
Abstract
A large number of patients undergoing bariatric surgery are deficient in copper, and Roux-en-Y gastric bypass can further aggravate it. Delays in diagnosis and treatment of copper deficiency can leave patients with residual neurological disability. This has led to recommendation from the British Obesity and Metabolic Surgery Society that copper levels should be monitored annually after gastric bypass. This review concludes that copper deficiency in adequately supplemented patients is rare and can be adequately treated if a related haematological or neurological disorder is diagnosed. The cost of routine monitoring may therefore not be justified for adequately supplemented, asymptomatic patients who have undergone Roux-en-Y gastric bypass. The screening may however be necessary for high-risk patient groups to prevent severe complications and permanent disability.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Copper (Cu), a coenzyme in a variety of metalloenzymes, is essential for normal haematopoiesis and nervous system functioning [1]. Its deficiency can lead to haematological disorders commonly anaemia and neutropenia, bone and connective tissue disorders, polyneuropathy, optic neuropathy, and myeloneuropathy. Roux-en-Y gastric bypass (RYGB) is widely regarded as the gold standard bariatric procedure and accounts for approximately 45 % all the bariatric procedures performed worldwide [2]. Morbidly obese patients referred for bariatric surgery can be deficient in a number of micronutrients [3]. When it comes to Cu, up to two-thirds [4] of potential bariatric surgery candidates can be deficient in it. RYGB can further reduce intake as well as absorption of Cu. This has led both the British Obesity and Metabolic Surgery Society (BOMSS) [5] and the American Society for Metabolic and Bariatric Surgery (ASMBS) [6] to recommend a minimum of 2 mg per day of Cu supplementation for patients undergoing RYGB. There is however little evidence in scientific literature to support this recommendation, and studies comparing adequacy of various doses of Cu supplementation in RYGB patients do not exist.
Patients, who are not routinely supplemented and/or are not concordant with their multivitamins and mineral intake, are at risk of developing Cu deficiency after RYGB. Whilst asymptomatic Cu deficiency is common after RYGB [7, 8], symptomatic deficiency is rare. If not suspected, symptomatic Cu deficiency can be difficult to diagnose and there are reports in literature of patients who have suffered permanent neurological disability because of delays in diagnosis and treatment [9–11].
This has led BOMSS to recommend [5] annual monitoring of serum Cu levels in patients after RYGB. Since RYGB is the commonest bariatric operation in the United Kingdom [12] and the rest of the world [2, 12], this has resource implications. Furthermore, this advice appears to contradict the advice by ASMBS [6] that routine monitoring is unnecessary and that Cu levels should only be evaluated in patients with unexplained anaemia, neutropenia, myeloneuropathy, or impaired wound healing. Apparent contradiction in these guidelines can be confusing for health-care practitioners of metabolic surgery worldwide and formed the basis for this systematic review. We investigated the entire English language scientific literature on copper deficiency after RYGB in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Methods
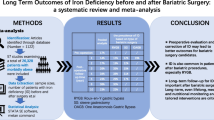
An online search of PubMed, MEDLINE, Embase, and Google Scholar was independently carried out by two researchers using keywords like “bariatric surgery,” “gastric bypass,” “Roux en Y Gastric Bypass,” and “Copper” to identify all articles on Cu deficiency in gastric bypass patients. Articles were also identified from references of relevant articles. Last of these searches was carried out on 30 November 2015. Articles reporting Cu deficiency in patients who underwent intestinal bypass (as it is no longer performed by bariatric surgeons) and other gastrointestinal procedures were excluded [13–16], as were those published in non-English language journals [17–19]. Articles on other bariatric procedures were also excluded [20–23]. Articles by Jaiser et al. [24] and Kumar [25] were excluded as these are reviews, and we have included most of the original reports of bariatric cases in these reviews. Studies by Papamargaritis et al. [26] and Halfdanarson et al. [1] were excluded from the systematic review as authors studied a number of bariatric procedures together and did not separately report results with RYGB patients. A total of 22 articles were identified on the subject of Cu deficiency after gastric bypass. Figure 1 gives a PRISMA flow chart for the article selection.

