
Abstract
Background
While evidence of improved renal function following gastric bypass exists, pre-operative predictors of this improvement are not completely known.
Objectives
To assess the glomerular filtration rate (GFR) 1 year after Roux-en-Y gastric bypass (RYGB) and to identify pre-operative predictors associated with the improvement of renal function.
Methods
A historical cohort study, which included 109 obese patients before and 12 months after RYGB, was classified into subgroups according to GFR (normofiltration, hypofiltration (GFR < 5th percentile), and hyperfiltration (GFR > 95th percentile)). The 5th and 95th percentiles were 90 and 120 mL/min/1.73 m2, respectively. The primary outcome was the variation of GFR (%GFR) estimated by the Chronic Kidney Disease - Epidemiology Collaboration (CKD-EPI) formula, calculated using serum creatinine, ethnicity, and gender.
Results
The mean age was 38.3 ± 10.3 years and 77% were female; 52.3% presented hypertension and 27.5% type 2 diabetes. One year after surgery, the mean BMI decreased from 36.7 ± 3.6 to 28.8 ± 3.3 kg/m2 (p < 0.001). Pre-surgically, 37.6% presented hypofiltration, 47.7% normofiltration, and 14.7% hyperfiltration. The overall GFR increased from 95.5 ± 19 to 104 ± 16.4 mL/min (10.9%) (p < 0.001). The overall post-surgical %GFR was negatively correlated with the pre-surgical GFR (R = − 0.687; p < 0.001). In the hypofiltration and normofiltration subgroups, the post-surgical %GFR was negatively correlated with age (R = − 0.328, p = 0.036; and R = − 0.355, p = 0.004, respectively) and pre-surgical GFR (R = − 0.436, p = 0.04; and R = − 0.528, p < 0.001, respectively).
Conclusion
RYGB led to a significant improvement in renal function, mainly among patients with a worse pre-operative renal function. In the hypofiltration and normofiltration subgroups, a younger age was associated with better outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of obesity has been rising steadily over the last decades, becoming a public health problem [1]. Obesity is associated with a deleterious influence on renal function, and this detrimental effect is linked to several pathophysiological mechanisms, which are associated with both overweight itself and obesity-related co-morbidities, such as diabetes mellitus, hypertension, and dyslipidemias [2, 3]. As a consequence, obesity can alter renal function and predispose to various renal changes, such as diabetic nephropathy, hypertensive nephrosclerosis, and focal and segmental glomerulosclerosis [4]. The mechanism by which these alterations are established may be summarized through a didactic form as the occurrence of the phenotypes of glomerular hyperperfiltration and hypofiltration, which may progress to chronic kidney disease (CKD) and eventually to end-stage renal disease. Glomerular hyperfiltration is an absolute increase in glomerular filtration rate (GFR), necessarily more than two standard deviations above the mean GFR of a healthy population. It may occur in healthy individuals in response to high protein loading; however, it may reflect a long-term loss of renal reserve and is considered an early marker of development of hypofiltration and eventually late-stage CKD. On the other hand, glomerular hypofiltration is a state of an already established decrease of GFR (more than two standard deviations below the mean GFR of a healthy population) [5].
The exact mechanisms by which obesity is associated with renal damage are not fully understood [6]. The adipose tissue, mainly through its visceral component, plays a relevant role in this context, acting as a metabolically active tissue and directly involved in several metabolic pathways responsible for a number of changes and diseases that accompany obesity [7, 8]. Bariatric surgery has become the gold standard treatment for refractory morbid obesity, as it leads to a significant and sustained long-term weight loss, in addition to leading to improved renal function; however, the exact mechanisms by which this improvement occurs are not completely known [9].
The objectives of this study were to assess the evolution of estimated GFR in obese individuals 1 year after Roux-en-Y gastric bypass (RYGB) and to identify pre-operative predictors associated with improvement of renal function.
Methods
Study Design
This is a historical cohort study based on a descriptive analysis of a prospectively collected database, which evaluated patients who consecutively underwent RYGB in the pre-operative period and 12 months after surgery in a public tertiary university hospital from September 2016 through August 2017. The study was approved by the local committee of ethics in research under the reference number 2.237.978/Unicamp and all participants signed an informed consent form.
