
Abstract
The purpose of this meta-analytic study is to summarize the current science concerning the (a) prevalence of alcohol use, (b) prevalence of sexual risk behaviors, and (c) association between alcohol use and sexual risk behaviors among people living with HIV/AIDS (PLWHA). Studies were included if they sampled PLWHA, evaluated both alcohol use and sexual risk behavior (e.g., condom use, multiple partners), and were published between January 1, 2012, and April 1, 2013. Comprehensive electronic database searches located 728 published studies with relevant keywords; 17 studies (k = 19 reports) were included. Findings indicate that a substantial proportion of PLWHA use alcohol and engage in sexual risk behaviors. Among PLWHA, alcohol use was significantly associated with unprotected sex (d + = 0.23, 95 % CI = 0.05, 0.40; k = 5). Secondary prevention programs for PLWHA that address alcohol use in the context of sexual behavior are needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The global HIV epidemic remains a public health challenge. More than 34 million people are currently living with HIV/AIDS worldwide with sub-Saharan Africa bearing the heaviest burden, accounting for 69 % of all people living with HIV [1]. The global HIV epidemic remains stable with an estimated 2.5 million people newly infected with HIV per year [1]. Unprotected sex continues to account for the largest proportion (80 %) of all new HIV infections globally [1, 2]. Because sexual transmission of HIV originates from individuals infected with HIV, national AIDS campaigns in the U. S. and elsewhere increasingly emphasize secondary prevention as critical to the control of HIV [3].
Most PLWHA remain sexually active after diagnosis, and many report engaging in unprotected sex [4–6]. Reductions in sexual risk behavior often occur immediately following an HIV diagnosis but for some PLWHA, changes in sexual risk behavior are difficult to maintain [7]. A meta-analytic review of U.S. adults unaware they are infected with HIV found that participants reported a 37 % reduction in unprotected sex after receiving notification of their HIV-positive status [6]. In another meta-analytic review, 26 % of HIV-positive men who have sex with men (MSM), living with HIV for a median of 70 months, reported engaging in unprotected anal sex [5]. Unprotected sex among PLWHA increases both the risk of HIV transmission to an uninfected partner and the possibility of acquiring drug-resistant strains of the virus from an infected partner [8, 9]. Thus, understanding the factors associated with sexual risk-taking among PLWHA is critical to the development of secondary prevention strategies.
Alcohol use has been implicated as a prominent risk factor in the transmission of HIV [10]. Alcohol consumption may increase an individual’s risk by impairing sexual decision-making and by weakening the immune system [11, 12•]. Baliunas, Rehm, Irving, and Shuper [13] found the incidence of HIV was associated with overall level of alcohol consumption. Drinkers were at 77 % higher risk of HIV infection than non-drinkers. Moreover, risk of HIV infection among heavy episodic drinkers was double that of non-heavy episodic drinkers. Another meta-analysis examining the association between alcohol use and HIV from studies conducted in Africa [14] found drinker status to be associated with HIV infection such that drinkers were 70 % more likely to be HIV-positive than non-drinkers. Again, risk of HIV was notably higher among problem drinkers vs. non-problem drinkers. Thus, alcohol use appears to increase the likelihood of becoming infected with HIV in dose-response fashion.
Alcohol use among people already infected with HIV is also associated with sexual risk behaviors. A meta-analysis of 27 studies examining the association between alcohol (any alcohol consumption, problematic drinking, and alcohol use before/during sex) and unprotected sex among people living with HIV/AIDS found a positive association between alcohol use and unprotected sex [15]. These findings suggest that alcohol use is a significant risk factor for transmission among PLWHA.
The purpose of this systematic review and meta-analysis was to determine the current state-of-the-science concerning the (a) prevalence of alcohol use, (b) prevalence of sexual risk behaviors, and (c) strength of the association between alcohol and sexual risk behavior among individuals infected with HIV. Prior meta-analyses of the alcohol-sexual risk-HIV literature [13–15] focused on the overall alcohol-risky sex and alcohol-HIV associations within studies published through 2008. To determine the current state-of-the-science, we restricted our meta-analysis to the most recently published studies (i.e., January 1, 2012 through April 1, 2013) that assessed alcohol use and sexual risk behaviors among PLWHA. (We restricted the time-frame of our search because the methods used and quality of reporting tends to be stronger in more recent literature [16].) We also evaluated whether characteristics of the study (e.g., geographical region) and sample (e.g., sex of participant, medication adherence) influenced the prevalence of alcohol use or sexual risk behaviors in this population.
Methods
Search Strategy, Inclusion Criteria, and Study Selection
We searched multiple electronic reference databases (PubMed, EMBASE, Global Health, PsycINFO, CINAHL, ERIC, SocIndex, The Cochrane Library, and Web of Science [social sciences and science citation indices]) using a Boolean search strategy: (((binge* OR drinking OR "drinking behavior"[mesh:noexp]) AND (liquor[all fields] OR alcohol OR ethanol OR alcoholic beverages)) OR binge drinking OR alcoholic beverages OR alcohol drinking OR alcohol abuse OR alcoholic OR alcohol OR "alcohol-related disorders" [MeSH] OR alcoholism OR intoxicat* OR drunk* OR liquor[all fields]) AND ((dangerous behavior OR risk taking OR risk factors AND sexu*[tiab]) OR sexual behavior OR sexual partners OR unsafe sex OR behavior disinhibition OR condoms OR "men who have sex with men" OR "men having sex with men" OR MSM) AND (AIDS[sb]). Our search strategy was developed with the assistance of an expert health sciences librarian in the Alpert Medical School of Brown University. Because many electronic databases have specific search methods (e.g., Medical Subject Heading [MeSH] terms used in PubMED are not available in other databases such as PsycINFO), our basic search strategy was modified based on the specific search requirements for each electronic database. All final electronic reference database searches were conducted on April 1, 2013.
