
Abstract
In order to evaluate the perceived quality of training and education among young Italian radiation oncologists (age <40), AIRO Giovani (Italian Association of Radiation Oncology-Young Members Working Group) carried out a nationwide online survey in 2011, employing a 63-item-based questionnaire, addressed to physician’s self-perception of personal training experience (during decade 2001–2011). Issues explored investigated demographics data, duration/organization/content/characteristics of residency programs, the quality of education in clinical oncology, radiation oncology, management and communication attitudes. A total of 382 questionnaires were sent out to physicians and 217 (56.8 %) were returned with 197 (51.6 %) appropriately filled in and considered for the analysis. The general perception of education and training is positive in most of the explored fields, however some specific contexts and skills still require optimization (combination therapy, peculiar clinical scenarios, particular radiotherapy technical issues, structural organization of residency programs). The present report is expected to be useful for residents, program directors and scientific societies (such as AIRO), to further continue the effort in the improvement of training in radiation oncology.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The Italian Association of Radiation Oncology (AIRO) is a scientific society for board-certified physicians in radiation oncology (RO) and RO trainees attending residency programs as delivered within the Italian University system [1]. Aims of the society are the promotion of RO as a medical discipline, the improvement of quality of care in cancer and the integration of RO within clinical oncology specialties, the management of institutional and health issues across the country and finally the support of research, education and training of RO professionals. The European Society for Radiotherapy and Oncology (ESTRO) endorsed at first a ‘minimum curriculum for the theoretical education in RO in Europe’, as early as 1991, contributing to a standard for training and education in Europe [2]. In 2004, the second edition of the curricula for the specialist education and training of medical practitioners in radiotherapy (radiation oncologists) was edited and endorsed by 35 European member states [3]. In 2011, the Core Curriculum was further updated shifting the focus from theoretical knowledge and skills to competency-based education and training system [4]. A depiction of educational and training demographics, characteristics and quality as career motivation and professional opportunities of residents and young radiation oncologists is undertaken on a regular basis in several European countries and in the United States [5–7]. Italy does not participate in these at present. The survey on training among young radiation oncologists in Italy (STYRO) project is a survey conducted among young AIRO members concerning their ongoing or recently completed residency program, to investigate perception on the quality of training, educational needs and expectations for their professional future as well as agreement with ESTRO core curriculum indications. The present survey was conducted in 2011, and in this study, we report the results.
Materials and methods
The STYRO project questionnaire was designed to investigate demographics and pertinent issues and suggestions also raised by the most recent ESTRO-endorsed core curriculum, like clinical oncology education, RO-specific training, relational and management attitude and to provide a global judgment on the residency program as attended [4]. The AIRO database was consulted in order to target young members (<40 years; both young specialists and residents) to participate in the survey. A total of 382 young professionals were identified and contacted via e-mail for participation to the STYRO project (anonymity was addressed in the presentation letter). Respondents attended RO residency programs within Italian University Institutions throughout a time period ranging from 2001 to 2011. Since 2009, the national residency program was modified in order to provide a competency-based educational system; hence, the residents participating in this survey were subdivided into an ‘old’ program or into a ‘new’ one. The survey was conducted on-line, employing the Internet-based SurveyMonkey platform (www.surveymonkey.com), and completion took about 15 min. The survey was open from June to December 2011. The completed questionnaires were collected and analyzed anonymously during 2012.
Questionnaire development
A 63 item-based, non-validated, self-produced questionnaire was designed by the STYRO Project Working Group (see “Appendix” for complete form). In order to assess whether questions were neutral and easy to understand, a sample questionnaire was administered to members (10 persons) of the Directive Council of AIRO Giovani (AIRO-Young Members Working Group). The format was consequently modified following their suggestions. In order to assess face validity of the questionnaire, the subsequent draft was sent to 3 external reviewers for suggestions regarding improvement of content, wording and flow of presented questions. The items were grouped in different domains according to pertinence: oncological education, medical oncology, tumor subsets, technical skills and special techniques in RO, research and fundamental disciplines, management skills, relational skills toward colleagues and patients and training organization. A Likert scale approach was used for response categories in case of multi-point items. A 4-step evaluation scale was employed to categorize answers involving a qualitative judgment on investigated issues (poor, moderate, good, excellent), specifically for all domains except training organization. A 5-step evaluation scale was used to categorize answers involving the frequency of items (always, often, sometimes, rarely, never), namely for the organization of training domain. Binary responses were reported as a yes/no mutually exclusive choice. An exploratory factor analysis to explore the construct and underlying factor structure of the questionnaire was not performed. Conversely, psychometric properties of multi-point items were analyzed (on the whole cohort on a post-audit basis) to estimate internal consistency, with the calculation of the Cronbach’s α of the overall questionnaire and of the different domains. In the 4-factor solution, α was 0.696; in the 5-factor solution, α ranged from 0.688 to 0.865. Cronbach’s α of the overall questionnaire was 0.907. Descriptive statistical analysis was performed using the Origin 9 software (OrginLab Corporation, Northampton, MA).