Study Population
Inclusion criteria were as follows: (1) obese patients who underwent RYGB; (2) of both genders; (3) aged 18 through 70 years old; (4) minimum follow-up of 12 months. Exclusion criteria were as follows: (1) CKD under dialysis; (2) smoking; (3) incomplete medical records; (4) use of nephrotoxic drugs; (5) vulnerable groups (underaged, people with mental disabilities, institutionalized individuals); (6) previous or current history of specific nephropathies not related to obesity; (7) previous or current history of obstructive urinary lithiasis; (8) history of previous renal surgery.
Of an initial population of 140 patients undergoing surgery, 31 were excluded, leaving a study population of 109 patients. The reasons for exclusion were as follows: follow-up of less than 12 months (n = 18), incomplete records (n = 5), smoking (n = 5), obstructive urinary lithiasis (n = 2), and use of nephrotoxic medication (n = 1).
All patients who undergo bariatric surgery at this institution participate in a pre-operative weight loss program that lasts from 4 to 12 weeks and is comprised of weekly consultations conducted by a multidisciplinary team. Patients undergo surgery when an average pre-operative weight loss of 10 to 20% is achieved [10]. The pre-operative clinical and laboratory data considered for the analyses were obtained after this weight loss period, immediately prior to the surgical procedure.
Indication and Surgical Technique
Surgery was indicated according to the National Institutes of Health Consensus criteria (body mass index (BMI) ≥ 40 kg/m2 or BMI ≥ 35 kg/m2) with obesity-related co-morbidities. The main features of the RYGB were a 30-mL gastric pouch, a 100-cm biliopancreatic loop, a 150-cm alimentary limb, and a common channel comprised of the remainder of the small intestine. All procedures were performed by the same surgical team and through an open approach.
Variables
The variables pre-operatively analyzed were age, gender, and self-reported ethnicity. Before and after surgery, BMI, serum creatinine, serum urea, and estimated GFR using the Chronic Kidney Disease - Epidemiology Collaboration (CDK-EPI) formula were assessed. One year after surgery, the percentage of variation of CKD-EPI was calculated.
The CKD-EPI formula was calculated according to the proposition of Levey et al. [11]. It was used to evaluate the estimated glomerular filtration rate and has the advantage of not taking into account the patient’s weight since, in obese patients, the formulas that consider this variable tend to overestimate the true values of GFR [12]. The CKD-EPI equation, expressed as a single equation, is:
GFR = 141 × min(Scr/κ, 1)α × max(Scr/κ, 1)−1.209 × 0.993Age × 1.018 [if female] × 1.159 [if black]
Scr is serum creatinine (mg/dL), κ is 0.7 for females and 0.9 for males, α is − 0.329 for females and − 0.411 for males, min indicates the minimum of Scr/κ or 1, and max indicates the maximum of Scr/κ or 1.
Subgroup Classification
Patients were classified into 3 groups according to their GFR at baseline: (1) normofiltration (GFR between the 5th and 95th percentiles of the study population), 90–120 mL/min/1.73 m2; (2) hypofiltration (GFR below the 5th percentile), GFR < 90 mL/min/1.73 m2; (3) hyperfiltration (GFR above the 95th percentile), GFR > 120 mL/min/1.73 m2 [13].
Outcomes
The primary outcome was the percentage of variation of GFR over time and the secondary outcomes were %EWL and changes in the subgroup classification of the study population according to renal function.
Statistical Analysis
Comparison of proportions was performed using the chi-square test or Fisher exact test, when necessary. Normality was assessed using the Shapiro-Wilk test. Comparisons of continuous or ordinal measurements between the two moments of assessment were performed using the Mann-Whitney test. The Kruskal-Wallis test was used to compare continuous measures between more than two independent groups and the Tukey post-test was used to identify which groups presented significant differences. Associations between continuous variables were calculated using linear regression models. Multiple regression models were used to perform an adjustment for possible confounding variables. The level of significance was set at 5% (p < 0.05).
