
Abstract
Background and Aims
Bariatric surgeries such as gastric banding (LAGB), gastric bypass (RYGB), vertical banded gastroplasty (VBG), and sleeve gastrectomy (LSG) decrease body weight in morbid obesity, leading to the resolution of coexisting diabetes mellitus and arterial hypertension in the majority of cases as well as improvements of renal function and liver steatosis. BS (LAGB, RYGB, VBG, and LSG) also reduce incident cases of diabetes, of cardiovascular diseases, and of cancer; these therapeutic and preventive effects on comorbidities of obesity have not been analyzed for malabsorptive surgeries such as biliopancreatic diversion (BPD) or biliointestinal bypass (BIBP). The aim of this study was to analyze the incidence of comorbidities, i.e., diabetes, cardiovascular diseases, and cancer, in obese subjects undergoing BPD and BIBP, in comparison with standard medical treatment of obesity.
Patients and Methods
Medical records of 1983 obese patients (body mass index (BMI) > 35 kg/m2, aged 18–65 years, undergoing surgery (n = 472, of which 111 with diabetes) or medical treatment (n = 1511, of which 422 with diabetes), during the period 1999–2008 (visit 1)) were collected; incident cases of comorbidities were ascertained through December 31, 2016.
Results
Observation period was 12.0 ± 3.48 years (mean ± SD). Compared to non-surgical patients matched for age, body mass index, and blood pressure, malabsorptive surgeries were associated with reduced new incident cases of diabetes (p = 0.001), cardiovascular diseases (p = 0.001), hyperlipidemia (p = 0.001), oculopathy (p = 0.021), and cancer (p = 0.001). The preventive effect of BS was similar in both nondiabetic and diabetic patients for cardiovascular diseases and hyperlipidemia (both p = 0.001). The preventive effect was significant in nondiabetic subjects for coronary heart disease and for cancer, not significant in diabetic subjects.
Conclusion
Patients undergoing malabsorptive bariatric surgery show less incident cases of diabetes, cardiovascular diseases, hyperlipidemia, oculopathy, and cancer than controls receiving medical treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bariatric surgeries decrease body weight in morbid obesity and lead to resolution of diabetes mellitus and of arterial hypertension [1,2,3,4,5,6,7,8,9,10,11] and improvement of renal function [12] and of liver steatosis [13], with differences in efficacy when employing different surgical techniques, at least in terms of weight loss and resolution of diabetes mellitus [1, 2].
Bariatric surgeries reduce long-term mortality (all-cause and cardiovascular (CV) mortality) [9,10,11,12,13,14], with an effect that seems unrelated to the surgical techniques that are employed.
Also interesting is the demonstration of prevention of incident cases of diabetes [3, 9, 10, 15], of CV diseases [4, 6, 8, 9, 11], of microvascular complications of diabetes mellitus [16,17,18,19,20], and of cancer [21,22,23,24,25,26,27]; however, prevention of comorbidities and early death has been evaluated for gastric banding (LAGB), gastric bypass (RYGB), and vertical banded gastroplasty (VBG), with some recent data for sleeve gastrectomy (LSG, the most used technique nowadays [10]).
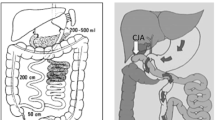
Prevention of diabetes mellitus, cardiovascular diseases, and cancer has not been evaluated for mainly malabsorptive bariatric surgeries such as biliopancreatic diversion (BPD) or biliointestinal bypass (BIBP). BPD [28] and BIBP [29,30,31] are two surgical techniques of great efficacy, but no data are available on their effect in prevention of comorbidities. Biliopancreatic diversion (BPD), a malabsorptive surgery, is considered the most effective bariatric technique in terms of weight loss and metabolic effects [1, 2]. Biliointestinal bypass (BIBP) is another malabsorptive bariatric technique, less frequently used than other surgical techniques for the treatment of morbid obesity, highly effective in inducing weight loss and in improving metabolic control [29,30,31].
Our aim was to analyze the incidence of comorbidities, i.e., diabetes mellitus, CV diseases, oculopathy, hyperlipidemia, and cancer, in obese subjects undergoing BPD (Scopinaro method [28]) and BIBP, in comparison with standard weight loss medical treatment of obesity.