PRISMA flow chart for article selection
Results
Studies on Symptomatic Cu Deficiency after Gastric Bypass
Table 1 [9–11, 21, 27–39] lists all the reports of symptomatic Cu deficiency after RYGB. There are 17 articles reporting 34 cases of symptomatic Cu deficiency after RYGB in the literature. Out of these, 33 (97 %) were female and the mean age of the patients was 47 years. On average, patients presented 8.6 years after RYGB. Information on supplements was not available for 20 (59 %) patients.
Thirteen out of 34 patients (38 %) were not on any Cu supplement. Only one out of 34 patients was on any multivitamin and mineral supplement; authors do not mention if the supplement contained any Cu. Out of 34 patients, 19 (56 %) presented with neurological symptoms and 17 (50 %) had haematological manifestations. Four out of 19 (21.0 %) patients with neurological complaints presented with optic neuropathy. Anaemia was the dominant haematological manifestation seen in all of the patients with haematological problems. Two out of 17 (11.7 %) patients with haematological disorders had pancytopenia, and a further four (23.5 %) had leucopenia/neutropenia in addition to anaemia.
Rapid clinical recovery was observed upon institution of treatment in all 15 out of 17 (88.0 %) patients with haematological disorders this information was available for. This information was not available for the remaining two patients. Eight out of 19 (42.0 %) patients with neurological manifestations in 4 studies were left with residual neurological deficits. Seven out of 19 patients (36.8 %) in 6 studies did not have any residual sequelae. This information was not available for the remaining 4 out of 19 patients.
Studies on Asymptomatic Cu Deficiency after Gastric Bypass
Table 2 [7, 8, 28, 40, 41] includes reports of asymptomatic Cu deficiency after gastric bypass. There are 5 studies reporting on 245 patients with a mean age and BMI of 41 years and 46.1 kg/m2, respectively. Out of these, 210 (85.7 %) were females. A total of 23 patients (9.38 %) were diagnosed with Cu deficiency at a mean follow-up of 21.7 months. Though all of the patients in these studies were prescribed a multivitamin and mineral supplement, dose ranged from 0.45 to 3.0 mg. Studies reveal a Cu deficiency rate of 3.8 [40] to 18.8 % [28] at a mean follow-up of 6 months to 5 years.
Discussion
Cu deficiency is rare in the general population because it is abundant in commonly consumed food items like legumes, potato and potato products, nuts, seeds, beef, and wheat. The recommended daily dietary allowance of 0.9 mg is thus easily met [28, 42]. Bariatric surgery candidates are at higher risk of being deficient in Cu [4]. RYGB can further aggravate Cu deficiency through reduced intake, reduced absorption due to the exclusion of the duodenum and proximal jejunum which are the predominant sites for Cu absorption, or due to excess zinc intake which interferes with copper absorption.
This review shows that approximately 10 % of patients develop asymptomatic Cu deficiency after RYGB. This is to be expected given that majority of the patients in the studies were not prescribed supplements containing the recommended 2.0 mg of Cu. Some authors recommended only 0.45 mg of Cu, which is less than the average daily requirement and significantly below the amounts recommended after RYGB. Others just recommended a multivitamin and mineral supplement without ensuring that the preparations contained Cu in the requisite amount. This is an important point as not all multivitamin and mineral supplements contain Cu and very few contain 2.0 mg of it.
Despite such a relatively high prevalence of asymptomatic Cu deficiency after RYGB, our review shows that only 34 symptomatic cases have been published in English language scientific literature with clear signs and symptoms attributable to Cu deficiency after RYGB. Interestingly, only one of these patients was documented to be on a supplement and even for this patient, we do not know the exact amount of Cu in the tablet.
Despite almost a complete lack of knowledge regarding routine Cu supplementation and early detection of symptomatic Cu deficiency after RYGB in the past, the literature has recorded very few patients with residual neurological deficits. We believe the incidence of neurological problems can be further reduced if clinicians focused on ensuring their patients were adequately supplemented with multivitamin/mineral tablets containing at least 2.0 mg of Cu. Papamargaritis et al. [26] found a 2.0 % Cu deficiency in patients prior to bariatric surgery and a 0–5 % deficiency rates after surgery. Patients were supplemented with a daily multivitamin and mineral tablet containing 2 mg of Cu, and importantly, the authors did not find any significant change in median serum Cu concentration during follow-up. In this study of 437 patients, 57 % patients underwent RYGB; the remaining underwent sleeve gastrectomy and gastric banding. Authors concluded that patients concordant with multivitamins and mineral supplements maintained normal Cu concentration during the first years after bariatric surgery. Since the calorie intake after surgery increases with passage of time and the bowel undergoes hypertrophy and adaptation, one can also expect copper levels to remain in the normal range in the longer term for well-supplemented patients.