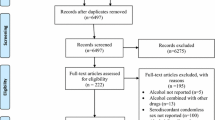
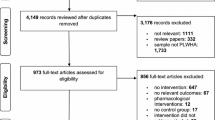
Studies (or portions of studies) were included if they (1) sampled PLWHA (i.e., 100 % of the sample was HIV-positive or outcomes were separated by HIV-status); (2) evaluated alcohol use and any sexual risk behavior (e.g., condom use, number of partners); (3) provided sufficient information to calculate effect sizes; and (4) were published (including electronic publications) between January 1, 2012, and April 1, 2013. Reference sections of relevant manuscripts (including published reviews obtained through the electronic reference database search) were also reviewed. Studies that fulfilled the inclusion criteria were included. When authors reported details and/or outcomes of the intervention in multiple studies, the studies were linked in the database and represented as a single study. The manuscript reporting the main trial outcomes was selected as the primary study; the publication date from the primary study was used to determine eligibility. The final sample included 17 studies reporting 19 reports (Fig. 1) [17–33].

Study selection process for the meta-analysis. Note. Two studies overlapped and were used as both a primary manuscript and a supplemental manuscript (pilot data) for another final study
Coding and Reliability
Two independent coders rated the study information, sample characteristics (e.g., gender), design (e.g., recruitment strategy) and measurement specifics, and length and content of control and intervention condition (e.g., number of sessions). If data from the same sample appeared in multiple publications, the most comprehensive report was used while supplementing missing data from the other report(s). Study methodological quality was assessed using 17 items (e.g., random assignment) from validated measures [34–36]; total possible quality score is 25. We examined inter-rater reliability for all study descriptors. For the categorical variables, raters agreed on 92 % of the judgments (mean Cohen’s κ = .82). Reliability for the continuous variables yielded an average intraclass correlation coefficient (ρ) of 0.85 across categories (median = 1.00). Disagreements between coders were resolved through discussion.
Study Outcomes and Effect Sizes
Effect sizes were calculated to assess both the prevalence and association between alcohol use and sexual risk behavior. Prevalence outcomes included any alcohol consumption, alcohol use before sex, condom use, condom use at last sexual event, and multiple sexual partners. Prevalence estimates were calculated as the proportion of HIV-positive persons who had engaged in alcohol use or sexual risk behavior divided by the total number of HIV-positive persons in the sample. (For sexual risk behaviors, we included only HIV-positive persons who were sexually active.) Consistent with standard meta-analytic methods [37], prevalence estimates (and the standard error and inverse variance weight) were converted to logits and used in all analyses. Results of the analyses (using the logits) were converted back into prevalence estimates (and corresponding confidence intervals) for ease of interpretation of study findings. The association between alcohol use and unprotected sex was determined from the analyses of binary data (i.e., 2 [alcohol use: yes, no] × 2 [unprotected sex: yes, no]). Because the raw cell frequencies of the 2 × 2 contingency tables were not reported in any of the studies, other statistical information (i.e., odds ratio, chi-square, correlation coefficients) was used to estimate the effect sizes (corrected for sample size bias) using standard procedures [37, 38]. Effect size estimates for the alcohol-risky sex association are expressed as a standardized mean difference (d) where the sign of d is positive when alcohol use was associated with unprotected sexual behavior.
From the 17 studies that met the inclusion criteria, 19 reports were analyzed. (Two studies provided outcomes separate for men and women [28] and treatment and control groups [33]). All of the studies reported at least one prevalence estimate (15 alcohol use, nine alcohol use before sex, 12 condom use, five condom use at last sex event, and 11 multiple sexual partners) or association (five alcohol and unprotected sex). Studies that specifically recruited PLWHA who engaged in alcohol or sexual risk behaviors (e.g., heavy drinkers [26, 27]; unprotected sex [26, 27, 31]) or recruited from high-risk samples (e.g., sex workers [18]) were excluded from corresponding analyses to avoid overestimating the prevalence of alcohol use (any) or sexual risk behaviors (condom use, condom use at last sex, and multiple sexual partners). Multiple effect size estimates were calculated from individual studies when they reported more than one outcome variable (e.g., condom use separated by steady and casual partners).
Statistical Analyses
Data analyses were conducted with Stata 12 [39] using published macros [37, 40]. Weighted mean logit effect sizes (prevalence estimates) and weighted standardized mean effect sizes (association) were calculated using random-effects procedures [37]. The 95 % confidence intervals (CIs) surrounding a weighted mean logit effect size were calculated; CIs indicate the degree of precision as well as the significance of the mean logit effect size [37]. The homogeneity statistic, Q, was calculated; a significant Q indicates a lack of homogeneity and an inference of heterogeneity. To assess the extent to which outcomes were consistent across studies, the I 2 index and its corresponding 95 % CIs were calculated [41, 42]. I 2 varies between 0 (homogeneous) and 100 % (heterogeneous) [43]. If the CIs around I 2 include a zero, the set of effect sizes is considered homogeneous.