Patients and Methods
Istituto Multimedica (Milan, Italy), Ospedale Civile (Magenta, Milan, Italy), INCO-Istituto Clinico Sant’Ambrogio (Milan, Italy), and Istituto Humanitas Gavazzeni (Bergamo, Italy) offer surgical and medical treatment of obesity. All institutions are connected with Università degli Studi di Milano, Milan, Italy, and belong to the LAGB10 study group [8], a network of physicians and surgeons interested in the care of obesity with bariatric surgeries and dietary/medical treatment in the Lumbardy Region (Italy). BPD [28] and BIBP [29] have been performed here since 1998, according to NIH guidelines [32], and virtually, all BPD and BIBP procedures are performed in these four institutions in the Lumbardy Region (Italy).
We considered all obese patients (body mass index (BMI) > 40 kg/m2 alone or > 35 kg/m2 in the presence of comorbidities) aged 18–65 years, seeking medical advice and referred to the outpatient obesity clinics during the period 1999–2008 (first visit), undergoing thereafter BPD or BIBP, or medical treatment. After evaluation of indications and contraindications, patients were offered BPD or BIBP; several patients declined the offer, mainly because of reluctance, lack of comprehension of the benefits in the decrease of body weight, fear of surgery and its complications, and inability or unwillingness to comply with the anticipated change of lifestyle habits or with the program of scheduled visits. Patients who declined surgery for any reason, but agreed to be followed up during medical treatment, were considered controls. All patients were treated with diet and received standard care (education on eating behaviors, advice on diet and exercise, plus drug treatment for diabetes and hypertension when present).
The study protocol was approved by local Ethics Committees in 2015 (Coordinating Center: Ospedale San Paolo, Comitato Etico Interaziendale di Milano Area A, official approval SC: 2015 ST 125). Being a retrospective study, informed consent was obtained from all individual participants included in the study who could be reached by interview, phone, or letter. From the medical records, birthdate and age, baseline anthropometric data (height, weight, BMI), systolic and diastolic blood pressure, and heart rate, metabolic data (fasting blood glucose, HbA1c (%), cholesterol, HDL and LDL cholesterol, triglycerides, transaminases AST and ALT, creatinine and estimated glomerular filtration rate (eGFR, Modified Diet in Renal Disease Calculation Equation) [33]), current treatments, clinical evidence of coronary heart disease (CHD), retinopathy, were derived and tabulated. Diagnosis of diabetes mellitus and of coronary heart disease (CHD) was based on medical records [8].
Outcomes
The presence of exemptions coded according the ICD-10 codes for diabetes mellitus, cardiovascular diseases, and cancer was searched in the Lumbardy Region Health Administrative Database among obese patients (diabetic and nondiabetic) undergoing bariatric malabsorptive surgeries vs obese patients undergoing medical and dietary treatments.
Procedures
Patients were identified through personal identification codes; codes were entered the Regional Lumbardy Administrative Database, and it was possible to ascertain whether patients were alive, were dead, or had moved to other regions. Table 1 shows clinical details of patients in the study. The National Health System (NHS) in Italy covers more than 95% of all hospital admissions, medical and surgical procedures, and medical expenses of citizens [34] (Italian Survey 2012). A Regional Lumbardy Administrative Database contains since 1988 all pertinent data of all citizens. For each citizen, four databases are linked through a single identification code, and the following databases include: (a) an archive of residents who receive NHS assistance, reporting demographic and administrative data; (b) diagnosis at discharge from public or private hospitals of the Region; (c) outpatient drug prescriptions reimbursable by the NHS, and (d) outpatient visits, including visits in specialist ambulatory care and diagnostic laboratories accredited by the NHS. Full details of the procedures are reported elsewhere, as this procedure has been previously validated [8, 35]. In the Italian National Health System, development of chronic diseases (diabetes mellitus, liver and cardiovascular diseases, cancer, selected thyroid, renal, and lung diseases) yields the right to exemption from medical charges (exemptions), which means life-long free prescriptions and examinations for the above diseases. Therefore, exemptions are considered the demonstration of new cases (incident) of chronic diseases.
For each patient, exemptions after first visit were identified and dated. Through registries of surgeons and the Regional Lumbardy Administrative Database it was also possible to retrieve patients who had new bariatric surgery procedures. Through the health districts (ASL) patients belonged to, it was possible to track nature of exemptions. Data from health districts were cross-checked with data from the Regional Lumbardy Administrative Database, to rule out inconsistencies and possible delays in transcriptions. The limit date of December 31, 2016, was established for all patients for exemptions. Exemptions were coded according to ICD-10 codes.
