
Abstract
Purpose of Review
The purpose of this review is to contribute to the knowledge about the existence of Candida auris as an emerging pathogenic fungus, multi-resistant to antifungal, and causing health care-associated infections (HCAI).
Recent Findings
C. auris emerges as yeast with clonal transmission resistance to three families of commonly used antifungals, mainly azoles (fluconazole and voriconazole), diminishing therapeutic options for the treatment of fungal infections. In 2009, C. auris was isolated for the first time in Japan and by the time of this review, it has been reported in different countries in Africa, America, Asia, and Europe.
Summary
It is important to identify yeasts of the Candida genus up to species, to perform susceptibility tests and to implement surveillance, prevention, and control measures, to minimize the global spread of this fungus, due to its impact on public health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Candida auris appears as an emerging yeast fungus, pathogenic in humans and multi-resistant to antifungals, mainly to azoles (fluconazole and voriconazole), and to a lesser extent to amphotericin B and echinocandins. This fungus can cause candidemia and invasive infections associated with health care, and may increase mortality in susceptible populations who have risk factors for the development of an invasive fungal disease (IFD), such as immuno-compromised, oncologic, and transplant patients, exposed to broad spectrum antibiotics, with prolonged stay in intensive care units and hospitalization rooms, among others [1, 2, 3••]. It has been described that C. auris infections are present mainly in the bloodstream, wounds, auditory canal, and in minor proportion in the urinary and respiratory tract, isolating particularly in the hospital environment; however, it is still unknown whether its isolation from the last three sources corresponds to an infection or colonization [2]. It has also been reported to cause infection in association with other Candida species, even when the patient receives antifungal therapy [2]. The appearance of this yeast is a cause for worldwide alert, as it is capable of transmitting resistance to antifungal quickly and clonally, which would explain the lack of clinical response to the treatment, causing a great impact on global public health [4].
Molecular Identification
In 2009, the first case of C. auris was described worldwide, having been isolated from the external auditory canal of a patient in Japan; subsequently, in five South Korean hospitals, it was also reported as the causative agent of otitis media in 15 patients [3••, 4, 5]. In 2011, three cases of C. auris bloodstream infections were reported in South Korea, stating that this species of the Candida genus was capable of causing invasive infections [3••, 5,6,7]. Afterwards, there have been reports of fungemia cases, due to this yeast, in several hospitals in India [8,9,10], South Africa [11], Kuwait [12], Venezuela, and Colombia [1, 13].
C. auris shows resistance to fluconazole and variable susceptibility to other azoles, amphotericin B and echinocandins. Its real prevalence is underestimated due to its misidentification as C. famata, C. sake, C. haemulonii, or Rhodotorula glutinis, when using conventional methods such as carbohydrate assimilation and commercial ones such as Vitek 2®, ID32C®, and API Auxacolor® in routine microbiology laboratories. It is phenotypically similar to the species that make up the Candida haemulonii Complex, and molecular methods are required to identify it properly [3, 14••]. C. auris and C. pseudohaemulonii are phylogenetically related to C. haemulonii in the Metschnikowiaceae clade, in which they have been grouped [3, 15••]. By the foregoing, C. auris represents a challenge at the time of its identification and subsequent treatment, especially when molecular methods are not available and access to antifungal other than fluconazole is limited [3, 14••, 15••].
Sequencing of the ITS regions, the major subunit of the rDNA D1/D2 domain and the region of the rDNA 28S gene is considered as the molecular reference method to correctly and definitively identify C. auris [1, 3••, 14••, 15••]. It is also possible to perform the identification by alternative techniques such as MALDI-TOF MS (Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry) which, in addition to allowing rapid and reliable identification, is also considered as a reference method for the identification of C. auris [1, 2, 3••, 13, 14••, 15••, 16,17,18].