To explain variability in the prevalence estimates, moderator analyses were conducted using a modified weighted regression analysis (following fixed-effects assumptions) with weights equivalent to the inverse of the variance for each effect size [37, 44]. Regression analyses examined a priori determined moderators. Study (geographical region based on the World Health Organization region groupings[45]) and sample (proportion women, proportion alcohol users, proportion MSM, proportion of participants with multiple partners, proportion currently on ART, proportion adhering to HIV medication) characteristics were examined as potential moderators of the prevalence estimates. Weighted regression analyses were conducted only for outcomes with sufficient studies (i.e., > 5 studies).
Results
Details of the 17 included studies are provided in Table 1. Studies were conducted in several geographical regions: 35 % Americas [19, 26, 28, 30–32], 29 % Africa [17, 18, 21, 23], 18 % South-East Asia [20, 29, 33], 12 % European [22, 27], and 6 % Western Pacific [24]. PLWHA were typically recruited through a clinic (65 %); 35 % were recruited through other venues (e.g., needle-exchange program, churches, research center). Studies were published in peer-reviewed journals in 2012 (88 %) and 2013 (12 %); data were collected between 2001 and 2011. Methodological quality (MQ) of the studies ranged from 10 to 21 (mean = 17 [68 %], SD = 3).
The study samples included 6257 PLWHA who consented to participate in the research. Women comprised nearly half (48 %) of the total sample; average age was 34 years (range = 21 to 45 years; SD = 9). The sample was ethnically diverse with 26 % Black African, 14 % White, 14 % Black non-African, 13 % Southeast Asian, 8 % East Asian, 7 % Hispanic, and the remaining 18 % of other ethnic/racial backgrounds (e.g., American Indian, mixed). Most of the PLWHA were currently sexually active (M = 87 %, SD = 0.20, Mdn = 100 %; n studies = 16). Slightly more than half were on antiretroviral medication (M = 51 %, SD = 0.33, n studies = 13) and 75 % (SD = 0.13, n studies = 4) were adherent to their medication, using definitions specific to individual studies (for details, see Table 1 note). Finally, 24 % (n studies = 13) of PLWHA reported using drugs and few of the studies (16 %, SD = 0.23, n studies = 3) reported IDU.
Prevalence of Alcohol Use and Sexual Behaviors among PLWHA
Results for studies reporting alcohol use and sexual risk behaviors are provided in Table 2. Because all effects were marked by substantial heterogeneity, analyses followed random-effects assumptions. Examination of I 2 confirmed high levels of heterogeneity.
Alcohol Use
The prevalence of any alcohol consumption among PLWHA is 37 % (95 % CI: 25, 51, Z = -1.88, p = .056). Alcohol use before sex was reported in 33 % of the sample (95 % CI: 18, 52, Z = -1.76, p = .079).
Sexual Risk Behavior
The prevalence of condom use and condom use during the last sexual occasion was 67 % (95 % CI: 56, 76, Z = 2.92, p = .003) and 76 % (95 % CI: 62, 86, Z = 3.42, p = .001), respectively. For sexual partners, the prevalence of having multiple sexual partners was 25 % (95 % CI: 11, 48, Z = -2.15, p = .03).
Moderators of Alcohol Use and Sexual Behaviors Among PLWHA
Moderator tests were conducted to examine whether a priori determined study (WHO region [45]) and sample (proportion women, proportion alcohol or drug users, proportion MSM, proportion of participants with multiple partners, proportion currently on ART, proportion adhering to HIV medication) characteristics related to the variability in prevalence estimates. Due to insufficient sample size (k ≤ 5), moderator tests were conducted only for alcohol use, alcohol use before sex, condom use, and multiple sex partners.
Alcohol Use
Alcohol use was more prevalent among studies conducted in the Americas (35 %; 95 % CI = 32, 38; k = 5) or South-East Asia (36 %; 95 % CI = 32, 40; k = 4) compared to Africa (27 %; 95 % CI = 25, 29; k = 5), Q B (2) = 28.29, p < .001. (Only a single study [22] reported alcohol use in the European region; it was excluded from analyses to avoid misrepresenting the prevalence of alcohol use in Europe.) The prevalence of alcohol consumption was higher when studies sampled fewer women (β = -0.69, p < .001, k = 15), more MSM (β = 0.71, p < .001, k = 14), drug users (β = 0.71, p < .001, k = 11), and participants reporting multiple sexual partners (β = 0.28, p < .001, k = 9). Alcohol use was less prevalent among PLWHA who were currently on ART (β = -0.49, p < .001, k = 12) and among those adherent to their HIV medication (β = -0.51, p = .05, k = 4).
Alcohol Use Before Sex
Alcohol use before sex was more prevalent among studies conducted in Africa (40 %; 95 % CI = 33, 47; k = 3) compared to South-East Asia (22 %; 95 % CI = 18, 27; k = 4), Q B (1) = 19.32, p < .001. (Two studies, one conducted in the European region [27] and another in the Western Pacific region [20], were excluded from the analyses.) The prevalence of alcohol use before sex was higher when studies sampled more women (β = 0.13, p = .043, k = 9), fewer MSM (β = -0.44, p < .001, k = 8), more drug users (β = 0.49, p < .001, k = 6), and participants who reported having multiple sexual partners (β = 0.79, p < .001, k = 7). Alcohol use before sex was less prevalent among PLWHA who were currently on ART (β = -0.60, p < .001, k = 8) and adherent to their HIV medication (β = -0.99, p = .010, k = 3).