Statistical Analysis
Data are shown as mean values (± SD) for continuous variables, or absolute numbers and frequencies for discrete variables. Data were analyzed for normality through the Kolmogorov-Smirnov equality-of-distributions test; since in some instances distribution was not Gaussian, we used rank sum test to compare variables between the two groups of patients, and the signed rank test for repeated analyses. Frequencies were compared with the Fisher exact test. Since the number of no-surgery patients greatly exceeded the number of surgery patients, we tried to make patients comparable for most variables in order to obtain meaningful data. Surgery and no-surgery patients were matched (nondiabetic and diabetic patients separately, 1:3 for nondiabetic patients, and 1:4 for diabetic patients). Matching was made for age, systolic and diastolic blood pressure, and body mass index. Patients were not matched for sex, as female sex is commonly more represented among surgery patients [1]. A multivariable analysis of risk factors for development of comorbidities was performed (logistic regression analysis) to assess the independent role of variables significant at univariate analysis: age, sex, presence of diabetes, presence of CHD, systolic blood pressure, eGFR, BMI. A p value < 0.05 was considered statistically significant. Statistical analyses were performed with STATA 12.0 for Macintosh.
Power Calculation and Sample Size
Being a retrospective study, power calculation and sample size were only calculated to understand if the study was meaningful. Given the high efficacy of bariatric surgeries in the long-term prevention of diabetes and of cancer [9, 22], we estimated that the occurrence of 100 exemptions in 500 bariatric surgery subjects and 600 exemptions in 1500 subjects undergoing dietary and medical treatment would be required to detect significant differences in the outcomes between the two groups [36, 37]. This manuscript was prepared following the guidelines of the STROBE statement [38].
Results
Median age of the whole cohort was 44 years. Patients receiving surgery differed from controls for sex (p = 0.01), for heart rate (p = 0.02), for Hab1c and duration of diabetes (p = 0.02 and p = 0.03, respectively), for cholesterol (p = 0.05), and for AST (0.01); all remaining variables had similar values. Patients receiving BPD (316, 73/242 men/women) and BIBP (156, 45/111 men/women) only differed for systolic BP (131.3 ± 13.05 vs 135.9 ± 12.14 mmHg, p = 0.003), diastolic BP (79.9 ± 7.33 vs 83.9 ± 9.52 mmHg, p = 0.0404), cholesterol (209.7 ± 22.46 vs 192.8 ± 33.43 mg/dl, p = 0.0180), heart rate (81.0 ± 6.81 vs 85.6 ± 7.31 bpm, p = 0.0002), and frequency of CHD (4/311 vs 11/156, χ2 = 11.31, p = 0.001); all remaining variables had similar values. The baseline clinical and metabolic data of patients in the study after matching for age, body mass index, and blood pressure are shown in Table 1. During the first year of follow-up, there were three deaths among surgery patients, which we can assume as surgery-related, and eight deaths among controls (NS).
Incident cases of diabetes mellitus, CV diseases (CHD and hypertension), hyperlipidemia, oculopathy (retinopathy and glaucoma), and cancer were all significantly decreased in surgery patients as compared with medically treated controls, with no significant differences for liver and kidney diseases (Table 2). Interestingly also, when analyzing separately incident cases of comorbidities between BPD and BIBP, there were no differences between the two surgical groups (diabetes mellitus 1/238 vs 1/123, NS; hypertension 15/279 vs 4/106, NS; coronary heart disease 24/312 vs 7/145, NS; CV diseases 35/279 vs 6/106, NS; hyperlipidemia 1/316 vs 0/156, NS; oculopathy 2/316 vs 0/156, NS; cancer 11/316 vs 3/156, NS); only patients without pre-existing conditions were considered. Prevention of hypertension, CV diseases, hyperlipidemia, and cancer by BPD and BIBP was significant also when nondiabetic and diabetic patients were considered separately, while prevention of CHD was only significant in nondiabetic patients, undergoing BPD or BIBP as compared with the control group.
