
Abstract
Background
Biplanar x-ray images obtained with patients in a standing weightbearing position allow reconstruction of three-dimensional (3-D) bone geometries, with lower radiation exposure than CT scans and better bone definition than MRI.
Questions/Purposes
We determined the reproducibility of 3-D parameter values of the hips and pelves of healthy children, using biplanar x-ray images.
Methods
We built 3-D models of the hips of 33 children without musculoskeletal problems: 10 subjects younger than 9 years and 23 who were 9 years or older. Three anatomic landmarks and nine hip and pelvic parameters were computed for each reconstruction. To determine the reliability of these landmarks and parameters, each bone was reconstructed four times by two independent observers, leading to a total of 264 reconstructions, and parameters were studied for the two age groups and compared between dancers and nondancers.
Results
Taking into account all reconstructions, the interobserver reproducibility ranged from 2 to 4 mm for landmark positions or distance parameters, and 2° to 6° for angular parameters. The most reproducible point was the center of the femoral head (range, 0.2–17 mm). The distance between this center and its projection on the plane fitting the edge of the acetabulum, and the pelvic tilt were the most reproducible parameters.
Conclusions
Reproducible 3-D reconstructions of hips and pelves of children were possible using biplanar x-ray images, regardless of the children’s ages. Although we report preliminary values for 3-D parameters in healthy children’s hips, further work is needed to obtain direct validation of our parameters using CT reconstructions of cadaveric specimens to avoid high doses of radiation.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Various measurements can be made on a plain radiograph of a child’s pelvis. As the hip is a three-dimensional (3-D) structure, it is important to evaluate 3-D parameters with the hip in its functional standing position. Three-dimensional methods of imaging have disadvantages: MRI provides a low definition for bone and CT requires a high radiation exposure too great to be used in common practice with children. Moreover, neither of these two modalities can provide images with the patient in a standing functional position. The EOS® system (EOS Imaging®, Biospace Med, Paris, France) and associated software allow reconstruction of 3-D bone geometries, based on two biplanar x-ray images taken with the patient in a standing position [1, 3, 7]. This technique provides better bone definition than MRI and lower radiation exposure than CT. Moreover, the duration for acquisition of the radiographs is approximately 20 seconds for an entire body, which is faster than CT and MRI, thus is particularly suited for children.
We applied this novel modeling process to improve characterization of children’s hips by introducing 3-D anatomic parameters of interest. We divided our study in three steps. First, we defined three anatomic landmarks and tested their reproducibility. Second, using these points, we computed nine 3-D parameters of interest and tested their reproducibility. Third, we compared these 3-D parameters between two age groups (younger or older than 9 years), and between dancers and nondancers.
Materials and Methods
We recruited 33 children who had minor orthopaedic problems, such as mechanical low back pain without radiographic abnormality. The mean age of the patients was 11 years (range, 3–17 years). This group was divided into three subgroups: (1) 10 were nondancers younger than 9 years; (2) 13 were nondancers older than 9 years; and (3) 10 were ballet dancers older than 9 years from the National Opera of Paris. These dancers needed spine radiographs for systematic spine control, required by the National Opera of Paris medical staff, before being accepted in the National ballet school. All radiographs were obtained for medical purposes, the child was fully informed, and the approval of both parents was required. The protocol (CPP-PRP-6001) was approved by our ethics and advisory council.
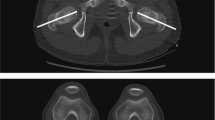
We used a biplanar x-ray system (EOS®, Biospace Med) to acquire radiographs of subjects in a standing position (Fig. 1) [7]. The 3-D geometries of the 66 hips were obtained using a specific reconstruction software based on a morphorealistic parametric subject-specific model [1, 3, 13] (Fig. 2). The software output coordinates of several anatomic regions, eg, the center of the femoral head, the points forming the acetabular edge. We then used a dedicated MATLAB® program (The Mathworks, Inc, Natick, MA, USA) to input these regions to define our three anatomic landmarks and compute the nine 3-D anatomic parameters of interest, based on the 3-D bone geometry model obtained for each patient. The three landmarks were: (1) the center (AC) of the least-square sphere fitting the acetabulum (Fig. 3A); (2) the orthogonal projection (M) of AC on the least-square plane (P) fitting the edge of the acetabulum (Fig. 3A); and (3) the center (Z) of the least-square sphere fitting the femoral head (Fig. 3B).

The patient is standing in the appropriate position in the biplanar x-ray machine.

