
Abstract
Background
Three-dimensional imaging (CT and MRI) is the gold standard for detecting femoral head-neck junction malformations in femoroacetabular impingement, yet plain radiographs are used for initial diagnostic evaluation. It is unclear, however, whether the plain radiographs accurately reflect the findings on three-dimensional imaging.
Questions/Purposes
We therefore: (1) investigated the correlation of alpha angle measurements on plain radiographs and radial reformats of CT scans; (2) determined which radiographic views are most sensitive and specific in detecting head-neck deformities present on CT scans; and (3) determined if specific radiographic views correlated with specific locations on the radial oblique CT scan.
Methods
We retrospectively reviewed 41 surgical patients with preoperative CT scans (radial oblique reformats) and plain radiographs (AP pelvis, 45° Dunn, frog lateral, and crosstable lateral). Alpha angles were measured on plain radiographs and CT reformats.
Results
The complete radiographic series was 86% to 90% sensitive in detecting abnormal alpha angles on CT. The maximum alpha angle on plain radiographs was greater than that of CT reformats in 61% of cases. Exclusion of the crosstable lateral did not affect the sensitivity (86%–88%). The Dunn view was most sensitive (71%–80%). The frog lateral showed the best specificity (91%–100%). Substantial correlations (intraclass correlation coefficients, 0.64–0.75) between radiograph and radial oblique CT position were observed, including AP/12:00 (superior), Dunn/1:00 (anterolateral), frog/3:00 (anterior), and crosstable/3:00 (anterior).
Conclusions
For diagnostic and treatment purposes, a three-view radiographic hip series (AP pelvis, 45° Dunn, and frog lateral) effectively characterizes femoral head-neck junction malformations.
Level of Evidence
Level II, diagnostic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Diagnosis of cam-type femoroacetabular impingement (FAI) relies on radiographic identification of deformity of the femoral head-neck junction [5]. This is most commonly performed with measurement of the alpha angle [21]. Although three-dimensional imaging (CT [2] and MRI [25]) is the gold standard for detection of femoral head-neck deformity, plain radiographs remain the initial diagnostic examination for FAI. Multiple radiographic views, including the AP pelvis [5], 45° Dunn lateral [17], frog lateral [6], and crosstable lateral [17], have been advocated to identify the deformity in cam-type FAI, yet limited information exists regarding the correlation of alpha angles on plain radiographs with those on three-dimensional imaging [1, 7, 8, 13]. To our knowledge, no study has directly compared all of these views with the gold standard of three-dimensional imaging.
Accurately identifying the precise location of deformity of the femoral head-neck junction is important in making decisions about treatment options and surgical technique selection [3]. Although maximal deformity most commonly occurs in the anterosuperior head-neck junction, it can also occur more superiorly or anteriorly [8, 22, 25]. Multiplanar reformatting of three-dimensional imaging to produce radial slices better identifies the location of maximal deformity compared with axial oblique imaging [25]. Radial oblique slices at the 12:00, 1:00, 2:00, and 3:00 positions are most useful because they are the common locations of deformity [25]. Several authors have studied the correlation of alpha angles on plain radiographs with those on three-dimensional imaging [1, 7, 8, 13]. Although the 45° and 90° Dunn views correlate with reformats of the anterosuperior neck (1:00–2:00), the correlation with measures on other radiographic views has not been established. In our experience, the AP pelvis, 45° Dunn view, and the frog lateral radiographs are complementary views in identifying deformity. It is unclear, however, whether the plain radiographs accurately reflect the findings on three-dimensional imaging.
The purposes of this study were: (1) to investigate the correlation of alpha angle measurements with a complete radiographic series and radial reformats of CT scans; (2) to determine which individual radiographic views or combinations of views are most sensitive and specific in detecting head-neck deformities present on CT scans; and (3) to determine if specific radiographic views correlated with specific locations on the radial oblique CT scan.
