
Abstract
Hispanics/Latinos have higher rates of type 2 diabetes (T2D), and the origins of these disparities are poorly understood. Environmental endocrine-disrupting chemicals (EDCs), including some metals and metalloids, are implicated as diabetes risk factors. Data indicate that Hispanics/Latinos may be disproportionately exposed to EDCs, yet they remain understudied with respect to environmental exposures and diabetes. The objective of this study is to determine how metal exposures contribute to T2D progression by evaluating the associations between 8 urinary metals and measures of glycemic status in 414 normoglycemic or prediabetic adults living in Starr County, Texas, a Hispanic/Latino community with high rates of diabetes and diabetes-associated mortality. We used multivariable linear regression to quantify the differences in homeostatic model assessments for pancreatic β-cell function, insulin resistance, and insulin sensitivity (HOMA-β, HOMA-IR, HOMA-S, respectively), plasma insulin, plasma glucose, and hemoglobin A1c (HbA1c) associated with increasing urinary metal concentrations. Quantile-based g-computation was utilized to assess mixture effects. After multivariable adjustment, urinary arsenic and molybdenum were associated with lower HOMA-β, HOMA-IR, and plasma insulin levels and higher HOMA-S. Additionally, higher urinary copper levels were associated with a reduced HOMA-β. Lastly, a higher concentration of the 8 metal mixtures was associated with lower HOMA-β, HOMA-IR, and plasma insulin levels as well as higher HOMA-S. Our data indicate that arsenic, molybdenum, copper, and this metal mixture are associated with alterations in measures of glucose homeostasis among non-diabetics in Starr County. This study is one of the first to comprehensively evaluate associations of urinary metals with glycemic measures in a high-risk Mexican American population.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus exerts a significant individual health burden while imposing a critical threat to public health. It is currently estimated that 34.2 million people in the USA have diabetes, with an additional 88 million adults with pre-diabetes and at high risk of developing diabetes [1]. This disease’s societal toll in the USA is significant, with diabetes-associated health costs estimated to be $327 billion annually [2]. Critically, the burden of diabetes disproportionately impacts communities of color. In the USA, Hispanics/Latinos have the highest lifetime risk of developing diabetes, with 80% higher rates of the disease than non-Hispanic whites [3]. Furthermore, Hispanics/Latinos disproportionately suffer from diabetes-associated complications [3]. Starr County, Texas, a primarily Hispanic/Latino community along the Rio Grande River, has some of the highest rates of diabetes in the USA [4]. The reasons behind these disparities are poorly understood; however, emerging evidence linking environmental toxicants to diabetes raises the potential that disproportionate exposure to these chemicals may contribute to disease disparities [5,6,7]. Among diabetogenic toxicants, metals and metalloids are implicated as potential risk factors; however, their specific associations with diabetes-related traits remain incompletely characterized [8].
Multiple metals and metalloids are required for normal physiological function. Among these, zinc, copper, and selenium are essential cofactors for enzymes and critical structural elements of proteins [9]. Of particular note is the role of zinc in the processing and packaging of insulin, a hormone essential for maintaining normal levels of blood sugar [10]. In contrast, elements such as arsenic and cadmium have no known role in human physiology and can disrupt normal cellular function and increase disease risk. Among these toxic metals and metalloids, some can be classified as endocrine-disrupting chemicals (EDC), exogenous chemicals, or mixtures of chemicals that interfere with hormone action [11]. Several EDCs have been shown to alter insulin secretion or action, disrupt whole-body glucose homeostasis, and are associated with increased diabetes risk [6, 7, 12].
Previous population-based studies suggest associations among various urinary metals and diabetes morbidity. Specifically, arsenic, zinc, selenium, vanadium, manganese, copper, lead, and cadmium have been linked to increased diabetes prevalence in highly exposed populations [8, 13,14,15]. In addition, epidemiologic data have also shown relationships among cobalt, nickel, copper, molybdenum, cadmium, and lead, with altered fasting blood glucose and other diabetes markers [16, 17]. Studies have also found that even essential nutrients can be diabetogenic at high doses, including vanadium, selenium, and molybdenum [18, 19]. Despite this, there are gaps in knowledge with regard to the specific effects of metal/metalloid exposures on diabetes development. Of these prior epidemiologic studies, most were conducted in populations with known elevated exposures and only evaluated the effect of single metals independently. Additionally, the impact of metal/metalloid exposures and their mixtures has not been completely characterized in diverse ethnic groups, including high-risk Mexican Americans, despite their markedly elevated disease rates.
To address current gaps in knowledge, this study aimed to evaluate the relationships among a comprehensive panel of urinary metal concentrations, individually and as a mixture, with diabetes-related traits among normoglycemic/prediabetic Hispanics/Latinos living in Starr County, Texas, USA. Critically, Starr County residents have a 70% lifetime risk of developing diabetes and one of the highest diabetes-associated mortality rates in the country [4, 20, 21]. This lifetime risk is 20% higher than the general US population of Hispanics/Latinos, and we hypothesize that environmental factors may play a role in this disparity [22].
Methods
Study Population and Design
The population for this analysis included Mexican American individuals from Starr County, Texas, who had participated in a previous study of novel diabetes risk factors [20], and individuals participating in an ongoing study of the gut microbiome and progression of dysglycemia [23]. Briefly, a systematic survey, largely representative of the age and sex distribution of the Starr County population, was conducted in 3,085 households within 309 blocks in Starr County from 2002 to 2006 to determine the frequency of diabetes. Predominantly from those who answered the survey, 1200 individuals (selected to include approximately half with diabetes) returned for a follow-up examination of novel diabetes risk factors in 2010–2014 [20]. Of these participants, 412 individuals were randomly selected for urinary metal analyses. The sample size was then supplemented with an additional 157 individuals (identified from the original survey) without known diabetes participating in an ongoing study of the gut microbiome on the progression of dysglycemia [21]. In total, 569 individuals were selected for urinary metal analyses, of which 414 participants without diabetes and without missing data on exposures, outcomes, and covariates were included in the present study.
