
Opinion statement
Cell therapy can be administered via injections delivered directly into the myocardium or as engineered cardiac tissue patches, which are the subject of this review. Engineered cardiac patches can be created from sheets of interconnected cells or by suspending the cells in a scaffold of material that is designed to mimic the native extracellular matrix. The sheet-based approach produces patches with well-aligned and electronically coupled cardiomyocytes, but cell-containing scaffolds are more readily vascularized by the host’s circulatory system and, consequently, are currently more suitable for applications that require a thicker patch. Cell patches can also be modified for the co-delivery of peptides that may promote cell survival and activate endogenous repair mechanisms; nevertheless, techniques for controlling inflammation, limiting apoptosis, and improving vascular growth need continue to be developed to make it a therapeutic modality for patients with myocardial infarction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although coronary interventions and associated medical therapies have improved care in patients with coronary artery disease, a significant portion of these patients still progress to end-stage heart failure [1]. To date, heart transplantation remains the only definitive therapy for restoring cardiac function in patients with end-stage heart failure. However, the availability of donor hearts is inadequate, and even when a suitable heart can be obtained, the patient’s lifespan is typically extended by just ~10 years [2]. Thus, therapies that can effectively limit adverse cardiac remodeling and regenerate or replace myocardial tissues that are lost to an ischemic event are urgently needed.
Tissue engineering was first introduced as a method for rebuilding organs in the early 1990s [3], and the first investigations of engineered myocardial tissues began around the start of the new millennium [4–10]. The benefits associated with the transplantation of tissue-engineered cardiac patches have been observed in both small- and large-animal models of myocardial injury [8, 10], and the effectiveness of this therapeutic approach will continue to improve as researchers seek to identify the optimal combination of cell types and to refine the methods used for patch creation and delivery. In this review, we summarize the progress in cardiac patch engineering by focusing on recent discoveries that may influence decisions on cell selection and on other components and techniques used to manufacture engineered cardiac patches for the treatment of myocardial disease.
Cell types
The human heart contains billions of cells of multiple lineages [11]; thus, effective methods for generating an engineered cardiac patch will require access to suitably large and pure populations of at least three distinct cell types: endothelial cells (ECs), smooth muscle cells (SMCs), and cardiomyocytes (CMs). Human-induced pluripotent stem cells (hiPSCs) are perhaps the most promising source of cells for patch creation because they can self-replicate an unlimited number of times, can differentiate into cells of any lineage, and can be created from each individual patient’s own somatic cells, thereby minimizing the immune/inflammatory response to implantation. However, their capacity for self-replication and differentiation can also lead to tumor formation and, consequently, hiPSCs need to be pre-differentiated before administration. Protocols for differentiating hiPSCs into SMCs are well-established [12•], and effective methods for generating ECs and CMs from hiPSCs (i.e., hiPSC-ECs and hiPSC-CMs, respectively) have recently been introduced.
Differentiating hiPSCs into endothelial cells
The most common methods used to generate ECs from hiPSCs (or human embryonic stem cells [hESCs]) have been based on co-culturing with murine stromal cells [13, 14] or the formation of embryoid bodies (EB) [15, 16] and typically involve growing the cells in a two-dimensional layer. However, the co-culture method can leave a small number of murine cells in the hiPSC-EC population [14, 15], while the efficiency of the EB protocol (i.e., the proportion of hiPSCs or hESCs that acquire an EC-like phenotype) is just 15 % [14–16]. Recent work suggests that the differentiation efficiency can be increased to ~44 % via a two-stage protocol performed with hiPSCs that are suspended in a three-dimensional fibrin scaffold [17]. In stage 1, the hiPSCs were cultured with activin A and BMP-4, which have been shown to direct hiPSCs toward the mesodermal lineage [18]; then, in stage 2, the cells were cultured with vascular endothelial growth factor (VEGF) [19], transforming growth factor β1 (TGFβ1) [20], and erythropoietin (EPO) [21], which are known to participate in hESC-EC differentiation or in the differentiation of endothelial progenitor cells. After purification to >95 % (based on expression of the EC marker CD31), the EC phenotype remained stable for 4 weeks, which is approximately 2 weeks longer than has been achieved with other methods [14, 15], and engineered cardiac patches created from the hiPSC-ECs, hiPSC-derived CMs, and smooth muscle cells began to contract just 3 days after synthesis, compared to 7 days afterward for patches that were created without hiPSC-ECs.