Patients and Methods
We retrospectively reviewed 212 surgical patients undergoing hip preservation surgery and identified 41 patients who underwent a CT scan of the hip from June 2008 and November 2009. CT scans were obtained by the treating surgeon for operative planning. Additionally, all patients had AP pelvis, 45° Dunn, frog lateral, and crosstable lateral radiographs performed (Fig. 1). Radiographs were performed using standardized techniques in the supine position, as previously described [5]. AP pelvis radiographs were performed with the legs internally rotated 15° and the beam centered midway between the anterosuperior iliac spines and pubic symphysis. Forty-five-degree Dunn radiographs were performed with the affected hip flexed 45° and abducted 20° in neutral rotation. Frog lateral radiographs were performed with the hip flexed 30° to 40° and abducted 45° such that the heel rests against the contralateral knee. The crosstable lateral radiographs were performed with the leg internally rotated 15° and the beam oriented at a 45° angle relative to the affected leg. These 41 patients comprised the cohort used in our study. Of the 41 hips included in the study, 28 were female and 13 were male with an average age of 31.7 years (range, 14–51 years). Diagnoses by the treating surgeon included cam FAI (56%), combined cam-pincer FAI (37%), hip dysplasia (5%), and normal structural anatomy (2%).

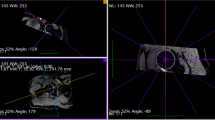
Case example demonstrating correlation between radiographic views and radial oblique CT reformats.
CT scans of the pelvis and proximal femur (Somaton Sensation 64; Siemens Medical Solutions USA, Inc, Malvern, PA, USA; 120 kV, 250 mAs, 0.75 mm slice thickness) were performed with protocols specific to this patient population. We used multiplanar reformatting of axial CT scans to generate radial oblique slices as previously described by Rakhra et al. [25]. This was done using Emageon Advanced Visualization software (Emageon, Birmingham, AL, USA) by one coauthor. Initial oblique axial and oblique sagittal plane reformats were generated parallel and perpendicular to the long axis of the femoral neck. Then, we used an oblique sagittal plane image to generate radial reformats at 30° intervals from the superior to anterior neck. Radial oblique slices were generated at the 12:00, 1:00, 2:00, and 3:00 positions (Fig. 2) with the 12:00 reformat representing the superior neck and the 3:00 reformat representing the anterior neck (all hips converted to standard nomenclature for a right hip) (Fig. 1).

Radial oblique CT reformats generated at the 12:00, 1:00, 2:00, and 3:00 positions with the 12:00 reformat representing the superior neck and the 3:00 reformat representing the anterior neck (all hips converted to standard nomenclature for a right hip).
We performed a power analysis for a power of 80% and a difference between alpha angles on radiographs and CT of 5°. A difference of 5° was chosen to reflect the minimum difference that would be considered like in our clinical experience. Power analysis determined approximately 40 subjects would be required.
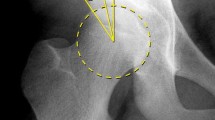
Alpha angles were measured as initially described by Notzli et al. [21] and adapted to plain radiographs [5] (Fig. 3). The alpha angle is the angle measured between two constructed lines: (1) a line is drawn from the center of the femoral head to the point on the anterolateral aspect of the head-neck junction where the radius of the femoral head first exceeds the radius of the femoral head found more centrally in the acetabulum; and (2) a line drawn from the center of the femoral head to the center of the femoral neck. Notzli et al. [21] originally reported an average alpha angle of 42° (range, 33°–48°) in normal control subjects compared with 74° (range, 55°–95°) in patients with symptomatic impingement. An alpha angle greater than 50° on any radial oblique CT image was considered indicative of cam-type FAI deformity [2, 12, 20]. As a secondary marker, an alpha angle greater than 63° was considered indicative of severe cam-type deformity [24].

Alpha angle measurements. (A–B) Abnormal alpha angles measurements on 12:00 CT reformat (89.4°) and AP pelvis radiograph (90.4°). (C–D) Normal alpha angles measurements on 3:00 CT reformat (46.7°) and frog lateral radiograph (48.0°).
