
Abstract
Insufficient femoral head-neck offset is common in femoroacetabular impingement (FAI) and reflected by the alpha angle, a validated measurement for quantifying this anatomic deformity in patients with FAI. We compared the alpha angle determined on magnetic resonance imaging (MRI) oblique axial plane images with the maximal alpha angle value obtained using radial images. The MRIs of 41 subjects with clinically suspected FAI were reviewed and alpha angle measurements were performed on both oblique axial plane images parallel to the long axis of the femoral neck and radial images obtained using the center of the femoral neck as the axis of rotation. The mean oblique axial plane and mean maximal radial alpha angle values were 53.4° and 70.5°, respectively. In 54% of subjects, the alpha angle was less than 55° on the conventional oblique axial plane image but 55° or greater on the radial plane images. Radial images yielded higher alpha angle values than oblique axial images. Patients with clinically suspected FAI may have a substantial contour abnormality that can be underestimated or missed if only oblique axial plane images are reviewed. Radial plane imaging should be considered in the MRI investigation of FAI.
Level of Evidence: Level III, diagnostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Femoroacetabular impingement (FAI) has become a well-recognized pathogenic factor in the evolution of hip osteoarthritis [2–5]. The impingement is secondary to an anatomic abnormality of the femoral head-neck junction and/or the acetabulum. In the pure cam form of FAI, the abnormality is an excess of bone and/or cartilage bulk at the anterosuperior femoral head-neck junction, resulting in reduced offset of the femoral head over the neck and femoral head asphericity. In the pure pincer form of FAI, impingement is the result of overcoverage of the femoral head by the acetabulum [2, 4, 5]. However, many FAI cases are mixed cam and pincer with varying degrees of both morphologic abnormalities [2]. Thus, a large proportion of patients with FAI will have a contour abnormality at the femoral head-neck junction making it imperative to evaluate this region.
Along with clinical history and physical examination, radiologic studies are essential for the diagnosis of FAI. Radiography [2, 8, 12], computed tomography [1], and magnetic resonance imaging (MRI) [5–7, 9, 10] are validated modalities for imaging the hip in the setting of FAI. MRI is an especially valuable modality given its multiplanar image acquisition capability. Images in the standard, oblique, and radial planes can be directly acquired or secondarily constructed by software reformations. It also offers the advantage of exquisite contrast resolution allowing for distinction and characterization of the labrum, cartilage, joint space, compact and cancellous bone, and regional soft tissues. These properties of MRI facilitate the evaluation of the femoral head-neck junction contour.
The alpha angle is a parameter used to quantify the degree of femoral deformity and reflects the insufficient anterolateral head-neck offset and femoral head asphericity [7, 9]. Prior MRI studies suggest an elevated alpha angle is associated with symptomatic impingement [1, 7, 9, 10]. The oblique axial plane parallel to the long axis of the femoral neck is the most frequently used imaging plane to evaluate the femoral head-neck junction. This plane optimally images the anterior contour of the femoral head-neck junction. However, several recent studies have reported that although the diminished offset is present anteriorly, it is most pronounced anterosuperiorly and potentially at any location within the anterosuperior quadrant [10, 11]. Thus, radial images have been recommended as a method for evaluating the femoral head-neck junction over its full circumference as opposed to just anteriorly as occurs using the more conventional oblique axial plane method [1, 4, 5, 10, 11].
The goals of this study were to: (1) compare the alpha angle value measured using oblique axial plane images with the maximal alpha value obtained using radial images in patients with clinically suspected FAI; (2) identify the location in which the maximal alpha angle occurred; and (3) determine any differences in the alpha angle values between various positions along the femoral head-neck junction in the anterosuperior quadrant.
Materials and Methods
We retrospectively examined the MRI image data of all 41 patients who underwent magnetic resonance arthrography (MRA) of the hip for FAI between June 1, 2006, and December 31, 2007. The patients had FAI clinically suspected on the basis of combined history, physical examination, and radiographs and were referred for MRI from a specialized orthopaedic hip practice (PB). The study included 18 men and 23 women (age range, 17–60 years; mean, 39 ± 11 years). There were 25 right and 16 left hips. The study was approved by the Ottawa Hospital Research Ethics Board.
