
Abstract
Background
In aneurysmal subarachnoid hemorrhage (aSAH), one of the main determinants of prognosis is delayed cerebral ischemia (DCI). Transcranial Doppler (TCD) is used to monitor vasospasm and DCI. We aimed to better understand cerebral hemodynamics response to hypertension induction (HI) with norepinephrine (NE) and inotropic therapy with milrinone so that TCD can be a bedside tool in helping to guide DCI therapies. Our primary objective was to determine TCD blood flow velocity (BFV) kinetics during HI and inotropic therapy for DCI treatment. Secondly, we performed an analysis by treatment subgroups and evaluated clinical response to therapies.
Methods
We performed a prospective observational cohort study in a Brazilian high-volume center for aSAH. Patients with aSAH admitted between 2016 and 2018 who received NE or milrinone for DCI treatment were included. TCDs were performed before therapy initiation (t0) and 45 (t1) and 90 min (t2) from the onset of therapy. For each DCI event, we analyzed the highest mean flow velocity (MFV) and the mean MFV and compared their kinetics over time. The National Institutes of Health Stroke Scale was determined at t0, t1, and t2.
Results
Ninety-eight patients with aSAH were admitted during the study period. Twenty-one (21.4%) developed DCI, of whom six had DCI twice, leading to a total of 27 analyzed DCI events (12 treated with HI and 15 with milrinone). Patients treated with NE had their mean arterial pressure raised (85 mm Hg in t0, 112 mm Hg in t2 [p < 0.001]), whereas those treated with milrinone had a significant decrease in mean arterial pressure over treatment (94 mm Hg in t0, 88 mm Hg in t2 [p = 0.004]). Among all treated patients, there was a significant drop from t0 to t2 but not to t1 in the highest MFV and in the highest mean MFV. Among those treated with HI, there were no significant changes from t0 to t1 or t2 (highest MFV in t0 163.2 cm/s, in t1 172.9 cm/s [p = 0.27], and in t2 164 cm/s [p = 0.936]). Conversely, in those treated with milrinone, there was a significant decrease from t0 to t1 and to t2 (highest MFV in t0 197.1 cm/s, in t1 172.8 cm/s [p = 0.012], in t2 159 cm/s [p = 0.002]). Regarding clinical outcomes, we observed a significant improvement in mean National Institutes of Health Stroke Scale scores from 17 to 16 in t1 (p < 0.001) and to 15 in t2 (p = 0.002).
Conclusions
BFV analyzed by TCD in patients with aSAH who developed DCI and were treated with milrinone or NE significantly decreased in a time-dependent way. Milrinone effectively decrease cerebral BFV, whereas NE do not. Clinical improvement was achieved with both treatment strategies.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH) is a condition with elevated morbidity and mortality [1,2,3].
One of the most devastating complications of aSAH is delayed cerebral ischemia (DCI). DCI is defined as a new focal neurological deficit or a decrease in the level of consciousness (reduction of at least 2 points in Glasgow Coma Scale [GCS]) that lasts for at least 1 h and is not explained by other causes. It should also not be apparent immediately after aneurysm occlusion [4, 5]. DCI has a multifactorial pathophysiology, including large vessel spasm, microthrombosis, microcirculation dysfunction, inflammation, and cortical spreading depression being recognized as part of the process [6, 7]. Large vessel vasospasm (VSP) has historically been linked to DCI and is perhaps the best studied and most easily identified component of the above mentioned complex pathophysiology [6, 7].
Transcranial Doppler (TCD) is an imaging tool frequently used for monitoring VSP in patients with aSAH. It measures cerebral blood flow velocities (BFVs) in the skull base arteries and can detect stenoses based on the physical principle that velocity is inversely proportional to the sectional area of the vessel lumen. Thus, an increase in BFV is the main finding in aSAH sonographic VSP [8, 9]. TCD has the advantages of being noninvasive, noncontrast dependent, and widely available. For middle cerebral artery (MCA), it has high specificity and positive predictive values of 99% and 97%, respectively [8, 9]. Systematic reviews have shown that for patients in whom TCD revealed a spasm, they were 17 times more likely to have a spasm shown in digital angiography than for those with no spasm seen in TCD. However, negative predictive value and the likelihood ratio for a negative test are low [10].
Although not definitively diagnostic of DCI, in the appropriate context, such as in the presence of symptoms or in patients under sedation, sonographic VSP can support the diagnosis and help in the decision of starting treatment for DCI [2, 11].
DCI can be reversible if aggressively treated right away; otherwise, it progresses to irreversible brain infarction [4, 5]. Treatment strategies for DCI usually comprise hypertension induction (HI) and inotropic agents, with or without endovascular therapy (intraarterial [IA] drugs and/or balloon angioplasty) [11,12,13,14,15]. Although largely used, these strategies have not yet been tested in robust trials with patient-centered outcomes [16,17,18]. Additionally, little is known about cerebral BFV kinetics and its behavior during DCI treatment. Few studies have demonstrated that therapies aiming at improving DCI led to a decrease in cerebral BFV, thus reflecting improvement in VSP [19,20,21]. None of such studies, however, evaluated treatment strategies recommended by the Neurocritical Care Society or the American Heart Association, such as HI or inotropic/vasodilator therapy [13, 14].