Reconstruction of the bony structures using two biplanar x-ray images is shown. The 2-D contours on the (A) lateral and (B) frontal views are seen on these radiographs. (C) The 3-D model was obtained after manual adjustments of the contours.

The anatomic landmarks and parameters are shown for (A) points M (the orthogonal projection of the AC), AC (the center of the least-square sphere fitting the acetabulum), and plane (P) fitting the acetabular edge; (B) the distance of the lateralization ratio (LR) between the center of the femoral head (Z) and its projection on the midplane; and (C) acetabular anteversion (ANT). (D) The three pelvic indexes, sacral slope (SS), pelvic index (PI), and pelvic tilt (PT) and (E) computation of acetabular formation and femoral head covering indexes are shown. The black points represent the acetabulum surface on the pelvis model and the zone of the head covered by the acetabulum on the femur model, respectively.
The nine 3-D anatomic parameters of interest were: (1) the distance (ZM) between the center of the femoral head (Z) and its projection (M) on the plane fitting the edge of the acetabulum, which is an index of the degree of decentralization [15]; (2) the intercenter distance (IC) between the center of the femoral head (Z) and the center of the acetabulum (AC); (3) the lateralization ratio (LR) (Fig. 3B), which is the distance between the center of the femoral head (Z) and its orthogonal projection on the midplane of the pelvis, normalized by the radius of the sphere fitting the acetabulum; (4) acetabular anteversion (Fig. 3C), (5) pelvic tilt (PT) (Fig. 3D), (6) pelvic incidence (PI) (Fig. 3D), (7) sacral slope (SS) (Fig. 3D); (8) index of formation of the acetabulum (AF), which is the ratio between the surface of the acetabulum and the surface of half the sphere fitting the acetabulum (Fig. 3D) (an AF index of 100 therefore would indicate a half-hemispheric acetabulum); and (9) the femoral head covering index (FHC), which is the ratio between the surface of the femoral head covered by the acetabulum and the surface of half the sphere fitting the femoral head (Fig. 3E).
To assess the reproducibility of our variables (anatomic landmarks and parameters), two operators (VV, VR) reconstructed two 3-D models per patient, thus giving a set of four values per variable and hip. To assess landmark position reproducibility, the mean of the four points were computed, then the distances (di, for i = 1, …4) between each of these four points and the mean were calculated. Finally, the mean distance (dm) was calculated and the differences (dfi = di – dm, for i = 1, …4), were computed. We then stored the dfi for each hip in a vector, thus giving 264 values (ie, four values for each of the 66 hips), and computed the 95% CI as two standard deviations of this vector. The reproducibility of each of the nine parameters was estimated using the following method: for each hip and each parameter, the mean of the four values obtained from the four models was calculated, then the differences between each of the four parameter values and this mean were evaluated and stored in a global vector. The 95% CI then was calculated as two standard deviations of this vector. Each parameter’s value was estimated for each hip by calculating the mean of the four values obtained from the four models. Mean and standard deviation values then were calculated for all children concerned. All calculations were performed for five subcohorts: all 33 children, 10 children younger than 9 years, 23 children older than 9 years, 13 nondancers, and 10 dancers (all older than 9 years). We used XLstat software (Addinsoft, Paris, France) for the statistical analyses.
Results
The three anatomic landmarks (Z, AC, and M) defined showed position reproducibility less than 4 mm (Table 1). The most reproducible point was the center of the femoral head (Z) with a 95% CI of 2 mm. There were no differences between the two age groups, however points were more reproducible for dancers than for nondancers.
Although the reproducibility of the ZM and IC distances was similar when considering all the children, these parameters tended to be more reproducible for dancers than for nondancers, but not statistically so (Table 1). The lateralization ratio had a 95% CI of 1 for all children; this value remained the same regardless of the age and activity of the child. When considering all the children, the most reproducible angle was pelvic tilt, with a 95% CI of 2°, whereas the anteversion angle was the least reproducible, with a 95% CI of 6°. There was better reproducibility of the femoral head covering index in older (p < 0.001) (older than 9 years) than in younger children.
The parameters values (Table 2) showed there was a difference between the two age groups concerning the lateralization ratio (p = 0.008), sacral slope (p = 0.01), pelvic incidence (p = 0.002), femoral head covering index (p < 0.0001), and index of formation of the acetabulum (p < 0.0001). Comparing nondancers with dancers, the difference occurred only for the lateralization ratio (p = 0.01).