Condom Use
Condom use was more prevalent among studies conducted in South-East Asia (76 %; 95 % CI = 71, 80; k = 4) and the Americas (73 %; 95 % CI = 70, 76; k = 4) compared to Africa (64 %; 95 % CI = 59, 68; k = 2), Q B (2) = 15.02, p < .001. (Two studies, one conducted in the European region [27] and another in the Western Pacific region [20], were excluded from the analyses.) The prevalence of condom use was higher when studies sampled more women (β = 0.17, p = .007, k = 12), fewer MSM (β = -0.48, p < .001, k = 11), fewer alcohol users (β = -0.67, p < .001, k = 12), fewer drug users (β = -0.19, p = .003, k = 10), and fewer participants who reported having multiple sexual partners (β = -0.64, p < .001, k = 9). Condom use was more prevalent among PLWHA who were currently on ART (β = 0.57, p < .001, k = 10). Self-reported HIV medication adherence was not a significant predictor of the prevalence of condom use (β = -0.05, p = .779, k = 4).
Multiple Sexual Partners
The prevalence of multiple sexual partners was greater among studies conducted in the Americas (50 %; 95 % CI = 46, 53; k = 4) compared with Africa (17 %; 95 % CI = 12, 23; k = 2) and South-East Asia (14 %; 95 % CI = 11, 18; k = 3), Q B (2) = 145.15, p < .001. (Two studies, one conducted in the European region [27] and another in the Western Pacific region [20], were excluded from the analyses.) The prevalence of participants with multiple sexual partners was higher when studies sampled fewer women (β = -0.22, p < .001, k = 11), more MSM (β = 0.24, p < .001, k = 11), more alcohol users (β = 0.21, p < .001, k = 11), and fewer drug users (β = -0.15, p < .001, k = 8). Multiple sexual partners were less prevalent among PLWHA who were currently on ART (β = -0.23, p < .001, k = 10) and were adherent to their HIV medication (β = -0.71, p < .001, k = 5).
Association between Alcohol Use and Unprotected Sex among PLWHA
Five studies [19, 20, 22, 24, 31] of the 17 studies (N = 1,589) assessed the association between any alcohol consumption (yes, no) and unprotected sex (yes, no). Alcohol use was associated with unprotected sex, d + = 0.23 (95 % CI = 0.05, 0.40). The effect sizes were homogeneous indicating consistency across studies, Q(4) = 4.50, p = .34, I 2 = 11 % (95 % CI = 0, 53).
Discussion
This systematic review and meta-analysis of 17 recent studies assessing alcohol use and sexual risk behaviors among nearly 6300 PLWHA shows that approximately one-third of PLWHA use alcohol and engage in sexual risk behaviors. Our findings also show that any alcohol consumption is associated with unprotected sex among PLWHA (d + = 0.23). The magnitude of the effect size for the alcohol-risky sex association was small to medium and is consistent with an earlier review of the literature (see [15], d + = 0.30, k = 9). Although these global association studies (i.e., studies that assess the extent to which an individual’s overall frequency of alcohol use and sexual risk behavior are related) cannot establish a causal link between alcohol and risky sexual behavior, our findings provide support for the growing consensus that alcohol use is an important risk factor for the transmission of HIV [12•, 46]. The studies included in the meta-analysis represent diverse samples of PLWHA from multiple geographical regions and significant heterogeneity was observed for the prevalence estimates. Weighted regression analyses indicated that the variability across effect sizes is moderated by study and sample characteristics (discussed below). Overall, our findings provide on-going support for the involvement of alcohol use in sexual risk-taking among PLWHA.
The results of our moderator tests show that geographical region is an important predictor of the prevalence of alcohol use and sexual risk behaviors among PLWHA. The prevalence of alcohol consumption was higher among the WHO regions of the Americas and South-East Asia compared to Africa but the prevalence of condom use was lower in Africa relative to the Americas and South-East Asia. Furthermore, alcohol use before sex was higher in Africa relative to South-East Asia (40 % vs. 22 %). These findings corroborate prior reviews that showed a high prevalence of alcohol use in sexual contexts in Africa [47, 48]. High-risk alcohol use may also be associated with the lower prevalence of condom use among Africans [47]. Greater attention of the influence of alcohol use on sexual risk-taking, especially among PLWHA in Africa, is warranted.
Moderator tests suggest that sample characteristics are important predictors of the prevalence of alcohol use and sexual risk behaviors among PLWHA. Consistent with prior research [49], alcohol use was less prevalent among studies that sampled women (vs. men). In contrast, women were more likely to consume alcohol prior to sex, perhaps because women consume alcohol as a means to reduce social inhibitions [50•]. MSM and drug users report high rates of alcohol use and sexual risk behaviors. The prevalence of condom use was lower among MSM and drug users; nonetheless, unlike drug users, MSM were more likely to have multiple sexual partners. Overall, alcohol users were more likely to report less condom use and more sexual partners. The pattern of results suggests that alcohol use and sexual risk behaviors may be more prevalent for certain populations and, overall, suggests that interventions tailored to subpopulations of PLWHA can help to reduce alcohol use and sexual risk behaviors that enhance HIV transmission [4].