Thus, we conducted this study to determine TCD BFV kinetics during HI and inotropic therapy for DCI treatment in patients with aSAH. We aimed to evaluate the impact of those strategies in cerebral hemodynamics using TCD. Secondly, we aimed to evaluate norepinephrine and milrinone sonographic responses separately and to correlate them with neurological examination changes during treatment and outcomes at discharge.
A better understanding of how cerebral BFV behaves during DCI treatment may help in guiding bedside decisions and estimating future prognosis. Hence, TCD may be used as a real-time tool in the management of DCI, particularly in those patients whom we cannot rely on neurological examination, such as high-grade hemorrhages or those under sedation.
Methods
This was a prospective cohort in a quaternary hospital and a high-volume center for aSAH in Brazil. It was approved by the local institutional review board. All patients with aSAH admitted to our neurological intensive care unit (ICU) between June 2016 and June 2018 were monitored and observed during hospitalization.
Those who developed DCI despite routine measures for DCI prophylaxis during hospital stay and who were chosen to be treated with HI or inotropic/vasodilator therapy were included.
DCI prophylaxis included oral nimodipine use since the time of hospital admission, maintenance of euvolemia, avoidance of hypotension, fever, and dysglycemia. Euvolemia was routinely ascertained by noninvasive measures: fluid balance (inputs and outputs), measurements of central venous pressure, bedside echocardiography, evaluation of inferior vena cava distensibility, and serum lactate levels. Attending physicians were instructed to follow our ICU protocols. Ultimately, however, decisions on how to assure euvolemia were made at their discretion. Our ICU protocol recommends avoiding negative fluid balance, aiming to maintain inputs and outputs balanced to slightly positive (+ 500 mL). Recommended central venous pressure (CVP) goals are between 8 and 12 mm Hg [14].
DCI was defined as a new focal neurological deficit or a decrease of 2 points or more in GCS that lasted for at least 1 h, was not apparent immediately after aneurysmal treatment, and was not explained by other causes. If the neurological deficit could be attributed to sonographic or angiographic spasm of one or more arteries, it was considered a DCI due to symptomatic VSP [4, 5]. Thus, in this article, whenever we mention DCI, we mean DCI caused by symptomatic large vessel spasm.
aSAH was diagnosed with brain computed tomography (CT) scan, magnetic resonance imaging, or lumbar puncture. Brain aneurysm was confirmed by CT angiography, magnetic resonance imaging angiography, or digital subtraction angiography. All patients were admitted to the neurological ICU on their hospital arrival or after aneurysmal treatment (surgical or endovascular).
For all patients admitted with aSAH, we collected the following: demographic characteristics; presence of risk factors for aSAH, such as hypertension, cigarette smoking, illicit drug, and alcohol intake; clinical characteristics of the initial presentation (Hunt and Hess and World Federation of Neurological Surgeons [WFNS] grades on admission); modified Fisher Scale and VASOGRADE from initial CT scan; treatment method (whether clipping or coiling); presence of hydrocephalus and the need of external ventricular drainage; presence of neurological and systemic complications during hospital admission, such as seizures and intracranial hypertension; and length of ICU and hospital stay.
For those patients who were awake and not under sedation, serial neurological examinations were considered the gold standard for DCI diagnosis. For patients with high-grade hemorrhages (WFNS grades 4–5) who were comatose or under sedation besides TCD with VSP, perfusion CT was used for DCI diagnosis. If DCI was diagnosed, patients were treated with HI with norepinephrine, unless the patient was already spontaneously hypertensive (systolic blood pressure [SBP] > 160 mm Hg), or if there was a formal clinical contraindication to HI, such as a recent myocardial infarction or severe heart failure. HI followed a stepwise protocol, beginning with a target SBP of 160 mm Hg. Serial neurological reevaluations were performed in 30-min intervals, and SBP was progressively raised until there was a full resolution of neurological symptoms, a maximum SBP of 220 mm Hg, a mean arterial pressure (MAP) of 130 mm Hg, or the occurrence of any adverse effect. When there was neurological improvement, the blood pressure target was maintained for 24–48 h, and then the drug was slowly withdrawn by decreasing 25% of the infusion every 12–24 h. If the neurological deficit returned at any time point, norepinephrine infusion was returned to the previous dosage at which the patient was asymptomatic (Fig. 1).

Intensive care unit protocol for treatment of delayed cerebral ischemia. BP, blood pressure, DCI, delayed cerebral ischemia, MAP, mean arterial pressure, SBP, systolic blood pressure
If HI failed or was contraindicated, inotropic therapy with milrinone was used. HI failure was defined as lack of clinical improvement despite maximum blood pressure targets for at least 30 min or the occurrence of adverse effects. Blood pressure limits included a maximum SBP of 220 mm Hg or a MAP of 130 mm Hg. When HI failed, inotropic therapy with milrinone was immediately started.
