
Abstract
Setting
The physiological and anatomical changes that occur as a consequence of bariatric surgery result in macro- and micro-nutritional deficiencies, especially iron deficiency. The reported incidence of iron deficiency and associated anemia after bariatric surgery varies widely across studies.
Objectives
The aim of this systematic review is to quantify the impact of Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG) on the incidence of iron deficiency.
Methods
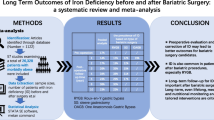
Databases including Ovid Medline, Ovid Embase, Helthstar, Scopus, Cochrane (CDSR), LILACS, and ClinicalKey were searched for original articles with additional snowballing search. Search terms included Obesity, nutrient deficiency, iron deficiency, iron deficiency anemia, bariatric surgery, Roux-en-Y gastric bypass, and sleeve gastrectomy. Original articles reporting the incidence of iron deficiency and anemia pre- and post-RYGB and SG from January 2000 to January 2015 with minimum 1-year follow-up were selected. Data extraction from selected studies was based on protocol-defined criteria.
Results
There were 1133 articles screened and 20 studies were included in the final analysis. The overall incidence of iron deficiency was 15.2% pre-operatively and 16.6% post-operatively. When analyzed by procedure, the incidence of iron deficiency was 12.9% pre-RYGB versus 24.5% post-RYGB and 36.6% pre-SG versus 12.4% post-SG. The incidence of iron deficiency-related anemia was 16.7% post-RYGB and 1.6% post-SG. Risk factors for iron deficiency were premenopausal females, duration of follow-up, and pre-operative iron deficiency. Prophylactic iron supplementation was reported in 16 studies and 2 studies provided therapeutic iron supplementation only for iron-deficient patients. Iron dosage varied from 7 to 80 mg daily across studies.
Conclusion
Iron deficiency is frequent in people with obesity and may be exacerbated by bariatric surgery, especially RYGB. Further investigation is warranted to determine appropriate iron supplementation dosages following bariatric surgery. Careful nutritional surveillance is important, especially for premenopausal females and those with pre-existing iron deficiency.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Bariatric surgery is known to provide effective long-term treatment of obesity and its related comorbidities [1, 2]. The physiological and anatomical changes that occur as a consequence of these procedures result in both macro- and micro-nutritional deficiencies [3]. As the number of bariatric procedures performed annually continues to increase, it is important to quantify the risk of such long-term complications.
Patients with obesity have a higher prevalence of micronutrient deficiencies compared to normal weight individuals and this is further exacerbated by bariatric surgery [4, 5]. Iron deficiency and anemia following bariatric surgery have been reported in several studies of varying quality with a wide range of reported incidence [6,7,8,9,10,11]. The type of operation has the potential to influence the risk of iron deficiency. Sleeve gastrectomy (SG) is a restrictive procedure that results in decreased distension and early satiety. The incidence of nutritional deficiencies is expected to be less with a restrictive procedure compared to a combined restrictive/malabsorptive procedure, such as the Roux-en-Y gastric bypass (RYGB) [12].
While many studies have examined the post-operative nutritional status after bariatric surgery, the reported incidence of iron deficiency in these studies varies widely due to differences in patient populations, supplement protocols, and the length/completeness of follow-up [13]. A recent meta-analysis reported that the risk of iron deficiency and anemia was similar for SG and RYGB [14]. However, this meta-analysis only included studies that directly compared the two procedures.
The aim of this systematic review is to estimate the incidence of iron deficiency and related anemia following RYGB and SG, to determine risk factors for developing iron deficiency and to assess the reported effectiveness of supplementation on post-operative serum iron levels and anemia.
Methods
We performed a systematic literature search of all full-text articles published between January 1980 and June 2018 according to the Preferred Reporting Items for Systematic reviews (PRISMA) protocol [15]. An institutional review board approval was not required for this study.