We also performed univariate and multivariate analyses of risk factors for the development of comorbidities (incident cases of diabetes, hypertension, CHD, oculopathy (retinopathy plus glaucoma), and cancer (Table 3)). Only risk factors for incident comorbidities significantly associated with bariatric surgery were considered. At univariate analysis, surgery (negatively) and age (positively) were significantly associated with all comorbidities, while female sex was negatively associated with diabetes, hypertension, and CHD; systolic BP was positively associated with diabetes and with CHD. At multivariable analysis, age was a risk factor for all comorbidities, and surgery was a significant protective risk factor for all comorbidities except for CHD; systolic BP was a significant risk factor for diabetes and hypertension, sex was a protective significant risk factor for CHD, and diabetes was a risk factor for oculopathy.
Discussion
To our knowledge, this is the first long-term study on development of comorbidities in obese subjects undergoing BPD and BIBP, in comparison with obese subjects receiving standard medical treatment of obesity. We observed a lower incidence of diabetes, cancer, CV diseases, hyperlipidemia, and oculopathy in subjects undergoing BPD and BIBP than in subjects receiving standard medical treatment of obesity. BPD and BIBP had a superimposable effect.
Prevention of diabetes has been described for other surgical techniques, especially for RYGB, VBG, and LAGB, and recently for LSG [3, 9, 10, 15], and prevention of microangiopathic diabetic complications has been demonstrated for most bariatric surgeries [16,17,18,19,20]. Prevention of arterial hypertension and of CV diseases has also been described for the above bariatric surgical techniques [4, 6, 8, 9, 11]. Prevention of cancer has been described for the above techniques in large studies and has been the subject of meta-analyses [21,22,23,24,25,26,27].
Mechanistic interpretations have been offered for these effects, with a pivotal role for weight loss, accompanied by additional effects of bariatric surgery [39]; for instance, changes of intestinal microbiota, accompanied by change of edonic responses, have been suggested as a reason for persistent weight loss after RYGB [40]; decrease of intestinal inflammation has been proposed as a possible mechanism for reduction of incidence of colon cancer [41]; improvement of IMT and of FMD might be involved in lower incidence of CV diseases [42]. In this respect, BPD and BIBP are able to induce remission of diabetes, to improve kidney function [28,29,30,31, 43], and to reduce serum cholesterol to an extent that is disproportionate to weight loss [43,44,45]. Additional effects of BPD (and probably of BIBP) are as follows: enhanced incretin secretion and satiety modulation [46], increased levels of adiponectin [47], decreased apolipoprotein A-IV levels [48], increased circulation of bile salts [49], and change of microbiota [50]. Although BPD is considered the most effective bariatric technique in terms of weight loss and metabolic effects [1, 2], its acceptance remains limited [51], likely because of several factors, such as technical difficulties and early morbidity and complications [52], and nutrition issues [53].
Due to the fact that different populations have been examined in different studies, it would be difficult to perform direct comparisons of efficacy of different surgical techniques (restrictive vs malabsorptive) in the prevention of new incident cases of diabetes, cancer, CV diseases, hyperlipidemia, and oculopathy. The effect of surgery may also be dependent on the age of patients at entry into the study, as well on other clinical conditions that are usually not considered in studies similar to the present one. As shown in our multivariable analysis of risk factors, surgery and age prevented and increased incidence of comorbidities respectively, with the exception of CV diseases. This is also a reason why direct comparisons between different populations are not possible. However, the effect observed with BPD and BIBP seems quite similar to the effect observed with RYGB for diabetes, for oculopathy, for cancer, and for hyperlipidemia and with RYGB-not-randomized studies for CV diseases.
Limitations
This retrospective study was not randomized, even though obese patients were from the same cohort; in fact, at the beginning of the study, randomization was considered nonethical. Also, the sample size might be considered small compared to other studies of similar duration, but the four institutions cover virtually all BPD and BIBP procedures performed in the Lumbardy Region. Small numbers of patients also depend on the fact that the institutions perform BPD and BIBP also in patients coming from other regions; patients migrating could not be followed up with the same degree of confidence and were not considered. On the other hand, BPD and BIBP are commonly performed in super obese patients, and one should perform a collaborative, nation-based study, to recruit greater numbers of patients, in order to confirm and extend these findings. In addition, treatments received by control patients could not be fully established, even though, by registries of surgeons and the Regional Lumbardy Administrative Database, it was possible to ascertain that these patients had no bariatric surgery procedures. A strength of this study is that it was totally unbiased, since physicians assigning the exemptions were hundreds and were not aware of the future performance of this retrospective analysis.