Statistical analysis
In order to provide a glimpse into eventual differences occurring during the decade (2001–2011) under investigation in terms of perceived quality of training during the residency program, a subgroup comparison was performed, according to the educational status of respondents (in training: residents; trained: specialists). Pearson’s chi-square (PCS) tests for independence (one degree of freedom at significance level α = 0.05 and α = 0.10) were performed using cross-tabulations for all the 63 investigated items. The investigation evaluated whether the dichotomous variable ‘educational status’ might be associated with the frequency distributions of the analyzed events considered as categorical variables in our sample (high vs low level of perceived quality: excellent/good vs moderate/poor; high vs low level of frequency: always/often vs low sometimes/rarely/never). The events we considered were mutually exclusive and had a total probability of 1. A test of goodness of fit was performed (assessing whether the observed frequency distribution differed from a theoretical distribution). Quantitative statistical analysis was performed with SPSS Statistics Software version 12.0 (IBM, Armonk, NY).
Results
A total of 217/382 (56.8 %) questionnaires were filled in at the end of December 2011. Approximately half, 197/382 (51.6 %), were completely filled in and consequently taken into account for the present analysis; those partially completed were automatically disregarded by the electronic platform.
General information and demographics
Among the 197 attending physicians, 144 were (73.1 %) female and 53 (26.9 %) male; mean age was 33.1 (range 25–41); about 2/3 of them were specialists (63.5 %), while the remaining were trainees (36.5 %); mean age among specialists was 34.6 (range 29–39) and 30.4 (range 25–39) among residents; most of the trainees (70.8 %) were attending their third or fourth year of the residency program; residents mainly belonged to the old residency module (70.8 vs 29.2 %); almost the same balance between male and female was found among residents and specialists (72.2 vs 27.8 %; 73.6 vs 26.4 %). For detailed demographic characteristics (analyzed respondents, not-analyzed respondents, not-respondents), see Table 1.
Clinical oncology
Oncological education
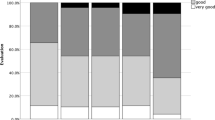
Up to 84.3 % of respondents judged their ability as excellent/good to make proper diagnosis and accurate staging of a given oncological setting (good: 73.1 %); up to 76.7 % of them judged their skills as good/excellent in the field of prognosis definition and therapy selection (good: 70.1 %); the expertise in molecular oncology was considered moderate/poor in 69.6 % of questionnaires (moderate: 50.8 %); knowledge in the context of evidence-based oncology was judged good/excellent by 67 % of radiation oncologists (good: 58.9 %); the operational knowledge of risks factors in oncology was considered excellent/good by 82.2 % of respondents (good: 76.6 %); up to 56.9 % of questionnaires judged poor/moderate the knowledge and management ability of the error in medicine (moderate: 40.1 %, but good: 41.6 %). For details see Fig. 1.

Oncological education
Medical oncology
The expertise in day hospital clinical activities and in those with inpatients, the management of concomitant systemic therapies and treatment-related side effects were considered good/excellent by 55.8 % (good: 47.2 %, but moderate: 29.9 %), 52 % (good: 47 %, but moderate: 29 %), 54.7 % (good: 51.3 %, but moderate: 30.5 %) and 81.2 % (good: 68 %) of respondents, respectively (Fig. 2).

