
Abstract
Background
The first global survey of bariatric/metabolic surgery based on data from the nations or national groupings of the International Federation for the Surgery of Obesity and Metabolic Diseases (IFSO) was published in 1998, followed by reports in 2003, 2009, 2011, and 2012. In this survey, we report a global overview of worldwide bariatric surgery in 2013.
Materials and Methods
A questionnaire evaluating the number and the type of bariatric procedure performed in 2013 was emailed to all members of bariatric societies belonging to IFSO. Trend analyses from 2003 to 2013 were also performed.
Results
There were 49/54 (90.7 %) responders; 37 of the 49 with national registries. The total number of bariatric procedures performed worldwide in 2013 was 468,609, 95.7 % carried out laparoscopically. The highest number (n = 154,276) was from the USA/Canada region. The most commonly performed procedure in the world was Roux-en-Y gastric bypass (RYGB), 45 %; followed by sleeve gastrectomy (SG), 37 %; and adjustable gastric banding (AGB), 10 %. Most significant were the rise in prevalence of SG from 0 to 37 % of the world total from 2003 to 2013, and the fall in AGB of 68 % from its peak in 2008 to 2013.
Conclusions
SG is currently the most frequently performed procedure in the USA/Canada and in the Asia/Pacific regions, and second to RYGB in the Europe and Latin/South America regions. The accuracy of the IFSO-based world survey of procedures would be enhanced if each nation or national group would create a national registry.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bariatric surgery is currently considered the most effective treatment option for morbid obesity; it results in greater improvement in weight loss outcomes and obesity-related comorbidities when compared with non-surgical interventions, regardless of the type of surgical procedure used [1, 2]. Different surgical options are available, and they are continuously evolving, influenced by literature results, specific local conditions, and the experience of the surgical staff in each country.
Bariatric surgery worldwide surveys have previously been published. The first global survey of bariatric/metabolic surgery was reported by Scopinaro in 1998 [3], after which Buchwald presented follow-up reports for 2003, 2009, and 2011 [4–6]. In a book chapter, Angrisani [7] reported the bariatric surgery worldwide survey of 2012. As emphasized by Buchwald in his latest report [6], the periodic assessment of the state of bariatric/metabolic surgery is not only important for the surgical community but also useful to patients and can influence healthcare providers and their resource allocation issues, as well as government analyses.
In this survey, we report a global overview of worldwide bariatric surgery, describing the numbers and types of procedures performed in the nations or national groupings of the International Federation for the Surgery of Obesity and metabolic disorders (IFSO) in 2013. We also performed a trend analysis from 2003 to 2008 to 2011 to 2013 to evaluate how the choice of procedures has changed over the last 10 years.
Methods
Survey
A questionnaire (Table 1) was emailed to the President and Executive Board of each member of bariatric societies belonging to IFSO. If this first contact and request was unanswered, further reminders via email, telephone calls, and personal contacts were initiated. The questionnaire that was e-mailed to IFSO members did not ask to report the surgical revisions separately but suggested to consider them as primary procedures; in fact, the evaluation of the revisional procedures, was not the aim of this survey.
Data Analysis
Tables and graphic presentations were compiled for the obtained data.
The relative prevalence of specific procedures is provided as weighted averages to account for the wide ranges in the number of procedures performed by the different IFSO member nations or national groupings.
Results
Response Rate
Among the 54 national bariatric societies or groups contacted, there were 49 (90.7 %) responders. Table 2 lists the 49 responding societies; 37 out of 49 (75.5 %) provided data from their National Registries. Among them, 34 had recorded all the procedures performed in 2013 in their National Registries; three bariatric societies did not register all the operations in the National Registry but provided partially estimated data. The remaining 12 national bariatric societies had not any National Registries and their data are completely estimated.
Number of Operations Performed
Figure 1 illustrates the number of bariatric procedures from the IFSO surveys that have been published to date. Table 3 showed the number of operations performed in all responding nations of the world. These data are divided into four regions: USA/Canada, Europe, Latin/South America, and Asia/Pacific.

