
Abstract
Long noncoding RNAs (lncRNAs) have been shown to regulate tumor biology and might be used for cancer diagnosis, prognosis and potential therapeutic targets. Although up-regulation of lncRNA UCA1 (urothelial carcinoma-associated 1) in several cancers has been found, its role in gastric cancer remains elusive. The aim of this study was to detect the expression of lncRNA UCA1 in gastric cancer and its clinical association. The expression of UCA1 was detected in 112 pairs of tumorous and adjacent normal tissues from patients with gastric cancer, as well as in four gastric cancer cell lines and a human normal gastric epithelium cell line using RT-qPCR. Results showed that UCA1 expression was remarkably increased in gastric cancer tissues and cell lines compared with that in the normal control. Clinicopathologic analysis revealed that high UCA1 expression correlated with worse differentiation, tumor size, invasion depth and TNM stage in gastric cancer. Kaplan–Meier analysis showed that increased UCA1 expression contributed to poor overall survival (p = 0.017) and disease-free survival (p = 0.024) of patients. A multivariate survival analysis also indicated that UCA1 could be an independent prognostic marker. The levels of UCA1 in gastric juice from gastric patients were significantly higher than those from normal subjects (p = 0.016). Moreover, validation analysis showed that UCA1 levels were robust in differentiating gastric cancer patients from control subjects [area under the curve (AUC) = 0.721; 95 % confidence interval (CI) = 0.655–0.788, p < 0.01]. These results suggested that UCA1 might serve as a promising biomarker for early detection and prognosis prediction of gastric cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gastric cancer (GC) is the fourth most frequent cancer and the second cancer-related death in the world [1]. Owing to lack of reliable tools for early detection, most patients are typically diagnosed at a late stage and have poor prognosis [2, 3]. Previous research has identified that several molecular markers were associated with prognosis and played crucial roles in development of GC, but the mechanisms of GC is still unclarified. Given this, it is important to identify high sensitive and specific carcinogenesis-associated molecules, which can help us develop effective treatments and preventive measures for gastric cancer patients.
Long non-coding RNAs (lncRNAs) are widely defined as transcribed RNA molecules more than 200 nucleotides in length and lacking an open reading frame of significant length [4]. Like protein-coding RNAs, lncRNAs are transcribed by RNA polymerase II and most have the processes of 5′-end capping, 3′-end polyadenylation, intracellular transport and splicing of introns [5]. Moreover, they are involved in a wide range of biological processes, including differentiation, development and tumorigenesis [6, 7]. Thus, lncRNAs can be used as novel biomarkers and targets specifically for cancers, offering a more effective way to detect the cancer mechanism and searching a new therapeutic approach for the diseases [8].
Recently, the functions of some of the lncRNAs have been reported as regulators in the genes [9]. For example, HOX antisense intergenic RNA (HOTAIR) has been shown to repress HOXD gene expression and promote breast cancer metastasis via binding PRC2 [10]. Several studies have also observed high expression of HOTAIR in multiple malignancies, including lung carcinoma, breast cancer, pancreatic cancer, colorectal cancer and gastric cancer [11]. In addition, metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) facilitated the motility of lung cancer cells via transcriptional and/or post-transcriptional regulation of motility and proliferation-related genes [12]. Recently, multiple lines of evidences link dysregulation of lncRNAs to gastric cancer, such as HOTAIR, MALAT1, maternally expressed gene 3 (MEG3) and growth arrest-specific 5 (GAS5) [13]. However, the function of most lncRNAs in gastric cancer and their clinical significance remain incompletely understood.
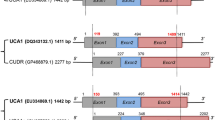
Urothelial carcinoma-associated 1 (UCA1) is a new lncRNA gene belonging to the human endogenous retrovirus H (HERV-H) family [14]. It was first identified in urinary bladder cancer (UBC) tissues and found to significantly enhance tumorigenicity and invasive potential in vitro and in vivo [15]. Forced expression of UCA1 in vitro increased colorectal cancer cell proliferation and inhibited cell apoptosis, whereas UCA1 inhibition induced growth arrest [16]. Recently, the aberrant expression of UCA1 was reported in UBC, melanoma, breast tumor, tongue squamous cell carcinomas and colorectal cancer [17]. However, no report of UCA1 in gastric cancer has been found.