We followed the Neurological Montreal Hospital protocol [22], with an initial bolus of 0.1–0.2 mg/kg of intravenous milrinone, followed by a continuous intravenous infusion of 0.75–1.25 μg/kg/minute. Because of the vasodilator property of milrinone, hypotension occurs often. MAP should be kept > 90 mm Hg, with the infusion of vasoactive drugs if necessary. If there was improvement and lack of recurrence, the infusion was maintained for 48 h, and then decreased by 0.25 μg/kg/minute every 24–48 h. If deterioration occurred, the protocol was restarted and milrinone was weaned at a slower rate (Fig. 1). If there was no improvement with either HI or milrinone infusion, patients received endovascular therapy. DCI treatment modality was a decision of the ICU team, independent of the investigators.
For patients in whom inotropic therapy was indicated because of failure of HI, norepinephrine was weaned off before starting milrinone. Vasoactive drugs were restarted or increased (if already being used previously to DCI treatment), only if hypotension occurred, to restore a MAP of at least 90 mm Hg, as previously mentioned. All patients with DCI were monitored with continuous electrocardiographic recording, an arterial line (zeroed at the heart level), a central venous catheter for measurement of central venous pressure, fluid balance, bedside echocardiography, daily electrolytes, and intracranial pressure monitoring when external ventricular drain was present. Selected and specific cases could have more invasive and advanced hemodynamic monitoring, with pulmonary artery catheters, transpulmonary thermodilution, and pulse contour monitors.
All patients with aSAH have TCD performed in a daily basis in our institution. The investigators were immediately called whenever a patient was diagnosed with DCI. Our protocol consisted of a full TCD examination performed before therapy initiation, with detection of the arteries that fulfilled VSP criteria (Tables 1, 2) for those who were included in the study. This baseline study was considered time 0 (t0) examination. TCDs were repeated twice (with 45-min intervals) by the same experienced neurosonologist during DCI treatment (at 45 [t1] and 90 [t2] minutes from the onset of therapy). Controversies were discussed with a second examiner certified by the Brazilian Academy of Neurology and the European Society of Neurosonology. Both t1 and t2 evaluations were selective studies focusing on the previous vessels with spasm to remain within the time constraints of the study. All TCDs were performed with a DWL, a Doppler Box X machine manufactured in Germany.
MCAs were evaluated by transtemporal windows, and BFVs were recorded every 2 mm from 44 to 64 mm depth. Additionally, using transtemporal windows, anterior cerebral arteries were recorded in two depths from 55 to 80 mm and posterior cerebral arteries from 60 to 70 mm. Through suboccipital window, intracranial vertebral arteries were recorded every 2 mm depth from 60 to 78 mm and the basilar artery from 80 to 120 mm. Through orbital windows, carotid siphons were evaluated from 60 to 80 mm depth and recorded twice. Extracranial internal carotid arteries were evaluated to calculate the Lindegaard index (LI) in those patients who had MCA spasm. Mean flow velocities (MFVs) were recorded according to the above mentioned protocol.
For each DCI event, among all arteries with spasm, the highest MFV obtained in each time (0, 45, and 90 min) was evaluated and compared. For each arterial segment with spasm, the mean MFV (mean of MFV obtained within all insonated depths) at each time was calculated, and the highest mean MFV was analyzed over time. The LI kinetics was also evaluated across all three examinations (in case of spasm in both MCAs, the mean LI was calculated and evaluated). We also analyzed BFV kinetics by vessel with spasm. All arteries with VSP criteria from all patients were evaluated. We compared, for each artery, the highest MFV obtained in each time, as well as the mean from all MFV recorded for each artery and its kinetics evolution over time.
The National Institutes of Health Stroke Scale scores and the GCS were calculated before therapy onset (t0) and at 45 (t1) and 90 min (t2) after therapy onset.
Hemodynamic parameters were recorded at each time point: SBP, diastolic blood pressure, MAP, and heart rate. Body temperature and blood partial pressure of carbon dioxide in those who were mechanically ventilated were also monitored. Renal function was followed from the intervention day until 48 h later to evaluate possible adverse effects. Clinical outcome was assessed by the Modified Rankin Scale (mRS) at hospital discharge for all patients and at 3 months for those who developed DCI.
Statistical analysis
Means and standard deviations or medians and interquartile intervals were used to describe the patients’ characteristics. The Independent Samples t-Test was used to compare means between those with aSAH who developed DCI and those who did not develop DCI. Nonparametric data were compared using the Mann–Whitney U-test. Categorical variables were compared with the χ2 test.
To evaluate longitudinal changes, we used generalized estimating equations using a first-order autoregressive model. The model’s results were presented as estimated means with confidence intervals as well as p values for comparisons between groups and moments.
The analyses were performed with the SPSS program version 24, considering a significance level of 5% (p < 0.05).
