
Abstract
Purpose
Fracture risk in hypothyroid patients is debated, and since the effects of hypothyroidism on bone microarchitecture and strength are unclarified, we investigated these characteristics by high-resolution peripheral quantitative computed tomography (HR-pQCT).
Methods
Two approaches were used: a cross-sectional control study, comparing 32 hypothyroid women (mean age; 47 ± 12 years) suffering from Hashimoto’s thyroiditis with 32 sex-, age-, and menopause-matched healthy controls; a prospective study, where 27 of the women were reexamined 1 year after restoration of euthyroidism. HR-pQCT of the distal radius and tibia, and dual-energy X-ray absorptiometry (DXA) of the spine and hip were performed. Bone strength was estimated using a finite element analysis (FEA).
Results
Cross-sectional control study: in the radius, total (mean 14.6 ± 29.3% (SD); p = 0.04) and trabecular bone areas (19.8 ± 37.1%, p = 0.04) were higher, and cortical volumetric bone mineral density (vBMD) lower (−2.2 ± 6.5%, p = 0.032) in hypothyroid patients than in controls. All indices of tibia cortical and trabecular vBMD, microarchitecture, and estimated bone strength were similar between groups, as was hip and spine areal BMD (aBMD). Prospective study: in the radius, mean cortical (−0.9 ± 1.8%, p = 0.02) and trabecular (−1.5 ± 4.6%, p = 0.02) vBMD decreased, and cortical porosity increased (18.9 ± 32.7%, p = 0.02). In the tibia, mean total vBMD (−1.1 ± 1.9%, p = 0.01) and cortical vBMD (−0.8 ± 1.4%, p = 0.01) decreased, while cortical porosity (8.2 ± 11.5%, p = 0.002) and trabecular area (0.2 ± 0.6%, p = 0.047) increased. No changes in FEA were detected. Lumbar spine aBMD decreased (−1.3 ± 3.0%, p = 0.04).
Conclusions
Hypothyroidism was associated with an increased trabecular bone area and a lower mineral density of cortical bone in the radius, as assessed by HR-pQCT. Restoration of euthyroidism mainly increased cortical porosity, while estimated bone strength was unaffected.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In Denmark, the lifetime risk of hypothyroidism is 2.7% [1], and the condition has been linked to somatic as well as psychiatric morbidities [2, 3] and increased mortality [4,5,6]. The thyroid hormones, triiodothyronine (T3) and thyroxine (T4), are essential for maintenance of skeletal bone strength in adults [7, 8]. Earlier studies on the effects of hypothyroidism on the skeleton showed the duration of osteoclastic bone resorption phase extended by twofold, and the osteoblastic bone formation phase and the secondary bone mineralization phase prolonged up to fourfold [9]. Overall, this decrease in bone turnover causes an accumulation of bone, especially in the outer (cortical) bone compartment [10, 11], while areal bone mineral density (aBMD), assessed by dual-energy X-ray absorptiometry (DXA). seems to be preserved in patients with hypothyroidism [12]. Despite the accumulation of bone, some studies [13, 14], but not all [15], have found that patients with overt hypothyroidism carry an increased risk of bone fractures. It is unknown to what extent this is related to a decrease in bone strength—in theory caused by hypermineralized bone or an accumulation of bone micro-fractures with inadequate bone remodeling—or is a consequence of an increased frequency of falls related to hypothyroidism per se or accompanying co-morbidities [13].
Similar to bone mass, microarchitecture, previously studied by bone biopsy, is a determinant of bone strength. With the advent of high-resolution peripheral quantitative computed tomography (HR-pQCT), noninvasive three-dimensional evaluation of bone microarchitecture of the distal radius and tibia, as well as estimates of bone strength, have become available. Emphasizing the importance of bone microarchitecture for skeletal strength, recent studies showed that bone microarchitecture indices obtained by HR-pQCT discriminate patients with fractures from those without fractures, independently of differences in aBMD [16].