Assessment of Outcomes
One 10-mL EDTA vacutainer of whole blood was collected at fasting in order to measure hemoglobin A1c (HbA1c) (Siemens DCA Vantage Analyzer point-of-care device, Malvern, PA), fasting plasma glucose (FPG), and fasting plasma insulin (Roche Cobas Analyzer, Chicago, IL) concentrations at enrollment. FPG was measured using a YSI 2300 STAT Plus Glucose and Lactate analyzer (YSI Life Sciences, Yellow Springs, Ohio). Steady-state insulin-glucose relationships were assessed using the homeostatic model assessments (HOMA) of β-cell function (HOMA-B), insulin sensitivity (HOMA-S), and insulin resistance (HOMA-IR). HOMA-B was calculated using \(\frac{{I}_{0}\left[\frac{pmol}{L}\right]*3.33}{{G}_{0}\left[\frac{mmol}{L}\right]-3.5}\); HOMA-S was calculated using \(\frac{22.5*18}{{G}_{0}\left[\frac{mg}{dL}\right]*{I}_{0}\left[\frac{\mu g}{mL}\right]}\); and HOMA-IR was calculating using \(\frac{{G}_{0}\left[\frac{nmol}{L}\right]*{I}_{0}[\frac{\mu U}{mL}]}{22.5}\) [24], where I0 represents fasting insulin and G0 represents fasting glucose. In the present analyses, we evaluated diabetes status, HbA1c, FPG, 2-h blood glucose, HOMA-B, HOMA-S, HOMA-IR, and fasting plasma insulin with urinary metal levels as described below.
Assessment of Exposure
Urinary evaluation of metal concentrations is a well-accepted method to evaluate the burden of metals in individuals. Specifically, urinary evaluation represents exposure from multiple sources and assesses chemicals with short half-lives. Although each metal has different excretory pathways, for example manganese in bile, urinary evaluation is still well accepted to determine exposures in individuals [25,26,27,28,29,30,31]. Spot urine samples were collected from each participant. Following collection, samples were immediately placed on ice, centrifuged within 30 min, aliquoted, and placed in a − 20 °C freezer. At the end of each day, samples were stored at − 70 °C until shipment to Dartmouth College where analyses were performed. The urine samples were analyzed for 19 elements—beryllium (Be), aluminum (Al), vanadium (V), chromium (Cr), manganese (Mn), iron (Fe), cobalt (Co), nickel (Ni), copper (Cu), zinc (Zn), arsenic (As), selenium (Se), molybdenum (Mo), cadmium (Cd), tin (Sn), antimony (Sb), mercury (Hg), lead (Pb), and uranium (U)—using the trace element analysis core at Dartmouth College. Briefly, samples were diluted tenfold in 1% HNO3 and analyzed on an 8900 ICP-QQQ mass spectrometer (Agilent, Santa Clara, CA) utilizing helium and oxygen modes (for Be, Cd, on-mass and V, As, Se, mass-shifted). The ICP-MS was calibrated using NIST-traceable multi-element standards (Inorganic Ventures, Christiansburg, VA) with seven calibration standard concentrations spanning the expected concentration range. Quality control included initial and continuing calibration checks, laboratory check solutions (past proficiency samples from the Center for Toxicology, Quebec, Canada), and reference materials (normal level urine, UTAK, Valencia, CA). We assigned calibration values from the instrument for concentrations below the limit of detection (LOD). A summary of quality control results and the method detection limits, calculated as 3 sigma of repeated blank concentrations run across the sample batches, is shown in Supplementary Table 1. The fraction of samples below the LOD for each metal were as follows: Be (99.04%), Al (87.48%), V (47.9%), Cr (94.50%), Mn (36.86%), Fe (47.18%), Co (2.75%), Ni (75.24%), Cu (0%), Zn (0.28%), As (0%), Se (0%), Mo (0%), Cd (0.69%), Sn (67.68%), Sb (50.21%), Hg (84.73%), U (67.54%), and Pb (46.49%). Only elements with < 50% of samples below the LOD were retained for analysis. Urinary creatinine was quantified from spot urine samples using DetectX Urinary Creatinine Kit (Arbor Assays, Ann Arbor, Michigan). Urinary metal concentrations were standardized by creatinine concentration to account for differences in participants’ hydration status.
Assessment of Covariates
Self-reported participant characteristics, including age (years), sex (male, female), years of education, employment status (full time, part time, unemployed, retired, or disabled), smoking status (current, former, never), pack-years of smoking, height (m), weight (kg), diabetes medication usage (no medication; insulin only; oral hypoglycemic agent only; other injectable hypoglycemic agent only; insulin and oral agent; insulin and other injectable; oral agent and other injectable; insulin, oral agent, and other injectable), and alcohol consumption (yes, no), were available from the baseline questionnaire administered to subjects. Participant’s height in meters and weight in kilograms were used to calculate body mass index (kg/m2).
Statistical Analyses
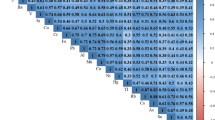
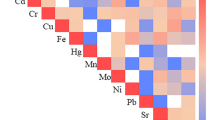
Demographic characteristics were summarized among the 414 participants overall. The median and interquartile range (IQR) for urinary metal concentration are presented overall. Correlations among the urinary metal concentrations were assessed using Spearman’s rank correlation coefficients.