The required sample size for this study was determined using PASS 2002 (Kaysville, UT) based on data from an original study measuring the alpha angle in femoroacetabular impingement [9]. In an equivalence test of means using two one-sided tests on data from a two-period crossover design, a sample size of 35 would achieve 99% power at a 5% one-sided significance level using the reference alpha angle mean in patients with FAI of 74° and standard deviation of 5.4°, and the range of the difference between these means that still results in the conclusion of equivalence is −5% to 5% of the reference mean. To account for possible differences between the previous and current study populations, this minimum required sample size was exceeded slightly to increase the accuracy of results.
As per the routine MRA protocol for the investigation of FAI, each hip was injected with 10 to 15 mL of a dilute (2 mmol) gadolinium-saline solution (Omniscan; GE Healthcare, Princeton, NJ) under fluoroscopic guidance by a musculoskeletal fellow or radiologist. The MRI scan was initiated within 30 minutes of the injection. MRA is the standard test used at our institution for the investigation of FAI to increase sensitivity for detection of associated labral and chondral injury. However, even nonarthrographic MRI protocols would give sufficient contrast and spatial resolution such that the contour of the femoral head-neck junction could be easily determined. The examinations were carried out on a 1.5-T scanner (Symphony Quantum; Siemens, Erlangen, Germany) with a flexible surface coil. All subjects underwent the routine hip MRA protocol at our institution, which included a three-dimensional isotropic, T1-weighted spoiled gradient echo (MPRAGE/Turbo-FLASH) sequence with water excitation (25-cm field of view, 1-mm slice thickness, 256 × 256 matrix, TR/TE/flip angle = 1970 ms/7 ms/15°, 1 average).
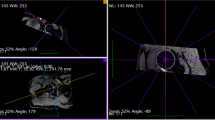
Multiplanar reformation (MPR) was carried out to generate 2-mm thick oblique axial and oblique sagittal plane images, parallel and perpendicular to, respectively, the long axis of the femoral neck. The latter plane was used to prescribe the radial MPR, using the center of the femoral neck as the axis of rotation, with 2-mm thick images generated at 15° intervals (Fig. 1A–C). As such, all radial MPR images were oriented orthogonal to the femoral head-neck junction. Acquisition and MPR images were sent to PACS (McKesson Horizon Rad Station 3.3, San Francisco, CA) for review.

Radial imaging shows (A) the axis of rotation is the center of the femoral neck (*) as demonstrated on an oblique sagittal image showing the femoral neck in cross-section/short axis. (B) Localizer image demonstrates superimposed radial reference lines at 15° intervals. A clockface nomenclature was implemented with the superior femoral head-neck junction denoted as 12 o’clock. Subsequent rotation of the axis generated images around the circumference of the femoral neck going from superior to anterior, from 12 o’clock to 3 o’clock. (C) Radial image optimally demonstrating the femoral head-neck contour (*) at the 2 o’clock vector is shown.