We performed alpha angle measurements using novel computer-assisted measurement software (HipMorphometry, Chicago, IL, USA) adapted from the previously validated HipAnalysis Suite [11, 14, 15]. This software prompts the reader for various radiographic landmarks and then performs measurements automatically. Radiographic measurements of the AP pelvis, 45° Dunn, and frog lateral were performed by seven experienced hip surgeons (HSH, YJK, MBM, JJN, DP, DS, ES) as part of a larger radiographic study. Each radiograph was reviewed by a randomly chosen group of four of the surgeons. The median alpha value for each radiographic view was used to minimize the effect of any outlier measurements. Intraobserver and interobserver reliability of alpha angle measurements in this group has intraclass correlation coefficients (ICCs) of 0.92 and 0.43, respectively. Alpha angle measurements on crosstable lateral radiographs and CT reformats were analyzed one time by one additional coauthor (JJN). CT reformatting and alpha angle measurements of CT reformats were performed by this reader blinded to the plain radiographs. The intraobserver reliability of alpha angle measurements of this reader was previously determined in a subset of 20 radiographs to have an ICC of 0.94 [19].
Of the 41 hips, an alpha angle greater than 50° was present on at least one of the radial CT images in 73% (30 of 41) of hips. Deformity was present on a single CT slice in 10 hips (24%) and two or more slices in 20 hips (49%). On CT, an alpha angle greater than 50° was most common at the 2:00 position (59% [24 of 41]) followed by the 1:00 (46% [19 of 41]), 3:00 (34% [14 of 41]), and 12:00 (22% [nine of 41]) positions. Mean alpha angles were greatest at the 1:00 and 2:00 positions (53.0° and 53.4°, respectively). The location of maximal deformity was at the 1:00 or 2:00 position in 29 hips (71%) (Table 1). On plain radiographs, alpha angles greater than 50° were most common on the Dunn view (76% [31 of 41]) followed by the AP pelvis (42% [17 of 41]), frog lateral (37% [15 of 41]), and crosstable lateral (34.1% [14 of 41]) views. An alpha angle greater than 50° was present on at least one radiographic view in 37 hips (90%) (Table 1). Deformity was present on a single radiographic view in 16 hips (39%) and two or more views in 21 hips (59%). Mean alpha angles on plain radiographs were greatest on the Dunn view (57.2°) followed by the AP pelvis (51.6°) and frog lateral (50.1°). Using an alpha angle greater than 63° as a marker of severe deformity, severe deformity was most commonly present on Dunn (24% [10 of 31]) and AP pelvis radiographs (22% [nine of 41]). On CT, severe deformity was present most commonly at the 1:00 (24% [10 of 41]) and 12:00 (22% [nine of 41]) positions. Severe deformity was present on at least one CT reformat in 34% (14 of 41) and at least one radiograph in 34% (14 of 41) of hips.
We calculated the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of all radiographic views combined (and each individual radiographic view) to the presence of cam-type deformity (any or severe). A similar analysis, including ICCs, was performed to correlate individual radiographic views with radial oblique CT reformat positions.
Results
The maximum alpha angle on any plain radiographic view was greater than the maximum alpha angle of CT reformats in 25 hips (61%). The mean maximal angle on radiographic views was 61.9° compared with 59.8° on the radial oblique CT slices. Maximal alpha angle values on any plain radiograph were within 10° of maximal alpha angles on any radial oblique CT position in 83% (34 of 41) of hips.