All multivariable models were adjusted for a priori confounders, including urinary creatinine, sex (male, female), age (years), smoking status (current, former, never), pack-years of smoking, BMI (kg/m2), and alcohol consumption (yes, no) [32]. To evaluate non-linear associations, we constructed quartiles of exposure based on each metal’s distribution in the overall study sample. The first quartile, representing participants with the lowest exposure levels, was used as the reference group. The p value for trend was obtained by modeling the quartiles of exposure as an ordinal variable. For continuous diabetes traits, natural log-transformation was used due to skewed distributions. Multivariable linear regression models were utilized to estimate percent changes in HOMA measures (i.e., HOMA-B, HOMA-S, and HOMA-IR), plasma insulin, and FPG as (e(ln2 × β) − 1) × 100% with respect to quartiles of metal concentrations. We restricted the analyses of these continuous measures to participants without diabetes. Multicollinearity between metals was not detected based on the variance inflation factor. A sensitivity analysis was conducted for analyses of mercury and arsenic to account for fish consumption by additionally including urinary arsenobetaine concentration (a proxy of seafood intake) as a covariate in the regression model due to their exposure source being fish and other marine organisms, which may themselves confer metabolic protection [33].
A quantile-based g-computation approach was implemented to assess the effect of metal mixtures on diabetes traits [34]. Quantile-based g-computation is a novel mixture method used to evaluate environmental mixtures and identify the mixture components driving phenotypic outcomes. In the current analyses, each metal was first categorized into quartiles, and then empirical weights were evaluated for each metal through a generalized linear regression model (binomial distribution for diabetes status and Gaussian distribution for log-transformed diabetes traits). Negative and positive weights were generated since the metal mixture included both essential trace and toxic metals. Weights were interpreted as the proportion of the negative or positive partial effect due to a specific metal. The overall effect of the metal mixture (ψ) with each outcome was estimated based on a marginal structural model via g-computation algorithms with a bootstrap of 1,000 iterations. The estimator, ψ, was calculated by summing the regression coefficients of the 8 included metals and interpreted as the OR of diabetes/pre-diabetes (or the change in log-transformed diabetes traits) corresponding to a simultaneous increase in all metals by one quartile.
SAS software version 9.4 (SAS Institute Inc., Cary, NC) was utilized to perform all analyses with the exception of the g-computation analyses, which were implemented using the qgcomp R package [34].
Results
Descriptive Statistics
Table 1 shows the characteristics of the 414 participants from Starr County, Texas. Most of the participants were women (76%), never smokers (71%), and not alcohol consumers (67%). Supplemental Table 2 summarizes the distribution of 8 urinary metal concentrations overall. Urinary metals showed low to moderate correlations, with Spearman’s rank correlation coefficients ranging from 0.09 to 0.70 (Supplemental Table 3).
Steady-State of Insulin-Glucose Dynamics
Table 2 summarizes the associations between urinary metal concentrations and HOMA assessments of insulin resistance and sensitivity as well as β-cell function among individuals without diabetes. First, a higher concentration of urinary total arsenic was associated with reduced HOMA-β (p for trend = 0.03) and HOMA-IR (p for trend = 0.02) and increased HOMA-S (p for trend = 0.02). A dose-dependent association was observed for increased urinary molybdenum with reduced HOMA-β (p for trend = 0.09), reduced HOMA-IR (p for trend = 0.048), and increased HOMA-S (p for trend = 0.049). Individuals with higher urinary copper had reduced HOMA-β compared to those with lower copper (p for trend = 0.046). Lastly, cadmium showed borderline statistically significant effects for reduced HOMA-β (p for trend = 0.08).
Plasma Insulin and Fasting Plasma Glucose
Because HOMA estimates may be influenced by FPG or fasting insulin levels, we examined associations with each component of the HOMA calculations separately. The associations of urinary metal concentrations with plasma insulin are summarized in Supplemental Table 4. Findings of this analysis mirror what we found for HOMA measures. Specifically, an inverse association with plasma insulin was observed for arsenic and molybdenum. Supplemental Table 5 summarizes the effect of urinary metal exposure and FPG among patients without diabetes. In these analyses, metals/metalloids appeared to exert minor effects on glucose. These data collectively suggest that associations between urinary metal levels and steady-state estimates of insulin-glucose dynamics using HOMA measurements are principally driven by alterations in insulin levels.
Metal Mixture
Utilizing quantile-based g-computation, exposure to the 8 metal mixtures was significantly associated with alterations in HOMA-β, HOMA-IR, HOMA-S, and plasma insulin when increasing all metals by one quartile (Table 3). A higher concentration of the total metal mixture was associated with reduced HOMA-β (p = 0.03), plasma insulin (p = 0.03), and HOMA-IR (p = 0.03) and increased HOMA-S (p = 0.03). Analysis of each metal’s proportional positive or negative contributions to the joint effect supported the results found in the multivariable linear regression (Supplemental Figs. 1–5).
Discussion
In this study, we investigated the associations between creatinine-standardized urinary concentrations of 8 metals/metalloids with diabetes-related traits in a cohort of 414 normoglycemic/prediabetic Mexican Americans living in Starr County, Texas, USA. We found urinary arsenic and molybdenum to be associated with reduced β-cell function, insulin resistance, and plasma insulin along with increased insulin sensitivity. Additionally, copper was associated with reduced β-cell function. Furthermore, increased urinary cadmium showed a non-significant trend toward reduced HOMA-β. Lastly, the ultimate 8 metal mixture was associated with alterations in measures of HOMA, and the weighted directionality of the individual metals within the mixture matched the findings of the individual metal regressions. To the best of our knowledge, this is one of the first studies to evaluate multiple metals individually and as a mixture with continuous diabetes measures in a homogenous, high-risk Hispanic/Latino population.