In this study, the expression levels of UCA1 were measured in gastric cancer tissues and adjacent normal tissues. We also investigated the association of UCA1 with clinicopathological characteristics and overall and disease-free survival of the patients and determined its prognostic role in GC, which might dramatically improve the therapeutic strategy of GC.
Materials and methods
Patients and tissue specimens
Following obtaining informed consent from all patients, fresh tumor tissue samples and matched normal adjacent tissue (NAT) samples were collected from 112 patients with gastric cancer in the Department of General Surgery, Ningbo No. 2 Hospital (Ningbo, China) between May 2007 and February 2009. None of these patients had received chemotherapy prior to surgery. All these tissues were immediately soaked in liquid nitrogen and kept freshly frozen at −80 °C until use. All patients had a clear histological diagnosis of gastric cancer. Patients’ clinical information, such as age, sex, differentiation, Lauren type, tumor size, invasion depth, lymphatic invasion, invaded adjacent organ, perineural invasion and TNM stage, was collected and stored in a database. Clinical staging was performed according to the 7th edition of the TNM staging system. Patient characteristics are shown in Table 1. Patients were closely followed every 3 months after surgery until September 2014.
Gastric juices were collected from 49 subjects, including 26 patients with gastric cancer (mean age, 61.7 ± 14.3 years) and 23 cases with normal mucosa or minimal gastritis (mean age, 52.8 ± 14.6 years) between July 2012 and November 2013 in the Endoscopy Center of the Ningbo No. 2 hospital. For each case, the diagnosis was confirmed by endoscopic examination followed by pathological diagnosis of biopsies. Cases with normal mucosa or minimal gastritis, which had no family history of gastric cancer, were treated as the controls. The juice was initially treated and stored as described before [18]. The study protocol was approved by the Ethics Committee of Ningbo No. 2 Hospital. All specimens were handled and made anonymous following the ethical and legal standards.
Cell culture
The human gastric cancer cell lines, SGC-7901, BGC-823, MKN-28 and AGS and the human normal gastric epithelial cell line, GES-1, were obtained from the Shanghai Institute of Biochemistry and Cell Biology, Chinese Academy of Sciences (Shanghai, China). Cells were cultured in RPMI 1640 Medium (Invitrogen, Grand Island, NY) containing 10 % fetal bovine serum, 50 U/ml penicillin and 50 U/ml streptomycin in flasks at 37 °C in a humidified chamber supplemented with 5 % CO2.
RNA isolation
Total RNA was extracted from the frozen tumor, adjacent normal specimen’s tissues and cell lines using Trizol (Invitrogen), according to the manufacturer’s instructions. The extraction of gastric juice RNA was performed using Trizol LS reagent (Invitrogen), following procedures that have been described elsewhere [19]. Then, 10 µl diethylpyrocarbonate (DEPC)-treated water was added to completely dissolve the total RNA. The A260/A280 ratio was evaluated to examine total RNA purity by using SmartSpec Plus spectrophotometer (Bio-Rad, Hercules, CA, USA).
Reverse transcription (RT) and quantitative PCR (qPCR)
The 10 μl RT reactions were performed using the GoScript reverse transcription (RT) system (Promega, Madison, WI, USA) following the manufacturer’s instructions. RT-PCR was performed using the 7500 real-time PCR system (Applied Biosystems, Hayward, CA, USA). The sequences of the PCR primers for glyceraldehyde 3-phosphate dehydrogenase (GAPDH) and UCA1 were as follows: 5′-ACCCACTCCTCCACCTTTGAC-3′ (sense) and 5′-TGTTGCTGTAGCCAAA TTCGTT-3′ (antisense) for GAPDH. The primer sequences were 5′-ACGCTAAC TGGCACCTTGTT-3′ and reverse 5′-TGGGGATTACTGGGGTAGGG-3′ for UCA1, and 5′-ACTCC TGTGT GGACC TGGAT-3′ (sense) and 5′-ACCAC GACCA GCAGA ATGC-3′ (antisense) for Her-2/neu. The PCR procedures were performed as previously reported. We adopted the GAPDH RNA as an endogenous reference compared to the expression level of UCA1. The relative amount of UCA1 to GAPDH RNA was calculated using the Equation 2−ΔCT, where ΔCT = (CTUCA1 − CTGAPDH). Relative RNA expression was calculated using the method of 2−ΔΔCT [20]. All samples were performed in triplicate.