The combination of all four radiographic views was 90% sensitive to detection of cam-type deformity (Table 2). Three hips had cam-type deformity on CT that was not seen on any radiograph. However, 10 hips had deformity on radiographs (most commonly the Dunn view) that was not seen on any CT reformat. The Dunn view alone had the highest sensitivity (80% [24 of 30]) of any single radiographic view. However, false-positives were most commonly seen with the Dunn view having seven, whereas no other view had more than two. The combination of Dunn and AP pelvis views maximized sensitivity (87%). Additionally, this combination had a positive predictive value of 79% and an overall agreement rate of 73% relative to deformity on CT scan. The addition of a frog lateral or crosstable lateral resulted in minimal improvement in the sensitivity. The frog lateral view had the best specificity (91%) of any radiographic view, correctly identifying 10 of 11 patients without deformity. The frog lateral view had the highest positive predictive value (93%) of any radiographic view with 14 of 15 hips with deformity on this radiograph view having deformity on CT. Similarly, for severe cam-type deformity (alpha angle > 63°), a sensitivity of 86% was found for the combination of all four radiographs. The Dunn view (71%) and the AP pelvis (64%) were most sensitive to the detection of severe deformity. Sensitivity was maximized with the combination of AP pelvis, Dunn, and frog lateral views (86%). No false-positives were noted for the AP pelvis, Dunn, or frog views, resulting in specificities and positive predictive values of 100% for each of these views. The rate of agreement between plain radiographs and CT was maximized with the combination of AP pelvis, Dunn, and frog lateral views (95%).
Substantial correlation was present between radiographs and corresponding radial locations on CT (AP pelvis/12:00–1:00, 45° Dunn/1:00–2:00, frog/crosstable/3:00) (Table 3). For these radiograph-radial oblique slice combinations, alpha angles on plain radiographs and radial oblique CT slices were within 10° in 68% to 83% of hips (Table 4). The AP pelvis had substantial correlation with the 12:00 and 1:00 positions. The AP pelvis radiograph was most sensitive to deformity at the 12:00 radial location (78%) (compared with other radial oblique positions). The 45° Dunn view had substantial correlation with the 1:00 and 2:00 positions. The Dunn view was 84% to 89% sensitive to deformity at any position on radial reformats. However, the Dunn view showed maximal rates of agreement (68%) and positive predictive value (68%) for the 2:00 CT position (Table 5). Both the frog lateral view and crosstable lateral view had substantial correlation with the 3:00 position. The frog lateral and crosstable radiographs were most sensitive to deformity at the 3:00 position (79% for both) (Table 5). Both the frog lateral and crosstable lateral radiographs had high positive predictive values (73%–79%) and overall accuracy (83%–85%) for the 3:00 position.
Discussion
Deformity of the femoral head-neck junction in cam-type FAI can occur at any position in the anterior to superior neck while most commonly occurring at the anterosuperior neck (1:00–2:00) [22, 25]. Detection of cam-type FAI on three-dimensional imaging studies (CT or MRI) with radial oblique reformats spanning the anterosuperior neck remains the current gold standard test [25]. Our study: (1) investigated the correlation of alpha angle measurements with a complete radiographic series and radial reformats of CT scans; (2) determined which radiographic views are most sensitive and specific in detecting head-neck deformities present on CT scans; and (3) determined if specific radiographic views correlated with specific locations on the radial oblique CT scan. Our study demonstrates that the use of the AP pelvis, 45° Dunn, and frog lateral radiographs can determine and characterize extension of the cam deformity to the superior, anterosuperior, and anterior neck, respectively.
Our study has several limitations. First, although radiographs were taken according to a standardized protocol, there was some degree of variation as a result of technique. This variability is minimized with the standardized technique performed at a single institution. Second, we used a single reader rather than a group of readers for measurement of alpha angles on radial oblique CT reformats and crosstable radiographs. Given the complexity of multiplanar reformatting, we believed measurement of these images was best performed by the individual performing the reformatting. Additionally, this reader was blinded to plain radiographic findings. Several previous studies have documented the high intraobserver and interobserver reliability of alpha angle measurement on plain radiographs and three-dimensional imaging [1, 16, 21], whereas other studies have questioned its interobserver reliability [4, 12]. Despite concerns over difficulty with this measurement, the alpha angle remains the current standard for radiographic characterization of cam-type deformity.