Discussion
As the hip is a 3-D functioning joint, it is important to evaluate 3-D parameters with the hip in its functional standing position. In this study two biplanar x-ray images were taken, using the EOS® system, which provides better bone definition than MRI and lower radiation exposure than CT. The goal of our study was to introduce 3-D anatomic parameters to improve characterization of children’s hips. First, we defined three anatomic landmarks and verified their reproducibility; second, these landmarks were used to compute nine reproducible parameters of interest. Third, we compared these parameters between children younger and older than 9 years, and between dancers and nondancers.
We acknowledge limitations of our study. First, the radiographs were taken with the first biplanar x-ray imaging system installed in 2003. Recent improvements in image quality could lead to greater reliability. Second, although the reconstruction methods have been validated for healthy adults and are reportedly accurate [1, 3], this has not been reported for children. To fully validate this system we would need to get high-resolution CT scans of cadaveric bones of children and compare their 3-D reconstruction with the ones from our system. Third, we have no data on the length of time the dancers had been dancing. High-intensity activity can affect remodeling [14, 16], and it is possible those who had been dancing longer could have had bony alterations whereas those who had been dancing for shorter periods would have not experienced such alterations and thus have had anatomy closer to that of nondancers. However, we found only one parameter (lateralization ratio) that differed between the two.
Reproducibility in position for anatomic landmarks was better for the center of the femoral head (Z) than for the center of the sphere fitting the acetabulum (AC) and its projection on the plane fitting the acetabulum edge (M), even though a previous study [8] proposed a method based on MRI to locate the center of the femoral head, advocating the usual difficulties to identify it in young children. The inferior point of the acetabulum also was difficult to find, especially in children younger than 10 years, as previously reported [2].
Reproducibility of pelvic parameters was good, with a 95% CI inferior to 3°, confirming the findings of Champain et al. [4]. They reported pelvic tilt had a reproducibility of 1.2°, sacral slope of 4.0°, and pelvic incidence of 3.4°. The anteversion angle was only slightly less reproducible, with a 95% CI of 5.6°. This could be because this parameter was based on the plane best fitting the acetabulum edge, which was difficult to define on the radiographs. Finally, even though we found no clear statistical evidence, we observed a tendency for better reproducibility of the parameters for the dancers, and this may be related to their increased bone mineral content in the lower limbs and femoral necks [12], making the radiographs sharper, and because all were older than 9 years. For all these parameters, values were comparable to the traditional 2-D measured ones. For the pelvic parameters (pelvic incidence, sacral slope, and pelvic tilt), the values in our series were comparable to values reported in the literature for each age group [10, 11, 18]. The lateralization ratio evaluated the position of the center of the femoral head with respect to the acetabulum. Although we found no reference value for this ratio in the literature, the reproducibility of this parameter made it reliable to use. It would be important to evaluate the evolution of this ratio in hips of patients with orthopaedic disorders to evaluate the radiographic changes of the hip and pelvis after a treatment.
The lower reproducibility of our parameters concerns the acetabular region. On traditional 2-D radiographs, the acetabular anteversion value is approximately 20° at the end of growth [5, 6, 9, 15, 17]. On 3-D CT scans, Dandachli et al. [6] measured acetabular anteversion and concluded that its normal value is approximately 17°, ranging from 1° to 31°. In the current study, the mean value was 8.3°, but as already explained, the uncertainty of this parameter is high, related to the difficulties in modeling the acetabulum edge. Although only the lateralization ratio was different between dancers and nondancers, we found that five of nine hip parameters were different between the children of the two age groups. In our series, there is an increase with age of the femoral head covering index and the index of formation of the acetabulum, matching the progressive lateral ossification of the acetabulum and of the femoral head coverage with growth. These findings suggest the proposed 3-D anatomic parameters are reproducible and therefore may be used to characterize children’s hips.
Our study provides preliminary values for 3-D parameters in healthy children’s hips. Three-dimensional reconstructions of the hips and pelves of children were created from biplanar x-ray images, regardless of the child’s age. Image quality improvements and modeling refinement should decrease the uncertainty of the parameters related to the acetabulum and its edge. Modeling a cartilaginous zone could be of particular interest. For example, the triradiate cartilage is used to draw a reference line to calculate many angles on the radiographs of a child’s hip. The reconstruction of these zones could be added in future studies to improve the accuracy of such 3-D models. Although most of our parameters were comparable to those in the literature, further work is needed to acquire biplanar x-ray images and CT scans, the latter remaining the gold standard for 3-D bone modeling, to obtain a direct validation. These studies will have to be performed on cadaveric specimens to avoid high radiation doses in children.