We selected specific images on which to measure the alpha angle. A clockface nomenclature was adopted for localization around the femoral head-neck junction with the anterior and superior locations designated 3 o’clock and 12 o’clock, respectively. From the oblique axial MPR series, the image through the middle of the neck was chosen; it would demonstrate the anterior-most region of the femoral head-neck junction (3 o’clock). From the radial MPR series, four images corresponding to the 12, 1, 2, and 3 o’clock positions were chosen, thus evaluating the anterosuperior quadrant of the femoral head-neck junction going from superior to anterior. In effect, the oblique axial image and the radial plane image at 3 o’clock evaluated the exact same location. The alpha angles were measured by two fellowship-trained musculoskeletal radiologists (KR, AS) working together in consensus using a previously published method [9] (Fig. 2). A best-fit circle was drawn around the perimeter of the femoral head. The first arm (1) of the angle was the long axis of the femoral neck, defined as the line drawn between the center of the femoral neck at its narrowest point and the center of the femoral head. The second arm (2) of the angle was drawn from the center of the femoral head anteriorly to the point where the head extends beyond the margin of the circle. The alpha angle formed provided a quantitative measurement of the degree of femoral head asphericity and/or lack of head-neck junction concavity. The alpha angle was measured using the same technique on both oblique axial and radial images. The readers were blinded to the originally issued MRI reports, radiographs, and to any clinical or surgical followup information. We determined the mean, minimum, and maximum alpha angle values along with the standard deviation for the oblique axial plane and for each of the four radial planes. For each subject, the maximal alpha angle value was noted. The minimum, maximum, and mean values for this maximal value were calculated for all subjects. Based on a previous study evaluating the alpha angle in symptomatic hips [9], our institution uses 55° as the threshold above which the alpha angle is considered abnormal. The number of subjects with an alpha angle less than 55° (contour normal) on the oblique axial plane image but 55° or greater (contour abnormal) on the radial plane image was recorded. Although several studies have documented cam impingement with lower alpha angles [1, 7], a higher cutoff of 55° was chosen to account for variability and measurement errors.

Measurement of the alpha angle (α) is shown. A best-fit circle is drawn over the femoral head. The alpha angle is formed by the axis of the femoral neck (1) and a line (2) drawn from the femoral head center to the point where the head extends beyond the margin of the best-fit circle (arrow).
The mean difference between the oblique axial and the maximal radial values was calculated and the difference determined using a two-tailed paired t test. A Kolmogorov-Smirnov one-sample test of normality was performed for both the oblique axial and maximal radial datasets, and the p values were 0.270 and 0.661, respectively. The mean difference between the maximal alpha angle of male and female patients was calculated and the difference also determined using a two-tailed paired t test. For each subject, the clockface vector at which the maximal radial plane alpha angle measurement occurred was noted. The frequency with which the maximal alpha angle occurred at each of the vectors was recorded. Analysis of variance (ANOVA) was used to evaluate differences between alpha angle values at the four radial clockface vectors. We used SPSS version 15.0.1 (SPSS, Inc, Chicago, IL) for all analyses.
Results
The mean alpha angle values, range, and standard deviation using the oblique axial and radial planes were determined (Table 1). Using the oblique axial plane, the mean alpha angle value was 53.4°. Considering the maximal radial alpha angle measurement for each subject, regardless of vector location, the mean maximum alpha angle value was 70.5° (Table 2). The maximal radial alpha angle values were greater (p < 0.001) than the oblique axial alpha angle values with the mean difference being 17.1°. The oblique axial and radial images of a subject had differing alpha angle values (Fig. 3). The mean maximal alpha angles of men and women were similar (p = 0.12), being 67.9° and 73.3°, respectively.

MRI arthrogram images of a 41-year-old woman with hip and groin pain with reduced internal rotation and positive impingement sign show (A) standard oblique axial plane image through the middle of the femoral neck demonstrates normal anterior (3 o’clock) concavity and offset at the femoral head-neck junction with an alpha angle of 42°. (B) Radial plane image (2 o’clock) reveals lack of concavity and reduced head-neck offset with an alpha angle of 64°. (Solid white arrows localize the femoral head neck junction.)
The maximal alpha angle value occurred most frequently in the 2 o’clock vector (20 of 41 [49%]) (Table 3). The vast majority (37 of 41 [90%]) of the maximal alpha angle values occurred at either the 1 or 2 o’clock position.
The radial alpha angle values varied (p < 0.001) at the various clockface vectors of the anterosuperior quadrant of the head-neck junction. The mean alpha angle values were highest at the radial 1 and 2 o’clock vectors, being 64.7° and 65.9°, respectively. We observed differences between the oblique axial and the radial 1 o’clock (p < 0.001) and radial 2 o’clock (p < 0.001) values.
In 22 of 41 hips (54%), the alpha angle was less than 55° on the conventional oblique axial plane image (contour normal) but 55° or greater on the radial plane images (contour abnormal) (Fig. 1). These subjects had mean oblique axial and maximal radial alpha angle values of 47.4° and 68.6°, respectively.