Antiretroviral therapy (ART) can play an important role in preventing the transmission of HIV. “Treatment as prevention” has garnered much attention due to the success of the National Institute of Health HPTN 052 trial, which found that ART for PLWHA reduced HIV transmission by 96 % between serodiscordant heterosexual couples [51]. The role of ART in reducing sexual risk behaviors in the broader community has been largely absent from subsequent discussions (see [52•] for a commentary on this issue). Moderator results from the current meta-analysis suggest that PLWHA who are currently on ART consume less alcohol and engage in fewer sexual risk behaviors. Of the few studies (k = 5) reporting relevant data, adherence to HIV medication was also associated with lower alcohol use, alcohol use before sex, and fewer sexual partners. Thus, it appears that engagement in medical care leads not only to a reduction in infectiousness but may also be associated with less risky behavior.
Limitations
Several limitations should be considered when interpreting these findings. First, using electronic bibliographic databases to identify relevant studies are restricted by publication source and authors’ choice of keywords [53]. Second, our meta-analysis was restricted to studies published between January 1, 2012 and April 1, 2013, which may not be representative of other studies of PLWHA. Nonetheless, our findings were consistent with prior reviews of the earlier literature with PLWHA [5, 6, 15]. Third, all outcomes involve self-reports, which are vulnerable to measurement, cognitive (e.g., memory), and social (e.g., self-presentation) biases [54]. Researchers typically use methods to minimize these biases and maximize data quality [55]. Fourth, our moderator tests were limited to the data available in the individual studies. Inconsistencies in reporting ‘problematic alcohol use’ (see description of measures in Table 1 note) as well as clinical and immunological markers (e.g., CD4 counts, viral load) prevented us from fully exploring potentially relevant moderators that may elucidate our findings. Finally, causality cannot be determined from the available data. The relation between alcohol and sexual risk may be explained by ‘third variables’ (e.g., partner drinking, drinking environment).[56]
Conclusion
Alcohol use is a prominent risk factor in the transmission of HIV. Our meta-analysis confirms that PLWHA frequently use alcohol and engage in sexual risk behaviors and that alcohol use is associated with sexual risk-taking. The accumulated evidence suggests that efforts to address the co-occurrence of alcohol use and sexual behavior are needed to reduce the transmission of HIV.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Joint United Nations Programme on HIV/AIDS (UNAIDS). Global Report: UNAIDS Report on the Global AIDS Epidemic. 2012. http://www.unaids.org/en/resources/publications/2012/name,76121,en.asp. Accessed July 17 2013.
Centers for Diease Control and Prevention. HIV Surveillance Report, 2011; vol. 23. 2013. http://www.cdc.gov/hiv/library/reports/surveillance/2011/surveillance_Report_vol_23.html. Accessed July 17 2013.
The White House Office of National AIDS Policy. National HIV/AIDS Strategy for the United States. 2010. http://aids.gov/federal-resources/national-hiv-aids-strategy/nhas.pdf. Accessed August 2 2013.
Fisher JD, Smith L. Secondary prevention of HIV infection: the current state of prevention for positives. Curr Opin HIV AIDS. 2009;4(4):279–87. doi:10.1097/COH.0b013e32832c7ce5.
Crepaz N, Marks G, Liau A, Mullins MM, Aupont LW, Marshall KJ, et al. Prevalence of unprotected anal intercourse among HIV-diagnosed MSM in the United States: a meta-analysis. AIDS (London, England). 2009;23(13):1617–29. doi:10.1097/QAD.0b013e32832effae.
Marks G, Crepaz N, Senterfitt JW, Janssen RS. Meta-analysis of high-risk sexual behavior in persons aware and unaware they are infected with HIV in the United States: implications for HIV prevention programs. J Acquir Immune Defic Syndr (1999). 2005;39(4):446–53.
Eaton LA, Kalichman SC. Changes in transmission risk behaviors across stages of HIV disease among people living with HIV. J Assoc Nurses AIDS Care. 2009;20(1):39–49. doi:10.1016/j.jana.2008.10.005.
Blackard JT, Mayer KH. HIV superinfection in the era of increased sexual risk-taking. Sex Transm Dis. 2004;31(4):201–4.
Campbell MS, Gottlieb GS, Hawes SE, Nickle DC, Wong KG, Deng W, et al. HIV-1 superinfection in the antiretroviral therapy era: are seroconcordant sexual partners at risk? PLoS ONE. 2009;4(5):e5690. doi:10.1371/journal.pone.0005690.
Bryant KJ. Expanding research on the role of alcohol consumption and related risks in the prevention and treatment of HIV/AIDS. Subst Use Misuse. 2006;41(10–12):1465–507. doi:10.1080/10826080600846250.
Steele CM, Josephs RA. Alcohol myopia. Its prized and dangerous effects. Am Psychol. 1990;45(8):921–33.
• Shuper PA, Neuman M, Kanteres F, Baliunas D, Joharchi N, Rehm J. Causal considerations on alcohol and HIV/AIDS--a systematic review. Alcohol Alcohol. 2010;45(2):159–66. doi:10.1093/alcalc/agp091. A systematic review of meta-analyses and narrative reviews conducted to date on the association between alcohol use and HIV. This review documents the (a) association between alcohol use and sexual risk behaviors and (b) effect of alcohol use on worsening the disease course.
Baliunas D, Rehm J, Irving H, Shuper P. Alcohol consumption and risk of incident human immunodeficiency virus infection: a meta-analysis. Int J Public Health. 2010;55(3):159–66.
Fisher JC, Bang H, Kapiga SH. The association between HIV infection and alcohol use: a systematic review and meta-analysis of African studies. Sex Transm Dis. 2007;34(11):856–63.