Effects of hypothyroidism on bone microarchitecture are not well established, and no longitudinal studies, using HR-pQCT, have examined the effects of treatment for hypothyroidism in Hashimoto’s thyroiditis on bone microarchitecture. Thus, the objectives of this study were to examine bone microarchitecture and estimate bone strength, based on HR-pQCT, in patients with Hashimoto’s thyroiditis in comparison to healthy control subjects, and to evaluate the effects of restoration of euthyroidism.
Materials and methods
Study design and participants
Our study was conducted at the Department of Endocrinology, Odense University Hospital, Denmark, between May 2011 and June 2016. Female patients between 20 and 85 years of age referred to our clinic were invited to participate. Inclusion criteria were newly diagnosed autoimmune thyroiditis, defined by positive thyroid peroxidase or thyroglobulin antibodies and overt (plasma TSH above the reference range of 0.3–4.0 mIU/L and total T4 below the reference range, i.e., 60–130 nmol/L) or mild hypothyroidism (plasma TSH above and total T4 within the reference ranges). Exclusion criteria were pregnancy beyond 12 weeks of gestation during the study period; treatment with oral glucocorticoids; reduced kidney function (i.e., serum creatinine above the reference range of 45–90 μmol/L); known osteoporosis or treatment with anti-osteoporotic agents, or diseases affecting bone metabolism. Use of oral contraceptives containing estradiol was allowed. Ongoing vitamin D supplementation continued during follow-up, while initiation or discontinuation of such supplements during the study period led to exclusion.
The patients received routine clinical care of their thyroid disorder. If not initiated by the referring physician, the patients were routinely started on levothyroxine (LT4) treatment at study enrollment. The LT4 dose was adjusted during the study period aiming at a plasma TSH within the reference range. The first study visit took place a few weeks after the study enrollment. The patients were reexamined (second study visit) after euthyroidism had been achieved for at least 12 months.
Control subjects, matched for age, sex, and menopausal status were used for comparison in the cross-sectional part of the study. The control subjects participated in a separate study examining age- and sex-related changes of bone microarchitecture in an adult population [17]. These subjects were randomly selected from the general population and examined once, during the same time period, using the same equipment, and a similar setup as that used in the patients.
Height, without shoes, was measured to the nearest 0.1 cm. Body weight, wearing indoor clothes, was measured to the nearest 0.1 kg. Body mass index was calculated as body weight divided by the square of the height (kg/m2).
Blood samples
At the first (baseline) and second (follow-up) study visits, fasting blood samples were drawn and stored at −20 °C for later analyses. From these samples, plasma levels of TSH, free T3 (reference range: 4.0–6.8 pmol/L), free T4 (10.0–22.0 pmol/L), and 25-hydroxyvitamin D (25-OHD) (50.0–160.0 nmol/L) were analyzed after study completion, using a two-site chemiluminescent immunometric assay on Cobas® 8000 (Roche Diagnostics, Basel, Switzerland). The coefficients of variation (CV) for TSH was 8.3% and 4.2% at levels of 0.084 and 11.3 mlU/L, respectively; for free T3, 2.1% and 2.0% at levels of 5.75 and 14.0 pmol/L, respectively; for free T4, 7.1% and 4.4% at levels of 17 and 33 pmol/L, respectively; and for 25-OHD, 5.1% and 5.7% at levels of 53 and 106 nmol/L, respectively.
Dual-energy X-ray absorptiometry (DXA)
DXA (Discovery, Hologic, Waltham, MA, USA) was used to measure aBMD of the lumbar spine (L1–L4) and the total hip region. In our unit, the CV for measurements is 1.5% at each of these anatomical sites.
High-resolution peripheral quantitative computed tomography (HR-pQCT)
Bone geometry, volumetric bone mineral density (vBMD), microarchitecture, and estimated bone strength of the nondominant distal radius and tibia were assessed using HR-pQCT (XtremeCT, Scanco Medical, Brüttisellen, Switzerland). The scan procedure and image evaluation have previously been described in detail [18]. In short, the region of interest (ROI) was positioned with a 9.5 and 22.5 mm offset from the radius and tibia endplates, respectively, and extended proximally, providing a total scan length of 9.02 mm. Each 3D segment consists of 110 2D slices with an isotropic 82 µm voxel size. The most distal slice was immediately viewed by the operator for motion artefacts (e.g., blurring or cortical discontinuities), and in such cases up to two repeat acquisitions at each site were performed. A matching procedure, based on changes in bone area throughout the scan region, was applied to ensure identical ROI at baseline and follow-up.