Statistical analysis
All statistical analyses were performed using SPSS software version 17.0 (SPSS Inc, Chicago, IL, USA). The relationships between UCA1 expression level and clinicopathologic factors were tested using t test or one-way analysis of variance (ANOVA). Receiver operating characteristic (ROC) curves were constructed to evaluate the diagnostic value of UCA1 levels, by plotting sensitivity versus 100 % specificity. The Kaplan–Meier survival analysis was used to examine the association between expression level and patient survival. Variables with a value of p < 0.05 in univariate analysis were subjected to multivariate analysis on the basis of Cox proportional hazards model. In all cases, p < 0.05 was considered to be statistically significant.
Results
The expression of UCA1 in gastric cancer
The relative expression of UCA1 is 17.24 ± 8.26 in gastric cancer tissues as well as 10.92 ± 6.64 in adjacent normal tissues, and the results showed a significant high expression of UCA1 in gastric cancer tissues compared with adjacent normal tissues (p < 0.01; Fig. 1a). In addition, we also found a significant high expression of UCA1 in gastric cancer cell lines (SGC-7901, BGC-823, MKN-28 and AGS) compared to normal gastric cell line GES-1 (p < 0.01, Fig. 1b).

a Relative expression of UCA1 in gastric cancer tissues and adjacent normal tissues. b Relative expression of UCA1 in four gastric cancer cell lines (SGC-7901, BGC-823, MKN-28 and AGS) and human normal gastric epithelial cell line (GES-1) analyzed by quantitative RT-PCR (*p < 0.05)
Association of UCA1 expression with clinicopathological features
For better understanding of the clinical relevance of UCA1 expression in gastric cancer, the 112 GC cases were classified into UCA1 high-expression group (n = 56) and UCA1 low-expression group (n = 56), according to the median expression level of UCA1 in all GC samples. As shown in Table 1, the UCA1 level was associated with cancer differentiation (p = 0.011), tumor size (p = 0.035), invasion depth (p < 0.01) and TNM stage (p = 0.029). However, there was no significant correlation between UCA1 expression and other clinicopathological features, such as gender, age, Lauren type, lymphatic metastasis, invaded adjacent organs, perineural invasion and expression of Her-2/neu.
Prognostic values of UCA1 expression in gastric cancer
To further evaluate the associations of UCA1 expression level with survival of patients with gastric cancer, the Kaplan–Meier method was performed. Survival analysis indicated that patients who had high UCA1 expression were correlated with shorter 5-year overall survival compared to patients who had low UCA1 expression (30.4 vs. 53.6 % p = 0.017, Fig. 2a). Moreover, the 5-year DFS of high UCA1 expression group was also significantly shorter than that of the low UCA1 expression group (26.8 vs. 48.2 %; p = 0.024, Fig. 2b). Univariate analysis for 5-year OS and 5-year DFS revealed that UCA1 expression, tumor size, lymphatic invasion, invaded adjacent organs, expression of Her-2/neu and TNM stage were prognostic factors for poor prognosis. Variables with a p value <0.05 were selected for multivariate Cox analysis. Multivariate analysis confirmed that UCA1 high expression level was retained as an independent prognostic indicator for both OS (HR = 2.351; 95 % CI 1.222–4.521; p = 0.01) and DFS (HR = 2.547; 95 % CI 1.327–4.973; p = 0.019, Table 2) in patients with GC in addition to the presence of invasion depth (p < 0.01) and lymphatic metastasis (p < 0.01) (Table 2). The results also revealed that the invaded adjacent organs correlated with OS (p = 0.015), but not with DFS (p > 0.05). The other clinicopathological features, such as tumor size and TNM stage, were not statistically significant prognostic factors (p > 0.05; Table 2).

Kaplan–Meier overall survival curves of gastric cancer patients according to the level of UCA1 expression. a Overall survival of patients with gastric cancer based on UCA1 expression status (*p < 0.05, long-rank). b Disease-free survival of patients with gastric cancer based on UCA1 expression status (*p < 0.05, long-rank)
Observation of the diagnostic value of using UCA1 as a marker
To evaluate the diagnostic performance of UCA1 in distinguishing gastric cancer tissue from normal tissue, a receiver operating characteristic (ROC) curve was constructed. The optimal cutoff value for UCA1 in GC patients was 13.74 with which the sensitivity and specificity were 67.2 and 80.3 %, respectively. The area under the ROC curve (AUC) was up to 0.721 (95 % CI = 0.655–0.788, p < 0.01, Fig. 3a). The Youden index was 0.475.