Shuper PA, Joharchi N, Irving H, Rehm J. Alcohol as a correlate of unprotected sexual behavior among people living with HIV/AIDS: review and meta-analysis. AIDS Behav. 2009;13(6):1021–36. doi:10.1007/s10461-009-9589-z.
Falagas ME, Grigori T, Ioannidou E. A systematic review of trends in the methodological quality of randomized controlled trials in various research fields. J Clin Epidemiol. 2009;62(3):227–31. doi:10.1016/j.jclinepi.2008.07.012. 31 e1-9.
Alcaide ML, Jones DL, Chitalu N, Weiss S. Chlamydia and gonorrhea infections in HIV-positive women in Urban Lusaka, Zambia. J Global Infect Dis. 2012;4(3):141–4. doi:10.4103/0974-777x.100566.
Braunstein SL, Wijgert JH, Vyankandondera J, Kestelyn E, Ntirushwa J, Nash D. Risk factor detection as a metric of STARHS performance for HIV incidence surveillance among female sex workers in Kigali, Rwanda. Open AIDS J. 2012;6(Special Issue 1):112–21.
Bruce D, Kahana S, Harper GW, Fernandez MI. The A. Alcohol use predicts sexual risk behavior with HIV-negative or partners of unknown status among young HIV-positive men who have sex with men. AIDS Care. 2012. doi:10.1080/09540121.2012.720363.
Clarke A, Kerr S, Honeybrook A, Cooper DA, Avihingsanon A, Duncombe C, et al. Adherence and risk behaviour in patients with HIV infection receiving antiretroviral therapy in Bangkok. Open Virol J. 2012;6:23–8. doi:10.2174/1874357901206010023.
Desmond K, Milburn N, Richter L, Tomlinson M, Greco E, van Heerden A, et al. Alcohol consumption among HIV-positive pregnant women in KwaZulu-Natal, South Africa: prevalence and correlates. Drug Alcohol Depend. 2012;120(1–3):113–8. doi:10.1016/j.drugalcdep.2011.07.004.
Dirks H, Esser S, Borgmann R, Wolter M, Fischer E, Potthoff A, et al. Substance use and sexual risk behaviour among HIV-positive men who have sex with men in specialized out-patient clinics. HIV Med. 2012;13(9):533–40. doi:10.1111/j.1468-1293.2012.01005.x.
Ezugwu EC, Agu P, Ohayi SA, Okeke TC, Dim CC, Obi SN. HIV sero-prevalence among pregnant women in a resource constrained setting, South East Nigeria. Niger J Med. 2012;21(3):338–42.
He H, Wang M, Zhang HB, Song DD, She M, Dong ZX, et al. The unprotected sexual behaviors and its influencing factors among HIV-infected men who have sex with men in Shanghai, China. Zhonghua yu fang yi xue za zhi [Chin J Prev Med]. 2012;46(11):976–81.
Kagimu M, Guwatudde D, Rwabukwali C, Kaye S, Walakira Y, Ainomugisha D. Religiosity for HIV prevention in Uganda: a case study among Christian youth in Wakiso district. Af Health Sci. 2012;12(1):17–25.
Malow RM, Devieux JG, Stein JA, Rosenberg R, Lerner BG, Attonito J, et al. Neurological function, information-motivation-behavioral skills factors, and risk behaviors among HIV-positive alcohol users. AIDS Behav. 2012;16(8):2297–308. doi:10.1007/s10461-012-0246-6.
Pace C, Lioznov D, Cheng D, Wakeman S, Raj A, Walley A, et al. Sexually transmitted infections among HIV-infected heavy drinkers in St Petersburg, Russia. Int J STD AIDS. 2012;23(12):853–8.
Paz-Bailey G, Shah N, Creswell J, Guardado ME, Nieto AI, Estrada MC, et al. Risk behaviors and STI prevalence among people with HIV in El Salvador. Open AIDS J. 2012;6:205–12. doi:10.2174/1874613601206010205.
Rongkavilit C, Naar-King S, Koken JA, Bunupuradah T, Chen X, Saengcharnchai P, et al. A feasibility study of motivational interviewing for health risk behaviors among thai youth living with HIV. J Assoc Nurses AIDS Care. 2012. doi:10.1016/j.jana.2012.02.008.
Rotheram-Borus MJ, Rice E, Comulada WS, Best K, Elia C, Peters K, et al. Intervention outcomes among HIV-affected families over 18 months. AIDS Behav. 2012;16(5):1265–75. doi:10.1007/s10461-011-0075-z.
Skeer MR, Mimiaga MJ, Mayer KH, O'Cleirigh C, Covahey C, Safren SA. Patterns of substance use among a large urban cohort of HIV-infected men who have sex with men in primary care. AIDS Behav. 2012;16(3):676–89. doi:10.1007/s10461-011-9880-7.
Whetten K, Reif S, Toth M, Jain E, Leserman J, Pence B. Relationship between trauma and high-risk behavior among HIV-positive men who do not have sex with men (MDSM). AIDS Care. 2012;24(11):1453–60.
Rongkavilit C, Naar-King S, Wang B, Panthong A, Bunupuradah T, Parsons JT, et al. Motivational Interviewing Targeting Risk Behaviors for Youth Living with HIV in Thailand. AIDS Behav. 2013. doi:10.1007/s10461-013-0407-2.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84.
Fowkes FG, Fulton PM. Critical appraisal of published research: introductory guidelines. BMJ. 1991;302(6785):1136–40.