Several authors have questioned the use of plain radiographs [8, 13], whereas others have even advocated the routine intraoperative use of CT [18]. Although CT provides excellent visualization of the bony deformity, limitations of its use include additional radiation exposure, cost, and routine availability of complex reconstructive sequences. At our institution, musculoskeletal pelvic CT results in a radiation exposure (6–7 mSv) equivalent to approximately 25 to 30 AP pelvis radiographs (0.24 mSv) or 12 to 15 three-view hip series (AP pelvis, Dunn, frog) (0.48 mSv) [10]. Advanced CT protocols have recently been developed at some centers to decrease this exposure by a factor of 2 to 3. The routine use of CT for diagnosis and treatment planning in FAI is extremely variable. MRI similarly provides excellent visualization of the structural anatomy including the acetabular labrum, but sequences for radial oblique reformatting are not uniformly available. Three-dimensional reformatting is not currently available for MRI as it is for CT. The three-view radiographic series can also be simulated fluoroscopically in the operating room to assess the adequacy of resection in each of these quadrants. Inadequate resection of cam-type deformity remains a common reason for revision hip preservation surgery [9, 23]. Nevertheless, three-dimensional imaging has additional advantages in deformity characterization and surgical planning for borderline cases or cases with severe deformities, yet, in most cases, plain radiographs characterize the severity and location of the deformity.
Limited information on the use of plain radiographs in the detection of cam-type FAI has been previously reported (Table 6) [1, 6, 7, 13]. Our study supports the findings of Barton et al. [1] and Domayer et al. [7] of the correlation of the Dunn view (45° or 90°) with the 1:00 to 2:00 position on the anterosuperior head-neck junction. Previous studies [1, 6, 7, 13] have not established a strong correlation between the AP pelvis, frog lateral, and crosstable lateral radiographs and positions on the femoral head-neck junction. Clohisy et al. [6] previously reported that the frog lateral radiograph (compared with AP pelvis and crosstable views) best differentiates between hips with cam-type deformity and normal hips. Konan et al. [13] recently questioned the validity of the frog lateral radiograph in evaluating FAI. They demonstrated poor correlation of alpha angles on frog lateral radiographs to measurements on three-dimensional imaging. However, we found strong correlation between the frog lateral radiograph and the 3:00 position. The frog lateral view exhibited less correlation with measurements at the 12:00 to 2:00 positions as would be expected. Collectively these data indicate that the frog lateral is clinically useful for identifying anterior (3:00) femoral malformations.
The 45° Dunn view is most sensitive radiograph (80%) to cam-type deformity of the head-neck junction. The 45° Dunn view most strongly correlates with the 1:00 to 2:00 radial oblique image, the most common location of deformity in this cohort. In nearly 30% of this population, maximal deformity was present at the superior or anterior neck, not the anterosuperior neck. This is higher than the rate of 9.8% previously reported by Rakhra et al. [25]. The AP pelvis radiograph correlates strongest with the 12:00 to 1:00 radial oblique slice. Both the frog lateral and crosstable lateral in 15° internal rotation radiographs correlated best with the 3:00 position.
The crosstable lateral (in addition to frog lateral view) does not appear to provide additional information. We advocate the use of the frog lateral radiograph, instead of the crosstable radiograph, for several reasons. In our study, the frog lateral radiograph had the best specificity and positive predictive value of any radiographic view. Thus, the presence of deformity on the frog lateral radiograph will likely correlate with CT imaging. Similarly, hips without deformity on CT were not likely to show deformity on the frog lateral radiograph. The frog lateral view, in addition to the AP pelvis and 45° Dunn views, maximized sensitivity to severe cam deformity. Additionally, in our clinical experience, we have found that the frog lateral radiograph is more consistently reliable than the crosstable lateral radiograph [6]. This may be at least partially the result of the greater ease of positioning for this view. Radiation exposure in the crosstable lateral view is increased relative to the frog lateral view. At our institution, the calculated radiation exposure from the AP pelvis, Dunn, frog lateral, and crosstable lateral were 0.24, 0.12, 0.12, and 0.89 mSv, respectively [10]. The radiation exposure of the crosstable view is nearly double the other three views combined. Both views have limitations in clinical use, including difficult visualization of bony contours as a result of improper penetration for the crosstable lateral view and overlap of the greater trochanter with the head-neck junction for the frog lateral view. Therefore, we recommend the frog lateral radiograph for characterization of the 3:00 position.