Standard evaluation software provided by the manufacturer was applied with extraction of the following variables, as summarized in Table 1: total, cortical, and trabecular area, trabecular vBMD, trabecular bone volume per tissue volume (BV/TV), trabecular number (Tb.N), trabecular thickness (Tb.Th), and trabecular separation (Tb.Sp). An extended cortical bone analysis was also performed, enabling measurements of cortical thickness (Ct.Th), and cortical porosity (Ct.Po) [19]. The separation of the cortical and trabecular regions was checked on a slice-by-slice basis by two of the authors (M.L.O. or P.N.), and corrections were performed where necessary, as recommended by the manufacturer. The interobserver CV was 0.6% for evaluation of the cortical thickness and 4.2% for the cortical porosity, respectively. Finally, a finite element analysis (FEA) solver, using software provided by the manufacturer (µFE Element Analysis Solver v.1.15; Scanco Medical, Brüttisellen, Switzerland), was employed to estimate bone strength (failure load). In our unit, the CVs are in the range of 0.4–0.8% for densities, 1.0–7.2% for extended cortical measures, 3.5–5.0% for trabecular microarchitecture parameters, and 1.2–1.7% for failure load [20].
Statistical analyses
Data are presented as mean ± standard deviation (SD) if normally distributed, and median [interquartile range] in case of non-normality. Baseline data and between-group differences were quantified using a Wilcoxon rank-sum test, student t-test, or Fisher’s exact test, as appropriate. In the cross-sectional control study, a multiple regression analysis was performed to explore the influence of body weight. The assumptions for the linear regression models were checked using histograms and normal probability plots of residuals. If assumptions were violated, a box–cox regression analysis guided the transformation of the dependent variable.
Two sensitivity analyses were performed using Wilcoxon rank-sum test or student t-test, as appropriate. In order to explore the impact of 25-OHD at the first study visit, the patients were divided into two groups, according to the median 25-OHD level among the patients. Similarly, patients were divided into two groups according to the TSH level being below or above the upper reference limit at the first study visit.
The study was designed to detect a 10% change in BV/TV with 80% power, and with a significance level of 95%. To achieve this, at least 20 patients had to be included. The sample size calculation was based on changes in BV/TV assessed by histomorphometric bone biopsy analysis in hyperthyroid patients before and following treatment [21].
All p values are two-sided and considered statistically significant if <0.05. Statistical analyses were performed using Stata Statistical Software release 15 (StataCorp LLC, Texas, USA).
Results
Clinical and biochemical characteristics
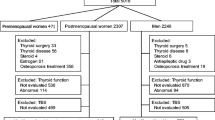
Table 2 shows the characteristics of the patients and the control group. Thirty-two Caucasian women with Hashimoto’s thyroiditis (9 with overt hypothyroidism and 23 with mild hypothyroidism) were included in the study and compared with 32 healthy control subjects. Four patients were withdrawn during the follow-up period due to donation of a kidney (n = 1), full term pregnancy (n = 1), a weight loss of 48% following gastric bypass surgery (n = 1), the diagnosis of an eating disorder (n = 1), while one was lost to follow-up. Thus, twenty-seven of the 32 participants completed the follow-up examinations. The mean period between initiation of treatment and the first study visit was 43 ± 28 days, while the median period between the first and second (follow-up) study visit was 15 months [interquartile range: 14–23 months]. At the first study visit (n = 32), seventeen patients had normalized their plasma TSH following initiation of treatment at the inclusion visit. The median value for TSH was 3.78 mIU/L [2.12–5.78]; for free T3 4.81 pmol/L [4.08–5.09]; for free T4 16.9 pmol/L [15.2–19.2], and for 25-OHD 65.3 [47.6–98.7]. At the final visit (n = 27), the median value for TSH was 2.14 mIU/L [0.58–4.32]; for free T3 4.21 pmol/L [3.78–4.84]; for free T4 18.8 pmol/L [17.1–22.1]; and for 25-OHD 67.9 nmol/L [61.6–96.8].