Through the use of Amplified Fragment Length Polymorphism (AFLP) analysis technique, it was possible to differentiate C. auris from closely related species such as C. haemulonii, C. pseudohaemulonii, and C. duobushaemulonii. This technique also demonstrated the clonality of C. auris in each geographical region where outbreaks have been reported [3••, 13, 14••, 15••, 16,17,18, 19•]. Schelenz et al. using AFLP and subsequent analysis of whole genome sequencing (WGS) demonstrated the clonal relationship between C. auris isolates from four hospitals in India [20]. Meanwhile, Lockhart et al. from the whole genome sequencing of thousands of single nucleotide polymorphisms, which gathers unique clades by geographic region, found clonality among isolates that were part of each clade; additionally, they also detected mutations in the ERG11 gene that were associated with resistance to azoles in each geographic clade [14].
Virulence Factors
The C. auris genome has a size of 12.3 Mb, which possesses genes common to pathogenic species of the Candida genus that are crucial for adaptation to different environments, such as those that encode its metabolism [21, 22]. C. auris shares numerous virulence factors with C. albicans, for example, genes and pathways involved in cell wall modeling and nutrient acquisition, histidine kinase-2 systems, iron acquisition, tissue invasion, enzymatic secretion and efflux, and expulsion or ejection pumps [3••, 16, 21,22,23,24]. However, an in vitro study of multiple isolates of C. auris from different geographic regions showed that the production of enzymes was strain-dependent; in particular, the production of phospholipase and proteinase was detected in 37.5 and 64% of the evaluated isolates, respectively [25]. In general, tested strains of C. auris showed weak phospholipase activity, with most isolates not producing this enzyme [22].
A significant part of the C. auris genome codes for the two efflux pump systems of the ATP-binding cassette (ABC) family and the major facilitator superfamily (MFS). The joint action of both efflux pumps could explain the multi-resistance of this pathogen to different antifungals [16, 22]. The ABC-type efflux pumps, which have a 6G Rhodamine transporter, were significantly higher for C. auris when compared to C. glabrata, a result that supports the intrinsic resistance of C. auris to azoles [21]. On the other hand, during the analysis of the whole genome sequence of C. auris, a close phylogenetic relationship was observed with C. lusitaniae, a species of Candida with recognized intrinsic antifungal resistance [16, 22].
A determinant virulence factor of C. auris is thermotolerance, since it develops well at 37 °C (98.6 °F) and is able to maintain its viability up to 42 °C (107.6 °F). Other factors such as tolerance to high concentrations of salt and cell aggregation, in large accumulations difficult to disperse, contribute to the persistence of the strains in the hospital environment [5, 23, 26]. The virulence of C. auris has also been demonstrated in murine models with invasive candidiasis where it was observed that the aggregation of yeasts in the animal’s kidneys led to a lethal infection, suggesting that aggregation could be a mode of evasion of the immune response; thus, favoring the persistence in the tissue [27].
The ability of adhesion to inert surfaces, such as catheters, is another virulence factor of C. auris, as it allows it to form biofilms and resist the action of antifungal agents [28]. However, a recent study reported that biofilms in C. auris were significantly thinner, displaying 50% less thickness compared with those produced by C. albicans [25, 28]. On the other hand, it has been demonstrated that C. auris has a minimum adhesion capacity to the silicone elastomer (catheter material) with respect to C. albicans [25]. Therefore, the low adherence capacity of C. auris suggests that this factor is not determinant in catheter-associated candidiasis, in contrast to C. albicans and C. parapsilosis, which are frequently related to these infections [23, 25].