Discussion
The alpha angle is a parameter used to quantify the contour abnormality of the femoral head-neck junction in FAI. Both oblique axial plane and radial images have been used in clinical and research settings to measure the alpha angle. However, to date, there has not been any study comparing the two different techniques in terms of potential variability in the alpha angle values. The goals of this study were to: (1) compare the alpha angle value measured using oblique axial plane images with the maximal alpha angle value obtained using radial images in patients with clinically suspected FAI; (2) identify the location in which the maximal alpha angle occurred; and (3) determine any differences in the alpha angle values between various positions along the femoral head-neck junction in the anterosuperior quadrant.
There are study limitations to be considered. All of the subjects referred for MRI were clinically suspected of having FAI. As such, there was a high pretest probability for the presence of a contour abnormality. No asymptomatic control subjects were included in this review. In the absence of a substantial anatomic deformity, it is unknown whether there would have been any difference between the oblique axial and radial plane alpha angle values. The implication is there may be a threshold beyond which, or perhaps only a certain range of femoral contours within which, the radial images are in fact substantially superior to the oblique axial plane images. The alpha angles were measured by two musculoskeletal radiologists by consensus. Independent and multiple readings would have allowed for determination of interobserver and intraobserver reliability. However, the presented alpha angle measurement technique reportedly has high inter- and intraobserver agreement [9].
Femoroacetabular impingement has become a well-recognized pathogenic factor in the evolution of hip osteoarthritis [2–5]. A lack of normal offset or concavity at the femoral head-neck junction is a frequent and surgically correctable anatomic abnormality in FAI. It renders the femoral head nonspherical and, subsequently, in conflict with the spherical acetabulum. The contour abnormality at the head-neck junction leads to reduced clearance for the femoral head and neck during joint movement. An impaired interaction between the femur and acetabulum causes mechanical and symptomatic limitations in the range of motion. The altered biomechanics result in injury to the chondrolabral complex, which may serve as an initiator in the pathway of hip osteoarthritis [2, 4]. Thus, it is imperative to evaluate the femoral head-neck junction in the radiologic investigation of FAI.
The conventional oblique axial plane can detect and allow quantification of the deformity through the alpha angle measurement. In this study, the oblique axial plane yielded mean alpha angle values lower than the radial plane images (53.4° versus 70.5°). This results from the fact that the oblique axial plane optimally evaluates the anterior region of the head-neck junction. Unfortunately, it suboptimally images the more superior aspect, which is where the contour abnormality is most pronounced [10, 11]. As the oblique axial plane extends superiorly, the surface of the head-neck junction is no longer orthogonal to the imaging plane as a result of the curvature of the femoral neck. As a result, the oblique axial plane underestimates and may even miss the deformity. In contrast, radial images are based on a rotating plane such that each image is orthogonal to the femoral surface and visualizes the head-neck junction in profile.
Two previous studies using the oblique axial MRI plane in patients with FAI reported average alpha angle measurements of 69.7° and 74.0° [7, 9]. These are higher than the value of 53.4° in the current project. An explanation for this difference is the variability in the location at which the alpha angles may have been drawn in previously published papers. In this study, the oblique axial image slice through the middle of the femoral neck was chosen because it could be easily determined and reproduced in all subjects. As well, it would allow for the optimal visualization of the anterior head-neck junction, 3 o’clock, where original papers assumed was the epicenter of the anatomic deformity. However, neither of the two studies explicitly stated whether the middle slice was selected. In fact, with protocols not using radial imaging, the oblique axial slice selected may be superior to the middle of the neck in an attempt to capture the area with the greatest degree of insufficient offset. This method would result in larger alpha angle measurements, but would not image the anterior 3 o’clock position exactly. As such, it may not be appropriate to directly compare the oblique axial alpha angle values between the current and previous studies.