HR-pQCT
Cross-sectional control study
In the tibia, irrespective of body weight, no significant differences were found in any of the parameters (Table 3). In the radius, patients had a significantly larger total bone area (mean difference 14.6 ± 29.3%; p = 0.01) and trabecular area (19.8 ± 37.1%, p = 0.01), as compared with the control group, while the cortical vBMD was significantly lower (−2.2 ± 6.5%; p = 0.03). Results were similar after adjustment for body weight (Table 3). In neither the radius nor the tibia did the estimated bone strength differ significantly between cases and controls.
Follow-up study
At the second study visit, where euthyroidism had been attained for at least 12 months, the trabecular area in the tibia had increased significantly (0.2 ± 0.6%, p = 0.047; Table 4). Total vBMD and cortical vBMD decreased significantly (−1.1 ± 1.9%, p = 0.01; and −0.8 ± 1.4%, p < 0.01, respectively), while cortical porosity increased (8.2 ± 11.5%, p < 0.01). No significant changes were found in the remaining microarchitecture parameters or in the estimated bone strength of the tibia (Table 4).
In the radius, both trabecular and cortical vBMD decreased significantly (−1.5 ± 4.6%, p = 0.02; and −0.9 ± 1.8%, p = 0.02, respectively), while cortical porosity increased (18.9 ± 32.7%, p = 0.02). A significant decrease in trabecular BV/TV was observed (−1.6 ± 4.6%, p < 0.01). No other significant changes were observed in microarchitecture or estimated bone strength in the radius (Table 4).
DXA
At baseline, aBMD was similar in patients and controls both at the spine and total hip (Table 3). After attainment of euthyroidism, total hip aBMD declined without reaching statistical significance (p = 0.07), while spine aBMD was significantly decreased (−1.3 ± 3.0%, p = 0.04; Table 4).
Sensitivity analyses
When dividing the patients into two groups, according to the upper reference limit of plasma TSH (i.e., 4.0 mIU/L), no differences between the lower-TSH group and the higher-TSH group were found in any of the HR-pQCT parameters, at baseline, at follow-up, or in the changes between the two study visits (data not shown). Likewise, no differences were found between those with high and low 25-OHD, according to the median 25-OHD level (i.e., 65.3 nmol/L).
Discussion
In this first study of bone structure using HR-pQCT in hypothyroid patients with Hashimoto’s thyroiditis, we demonstrated that restoration of euthyroidism following LT4 replacement therapy causes alterations in the bone microarchitecture. The main effects were seen in the cortical compartment of both the radius and the tibia where the cortex became less dense and more porous. The decline in bone mineral density, observed using DXA as well as HR-pQCT, is likely explained by an increase in the bone remodeling rate induced by the LT4 treatment. In thyroid function disorders, it remains unresolved if TSH, independent of the influence by thyroid hormones, has an impact on bone metabolism [7]. It has also been suggested that thyroid autoimmunity per se may be of importance in this context [22]. Ideally, a control group of untreated patients should have been included for comparison in our study, but this was not feasible for practical and ethical reasons. However, it is most likely that the observed changes in bone microarchitecture were caused by restoration of euthyroidism, since our results are in line with previous studies based on histomorphometric and biochemical data, showing that bone turnover is increased by LT4 treatment [11, 23].