Differentiating hiPSCs into cardiomyocytes
Embryonic or induced pluripotent stem cells were first differentiated into CMs by culturing them with endodermal cells [22], but the efficiency of the differentiation protocol can be increased by culturing the cells as monolayers or embryoid bodies. Like hiPSC-EC differentiation, the differentiation of hiPSC-CMs begins by committing the cells to the mesodermal lineage with factors such as BMP4, activin A, and/or WNT3A [23, 24]; then, the cells are directed toward a cardiac lineage via the addition of BMP inhibitors and/or Wnt inhibitors such as Noggin and DKK1 [25, 26]. However, when hESC-CMs were obtained and purified via EB formation and Percoll separation, only 35–66 % of the isolated cells expressed slow myosin heavy chain or cardiac troponin T [27], which suggests that the population may have contained a substantial number of residual partially differentiated cells. When differentiated via the sandwich method [28•] and isolated via micro-dissection and preplating, the purity was as high as 93 % [12•, 18].
Methods of patch creation
In general, engineered cardiac patches can be classified into one of two categories, cell sheets or cell-containing scaffolds, both of which are summarized below.
Cell sheets
Cell sheets are created by culturing cells on dishes until confluent, and if the dish is coated with a temperature-sensitive polymer, poly(N-isopropylacrylamide) (PIPAAm) [29], the sheets can be released intact by reducing the culture temperature from 37 to 32 °C, thereby preserving the extracellular matrix, the cells’ alignment, and intercellular connections, including the gap junctions necessary for electronic signal transduction between neighboring CMs [30]. Individual sheets can be stacked to form three-dimensional engineered cardiac grafts [4], and the CMs in adjacent layers can become fully electrically coupled within 1 h of layering [31]. However, grafts constructed with four or more layers resist vascularization, and vascularization can also be impeded by the epicardium after the sheet is applied to the surface of the heart.
Techniques for producing adequately large and pure populations of hiPSC-CMs were unavailable until recently, so studies performed with hiPSC-CM sheets are relatively rare [10, 32]. Nevertheless, hiPSC-CM sheets have been shown to beat spontaneously [33], conduct action potentials [34], and become electronically coupled when layered [35, 36], and are associated with improvements in cardiac function, vascularity, and fibrosis [37]. After transplantation, the contractile activity of CM sheets is expected to contribute directly to myocardial performance. However, the transplanted sheet may remain electronically isolated from the native myocardium; if so, any observed improvements are likely to have evolved primarily through the release of cytokines that promote angiogenesis, activate endogenous progenitor cells [38, 39•], or stimulate other beneficial paracrine pathways.
Because inadequate perfusion is the primary cause of attrition in transplanted cells [40], researchers have attempted to improve the vascularity of CM sheets by adding other cell types [41, 42]. The inclusion of human umbilical vein endothelial cells (HUVECs) and primary human bone marrow stromal cells significantly increased the vascularity of cultured hESC-CM sheets [42], and the stromal cells also produced an abundance of matrix components, including fibrillar collagen, hyaluronan, and versican. Sheets composed of hESC-CMs, ECs (HUVECs or hESC-derived ECs), and mouse embryonic fibroblasts also formed vascular networks in culture, and after the sheets were transplanted into rats, the preformed vessels integrated with the host animal’s circulation and the engrafted sheets were approximately tenfold larger than the grafts of sheets created from hESC-CMs alone [41].
Studies with skeletal myocytes (SkMs) suggest that vascularization can also be induced in multilayered, CM sheet patches by sandwiching ECs between the sheets. Patches composed of human SkMs and HUVECs were penetrated by capillary-like structures in vitro, and the preformed endothelial network became connected to the host animal’s circulation after subcutaneous transplantation into nude rats [40]. SkM sheets have also been prevascularized by wrapping them with omentum [43]; in porcine [44] and rodent [40] MI models, measurements of vascularity, cell survival, cardiac function, and infarct size improved significantly when SkM sheets were wrapped and cultured with omentum before transplantation.