Candida auris in Hospital Outbreaks
Recent studies have reported the persistent colonization of C. auris, both in hospital environments and in multiple anatomical areas of patients, a condition that contributes to the increased transmissibility of this pathogen, to the contamination of the sanitary environment, and to the prolongation of outbreaks [14••, 19•, 20, 23, 29]. At a London cardiothoracic center, between April 2015 and July 2016, an outbreak occurred with 50 C. auris cases, in which AFLP technique demonstrated that isolates of this yeast from the hospital environment near the patients were the cause of the outbreak [3••, 19•]. In this same outbreak, a case of a health worker was described, who had under his care a patient highly colonized by C. auris, who presented a positive nasal swab for this pathogen [19•]. Vallabhaneni et al. indicated that between May 2013 and August 2016, the first seven cases of identified C. auris infection occurred in the USA [3••, 24, 30]. By analyzing the complete genome of C. auris isolates, it was shown that isolates of this yeast from patients entering a New Jersey hospital were almost identical to isolates obtained from patients admitted to an Illinois hospital; additionally, pathogen isolation was achieved in inert sites through samples taken from the mattress, bedside, eating table, and patient bed rail, proving that the C. auris present in the furniture and hospital setting was responsible for the outbreak, as in the London study [14••, 15••, 19•].
Several authors have emphasized that it is essential to apply strict measures for the control and prevention of infections in order to avoid the transmission of C. auris among contacts. The isolation of the patient and their contacts, the hand hygiene, use of protective clothing by health workers, decontamination of skin with chlorhexidine, cleaning of the environment with reagents based on chlorine, and final decontamination with hydrogen peroxide steam or ultraviolet (UV) light, as well as proper disposal of biological and non-biological waste, may be some of the measures to be implemented to prevent the spread of infection caused by this pathogen [3••, 19•, 20, 23, 24, 29, 30].
Emergence of Candida auris in Venezuela
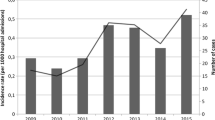
The occurrence of C. auris in Venezuela was detected in 2016, during an outbreak in a third-level hospital located in the city of Maracaibo, where 18 episodes of candidemia were described, whose causative agents were initially identified as C. haemulonii [1]. This outbreak and its persistence over time were reported to the Mycology Department of the “Rafael Rangel” National Institute of Hygiene (RRNIH), requesting the verification of the identification of the isolates being sent. The isolates were again identified as C. haemulonii by conventional and automated methods such as the Vitek 2 Compact®, and susceptibility tests were also performed by the Etest® technique. These isolates, along with others received at the RRNIH from hospitals in the city of Caracas, including other isolates from the city of Maracaibo, were sent to the Centers for Disease Control and Prevention (CDC) located in Atlanta, USA, for confirmation of identification by the MALDI-TOF technique and performance of susceptibility tests.
From a total of 81 isolates, 71 (87.7%) were confirmed as C. auris (68 from Maracaibo), five were C. haemulonii, two were C. haemulonii var.vulnera, and the others were C. duobushaemulonii, C. parapsilosis, and C. pseudohaemulonii (one of each). In terms of phenotypic C. auris features, the highlight was that the 71 isolates (100%) developed at 42 °C (107.6 °F), only 70 (98.6%) showed blastoconidia without pseudohifas in corn flour agar and in chromogenic agar presented a cream color, 50 (70%) grew in 10% sodium chloride broth, and 58 (81.7%) grew on Mycosel® agar, similar to that described by other authors [21, 22, 24, 25].
Routine microbiology laboratories, as well as some reference laboratories, located in developing countries, have neither molecular methods nor mass spectrometry for the confirmatory identification of C. auris. On the other hand, conventional and commercial identification methods are not able to discriminate between the C. haemulonii Complex and C. auris, nor between cryptic and phylogenetically related species [32]. This situation creates a serious problem of worldwide underreporting. Therefore, in terms of C. haemulonii isolates or other species of the Candida genus described above, which in turn present resistance to azoles and possibly to amphotericin B, C. auris should be suspected [33, 34]; these isolates should be sent to reference laboratories that have the necessary methodology for their correct identification and should be preserved in culture collections for further studies.