a Receiver operation characteristics (ROC) curve of using UCA1 for differentiating gastric cancer patients from normal control subjects. The area under the ROC curve (AUC) is up to 0.721. b Relative expression of gastric juice UCA1 from gastric cancer patients and normal subjects
Gastric juice is a simple and easy-to-obtain sample which can provide available information in the diagnosis of gastric cancer. To evaluate the diagnostic value of UCA1, the levels of gastric juice UCA1 were detected in gastric juice between GC patients and normal cases. Interestingly, we found that UCA1 levels in gastric juice from patients with gastric cancer were significantly higher than those from normal subjects (p = 0.016, Fig. 3b).
Discussion
Molecular biomarkers incorporated with clinicopathological factors might improve patient therapeutic strategy of gastric cancer [21, 22]. Recently, many evidences suggested that dysregulated expression of lncRNAs have been linked to clinicopathological features in cancer [23]. HULC (highly up-regulated in liver cancer), which is high expressed in hepatocellular carcinoma, could induce the HBx-enhanced cell proliferation through up-regulating p18 [24]. Meanwhile, plasma HULC might act as a promising novel biomarker for the detection of hepatocellular carcinoma [25]. Overexpression of lncRNA GAS5 could inhibit cell proliferation both in vitro and in vivo and predict a poor prognosis in patients with colorectal cancer [26]. Metastasis-associated lung adenocarcinoma transcript 1 (MALAT1) was reported to be a negative prognostic factor for NSCLC, colon, breast, gastric and pancreatic cancer patient survival [27, 28]. These findings suggested that lncRNAs might play a crucial role in carcinogenesis and have a great impact on clinical application.
UCA1 is located at the human chromosome 19p13.12, which was first discovered as a novel noncoding RNA gene dramatically up-regulated in bladder transitional cell carcinoma using reverse transcription-PCR by Wang [29] in 2006. A growing number of evidence also examined the expression level and function of UCA1 in different types of malignancies [30]. However, the UCA1 expression level and biological role in GC remain unclear. Since several studies reported that UCA1 acted as an oncogenic lncRNA in various tumors, we hypothesized that UCA1 also had similar impact on the progression of GC, which might be associated with the prognosis of GC patients.
To confirm these hypotheses, we firstly investigated whether UCA1 was detectable and altered in 112 pairs of gastric cancer tissues and adjacent normal tissues by RT-qPCR. Results showed that the expression level of UCA1 was increased in GC compared with that in adjacent normal specimens. Additionally, UCA1 expression is markedly increased in gastric cancer cell lines compared with normal gastric epithelium cell line. An ROC curve was constructed for differentiating GC tissues from normal tissues, and the results indicated that the AUC was 0.721. Gastric juice UCA1 levels in gastric cancer patients were further found to be significantly higher than those of normal subjects. Previously, several studies showed that UCA1 was increased in various tumors [31, 32]. Our results provided the first evidence that expression level of UCA1 was up-regulated in human GC. These findings indicated that UCA1 may play a positive role in GC development.
Then we went further to evaluate the association between UCA1 expression and different clinicopathological parameters in gastric cancer tissues. Our findings revealed that high UCA1 expression was more frequently detected in tumors with worse differentiation, larger tumor size, deeper invasion depth and advanced TNM stage. Since the clinicopathological parameters of tumor size, depth of invasion and tumor stage represent partially the deterioration and progress of the tumor, UCA1 might be involved in the tumorigenesis and progression of gastric cancer. This association is consistent with previous findings in bladder and colorectal cancers, which also found that UCA1 could promote cell proliferation, migration and invasion in these tumors [16, 33].