Arsenic is a well-studied, toxic metalloid found in many human water and food sources around the globe [35]. Water supplies in the USA have low to moderate levels of arsenic relative to the World Health Organization (WHO) standard of < 10 µg/L [36]. Despite this, Starr County, Texas, has been noted to have groundwater arsenic levels above the WHO standard [37]. Fish and rice consumption are other potential sources for arsenic exposure and studies have shown that minority populations, including Hispanics/Latinos, consume higher amounts of both fish and rice that could lead to disproportionate exposures to arsenic [38]. There is robust research on arsenic’s effect on diabetes risk, but few studies are conducted in low exposure, minority populations. Additionally, minimal studies focus on the pathophysiology of diabetes to discern the mechanisms by which arsenic impacts diabetes risk. Many studies conducted in high arsenic exposure regions have revealed increased prevalence and incidence of type 2 diabetes [39, 40], with multiple systematic reviews and meta-analyses corroborating a link between arsenic exposure and increased type 2 diabetes risk. A meta-analysis by Sung et al. evaluated 38 studies and showed a significant association with arsenic exposure and diabetes risk [41]. Furthermore, Navas-Acien et al. reviewed 19 epidemiological studies in both high and low arsenic exposure groups and found consistent results for an increased risk of diabetes in highly exposed regions, but further studies being needed for low exposure groups [42]. These population-based studies are supported by both in vivo and in vitro studies that have shown that arsenic disrupts insulin synthesis and secretion due to β-cell toxicity [12, 43,44,45,46], which also support our findings indicating a significant reduction in β-cell function and fasting insulin among individuals in Starr County with the highest levels of urinary arsenic.
Molybdenum is an essential trace element that is a cofactor for several enzymes required for normal human physiology. Although it is necessary for human life, there is evidence that high concentrations are toxic, and acute toxic doses result in immediate clinical symptoms, including diarrhea, anemia, gout, and psychosis [47]. Individuals in Starr County could be exposed to molybdenum through a variety of sources. The most common source of molybdenum is food derived from plants and dairy products. Drinking water exposure is common in areas with industrial waste containing molybdenum, especially from mining, which is prominent in Southern Texas and along the Rio Grande River [28, 48]. Lastly, there is evidence that Hispanics/Latinos living in the USA are more likely to work in high-risk occupations for environmental chemical exposures, including solvents, metals, and pesticides [49].
The observed association between higher urinary molybdenum levels and alterations in HOMA measures (including reduced HOMA-β, HOMA-IR, and fasting insulin and increased HOMA-S) is consistent with some previous epidemiological studies. Specifically, an analysis of the Study of Women’s Health Across the Nation (SWAN) cohort found a significant inverse association between urinary molybdenum and HOMA-IR, but it did not find any association with HOMA-β [50]. In other cohort studies, urinary molybdenum was associated with increased diabetes prevalence, with molybdenum levels higher in those with diabetes compared to individuals with normoglycemia [8]. In contrast, other studies have found positive associations between molybdenum and increased HOMA-IR in participants without diabetes in both US and Chinese populations [16, 51]. These studies were not performed in Hispanic/Latino populations.
In addition to this epidemiological literature, there are cell-based, animal, and human data that support mechanistic links between molybdenum and altered glucose-insulin homeostasis. Molybdenum has been shown to reduce insulin secretion in pancreatic β-cells while promoting β-cell apoptosis in both RIN-m5f cells and isolated murine islets through oxidative stress and other mechanisms [52]. This linkage between molybdenum and oxidative stress is supported by data from a cohort study that found a significant association between molybdenum levels and biomarkers of oxidative stress in a general population in Spain [53]. Other studies have found that β-cells have a limited capacity to handle oxidative stress, which may contribute to diabetes pathogenesis when exposed to chemicals that increase free radicals; this association has been further corroborated by a study of oxidative damage due to metals and type 2 diabetes in Chinese adults [51, 54]. Lastly, molybdenum exposure has been linked to other endocrine-disrupting health outcomes with similar mechanisms of toxicity, including infertility, hypertension, and liver dysfunction [55,56,57].
In addition to arsenic and molybdenum, there is supportive evidence for an impact of copper on pancreatic β-cell function and overall diabetes risk. The most common source of copper exposure in the USA is through drinking water as it leaches into water supplies through copper pipes [58]. Both individual studies and meta-analyses have found positive associations for serum copper with diabetes prevalence and HbA1c [59, 60]. Other studies have shown that increased copper exposure and alterations in copper metabolism are associated with oxidative stress and increased risk for diabetes mellitus [61]. Furthermore, copper chelation has been proposed as an alternative diabetes treatment [62, 63]. Despite these findings, there is still limited evidence on the pathophysiological impact of copper overload on diabetes, and further studies are clearly needed to explore these relationships further.
Although our assessments of cadmium’s links to disrupted glucose-insulin homeostasis did not reach statistical significance, there is evidence that cadmium is associated with metabolic dysfunction. Cadmium has been implicated in diabetes pathogenesis with evidence of cadmium-induced disruptions in adipocyte responses to insulin and pancreatic islet function [64, 65]. Cadmium exposure is widespread through multiple routes, including air pollution as well as agricultural, food, and water contamination [66]. The heavy metal is also found in cigarettes, alloys, pigments, plastics, and batteries. The impact of cadmium exposure on diabetes risk needs to be evaluated further, particularly in high-risk minority populations, as evidence of an effect within general populations is somewhat conflicting [67, 68].
People are simultaneously exposed to multiple metals rather than as isolated elements. In this study, we found an association between the simultaneous exposure to 8 metals as a mixture and alterations of steady-state measures of glycemic status. Additionally, the proportional positive or negative contributions of each metal of the joint effect according to quantile-based g-computation support the findings from the individual regression models. Few studies have investigated the role of metal mixtures on diabetes or diabetes-related traits. A study of 1262 US women in the SWAN cohort utilized adaptive elastic-net models as well as an environmental risk score and found associations of metal mixtures with decreased HOMA-β (higher arsenic and zinc, but lower cobalt) and elevated HOMA-IR (higher copper, lead, and zinc, but lower molybdenum) [50]. Another analysis of the same data observed an association between exposure to 20 metals as a mixture and increased risk of diabetes based on k-mean clustering [69]. As these statistical techniques are novel, future studies are required to corroborate results, but these innovative approaches will illuminate real-world exposure patterns and provide vital information about the physiological consequences of interactions among EDCs.