Collectively, these observations suggest that patches composed of CM sheets need to contain supporting cells for optimal vascularity and perfusion. However, capillary density was significantly better in mice transplanted with patches containing ESC-derived CMs, ECs, and vascular mural cells than when the ESC-derived CMs were omitted; thus, CMs also appear to contribute to vascular growth. Cardiac functional parameters were also significantly better in animals treated with patches containing all three cell types [38].
Scaffolds and decellularized tissues
Scaffold-based engineered cardiac patches are created by suspending cells in a matrix of biomaterial, and because the matrix is less resistant than sheets to infiltration by the vascular network of the native myocardium, patches made with this technique are generally more suitable for applications that require thicker engineered cardiac patches. The matrix of the scaffold is usually composed of naturally occurring biomaterials such as collagen and fibrin [45], but can also be created from synthetic polymers [46–49], and the scaffold can be modified for delivery of growth factors and other cytokines that may further improve angiogenesis, impede apoptosis, and activate endogenous repair mechanisms. However, scaffolds do not produce patches with well-aligned CMs, and the scaffold material may interfere with electronic signal transduction. Thus, a number of strategies, including electrical field stimulation [50] and chronic mechanical stretching [51, 52], have been used to promote cell alignment and the synchronization of contractile activity.
Collagen
Collagen is the most prevalent extracellular component of the myocardium and can be molded into a variety of shapes. The first mammalian engineered cardiac patch was created by suspending neonatal rat heart cells in a collagen scaffold [53], and patches composed of collagen, ECs, stromal cells, and hESC-CMs or hiPSC-CMs contained vascular structures of human origin and were perfused by the host circulation just 1 week after transplantation onto uninjured rat hearts [54]. Collagen has also been combined with Matrigel and neonatal rat CMs to form rings of engineered cardiac tissue that were maintained with phasic mechanical stretching. The rings can be cut to form strips of engineered cardiac tissue [51, 55], which survived, matured, and continued to beat after transplantation into healthy hearts [5], or left intact to generate more complex structures; for example, the rings can be stacked to form asterisk-shaped patches, which improved contractile function in a rat MI model [8], or fused on edge to create pouches of cardiac tissue, which may be used to encase and support the function of failing hearts [56].
Fibrinogen/fibrin
In response to wounding, individual monomers of fibrinogen are converted to fibrin by exposure to thrombin; then, the fibrin molecules cross-link to form an insoluble mesh that traps blood cells to form a clot. Thus, fibrin scaffolds can be incorporated into engineered cardiac patches by mixing a cell-containing solution of fibrinogen with thrombin, and because the mixture typically solidifies in less than 1 min, the patch can be created in situ by injecting the two solutions into a mold placed over the infarct site. This method has been used to deliver hESC-derived smooth muscle cells and endothelial cells to the infarcted hearts of both swine and mice [10, 39, 57•]; the treatment was associated with improvements in myocardial function, perfusion, energy metabolism, left ventricular wall stress, and remodeling [58]. Fibrin scaffolds can also be modified with polyethylene glycol (i.e., PEGylated) and used to deliver growth factors and other beneficial proteins [59].
Therapeutic benefits and mechanisms of action
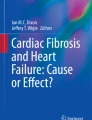
After a patient recovers from an acute infarct event, myocardial tissue in the injured region of the compensated heart may have been replaced by a thin, fibrotic scar, which bulges during systole and increases wall stress in the surrounding tissues. This increase in wall stress is believed to trigger metabolic changes in nearby cells, such as declines in the ATP turnover rate and in the ratio of phosphocreatine to ATP (i.e., the PCr/ATP ratio) [57•, 60–62], which cause the region of dysfunction and adverse cardiac remodeling to grow and encompass a progressively larger proportion of myocardial tissue. Thus, the additional thickness and rigidity provided by an engineered cardiac patch may improve myocardial performance or impede disease progression by preventing the infarct from bulging, which could explain, at least in part, why implanted patches have been associated with improvements in infarct size, even when the patches did not contain CMs [63]. However, the CM-free patches did not improve myocardial function, whereas measurements of left ventricular ejection fraction and fractional shortening in rats that were treated with CM-containing patches were similar to measurements in sham-operated animals [63]. Furthermore, transplanted hiPSC-ECs and hiPSC-SMCs, when administered via an in situ fibrin patch over the site of infarction in swine hearts, were associated with improvements in indices of cellular ATP metabolism, wall stress, infarct size, and contractile function at the border of the infarction, and the transplanted cells also secreted cytokines that promote vascular growth, impede apoptosis, and induce cell migration (Fig. 1) [12•]. Thus, much of the benefit associated with an implanted engineered cardiac patch may evolve from the structural support of the patch or from the cytokines produced by the transplanted cells, rather than from direct remuscularization of the injured region.