Medical oncology
Skills according to tumor subset
Knowledge and skills were judged excellent/good for breast (90 %; excellent: 31 %), genito-urinary tract (76 %; good: 60 %), central nervous system (69 %; good: 54 %), gastro-intestinal tract (65 %; good: 52 %, but moderate: 24 %), thoracic region (65 %; good: 54 %, but moderate: 26 %) and head and neck region (64 %; good: 48 %, but moderate: 24 %) cancers. For onco-hematology and pediatric oncology, the majority of respondents judge their skills as moderate/poor (52 and 85 %, respectively). Specifically, for onco-hematology, negative answers were subdivided (with respect to total answers) into moderate (34 %) and poor (18 %); for pediatric oncology, into moderate (21 %) and poor (64 %) (Fig. 3).

Skills according to tumor subset
Radiation oncology
Technical skills in RO
Definition of volumes of interest was perceived as excellent/good in 81.7 % (good: 67 %); the confidence in dose prescription was thought to be excellent/good in 65 % (but moderate: 27.9 %); treatment plan evaluation was judged excellent/good by 69 % of physicians (but moderate: 22.3 %); expertise in the use of treatment planning software (TPS)—calculating algorithms—radiobiological modeling was excellent/good for 28.9 % (good: 25.9 %) and moderate/poor for 71.1 % (moderate: 38.6 %); treatment interruption management was thought to be excellent/good in 57.9 % of cases (but moderate: 33.5 %); knowledge and skills in 3D CRT were excellent/good for 72.1 % (good: 56.8 %) of respondents; finally, expertise in IGRT and its clinical implications was considered excellent/good by 50.7 % (good: 42.6 %) and moderate/poor by 49.3 % (moderate: 25.9 %). See Fig. 4 for details.

Technical skills in radiation oncology
Special techniques
Knowledge and expertise in IMRT was considered excellent/good in 53.8 % of questionnaires (good: 49.7 %, but moderate: 27.4 %); stereotactic approaches were excellent/good for 43.7 % (good: 37.6 %) of radiation oncologist (moderate: 28.9 %; poor: 27.4 %); the majority of respondents considered moderate/poor their skills in total body irradiation and brachytherapy (78 %; moderate: 32 %; poor: 46.2 %) and intra-operative radiotherapy (84.8 %; poor: 65.5 %) (Fig. 5).

Special techniques in radiotherapy
Research and fundamental disciplines
Most of the respondents had a strong interest in clinical research in RO (excellent/good: 70.6 %), but few felt to have a valuable experience (moderate/poor: 68 %). Knowledge in radioprotection, medical physics and radiobiology was considered moderate/poor by 68 % (moderate: 35.5 %), 69.5 % (moderate: 47.7 %) and 72.1 % (moderate: 44.7 %), respectively (Fig. 6).

Research and fundamental disciplines
Relational and managing attitude
Management skills
The ability to relate to patients, patient organizations and/or healthcare companies was considered excellent/good by 52.8 % (good: 43.7 %, but moderate: 39.6 %) of respondents; the ability to supervise students was perceived as good/excellent in 70.6 % of questionnaires (good: 60.4 %, but moderate: 23.9 %); the expertise in using technology to optimize working activities was thought to be good/excellent in 72.1 % (good: 64 %, but moderate: 23.4 %); the capability to use technology to optimize patients management was considered good–excellent by 82.4 % of radiation oncologists (good: 70.6 %); the ability in the organization of working activities was judged as good/excellent by 87.3 % (good: 65 %) (Fig. 7).

Management skills
Relational skills toward colleagues
Helpfulness toward colleagues was considered good/excellent by 95.4 % of radiation oncologists (excellent: 39.6 %); the ability to constructively attend to interdisciplinary meetings was perceived as good/excellent by 80.8 % (good: 57.4 %); the attitude toward sharing scientific knowledge with colleagues was considered good/excellent in 93.9 % of questionnaires (excellent: 35 %); the ability to help colleagues was judged as good/excellent in 95.6 % (excellent: 38.6 %) (Fig. 8).

Relational skills toward colleagues
Relational skills toward patients
The ability to listen to patients was considered good/excellent by 97.5 % of respondents (excellent: 46.2 %); the ability to understand patients was perceived as good/excellent by 83.9 % (good: 65.5 %); the sensibility to give bad news to patients and relatives was thought to be good/excellent in 77.7 % of questionnaires (good: 64 %); the attitude to deal with problematic medical, psychological, social issues was considered excellent/good in 79.2 % (good: 65 %); the ability to build a constructive relationship with patients was judged as good/excellent by 92.4 % of respondents (good: 66 %) (Fig. 9).