Results
Demographic Data
Patients presented a mean age of 38.3 ± 10.3 years and 77% were female. As to self-declared ethnicity, 79 were white (72.5%) and 30 black or brown (27.5%); 52.3% presented hypertension and 27.5% presented type 2 diabetes (16.7% under use of insulin alone, 76.7% using oral antidiabetics, and the remaining on both types of medication).
Renal Function Outcomes
Serum Creatinine, Urea, and Glomerular Filtration Rate
One year after surgery, there were significant reductions in serum creatinine (0.84 ± 0.2 versus 0.75 ± 0.2 mg/dL; p < 0.001) and urea levels (31.7 ± 10.9 versus 27 ± 8 mg/dL; p < 0.001); the estimated GFR increased significantly from 95.5 ± 19 to 104 ± 16.4 mL/min (p < 0.001). The mean post-operative percentage of variation in GFR was 10.9%. There were no significant differences in GFR variation between patients with or without T2D (p = 0.2) and with or without hypertension (p = 0.7).
Weight Loss Outcomes
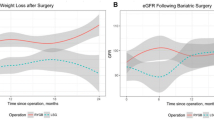
One year after surgery, there were significant reductions in weight (99.9 ± 13.5 versus 79.8 ± 10.9 kg; p < 0.001) and BMI (36.7 ± 3.6 versus 28.8 ± 3.3 kg/m2; p < 0.001). The mean %EWL was 79.2 ± 26.1% and the mean %TWL was 23.1 ± 9.1%.
Correlation Analysis
The overall variation of the estimated GFR showed significant negative correlations with the pre-operative value of GFR (R = − 0.687; p < 0.001) and age (R = − 0.215; p = 0.018); i.e., the lower the pre-operative GFR and age, the greater the percent variation in GFR. There were significant positive correlations between the GFR variation and the pre-operative values of creatinine (R = 0.676; p < 0.001) and urea (R = 0.417; p < 0.001); i.e., the higher the pre-operative levels of creatinine and urea, the greater the percentage of change in GFR. There were no significant correlations between GFR variation and %EWL (R = − 0.0243; p = 0.8),%TWL (R = 0.002; p = 1), and pre-operative BMI (R = 0.06, p = 0.5). Figure 1 presents graphical representations of the correlation analyses between the percentage variation of GFR and the variables studied. After an adjustment for age, gender, and pre-operative BMI, pre-operative GFR was detected as independently correlated with the variation of GFR (R = − 0. 678; p < 0.001), as well as age (R = − 0.211; p = 0.02).

Correlations between the studied variables and the overall percent variation of estimated glomerular filtration rate over time. GFR, glomerular filtration rate; %EWL, percentage of excess weight loss; BMI, body mass index. Bold indicates statistical significance
Subgroup Analysis
Baseline Classification and Post-Operative Evolution
Before surgery, hypofiltration was present in 37.6% of patients, whereas 47.7% presented normofiltration and 14.7% hyperfiltration. Patients with pre-operative hypofiltration had an average increase in GFR of 20.5 ± 17.3%, whereas among those with hyperfiltration there was an average reduction of 5.9 ± 26% after surgery. Among patients with pre-operative normofiltration, there was an average increase of 6.6 ± 8.4% after surgery. The GFR variation was significantly higher among the subjects with hypofiltration than the other two groups (p < 0.001). The GFR increased significantly in the pre-operative hypofiltration (75.8 ± 11.6 versus 90.6 ± 15.3; p < 0.001) and normofiltration groups (102.4 ± 8 versus 108.9 ± 8.3; p = 0.004); in the pre-operative hyperfiltration group, there was a significant reduction in GFR (123.3 ± 2 versus 118.2 ± 9.8; p < 0.001). Figure 2 shows the comparisons between pre- and post-operative GRF in the three subgroups.

Comparisons between pre- and post-operative estimated glomerular filtration rates, according to subgroup
Table 1 shows the complete comparison among the anthropometric, clinical, and biochemical characteristics of each group before and after surgery.