Given such a low frequency of symptomatic Cu deficiency, routine lifelong screening may not be justified for all patients undergoing RYGB and can be reserved for high-risk and clinically symptomatic patients. Routine screening does not come without its own problems. Apart from the obvious cost implications, diagnosis of clinically insignificant biochemical abnormalities can potentially result in unnecessary patient anxiety. Currently, bariatric surgery patients are required to undergo lifelong screening blood tests for early detection of a number of micronutrient deficiencies. A complete risk-vs-benefit evaluation, including a cost analysis, has not been performed for the vast majority of these investigations. Majority of these asymptomatic laboratory abnormalities may not necessarily result in any clinical harm.
This review supports that there is a definite prevalence of Cu deficiency after RYGB. It would hence seem prudent that patients are advised to take a multivitamin and mineral tablet containing 2 mg of Cu per day after bariatric surgery, as has been recommended by both British [5] and American guidelines [6], at least until comparative studies examining various supplement doses become available. Since zinc can interfere with Cu absorption, it is recommended that patients on zinc supplements are also supplemented with Cu (1 mg Cu for 8–5 mg zinc) [5]. It is important to note in this context that not all multivitamin and mineral preparations contain the required amount of Cu or indeed any at all.
Most patients with clinical Cu deficiency after RYGB can be adequately treated with timely diagnosis and treatment. It is hence crucial that health-care professionals consider measuring Cu levels in patients with anaemia, neutropenia, myeloneuropathy, or impaired wound healing. Patients should also be advised to report any neurological symptoms early to avoid irreversible damage. Patients at high risk of copper deficiency, e.g. those with established neurological deficits, non-compliance to vitamin and mineral supplements, pregnant and lactating women, patients with prolonged severe diarrhoea or vomiting, prolonged zinc supplement intake, alcoholics, and those with previous history of copper deficiency requiring hospitalization, should undergo a careful haematological and neurological assessment backed by monitoring of copper levels as and when clinically indicated. It is also worth bearing in mind in this context that in clinical practice diagnosis of clinical Cu deficiency can only be made when deficiencies of other micronutrient like iron, vitamin B12, and thiamine have either been ruled out or corrected. Furthermore, though rare after RYGB, patients after malabsorptive bariatric procedures may harbour multiple co-existing micronutrient deficiencies leading to complex clinical presentations. It would seem prudent to take an opinion from a dedicated bariatric physician or chemical pathologist for such patients.
There are several weaknesses to this review. Most of the studies in this review are either case reports or cohort studies. This limits the conclusion that can be reached from this review. Future studies need to determine the prevalence of symptomatic Cu deficiency in adequately supplemented patients as well as the ideal supplemental dose in RYGB patients. This review specifically examines RYGB patients only, and results cannot hence be extrapolated to other bariatric procedures. It is though likely that patients undergoing sleeve gastrectomy or gastric band will be at a lesser risk of developing Cu deficiency.
Conclusion
Approximately 10 % of patients can be deficient in Cu after RYGB, but symptomatic deficiency is rare. Clinically manifested Cu deficiency can be easily and completely corrected if diagnosis is suspected early; delays however, may result in permanent neurological deficits. Routine monitoring of Cu levels is probably unnecessary after RYGB. Clinicians should instead focus on supplementing their patients with daily multivitamin and mineral tablets containing at least 2.0 mg of copper and target their investigations to patients with unexplained haematological or neurological abnormalities. High-risk patients should undergo a careful haematological and neurological assessment with a low threshold for copper level monitoring.
Abbreviations
- ASMBS:
-
American Society for Metabolic and Bariatric Surgery
- BOMSS:
-
British Obesity and Metabolic Surgery Society
- Cu:
-
copper
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RYGB:
-
Roux-en-Y gastric bypass
References
Halfdanarson TR, Kumar N, Li CY, et al. Hematological manifestations of copper deficiency: a retrospective review. Eur J Haematol. 2008;80(6):523–31.
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery worldwide 2013. Obes Surg. 2015;25(10):1822–32.