Relational skills toward patients
Organization of training during residency program
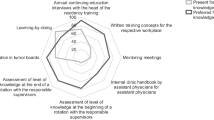
For a detailed depiction of this issue see Fig. 10. A rotational program was scheduled in most of the cases (92.9 %) with a slight decrease in the real accomplishment (75.1 %). Lectures and seminars were undertaken on a regular basis in 42.1 % and sporadically in 21.8 %; 36 % of respondents declared lack of these. Training in other clinical and imaging disciplines was regularly undertaken in 13.7 %, sporadically in 17.3 % but lacking in 69 % of questionnaires. Training in foreign institution was regularly provided during residency in 26.8 %, sporadically in 17.8 % but not in 64.5 %. Practical training in radiobiology laboratories was lacking for 91.9 % of respondents. Time to study was considered sufficiently by 31 % and insufficient by 38 %. Economic support to attend meetings and courses was provided on a regular basis for 29 % of respondents, while it was sporadic for 24 % and not available for 47 %. Constant active involvement in research programs was declared by 44 % of questionnaires, sporadic by 24 % and not at all by 32 %. Conversely a formal research period within the rotational program was present in 19 % (missing in 62 %). Involvement in teaching activities (tutorial, seminars) within the School of Medicine was not expected in 75 % (sporadic 17 %). Involvement in quality assurance programs was undertaken by 32 % of respondents but not in 68 %.

Organization of training
Miscellaneous
The most represented factors influencing the choice to attend a residency program in RO were (multiple answers allowed): (a) consistent teaching lessons in RO and clinical oncology during the medical school program (113/197), (b) advice received by colleagues and friends (60/197), (c) intrinsic interest in RO, radiobiology and/or oncological research (53/197), (d) previous working experience in the field of clinical oncology (47/197), (e) expectancy of favorable professional quality of life during and after residency program (36/197). The duration of the residency program was considered adequate for a proper professional profile by 85.8 % of respondents. The organization and characteristics of the residency program adequately satisfied the requirements for an undemanding inclusion in the professional activities for 69.9 % of radiation oncologists with finalized training (125 respondents). The monthly income for a resident was considered adequate in 75.6 % of questionnaires. Professional expectations at the end of the residency program were (multiple answers allowed): full staff position within a public hospital (86 %), academic career or research activity (22 %), full staff position within a private hospital (15 %), possibility to work abroad (12 %). The knowledge of the ESTRO core curriculum was considered moderate/poor by 78.6 % of radiation oncologists and the correspondence of the attended residency program with the ESTRO core curriculum was considered insufficient by 61.9 % of respondents; a more extended correspondence between Italian residency programs and European standards was requested by 93.4 % of colleagues.
Statistical comparison between trainees and specialists
Among the investigated issues, only 2 items reached a PCS value ≥3.84 (critical value at α = 5 %), namely head and neck cancer management and treatment plan evaluation. A PCS value ≥2.71 (critical value at α = 10 %) was reached for diagnosis and staging in oncology, volume of interest definition, IMRT, side effects management and radioprotection. For details see Table 2.