Several studies, with conflicting findings, have examined the effect of LT4 treatment on bone. Some found no long-term effects of LT4 therapy [24, 25], while others suggested an unfavorable impact, mainly because of LT4 overtreatment [15, 23, 26, 27]. We observed that the trabecular area in the tibia increased during follow-up. In theory, this may be caused by an increase in bone resorption at the endocortical surface following the normalization of bone remodeling rate. The endocortical surface has been shown to be more metabolically active than the periosteal surface [28]. Accordingly, bone resorption at this site, with inadequate bone formation, will gradually shift the border of trabecular and cortical bone outwards enlarging the trabecular area. However, changes in our study were minute, and we did not observe any significant impact on the cortical area or the cortical thickness in the tibia, and there were no corresponding changes in the radius either. Overall, our results do not suggest that restoration of euthyroidism with LT4 alters bone compartmental geometry or trabecular bone microarchitecture to any significant degree, when assessed following at least one year of euthyroidism. Considering the slow turnover of bone tissue, where a bone remodeling cycle usually is completed after ~6 months [29], the length of follow-up in our study may be too short to obtain a complete evaluation of the impact of hypothyroidism on bone tissue. Two recent studies, both cross-sectional, have investigated bone microarchitecture using HR-pQCT in thyroidectomized patients treated with LT4 [24, 30]. In accordance with our findings, no differences in bone microarchitecture between patients and a control group were found, independently of whether the treatment aimed for normalizing [24], or suppressing plasma TSH [30]. These observations suggest that LT4 treatment beyond one year does not per se cause major alteration in bone microarchitecture.
When comparing bone microarchitecture in hypothyroid patients with control subjects, we found that patients had larger total and trabecular bone area in the radius, while all geometric parameters in the tibia were similar to those observed in the control group. Indices of trabecular bone microarchitecture were similar at both sites. We adjusted our data for body weight because weight is known to affect HR-pQCT parameters [31, 32]. The weight-adjusted analysis aimed at elucidating whether the changes in bone microstructure were due to hypothyroidism per se, or merely related to alterations in body weight. However, an increase in body weight is an inherent feature of hypothyroidism, and it can be questioned whether adjustment for body weight is justified in this context.
In hypothyroidism, histomorphometric studies suggest that the amount of bone resorbed and formed in each bone remodeling cycle is slightly altered, resulting in a slow accrual of primarily cortical bone width, and without any change in trabecular bone volume [10, 11]. Although disease and treatment effects may be skeletal site specific, depending on whether the bone is weight bearing or not, our results do not support that hypothyroidism per se causes accrual of bone, or substantially affects either bone geometry or microarchitecture. An important function of the skeleton is to withstand mechanical strain to prevent fracture; the HR-pQCT entity “failure load” reflects this feature. This variable did not change in the follow-up period, and no difference was demonstrated between the patients and the control group. Thus, hypothyroidism might not have any adverse effects in the context of bone strength. In support of this, several studies found no increased fracture risk in patients with overt or mild hypothyroidism [15, 33, 34], but opposite findings exist [13, 14]. These inconsistent results may reflect that any increased fracture risk, if present, is caused by accidental falls related to the hypothyroidism, overtreatment with LT4 [15], or the co-morbidities shown to be associated with hypothyroidism [2], rather than by a detrimental effect per se on the bone tissue. In theory, the increased mineralization and the slower bone turnover associated with hypothyroidism might increase the fracture risk, in parallel with the situation seen in osteopetrosis (i.e., defects in osteoclast development or function) [35]. In the FEA used in our study, the degree of bone mineralization is standardized. If the bone mineralization were significantly affected in our patients compared with this standard value, the bone strength would potentially be underestimated. However, we believe this problem to be of minor significance as mineralization and bone strength to a large degree are positively correlated.
In addition to the issues discussed above, other limitations to our study should be mentioned. First, the study is sensitive to selection bias since not all hypothyroid patients referred to our clinic were eligible for the study. Thus, our results are confined only to women with hypothyroidism due to autoimmunity and may not be applicable to all hypothyroid patients. Second, most of our patients (23 of 32) had mild rather than overt hypothyroidism. In mild hypothyroidism, a meta-analysis found the risk of fracture to be similar to that in the reference population [34]. Intuitively, one would assume that any impact on bone tissue depends on the severity and duration of the hypothyroid state. However, the rather small size of our study, albeit adequately powered for our main outcome, excluded us from doing such sub-analyses. Thus, our findings might have been more pronounced, if all patients had suffered from overt hypothyroidism. Third, data on biomarkers reflecting bone turnover might have supported the structural findings by HR-pQCT, but such an analysis was beyond the scope of our study. Finally, seventeen patients had normalized their plasma TSH at the first study visit due to the initiation of the LT4 treatment before referral to our clinic. However, bone tissue has a slow metabolic turnover and we find it unlikely that a short period of LT4 therapy should have normalized the bone structure to any significant degree. Nevertheless, to take this potential problem into account, we divided the patients into two groups, according to the upper reference limit of plasma TSH. Using such a stratification, no differences between the lower-TSH group and the higher-TSH group were found in any of the HR-pQCT parameters.