Results of susceptibility testing, performed by the Etest® method at the RRNIH, C. auris isolates showed resistance to fluconazole, voriconazole, and echinocandins (100, 95.8, and 21%, respectively), and no resistance to amphotericin B was detected. These results were confirmed by the CDC using Etest® and the CLSI reference method [33, 34]. The resistance to the fluconazole of the Venezuelan strains, coincided with reports of C. auris isolates of fungemia cases resistant to the fluconazole, with minimal inhibitory concentrations (MIC) > 64 mg/L [3••, 14••, 15••, 17, 18, 22]. Voriconazole values differ to those published by other authors, where the percentage of resistance was lower [3••, 13, 14••, 15••]. According to the results obtained with the azoles, it is possible to predict that one of the mechanisms of resistance that the Venezuelan strains present are the CDR- and MDR-type efflux pumps and we cannot rule out the point mutations in the gene encoding the 14-α-dimethyl-anesterase enzyme; both mechanisms have been described for the Candida genus [3••, 14••, 15••, 23]. With respect to echinocandins, the resistance percentage of Venezuelan strains was greater than that reported by Chowdhary et al. and Lockhart et al., and higher than the one reported in the study published by Kathuria et al. where they also reported resistance to amphotericin B [8, 14••, 15••].
Multi-Resistance to Antifungals
The emergence of this pathogen causing health care-associated infections (HCAI) is a cause for concern and alarm for all worldwide health service providers, since the transmission of resistance to the three antifungal families (azoles, polyenes, and echinocandins), frequently used for the treatment of patients with risk factors of developing invasive candidiasis, is of the clonal type [3••, 19•, 20,21,22,23,24, 29, 30, 35–38]. The investigations carried out so far, agree that C. auris infection represents a therapeutic challenge, and there is no consensus for the choice and application of an optimal treatment [23, 24].
Some studies have reported that MIC values > 32 μg/mL for fluconazole in C. auris isolates from a fungemia suggest intrinsic resistance against this drug [3••, 7,8,9]. Although there are no epidemiological cutoff values (ECV) or clinical cut-off points for C. auris, new azoles such as posaconazole, ranging from 0.06–1 μg/mL, and isavuconazole, with values < 0.015–0.5 μg/mL, have shown excellent in vitro activity against C. auris [4, 5, 7, 15••, 19•, 23, 24]. Variable susceptibility values for amphotericin B have been observed in 15 to 30% of C. auris isolates with MICs > 2 μg/mL [9, 15••] and poor resistance to echinocandins (2 to 8%) has been observed [9, 14••, 15••].
Nearly half of the isolates have multidrug-resistance (MDR) efflux pumps, which encode resistance to two kinds of antifungal families and a low percentage (4%) of resistance to all kinds of antifungal [2, 9, 12, 15••, 16, 19•, 23, 24]. Echinocandins remain the first-line therapeutic option for C. auris infections, as long as susceptibility testing is performed as soon as possible [24, 36, 38]. It has also been demonstrated that a novel oral bioavailable drug, SCY-078, which is the first inhibitor of 1,3-β-D-glucan synthesis, has a powerful activity against various Candida species, including C. auris; moreover, it showed anti-biofilms activity so it could be an important antifungal for the treatment of isolates with CDR- and MDR-type effluent pumps [3••, 20, 24, 25].
Currently, the mechanisms of resistance to the C. auris antifungal are not well defined. The recent genome project for this yeast revealed the presence of individual copies of the ERG3, ERG11, FKS1, FKS2, and FKS3 genes [3••, 15••, 16, 22, 23]. In the ERG11 mutation analysis, when comparing the C. albicans and C. auris sequences, nine amino acid substitutions were identified, which have been described in C. albicans non-wild-type resistant isolates. We further identified three additional amino acid substitutions that are decisive to significantly increase C. albicans resistance to fluconazole [21, 22]. These substitutions were strongly associated with each clade-specific geographic data by country; so we have F126T in South Africa, Y132F in Venezuela, and Y132F or K143R in India and Pakistan [14••]. Selective pressure for the indiscriminate use of antifungal drugs is likely to be the trigger for mutations leading to an early-stage antifungal resistance.