The working hypothesis of the mechanism of action using a cardiac patch. A circular, three-dimensional, porous, biodegradable engineered cardiac patch (blue) can be created over the infarcted region by mixing thrombin and fibrinogen solutions containing a variety of cell types, including adult stem/progenitor cells (e.g., mesenchymal stem cells, endothelial progenitor cells), hESC- or hiPSC-derived cardiomyocytes and vascular cells, or combinations of multiple cell types. The fibrinogen can also be modified to bind peptides that guide differentiation, impede apoptosis, or promote other beneficial paracrine mechanisms. After mixing, the solution typically solidifies in less than 1 min, forming a semi-solid matrix that not only serves as a delivery vehicle for the transplanted cells but may also increase the cell engraftment rate and provide structural support for the weakened myocardium that is exposed to myocardial infarction or ischemia reperfusion, while the transplanted cells release growth factors and other cytokines that reduce apoptosis, promote angiogenesis, and activate endogenous mechanisms for cardiomyocyte renewal. Furthermore, perhaps by reducing LV wall stress and bulging at the site of the infarction, the in vivo measurements of myocardial bioenergetics and the ATP hydrolysis rate (via [31] P magnetization-saturation transfer) suggest that the patch also protects against adverse changes in myocardial energy metabolism. Collectively, these benefits may reduce infarct size; improve myocardial perfusion, metabolism, and contractile function; and consequently impede the progression of LV dilatation (panels b and k courtesy of Xiong Q et al. [39]; panels f, g, i, j, and l courtesy of Xiong Q et al. [57]).
Conclusion
The beneficial effects of engineered cardiac patches have been clearly demonstrated in animal models, and their clinical feasibility is supported by the successful transplantation of sheets of skeletal myoblasts [64] and of collagen sponges that contained bone marrow cells [65, 66] in patients. hiPSCs are perhaps a promising source of cells for patch creation because their capacity for self-renewal and differentiation is (theoretically) unlimited, and they can be created from each individual patient’s own somatic cells, thereby minimizing the immune/inflammatory response to implantation. Effective methods for differentiating hiPSCs into SMCs, ECs, and CMs are now available, and techniques for creating engineered cardiac patches from sheets of hiPSC-derived cells or by suspending the cells in a biocompatible scaffold continue to be refined. Cell sheet technology produces patches with well-aligned and electronically coupled CMs, but grafts composed of more than three sheets resist vascularization, so scaffold-based approaches are currently more suitable for applications that require thicker patches. Regardless of the technique used for patch manufacture, strategies for controlling inflammation and improving vascular growth will be needed to optimize this therapeutic approach.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance
Weir RA, McMurray JJ. Epidemiology of heart failure and left ventricular dysfunction after acute myocardial infarction. Curr Heart Failure Rep. 2006;3:175–80.
Lund LH, Edwards LB, Kucheryavaya AY, Dipchand AI, Benden C, Christie JD, et al. The registry of the international society for heart and lung transplantation: thirtieth official adult heart transplant report—2013; focus theme: age. J Heart Lung Transplant. 2013;32:951.
Langer R, Vacanti JP. Tissue engineering. Science. 1993;260:920–6.
Shimizu T, Yamato M, Isoi Y, Akutsu T, Setomaru T, Abe K, et al. Fabrication of pulsatile cardiac tissue grafts using a novel 3-dimensional cell sheet manipulation technique and temperature-responsive cell culture surfaces. Circ Res. 2002;90:e40.
Zimmermann WH, Didie M, Wasmeier GH, Nixdorff U, Hess A, Melnychenko I, et al. Cardiac grafting of engineered heart tissue in syngenic rats. Circulation. 2002;106:I151–7.