Results
A total of 98 patients were admitted to our hospital from June 2016 to June 2018 with a confirmed diagnosis of aSAH. Twenty-one (21.4%) met the stablished criteria for DCI. Six of them had DCI symptoms in two different moments, and then were treated and included in our analysis twice, leading to a total of 27 analyzed DCI events.
Patients with DCI were mainly women, with a mean age of 50.1 ± 13.4 years and a history of arterial hypertension (61.9%) and smoking (42.9%). A total of 23.8% of the patients had a WFNS 4–5 and 81% a modified Fisher scale 3–4. Patients’ characteristics, demographics, clinical and neuroimaging scales are summarized in Table 3. Comparisons between patients who developed or not DCI are shown in Supplementary Table 3.
Sonographic spasm began a median of 9 days post bleeding (quartile 1 [Q1] 5–quartile 3 [Q3] 9), DCI manifested in a median of 12 days (Q1 8–Q3 14), and spasm resolved in a median of 17 days post bleeding (Q1 13–Q3 21). Most patients had spasm in more than one artery when DCI was detected, and decrease in level of consciousness was the most common manifestation of DCI. Data about VSP and DCI detection are summarized in Table 4.
Of the 27 DCI events, 12 (44.4%) were treated with HI, and 15 (55.6%), with inotropic/vasodilator therapy, all according to our above mentioned institution protocol. In nine of the 15 events treated with inotropic therapy, milrinone was used as the initial therapy instead of norepinephrine because the patients were already spontaneously hypertensive (SBP > 140 to 160 mm Hg). The other six patients received HI previously and did not improve or had relapsed symptoms later, and therefore were treated with milrinone. Two patients (7.4%) had additional endovascular therapy (because of a low availability of endovascular intervention in our center, it is not routinely performed, being reserved for selected refractory cases).
The median duration of DCI treatment was 48 h (Q1 24–Q3 120, range 6–288 h). Norepinephrine was used for a median of 36 h (Q1 24–Q3 60, range 6–288); milrinone, for a median of 120 h (Q1 24–Q3 144, range 18–264), with a trend toward a significant difference between groups (p = 0.05).
In 6 of the 27 events (22.2%), therapy had to be interrupted. For patients receiving norepinephrine, the drug was titrated to reach the desirable blood pressure target until a maximum dose of 0.5 μg/kg/minute. There were no severe systemic adverse effects reported (such as myocardial infarction, acute pulmonary edema, or arrhythmias). For patients receiving milrinone, treatment interruptions were due to severe hypotension or tachycardia. SPB, diastolic blood pressure, and MAP were monitored during treatment, and there was a significant increase in those taking norepinephrine and a significant time-dependent decrease in those treated with milrinone. These data are summarized in Supplementary Board 3 and Supplementary Table 4. In 14 of the 15 (93.3%) events treated with milrinone, NE had to be started/ increased with the aim to avoid hypotension, defined as MAP below 90 mm Hg (including those primarily treated with milrinone and those who received milrinone as a second-line therapy).
Cardiac output and cardiac indexes could not be monitored in all patients to help guide treatment due to general availability and costs. We followed the Neurological Montreal Hospital protocol for those who underwent milrinone in which cardiac monitoring was not required [22]. Bedside echocardiography is an available tool in our ICU. In 10 of the 15 events treated with milrinone, a bedside echocardiogram was performed. However, results were not used to tailor therapy.
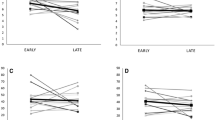
Among all arteries with spasm in all treated patients, there was a significant drop from t0 to t2 but not to t1 in the highest MFV (Table 5). Among those treated with HI, there were no significant changes from t0 to t1 or t2. Conversely, in those treated with milrinone, there was a significant decrease from t0 to t1 and to t2.
We also analyzed the artery with the highest mean MFV of each patient, in each time, and the findings were similar to those described with the highest MFV. These data are summarized in Fig. 2 and Table 5.

Kinetics of TCD BFV analyzed by patients. a Highest MFV. All patients: t1, p = 0.08; t2, p = 0.002. Norepinephrine: t1, p = 0.27; t2, p = 0.93. Milrinone: t1, p = 0.01; t2, p = 0.002. b Highest mean MFV. All patients: t1, p = 0.13; t2, p = 0.001. Norepinephrine: t1, p = 0.37; t2, p = 0.99. Milrinone: t1, p = 0.04; t2, p = 0.002. BFV, blood flow velocity, MFV, mean flow velocity, t1, 45 min from the onset of therapy, t2, 90 min from the onset of therapy, TCD, transcranial Doppler
Regarding kinetics of LI, considering all treated events, there was a significant decrease in mean LI in both t1 and t2 as compared with t0 (Table 5). The same behavior was observed for those treated with milrinone. Among those treated with norepinephrine, there was a significant drop from t0 in mean LI in t1, but not in t2. When comparing both treatment groups, LI were significantly higher in those taking milrinone in t0 and t1, and equivalent in t2 (Table 5).
