2% of the entire population. The patients who underwent low-level treadmill testing were significantly less likely to report symptoms of dizziness, shortness of breath, nausea, and palpitations (see Table 2). Regadenoson administration was well tolerated, with only 1.3% receiving aminophylline for severe chest pain, shortness of breath, or heart block. There was no increased frequency of shortness of breath in the patients with COPD/asthma (201 patients, 16%). In our study, 96 patients (7.6%) had reactive airway disease (asthma), and 105 patients (8.3%) had COPD (frequency of reactive airway disease in these patients was not documented).
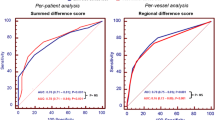
The MPI findings of the entire population as well as the population divided into the low-level treadmill exercise and supine groups during regadenoson administration are listed in Table 3. There was a trend toward significant difference between the groups in terms of overall test impression: 35% of the tests were considered abnormal in the entire study population, whereas 33% were considered abnormal in the low-level treadmill exercise group, and 37% in the supine group were considered abnormal (P-value = 0.067). There was no significant difference between the groups in terms of SRS, SSS, and summed difference score. However, the patients who underwent supine regadenoson MPI had a significantly decreased stress EF and increased stress ESV (P-values of 0.0002 and 0.024, respectively).
Discussion
In our real-world clinical setting, regadenoson appears to be a safe and well tolerated. In our patient population, although 20% identified themselves as having reactive airway disease, aminophylline administration was necessary in 1.3% of our patients. Adverse effects such as chest pain and dyspnea was comparable between our population and what has been previously reported in the literature with regadenoson administration.3,4,6-8,12 In our study, regadenoson administration in patients with known reactive airway disease (asthma) and COPD was safe if the lung exam was normal prior to MPI. Headaches were less common then in prior reports. Shortness of breath, dizziness, palpitations, transient heart block, and nausea seem to be less frequent when patients are able to exercise. We acknowledge that the patients who underwent low-level treadmill exercise regadenoson MPI had few co-morbidities, which may also contribute to the less frequent symptom profile. A prospectively designed trial which randomizes patients into the low-level treadmill vs supine regadenoson MPI would help to distinguish if exercise alone helps to diminish the side effects. A significant fall in BP seems to be more common in patients who exercise. This incremental drop in blood pressure did not correlate with symptoms and may be related to positional hypotension with a relatively dehydrated fasting population. In the recent RegEx trial, which included 60 patients, there were no differences in blood pressure response between the 39 patients who received regadenoson vs the 21 patients who received a placebo while undergoing low-level treadmill testing.12 However, this was a small study and did not evaluate the differences between patients who underwent regadenoson treadmill testing vs those who underwent regadenoson administration while supine.
Previous studies have demonstrated that highly selective (specific) A2A-agonists augment myocardial blood flow also without inducing AV block, bronchospasm, dyspnea, chest and jaw pain, flushing, or significant hypotension.12-14 Furthermore, regadenoson has been shown to effectively induce ischemia as a single fixed unit bolus in patients, regardless of age, gender, body mass index, or diabetes.7 However, in the clinical trials patients still experienced these adverse effects with regadenoson administration.3,8 This may be due to the dose-dependent receptor subtype selectivity of regadenoson, and the side effects observed may be a result of reduced selectivity for A2A receptors at the currently approved dose. Furthermore, chest pain, dyspnea, flushing, and headaches may not be a result of solely A2A receptor activation as previously thought15 but, may also be mediated by sympathetic stimulation. Previous studies have also demonstrated regadenoson’s effect on the sympathetic system.16,17 Other side effects such as high-degree (second or third) AV block were rare, consistent with prior experimental studies.18,19 In contrast, the reported incidence of second- or third-degree AV block with adenosine (140 μg kg−1 min−1 with a 6-minute infusion) is 4-5%.20
Conclusions
In a routine clinical setting, Regadenoson and Regadenoson combined with low level exercise MPI are safe and well tolerated. Shortness of breath, dizziness, palpitations, transient heart block, and nausea are less frequent when patients are able to exercise. An asymptomatic fall in BP seems to be more common in patients who undergo low-level treadmill testing.
References
Cerqueira MD, Verani MS, Schwaiger M, Heo J, Iskandrian AS. Safety profile of adenosine stress perfusion imaging: Results from the Adenoscan Multicenter Trial Registry. J Am Coll Cardiol 1994;23(2):384-9.
Balan KK, Critchley M. Is the dyspnea during adenosine cardiac stress test caused by bronchospasm? Am Heart J 2001;142(1):142-5.
Iskandrian AE, Bateman TM, Belardinelli L, Blackburn B, Cerqueira MD, Hendel RC, et al. Adenosine versus regadenoson comparative evaluation in myocardial perfusion imaging: Results of the ADVANCE phase 3 multicenter international trial. J Nucl Cardiol 2007;14(5):645-58.