Conclusion
In conclusion, this retrospective study shows a lower incidence of diabetes, cancer, cardiovascular diseases, hyperlipidemia, and oculopathy in obese subjects undergoing BPD and BIBP than in obese subjects receiving standard medical treatment of obesity, similar to what has been described for other surgical techniques.
References
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724–37.
Buchwald H, Estok R, Fahrbach K, et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am J Med. 2009;122:248–56.
Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683–93.
Sjöström L, Peltonen M, Jacobson P, et al. Bariatric surgery and long-term cardiovascular events. JAMA. 2012;307:56–65.
Ikramuddin S, Korner J, Lee WJ, et al. Roux-en-Y gastric bypass vs intensive medical management for the control of type 2 diabetes, hypertension, and hyperlipidemia. The Diabetes Surgery Study randomized clinical trial. JAMA. 2013;309:2240–9.
Eliasson B, Liakopoulos V, Franzén S, et al. Cardiovascular disease and mortality in patients with type 2 diabetes after bariatric surgery in Sweden: a nationwide, matched, observational cohort study. Lancet Diabetes Endocrinol. 2015;3:847–54.
Chang SH, Stoll CR, Song J, et al. The effectiveness and risks of bariatric surgery. An updated systematic review and meta-analysis, 2003-2012. JAMA Surg. 2014;149:275–87.
Pontiroli AE, Zakaria AS, Mantegazza E, et al. Long-term mortality and incidence of cardiovascular diseases and type 2 diabetes in diabetic and nondiabetic obese patients undergoing gastric banding: a controlled study. Cardiovasc Diabetol. 2016;15:39.
Adams TD, Davidson LE, Litwin SE, et al. Weight and metabolic outcomes 12 years after gastric bypass. N Engl J Med. 2017;377:1143–55.
Thereaux J, Lesuffleur T, Czernichow S, et al. Association between bariatric surgery and rates of continuation, discontinuation, or initiation of antidiabetes treatment 6 years later. JAMA Surg. 2018; https://doi.org/10.1001/jamasurg.2017.6163.
Benotti PN, Wood GC, Carey DJ, et al. Gastric bypass surgery produces a durable reduction in cardiovascular disease risk factors and reduces the long-term risks of congestive heart failure. J Am Heart Assoc. 2017;6:e005126.
Chang AR, Chen Y, Still C, et al. Bariatric surgery is associated with improvement in kidney outcomes. Kidney Int. 2016;90:164–71.
Folini L, Veronelli A, Benetti A, et al. Liver steatosis (LS) evaluated through chemical-shift magnetic resonance imaging liver enzymes in morbid obesity; effect of weight loss obtained with intragastric balloon gastric banding. Acta Diabetol. 2014;51:361–8.
Pontiroli AE, Morabito A. Long-term prevention of mortality in morbid obesity through bariatric surgery. A systematic review and meta-analysis of trials performed with gastric banding and gastric bypass. Ann Surg. 2011;253:484–7.
Merlotti C, Morabito A, Pontiroli AE. Prevention of type 2 diabetes; a systematic review and meta-analysis of different intervention strategies. Diabetes Obes Metab. 2014;16:719–27.
Sjöström L, Peltonen M, Jacobson P, et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA. 2014;311:2297–304.
Carlsson LMS, Sjöholm K, Karlsson C, et al. Long-term incidence of microvascular disease after bariatric surgery or usual care in patients with obesity, stratified by baseline glycaemic status: a post-hoc analysis of participants from the Swedish Obese Subjects study. Lancet Diabetes Endocrinol. 2017;5:271–9.
Jakobsen GS, Småstuen MC, Sandbu R, et al. Association of bariatric surgery vs medical obesity treatment with long-term medical complications and obesity-related comorbidities. JAMA. 2018;319:291–301.
Sheng B, Truong K, Spitler H, et al. The long-term effects of bariatric surgery on type 2 diabetes remission, microvascular and macrovascular complications, and mortality: a systematic review and meta-analysis. Obes Surg. 2017;27:2724–32.
Merlotti C, Ceriani V, Morabito A, et al. Bariatric surgery and diabetic retinopathy: a systematic review and meta-analysis of controlled clinical studies. Obes Rev. 2017;18:309–16.
Christou NV, Lieberman M, Sampalis F, et al. Bariatric surgery reduces cancer risk in morbidly obese patients. Surg Obes Relat Dis. 2008;46:691–5.