Final Comments
The authors of this review consider that the information generated so far about C. auris represents only the tip of a large iceberg. The debut of this yeast in the history of medical mycology raises many interesting questions that need to be answered in a short time, since the available information on the epidemiology and behavior of this pathogen is very recent. Research subsequent to the year 2009, held in a South Korean culture collection, detected the existence of C. auris since 1996 [3••, 7]. The obvious question that arises is whether this pathogen existed long before 1996 and simply could not be identified [3••]; however, the review of isolates preserved in culture collections from other global research centers showed no isolation of C. auris before 1996.
We do not know why C. auris emerged almost simultaneously in several countries of the world. It has been shown, at a phylogenetic level, that there are large genetic differences between geographic clades and a high clonality within them; however, a common feature is its high level of antifungal resistance, which is not frequent in other Candida species [3••, 14••, 19•, 22, 24].
C. auris is the only species in which several isolates with resistance to the four classes of antifungals have been identified [23, 24]. It is logical to think that the misuse or abuse of antifungals is one of the factors that favor resistance, without ruling out the intrinsic resistance, since there are still researches in development that seek to explain the C. auris behavior. Most of the revised publications have reported that environmental factors play an important role in outbreaks and infections associated with health care; these include the prolonged survival of the micro-organism by skin colonization, both in patients and asymptomatic carriers, as well as everything related to the environment for the operability of health centers. It is undoubtedly justified to continue investigating multiple aspects of C. auris, which apparently possess the typical characteristics of other well-known pathogens, also related to health care, such as gram-negative producers of carbapenemase, Clostridium difficile, Enterococcus resistant to vancomycin, and methicillin-resistant Staphylococcus aureus [37].
Knowing the behavior of the pathogens named above, it is expected, a greater spread of C. auris in the sanitary environments on a worldwide scale. In fact, the appearance of C. auris has prompted the Centers for Disease Control and Prevention (CDC) (http://www.cdc.gov/fungal/diseases/candidiasis/candida-auris-alert.html), the executive agency of the UK Department of Health in London (Public Health England, PHE), (https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/534174/GuidanceCandidaauris.pdf), and the European Centre for Disease prevention and Control (ECDC) (http://ecdc.europa.eu/en/publications/Publications/Candida-in-healthcare-settings_19-Dec-2016.pdf), to issue health alerts for the strict monitoring of the C. auris cases [19•, 24].
Conclusions
Future research should focus on ecology, evolution, epidemiology, and mechanisms of resistance to antifungal agents, which will provide a clearer view on the clonal transmission of C. auris and its efficient global dissemination, as well as the knowledge to be able to offer an adequate and precocious treatment, in addition to implementing measures of containment, control and prevention of infection.
As an emerging fungal pathogen, C. auris could become the agent that motivates the inclusion of opportunistic mycoses, particularly fungemia, as notifiable diseases in all public health systems at local, regional, and global levels. The rapid increase in its incidence, as well as the increase in morbidity and mortality in populations at risk of acquiring an invasive fungal disease (IFD), seems to lead in that direction.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Calvo B, Melo AS, Perozo-Mena A, Hernandez M, Francisco EC, Hagen F, et al. First report of Candida auris in America: clinical and microbiological aspects of 18 episodes of candidemia. J Inf Secur. 2016;73:369–74. https://doi.org/10.1016/j.jinf.2016.07.008.
Escandón P, Duarte C, Rivera S, Durán MA, Beltrán M, Pacheco O. Instituto Nacional de Salud de Bogotá. Colombia. Lineamientos de Vigilancia en Salud Pública 2016. Available in: http://www.ins.gov.co/lineas-de-accion/Subdireccion-Vigilancia/Lineamientos%20y%20Documentos/01%20Lineamientos%202016.pdf. Accesed 1 july, 2017.