Li RK, Jia ZQ, Weisel RD, Mickle DA, Choi A, Yau TM. Survival and function of bioengineered cardiac grafts. Circulation. 1999;100:II63–9.
Leor J, Aboulafia-Etzion S, Dar A, Shapiro L, Barbash IM, Battler A, et al. Bioengineered cardiac grafts: a new approach to repair the infarcted myocardium? Circulation. 2000;102:III56–61.
Zimmermann WH, Melnychenko I, Wasmeier G, Didie M, Naito H, Nixdorff U, et al. Engineered heart tissue grafts improve systolic and diastolic function in infarcted rat hearts. Nat Med. 2006;12:452–8.
Miyahara Y, Nagaya N, Kataoka M, Yanagawa B, Tanaka K, Hao H, et al. Monolayered mesenchymal stem cells repair scarred myocardium after myocardial infarction. Nat Med. 2006;12:459–65.
Kawamura M, Miyagawa S, Miki K, Saito A, Fukushima S, Higuchi T, et al. Feasibility, safety, and therapeutic efficacy of human induced pluripotent stem cell-derived cardiomyocyte sheets in a porcine ischemic cardiomyopathy model. Circulation. 2012;126:S29–37.
Olivetti G, Cigola E, Maestri R, Corradi D, Lagrasta C, Gambert SR, et al. Aging, cardiac hypertrophy and ischemic cardiomyopathy do not affect the proportion of mononucleated and multinucleated myocytes in the human heart. J Mol Cell Cardiol. 1996;28:1463–77.
Ye L, Chang YH, Xiong Q, Zhang P, Zhang L, Somasundaram P, et al. Cardiac repair in a porcine model of acute myocardial infarction with human induced pluripotent stem cell-derived cardiovascular cells. Cell Stem Cell. 2014;15:750–61. 1) Human iPSCs (hiPSCs) were differentiated into three cardiac lineages: myocytes, endothelial cells and smooth muscle cells; 2) hiPSC-derived cells were transplanted into a porcine model of myocardial infarction, and 3) Engraftment in combination with IGF-1-fibrin patch improves cardiac function.
Woll PS, Morris JK, Painschab MS, Marcus RK, Kohn AD, Biechele TL, et al. Wnt signaling promotes hematoendothelial cell development from human embryonic stem cells. Blood. 2008;111:122–31.
Choi KD, Yu J, Smuga-Otto K, Salvagiotto G, Rehrauer W, Vodyanik M, et al. Hematopoietic and endothelial differentiation of human induced pluripotent stem cells. Stem Cells. 2009;27:559–67.
Li Z, Hu S, Ghosh Z, Han Z, Wu JC. Functional characterization and expression profiling of human induced pluripotent stem cell- and embryonic stem cell-derived endothelial cells. Stem Cells Dev. 2011;20:1701–10.
Rufaihah AJ, Huang NF, Jame S, Lee JC, Nguyen HN, Byers B, et al. Endothelial cells derived from human iPSCS increase capillary density and improve perfusion in a mouse model of peripheral arterial disease. Arterioscler Thromb Vasc Biol. 2011;31:e72–9.
Zhang S, Dutton JR, Su L, Zhang J, Ye L. The influence of a spatiotemporal 3D environment on endothelial cell differentiation of human induced pluripotent stem cells. Biomaterials. 2014;35:3786–93.
Ye L, Zhang S, Greder L, Dutton J, Keirstead SA, Lepley M, et al. Effective cardiac myocyte differentiation of human induced pluripotent stem cells requires VEGF. PLoS ONE. 2013;8, e53764.
Yamashita J, Itoh H, Hirashima M, Ogawa M, Nishikawa S, Yurugi T, et al. Flk1-positive cells derived from embryonic stem cells serve as vascular progenitors. Nature. 2000;408:92–6.
Gualandris A, Annes JP, Arese M, Noguera I, Jurukovski V, Rifkin DB. The latent transforming growth factor-beta-binding protein-1 promotes in vitro differentiation of embryonic stem cells into endothelium. Mol Biol Cell. 2000;11:4295–308.
Bahlmann FH, DeGroot K, Duckert T, Niemczyk E, Bahlmann E, Boehm SM, et al. Endothelial progenitor cell proliferation and differentiation is regulated by erythropoietin. Kidney Int. 2003;64:1648–52.