Discussion
In recent years, several substantial modifications have been observed within the field of RO, including new therapeutic opportunities driven by technologic improvements (imaging, planning and delivery), evidence-based clinical data supporting the role of radiotherapy in different clinical scenarios, a more frequent integration with chemotherapy and targeted agents and an expanding perspective endorsing the multidisciplinary approach in the management of cancer patients [8–10]. All these innovations highlight the need for a more accurate investigation and understanding of RO education and training, focusing on the structure and characteristics of residency programs developed within academic Institutions, in order to look for a virtuous correspondence between radiotherapy training environments and educational needs to end up with an updated professional profile consistent with modern RO. In this sense, the recent ESTRO Core curriculum (2011) included a modification in the general orientation of RO education, shifting the attention from theoretical knowledge and skills to competency-based education and training [4]. An ideal formation should encompass student’s ability to gather constructively knowledge, skills and attitude to provide an adequate professional act targeted to a specific situation [4]. This approach has been inspired by the 7 roles identified by the Royal College of Physicians and Surgeons of Canada to delineate the most comprehensive characteristics of a physician in terms of competencies: medical expertise, communication, collaboration, knowledge science, health advocacy/social actions, management/organization and professionalism [11]. As pointed out by the ESTRO core curriculum, this paradigm shift requires a substantial extension of medical education with a specific endorsement of training in practical environment, competency-based supervision and evaluation during training [4]. The STYRO 2011 project, the first being conducted in Italy, was designed to assess the perceived quality of training during the residency program period, as to portray the appropriateness and depth of clinical education as well as the likelihood of didactics, research programs and working condition (and other pertinent items) among Italian radiation oncologists and RO residents attending residency programs throughout Italy in a time period ranging from 2001 to 2011. The STYRO project was also planned to be a potential useful source of data regarding training programs and educational opportunities to be used for eventual system ameliorations. The 2009 update of the residency programs in RO performed by the Italian Ministry of Instruction, University and Research (MIUR) increased the duration of the whole educational path to 5 years (instead of 4 as previously), dividing it into 2 steps: (1) a common segment (together with Radiology and Nuclear Medicine) devoted to acquire a theoretical and practical knowledge and a proper attitude to build up a consistent methodology and culture to enable professional, decisional and operative autonomy (basic information underlying professional skills, molecular biology and genetics, disease pathogenesis, methodology in prevention/diagnosis/cure/follow up in oncology, communication ability with patients and cooperation capability with colleagues) (2) a second segment addressing pertinent RO issues and including basic objectives (medical physics, informatics, statistics, tumor epidemiology, pathology, biology, radioprotection, dosimetry, dose calculation, quality assurance as well as clinical pharmacology and anti-neoplastic drugs), RO-specific objectives (radiobiology, bio-imaging, clinical oncology, multidisciplinary management of cancer) and ancillary integrated objectives (organization and administration of a RO department, legal issues in RO, science and research) [12]. In order to provide a competency-based approach to the residency program, the 2009 update described in details type and timing of practical abilities and skills to be obtained during training: at least 18 months spent within an oncological day hospital and ward; at least 6 months spent also within a brachytherapy department; at least 36 months spent in an external beam radiotherapy (EBRT) section of a RO department. At the end of the residency program, every resident should have taken care of at least 450 patients in total and have been involved in controlled clinical trials and research protocols. At the time of the STYRO 2011 project, the vast majority of physicians attended or were attending the ‘old’ residency program (125 specialists and 51 residents; 89 % of the sample size), while only 21 respondents were attending the residency program as updated in 2009 (11 %). Thus, practical repercussions of the 2009 modifications of the educational residency program are likely to be observed in forthcoming years. The STYRO 2011 project was hence intended to provide a picture of the perceived quality of training in Italy among a decade (2001–2011). We had a response rate of 56.8 % (with 51.6 % questionnaire properly filled in for analysis). These results were considerably higher than response rates observed during previous survey experiences performed by the AIRO-Young Members Working Group, which ranged from 28 to 41 % [13–16]. However, to avoid selection bias, attending physicians were previously informed about the anonymity of the whole project. Moreover, non-respondents characteristics were collected and found similar to those of attending subjects (Table 1). Our questionnaire design process did not evaluate the most appropriate factorial solution in terms of content and meaning of underlying domains; however, the Cronbach’s α values for both the overall questionnaire and the single domains stand in the range of acceptable/good reliability. One potential pitfall might be the lack of evidence on the degree of accuracy regarding the evaluation of performance of respondents, since no standardized testing has been performed before administration of the STYRO 2011 Project questionnaire. Another one could be the fact that the slenderness of the sample size did not allow us to perform a subset analysis according to the level of training at the time of the questionnaire administration; hence, some of the answers given might