Number of bariatric procedures reported by the bariatric surgery surveys published so far
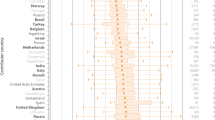
The total population, total bariatric procedures per country, the percentage of procedures for the total population, the total number of bariatric centers, and their number of cases per year are presented in Table 4. The total number of bariatric procedures performed in 2013 was 468,609, 95.7 % of which were carried out laparoscopically. USA/Canada was the region with the highest number of bariatric procedures (n = 154,276).
Other nations or national grouping that reported 10,000 or more bariatric procedures were Brazil (n = 86,840), France (n = 37,300), Argentina (n = 30,378), Saudi Arabia (n = 13,194), Belgium (n = 12,000), Israel (n = 11,452), Australia-New Zealand (n = 10,467), and India (n = 10,002). The number of operations performed as a percentage of the national population never reached 1 %. For the total population of the 54 IFSO nations or national groupings of 4,700,023,295, the 468,609 bariatric/metabolic operations performed in 2013 and represented 0.01 % of the total population. The nation that showed the greatest number of bariatric/metabolic procedures as a function of the total population was Israel (0.14 %).
Table 4 also reports the centers of bariatric/metabolic surgery of each nation/national grouping weighted according to the number of bariatric procedure performed yearly. The highest total number of centers (n = 1441) was in Latin America, but USA/Canada had the greater number of high volume centers (>100 cases/year) (n = 488)
Types of Procedures Performed
The type of procedures reported by USA/Canada, Europe, Latin/South America, and Asia-Pacific was reported in Table 5.
The most commonly performed procedure in the world in 2013 was Roux-en-Y gastric bypass (RYGB), 45 %, followed by sleeve gastrectomy (SG), 37 %, and adjustable gastric banding (AGB), 10 %. No other single procedure exceeded 2.5 %.
Trends
Trend analyses from 2003 to 2013 were performed and are based on the current results and previously published data [4–6].
Worldwide
The worldwide trends expressed as number and percentage of RYGB, SG, AGB, and biliopancreatic diversion/duodenal switch (BPD/DS) are shown in Figs 2 and 3, respectively.

Trends in number of procedures worldwide: from 2003 to 2008 to 2011 to 2013

Trends in percentage of procedures worldwide: from 2003 to 2008 to 2011 to 2013
RYGB decreased from 2003 to 2008 (−16 %) and continued to decrease slightly from 2011 to 2013 (−1.6 %). Nevertheless, it still represents the most performed bariatric/metabolic operation throughout the world.
SG showed a steep increase from 2003 to 2013 (+37 %), thus becoming the second most performed bariatric/metabolic procedure in the world. AGB peaked in 2008 (42.3 %), then had a significant decrease in 2011 (−24.5 %) and in 2013 (−7.8 %). There was a decrease also in BPD/DS: from 4.8 % in 2003 to 1.5 % in 2013.
Regional
USA/Canada
The regional trend in USA/Canada percentages is given in Fig. 4. There was a marked decrease in RYGB from 2003 to 2008 (−34 %), with a plateauing in 2011 (−3 %) and again a significant decrease in 2013 (−11.7 %). SG steadily rose from 2003 to 2011 (+19.2 %) and peaked in 2013 (+23.8 %), becoming the most performed bariatric/metabolic procedure in USA/Canada. From 2003 to 2008, AGB rose from 9.0 to 44.0 % and then fell to 27.2 % in 2011 and to 10 % in 2013.