•• Chowdhary A, Sharma C, Meis JF. Candida auris: a rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLoS Pathog. 2017;13(5):e1006290. https://doi.org/10.1371/journal.ppat.1006290. This article highlights key aspects of the behavior of C. auris in a global way, ranging from identification, epidemiology, genetics, virulence, clonal transmission, antifungal resistance, impact on public health, and treatment.
Organización Panamericana de la Salud / Organización Mundial de la Salud. Alerta Epidemiológica: brotes de Candida auris en servicios de atención de salud. 3 de octubre, Washington, D.C.:OPS/OMS; 2016. Available in: www.paho.org. Accesed: 3 july, 2017.
Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009;53:41–4. https://doi.org/10.1111/j.1348-0421.2008.00083.x.
Kim MN, Shin JH, Sung H, Lee K, Kim EC, Ryoo N, et al. Candida haemulonii and closely related species at 5 university hospitals in Korea: identification, antifungal susceptibility, and clinical features. Clin Infect Dis. 2009;48:e57–61. https://doi.org/10.1086/597108.
Lee WG, Shin JH, Uh Y, Kang MG, Kim SH, Park KH, et al. First three reported cases of nosocomial fungemia caused by Candida auris. J Clin Microbiol. 2011;49:3139–42. https://doi.org/10.1128/JCM.00319-11.
Chowdhary A, Sharma C, Duggal S, Agarwal K, Prakash A, Singh PK, et al. New clonal strain of Candida auris, Delhi, India. Emerg Infect Dis. 2013;19:1670–3. https://doi.org/10.3201/eid1910.130393.
Chakrabarti A, Sood P, Rudramurthy SM, Chen S, Kaur H, Capoor M, et al. Incidence, characteristics and outcome of ICU-acquired candidemia in India. Intensive Care Med. 2015;41:285–95. https://doi.org/10.1007/s00134-014-3603-2.
Chowdhary A, Anil Kumar V, Sharma C, Prakash A, Agarwal K, Babu R, et al. Multidrug-resistant endemic clonal strain of Candida auris in India. Eur J Clin Microbiol Infect Dis. 2014;33:919–26. https://doi.org/10.1007/s10096-013-2027-1.
Magobo RE, Corcoran C, Seetharam S, Govender NP. Candida auris-associated candidemia, South Africa. Emerg Infect Dis. 2014;20:1250–1. https://doi.org/10.3201/eid2007.131765.
Emara M, Ahmad S, Khan Z, Joseph L, Al-Obaid I, Purohit P, et al. Candida auris candidemia in Kuwait, 2014. Emerg Infect Dis. 2015;21:1091–2. https://doi.org/10.3201/eid2106.150270.
Morales-López SE, Parra-Giraldo CM, Ceballos-Garzón A, Martínez HP, Rodríguez GJ, Álvarez-Moreno CA, et al. Invasive infections with multidrug-resistant yeast Candida auris, Colombia. Emerg Infect Dis. 2017;23:1. https://doi.org/10.3201/eid2301.161497.
•• Lockhart SR, Etienne KA, Vallabhaneni S, Farooqi J, Chowdhary A, Govender NP, et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin Infect Dis. 2017;64(2):134–40. https://doi.org/10.1093/cid/ciw691. This article describes how the analysis of the whole genome sequencing (WGS) facilitates the understanding of the emergence and epidemiology of this pathogen, associated with health care infections of high mortality by clonal transmission of resistance to the antifungal agents in populations of the three continents.