Sjöström L, Gummesson A, Sjöström CD, et al. Effects of bariatric surgery on cancer incidence in obese patients in Sweden (Swedish Obese Subjects Study): a prospective, controlled intervention trial. Lancet Oncol. 2009;10:653–62.
Adams TD, Stroup AM, Gress RE, et al. Cancer incidence and mortality after gastric bypass surgery. Obesity. 2009;17:796–802.
Casagrande DS, Rosa DD, Umpierre D, et al. Incidence of cancer following bariatric surgery: systematic review and meta-analysis. Obes Surg. 2014;24:1499–509.
Afshar S, Kelly SB, Seymour K, et al. The effects of bariatric surgery on colorectal cancer risk: systematic review and meta-analysis. Obes Surg. 2014;24:1793–9.
Zhou X, Yu J, Li L, et al. Effects of bariatric surgery on mortality, cardiovascular events, and cancer outcomes in obese patients: systematic review and meta-analysis. Obes Surg. 2016;26:2590–601.
Anveden Å, Taube M, Peltonen M, et al. Long-term incidence of female-specific cancer after bariatric surgery or usual care in the Swedish Obese Subjects Study. Gynecol Oncol. 2017;145:224–9.
Scopinaro N, Adami GF, Marinari GM, et al. Biliopancreatic diversion. World J Surg. 1998;22:936–46.
Eriksson F. Biliointestinal bypass. Int J Obes. 1981;5:437–47.
Doldi SB, Lattuada E, Zappa MA, et al. Biliointestinal bypass: another surgical option. Obes Surg. 1998;8:566–9.
Del Genio G, Gagner M, Limongelli P, et al. Remission of type 2 diabetes in patients undergoing biliointestinal bypass for morbid obesity: a new surgical treatment. Surg Obes Relat Dis. 2016;12:815–21.
National Institutes of Health. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Obes Res. 1998;6(Suppl 2):51S–209S.
Levey AS, Coresh J, Greene T, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145:247–54.
www.agenziafarmaco.it, www.epicentro.iss.it/farmaci. Rapporto OSMED 2011, first published 2012. Accessed 22.06.2015.
Corrao G, Ibrahim B, Nicotra F, et al. Statins and the risk of diabetes: evidence from a large population-based cohort study. Diabetes Care. 2014;37:2225–32.
Freedman LS. Tables of the number of patients required in clinical trials using the logrank test. Stat Med. 1982;1:121–9.
Schoenfeld DA. Sample-size formula for the proportional-hazards regression model. Biometrics. 1983;39:499–503.
Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4:e297.
Boido A, Ceriani V, Cetta F, et al. Bariatric surgery and prevention of cardiovascular events and mortality in morbid obesity: mechanisms of action and choice of surgery. Nutr Metab Cardiovasc Dis. 2015;25:437–43.
Moran CP, Shanahan F. Gut microbiota and obesity: role in aetiology and potential therapeutic target. Best Pract Res Clin Gastroenterol. 2014;28:585–97.
Afshar S, Malcomson F, Kelly SB, et al. Biomarkers of colorectal cancer risk decrease 6 months after Roux-en-Y gastric bypass surgery. Obes Surg. 2018;28:945–54.
Tromba L, Tartaglia F, Carbotta S, et al. The role of sleeve gastrectomy in reducing cardiovascular risk. Obes Surg. 2017;27:1145–51.
Ceriani V, Cetta F, Lodi T, et al. Clinical and metabolic effects of biliopancreatic diversion persist after reduction of the gastric pouch and elongation of the common alimentary tract. Preliminary report in a series of patients with a 10-year follow-up. Obes Surg. 2017;27:1493–500.
Pontiroli AE, Laneri M, Veronelli A, et al. Biliary pancreatic diversion and laparoscopic adjustable gastric banding in morbid obesity: their long-term effects on metabolic syndrome and on cardiovascular parameters. Cardiovasc Diabetol. 2009;8:37.
Benetti A, Del Puppo M, Crosignani A, et al. Cholesterol metabolism after bariatric surgery in grade 3 obesity: differences between malabsorptive and restrictive procedures. Diabetes Care. 2013;36:1443–7.
Cazzo E, Pareja JC, Chaim EA, et al. Glucagon-like peptides 1 and 2 are involved in satiety modulation after modified biliopancreatic diversion: results of a pilot study. Obes Surg. 2018;28:506–12.