Search strategy
The initial search strategy was completed by May 2015 by a health science librarian (E.L). A comprehensive search of all electronic databases was performed in MEDLINE, Embase, Helthstar, Scopus, Cochrane, LILACS, DynaMEd, Clinical Key, TRIP+, OTSeeker, Johanne Briggs Institute, and AMED. The search terms used were “Bariatric Surgery” OR “Roux-En-Y” OR “Sleeve Gastrectomy” OR “Obesity” for intervention terms AND “iron” OR “iron deficiency’” OR “iron deficiency anemia” OR “Nutritional deficiencies” with all possible variations. To increase the sensitivity of the search strategy, we combined key words with Medical Subjects Heading (MeSH) terms individually (key words AND MeSH), as well as a gray literature search. A more detailed search strategy is available on request. The search was re-run for a final retrieval (check) in June 2018.
Study selection
Selection criteria included original articles reporting the incidence of iron deficiency and anemia pre- and post-RYGB and SG with a minimum 12-month follow-up post-operatively. All studies were required to present data on (1) serum iron or ferritin level (2) hemoglobin level, and (3) incidence of iron deficiency anemia pre- and post-bariatric procedures in adult population.
Studies with information about iron supplements were included.
Study selection was completed through two levels of study screening. At the first level of screening, we excluded studies with the following exclusion criteria: publications of abstracts only, case reports, case series, letters, comments, and reviews; follow-up less than 1 year; non-English articles; studies with data on participants who underwent vertical banded gastroplasty, laparoscopic biliopancreatic diversion with duodenal switch, or adjustable gastric banding; and studies reporting data on participants with conditions other than obesity. Full articles were then obtained for all studies accepted at level one. For level two screening, studies reporting either the incidence of iron deficiency anemia or iron levels were included. Figure 1 illustrates the literature search and study selection.

Literature search and study selection
Data extraction
Quality assessment of the included studies was done independently by two reviewers (G.E. and M.D) using the Newcastle–Ottawa Scale (NOS) assessment tool for non-randomized studies [16] and the Cochrane Collaboration’s tool for randomized controlled trials. Two reviewers (G.E. and E.B.) extracted data from the included papers. This included data on study characteristics and type (author, published year, study design, and length of follow-up); patients’ demographics [mean age, male to female ratio and pre- and post-operative body mass index (BMI)]; type of surgery performed; number of participants and outcomes measured (incidents of post-operative serum iron deficiency, iron deficiency anemia, and supplements intake). The incidence of iron deficiency and anemia was extracted at 0 and 12 months after surgery. Pooled data of categorical variables were reported as frequency and percentages.
Summary statistics are reported as total and percentages for categorical variables. Meta-analysis was performed using Review Manager Version 5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.). The risk of iron deficiency and unclassified anemia was compared pre-operatively to 1 year post-RYGB and SG. Pooled risk ratios were calculated using inverse variance weighting of risk ratios for each study. Random effects model was used as a significant amount of heterogeneity was observed in all analyses (i.e., I2 > 50% or Cochran Q < 0.05). Publication bias was assessed visually using funnel plots for analyses with more than 10 studies but no conclusions could be made given the small number of studies. Analyses for publication bias were performed on STATA Version 14.2 (StataCorp, 405 Lakeway Drive, College Station, Texas).
Results
Search results
There were 1133 articles identified for screening. Of those, 1041 articles were removed after level one screening of abstracts based on exclusion criteria. Full extraction and review of the remaining 95 articles in level two screening yielded a total of 15 included studies [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Two additional studies from the snowball search method that met our inclusion criteria were included [17, 18] and three additional studies were found on our updated search [13, 34, 35] (Fig. 1). In the final analysis, there were three randomized controlled trials (RCT) [13, 19, 20], 4 controlled studies [18, 21, 22, 27], 5 prospective studies [17, 23,24,25,26], and 8 retrospective studies [28,29,30,31,32,33,34,35].
Included studies
A total of 20 studies with 4007 patients were included for this review. Of those, 1897 patients had RYGB and 2110 patients had SG. Ten studies included RYGB cohorts, four included SG cohorts, and five compared SG to RYGB (Table 1).
The average follow-up time was 27.8 months (range 12–120). Mean age of the participants was 41.9 ± 18.4 years (range 32.6–46.4). Sixty-six percent of the patients were females. Body mass index was 52.1 kg/m2 at baseline and 30.5 kg/m2 post-operatively. The mean excess weight loss percentage (EWL%) could not be estimated due to inconsistency of reporting across studies (Table 1).