In an analysis by vessel, all intracranial arteries with spasm from all DCI events were included, which led to a total of 63 vessels evaluated. The mean of the highest MFV, considering all vessels, independent of treatment modality, significantly reduced from t0 to t1 and to t2 (Table 5). For the subgroup of vessels treated with milrinone, the mean of the highest MFV significantly reduced from t0 to t1 and to t2. For those arteries treated with HI, the mean of the highest MFV did not significantly change from t0 to t1 or to t2. MFV in t0 of the arteries treated with milrinone were higher than MFV of those treated with norepinephrine. We also analyzed the mean BFV of all 63 arteries with VSP, considering all recorded depths in TCD examination and their behavior over time. The findings were similar to those described with the highest MFV by vessel. These data are summarized in Fig. 3 and Table 6.

Kinetics of TCD BFV analyzed by arteries. a Highest MFV. All patients: t1, p = 0.01; t2, p < 0.001. Norepinephrine: t1, p = 0.39; t2, p = 0.44. Milrinone: t1, p < 0.001; t2, p < 0.001. b Mean MFV. All patients: t1, p = 0.08; t2, p < 0.001. Norepinephrine: t1, p = 0.3; t2, p = 0.57. Milrinone: t1, p = 0.004; t2, p < 0.001. BFV, blood flow velocity, MFV, mean flow velocity, t1, 45 min from the onset of therapy, t2, 90 min from the onset of therapy, TCD, transcranial doppler
We observed a significant improvement in mean National Institutes of Health Stroke Scale score with the instituted treatment. The same was noticed when analyzing separately those treated with HI and milrinone. A significant increase in mean GCS score was shown in t1, but not in t2. For those treated with milrinone, a significant improvement was seen at t1 and t2, as compared with t0. These data are summarized in Table 7 and Supplementary Board 1.
We also evaluated neuroimaging of the patients with DCI to determine the presence of delayed cerebral infarction. According to the literature, we examined CT or magnetic resonance imaging at approximately 6 weeks after the bleeding or the last one before death (in cases patients died before 6 weeks). Eleven patients had cerebral infarction (52.4%), most of them in MCA territory (45.4%), cortical (72.7%). We observed a frequent correspondence between the vessel with spasm and infarction territory (81.2%). These data are summarized in Supplementary Board 2.
Patients with DCI had a significant longer ICU and hospital stay than those with aSAH and no DCI events (median length of ICU stay 19 days, Q1 15–Q3 25 versus 8 days, Q1 5–Q3 15; median length of hospitalization 23 days, Q1 18–Q3 36 versus 15 days, Q1 9–Q3 21).
Median mRS at hospital discharge was similar between those with and without DCI (3 vs. 2, p = 0.232). Patients with DCI had a median 3 months mRS of 2; with 73.7% of mRS 0–3 and 26.3% 4–6. There were no differences regarding functional outcomes of those treated with HI or milrinone (p = 0.212).
Discussion
The main finding of this study was the significant time-dependent decrease in BFV analyzed by TCD in patients with aSAH who developed DCI and were treated with milrinone or HI. When analyzed separately, we noticed that milrinone was highly effective in decreasing cerebral BFV and improving cerebral vasospasm, which was not noticed with treatment with norepinephrine.
It is important to emphasize that BFV are directly proportional to blood flow and inversely proportional to the cross-sectional area of the vessel insonated. Therefore, any treatment for DCI that acts exclusively by increasing blood flow would also increase BFV. On the other hand, treatments that target the vasospasm itself would promote a decrease in BFV. Finally, treatments that have the potential to affect both blood flow and the vasospasm can have unpredictable effects on BFV.
The rationale of raising BP in DCI is that, in a brain with impaired autoregulation, an increase in MAP leads to activation of collateral blood supply [11] and to an increase in cerebral perfusion pressure, both of which favor an increased cerebral blood flow (CBF) in the ischemic territory. According to this mechanism of action, norepinephrine should promote an increase in BFV. Our finding of nonsignificant changes in BFV after the infusion of norepinephrine suggests that either cardiac output was negatively affected or that norepinephrine affected both CBF and vasospasm.
Norepinephrine (NE) is also a stress hormone that is endogenously related to arousal. In part, it acts via beta and α-1 receptors located within multiple subcortical structures (not only locus coeruleus but also medial septal area and medial preoptic areas). It is, therefore, possible that exogenously administered NE helped improve consciousness level. However, we do not know if and how exogenous NE crosses the blood–brain-barrier. Also, NE is used in multiple conditions in patients who are critically ill (neurological and nonneurological), and improvement in consciousness level is not usually reported (except when hypotension is present). Furthermore, improvement in arousal could be explained by that theory, but improvement in focal deficits would be less probable.
The literature about cerebrovascular effects of norepinephrine is scattered and confusing, with some studies demonstrating a reduction in CBF and others demonstrating an increase in CBF.