Although the 45° Dunn view was highly sensitive to deformity at any location, it was very poorly specific. Seven hips had evidence of deformity on the Dunn view but not on any CT reformat. The mean alpha angle on the Dunn view was more than 5° greater than that of any other radiograph. If the presence of deformity on CT or radiograph is used as the gold standard, the Dunn view is actually more sensitive (93%) than CT (75%) for the detection of deformity. The reason for this is somewhat unclear. The Dunn view may detect subtle deformity at the 1:30 position that was not seen at the 1:00 or 2:00 positions. However, six of the seven hips with this discrepancy had an alpha angle between 50° and 55°, suggesting it may be a result of creation of a dichotomous variable.
Radiographic evaluation of the young adult hip with the AP pelvis, 45° Dunn, and frog lateral radiographs accurately characterizes deformity of cam-type FAI. This three-view series is diagnostic for most patients without the need additional radiation exposure from crosstable radiographs or three-dimensional imaging/CT. The AP pelvis, 45° Dunn, and frog lateral views best characterize the superior, anterosuperior, and anterior positions on the femoral head-neck junction, respectively.
References
Barton C, Salineros MJ, Rakhra KS, Beaule PE. Validity of the alpha angle measurement on plain radiographs in the evaluation of cam-type femoroacetabular impingement. Clin Orthop Relat Res. 2010;469:464–469.
Beaule PE, Zaragoza E, Motamedi K, Copelan N, Dorey FJ. Three-dimensional computed tomography of the hip in the assessment of femoroacetabular impingement. J Orthop Res. 2005;23:1286–1292.
Bedi A, Zaltz I, De La Torre K, Kelly BT. Radiographic comparison of surgical hip dislocation and hip arthroscopy for treatment of cam deformity in femoroacetabular impingement. Am J Sports Med. 2011;39(Suppl):20S–28S.
Carlisle JC, Zebala LP, Shia DS, Hunt D, Morgan PM, Prather H, Wright RW, Steger-May K, Clohisy JC. Reliability of various observers in determining common radiographic parameters of adult hip structural anatomy. Iowa Orthop J. 2011;31:52–58.
Clohisy JC, Carlisle JC, Beaule PE, Beaulé PE, Kim YJ, Trousdale RT, Sierra RJ, Leunig M, Schoenecker PL, Millis MB. A systematic approach to the plain radiographic evaluation of the young adult hip. J Bone Joint Surg Am. 2008;90(Suppl 4):47–66.
Clohisy JC, Nunley RM, Otto RJ, Schoenecker PL. The frog-leg lateral radiograph accurately visualized hip cam impingement abnormalities. Clin Orthop Relat Res. 2007;462:115–121.
Domayer SE, Ziebarth K, Chan J, Bixby S, Mamisch TC, Kim YJ. Femoroacetabular cam-type impingement: Diagnostic sensitivity and specificity of radiographic views compared to radial MRI. Eur J Radiol. 2011;80:805–810.
Dudda M, Albers C, Mamisch TC, Werlen S, Beck M. Do normal radiographs exclude asphericity of the femoral head-neck junction? Clin Orthop Relat Res. 2009;467:651–659.
Heyworth BE, Shindle MK, Voos JE, Rudzki JR, Kelly BT. Radiologic and intraoperative findings in revision hip arthroscopy. Arthroscopy. 2007;23:1295–1302.
Huda W, Gkanatsios NA. Effective dose and energy imparted in diagnostic radiology. Med Phys. 1997;24:1311–1316.