The combined total incidence of post-operative iron deficiency in patients undergoing either RYGB or LSG was 17.2% compared to 26.2% pre-operatively [13, 14, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35]. Differences in iron deficiency, iron deficiency anemia, and unclassified anemia existed between patients undergoing RYGB versus SG (Table 2).
RYGB
Iron deficiency
The total incidence of iron deficiency for RYGB is shown in Table 2. An increase in the incidence of iron deficiency pre- versus post-RYGB was observed in 12 studies [13, 18, 20, 21, 23,24,25, 27, 30,31,32, 35] (Table 3). Three studies [19, 22, 29] showed no increase in iron deficiency 1 year post-operatively, but one of these studies showed worsening iron deficiency at 36 months post-RYGB [29]. One study that provided 18 mg of daily iron supplementation did not prevent iron deficiency after RYGB [33].
The pooled analysis of 6 studies that assessed the number or percentage of patients who developed iron deficiency found a higher risk 1-year after RYGB OR 1.67 (95% CI 1.41–1.98). However, there was a significant heterogeneity detected for this comparison (χ2 = 93.28, df = 13 (P < 0.00001); I2 = 86%) (Fig. 2a).

A The incidence of iron deficiency post-Roux-en-Y Gastric bypass. B The incidence of unclassified anemia post-Roux-en-Y gastric bypass. C The incidence of iron deficiency post-sleeve gastrectomy. D The incidence of unclassified anemia post-sleeve gastrectomy
Anemia
There was a significant increase in patients with unclassified anemia at 1 year post-RYGB in seven studies: 22.9% post-operatively compared to 11.2% pre-operatively [18, 19, 25, 29, 30, 32, 33] and this showed further increase by 4-year follow-up in two studies [29, 32] (Table 3). Four RYGB studies showed no significant change in the incidence of unclassified anemia at 1-year follow-up compared to baseline [19, 22, 31, 32]. However, one study showed an increased incidence of anemia at 24, 36, and 48 months of follow-up [13].
The pooled analysis of the 14 studies that reported the incidence of anemia after RYGB showed higher risk of anemia at 1-year post-surgery OR 2.49 (95% CI 2.04–3.05). This comparison had significant heterogeneity (χ2 = 55.89, df = 13 (P < 0.00001); I2 = 77%) (Fig. 2b).
Iron deficiency anemia
The post-operative incidence was reported in only 5 studies (Table 3) [20, 23, 26, 33, 35]. Iron deficiency was most responsible for anemia in one study [61% of patients with anemia de novo (P < 0. 001)] [25]. One study found a significant increase in the incidence of iron deficiency anemia at 18-month follow-up (1.5 vs. 23.9, P < 0.05) [23].
Risk factors for iron deficiency
Risk factors for the development of iron deficiency anemia in patients undergoing RYGB included female sex, low pre-operative ferritin, and younger age. Four studies reported a significant risk of new iron deficiency anemia post-operatively in females compared to males (21.7% vs. 4.6%, female vs. male; P = 0.005) [20, 23, 26, 33]. Two studies found a significant drop in iron level post-operatively among menstruating women [25, 31] and two studies reported increased incidence of anemia and low iron level post-operatively [13, 29]. Another risk factor for iron deficiency anemia included greater weight loss [25, 31]. The length of Roux limb did not seem to correlate with the development of iron deficiency [25].
Iron supplementation
Eleven studies [13, 18, 21, 22, 25, 28, 29, 31,32,33, 35] reported the administration of empiric iron supplementation to patients post-operatively. Two studies [19, 24] provided therapeutic iron only for those with iron deficiency and 2 other studies [17, 30] did not supplement at all. The effectiveness of supplement use is difficult to quantify due to lack of consistent dosage and documented compliance of intake. Iron supplements varied across studies from 7 to 80 mg (Table 3). Studies that provided an iron supplement dose of 60 and 80 mg daily did not have worsening incidence of iron level from baseline at 1 year post-operatively [13, 19, 31] or showed decreased incidence of iron deficiency from baseline [21, 33]. One RCT found significant correlation between improvement of post-operative iron deficiency and taking prescribed iron supplementation of 320 mg per day (P < 0.05) [20]. Brolin’s study found that adherence to multivitamin supplements was associated with improvement in 41% of iron deficiencies and 22% of anemias [20].