Leaker BR, O’Connor B, Hansel TT, Barnes PJ, Meng L, Mathur VS, et al. Safety of regadenoson, an adenosine A2A receptor agonist for myocardial perfusion imaging, in mild asthma and moderate asthma patients: A randomized, double-blind, placebo-controlled trial. J Nucl Cardiol 2008;15(3):329-36.
Lieu HD, Shryock JC, von Mering GO, Gordi T, Blackburn B, Olmsted AW, et al. Regadenoson, a selective A2A adenosine receptor agonist, causes dose-dependent increases in coronary blood flow velocity in humans. J Nucl Cardiol 2007;14(4):514-20.
Thomas GS, Tammelin BR, Schiffman GL, Marquez R, Rice DL, Milikien D, et al. Safety of regadenoson, a selective adenosine A2A agonist, in patients with chronic obstructive pulmonary disease: A randomized, double-blind, placebo-controlled trial (RegCOPD trial). J Nucl Cardiol 2008;15(3):319-28.
Cerqueira MD, Nguyen P, Staehr S, Underwood R, Iskandrian AE, on behalf of the ADVANCE-MPI Trial Investigators. Effects of age, gender, obesity, and diabetes on the efficacy and safety of the selective A2A agonist regadenoson versus adenosine in myocardial perfusion imaging: Integrated ADVANCE-MPI trial results. J Am Coll Cardiol Imaging 2008;1(3):307-16.
Hendel RC, Bateman TM, Cerqueira MD, Iskandrian AE, Leppo JA, Blackburn B, et al. Initial clinical experience with regadenoson, a novel selective A2A agonist for pharmacologic stress single-photon emission computed tomography myocardial perfusion imaging. J Am Coll Cardiol 2005;46(11):2069-75.
Germano G, Kavanagh PB, Chen J, Waechter P, Su HT, Kiat H, et al. Operator-less processing of myocardial perfusion SPECT studies. J Nucl Med 1995;36(11):2127-32.
Berman DS, Hachamovitch R, Kiat H, Cohen I, Cabico JA, Wang FP, et al. Incremental value of prognostic testing in patients with known or suspected ischemic heart disease: A basis for optimal utilization of exercise technetium-99m sestamibi myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol 1995;26(3):639-47.
Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med 1995;36(11):2138-47.
Thomas GS, Thompson RC, Miyamoto MI, Ip TK, Rice DL, Milikien D, et al. The RegEx trial: A randomized, double-blind, placebo- and active-controlled pilot study combining regadenoson, a selective A(2A) adenosine agonist, with low-level exercise, in patients undergoing myocardial perfusion imaging. J Nucl Cardiol 2009;16(1):63-72.
Fredholm BB, AP IJ, Jacobson KA, Klotz KN, Linden J. International union of pharmacology XXV nomenclature and classification of adenosine receptors. Pharmacol Rev 2001;53(4):527-52.
Shryock JC, Belardinelli L. Adenosine and adenosine receptors in the cardiovascular system: Biochemistry, physiology, and pharmacology. Am J Cardiol 1997;79(12A):2-10.
Bertolet BD, Belardinelli L, Franco EA, Nichols WW, Kerensky RA, Hill JA. Selective attenuation by N-0861 (N6-endonorboran-2-yl-9-methyladenine) of cardiac A1 adenosine receptor-mediated effects in humans. Circulation 1996;93(10):1871-6.
Dhalla AK, Wong MY, Wang WQ, Biaggioni I, Belardinelli L. Tachycardia caused by A2A adenosine receptor agonists is mediated by direct sympathoexcitation in awake rats. J Pharmacol Exp Ther 2006;316(2):695-702.
Dhalla AK, Shryock JC, Shreeniwas R, Belardinelli L. Pharmacology and therapeutic applications of A1 adenosine receptor ligands. Curr Top Med Chem 2003;3(4):369-85.
Gao Z, Li Z, Baker SP, Lasley RD, Meyer S, Elzein E, et al. Novel short-acting A2A adenosine receptor agonists for coronary vasodilation: Inverse relationship between affinity and duration of action of A2A agonists. J Pharmacol Exp Ther 2001;298(1):209-18.
Trochu JN, Zhao G, Post H, Xu X, Belardinelli L, Belloni FL, et al. Selective A2A adenosine receptor agonist as a coronary vasodilator in conscious dogs: Potential for use in myocardial perfusion imaging. J Cardiovasc Pharmacol 2003;41(1):132-9.
Cerqueira MD, Verani MS, Schwaiger M, Heo J, Iskandrian AS. Safety profile of adenosine stress perfusion imaging: Results from the Adenoscan Multicenter Trial Registry. J Am Coll Cardiol 1994;23(2):384-9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kwon, D.H., Cerqueira, M.D., Young, R. et al. Lessons from regadenoson and low-level treadmill/regadenoson myocardial perfusion imaging: Initial clinical experience in 1263 patients. J. Nucl. Cardiol. 17, 853–857 (2010). https://doi.org/10.1007/s12350-010-9229-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-010-9229-z