Strengths and Limitations
This study comprehensively investigated the associations of 8 urinary metals and their mixture with five diabetes-related traits in a US Hispanic/Latino population. In addition, we utilized a novel statistical approach to evaluate the potential combined effects of metals as a mixture. Finally, to our knowledge, our study serves as the first to evaluate these associations in a Mexican American population. Despite these strengths, our study has limitations. The study’s cross-sectional nature renders us unable to conclude the temporality of the associations, and the urinary metal levels were measured using a single spot urine sample. Future research that examines diabetes status longitudinally and is able to characterize long-term exposure will allow for a more robust understanding of any causal association between metals/metalloids and diabetic trait trajectories. Furthermore, alternative novel methods for assessing essential mineral status using erythrocytes rather than whole blood may augment assessments of metal/metalloid status [70]. Additionally, as this observational study examined the impacts of metal exposures in non-endemic regions, the exposure levels may not be sufficiently high to see overt effects with our limited sample size. As a result, borderline non-significant associations were observed that should be evaluated both longitudinally and in a larger cohort. In addition, some misclassification of both urinary creatinine and the metals could be possible, as kidney function can be influenced by metal exposure and diabetes status [71]; similarly, increased urinary metal concentrations could be due to increased urinary excretion rather than increased exposure, raising the possibility that associations of higher levels with diabetes traits may reflect reduced cellular and tissue metal/metalloid levels. We also acknowledge that the HOMA measurements may be imperfect markers of glycemic status, as it can be less valid in participants with lean type 2 diabetes mellitus and insulin secretory defects [72]; however, given that the average BMI of our study population was in the obese range and those with diabetes were excluded from HOMA analyses, we expect this to minimally affect our conclusions. We recognize the potential for residual confounding, as some variables that could influence diabetes status were not measured, such as dietary intake of supplements, co-exposure to other environmental pollutants, or other measures of socioeconomic status. We also acknowledge the possibility for inflated type I error, given the multiple tests conducted, but note the consistency of our results across multiple statistical methods and parameterization of glycemic/diabetic status.
Conclusions
In this study of 414 Mexican Americans living in Starr County, Texas, we found a strong association between increased urinary arsenic, molybdenum, copper, and the eight-metal mixture with alterations in steady-state measures of insulin-glucose homeostasis and fasting insulin levels. While requiring further investigation in prospective studies, these findings illuminate potential roles of these metals/metalloids in the pathogenesis of diabetes or as a marker of active or impending glycemic disruption within this historically high-risk Mexican American population living in Starr County, Texas. Importantly, identifying metals/metalloids that are pathogenically linked to diabetes development in diverse high-risk populations raises the possibility that individual- and policy-based exposure reduction strategies may offer novel approaches for mitigating the devastating burden of diabetes and its complications in vulnerable groups.
References
Centers for Disease Control and Prevention (2020) National Diabetes Statistics Report, 2020. https://www.cdc.gov/diabetes/library/features/diabetes-stat-report.html
American Diabetes Association (2018) Economic Costs of Diabetes in the US in 2017. Diabetes Care 41(5):917–28. https://doi.org/10.2337/dci18-0007
Aguayo-Mazzucato C, Diaque P, Hernandez S, Rosas S, Kostic A, Caballero AE (2019) Understanding the growing epidemic of type 2 diabetes in the Hispanic population living in the United States. Diabetes Metab Res Rev 35(2):e3097. https://doi.org/10.1002/dmrr.3097
Hanis CL, Ferrell RE, Barton SA, Aguilar L, Garza-Ibarra A, Tulloch BR et al (1983) Diabetes among Mexican Americans in Starr County. Texas Am J Epidemiol 118(5):659–672. https://doi.org/10.1093/oxfordjournals.aje.a113677
Heindel JJ, Blumberg B, Cave M, Machtinger R, Mantovani A, Mendez MA et al (2017) Metabolism disrupting chemicals and metabolic disorders. Reprod Toxicol 68:3–33. https://doi.org/10.1016/j.reprotox.2016.10.001
Neel BA, Sargis RM (2011) The paradox of progress: environmental disruption of metabolism and the diabetes epidemic. Diabetes 60(7):1838–1848. https://doi.org/10.2337/db11-0153
Ruiz D, Becerra M, Jagai JS, Ard K, Sargis RM (2018) Disparities in environmental exposures to endocrine-disrupting chemicals and diabetes risk in vulnerable populations. Diabetes Care 41(1):193–205. https://doi.org/10.2337/dc16-2765
Menke A, Guallar E, Cowie CC (2016) Metals in urine and diabetes in US adults. Diabetes 65(1):164–71. https://doi.org/10.2337/db15-0316