Trends in percentage of procedures in USA/Canada from 2003 to 2008 to 2011 to 2013
Europe
The regional trend in Europe in percentages is given in Fig. 5. The RYGB rose from 11.1 to 39.0 % between 2003 and 2008, then continued to slightly increase up to 43.5 % in 2011, and finally decreased in 2013 (38 %); however, RYGB still represents the most performed bariatric/metabolic procedure in Europe. SG rose significantly over the 10-year period from 0.0 to 37 %, becoming the second most performed bariatric/metabolic procedure in Europe. AGB fell down from 63.7 in 2003 to 17.8 % in 2011; a further slight reduction in 2013 (15 %) has been observed.

Trends in percentage of procedures in Europe from 2003 to 2008 to 2011 to 2013
Latin/South America
The regional trend in Latin/South America in percentages is given in Fig. 6. From 2003 to 2008, RYGB strongly increased, then plateaued: 57.9 % in 2011; 65 % in 2013; however, RYGB still represents by far the most performed bariatric/metabolic procedure in Latin/South America. SG climbed from 0.0 in 2003 to 9.2 in 2008 to 30.1 % in 2011, but it decreased in 2013 (−5.1 %). AGB fell from 61.5 % in 2003 to 20.4 % (−41.1 %) in 2008 and continued to decrease in 2011 (−15.1 %) and 2013 (−1.3 %).

Trends in percentage of procedures in Latin/South America from 2003 to 2008 to 2011 to 2013
Asia/Pacific
The regional trend in the Asia/Pacific region percentages is given in Fig. 7. RYGB never rose to over 10 % prevalence in the Asia/Pacific region until 2013, when it had a significant increase (25 %) overtaking AGB and becoming the second most performed bariatric/metabolic procedure. SG climbed from 0.0 % in 2003 to 4.1 in 2008 to 55.1 % in 2011, and afterwards had a slight decrease in 2013 (49 %). AGB held steady from 2003 to 2008 (+2.1 %) and then fell in 2011(−49.9 %) and again in 2013 (−18.6 %).