Recently, a systematic review in that topic identified 62 animal studies and 26 human studies (few studies focused on the direct effects of norepinephrine on cerebral vasculature). From animal studies and one human study, it seems that norepinephrine stimulates alpha receptors and leads to a degree of constriction on cerebral vessels, similar to its effect on other systemic vessels. This could potentially lead to derangements of cerebral autoregulation and cerebrovascular reactivity. However, the other 25 human studies did not confirm such findings that for sure require future investigation [23].
It seems possible that norepinephrine's effect on CBF can be related to alterations in cerebral blood volume and, consequently, in intracranial pressure. Also, the blood–brain barrier's integrity may influence the norepinephrine's role on cerebral blood vessels [23]. There are no studies in humans showing NE-dosing impact on cerebrovascular reactivity and CBF in patients with subarachnoid hemorrhage. Also, it should be noticed that most human studies measured CBF using MCA flow velocities as a surrogate, which is indeed not an accurate measure of global or regional CBF [23].
Milrinone is a drug with inotropic and vasodilator properties [17]. It is possible that the additional cerebral vasodilator effect of milrinone explains the more robust decrease in cerebral BFV in TCD when compared with norepinephrine in our series. More definitive conclusions on the effect of norepinephrine and milrinone on DCI would require the use of methods that directly evaluate CBF, such as computed tomography with perfusion (CTP) or CT with xenonium [24].
Some studies using CT with xenonium have demonstrated that the role of increased cardiac output (CO) in improving cerebral perfusion seems to be independent of the effect on MAP. However, the physiological mechanism of this connection is not fully understood yet. It is thought that increased pulse pressure and increased pulsatile flow may result in increased CBF by activation of collateral vessels in the setting of vasospasm. Another possibility would be that the increase in CO induced by milrinone could decrease venous pressure benefiting CBF on the venous side [25].
In a pilot study evaluating CBF velocities kinetics via TCD in three patients with vasospasm who were treated with dantrolene (a drug with vasodilator properties), a decrease in BFV with treatment was demonstrated [19]. Another study by the same authors evaluating ten patients and 16 arteries with VSP in aSAH treated with dantrolene also showed a decrease in TCD CBF velocities with treatment [20].
In a retrospective analysis of TCD BFV in 19 patients with aSAH and DCI and a total of 33 MCAs with VSP who underwent IA treatment with nicardipine or milrinone, an increase in highest and mean MFV and systolic peak velocities was seen in days preceding treatment, whereas, after treatment, flow velocities were consistently reduced, demonstrating effectiveness of IA treatment in reversing VSP [21]. Our study, with more DCI events and more vessels treated with intravenous therapies (HI or milrinone), those recommended by the current guidelines of aSAH, was to first to describe the results of the kinetics of cerebral BFV and the reversal of VSP post treatment using a real-time and bedside tool such as TCD. Those findings may lead to a better understanding of how HI and milrinone therapy act on reversing DCI and improving neurological outcomes.
In a comparison of milrinone versus magnesium sulfate for the prevention of sonographic or angiographic VSP in patients with aSAH, the kinetics of CBF measured by TCD in patients who underwent milrinone or magnesium for 21 days post bleeding was described. MFV increased in those treated with milrinone and decreased in those with magnesium. In the same study GCS significantly improved in the magnesium group compared with the milrinone group through days 7, 14, and 21 [26]. However, because the authors were evaluating prevention of vasospasm and not treatment of DCI, a comparison with our data is not feasible.
Besides the above mentioned sonographic improvement reflected by the decrease of BFV, we also noticed clinical improvement during DCI treatment. It is interesting to notice that, even in patients treated with HI and without significant changes in BFV, clinical improvement could be noticed. It is possible that the early clinical improvement observed in such patients may not be related to the resolution of VSP, but to changes in cerebral perfusion pressure. This clinical improvement during DCI treatment with hemodynamic therapy was not previously described.
In our series, more than half of the patients with DCI had a mRS ≤ 3 at hospital discharge, and more than 70%, at 3 months. Interestingly, mRS scores did not differ between patients with and without DCI in our series, raising the possibility that the effective treatment of DCI might have an influence on prognosis. Some studies mention clinical outcomes post DCI treatment. In a series evaluating milrinone for the treatment of DCI, 75% of the patients had an mRS ≤ 2 [22, 27] at 3 months. For patients treated with norepinephrine, a study found a 27% reduction of mRS ≥ 4 [28]. A large Canadian study evaluated mortality in patients with high-grade aSAH (DCI was not registered) and found 48% of mRS ≤ 3 at 3 months post bleeding [29].
The role of HI in patients with subarachnoid hemorrhage and DCI has been challenged by the results of one randomized clinical trial. The trial aiming to include 240 patients ended with only 41 patients included due to low recruitment and lack of effect of HI on cerebral perfusion, leaving the question of the effectiveness of HI for DCI unanswered. In the trial a question about the safety of HI was posed [30]. In our series, we had to interrupt DCI treatment in 22.2% of our patients, a frequency somewhat higher than that described in other series [22, 27, 31, 32]. Interruption happened mainly due to difficulties in reaching the desired target or lack of clinical response. Hypotension and tachycardia were adverse side effects reported with milrinone, whereas none was described with norepinephrine.