Correlation Analysis per Subgroup
Hypofiltration
There were significant negative correlations of the percentage of variation of GFR with pre-operative GFR (R = − 0.435; p < 0.001) and age (R = − 0.328; p = 0.036), i.e., the lower the pre-operative age and GFR, the greater the GFR variation, as well as a significant positive correlation with baseline creatinine (R = 0.326, p = 0.0374), i.e., the higher the pre-operative creatinine level, the higher the GFR variation. After an adjustment for age, gender, and pre-operative BMI, pre-operative GFR was independently associated with the GFR variation (R = − 0.369; p = 0.018).
Normofiltration
There were significant negative correlations between the GFR variation and the pre-operative GFR (R = − 0.529; p < 0.001) and age (R = − 0.355; p = 0.004), the lower the pre-operative GFR and age, the greater the GFR variation, and a significant positive correlation with the baseline creatinine (R = 0.489; p < 0.001), i.e., the higher the pre-operative creatinine level, the greater the GFR variation. After an adjustment for age, gender, and pre-operative BMI, pre-operative GFR was independently associated with the GFR variation (R = − 0.59; p < 0.001), as well as age (R = − 0.355; p = 0.003).
Hyperfiltration
There were no significant correlations between any of the studied variables.
Discussion
The current study demonstrated that pre-operative markers of renal function were the main predictors of a greater alteration in renal function after surgery, i.e., the worse the pre-operative renal function in individuals with hypofiltration (without terminal disease or under dialysis), the better the outcomes after surgery. Magalhães et al. [14] observed similar findings, confirming that the improvement was more significant among individuals with worse pre-operative renal function; Ngoh et al. [15] observed a reversal of both hypofiltration and glomerular hyperfiltration after bariatric surgery. However, unlike the current study, they showed a significant correlation between weight loss and improvement of renal function. Favre et al. [16] demonstrated that a pre-operative inflammatory state correlated significantly with the improvement of hyperfiltration. Hou et al. [17], analyzing 233 obese patients before and 1 year after bariatric surgery, observed results comparable with those of the present study. In addition, von Scholten et al. [18] observed that body weight reduction is associated with a reduction in GFR, but puts into question the role of creatinine in calculating the values, suggesting that creatinine changes may be associated with the loss of lean mass in the post-operative period, thus overestimating the calculations of GFR.
In a meta-analysis of 23 studies evaluating the effects of bariatric surgery on renal function parameters, Bilha et al. [19] observed that the creatinine values did not change in some studies; however, the GFR decreased in patients with hyperfiltration and increased in patients who had low values of GFR pre-operatively. The latter finding was corroborated by our findings; the lower the pre-operative GFR values, the greater the variation found after the procedure. Another systematic review and meta-analysis of Li et al. [20] evaluated 30 studies and observed a statistically significant reduction in the frequency of hyperfiltration, albuminuria, and proteinuria after bariatric surgery.
In the present study, the volume of weight loss was not significantly associated with improvement in renal function. This finding was also identified by the meta-analysis of Bilha et al. [19], which concluded that the increase in GFR was a consequence of changes in several parameters such as glycemia, urea, and creatinine.
The key findings of the present study were the improvement of renal function both in individuals with hypofiltration and in those with hyperfiltration, as well as the identification of a younger age, and a more deteriorated baseline renal function as predictors of better results in individuals with hypofiltration and normofiltration. These results demonstrate that, in individuals such as those in the study population, that is, without end-stage renal failure, a precocious surgical indication leads to great benefits even in scenarios of significant deterioration of renal function.
The present study presents limitations that must be taken into consideration. A point to be considered is the fact that the decrease in serum creatinine levels may be associated to some extent with the surgically induced weight loss-related sarcopenia, making its use somewhat misleading. The GFR estimation model was appropriate for this population study model, but it does not present the same accuracy of direct measurements through total urine collection in 24 h and calculation of clearance, despite their expensiveness and difficult execution; moreover, the changes in body composition after surgery may also have biased our findings to some degree [18]. Moreover, the ethnically admixtured nature of our population and the usage of a self-declared ethnic classification, as the Brazilian law requires, for the calculation of GFR is also problematic. Nonetheless, the findings presented in the current study were consistent, corroborating and expanding several previous observations of other authors.