In conclusion, bone microarchitecture in women with hypothyroid Hashimoto’s thyroiditis did not differ considerably from healthy control subjects. Only small differences were detected after LT4 treatment, primarily in the cortical bone compartment, and possibly reflecting a normalization of bone remodeling. The alteration of bone microarchitecture by hypothyroidism per se and the restoration of euthyroidism seem not to affect the estimated bone strength. Future studies, including larger numbers of patients, a broader range of disease phenotypes as well as longer follow-up after treatment initiation, are needed to further qualify the influence of hypothyroidism and its treatment on bone microarchitecture. Such studies might clarify whether HR-pQCT variables are of value in the prediction of bone fractures in patients with hypothyroidism.
References
A. Carle, P. Laurberg, I.B. Pedersen, N. Knudsen, H. Perrild, L. Ovesen, L.B. Rasmussen, T. Jorgensen, Epidemiology of subtypes of hypothyroidism in Denmark. Eur. J. Endocrinol. 154, 21–28 (2006)
M. Thvilum, F. Brandt, D. Almind, K. Christensen, T.H. Brix, L. Hegedus, Type and extent of somatic morbidity before and after the diagnosis of hypothyroidism. a nationwide register study. PLoS ONE 8, e75789 (2013)
M. Thvilum, F. Brandt, D. Almind, K. Christensen, T.H. Brix, L. Hegedus, Increased psychiatric morbidity before and after the diagnosis of hypothyroidism: a nationwide register study. Thyroid 24, 802–808 (2014)
T.H. Brix, C. Ferlov-Schwensen, M. Thvilum, L. Hegedus, Death by unnatural causes, mainly suicide, is increased in patients with Hashimoto’s thyroiditis. A nationwide Danish register study. Endocrine 65, 616–622 (2019)
M. Lillevang-Johansen, B. Abrahamsen, H.L. Jorgensen, T.H. Brix, L. Hegedus, Over- and under-treatment of hypothyroidism is associated with excess mortality: a register-based cohort study. Thyroid 28, 566–574 (2018)
M. Thvilum, F. Brandt, D. Almind, K. Christensen, L. Hegedus, T.H. Brix, Excess mortality in patients diagnosed with hypothyroidism: a nationwide cohort study of singletons and twins. J. Clin. Endocrinol. Metab. 98, 1069–1075 (2013)
G.R. Williams, J.H.D. Bassett, Thyroid diseases and bone health. J. Endocrinol. Investig. 41, 99–109 (2018)
B. Abrahamsen, H.L. Jorgensen, A.S. Laulund, M. Nybo, T.H. Brix, L. Hegedus, Low serum thyrotropin level and duration of suppression as a predictor of major osteoporotic fractures-the OPENTHYRO register cohort. J. Bone Miner. Res. 29, 2040–2050 (2014)
E.F. Eriksen, L. Mosekilde, F. Melsen, Kinetics of trabecular bone resorption and formation in hypothyroidism: evidence for a positive balance per remodeling cycle. Bone 7, 101–108 (1986)
L. Mosekilde, F. Melsen, Morphometric and dynamic studies of bone changes in hypothyroidism. Acta Pathol. Microbiol. Scand. A 86, 56–62 (1978)
J.M. Coindre, J.P. David, L. Riviere, J.F. Goussot, P. Roger, A. de Mascarel, P.J. Meunier, Bone loss in hypothyroidism with hormone replacement. A histomorphometric study. Arch. Intern. Med. 146, 48–53 (1986)
J.H. Bassett, G.R. Williams, Role of thyroid hormones in skeletal development and bone maintenance. Endocr. Rev. 37, 135–187 (2016)
P. Vestergaard, L. Mosekilde, Fractures in patients with hyperthyroidism and hypothyroidism: a nationwide follow-up study in 16,249 patients. Thyroid 12, 411–419 (2002)