We observed the maximal alpha angle in the anterosuperior region of the femoral head-neck junction from the 1 to 2 o’clock positions in 90% of subjects. The observation that the greatest degree of deformity and the largest alpha angle value occur anterosuperiorly but not anteriorly at 3 o’clock has also been made in prior studies involving radial MRI of the hip [10, 11].
Our finding that the alpha angle can vary at different locations within the anterosuperior quadrant of the femoral head-neck junction in patients with FAI has also been obtained in a previous study [10].
We found radial images identified a substantial proportion of subjects (54%) with a seemingly normal contour on oblique axial images who had in fact an abnormal contour. This may be clinically important when investigating hip pain in which FAI is in the differential diagnosis. Although the lack of concavity and head-neck junction offset alone may not be diagnostic of FAI, it may influence the physician’s impression in cases in which the history, physical examination, or radiographs are inconclusive. Furthermore, it may change the management plan from nonoperative to operative and determine whether any surgical treatment is arthroscopic versus open. The presence of the contour abnormality may also direct the radiologist and surgeon to search for other known associated pathologies such as labral tears and chondral lesions.
In the future, the radiologic detection of the femoral contour abnormality alone may not be sufficient for the surgical management of FAI. Given the advancement of minimally invasive and computer-assisted surgical techniques, preoperative mapping and quantification of the deformity will become increasingly important. Accurate imaging and postprocessing algorithms, sensitive to the complex geometries of the femur and pathologic osteochondral deformities, will be essential.
We present a simple MRI protocol readily performed on current commercial scanners. It allows for multiplanar reformations, including radial images and accurate measurement of the alpha angle. Our data support our belief that radial images are more sensitive to the presence and size of the anatomic deformity than conventional oblique axial images. Thus, we advocate that radial imaging be considered in the MRI investigation of FAI.
References
Beaulé P, Zaragoza E, Motamedi E, Copelan N, Dorey F. Three-dimensional computed tomography of the hip in the assessment of femoroacetabular impingement. J Orthop Res. 2005;23:1286–1292.
Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage. J Bone Joint Surg Br. 2005;87:1012–1018.
Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: an integrated mechanical concept. Clin Orthop Relat Res. 2008;466:264–272.
Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120.
Ito K, Minka KA, Leunig M, Werlen S, Ganz R. Femoroacetabular impingement and the cam-effect: a MRI-based quantitative anatomical study of the femoral head-neck offset. J Bone Joint Surg Br. 2001;83:171–176.
James SLJ, Ali K, Malara F, Young D, O’Donnell J, Connell DA. MRI findings of femoroacetabular impingement. AJR Am J Roentgenol. 2006;187:1412–1419.
Kassarjian A, Yoon LS, Belzile E, Connolly SA, Millis MB, Palmer WE. Triad of MR arthrographic findings in patients with cam-type femoroacetabular impingement. Radiology. 2005;236:588–592.
Meyer DC, Beck M, Ellis T, Ganz R, Leunig M. Comparison of six radiographic projections to assess femoral head/neck asphericity. Clin Orthop Relat Res. 2006;445:181–185.
Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002;84:556–560.
Pfirrmann CWA, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J. Cam and pincer Femoroacetabular impingement: characteristic MR arthrographic findings in 50 patients. Radiology. 2006;240:778–785.
Siebenrock KA, Wahab KHA, Werlen S, Kalhor M, Leunig M, Ganz R. Abnormal extension of the femoral head epiphysis as a cause of cam impingement. Clin Orthop Relat Res. 2004;418:54–60.
Tannast M, Sienbenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis—what the radiologist should know. AJR Am J Roentgenol. 2007;188:1540–1552.
Acknowledgments
We thank Anna Fazekas and Simon Dagenais for assistance in study design and statistical analysis and Natasha La Russa for postprocessing reformations of the MRI studies.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution has approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
About this article
Cite this article
Rakhra, K.S., Sheikh, A.M., Allen, D. et al. Comparison of MRI Alpha Angle Measurement Planes in Femoroacetabular Impingement. Clin Orthop Relat Res 467, 660–665 (2009). https://doi.org/10.1007/s11999-008-0627-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-008-0627-3