Iron deficiency
The SG patients had a reported incidence of iron deficiency of 12.4% post-operatively versus 36.6% pre-operatively [17,18,19, 22, 24, 27, 28, 34]. Four studies reported no alteration in the serum iron and ferritin levels post-operatively [17, 24, 28, 34]. One study reported the development of iron deficiency as insignificant one-year post-SG, but this finding could be explained by the fact that patients with baseline iron deficiency and anemia were excluded [17]. None of the SG studies showed a significant increase in the incidence of the unclassified anemia at one year post-operatively (Table 2) [17, 18, 28, 34]. Saif et al. [28] showed that pre-operative anemia incidence improved at 1- and 3-year follow-up but returned to pre-operative level by 5 years.
Two studies in the SG group provided prophylactic supplementation [24, 34]. One study did not provide any supplementation [17] and an additional study provided therapeutic iron supplementation for those with pre-operative or post-operative iron deficiency or anemia only [28]. Adherence to supplementation was assessed in one study where only 28.9% of patients reported taking supplements at year 1 and 42.9% at year 3 and 63.3% at year 5 follow-up [28]. However, blood serum level of micronutrient did not seem to correlate with supplement use and some supplements were inadequate to normalize low serum iron level [28].
The pooled risk of post-operative iron deficiency or unclassified anemia was not higher after LSG 0.22 (95% CI 0.19–0.26) and 1.03 (95% CI 0.87–1.21), respectively (Fig. 2C, D).
RYGB versus SG
When comparing the two procedures, one study found that patients who underwent RYGB were more susceptible to develop post-operative iron deficiency (15% post-op vs. 2% pre-op; P < 0.01) than the SG patients (0% post-op vs. 0% pre-op) [18]. Two other studies found no change in the incidence of iron deficiency at 1-year follow-up compared to baseline between the two procedures [19, 22].
The effect of iron supplementation on the incidence of iron deficiency was examined in few studies. Supplementation was found to be protective in 2 studies with RYGB cohorts [31, 33], while 2 studies with SG cohorts did not identify such protective effect [24, 28].
Discussion
Nutritional deficiencies after bariatric surgery are related to several factors: (1) reduced intake of nutrients, such as red meat, (2) anatomical changes in the gastrointestinal tract, (3) high rates of pre-operative nutritional deficiencies. Iron deficiency was reported among 5.9 to 42% of patients undergoing bariatric surgery [7, 17, 20, 26, 30, 33, 36]. Most of the anemia identified post-RYGB was attributed to iron deficiency with a rate of 16–26% [7, 17, 20, 23, 26, 30, 32, 33]. Patients with pre-operative iron deficiency had worsening of their iron levels following RYGB. It is important to monitor iron indices before and after weight loss surgery [20, 25, 30]. The American Society of Metabolic and Bariatric Surgery (ASMBS) guidelines recommended diagnosing iron deficiency prior to weight loss surgery, at 3 months post-operatively, then every 3–6 months for the 12-months post-operatively and annually thereafter by measuring serum iron, serum transferrin and TIBC [37]. However, there are no standard guidelines for the management of iron deficiency in those who are identified pre-operatively.
The studies that compared iron deficiency pre- and post-SG found either no change or decreased incidence of iron deficiency after surgery [17, 24, 28]. Hakeem’s study did not report iron deficiency at one-year post-SG even though the post-operative supplements did not include iron [17]. However, their study only included patients with normal iron levels pre-operatively. Therefore, iron deficiency found after SG could be partially explained by pre-operative iron deficiency state. The included studies reported higher pre-operative rate of iron deficiency in patients undergoing SG compared to RYGB (36.6% vs. 14.7%). An explanation for this vast difference could not be inferred from the included studies. However, one can assume that SG may be better offered to patients with higher risk to develop iron deficiency post-operatively than RYGB, e.g., menstruating females, those with pre-operative deficiency.