reflect more the timepoint within the educational program, than a comprehensive evaluation of the item given with finalized training perspective. In adjunct it is known as a general finding the fact that individuals tend to over-rate their own training and practice to enlighten their professional abilities. However, in the present survey, oncological education was generally perceived as high quality (risk factors/diagnosis/staging/therapy/prognosis in oncology, evidence-based oncology), but few gaps were perceived in the knowledge of molecular oncology and in the management of the error in medicine/oncology (maybe an issue not clearly addressed during training). In the area of medical oncology, training was only partially perceived as positive; this finding seems to point out the need for a more relevant educational effort in theoretical and practical implications of medical oncology issues in order to allow RO professionals to obtain the requested skills to appropriately manage systemic therapies, particularly within an inpatient ward/day hospital environment. Moreover, the expertise was considered consistent for almost all tumor subsets (breast, genito-urinary tract, central nervous system, gastro-intestinal tract, thoracic and head/neck region cancer), except for rare oncological contexts such as pediatric malignancies (70 % moderate/poor expertise) and onco-hematology (52 % moderate/poor), claiming for a well-structured organization of rotational programs among centers with different patients throughput and specialization to fulfill this hiatus. In the area of RO, most of the technical skills were perceived as high quality (3D CRT, treatment interruption management, treatment plan evaluation, volumes of interest definition, dose prescription), with the exception of the knowledge in functioning of TPS-calculating algorithms/radiobiology modeling (71.1 % moderate/poor), calling for a more frequent interaction with physics departments; training in IGRT was perceived as excellent/good by 50.7 % of respondents, probably reflecting the incomplete spread of this technology throughout the country. The expertise in special techniques was considered good for IMRT (53.8 %) even if not highly; conversely, partially lacking was perceived the knowledge in stereotactic radiotherapy (56.3 %), total body irradiation (78 %), brachytherapy (78.2 %) and intra-operative radiotherapy (84.8 %): some of these techniques need high specialization, and this is reflected in the uneven distribution of part of these across the country. These data suggest the need for consistent rotations between RO departments routinely performing different specialized radiotherapy techniques. The interest in research was consistent in the majority of respondents (70.6 % excellent/good), but fewer (32 %) felt to have acquired a notable research experience during residency, even if an active involvement in research programs was declared by about 2/3 of respondents. The knowledge in fundamental disciplines (medical physics, radiobiology, radioprotection) was perceived as lacking (moderate/poor 68, 69.5, 72.1 %), pointing out some room for improvement in this area. Managementskills were perceived as high quality (colleagues supervision, workload optimization, use of technology for patients management optimization) as relational skills toward colleagues (availability, interdisciplinary meetings, sharing scientific knowledge, helping colleagues) and patients (to listen to patients, to understand them, to give bad news, to deal with problematic issues, to build a constructive relationship with them). As far as the judgment on the organization of training is concerned, rotational programs are scheduled and accomplished. Areas to be ameliorated, according to respondents’ perception, are regular lectures (lacking in 36 % of cases), training in other imaging specialties (lacking in 68.9 %), training in foreign institution (lacking in 64.5 %), economic support for meeting (lacking in 47 %) and formal research period within rotation (missing in 47 %). Nevertheless, 69.9 % of respondents with finalized training felt that their residency program fulfilled the needs for a successful introduction in the professional world. To give a depiction of the time trend and eventual modifications in the perception of the residency programs during the decade under examination (2001–2011), we compared the answers of specialists and residents with all investigated items findings a statistical difference in terms of high-quality perception (in favor of specialists) for specific issues: head and neck cancer management, treatment plan evaluation (highly significant), diagnosis and staging in oncology, volume of interest definition, IMRT, side effects management, radioprotection (moderately significant). A simple explanation for these findings is that, at the time of the project, up to 65 % of respondents residents were attending their first 3 years of residency, while only 35 % were at their last year; thus, some of the aforementioned items and abilities might not have been dealt with yet in the education path at the time of investigation. Another explanation might be a misperception of knowledge and skills of specialists potentially referring their abilities to the time of questionnaire fulfillment and not to the time of residency program completion.
Conclusion
In conclusion, the STYRO 2011 provided a consistent depiction of perceived quality of training in Italy within a decade. Training quality perception is only a partial tool to evaluate competencies and education. Evaluation of competencies is an ongoing process that might be performed in several manners employing different criteria. However, this outside-in perspective driven by subject-centric perception of quality gives a somehow reliable measure of RO training achievements. Some of items perceived as lacking in the present investigation are specifically addressed in the 2009 upgrade of the residency program. Future surveys and analysis (already planned for forthcoming years) will provide information on the consequences of these modifications. However, hopefully, the present report might be useful for residents, program directors and scientific societies (such as AIRO), to further continue the effort in the improvement of training in RO.