Sánchez A, Rojas P, Basfi-Fer K, et al. Micronutrient deficiencies in morbidly obese women prior to bariatric surgery. Obes Surg. 2015. doi:10.1007/s11695-015-1773-9.
de Luis DA, Pacheco D, Izaola O, et al. Micronutrient status in morbidly obese women before bariatric surgery. Surg Obes Relat Dis. 2013;9(2):323–7.
O’Kane M, Pinkney J, Aasheim E, et al. BOMSS guidelines on perioperative and postoperative biochemical monitoring and micronutrient replacement for patients undergoing bariatric surgery. Adopted by BOMSS Council September 2014. http://www.bomss.org.uk/wp-content/uploads/2014/09/BOMSS-guidelines-Final-version1Oct14.pdf. Accessed 7 July 2015.
Mechanick JI, Youdim A, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Obesity (Silver Spring). 2013;21(1):S1–27. doi:10.1002/oby.20461.
Ernst B, Thurnheer M, Schultes B. Copper deficiency after gastric bypass surgery. Obesity (Silver Spring). 2009;17(11):1980–1.
Gobato RC, Seixas Chaves DF, Chaim EA. Micronutrient and physiologic parameters before and 6 months after RYRYGB. Surg Obes Relat Dis. 2014;10(5):944–51.
Juhasz-Pocsine K, Rudnicki SA, Archer RL, et al. Neurologic complications of gastric bypass surgery for morbid obesity. Neurology. 2007;68(21):1843–50.
Rounis E, Laing CM, Davenport A. Acute neurological presentation due to copper deficiency in a hemodialysis patient following gastric bypass surgery. Clin Nephrol. 2010;74(5):389–92.
Pineles SL, Wilson CA, Balcer LJ, et al. Combined optic neuropathy and myelopathy secondary to copper deficiency. Surv Ophthalmol. 2010;55(4):386–92.
Welbourn R, Small P, Finlay I, et al. Second national bariatric surgery report. http://www.bomss.org.uk/wp-content/uploads/2014/04/Extract_from_the_NBSR_2014_Report.pdf. Accessed 22 August 2015.
Tan JC, Burns DL, Jones HR. Severe ataxia, myelopathy, and peripheral neuropathy due to acquired copper deficiency in a patient with history of gastrectomy. JPEN J Parenter Enteral Nutr. 2006;30(5):446–50.
Kumar N, McEvoy KM, Ahlskog JE. Myelopathy due to copper deficiency following gastrointestinal surgery. Arch Neurol. 2003;60(12):1782–5.
Nakagawa M, Kojima K, Inokuchi M, et al. Assessment of serum copper state after gastrectomy with Roux-en-Y reconstruction for gastric cancer. Dig Surg. 2015;32(4):301–5.
Dalal N, Hooberman A, Mariani R, et al. Copper deficiency mimicking myelodysplastic syndrome. Clin Case Rep. 2015;3(5):325–7. doi:10.1002/ccr3.207.
Oliveira YS, Iba Ba J, Mba Angoué JM, et al. Copper deficiency and peripheral neuropathy as an outcome of gastrectomy. Rev Med Interne. 2013;34(4):234–6.
Basfi-fer K, Valencia A, Rojas P, et al. Quality of the diet of women with severe and morbid obesity undergoing gastric bypass and sleeve gastrectomy. Arch Latinoam Nutr. 2011;61(1):28–35.
Beltrán Sánchez AM, Morchón Simón D, Pérez Castrillón JL. Copper deficiency after bariatric surgery simulating a myelodysplastic syndrome. Med Clin (Barc). 2011;136(10):460–1.
Btaiche IF, Yeh AY, Wu IJ, et al. Neurologic dysfunction and pancytopenia secondary to acquired copper deficiency following duodenal switch: case report and review of the literature. Nutr Clin Pract. 2011;26(5):583–92.
de Luis DA, Pacheco D, Izaola O, et al. Zinc and copper serum levels of morbidly obese patients before and after biliopancreatic diversion: 4 years of follow-up. J Gastrointest Surg. 2011;15(12):2178–81.
Böyük A, Banlı O, Gümüş M, et al. Plasma levels of zinc, copper, and ceruloplasmin in patients after undergoing laparoscopic adjustable gastric banding. Biol Trace Elem Res. 2011;143(3):1282–8.