Trends in percentage of procedures in Asia-Pacific from 2003 to 2008 to 2011 to 2013
Discussion
This survey indicates that there has been a constant increase, except for a plateauing in 2011, in the total number of bariatric procedures performed worldwide over the past 10 years. These data, however, must be interpreted with caution when considering the higher response rate of the current survey (90.7 %) when compared to previously published reports [3–6]. Furthermore, a large number of the 54 IFSO member nations or national groupings reported data from their National Registries; whereas, in the previous surveys, data were mainly estimated. For these reasons, the steep increase in the total number of procedures performed from 2011 to 2013 could be at least in part due to more accurate reporting by national societies and their registries.
Our results show that about 0.01 % of the world’s population underwent bariatric surgery in 2013. This percentage appears extremely low if we take into account that the World Health Organization estimates that more than 10 % of the world’s adult population is obese [8]. To date, there is a robust body of literature to support the safety and efficacy of bariatric surgery not only in patients affected by morbid obesity but also in patients with class I obesity (body mass index (BMI) 30–35 kg/m2) [9]. Furthermore, our data demonstrate that about 95.7 % of bariatric procedures were performed laparoscopically in 2013, with less complications and shorter hospital stays compared to previous data with the open approach. The high percentage of minimally-invasive procedures could also be explained by the higher prevalence of centers of excellence and bariatric accreditation programs in the nations or national groupings of the survey.
Within the total number of procedures performed, there have been marked shifts in the relative percentages of the specific bariatric operations being done. Worldwide trends over the past 10 years show a decrease in the number of RYGB; nevertheless, this operation still represents the most performed bariatric/metabolic operation throughout the world. However, analysis of the regional trends demonstrate that only in Latin/South America, and less evidently in Europe, does RYGB remains the most performed bariatric/metabolic procedure; in the other regions (USA/Canada and Asia Pacific), it has been overtaken by SG, which has become the most frequently performed procedure in these regions. Our data indicate that SG worldwide climbed from 0 to 37 % of total procedures between 2003 and 2013. From 2011 to 2013, SG increased in all the analyzed geographic areas; in USA/Canada, a nearly 2.5-fold increase was observed. The easier surgical technique of SG compared to RYGB, together with the promise in short-term weight loss outcomes, could explain the steep increase of this procedure worldwide. Long-term proof of the efficacy of SG is starting to be available [10]; however, they are still limited to small patient samples. At the same time, this survey confirms the steep reciprocal decrease of AGB throughout the world, as previously reported in the bariatric surgery survey of 2011 [6].
There are several limitations in this survey. The first is that among the 49 responding nations or national groupings, 12 bariatric societies had no National Registries and provided completely estimated data, while three societies, although they had National Registries, declared that the procedures were only partially recorded. The second one was that we were not able to know how the member of the societies came up with the estimates and/or utilized the registries in developing their estimates. Moreover, the national registries often did not include the bariatric procedures performed in private healthcare. Therefore, the number of bariatric procedures actually performed in the world could be greater compared to the figures examined in the survey.
Finally, we reported as “others” the procedures that were not listed in the questionnaire. In fact, most national bariatric societies did not specify which were the procedures included as “others” and in some countries, such as USA/Canada, the total amount of procedures listed as others were enormous (n = 15,792).
National and International registries are very useful and accurate to analyze the procedure outcomes, but they require time and resources. National and International survey addressing number and type of Bariatric and Metabolic procedures are much simpler, less expensive, and provide some important information to the IFSO Bariatric Surgeons community.
Therefore, the report of this worldwide survey should encourage all the IFSO nations or national groupings to create a national registry and/or collect in detail all the bariatric procedures performed (including those in private healthcare) and improve the accuracy of the data.
References
Picot J1, Jones J, Colquitt JL, Gospodarevskaya E, Loveman E, Baxter L, Clegg AJ. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess. 2009;13(41):1–190, 215–357, iii-iv. doi:10.3310/hta13410
Colquitt JL, Pickett K, Loveman E, et al. Surgery for weight loss in adults. Cochrane Database Syst Rev. 2014;8:CD003641.
Scopinaro N. The IFSO and obesity surgery throughout the world. Obes Surg. 1998;8:3–8.
Buchwald H, Williams SE. Bariatric surgery worldwide 2003. Obes Surg. 2004;14:1157–64.
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2008. Obes Surg. 2009;19(12):1605–11. doi:10.1007/s11695-009-0014-5.
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2011. Obes Surg. 2013;23(4):427–36. doi:10.1007/s11695-012-0864-0.
AngrisaniL, Lorenzo M. Bariatric Surgery Worldwide: Overview and Results. Foletto, Rosenthal Springer-Verlag 2014
World Health Organization. Obesity and overweight fact sheet N° 311, August 2014. http://www.who.int/mediacentre/factsheets/fs311/en/. Accessed Oct 2014
Busetto L, Dixon J, De Luca M, et al. Bariatric surgery in class I obesity: a Position statement from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes Surg. 2014;24(4):487–519. doi:10.1007/s11695-014-1214-1.
Diamantis T, Apostolou KG, Alexandrou A, et al. Review of long-term weight loss results after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2014;10(1):177–83. doi:10.1016/j.soard.2013.11.007.
Acknowledgments
We thank Francesco Carignani and Manuela Mazzarella of IFSO Secretariat for their support.
Conflict of Interest Statement
L. Angrisani, A. Santonicola, P. Iovino, G. Formisano, H. Buchwald, N. Scopinaro have not any conflicts of interest to declare.
Statement of Informed Consent
This is a survey in which we do not directly involve human beings but we just analyze the number of bariatric procedures performed around the world.
Statement of Human and Animal Rights
This is a survey in which we do not directly involve human beings or animals but we just analyze the number of bariatric procedures performed around the world
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Angrisani, L., Santonicola, A., Iovino, P. et al. Bariatric Surgery Worldwide 2013. OBES SURG 25, 1822–1832 (2015). https://doi.org/10.1007/s11695-015-1657-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-015-1657-z