Kazi TG, Afridi HI, Kazi N, Jamali MK, Arain MB, Jalbani N et al (2008) Copper, chromium, manganese, iron, nickel, and zinc levels in biological samples of diabetes mellitus patients. Biol Trace Elem Res 122(1):1–18. https://doi.org/10.1007/s12011-007-8062-y
Cruz KJC, de Oliveira ARS, Morais JBS, Severo JS, Mendes PMV, de Sousa Melo SR et al (2018) Zinc and insulin resistance: biochemical and molecular aspects. Biol Trace Elem Res 186(2):407–412. https://doi.org/10.1007/s12011-018-1308-z
Endocrine Society (2018) Endocrine-disrupting chemicals. An Endocrine Society Position Statement. https://www.endocrine.org/advocacy/position-statements/endocrine-disrupting-chemicals
Mimoto MS, Nadal A, Sargis RM (2017) Polluted pathways: mechanisms of metabolic disruption by endocrine disrupting chemicals. Curr Environ Health Rep 4(2):208–222. https://doi.org/10.1007/s40572-017-0137-0
Li XT, Yu PF, Gao Y, Guo WH, Wang J, Liu X et al (2017) Association between plasma metal levels and diabetes risk: a case-control study in China. Biomed Environ Sci 30(7):482–491. https://doi.org/10.3967/bes2017.064
Guo FF, Hu ZY, Li BY, Qin LQ, Fu C, Yu H et al (2019) Evaluation of the association between urinary cadmium levels below threshold limits and the risk of diabetes mellitus: a dose-response meta-analysis. Environ Sci Pollut Res Int 26(19):19272–19281. https://doi.org/10.1007/s11356-019-04943-3
Li Y, Zhang Y, Wang W, Wu Y (2017) Association of urinary cadmium with risk of diabetes: a meta-analysis. Environ Sci Pollut Res Int 24(11):10083–10090. https://doi.org/10.1007/s11356-017-8610-8
Feng W, Cui X, Liu B, Liu C, Xiao Y, Lu W et al (2015) Association of urinary metal profiles with altered glucose levels and diabetes risk: a population-based study in China. PLoS ONE 10(4):e0123742. https://doi.org/10.1371/journal.pone.0123742
Ettinger AS, Bovet P, Plange-Rhule J, Forrester TE, Lambert EV, Lupoli N et al (2014) Distribution of metals exposure and associations with cardiometabolic risk factors in the “Modeling the Epidemiologic Transition Study.” Environ Health 13:90. https://doi.org/10.1186/1476-069X-13-90
Laclaustra M, Navas-Acien A, Stranges S, Ordovas JM, Guallar E (2009) Serum selenium concentrations and diabetes in US adults: National Health and Nutrition Examination Survey (NHANES) 2003–2004. Environ Health Perspect 117(9):1409–13. https://doi.org/10.1289/ehp.0900704
Bleys J, Navas-Acien A, Guallar E (2007) Serum selenium and diabetes in U.S. adults. Diabetes Care 30(4):829–34. https://doi.org/10.2337/dc06-1726
Hanis CL, Redline S, Cade BE, Bell GI, Cox NJ, Below JE et al (2016) Beyond type 2 diabetes, obesity and hypertension: an axis including sleep apnea, left ventricular hypertrophy, endothelial dysfunction, and aortic stiffness among Mexican Americans in Starr County. Texas Cardiovasc Diabetol 15:86. https://doi.org/10.1186/s12933-016-0405-6
Jun G, Aguilar D, Evans C, Burant CF, Hanis CL (2020) Metabolomic profiles associated with subtypes of prediabetes among Mexican Americans in Starr County, Texas. USA Diabetologia 63(2):287–295. https://doi.org/10.1007/s00125-019-05031-4
Center for Disease Control and Prevention (2021) Hispanic/Latino Americans and Type 2 Diabetes. https://www.cdc.gov/diabetes/library/features/hispanic-diabetes.html
Brown EL, Essigmann HT, Hoffman KL, Palm NW, Gunter SM, Sederstrom JM, et al. (2020) Impact of Diabetes on the Gut and Salivary IgA Microbiomes. Infect Immun 88(12):e00301–20. https://doi.org/10.1128/IAI.00301-20.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28(7):412–419. https://doi.org/10.1007/BF00280883
Agency for Toxic Substances and Disease Registry (ATSDR) (2007) Toxicological profile for Arsenic. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. https://www.atsdr.cdc.gov/toxprofiles/tp2.pdf
Agency for Toxic Substances and Disease Registry (ATSDR) (2005) Toxicological profile for Tin and Tin Compounds. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. https://www.atsdr.cdc.gov/toxprofiles/tp55.pdf
Agency for Toxic Substances and Disease Registry (ATSDR) (2004) Toxicological profile for Copper. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. https://www.atsdr.cdc.gov/toxprofiles/tp132.pdf
Agency for Toxic Substances and Disease Registry (ATSDR) (2020) Toxicological profile for Molybdenum. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. https://www.atsdr.cdc.gov/toxprofiles/tp212.pdf
Agency for Toxic Substances and Disease Registry (ATSDR) (2005) Toxicological profile for Nickel. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service
Agency for Toxic Substances and Disease Registry (ATSDR) (2003) Toxicological profile for Selenium. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. https://www.atsdr.cdc.gov/ToxProfiles/tp92.pdf
Li S, Wang J, Zhang B, Liu Y, Lu T, Shi Y et al (2018) Urinary Lead Concentration Is an Independent Predictor of Cancer Mortality in the U.S General Population. Front Oncol 8:242. https://doi.org/10.3389/fonc.2018.00242
Brookhart MA, Sturmer T, Glynn RJ, Rassen J, Schneeweiss S (2010) Confounding control in healthcare database research: challenges and potential approaches. Med Care 48(6 Suppl):S114–S120. https://doi.org/10.1097/MLR.0b013e3181dbebe3