Patients with obesity are counseled to continue lifelong nutritional supplements after RYGB [38]. Recommendations for RYGB include starting the supplementation within 30 days post-operatively and continuing lifelong [39]. Commercial multivitamin supplementations contain a small amount of iron (10–20 mg) which is generally insufficient to prevent iron deficiency post-operatively. Few studies recommended adequate supplementation based on laboratory surveillance in the pre- and post-operative period for patients undergoing sleeve gastrectomy [25, 40, 41]. Eighteen milligram of elemental iron daily is recommended for average risk patients and 40–65 mg (200–400 mg of ferrous sulfate) for women in their reproductive years and patients with history of anemia [37]. However, this dose is increased in patients with anemia post-bariatric surgery to 150–200 mg (400–800 mg of ferrous sulfate) [37, 39, 42, 43]. Brolin et al. found in a randomized controlled trial that prophylactic supplementations of 320 mg of oral ferrous sulfate twice daily prevented iron deficiency anemia [20]. Parenteral iron should be administered if a patient fails to respond to oral iron supplementation post-operatively [20, 24, 32, 33].
Patients’ compliance to supplementation plays an important role in developing deficiencies post-RYGB. Brolin et al. reported post-RYGB iron deficiency of 47% when only 35% of the patients were compliant with iron supplements [26]. Compliance after bariatric surgery has been reported as 29% after the first year and increasing to 63% by the fifth year, emphasizing the need for close observation, continued patient education, and treating iron deficiency beyond 1 year in the post-operative period [28]. Skroubis reported an increased incidence of anemia and iron deficiency at 4-year follow-up from baseline (anemia: 18.1% pre-op vs. 44.4% post-op and iron deficiency: 26.0% pre-op vs. 38.9% post-op) [32]. Moreover, the mean time to recognize iron deficiency after RYGB in men was almost 2 years after that in women with a mean of 29 months [20].
Iron deficiency is more common in women than men, especially premenopausal females [29, 30, 44]. This is noteworthy given that premenopausal women compromise almost 80% of bariatric surgery candidates [44]. Younger age was also found to a be risk for iron deficiency post-RYGB [7, 30, 36].
Limitations
Considerable heterogeneity was observed across studies, likely due to diversity in study participants, baseline iron deficiency, iron supplementation dose, and length of follow-up. There were few RCTs assessing the risk of iron deficiency post-bariatric surgery. The results of this analysis should be interpreted with caution due to the inevitable risk of selection bias with observational studies. Also, due to the small number of studies included in our analysis, we could not confidently assess the risk of bias in the included studies. Most of the studies could not attribute the rate of unclassified anemia to iron deficiency or other micronutrient deficiency, such as vitamin B12 or folate deficiency. Finally, most of our findings are based on observational studies and, thus, causal association cannot be established.
Conclusions
Long-term follow-up for iron deficiency is important after RYGB, especially for those patients with increased risk: premenopausal women, young populations, and those with pre-operative anemia and iron deficiency. Medical and nutritional surveillance is also important during the post-operative period, including the prescription of prophylactic iron and early parenteral replacement when indicated. The incidence of iron deficiency tends to increase with time post-operatively.