Miller WR, Brown JM, Simpson TL, Handmaker NS, Bien TH, Luckie LF. What works? A methodological analysis of the alcohol treatment outcome literature. In: Hester RK, Miller WR, editors. Handbook of alcoholism treatment approaches: Effective alternatives. 2nd ed. Needham Heights: Allyn & Bacon; 1995. p. 12–44.
Lipsey MW, Wilson DB. Practical meta-analysis. Applied social research methods series. Thousand Oaks: Sage; 2001.
Borenstein M, Hedges LV, Higgins JPT, Rothestein HR. Introduction to meta-analysis. West Sussex: Willey; 2009.
StataCorp. Stata/SE. 12.1 for Windows ed. College Station: StataCorp LP; 2013.
Wilson DB. Meta-analysis macros for SAS, SPSS, and Stata. 2001.
Huedo-Medina TB, Sanchez-Meca J, Marin-Martinez F, Botella J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods. 2006;11(2):193–206. doi:10.1037/1082-989X.11.2.193.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58. doi:10.1002/sim.1186.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. doi:10.1136/bmj.327.7414.557.
Hedges LV. Fixed effects models. In: Cooper H, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation; 1994. p. 285–99.
World Health Organization. Global burden of disease: Definitions of region groupings. 2013. http://www.who.int/about/regions/en/index.html. Accessed July 26 2013.
Leigh BC, Stall R. Substance use and risky sexual behavior for exposure to HIV. Issues in methodology, interpretation, and prevention. Am Psychol. 1993;48(10):1035–45.
Woolf-King SE, Steinmaus CM, Reingold AL, Hahn JA. An update on alcohol use and risk of HIV infection in sub-Saharan Africa: Meta-analysis and future research directions. Int J Alcohol Drug Res. 2013;2(1):99–110.
Kalichman SC, Simbayi LC, Kaufman M, Cain D, Jooste S. Alcohol use and sexual risks for HIV/AIDS in sub-Saharan Africa: systematic review of empirical findings. Prev Sci. 2007;8(2):141–51. doi:10.1007/s11121-006-0061-2.
Nolen-Hoeksema S. Gender differences in risk factors and consequences for alcohol use and problems. Clin Psychol Rev. 2004;24(8):981–1010. doi:10.1016/j.cpr.2004.08.003.
• Barbor T, Caetano R, Casswell S, Edwards G, Glesbrecht N, Graham K, et al. Alcohol, no ordinary commodity: Research and public policy. 2nd ed. Oxford: Oxford University Press; 2010. This book provides an overview of the evidence establishing alcohol use as a major contributor of the global burden of injury and disease, alcohol-related policies, and intervention and prevention opportunities.
Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505. doi:10.1056/NEJMoa1105243.
• Holtgrave DR, Maulsby C, Wehrmeyer L, Hall HI. Behavioral factors in assessing impact of HIV treatment as prevention. AIDS Behav. 2012;16(5):1085–91. doi:10.1007/s10461-012-0186-1. A commentary on the lack of discussion regarding HIV-related risk behaviors following the success of the National Institute of Health’s HPTN 052 study.
Matt GE, Cook TD. Threats to the validity of research synthesis. In: Cooper H, Hedges LV, editors. The handbook of research synthesis. New York: Russell Sage Foundation; 1994. p. 503–29.
Schroder KE, Carey MP, Vanable PA. Methodological challenges in research on sexual risk behavior: II. Accuracy of self-reports. Ann Behav Med. 2003;26(2):104–23.
Del Boca FK, Noll JA. Truth or consequences: the validity of self-report data in health services research on addictions. Addiction. 2000;95 Suppl 3:S347–60.
Cooper ML. Does drinking promote risky sexual behavior? A complex answer to a simple question. Curr Dir Psychol Sci. 2006;15:19–23.
Braunstein SL, Nash D, Kim AA, Ford K, Mwambarangwe L, Ingabire CM, et al. Dual testing algorithm of BED-CEIA and AxSYM Avidity Index assays performs best in identifying recent HIV infection in a sample of Rwandan sex workers. PLoS ONE. 2011;6(4):e18402. doi:10.1371/journal.pone.0018402.
Rotheram-Borus MJ, Richter L, Van Rooyen H, van Heerden A, Tomlinson M, Stein A, et al. Project Masihambisane: a cluster randomised controlled trial with peer mentors to improve outcomes for pregnant mothers living with HIV. Trials. 2011;12:2. doi:10.1186/1745-6215-12-2.
Kagimu M, Kaye S, Ainomugisha D, Lutalo I, Walakira Y, Guwatudde D, et al. Evidence-based monitoring and evaluation of the faith-based approach to HIV prevention among Christian and Muslim youth in Wakiso district in Uganda. Af Health Sci. 2012;12(2):119–28. doi:10.4314/ahs.v12i2.7.
Harper GW, Fernandez IM, Bruce D, Hosek SG, Jacobs RJ. The role of multiple identities in adherence to medical appointments among gay/bisexual male adolescents living with HIV. AIDS Behav. 2013;17(1):213–23. doi:10.1007/s10461-011-0071-3.
Bruce D, Harper GW, Suleta K. Sexual risk behavior and risk reduction beliefs among HIV-positive young men who have sex with men. AIDS Behav. 2012. doi:10.1007/s10461-012-0155-8.
Bruce D, Harper GW, Fernandez MI. The adolescent medicine trials network for HIV/AIDS I. Heavy marijuana use among gay and bisexual male emerging adults living with HIV/AIDS. J HIV/AIDS Soc Ser. 2013;12(1):26–48. doi:10.1080/15381501.2012.735171.