The current study has important strengths and limitations.
Strengths include being the first prospective work evaluating the most commonly used drugs (HI with norepinephrine and inotropic therapy with milrinone) in treating DCI and how they act on reversing neurological symptoms and/or sonographic vasospasm. Besides, TCD is a widely available, bedside tool that can be extremely helpful in the real-time management of DCI treatment. In those receiving milrinone, since we realized that clinical and sonographic improvement coincided, TCD may be used as an auxiliary strategy to guide therapy (even in patients without a reliable neurological examination or who are under sedation). On the other hand, for those receiving norepinephrine, a method evaluating cerebral perfusion might be more suitable. Some of the limitations include low power and inclusion of patients from a single center. Besides, due to low availability, more advanced cardiac monitoring through invasive and less invasive methods was not routinely performed on all patients, thus could not be analyzed in the study. We could not evaluate milrinone's direct impact on CO and could not guarantee that our hemodynamic target was achieved.
Our case report forms did not include hemodynamic variables such as central venous pressure (CVP) or CO, and we only have fluid balance from 15 patients. But these data were incomplete and therefore we could not use them for statistical adjustment. As the clinical investigator evaluating neurological deficits at each time point of the study was not blinded to the drug being administered, an assessor bias cannot be excluded. However, as our aim was not to compare therapies or to confirm the effectiveness of the drugs evaluated, this becomes less important. Furthermore, all neurological evaluations were performed by the same clinical investigator and were concordant with the assessment of the clinical team not involved with the study.
Also, we sonographically monitored our participants for a short period of time. Although daily TCD is a part of our institutional protocol for patients with aSAH, we did not collect posterior sonographic data. Therefore, we are only allowed to draw conclusions about the initial kinetics of cerebral BFV post treatment onset. We also did not register the cumulative dosages of milrinone and norepinephrine used, in a way that we cannot correlate dosages with side effects, sonographic or clinical outcomes.
Conclusions
In conclusion, in patients with aSAH and vasospasm, mean and highest MFV analyzed by TCD decrease with treatment for DCI in a time-dependent way. Clinical and sonographic responses to DCI therapies did not necessarily occur in a dependent way. Milrinone seemed effective in reversing sonographic vasospasm, while norepinephrine probably works by a different pathophysiology other that leading to improvement of spasm.
This is the first study evaluating, in a prospective way, the kinetics of cerebral BFV by TCD in patients with aSAH and DCI who were treated with the current recommended intravenous therapies (HI or milrinone) and therefore sheds light to the understanding of how VSP behaves during DCI therapy and raised the question of how we can sustain the clinical improvement observed in the first hours of treatment.
References
Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJ. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 2009;8(7):635–42.
de Oliveira Manoel AL, Goffi A, Marotta TR, Schweizer TA, Abrahamson S, Macdonald RL. The critical care management of poor-grade subarachnoid haemorrhage. Crit Care. 2016;20:21.
Lawton MT, Vates GE. Subarachnoid hemorrhage. N Engl J Med. 2017;377(3):257–66.
Vergouwen MD, Vermeulen M, van Gijn J, Rinkel GJ, Wijdicks EF, Muizelaar JP, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. 2010;41(10):2391–5.
Macdonald RL. History and definition of delayed cerebral ischemia. Acta Neurochir Suppl. 2013;115:3–7.
Cossu G, Messerer M, Oddo M, Daniel RT. To look beyond vasospasm in aneurysmal subarachnoid haemorrhage. Biomed Res Int. 2014;628587:1–1.
Budohoski KP, Guilfoyle M, Helmy A, Huuskonen T, Czosnyka M, Kirollos R, et al. The pathophysiology and treatment of delayed cerebral ischaemia following subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 2014;85(12):1343–53.
Oliveira Manoel AL, Mansur A, Murphy A, Turkel-Parrella D, MacDonald M, MacDonald RL, et al. Aneurysmal subarachnoid haemorrhage from a neuroimaging perspective. Crit Care. 2014;18(6):557.
Sloan MA, Alexandrov AV, Tegeler CH, Spencer MP, Caplan LR, Feldmann E, et al. Assessment: transcranial Doppler ultrasonography: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2004;62(9):1468–81.
Lysakowski C, Walder B, Constanza MC, Tremer MR. Transcranial doppler versus angiography in patients with vasospasm due to a ruptured cerebral aneurysm: a systematic review. Stroke. 2001;32:2292–8.
Francoeur CL, Mayer SA. Management of delayed cerebral ischemia after subarachnoid hemorrhage. Crit Care. 2016;20(1):277.
de Oliveira Manoel AL, Turkel-Parrella D, Duggal A, Murphy A, McCredie V, Marotta TR. Managing aneurysmal subarachnoid hemorrhage: it takes a team. Cleve Clin J Med. 2015;82(3):177–92.
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. American Heart Association Stroke Council; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43(6):1711–37
Diringer MN, Bleck TP, Claude Hemphill J 3rd, Menon D, Shutter L, Vespa P, et al. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocrit Care. 2011;15(2):211–40.