References
Maggard MA, Shugarman LR, Suttorp M, Maglione M, Sugerman HJ, Livingston EH et al (2005) Meta-analysis: surgical treatment of obesity. Ann Intern Med 142:547–559
Sjostrom L, Narbro K, Sjostrom CD, Karason K, Larsson B, Wedel H et al (2007) Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 357:741–752
Kushner RF (2006) Micronutrient deficiencies and bariatric surgery. Curr Opin Endocrinol Diabetes 13:405–411
Aasheim ET, Hofso D, Hjelmesaeth J et al (2008) Vitamin status in morbidly obese patients: a cross-sectional study. Am J Clin Nutr 87:362–369
Ernst B, Thurnheer M, Schmid SM et al (2009) Evidence for the necessity to systematically assess micronutrient status prior to bariatric surgery. Obes Surg 19:66–73
Brolin RE, Leung M (1999) Survey of vitamin and mineral supplementation after gastric bypass and biliopancreatic diversion for morbid obesity. Obes Surg 9:150–154
Brolin RE, LaMarca LB, Kenler HA, Cody RP (2002) Malabsorptive gastric bypass in patients with superobesity. J Gastrointest Surg 6:195–203
van Rutte PWJ, Aarts EO, Smulders JF, Nienhuijs SW (2014) Nutrient deficiencies before and after sleeve gastrectomy. Obes Surg 24:1639–1646
von Drygalski A, Andris DA (2009) Anemia after bariatric surgery: more than just iron deficiency. Nutr Clin Pract 24:217–226
Malinowski SS (2006) Nutritional and metabolic complications of bariatric surgery. Am J Med Sci 331:219–225
Marinella MA (2008) Anemia following Roux-en-Y surgery for morbid obesity: a review. South Med J 101:1024–1031
Kalfarentzos F, Kechagias I, Soulikia K et al (2001) Weight loss following vertical banded gastroplasty: intermediate results of a prospective study. Obes Surg 11:265–270
Kheniser KG, Kashyap SR, Schauer PR, Lam ET, Kullman ES (2017) Prevalence of anemia in subjects randomized into Roux-en-Y gastric bypass or sleeve gastrectomy. Obes Surg 27(5):1381–1386
Kwon Y, Kim HJ, Lo Menzo E, Park S, Szomstein S, Rosenthal RJ (2014) Anemia, iron and vitamin B12 deficiencies after sleeve gastrectomy compared to Roux-en-Y gastric bypass: a meta-analysis. Surg Obes Relat Dis 10(4):589–597
PLoS Medicine (OPEN ACCESS), Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(6):e1000097. https://doi.org/10.1371/journal.pmed1000097
Wells GA, Shea B, O’connell D, Peterson JE, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses
Hakeam HA, O’Regan PJ, Salem AM, Bamehriz FY, Eldali AM (2009) Impact of laparoscopic sleeve gastrectomy on iron indices: 1 year follow-up. Obes Surg 19(11):1491–1496
Toh SY, Zarshenas N, Jorgensen J (2009) Prevalence of nutrient deficiencies in bariatric patients. Nutrition 25(11):1150–1156
Kehagias I, Karamanakos SN, Argentou M, Kalfarentzos F (2011) Randomized clinical trial of laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy for the management of patients with BMI < 50 kg/m2. Obes Surg 21(11):1650–1656
Brolin RE et al (1998) Prophylactic iron supplementation after Roux-en-Y gastric bypass: a prospective, double-blind, randomized study. Arch Surg 133(7):740–744
Coupaye M, Puchaux K, Bogard C, Msika S, Jouet P, Clerici C, Larger E, Ledoux S (2009) Nutritional consequences of adjustable gastric banding and gastric bypass: a 1-year prospective study. Obes Surg 19(1):56–65
Moizé V, Andreu A, Flores L, Torres F, Ibarzabal A, Delgado S, Lacy A, Rodriguez L, Vidal J (2013) Long-term dietary intake and nutritional deficiencies following sleeve gastrectomy or Roux-En-Y gastric bypass in a Mediterranean population. J Acad Nutr Diet 113(3):400–410
Ruz M, Carrasco F, Rojas P, Codoceo J, Inostroza J, Rebolledo A, Basfi-fer K, Csendes A, Papapietro K, Pizarro F, Olivares M (2009) Iron absorption and iron status are reduced after Roux-en-Y gastric bypass. Am J Clin Nutr 90(3):527–532
Van Rutte PW, Aarts EO, Smulders JF, Nienhuijs SW (2014) Nutrient deficiencies before and after sleeve gastrectomy. Obes Surg 24(10):1639–1646
Aarts EO, van Wageningen B, Janssen IM, Berends FJ (2012) Prevalence of anemia and related deficiencies in the first year following laparoscopic gastric bypass for morbid obesity. J Obes 13:2012