To further confirm the prognostic value of UCA1 overexpression, Kaplan–Meier analysis and log-rank test were performed. Our results showed that patients with a high expression of UCA1 tended to have shorter overall and disease-free survival than patients with lower levels. Furthermore, multivariate Cox analysis proved that UCA1 constituted a prognostic indicator independent of adjusted well-known prognostic factors for GC including serum CEA level, tumor size, invasion depth, lymphatic invasion and TNM stage. Therefore, UCA1 might serve to identify high-risk individual patients with GC who have higher risk of death and, thus, are good candidates for receiving more aggressive and effective treatment. Based on available evidences, the negative effect of UCA1 on cancer survival might be to some extent caused by its target gene. In the study by Wang et al. [34], UCA1 could induce tumor cell growth through blocking recruitment of Brahma-related gene 1 (BRG1) to target promoters. However, the precise molecular mechanisms underlying the high expression of UCA1 in GC and its function are still incompletely known. More studies should be applied to elucidate the molecular mechanisms of both the cause and effects of altered expression of UCA1 in the progression of GC.
In conclusion, we demonstrated that UCA1 was significantly up-regulated in GC tissues and some GC cell lines. Its level was associated with tumor progression and poor prognosis. Our data also implied that UCA1 might be capable of distinguishing between cancerous and non-cancerous conditions by examining the expression of UCA1 in tissues and gastric juices. In addition, the high risk of recurrent GC might be predicted by evaluating UCA1 expression in GC samples collected. These findings suggested that UCA1 might be useful as a diagnostic and prognostic biomarker for GC and might be a possible target for diagnosis and gene therapy. However, larger clinical and prospective studies will need to be performed to confirm these preliminary results.
References
de Martel C, Forman D, Plummer M. Gastric cancer: epidemiology and risk factors. Gastroenterol Clin North Am. 2013;42:219–40.
Patru CL, Surlin V, Georgescu I, Patru E. Current issues in gastric cancer epidemiology. Rev Med Chir Soc Med Nat Iasi. 2013;117:199–204.
Kawaguchi T, Komatsu S, Ichikawa D, Kubota T, Okamoto K, Konishi H, et al. Clinical significance of chemotherapy for geriatric patients with advanced or recurrent gastric cancer. Mol Clin Oncol. 2015;3:83–8.
Hauptman N, Glavac D. Long non-coding RNA in cancer. Int J Mol Sci. 2013;14:4655–69.
Ernst C, Morton CC. Identification and function of long non-coding RNA. Front Cell Neurosci. 2013;7:168.
Kunej T, Obsteter J, Pogacar Z, Horvat S, Calin GA. The decalog of long non-coding RNA involvement in cancer diagnosis and monitoring. Crit Rev Clin Lab Sci. 2014;51:344–57.
Maass PG, Luft FC, Bahring S. Long non-coding RNA in health and disease. J Mol Med (Berl). 2014;92:337–46.
Wang GY, Zhu YY, Zhang YQ. The functional role of long non-coding RNA in digestive system carcinomas. Bull Cancer. 2014;101:27–31.
Song X, Cao G, Jing L, Lin S, Wang X, Zhang J, et al. Analysing the relationship between lncRNA and protein-coding gene and the role of lncRNA as ceRNA in pulmonary fibrosis. J Cell Mol Med. 2014;18:991–1003.
Li JT, Wang LF, Zhao YL, Yang T, Li W, Zhao J, et al. Nuclear factor of activated T cells 5 maintained by Hotair suppression of miR-568 upregulates S100 calcium binding protein A4 to promote breast cancer metastasis. Breast Cancer Res. 2014;16:454.
Yao Y, Li J, Wang L. Large intervening non-coding RNA HOTAIR is an indicator of poor prognosis and a therapeutic target in human cancers. Int J Mol Sci. 2014;15:18985–99.
Park JY, Lee JE, Park JB, Yoo H, Lee SH, Kim JH. Roles of long non-coding RNAs on tumorigenesis and glioma development. Brain Tumor Res Treat. 2014;2:1–6.
Qiu MT, Hu JW, Yin R, Xu L. Long noncoding RNA: an emerging paradigm of cancer research. Tumour Biol. 2013;34:613–20.
Wang Y, Chen W, Yang C, Wu W, Wu S, Qin X, et al. Long non-coding RNA UCA1a(CUDR) promotes proliferation and tumorigenesis of bladder cancer. Int J Oncol. 2012;41:276–84.
Wang F, Li X, Xie X, Zhao L, Chen W. UCA1, a non-protein-coding RNA up-regulated in bladder carcinoma and embryo, influencing cell growth and promoting invasion. FEBS Lett. 2008;582:1919–27.