•• Kathuria S, Singh PK, Sharma C, Prakash A, Masih A, Kumar A, et al. Multidrug-resistant Candida auris misidentified as Candida haemulonii: characterization by matrix-assisted laser desorption ionization-time of flight mass spectrometry and DNA sequencing and its antifungal susceptibility profile variability by Vitek 2, CLSI broth microdilution, and Etest method. J Clin Microbiol. 2015;53:1823–30. https://doi.org/10.1128/JCM.00367-15. The interesting thing about this research was the comparison of the antifungal susceptibility profile of C. auris and C. haemulonii , performed by commercial and reference methods, to detect reliable and valid resistance
Sharma C, Kumar N, Pandey R, Meis JF, Chowdhary A. Whole genome sequencing of emerging multidrug resistant Candida auris isolates in India demonstrates low genetic variation. New Microbes New Infect. 2016;13:77–82. https://doi.org/10.1016/j.nmni.2016.07.003.
Kumar A, Prakash A, Singh A, Kumar H, Hagen F, Meis JF, et al. Candida haemulonii species complex: an emerging species in India and its genetic diversity assessed with multilocus sequence and amplified fragment-length polymorphism analyses. Emerg Microbes Infect. 2016;5:e49. https://doi.org/10.1038/emi.2016.49.
Prakash A, Sharma C, Singh A, Singh PK, Kumar A, Hagen F, et al. Evidence of genotypic diversity among Candida auris isolates by multilocus sequence typing, matrix-assisted laser desorption ionization-time of flight mass spectrometry and amplified fragment length polymorphism. Clin Microbiol Infect. 2015;22(3):277.e1–9. https://doi.org/10.1016/j.cmi.2015.10.022.
• Schelenz S, Hagen F, Rhodes JL, Abdolrasouli A, Chowdhary A, Hall A, et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob Resist Infect Control. 2016;5:35. https://doi.org/10.1186/s13756-016-0132-5. This research describes the genotypic relationship of the C. auris outbreak, highlighting the appropriate identification, rapid detection and the implementation of measures to contain the transmission acquired in the hospital.
Chowdhary A, Sharma C, Duggal S, Agarwal K, Prakash A, Kumar Singh P, et al. New clonal strain of Candida auris, Delhi, India. Emerg Infect Dis. 2013;19(10):1670–3. https://doi.org/10.3201/eid1910.130393.
Sharma C, Kumar N, Meis JF, Pandey R, Chowdhary A. Draft genome sequence of a fluconazole-resistant Candida auris strain from a candidemia patient in India. Genome Announc. 2015;3(4):e00722-15. https://doi.org/10.1128/genomeA.00722-15.
Chatterjee S, Alampalli SV, Nageshan RK, Chettiar ST, Joshi S, Tatu US. Draft genome of a commonly misdiagnosed multidrug resistant pathogen Candida auris. BMC Genomics. 2015;16:686. https://doi.org/10.1186/s12864-015-1863-z.
Sears D, Schwartz BS. Candida auris: an emerging multidrug-resistant pathogen. Intern J Infect Dis. 2017;63:95–8. https://doi.org/10.1016/j.ijid.2017.08.017.
Lockhart S, Jackson B, Vallabhaneni S, Ostrosky-Zeichner L, Pappas P, Chiller T. Thinking beyond the common Candida species: need for speciation of Candida due to the emergence of multidrug resistant Candida auris. J Clin Microbiol. 2017: Posted Online 13 September 2017; https://doi.org/10.1128/JCM.01355-17.
Larkin E, Hager C, Chandra J, Mukherjee PK, Retuerto M, Salem I, et al. The emerging Candida auris: characterization of growth phenotype, virulence factors, antifungal activity, and effect of SCY-078, a novel glucan synthesis inhibitor, on growth morphology and biofilm formation. Antimicrob Agents Chemother. 2017;61:e02396–16. https://doi.org/10.1128/AAC.02396-16.
Borman AM, Szekely A, Johnson EM. Comparative pathogenicity of United Kingdom isolates of the emerging pathogen Candida auris and other key pathogenic Candida species. mSphere. 2016;1(4):e00189-16. https://doi.org/10.1128/mSphere.00189-16.