Adami GF, Gradaschi R, Andraghetti G, et al. Serum leptin and adiponectin concentration in type 2 diabetes patients in the short and long term following biliopancreatic diversion. Obes Surg. 2016;26(10):2442–8.
Cazzo E, Pareja JC, Geloneze B, et al. Biliopancreatic diversion decreases postprandial apolipoprotein A-IV levels in mildly obese individuals with type 2 diabetes mellitus: a prospective study. Obes Surg. 2017;27:1008–12.
Ferrannini E, Camastra S, Astiarraga B, et al. Increased bile acid synthesis and deconjugation after biliopancreatic diversion. Diabetes. 2015;64:3377–85.
Borbély YM, Osterwalder A, Kröll D, et al. Diarrhea after bariatric procedures: diagnosis and therapy. World J Gastroenterol. 2017;23:4689–700.
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2011. Obes Surg. 2013;23:427–36.
de la Matta-Martin M, Acosta-Martinez J, Morales-Conde S, et al. Perioperative morbi-mortality associated with bariatric surgery: from systematic biliopancreatic diversion to a tailored laparoscopic gastric bypass or sleeve gastrectomy approach. Obes Surg. 2012;22:1001–7.
Homan J, Schijns W, Aarts EO, et al. Treatment of vitamin and mineral deficiencies after biliopancreatic diversion with or without duodenal switch: a major challenge. Obes Surg. 2018;28:234–41.
Acknowledgements
The LAGB10 working group includes people from Ospedale San Paolo and Università degli Studi di Milano (Annamaria Veronelli, MD; Barbara Zecchini, BSc; Ahmed Zakaria, PhD; Francesca Frigè, BSc; Luca Rossetti, MD; Alberto Benetti, MD; Maurizio Cristina, MD; Ermanno Mantegazza, BSc; Marco Fanchini, BSc; Alberto Morabito, PhD; Franco Folli, MD; Antonio E. Pontiroli, MD); from IRCCS Policlinico (Enrico Mozzi, MD); from Ospedale San Raffaele (Alessandro Saibene, MD; Michele Paganelli, MD; Paola Vedani, MD); from Istituto Clinico Sant’Ambrogio (Giancarlo Micheletto, MD; Alessandro Giovanelli, MD); from Istituto Multimedica (Valerio Ceriani, Chiara Osio); from Ospedale Civile, Magenta (Giuliano Sarro, MD); from Istituto Humanitas Gavazzeni (Italo Nosari, MD); and from the Health Districts (Maria Grazia Angeletti, MD; Mariangela Autelitano, MD; Luca Cavalieri d’Oro, MD; Piergiorgio Berni, MD; Antonio G. Russo, MD).
The authors wish to thank Dr. Antonio G. Russo, Osservatorio Epidemiologico, ATS, Città Metropolitana di Milano, for the precious help in identifying causes of exemptions of patients in the study.
Funding
Università degli Studi di Milano, Ospedale San Paolo, Istituto Multimedica, Ospedale di Magenta, Istituto Humanitas Gavazzeni, INCO-Istituto Clinico Sant’Ambrogio. Grant “Ricerca Corrente” to Istituto Multimedica from Ministero della Salute (Ministry of Health), Italy
Author information
Authors and Affiliations
Consortia
Contributions
VC, GS, CO, GM, and AG performed all bariatric procedures, searched data, and contributed to discussion; ASZ, MF, IN, AMV, FF searched data, prepared the database, contributed to analysis, and contributed to discussion; AEP planned the research, contributed to discussion, and wrote the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
The study protocol was approved by local Ethics Committees in 2015 (Coordinating Center: Ospedale San Paolo, Comitato Etico Interaziendale di Milano Area A, official approval SC: 2015 ST 125). Being a retrospective study, informed consent was obtained from all individual participants included in the study who could be reached by interview, phone, or letter.
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Pontiroli, A.E., Ceriani, V., Sarro, G. et al. Incidence of Diabetes Mellitus, Cardiovascular Diseases, and Cancer in Patients Undergoing Malabsorptive Surgery (Biliopancreatic Diversion and Biliointestinal Bypass) vs Medical Treatment. OBES SURG 29, 935–942 (2019). https://doi.org/10.1007/s11695-018-3601-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-3601-5