Jacobson JO, Creswell J, Guardado ME, Lee JC, Isabel Nieto A, Paz-Bailey G. Coverage of HIV prevention components among people with long-standing diagnosed HIV infection in El Salvador. Sex Transm Dis. 2012;39(9):694–700. doi:10.1097/OLQ.0b013e3182593b33.
Rice E, Lester P, Flook L, Green S, Valladares ES, Rotheram-Borus MJ. Lessons learned from “integrating” intensive family-based interventions into medical care settings for mothers living with HIV/AIDS and their adolescent children. AIDS Behav. 2009;13(5):1005–11.
Rotheram-Borus MJ, Murphy DA, Miller S, Draimin BH. An intervention for adolescents whose parents are living with AIDS. Clin Child Psychol Psychiatry. 1997;2(2):201–19.
Traeger L, O'Cleirigh C, Skeer MR, Mayer KH, Safren SA. Risk factors for missed HIV primary care visits among men who have sex with men. J Behav Med. 2012;35(5):548–56. doi:10.1007/s10865-011-9383-z.
Safren SA, O’Cleirigh C, Skeer MR, Driskell J, Goshe BM, Covahey C, et al. Demonstration and evaluation of a peer-delivered, individually-tailored, HIV prevention intervention for HIV-infected MSM in their primary care setting. AIDS Behav. 2011;15(5):949–58.
Knauz RO, Safren SA, O’Cleirigh C, Capistrant BD, Driskell JR, Aguilar D, et al. Developing an HIV-prevention intervention for HIV-infected men who have sex with men in HIV care: project enhance. AIDS Behav. 2007;11(1):117–26.
Safren SA, O'Cleirigh CM, Skeer M, Elsesser SA, Mayer KH. Project enhance: a randomized controlled trial of an individualized HIV prevention intervention for HIV-infected men who have sex with men conducted in a primary care setting. Health Psychol. 2013;32(2):171–9. doi:10.1037/a0028581.
O’Cleirigh C, Skeer M, Mayer KH, Safren SA. Functional impairment and health care utilization among HIV-infected men who have sex with men: the relationship with depression and post-traumatic stress. J Behav Med. 2009;32(5):466–77.
Pence BW, Mugavero MJ, Carter TJ, Leserman J, Thielman NM, Raper JL, et al. Childhood trauma and health outcomes in HIV-infected patients: an exploration of causal pathways. J Acquir Immune Defic Syndr. 2012;59(4):409–16. doi:10.1097/QAI.0b013e31824150bb.
Pence BW, Reif S, Whetten K, Leserman J, Stangl D, Swartz M, et al. Minorities, the poor, and survivors of abuse: HIV-infected patients in the US deep South. South Med J. 2007;100(11):1114–22. doi:10.1097/01.smj.0000286756.54607.9f.
Leserman J, Whetten K, Lowe K, Stangl D, Swartz MS, Thielman NM. How trauma, recent stressful events, and PTSD affect functional health status and health utilization in HIV-infected patients in the south. Psychosom Med. 2005;67(3):500–7. doi:10.1097/01.psy.0000160459.78182.d9.
Lunze K, Cheng DM, Quinn E, Krupitsky E, Raj A, Walley AY, et al. Nondisclosure of HIV infection to sex partners and alcohol's role: a Russian experience. AIDS Behav. 2013;17(1):390–8. doi:10.1007/s10461-012-0216-z.
Raj A, Kidd JD, Cheng DM, Coleman S, Bridden C, Blokhina EA, et al. Associations between partner violence perpetration and history of STI among HIV-infected substance using men in Russia. AIDS Care. 2013;25(5):646–51. doi:10.1080/09540121.2012.722188.
Tyurina A, Krupitsky E, Cheng DM, Coleman SM, Walley AY, Bridden C, et al. Is cannabis use associated with HIV drug and sex risk behaviors among Russian HIV-infected risky drinkers? Drug Alcohol Depend. 2013. doi:10.1016/j.drugalcdep.2013.01.009.
Acknowledgments
The authors thank Erika Sevetson, MS, for her assistance with determining the search terms and profile for the current meta-analysis and the study authors who provided additional data to assist our coding and analyses of their studies.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Blair T. Johnson received support for travel to meetings for the study or otherwise from NIH/NIAAA (R01-AA021355).
Lori A. J. Scott-Sheldon, Paige Walstrom, Kate B. Carey, Michael P. Carey, and MASH Research Team (i.e., Chiao-Wen Lan, Matthew Pina, Xinmiao Tan) declare that they have no conflict of interest.
Funding
Research reported in this paper was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under award number R01 AA021355 to Lori A. J. Scott-Sheldon. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Meta-Analyses of Alcohol, Sexual Risk Behaviors, and HIV (MASH) team members who assisted with this project included Chiao-Wen Lan, BS, BA, Matthew Pina, BS, and Xinmiao Tan, BMed.
Rights and permissions
About this article
Cite this article
Scott-Sheldon, L.A.J., Walstrom, P., Carey, K.B. et al. Alcohol Use and Sexual Risk Behaviors among Individuals Infected with HIV: A Systematic Review and Meta-Analysis 2012 to Early 2013. Curr HIV/AIDS Rep 10, 314–323 (2013). https://doi.org/10.1007/s11904-013-0177-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11904-013-0177-5