Ben-Ami R, Berman J, Novikov A, Bash E, Shachor-Meyouhas Y, Zakin S, et al. Multidrug-resistant Candida haemulonii and C. auris, Tel Aviv, Israel. Emerg Infect Dis. 2017;23:195–203. https://doi.org/10.3201/eid2302.161486.
Sherry L, Ramage G, Kean R, Borman A, Johnson EM, Richardson MD, et al. Biofilm-forming capability of highly virulent, multidrug-resistant Candida auris. Emerg Infect Dis. 2017;23:328–31. https://doi.org/10.3201/eid2302.161320.
Ruiz Gaitan AC, Moret A, Lopez Hontangas JL, Molina JM, Aleixandre Lopez AI, Cabezas AH, et al. Nosocomial fungemia by Candida auris: first four reported cases in continental Europe. Rev Iberoam Micol. 2017;34:23–7. https://doi.org/10.1016/j.riam.2016.11.002.
Vallabhaneni S, Kallen A, Tsay S, Chow N, Welsh R, Kerins J, et al. Investigation of the first seven reported cases of Candida auris, a globally emerging invasive, multidrug-resistant fungus-United States, May 2013–August 2016. MMWR Morb Mortal Wkly Rep. 2016;65:1234–7. 10.15585/mmwr.mm6544e1.
Posteraro B, Efremov L, Leoncini E, Amore R, Posteraro P, Ricciardi W, et al. Are the conventional commercial yeast identification methods still helpful in the era of new clinical microbiology diagnostics? A meta-analysis of their accuracy. J Clin Microbiol. 2015;53:2439–50. https://doi.org/10.1128/JCM.00802-15.
Mizusawa M, Miller H, Green R, Lee R, Durante M, Perkins R, et al. Can multidrug-resistant Candida auris be reliably identified in clinical microbiology laboratories? J Clin Microbiol. 2017;55:638–40. https://doi.org/10.1128/JCM.02202-16.
Clinical and Laboratory Standards Institute. Reference method for broth dilution antifungal susceptibility testing of yeasts: approved standard. CLSI document M27-A3.Wayne, PA, USA: clinical and laboratory standards institute; 2008.
Clinical and Laboratory Standards Institute. M27-S4 reference method for broth dilution antifungal susceptibility testing of yeasts: fourth informational supplement. Wayne, PA: Clinical and Laboratory Standards Institute, 2012.
Rudramurthy SM, Chakrabarti A, Paul RA, Sood P, Kaur H, Capoor MR, et al. Candida auris candidaemia in Indian ICUs: analysis of risk factors. J Antimicrob Chemother. 2017;72(6):1794–801. https://doi.org/10.1093/jac/dkx034.
Chowdhary A, Voss A, Meis JF. Multidrug-resistant Candida auris: ‘new kid on the block’ in hospital associated infections? J Hosp Infect. 2016;94:209–12. https://doi.org/10.1016/j.jhin.2016.08.004.
Anderson DJ, Chen LF, Weber DJ, Moehring RW, Lewis SS, Triplett PF, et al. Enhanced terminal room disinfection and acquisition and infection caused by multidrug-resistant organisms and Clostridium difficile (the benefits of enhanced terminal room disinfection study): a cluster-randomised, multicentre, crossover study. Lancet. 2017;389:805–14. https://doi.org/10.1016/S0140-6736(16)31588-4.
Pappas P, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1–50. https://doi.org/10.1093/cid/civ933.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of Interests
The authors declare that they have no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Topical Collection on Clinical Mycology Lab Issues
Rights and permissions
About this article

Cite this article
Dolande, M., García, N., Capote, A.M. et al. Candida auris: Antifungal Multi-Resistant Emerging Yeast. Curr Fungal Infect Rep 11, 197–202 (2017). https://doi.org/10.1007/s12281-017-0299-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12281-017-0299-0