Han Y, Yang YN, Yuan HH, Zhang TT, Sui H, Wei XL, et al. UCA1, a long non-coding RNA up-regulated in colorectal cancer influences cell proliferation, apoptosis and cell cycle distribution. Pathology. 2014;46:396–401.
Shi X, Sun M, Liu H, Yao Y, Song Y. Long non-coding RNAs: a new frontier in the study of human diseases. Cancer Lett. 2013;339:159–66.
Zhang X, Cui L, Ye G, Zheng T, Song H, Xia T, et al. Gastric juice microRNA-421 is a new biomarker for screening gastric cancer. Tumour Biol. 2012;33:2349–55.
Shao Y, Ye M, Jiang X, Sun W, Ding X, Liu Z, et al. Gastric juice long noncoding RNA used as a tumor marker for screening gastric cancer. Cancer. 2014;120:3320–8.
Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods. 2001;25:402–8.
Pinheiro Ddo R, Ferreira WA, Barros MB, Araujo MD, Rodrigues-Antunes S, Borges Bdo N. Perspectives on new biomarkers in gastric cancer: diagnostic and prognostic applications. World J Gastroenterol. 2014;20:11574–85.
Razzak M. Genetics: new molecular classification of gastric adenocarcinoma proposed by The Cancer Genome Atlas. Nat Rev Clin Oncol. 2014;11:499.
Serviss JT, Johnsson P, Grander D. An emerging role for long non-coding RNAs in cancer metastasis. Front Genet. 2014;5:234.
Du Y, Kong G, You X, Zhang S, Zhang T, Gao Y, et al. Elevation of highly up-regulated in liver cancer (HULC) by hepatitis B virus X protein promotes hepatoma cell proliferation via down-regulating p18. J Biol Chem. 2012;287:26302–11.
Xie H, Ma H, Zhou D. Plasma HULC as a promising novel biomarker for the detection of hepatocellular carcinoma. Biomed Res Int. 2013;2013:136106.
Yin D, He X, Zhang E, Kong R, De W, Zhang Z. Long noncoding RNA GAS5 affects cell proliferation and predicts a poor prognosis in patients with colorectal cancer. Med Oncol. 2014;31:253.
Gutschner T, Hammerle M, Diederichs S. MALAT1—a paradigm for long noncoding RNA function in cancer. J Mol Med (Berl). 2013;91:791–801.
Tano K, Akimitsu N. Long non-coding RNAs in cancer progression. Front Genet. 2012;3:219.
Wang XS, Zhang Z, Wang HC, Cai JL, Xu QW, Li MQ, et al. Rapid identification of UCA1 as a very sensitive and specific unique marker for human bladder carcinoma. Clin Cancer Res. 2006;12:4851–8.
Yang G, Lu X, Yuan L. LncRNA: a link between RNA and cancer. Biochim Biophys Acta. 2014;1839:1097–109.
Fang Z, Wu L, Wang L, Yang Y, Meng Y, Yang H. Increased expression of the long non-coding RNA UCA1 in tongue squamous cell carcinomas: a possible correlation with cancer metastasis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;117:89–95.
Tian Y, Zhang X, Hao Y, Fang Z, He Y. Potential roles of abnormally expressed long noncoding RNA UCA1 and Malat-1 in metastasis of melanoma. Melanoma Res. 2014;24:335–41.
Xue M, Li X, Li Z, Chen W. Urothelial carcinoma associated 1 is a hypoxia-inducible factor-1α-targeted long noncoding RNA that enhances hypoxic bladder cancer cell proliferation, migration, and invasion. Tumour Biol. 2014;35:6901–12.
Wang X, Gong Y, Jin B, Wu C, Yang J, Wang L, et al. Long non-coding RNA urothelial carcinoma associated 1 induces cell replication by inhibiting BRG1 in 5637 cells. Oncol Rep. 2014;32:1281–90.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (No. 81130057 and 81201905) and Nature Science Research Grants in University of Jiangsu Province of P.R. China (No. 12KJB320009).
Conflict of interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Q. Zheng and F. Wu contributed equally to this work.
Rights and permissions
About this article

Cite this article
Zheng, Q., Wu, F., Dai, WY. et al. Aberrant expression of UCA1 in gastric cancer and its clinical significance. Clin Transl Oncol 17, 640–646 (2015). https://doi.org/10.1007/s12094-015-1290-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-015-1290-2