Mummery CL, Zhang J, Ng ES, Elliott DA, Elefanty AG, Kamp TJ. Differentiation of human embryonic stem cells and induced pluripotent stem cells to cardiomyocytes: a methods overview. Circ Res. 2012;111:344–58.
Paige SL, Osugi T, Afanasiev OK, Pabon L, Reinecke H, Murry CE. Endogenous Wnt/beta-catenin signaling is required for cardiac differentiation in human embryonic stem cells. PLoS ONE. 2010;5:e11134.
Kattman SJ, Witty AD, Gagliardi M, Dubois NC, Niapour M, Hotta A, et al. Stage-specific optimization of activin/nodal and BMP signaling promotes cardiac differentiation of mouse and human pluripotent stem cell lines. Cell Stem Cell. 2011;8:228–40.
Yuasa S, Itabashi Y, Koshimizu U, Tanaka T, Sugimura K, Kinoshita M, et al. Transient inhibition of BMP signaling by noggin induces cardiomyocyte differentiation of mouse embryonic stem cells. Nat Biotechnol. 2005;23:607–11.
Yang L, Soonpaa MH, Adler ED, Roepke TK, Kattman SJ, Kennedy M, et al. Human cardiovascular progenitor cells develop from a KDR embryonic-stem-cell-derived population. Nature. 2008;453:524–8.
Xu C, Police S, Hassanipour M, Gold JD. Cardiac bodies: a novel culture method for enrichment of cardiomyocytes derived from human embryonic stem cells. Stem Cells Dev. 2006;15:631–9.
Zhang J, Klos M, Wilson GF, Herman AM, Lian X, Raval KK, et al. Extracellular matrix promotes highly efficient cardiac differentiation of human pluripotent stem cells: the matrix sandwich method. Circ Res. 2012;111:1125–36. The first report that since changed the efficiency of the efficiency in differentiation of pluripotent stem cells to cardiomyocytes.
Okano T, Yamada N, Sakai H, Sakurai Y. A novel recovery system for cultured cells using plasma-treated polystyrene dishes grafted with poly(N-isopropylacrylamide). J Biomed Mater Res. 1993;27:1243–51.
Wang CC, Chen CH, Lin WW, Hwang SM, Hsieh PC, Lai PH, et al. Direct intramyocardial injection of mesenchymal stem cell sheet fragments improves cardiac functions after infarction. Cardiovasc Res. 2008;77:515–24.
Haraguchi Y, Shimizu T, Yamato M, Kikuchi A, Okano T. Electrical coupling of cardiomyocyte sheets occurs rapidly via functional gap junction formation. Biomaterials. 2006;27:4765–74.
Kawamura M, Miyagawa S, Fukushima S, Saito A, Miki K, Ito E, et al. Enhanced survival of transplanted human induced pluripotent stem cell-derived cardiomyocytes by the combination of cell sheets with the pedicled omental flap technique in a porcine heart. Circulation. 2013;128:S87–94.
Itabashi Y, Miyoshi S, Kawaguchi H, Yuasa S, Tanimoto K, Furuta A, et al. A new method for manufacturing cardiac cell sheets using fibrin-coated dishes and its electrophysiological studies by optical mapping. Artif Organs. 2005;29:95–103.
Itabashi Y, Miyoshi S, Yuasa S, Fujita J, Shimizu T, Okano T, et al. Analysis of the electrophysiological properties and arrhythmias in directly contacted skeletal and cardiac muscle cell sheets. Cardiovasc Res. 2005;67:561–70.
Matsuura K, Wada M, Shimizu T, Haraguchi Y, Sato F, Sugiyama K, et al. Creation of human cardiac cell sheets using pluripotent stem cells. Biochem Biophys Res Commun. 2012;425:321–7.
Lee P, Klos M, Bollensdorff C, Hou L, Ewart P, Kamp TJ, et al. Simultaneous voltage and calcium mapping of genetically purified human induced pluripotent stem cell-derived cardiac myocyte monolayers. Circ Res. 2012;110:1556–63.
Fujita J, Itabashi Y, Seki T, Tohyama S, Tamura Y, Sano M, et al. Myocardial cell sheet therapy and cardiac function. Am J Physiol Heart Circ Physiol. 2012;303:H1169–82.