P. Vestergaard, J. Weeke, H.C. Hoeck, H.K. Nielsen, J. Rungby, L. Rejnmark, P. Laurberg, L. Mosekilde, Fractures in patients with primary idiopathic hypothyroidism. Thyroid 10, 335–340 (2000)
B. Abrahamsen, H.L. Jorgensen, A.S. Laulund, M. Nybo, D.C. Bauer, T.H. Brix, L. Hegedus, The excess risk of major osteoporotic fractures in hypothyroidism is driven by cumulative hyperthyroid as opposed to hypothyroid time: an observational register-based time-resolved cohort analysis. J. Bone Miner. Res. 30, 898–905 (2015)
E.J. Samelson, K.E. Broe, H. Xu, L. Yang, S. Boyd, E. Biver, P. Szulc, J. Adachi, S. Amin, E. Atkinson, C. Berger, L. Burt, R. Chapurlat, T. Chevalley, S. Ferrari, D. Goltzman, D.A. Hanley, M.T. Hannan, S. Khosla, C.T. Liu, M. Lorentzon, D. Mellstrom, B. Merle, M. Nethander, R. Rizzoli, E. Sornay-Rendu, B. Van Rietbergen, D. Sundh, A.K.O. Wong, C. Ohlsson, S. Demissie, D.P. Kiel, M.L. Bouxsein, Cortical and trabecular bone microarchitecture as an independent predictor of incident fracture risk in older women and men in the Bone Microarchitecture International Consortium (BoMIC): a prospective study. Lancet Diabetes Endocrinol. 7, 34–43 (2019)
V.V. Shanbhogue, K. Brixen, S. Hansen, Age- and sex-related changes in bone microarchitecture and estimated strength: a three-year prospective study using HRpQCT. J. Bone Miner. Res. 31, 1541–1549 (2016)
S. Boutroy, M.L. Bouxsein, F. Munoz, P.D. Delmas, In vivo assessment of trabecular bone microarchitecture by high-resolution peripheral quantitative computed tomography. J. Clin. Endocrinol. Metab. 90, 6508–6515 (2005)
A.J. Burghardt, H.R. Buie, A. Laib, S. Majumdar, S.K. Boyd, Reproducibility of direct quantitative measures of cortical bone microarchitecture of the distal radius and tibia by HR-pQCT. Bone 47, 519–528 (2010)
S. Hansen, E.M. Hauge, J.E. Beck Jensen, K. Brixen, Differing effects of PTH 1-34, PTH 1-84, and zoledronic acid on bone microarchitecture and estimated strength in postmenopausal women with osteoporosis: an 18-month open-labeled observational study using HR-pQCT. J. Bone Miner. Res. 28, 736–745 (2013)
L. Mosekilde, M.S. Christensen, F. Melsen, N.S. Sorensen, Effect of antithyroid treatment on calcium-phosphorus metabolism in hyperthyroidism. I: chemical quantities in serum and urine. Acta Endocrinol. 87, 743–750 (1978)
S.P. Polovina, D. Miljic, S. Zivojinovic, N. Milic, D. Micic, V.P. Brkic, The impact of thyroid autoimmunity (TPOAb) on bone density and fracture risk in postmenopausal women. Hormones 16, 54–61 (2017)
C. Meier, M. Beat, M. Guglielmetti, M. Christ-Crain, J.J. Staub, M. Kraenzlin, Restoration of euthyroidism accelerates bone turnover in patients with subclinical hypothyroidism: a randomized controlled trial. Osteoporos. Int. 15, 209–216 (2004)
E. Moser, T. Sikjaer, L. Mosekilde, L. Rejnmark, Bone Indices in thyroidectomized patients on long-term substitution therapy with levothyroxine assessed by DXA and HR-pQCT. J. Thyroid Res. 2015, 796871 (2015)
J.D. Pedrera-Zamorano, R. Roncero-Martin, J.F. Calderon-Garcia, M. Santos-Vivas, V. Vera, M. Martinez-Alvarez, P. Rey-Sanchez, Treatment of subclinical hypothyroidism does not affect bone mass as determined by dual-energy X-ray absorptiometry, peripheral quantitative computed tomography and quantitative bone ultrasound in Spanish women. Arch. Med. Sci. 11, 1008–1014 (2015)