Krishnakumar PK, Qurban MA, Stiboller M, Nachman KE, Joydas TV, Manikandan KP et al (2016) Arsenic and arsenic species in shellfish and finfish from the western Arabian Gulf and consumer health risk assessment. Sci Total Environ 566–567:1235–1244. https://doi.org/10.1016/j.scitotenv.2016.05.180
Keil AP, Buckley JP, O’Brien KM, Ferguson KK, Zhao S, White AJ (2020) A Quantile-Based g-Computation Approach to Addressing the Effects of Exposure Mixtures. Environ Health Perspect 128(4):47004. https://doi.org/10.1289/EHP5838
Thomas DJ, Styblo M, Lin S (2001) The cellular metabolism and systemic toxicity of arsenic. Toxicol Appl Pharmacol 176(2):127–144. https://doi.org/10.1006/taap.2001.9258
National Research Council (US) (1999) Subcommittee on Arsenic in Drinking Water. Arsenic in Drinking Water. Washington (DC): National Academies Press (US). Available from: https://www.ncbi.nlm.nih.gov/books/NBK230893/. https://doi.org/10.17226/6444
Ryker S (2001) Mapping arsenic in groundwater -- A real need, but a hard problem. Geotimes Newsmagazine Earth Sci p. 34–6. http://www.agiweb.org/geotimes/nov01/feature_Asmap.html
Gilbert-Diamond D, Cottingham KL, Gruber JF, Punshon T, Sayarath V, Gandolfi AJ et al (2011) Rice consumption contributes to arsenic exposure in US women. Proc Natl Acad Sci U S A 108(51):20656–20660. https://doi.org/10.1073/pnas.1109127108
Del Razo LM, Garcia-Vargas GG, Valenzuela OL, Castellanos EH, Sanchez-Pena LC, Currier JM et al (2011) Exposure to arsenic in drinking water is associated with increased prevalence of diabetes: a cross-sectional study in the Zimapan and Lagunera regions in Mexico. Environ Health 10:73. https://doi.org/10.1186/1476-069X-10-73
Tseng CH, Tai TY, Chong CK, Tseng CP, Lai MS, Lin BJ et al (2000) Long-term arsenic exposure and incidence of non-insulin-dependent diabetes mellitus: a cohort study in arseniasis-hyperendemic villages in Taiwan. Environ Health Perspect 108(9):847–851. https://doi.org/10.1289/ehp.00108847
Sung TC, Huang JW, Guo HR (2015) Association between Arsenic Exposure and Diabetes: A Meta-Analysis. Biomed Res Int 2015:368087. https://doi.org/10.1155/2015/368087
Navas-Acien A, Silbergeld EK, Streeter RA, Clark JM, Burke TA, Guallar E (2006) Arsenic exposure and type 2 diabetes: a systematic review of the experimental and epidemiological evidence. Environ Health Perspect 114(5):641–648. https://doi.org/10.1289/ehp.8551
Dover EN, Patel NY, Styblo M (2018) Impact of in vitro heavy metal exposure on pancreatic beta-cell function. Toxicol Lett 299:137–144. https://doi.org/10.1016/j.toxlet.2018.09.015
Liu S, Guo X, Wu B, Yu H, Zhang X, Li M (2014) Arsenic induces diabetic effects through beta-cell dysfunction and increased gluconeogenesis in mice. Sci Rep 4:6894. https://doi.org/10.1038/srep06894
Kirkley AG, Carmean CM, Ruiz D, Ye H, Regnier SM, Poudel A et al (2018) Arsenic exposure induces glucose intolerance and alters global energy metabolism. Am J Physiol Regul Integr Comp Physiol 314(2):R294–R303. https://doi.org/10.1152/ajpregu.00522.2016
Sargis RM (2014) The hijacking of cellular signaling and the diabetes epidemic: mechanisms of environmental disruption of insulin action and glucose homeostasis. Diabetes Metab J 38(1):13–24. https://doi.org/10.4093/dmj.2014.38.1.13
Momcilovic B (1999) A case report of acute human molybdenum toxicity from a dietary molybdenum supplement–a new member of the “Lucor metallicum” family. Arh Hig Rada Toksikol 50(3):289–297
Scott R, Eugenia GS, Melanie AWB, Sara ED, Thomas EG, Keith HP (2020) Spatial and temporal patterns of heavy metal deposition resulting from a smelter in El Paso. Texas Journal of Geochemical Exploration 210:106414. https://doi.org/10.1016/j.gexplo.2019.106414
Bulka CM, Daviglus ML, Persky VW, Durazo-Arvizu RA, Aviles-Santa ML, Gallo LC et al (2017) Occupational Exposures and Metabolic Syndrome Among Hispanics/Latinos: Cross-Sectional Results From the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). J Occup Environ Med 59(11):1047–1055. https://doi.org/10.1097/JOM.0000000000001115
Wang X, Mukherjee B, Karvonen-Gutierrez CA, Herman WH, Batterman S, Harlow SD et al (2020) Urinary metal mixtures and longitudinal changes in glucose homeostasis: The Study of Women’s Health Across the Nation (SWAN). Environ Int 145:106109. https://doi.org/10.1016/j.envint.2020.106109
Xiao L, Zhou Y, Ma J, Sun W, Cao L, Wang B et al (2018) Oxidative DNA damage mediates the association between urinary metals and prevalence of type 2 diabetes mellitus in Chinese adults. Sci Total Environ 627:1327–1333. https://doi.org/10.1016/j.scitotenv.2018.01.317
Yang TY, Yen CC, Lee KI, Su CC, Yang CY, Wu CC et al (2016) Molybdenum induces pancreatic beta-cell dysfunction and apoptosis via interdependent of JNK and AMPK activation-regulated mitochondria-dependent and ER stress-triggered pathways. Toxicol Appl Pharmacol 294:54–64. https://doi.org/10.1016/j.taap.2016.01.013
Domingo-Relloso A, Grau-Perez M, Galan-Chilet I, Garrido-Martinez MJ, Tormos C, Navas-Acien A et al (2019) Urinary metals and metal mixtures and oxidative stress biomarkers in an adult population from Spain: The Hortega Study. Environ Int 123:171–180. https://doi.org/10.1016/j.envint.2018.11.055