Hui AJ, McCalden RW, Martell JM, MacDonald SJ, Bourne RB, Rorabeck CH. Validation of two and three-dimensional radiographic techniques for measuring polyethylene wear after total hip arthroplasty. J Bone Joint Surg Am. 2003;85:505–511.
Johnston TL, Schenker ML, Briggs KK, Philippon MJ. Relationship between offset angle alpha and hip chondral injury in femoroacetabular impingement. Arthroscopy. 2008;24:669–675.
Konan S, Rayan F, Haddad FS. Is the frog lateral plain radiograph a reliable predictor of the alpha angle in femoroacetabular impingement? J Bone Joint Surg Br. 2010;92:47–50.
Kraay MJ, Moore RD, Martell JM, Rimnac CM. Reassessment of computerized wear measurement for total hip arthroplasty with correction for projectional image distortion: a brief follow-up report. J Bone Joint Surg Am. 2010;92:1858–1867.
Martell JM, Berdia S. Determination of polyethylene wear in total hip replacements with use of digital radiographs. J Bone Joint Surg Am. 1997;79:1635–1641.
Mast NH, Impellizzeri F, Keller S, Leunig M. Reliability and agreement of measures used in radiographic evaluation of the adult hip. Clin Orthop Relat Res. 2011;469;188–199.
Meyer DC, Beck M, Ellis T, Ganz R, Leunig M. Comparison of six radiographic projections to assess femoral head/neck asphericity. Clin Orthop Relat Res. 2006;445:181–185.
Mofidi A, Shields JS, Tan JS, Poehling GG, Stubbs AJ. Use of intraoperative computed tomography scanning in determining the magnitude of arthroscopic osteochondroplasty. Arthroscopy. 2011;27:1005–1013.
Nepple JJ, Brophy RH, Matava MJ, Wright RW, Clohisy JC. Radiographic findings of femoroacetabular impingement nfl combine athletes undergoing radiographs for previous hip or groin pain. Arthroscopy. 2012 Jun 13 [Epub ahead of print].
Nepple JJ, Carlisle JC, Nunley RM, Clohisy JC. Clinical and radiographic predictors of intra-articular hip disease in arthroscopy. Am J Sports Med. 2011;39:296–303.
Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002;84:556–560.
Pfirrmann CW, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J. Cam and pincer femoroacetabular impingement: characteristic MR arthrographic findings in 50 patients. Radiology. 2006;240:778–785.
Philippon MJ, Schenker ML, Briggs KK, Kuppersmith DA, Maxwell RB, Stubbs AJ. Revision hip arthroscopy. Am J Sports Med. 2007;35:1918–1921.
Pollard TC, Villar RN, Norton MR, Fern ED, Williams MR, Simpson DJ, Murray DW, Carr AJ. Femoroacetabular impingement and classification of the cam deformity: the reference interval in normal hips. Acta Orthop. 2010;81:134–141.
Rakhra KS, Sheikh AM, Allen D, Beaule PE. Comparison of MRI alpha angle measurement planes in femoroacetabular impingement. Clin Orthop Relat Res. 2009;467:660–665.
Acknowledgments
We thank Karen Steger-May for assistance with statistical analyses as well as Dr Daniel Wessel and Tim Keys for assistance in determining radiation exposure.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
ANCHOR Study Group: J. C. Clohisy, H. S. Hosalkar, Y.-J. Kim, J. M. Martel, M. B. Millis, J. J. Nepple, D. Podeszwa, D. Sucato, E. Sink, I. Zaltz
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
All investigations were conducted in conformity with ethical principles of research and informed consent for participation in the study was obtained.
This work was performed at Washington University School of Medicine, St Louis, MO, USA, and various centers of the ANCHOR Study Group.
About this article
Cite this article
Nepple, J.J., Martel, J.M., Kim, YJ. et al. Do Plain Radiographs Correlate With CT for Imaging of Cam-type Femoroacetabular Impingement?. Clin Orthop Relat Res 470, 3313–3320 (2012). https://doi.org/10.1007/s11999-012-2510-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2510-5