AlHassany AA. Night blindness due to vitamin A deficiency associated with copper deficiency myelopathy secondary to bowel bypass surgery. BMJ Case Rep. 2014. doi:10.1136/bcr-2013-202478.
Jaiser SR, Winston GP. Copper deficiency myelopathy. J Neurol. 2010;257(6):869–81.
Kumar N. Copper deficiency myelopathy (human swayback). Mayo Clin Proc. 2006;81(10):1371–84.
Papamargaritis D, Aasheim ET, Sampson B, et al. Copper, selenium and zinc levels after bariatric surgery in patients recommended to take multivitamin-mineral supplementation. J Trace Elem Med Biol. 2015;31:167–72.
Griffith DP, Liff DA, Ziegler TR, et al. Acquired copper deficiency: a potentially serious and preventable complication following gastric bypass surgery. Obesity (Silver Spring). 2009;17(4):827–31.
Gletsu-Miller N, Broderius M, Frediani JK, et al. Incidence and prevalence of copper deficiency following Roux-en-Y gastric bypass surgery. Int J Obes. 2012;36(3):328–35.
Shah AR, Tamhankar MA. Optic neuropathy associated with copper deficiency after gastric bypass surgery. Retin Cases Brief Rep. 2014;8(1):73–6.
Yarandi SS, Griffith DP, Sharma R, et al. Optic neuropathy, myelopathy, anemia, and neutropenia caused by acquired copper deficiency after gastric bypass surgery. J Clin Gastroenterol. 2014;48(10):862–5.
Robinson SD, Cooper B, Leday TV. Copper deficiency (hypocupremia) and pancytopenia late after gastric bypass surgery. Proc (Baylor Univ Med Cent). 2013;26(4):382–6.
Naismith RT, Shepherd JB, Weihl CC, et al. Acute and bilateral blindness due to optic neuropathy associated with copper deficiency. Arch Neurol. 2009;66(8):1025–7.
Choi EH, Strum W. Hypocupremia-related myeloneuropathy following gastrojejunal bypass surgery. Ann Nutr Metab. 2010;57(3–4):190–2.
Khambatta S, Nguyen DL, Wittich CM. 38-year-old woman with increasing fatigue and dyspnea. Mayo Clin Proc. 2010;85(4):392–5.
O’Donnell KB, Simmons M. Early-onset copper deficiency following Roux-en-Y gastric bypass. Nutr Clin Pract. 2011;26(1):66–9.
Shahidzadeh R, Sridhar S. Profound copper deficiency in a patient with gastric bypass. Am J Gastroenterol. 2008;103(10):2660–2.
Goldberg ME, Laczek J, Napierkowski JJ. Copper deficiency: a rare cause of ataxia following gastric bypass surgery. Am J Gastroenterol. 2008;103(5):1318–9.
Sonu RJ, Rashidi HH. Concurrent copper and iron deficiency in a gastric bypass patient: a great mimicker of MDS. Blood. 2015;125(16):2582.
Chai Y, Bertorini TE. A female with progressive four-limb paresthesias and gait difficulty. J Clin Neuromuscul Dis. 2010;11(4):191–7.
Balsa JA, Botella-Carretero JI, Gómez-Martín JM, et al. Copper and zinc serum levels after derivative bariatric surgery: differences between Roux-en-Y gastric bypass and biliopancreatic diversion. Obes Surg. 2011;21(6):744–50.
Rojas P, Carrasco F, Codoceo J, et al. Trace element status and inflammation parameters after 6 months of Roux-en-Y gastric bypass. Obes Surg. 2011;21(5):561–8.
Higdon J, Drake VJ, Delage B, Prohaska J. Copper. Linus Pauling Institute. http://lpi.oregonstate.edu/mic/minerals/copper. Accessed 22 November 2015.
Authors’ Contributions
KM conceived the idea for the topic. PK, KM, NH independently collected information and analysed it. All authors participated in discussions on the topic and manuscript writing. All authors have seen the final version and approve of it.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
Not applicable
Rights and permissions
About this article

Cite this article
Kumar, P., Hamza, N., Madhok, B. et al. Copper Deficiency after Gastric Bypass for Morbid Obesity: a Systematic Review. OBES SURG 26, 1335–1342 (2016). https://doi.org/10.1007/s11695-016-2162-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-016-2162-8