Robertson RP, Harmon J, Tran PO, Tanaka Y, Takahashi H (2003) Glucose toxicity in beta-cells: type 2 diabetes, good radicals gone bad, and the glutathione connection. Diabetes 52(3):581–587. https://doi.org/10.2337/diabetes.52.3.581
Mendy A, Gasana J, Vieira ER (2012) Urinary heavy metals and associated medical conditions in the US adult population. Int J Environ Health Res 22(2):105–118. https://doi.org/10.1080/09603123.2011.605877
Meeker JD, Rossano MG, Protas B, Padmanahban V, Diamond MP, Puscheck E et al (2010) Environmental exposure to metals and male reproductive hormones: circulating testosterone is inversely associated with blood molybdenum. Fertil Steril 93(1):130–140. https://doi.org/10.1016/j.fertnstert.2008.09.044
Shiue I, Hristova K (2014) Higher urinary heavy metal, phthalate and arsenic concentrations accounted for 3–19% of the population attributable risk for high blood pressure: US NHANES, 2009–2012. Hypertens Res 37(12):1075–1081. https://doi.org/10.1038/hr.2014.121
Taylor AA, Tsuji JS, Garry MR, McArdle ME, Goodfellow WL Jr, Adams WJ et al (2020) Critical Review of Exposure and Effects: Implications for Setting Regulatory Health Criteria for Ingested Copper. Environ Manage 65(1):131–159. https://doi.org/10.1007/s00267-019-01234-y
Qiu Q, Zhang F, Zhu W, Wu J, Liang M (2017) Copper in Diabetes Mellitus: a Meta-Analysis and Systematic Review of Plasma and Serum Studies. Biol Trace Elem Res 177(1):53–63. https://doi.org/10.1007/s12011-016-0877-y
Sobczak AIS, Stefanowicz F, Pitt SJ, Ajjan RA, Stewart AJ (2019) Total plasma magnesium, zinc, copper and selenium concentrations in type-I and type-II diabetes. Biometals 32(1):123–138. https://doi.org/10.1007/s10534-018-00167-z
Bjorklund G, Dadar M, Pivina L, Dosa MD, Semenova Y, Aaseth J (2020) The Role of Zinc and Copper in Insulin Resistance and Diabetes Mellitus. Curr Med Chem 27(39):6643–6657. https://doi.org/10.2174/0929867326666190902122155
Lowe J, Taveira-da-Silva R, Hilario-Souza E (2017) Dissecting copper homeostasis in diabetes mellitus. IUBMB Life 69(4):255–262. https://doi.org/10.1002/iub.1614
Cooper GJ (2011) Therapeutic potential of copper chelation with triethylenetetramine in managing diabetes mellitus and Alzheimer’s disease. Drugs 71(10):1281–1320. https://doi.org/10.2165/11591370-000000000-00000
Tinkov AA, Filippini T, Ajsuvakova OP, Aaseth J, Gluhcheva YG, Ivanova JM et al (2017) The role of cadmium in obesity and diabetes. Sci Total Environ 601–602:741–755. https://doi.org/10.1016/j.scitotenv.2017.05.224
Edwards J, Ackerman C (2016) A Review of Diabetes Mellitus and Exposure to the Environmental Toxicant Cadmium with an Emphasis on Likely Mechanisms of Action. Curr Diabetes Rev 12(3):252–258. https://doi.org/10.2174/1573399811666150812142922
RafatiRahimzadeh M, RafatiRahimzadeh M, Kazemi S, Moghadamnia AA (2017) Cadmium toxicity and treatment: An update. Caspian J Intern Med 8(3):135–45. https://doi.org/10.22088/cjim.8.3.135
Wu M, Song J, Zhu C, Wang Y, Yin X, Huang G et al (2017) Association between cadmium exposure and diabetes mellitus risk: a prisma-compliant systematic review and meta-analysis. Oncotarget 8(68):113129–41
Kuo CC, Moon K, Thayer KA, Navas-Acien A (2013) Environmental chemicals and type 2 diabetes: an updated systematic review of the epidemiologic evidence. Curr Diab Rep 13(6):831–849. https://doi.org/10.1007/s11892-013-0432-6
Wang X, Karvonen-Gutierrez CA, Herman WH, Mukherjee B, Harlow SD, Park SK (2020) Urinary metals and incident diabetes in midlife women: Study of Women's Health Across the Nation (SWAN). BMJ Open Diab Res Care 8(1):e001233. https://doi.org/10.1136/bmjdrc-2020-001233
Pokorska-Niewiada K, Brodowska A, Szczuko M (2021) The Content of Minerals in the PCOS Group and the Correlation with the Parameters of Metabolism. Nutrients 13(7): 2214. https://doi.org/10.3390/nu13072214
Lunyera J, Smith SR (2017) Heavy metal nephropathy: considerations for exposure analysis. Kidney Int 92(3):548–550. https://doi.org/10.1016/j.kint.2017.04.043
Kang ES, Yun YS, Park SW, Kim HJ, Ahn CW, Song YD et al (2005) Limitation of the validity of the homeostasis model assessment as an index of insulin resistance in Korea. Metabolism 54(2):206–211. https://doi.org/10.1016/j.metabol.2004.08.014
Funding
This work was supported by the National Institutes of Health (R01 ES028879 and R21 ES030884 supporting RMS; P30 ES027792 supporting MA and RMS; UL1 TR002003 supporting MA and RMS via the UIC Center for Clinical and Translational Science; University of Illinois at Chicago’s Medical-Scientist Training Program T32 GM079086 supporting MS; and R01 DK116378 supporting DA and CLH). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
RMS declares he has received honoraria from CVS/Health and the American Medical Forum, neither of which relate to the present study.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Weiss, M.C., Shih, YH., Bryan, M.S. et al. Relationships Between Urinary Metals and Diabetes Traits Among Mexican Americans in Starr County, Texas, USA. Biol Trace Elem Res 201, 529–538 (2023). https://doi.org/10.1007/s12011-022-03165-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-022-03165-y