Masumoto H, Matsuo T, Yamamizu K, Uosaki H, Narazaki G, Katayama S, Marui A, Shimizu T, Ikeda T, Okano T, Sakata R, Yamashita JK. Pluripotent stem cell-engineered cell sheets re-assembled with defined cardiovascular populations ameliorate reduction in infarct heart function through cardiomyocyte-mediated neovascularization. Stem cells. 2012
Xiong Q, Ye L, Zhang P, Lepley M, Swingen C, Zhang L, et al. Bioenergetic and functional consequences of cellular therapy: activation of endogenous cardiovascular progenitor cells. Circ Res. 2012;111:455–68. The findings demonstrate myocardial patch enhanced delivery of cardiovascular progenitor cells result in improved LV chamber function that is associated by reduction of LV dilatation and LV wall stresses, the improvement of myocardial perfusion and metabolism in the in vivo heart.
Suzuki R, Hattori F, Itabashi Y, Yoshioka M, Yuasa S, Manabe-Kawaguchi H, et al. Omentopexy enhances graft function in myocardial cell sheet transplantation. Biochem Biophys Res Commun. 2009;387:353–9.
Stevens KR, Kreutziger KL, Dupras SK, Korte FS, Regnier M, Muskheli V, et al. Physiological function and transplantation of scaffold-free and vascularized human cardiac muscle tissue. Proc Natl Acad Sci U S A. 2009;106:16568–73.
Kreutziger KL, Muskheli V, Johnson P, Braun K, Wight TN, Murry CE. Developing vasculature and stroma in engineered human myocardium. Tissue Eng A. 2011;17:1219–28.
Sasagawa T, Shimizu T, Sekiya S, Haraguchi Y, Yamato M, Sawa Y, et al. Design of prevascularized three-dimensional cell-dense tissues using a cell sheet stacking manipulation technology. Biomaterials. 2010;31:1646–54.
Shudo Y, Miyagawa S, Fukushima S, Saito A, Shimizu T, Okano T, et al. Novel regenerative therapy using cell-sheet covered with omentum flap delivers a huge number of cells in a porcine myocardial infarction model. J Thorac Cardiovasc Surg. 2011;142:1188–96.
Rane AA, Christman KL. Biomaterials for the treatment of myocardial infarction a 5-year update. J Am Coll Cardiol. 2011;58:2615–29.
Fukuhara S, Tomita S, Nakatani T, Fujisato T, Ohtsu Y, Ishida M, et al. Bone marrow cell-seeded biodegradable polymeric scaffold enhances angiogenesis and improves function of the infarcted heart. Circ J. 2005;69:850–7.
Matsubayashi K, Fedak PW, Mickle DA, Weisel RD, Ozawa T, Li RK. Improved left ventricular aneurysm repair with bioengineered vascular smooth muscle grafts. Circulation. 2003;108 Suppl 1:II219–25.
Engelmayr Jr GC, Cheng M, Bettinger CJ, Borenstein JT, Langer R, Freed LE. Accordion-like honeycombs for tissue engineering of cardiac anisotropy. Nat Mater. 2008;7:1003–10.
Feinberg AW, Feigel A, Shevkoplyas SS, Sheehy S, Whitesides GM, Parker KK. Muscular thin films for building actuators and powering devices. Science. 2007;317:1366–70.
Radisic M, Park H, Shing H, Consi T, Schoen FJ, Langer R, et al. Functional assembly of engineered myocardium by electrical stimulation of cardiac myocytes cultured on scaffolds. Proc Natl Acad Sci U S A. 2004;101:18129–34.
Zimmermann WH, Schneiderbanger K, Schubert P, Didie M, Munzel F, Heubach JF, et al. Tissue engineering of a differentiated cardiac muscle construct. Circ Res. 2002;90:223–30.
Fink C, Ergun S, Kralisch D, Remmers U, Weil J, Eschenhagen T. Chronic stretch of engineered heart tissue induces hypertrophy and functional improvement. FASEB J. 2000;14:669–79.
Zimmermann WH, Fink C, Kralisch D, Remmers U, Weil J, Eschenhagen T. Three-dimensional engineered heart tissue from neonatal rat cardiac myocytes. Biotechnol Bioeng. 2000;68:106–14.