R.P. Babu, A. Christy, A. Hegde, P. Manjrekar, V. D’Souza, Do premenopausal hypothyroid women on levothyroxine therapy need bone status monitoring? Clin. Med. Insights Womens Health 8, 1–6 (2015)
M. Karimifar, F. Esmaili, A. Salari, A. Kachuei, Z. Faragzadegan, M. Karimifar, Effects of Levothyroxine and thyroid stimulating hormone on bone loss in patients with primary hypothyroidism. J. Res. Pharm. Pract. 3, 83–87 (2014)
R. Balena, M.S. Shih, A.M. Parfitt, Bone resorption and formation on the periosteal envelope of the ilium: a histomorphometric study in healthy women. J. Bone Miner. Res. 7, 1475–1482 (1992)
E.F. Eriksen, Cellular mechanisms of bone remodeling. Rev. Endocr. Metab. Disord. 11, 219–227 (2010)
G. Mendonca Monteiro de Barros, M. Madeira, L. Vieira Neto, F. de Paula Paranhos Neto, L.M. Carvalho Mendonca, I. Correa Barbosa Lima, R. Corbo, M.L. Fleiuss Farias, Bone mineral density and bone microarchitecture after long-term suppressive levothyroxine treatment of differentiated thyroid carcinoma in young adult patients. J. Bone Miner. Metab. 34, 417–421 (2016)
J. Frolich, S. Hansen, L.A. Winkler, A.K. Andresen, A.P. Hermann, R.K. Stoving, The role of body weight on bone in anorexia nervosa: a HR-pQCT study. Calcif. Tissue Int. 101, 24–33 (2017)
K.D. Frederiksen, S. Hanson, S. Hansen, K. Brixen, J. Gram, N.R. Jorgensen, R.K. Stoving, Bone structural changes and estimated strength after gastric bypass surgery evaluated by HR-pQCT. Calcif. Tissue Int. 98, 253–262 (2016)
L.J. Melton 3rd, E. Ardila, C.S. Crowson, W.M. O’Fallon, S. Khosla, Fractures following thyroidectomy in women: a population-based cohort study. Bone 27, 695–700 (2000)
M.R. Blum, D.C. Bauer, T.H. Collet, H.A. Fink, A.R. Cappola, B.R. da Costa, C.D. Wirth, R.P. Peeters, B.O. Asvold, W.P. den Elzen, R.N. Luben, M. Imaizumi, A.P. Bremner, A. Gogakos, R. Eastell, P.M. Kearney, E.S. Strotmeyer, E.R. Wallace, M. Hoff, G. Ceresini, F. Rivadeneira, A.G. Uitterlinden, D.J. Stott, R.G. Westendorp, K.T. Khaw, A. Langhammer, L. Ferrucci, J. Gussekloo, G.R. Williams, J.P. Walsh, P. Juni, D. Aujesky, N. Rodondi, C. Thyroid Studies, Subclinical thyroid dysfunction and fracture risk: a meta-analysis. JAMA 313, 2055–2065 (2015)
Z. Stark, R. Savarirayan, Osteopetrosis. Orphanet J. Rare Dis. 4, 5 (2009)
Acknowledgements
We wish to thank technicians at the Osteoporosis clinic for performing bone scans and in particular Steffanie Christensen for her help in study coordination.
Funding
This study received funding from “The Music Publishers Agnes and Knut Mørk’s Foundation”, from the “Danish Thyroid Federation”, and from research grants at Odense University Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Regional Research Ethics Committee of Southern Denmark (S-2011–0018) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Obling, M.L., Nicolaisen, P., Brix, T.H. et al. Restoration of euthyroidism in women with Hashimoto’s thyroiditis changes bone microarchitecture but not estimated bone strength. Endocrine 71, 397–406 (2021). https://doi.org/10.1007/s12020-020-02398-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12020-020-02398-y