References
Baudouin A, Skalli W, de Guise JA, Mitton D. Parametric subject-specific model for in vivo 3D reconstruction using bi-planar X-rays: application to the upper femoral extremity. Med Biol Eng Comput. 2008;46:799–805.
Broughton NS, Brougham DI, Cole WG, Menelaus MB. Reliability of radiological measurements in the assessment of the child’s hip. J Bone Joint Surg Br. 1989;71:6–8.
Chaibi Y, Cresson T, Aubert B, Hausselle J, Neyret P, Hauger O, de Guise JA, Skalli, W. Fast three-dimensional reconstruction of the lower limb using a parametric model and statistical inferences and clinical measurements calculation from biplanar X-rays. Comput Methods Biomech Biomed Engin. 2012;15:457–466.
Champain S, Benchikh K, Nogier A, Mazel C, De Guise JA, Skalli W. Validation of new clinical quantitative analysis software applicable in spine orthopaedic studies. Eur Spine J. 2006;15:982–991.
Cirotteau Y. [Correlations between the bony structures of the hip][in French]. Rev Chir Orthop Reparatrice Appar Mot. 1982;68:14–19.
Dandachli W, Kannan V, Richards R, Shah Z, Hall-Craggs M, Witt J. Analysis of cover of the femoral head in normal and dysplastic hips: new CT-based technique. J Bone Joint Surg Br. 2008;90:1428–1434.
Dubousset J, Charpak G, Dorion I, Skalli W, Lavaste F, Deguise JA, Kalifa G, Ferey S. [A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: the EOS system][in French]. Bull Acad Natl Med. 2005;189:287–297; discussion 297–300.
Inan M, Senaran H, Mackenzie WG. Center of the femoral head: a magnetic resonance imaging study. J Pediatr Orthop. 2006;26:471–473.
Lude L, TaillardW. [Development of articular congruence of the hip in children (study of a radiologic profile)][in French]. Rev Chir Orthop Reparatrice Appar Mot. 1964; 50: 757–777.
Mac-Thiong JM, Berthonnaud E, Dimar JR 2nd, Betz RR, Labelle H. Sagittal alignment of the spine and pelvis during growth. Spine (Phila Pa 1976). 2004;29:1642–1647.
Mac-Thiong JM, Labelle H, Berthonnaud E, Betz RR, Roussouly P. Sagittal spinopelvic balance in normal children and adolescents. Eur Spine J. 2007;16:227–234.
Matthews BL, Bennell KL, McKay HA, Khan KM, Baxter-Jones AD, Mirwald RL, Wark JD. Dancing for bone health: a 3-year longitudinal study of bone mineral accrual across puberty in female non-elite dancers and controls. Osteoporos Int. 2006;17:1043–1054.
Mitton D, Deschênes S, Laporte S, Godbout B, Bertrand S, de Guise JA, Skalli W. 3D reconstruction of the pelvis from bi-planar radiography. Comput Methods Biomech Biomed Engin. 2006;9:1–5.
Murray RO, Duncan C. Athletic activity in adolescence as an etiological factor in degenerative hip disease. J Bone Joint Surg Br. 1971;53:406–419.
Pouletaut P, Claude I, Winzenrieth R, Ho Ba Tho MC, Sebag G. Automated analysis of MR image of hip: geometrical evaluation of the Legg-Calve-Perthes disease. Med Eng phys. 2005;27: 415–424.
Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC. The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res. 2011;469:3229–3240.
Tönnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976;119:39–47.
Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am. 2005;87:260–267.
Acknowledgments
We thank B. Sandoz PhD for his involvement in the data collection protocol. We also thank V. Vasta for the 3-D reconstructions and C. Fedelich and T. Bellot MD for technical support.
Author information
Authors and Affiliations
Corresponding author
Additional information
The Laboratoire de Biomecanique, Arts et métiers Paristech has received funding from the Agence Nationale pour la Recherche (ANR, Paris, France) (project SECUR_ENFANT_06_0385) and by MEDICEN (Paris, France).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at Arts et Métiers Paristech, Paris, France.
About this article
Cite this article
Rampal, V., Hausselle, J., Thoreux, P. et al. Three-dimensional Morphologic Study of the Child’s Hip: Which Parameters Are Reproducible?. Clin Orthop Relat Res 471, 1343–1348 (2013). https://doi.org/10.1007/s11999-012-2660-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2660-5