Amaral JF et al (1985) Prospective hematologic evaluation of gastric exclusion surgery for morbid obesity. Ann Surg 201(2):186
Ruz M, Carrasco F, Rojas P, Codoceo J, Inostroza J, Basfi-fer K, Valencia A, Csendes A, Papapietro K, Pizarro F, Olivares M (2012) Heme-and nonheme-iron absorption and iron status 12 mo after sleeve gastrectomy and Roux-en-Y gastric bypass in morbidly obese women. Am J Clin Nutr 96(4):810–817
Saif T, Strain GW, Dakin G, Gagner M, Costa R, Pomp A (2012) Evaluation of nutrient status after laparoscopic sleeve gastrectomy 1, 3, and 5 years after surgery. Surg Obes Relat Dise 8(5):542–547
Blume CA, Boni CC, Casagrande DS, Rizzolli J, Padoin AV, Mottin CC (2012) Nutritional profile of patients before and after Roux-en-Y gastric bypass: 3-year follow-up. Obes Surg 22(11):1676–1685
Gesquiere I, Lannoo M, Augustijns P, Matthys C, Van der Schueren B, Foulon V (2014) Iron deficiency after Roux-en-Y gastric bypass: insufficient iron absorption from oral iron supplements. Obes Surg 24(1):56–61
Salgado W, Modotti C, Nonino CB, Ceneviva R (2014) Anemia and iron deficiency before and after bariatric surgery. Surg Obes Relat Dis. 10(1):49–54
Skroubis G, Sakellaropoulos G, Pouggouras K, Mead N, Nikiforidis G, Kalfarentzos F (2002) Comparison of nutritional deficiencies after Rouxen-Y gastric bypass and after biliopancreatic diversion with Roux-en-Y gastric bypass. Obes Surg 12(4):551–558
Vargas-Ruiz AG, Hernández-Rivera G, Herrera MF (2008) Prevalence of iron, folate, and vitamin B12 deficiency anemia after laparoscopic Roux-en-Y gastric bypass. Obes Surg 18(3):288–293
Al-Mutawa A, Al-Sabah S, Anderson AK, Al-Mutawa M (2018) Evaluation of nutritional status post laparoscopic sleeve gastrectomy—5-year outcomes. Obes Surg 28(6):1473–1483
Monaco-Ferreira DV, Leandro-Merhi VA (2017) Status of iron metabolism 10 years after Roux-en-Y gastric bypass. Obes Surg 27(8):1993–1999
Flancbaum L, Belsley S, Drake V, Colarusso T, Taylor E (2006) Preoperative nutritional status of patients undergoing Roux-en-Y gastric bypass for morbid obesity. J Gastrointest Surg 10:1033–1037
Parrott J, Frank L, Rabena R, Craggs-Dino L, Isom KA, Greiman L (2017) American Society for Metabolic and Bariatric Surgery integrated health nutritional guidelines for the surgical weight loss patient 2016 update: micronutrients. Surg Obes Relat Dis 13(5):727–741
Parkes E (2006) Nutritional management of patients after bariatric surgery. Am J Med Sci 331(4):207–213
Colossi FG, Casagrande DS, Chatkin R et al (2008) Need for multivitamin use in the postoperative period of gastric bypass. Obes Surg 18:187–191
Damms-Machado A, Friedrich A, Kramer KM et al (2012) Pre- and postoperative nutritional deficiencies in obese patients undergoing laparoscopic sleeve gastrectomy. Obes Surg 22:881–889
Gehrer S, Kern B, Peters T et al (2010) Fewer nutrient deficiencies after laparoscopic sleeve gastrectomy (LSG) than after laparoscopic Roux-Y-gastric bypass (LRYGB)-a prospective study. Obes Surg 20(447–53):15
Alvarez-Leite JI (2004) Nutrient deficiencies secondary to bariatric surgery. Curr Opin Clin Nutr Metab Care 7:5669–5675
Malindowski SS (2006) Nutritional and metabolic complications of bariatric surgery. Am J Med Sci 33(14):219–225
Aills L, Blankenship J et al (2008) ASMBS Allied Health Nutritional Guidelines for the surgical weight loss patient. Surg Obes Relat Dis 4:S73–S108
Funding
None
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Ghada Enani, Elif Bilgic, Ekaterina Lebedeva, Megan Delisle, Ashley Vergis, and Krista Hardy have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Enani, G., Bilgic, E., Lebedeva, E. et al. The incidence of iron deficiency anemia post-Roux-en-Y gastric bypass and sleeve gastrectomy: a systematic review. Surg Endosc 34, 3002–3010 (2020). https://doi.org/10.1007/s00464-019-07092-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07092-3