Rouanet C, Silva GS. Aneurysmal subarachnoid hemorrhage: current concepts and updates. Arq Neuropsiquiatr. 2019;77(11):806–14.
Dankbaar JW, Slooter AJ, Rinkel GJ, Schaaf IC. Effect of different components of triple-H therapy on cerebral perfusion in patients with aneurysmal subarachnoid haemorrhage: a systematic review. Crit Care. 2010;14(1):R23.
Lannes M, Zeiler F, Guichon C, Teitelbaum J. The use of milrinone in patients with delayed cerebral ischemia following subarachnoid hemorrhage: A systematic review. Can J Neurol Sci. 2017;44(2):152–60.
Venkatraman A, Khawaja AM, Gupta S, Hardas S, Deveikis JP, Harrigan MR, et al. Intra-arterial vasodilators for vasospasm following aneurysmal subarachnoid hemorrhage: a meta-analysis. J Neurointerv Surg. 2018;10(4):380–7.
Muehlschlegel S, Rordorf G, Bodock M, Sims JR. Dantrolene mediates vasorelaxation in cerebral vasoconstriction: a case series. Neurocrit Care. 2009;10(1):116–21.
Muehlschlegel S, Rordorf G, Sims J. Effects of a single dose of dantrolene in patients with cerebral vasospasm after subarachnoid hemorrhage: a prospective pilot study. Stroke. 2011;42(5):1301–6.
Daftari Besheli L, Tan CO, Bell DL, Hirsch JA, Gupta R. Temporal evolution of vasospasm and clinical outcome after intra-arterial vasodilator therapy in patients with aneurysmal subarachnoid hemorrhage. PLoS ONE. 2017;12(3):e0174676.
Lannes M, Teitelbaum J, del Pilar CM, Cardoso M, Angle M. Milrinone and homeostasis to treat cerebral vasospasm associated with subarachnoid hemorrhage: the Montreal Neurological Hospital Protocol. Neurocrit Care. 2012;16(3):354–62.
Froese L, Dian J, Gomez A, Unger B, Zeiler FA. The cerebrovascular response to neropineprhine: a scoping systematic review of the animal and human literature. Pharmacol Res Perspect. 2020;8(5):e00655. https://doi.org/10.1002/prp2.655.
Gathier CS, Dankbaar JW, van der Jagt M, Verweji BH, Oldenbeuving AW, Rinkel GJ, et al. Effects of induced hypertension on cerebral perfusion in delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: a randomized clinical trial. Stroke. 2015;46(11):3277–81.
Kim DH, Joseph M, Ziadi S, Nates J, Dannenbaium M, et al. Increase in cardiac output can reverse flow deficits from vasospasm independent of blood pressure: a study using xenon computed tomographic measurement of cerebral blood flow. Neurosurgery. 2003;53:1044–52.
Soliman R, Zohry G. Effect of magnesium sulphate and milrinone on cerebral vasospasm after aneurysmal subarachnoid hemorrhage: a randomized study. Rev Bras Anestesiol. 2019;69(1):64–71.
Alamri AS, Alturki A, Badawy M, Letourneau J, Lannes M, Angle M, et al. Safety and outcome of high doses IV milirinone in subarachnoid hemorrhage with refractory vasospasm. Stroke. 2016;47:ATM101–ATM101.
Haegens NM, Gathier CS, Horn J, Coert BA, Verbaan D, van den Bergh WM. Induced hypertension in preventing cerebral infarction in delayed cerebral ischemia after subarachnoid hemorrhage. Stroke. 2018;49(11):2630–6.
de Oliveira Manoel AL, Mansur A, Silva GS, Germans MR, Jaja BNR, Kouzmina E, et al. Functional outcome after poor-grade subarachnoid hemorrhage: a single-center study and systematic literature review. Neurocrit Care. 2016;25(3):338–50.
Gathier CS, van den Bergh WM, van der Jagt M, Verweij BH, Dankbaar JW, Muller MC, et al. Induced hypertension for delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: a randomized clinical trial. Stroke. 2018;49(1):76–83.
Otsubo H, Takemae T, Inoue T, Kobayashi S, Sugita K. Normovolaemic induced hypertension therapy for cerebral vasospasm after subarachnoid haemorrhage. Acta Neurochir. 1990;103:18–26.
Lasry O, Marcoux J. The use of intravenous milrinone to treat cerebral vasospasm following traumatic subarachnoid haemorrhage. Springerplus. 2014;3:633.
Funding
This study received no funding.
Author information
Authors and Affiliations
Contributions
All authors contributed equally to this work.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflicts.
Ethical approval/informed consent
The current study has been approved by the appropriate institutional and national research ethics committee and has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent has been provided by all participants of this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rouanet, C., Chaddad, F., Freitas, F. et al. Kinetics of cerebral blood flow velocities during treatment for delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage. Neurocrit Care 36, 226–239 (2022). https://doi.org/10.1007/s12028-021-01288-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-021-01288-z