Tulloch NL, Muskheli V, Razumova MV, Korte FS, Regnier M, Hauch KD, et al. Growth of engineered human myocardium with mechanical loading and vascular coculture. Circ Res. 2011;109:47–59.
Tiburcy M, Didie M, Boy O, Christalla P, Doker S, Naito H, et al. Terminal differentiation, advanced organotypic maturation, and modeling of hypertrophic growth in engineered heart tissue. Circ Res. 2011;109:1105–14.
Yildirim Y, Naito H, Didie M, Karikkineth BC, Biermann D, Eschenhagen T, et al. Development of a biological ventricular assist device: preliminary data from a small animal model. Circulation. 2007;116:I16–23.
Xiong Q, Ye L, Zhang P, Lepley M, Tian J, Li J, et al. Functional consequences of human induced pluripotent stem cell therapy: myocardial ATP turnover rate in the in vivo swine heart with postinfarction remodeling. Circulation. 2013;127:997–1008. 1) the first report of quantification of myocardial ATP hydrolysis rate in the in vivo heart; 2) this rate is significantly reduced at peri scar border zone myocardium of a infarcted hearts; and 3) the patch enhanced cell therapy is accompanied by a significant improvement of myocardial ATP hydrolysis rate in the in vivo heart.
Xiong Q, Hill KL, Li Q, Suntharalingam P, Mansoor A, Wang X, et al. A fibrin patch-based enhanced delivery of human embryonic stem cell-derived vascular cell transplantation in a porcine model of postinfarction left ventricular remodeling. Stem Cells. 2011;29:367–75.
Zhang G, Nakamura Y, Wang X, Hu Q, Suggs LJ, Zhang J. Controlled release of stromal cell-derived factor-1 alpha in situ increases c-kit cell homing to the infarcted heart. Tissue Eng. 2007;13:2063–71.
Feygin J, Mansoor A, Eckman P, Swingen C, Zhang J. Functional and bioenergetic modulations in the infarct border zone following autologous mesenchymal stem cell transplantation. Am J Physiol Heart Circ Physiol. 2007;293:H1772–80.
Bolognese L, Neskovic AN, Parodi G, Cerisano G, Buonamici P, Santoro GM, et al. Left ventricular remodeling after primary coronary angioplasty: patterns of left ventricular dilation and long-term prognostic implications. Circulation. 2002;106:2351–7.
Hu Q, Wang X, Lee J, Mansoor A, Liu J, Zeng L, et al. Profound bioenergetic abnormalities in peri-infarct myocardial regions. Am J Physiol Heart Circ Physiol. 2006;291:H648–57.
Wendel JS, Ye L, Zhang P, Tranquillo RT, Zhang JJ. Functional consequences of a tissue-engineered myocardial patch for cardiac repair in a rat infarct model. Tissue Eng A. 2014;20:1325–35.
Sawa Y. [Myocardial regeneration for heart failure]. Nihon rinsho. Jpn J Clin Med. 2010;68:719–25.
Chachques JC, Trainini JC, Lago N, Masoli OH, Barisani JL, Cortes-Morichetti M, et al. Myocardial assistance by grafting a new bioartificial upgraded myocardium (magnum clinical trial): one year follow-up. Cell Transplant. 2007;16:927–34.
Chachques JC, Trainini JC, Lago N, Cortes-Morichetti M, Schussler O, Carpentier A. Myocardial assistance by grafting a new bioartificial upgraded myocardium (magnum trial): clinical feasibility study. Ann Thorac Surg. 2008;85:901–8.
Compliance with Ethics Guidelines
Conflict of Interest
Jianyi (Jay) Zhang reports grants supported by NIH RO1, grants supported by NIH RO1, grants supported by NIH RO1, and grants supported by NIH UO1. In addition, Dr. Zhang has a patent fibrin-based biomatrix issued.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Regenerative Medicine and Stem-cell Therapy
Rights and permissions
About this article

Cite this article
Zhang, J. Engineered Tissue Patch for Cardiac Cell Therapy. Curr Treat Options Cardio Med 17, 37 (2015). https://doi.org/10.1007/s11936-015-0399-5
Published:
DOI: https://doi.org/10.1007/s11936-015-0399-5