References
Filippi AR, Alongi F, Ciammella P, et al. A strategy for young members within national radiation oncology societies: the Italian experience (AIRO Giovani Group). Rep Pract Oncol Radiother. 2012;17:259–61.
Leer JW, Overgaard J, Heeren G. The European core curriculum on radiotherapy. Radiother Oncol. 1997;43:97–101.
Baumann M, Leer JW, Dahl O, et al. Updated European core curriculum for radiotherapists (radiation oncologists). Recommended curriculum for the specialist training of medical practitioners in radiotherapy (radiation oncology) within Europe. Radiother Oncol. 2004;70:107–13.
Eriksen JG, Beavis AW, Coffey MA, et al. The updated ESTRO core curricula 2011 for clinicians, medical physicists and RTTs in radiotherapy/radiation oncology. Radiother Oncol. 2012;103:103–8.
Semarau R, Hansemann K, Adam M, et al. Quality of training in radiation oncology in Germany. Results of a 2006 survey. Strahlenther Onkol. 2008;184:239–44.
Kantor G, Huguet F, Toledano A, et al. Radiation oncology training in France: demography, analysis of motivations of the young specialists, evaluation of the training. Cancer Radiother. 2005;9:435–43.
Gondi V, Bernard JR Jr, Jabbari S, et al. Results of the 2005–2008 association of residents in radiation oncology survey of chief residents in the United States: clinical training and resident working conditions. Int J Radiat Oncol Biol Phys. 2011;81:1120–7.
Franco P, Catuzzo P, Cante D, et al. TomoDirect: an efficient means to deliver radiation at static angles with tomotherapy. Tumori. 2011;97:498–502.
Cante D, Franco P, Sciacero P, et al. Five-years results of a prospective case series of accelerated hypofractionated whole breast radiation with concomitant boost to the surgical bed after conserving surgery for early breast cancer. Med Oncol. 2013;30:518.
Ricardi U, Racca P, Franco P, et al. Prospective phase II trial of neoadjuvant chemo-radiotherapy with Oxaliplatin and Capecitabine in locally advanced rectal cancer (XELOXART). Med Oncol. 2013;30:581.
CanMEDS2000: extract form the CANMEDS2000 project societal needs working group report. Med Teach. 2000;22:549–54.
Offerta Formativa-Scuole di Specializzazione-Obiettivi della classe della diagnostica per immagini e radioterapia-Ministero Istruzione Università e Ricerca. http://www.miur.it. Accessed 28 April 2013.
De Bari B, Chiesa S, Filippi AR, et al. The INTER-ROMA project—a survey among Italian radiation oncologists on their approach to the treatment of bone metastases. Tumori. 2011;97:177–84.
Alongi F, De Bari B, Franco P, et al. The PROCAINA (PROstate Cancer Indication Attitudes) Project (Part I): a survey among young Italian radiation oncologists on postoperative radiotherapy in prostate cancer. Radiol Med. 2013;118:660–78.
De Bari B, Alongi F, Franco P, et al. The PROCAINA (PROstate Cancer Indication Attitudes) Project (Part II): a survey among young Italian radiation oncologists on radical radiotherapy in prostate cancer. Radiol Med. 2013. doi:10.1007/s11547-013-0925-z.
Ciammella P, De Bari B, Fiorentino A, et al. The ‘BUONGIORNO’ project: Burn Out Syndrome among Young Italian Radiation Oncologists. Cancer Invest. 2013. doi:10.3109/07357907.2013.830735.
Conflict of interest
No conflicts of interest to be declared.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was carried out on behalf of AIRO Giovani (Italian Association of Radiation Oncology-Young Members Working Group)
Appendix: Questionnaire complete form
Appendix: Questionnaire complete form







Rights and permissions
About this article
Cite this article
Franco, P., Ciammella, P., Peruzzo Cornetto, A. et al. The STYRO 2011 project: a survey on perceived quality of training among young Italian radiation oncologists. Med Oncol 30, 729 (2013). https://doi.org/10.1007/s12032-013-0729-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12032-013-0729-y