Conclusion
RYGB was associated with a significant improvement in renal function; the overall improvement was more pronounced among those with a worse baseline renal function. In individuals with pre-operative hypofiltration or normofiltration, a younger age was associated with a more pronounced post-operative renal function improvement.
References
Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019;92:6–10.
Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382(9889):339–52.
Ecder T. Early diagnosis saves lives: focus on patients with chronic kidney disease. Kidney Int Suppl. 2011;3(4):335–6.
Kopple JD. Obesity and chronic kidney disease. J Ren Nutr. 2010;20:S29–30.
Tsuboi N, Okabayashi Y, Shimizu A, et al. The renal pathology of obesity. Kidney Int Rep. 2017;2(2):251–60.
Eckardt KU, Coresh J, Devuyst O, et al. Evolving importance of kidney disease: from subspecialty to global health burden. Lancet. 2013;382(9887):158–69.
Sitticharoon C, Chatree S, Churintaraphan M. Expressions of neuropeptide Y and Y1 receptor in subcutaneous and visceral fat tissues in normal weight and obese humans and their correlations with clinical parameters and peripheral metabolic factors. Regul Pept. 2013;185:65–72.
LeRoux CW, Welbourn R, Werling M, et al. Gut hormones as mediators of appetite and weight loss after Roux-en-Y gastric bypass. Ann Surg. 2007;246(5):780–5.
LeRoux CW, Heneghan HM. Bariatric surgery for obesity. Med Clin North Am. 2018;102(1):165–82.
Chaim EA, Pareja JC, Gestic MA, et al. Pre-operative multidisciplinary program for bariatric surgery: a proposal for the Brazilian public health system. Arq Gastroenterol. 2017;54(1):70–4.
Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Matsushita K, Mahmoodi BK, Woodward M, et al. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA. 2012;307:1941–51.
Okada R, Yasuda Y, Tsushita K, et al. The number of metabolic syndrome components is a good risk indicator for both early- and late-stage kidney damage. Nutr Metab Cardiovasc Dis. 2014;24(3):277–85.
Magalhães DSC, Pedro JMP, Souteiro PEB, et al. Analyzing the impact of bariatric surgery in kidney function: a 2-year observational study. Obes Surg. 2019;29(1):197–206.
Ngoh CLY, So JBY, Tiong HY, et al. Effect of weight loss after bariatric surgery on kidney function in a multiethnic Asian population. Surg Obes Relat Dis. 2016;12(3):600–5.
Favre G, Anty R, Canivet C, et al. Determinants associated with the correction of glomerular hyper-filtration one year after bariatric surgery. Surg Obes Relat Dis. 2017;13(10):1760–6.
Hou CC, Shyu RS, Lee WJ, et al. Improved renal function 12 months after bariatric surgery. Surg Obes Relat Dis. 2013;9(2):202–6.
von Scholten BJ, Persson F, Svane MS, et al. Effect of large weight reductions on measured and estimated kidney function. BMC Nephrol. 2017;18(1):52.
Bilha SC, Nistor I, Nedelcu A, et al. The effects of bariatric surgery on renal outcomes: a systematic review and meta-analysis. Obes Surg. 2018;28(12):3815–33.
Li K, Zou J, Ye Z, et al. Effects of bariatric surgery on renal function in obese patients: a systematic review and meta analysis. PLoS One. 2016;11(10):e0163907.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Statement of Human and Animal Rights
The study was approved by the local committee of ethics in research under the reference number 2.237.978/Unicamp and all participants signed an informed consent form. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Garcia, M.S., Calderoni, D.R., Jimenez, L.S. et al. Renal Function 1 Year After Bariatric Surgery: Influence of Roux-en-Y Gastric Bypass and Identification of Pre-Operative Predictors of Improvement. OBES SURG 30, 860–866 (2020). https://doi.org/10.1007/s11695-019-04249-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-04249-w