
Abstract
Purpose
The purpose of this study is to develop a radiomics model for predicting the Ki-67 proliferation index in patients with invasive ductal breast cancer through magnetic resonance imaging (MRI) preoperatively.
Materials and methods
A total of 128 patients who were clinicopathologically diagnosed with invasive ductal breast cancer were recruited. This cohort included 32 negative Ki67 expression (Ki67 proliferation index < 14%) and 96 cases with positive Ki67 expression (Ki67 proliferation index ≥ 14%). All patients had undergone diffusion-weighted imaging (DWI) MRI before surgery on a 3.0T MRI scanner. Radiomics features were extracted from apparent diffusion coefficient (ADC) maps which were obtained by DWI-MRI from patients with invasive ductal breast cancer. 80% of the patients were divided into training set to build radiomics model, and the rest into test set to evaluate its performance. The least absolute shrinkage and selection operator (LASSO) was used to select radiomics features, and then, the logistic regression (LR) model was established using fivefold cross-validation to predict the Ki-67 index. The performance was evaluated by receiver-operating characteristic (ROC) analysis, accuracy, sensitivity and specificity.
Results
Quantitative imaging features (n = 1029) were extracted from ADC maps, and 11 features were selected to construct the LR model. Good identification ability was exhibited by the ADC-based radiomics model, with areas under the ROC (AUC) values of 0.75 ± 0.08, accuracy of 0.71 in training set and 0.72, 0.70 in test set.
Conclusions
The ADC-based radiomics model is a feasible predictor for the Ki-67 index in patients with invasive ductal breast cancer. Therefore, we proposed that three-dimensional imaging features from ADC maps could be used as candidate biomarker for preoperative prediction the Ki-67 index noninvasively.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Breast cancer is a highly heterogeneous disease and the most common cancer in women [1]. 2011 St. Gallen panel suggests using immunohistochemical (IHC) biomarkers including estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2) and Ki-67 as substitutive molecular subtypes [2].
Ki-67 is a non-histone nuclear protein expressed during every active phases of the cell cycle, except G0, and also an important factor in the synthesis of ribosomes in dividing cells. It is considered to be one of the most reliable indicators to evaluate the degree of proliferation of malignant tumor cells [3]. For breast cancer, Ki-67 has been proposed as a clinically valuable marker to distinguish the two subtypes of ER-positive and HER2-negative breast cancers as Luminal A and Luminal B breast cancers. Luminal A subtypes were less responsive to chemotherapy, whereas luminal B subtypes were responsive not only to chemotherapy but also to endocrinotherapy plus molecular-targeted therapy [4]. Therefore, the Ki-67 index could be a potential indicator for the treatment of ER-positive and HER2-negative breast cancer patients. A meta-analysis conducted by Petrelli et al. from 41 studies (including 64,196 breast cancer patients) was reported that there was a distinct correlation between Ki-67 expression and disease-free survival and overall survival [5].
Therefore, early detection of such highly malignant breast cancer has great significance in aspects of patients’ prognosis, diagnosis and treatment. So far, the detection of these molecular markers relies mainly on immunohistochemical analysis from core needle biopsy or surgically removed samples which are only partial tumor tissue. Such method has certain limitation considering the heterogeneity of tumors, especially the larger ones. On the contrary, imaging can provide overall anatomical and functional properties of tumor tissue.
Diffusion-weighted imaging can use the diffusion motion of water molecule in vivo to display the spatial information and cell density in human tissues at molecular level [6]. The parameter apparent diffusion coefficient (ADC) is the most commonly used clinical parameter that reflects the degree of tissue distribution for the diffusion of water molecule. ADC (mm2/s) is calculated based on at least two b-values, and then a corresponding parameter map (ADC map) is formed. Displaying the correlation between ADC values and cell density is one of the advantages of the ADC maps. Moreover, ADC values are related to the Ki-67 index according to previous studies [7].
At present, the technology of imaging has gradually developed toward the direction of automated analysis and high-throughput extraction of quantitative features which perfectly concluded the conception of radiomics [8,9,10]. Since the theoretical basis of radiomics is heterogeneities and genetic heterogeneity is ubiquitous in tumor tissues generating different imaging phenotypes. Radiomics is a procedure which is designed to extract a great number of quantitative features from digital images, and further, highly diversified statistical analysis is used to obtain the key information from the data pool. The processed information can significantly facilitate the diagnosis and treatment of the disease. Recently, most studies on radiomics mainly focus on topics in respects of tumor molecular subtype [11], diagnosis [12, 13], stage classification [14], genetic phenotype prediction [15], treatment selection [16] and tumor prognosis [17]. In a study by Liang, C, a radiomics classifier based on T2WI was an important predictor of Ki-67 index in breast cancer patients [18] which suggested that noninvasive evaluation of the Ki-67 index can be performed preoperatively by radiomics.
No studies have been done so far to evaluate the correlation between DWI-MRI and the Ki-67 index based on radiomics. Therefore, our work aims to assess the accuracy of ADC-based radiomics to noninvasively predict the Ki-67 index in patients with breast cancer preoperatively.
Materials and methods
Patients
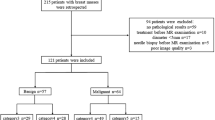
Our institutional review board approved this retrospective study and abandoned the informed consent requirement. A total of 128 selected patients with pathologically confirmed invasive ductal breast cancer at our hospital between April 2013 and December 2018 were included in this study. Inclusion criteria include: (1) All patients had undergone DWI-MRI; (2) No treatment received before surgery; (3) Pathologically verified invasive ductal breast cancer; (4) IHC examination including the Ki-67 index.
Ultimately, 128 patients were analyzed and randomly divided into the training dataset (n = 101) and the test dataset (n = 27) by 80% and 20%.
Immunohistochemistry of Ki-67
The expression status of Ki-67 was measured via standard IHC examinations. The Ki-67 proliferation index was analyzed by counting the percentage of positively stained malignant cells. Less than 14% positive staining was identified as negative expression, while more than 14% positive staining was identified as positive expression [2].
MR data acquisition
Magnetom Verio 3.0T system (Siemens, Erlangen, Germany) (81 patients) or a Discovery MR750w 3.0T system (General Electric Healthcare, GE, Milwaukee, USA) (47 patients) was applied together with an eight-channel phased-array breast coil which was placed under the patient in a prone position. The diffusion-weighted images’ parameters (for both equipments) are reported in Table 1. DWI images were acquired using two b-values (namely, 50, 800 s/mm2). The Siemens or GE workstation generates ADC maps automatically.
Tumor segmentation
Preoperative MRIs were analyzed by two radiologists with two- and ten-years’ experience. Because of the higher resolution of DWI compared to ADC maps, the regions of interest (ROI) were delineated on DWI with the b-value of 800 s/mm2 at first and then copied to the corresponding ADC maps on each slice. Then, the computer automatically generated the three-dimensional volume of interest (VOI).
Intensity normalization
The inconsistency in intensity information is unavoidable in imaging and storage of medical images. We normalized the intensity of the MRI image using the following formula to minimize the intensity inconsistency [f(x) the normalized intensity, x the original intensity, μ mean value, \( \delta \) variance, s optional scaling, by default, it is set to 1] [19].
Radiomics feature extraction
A total of 1029 features were extracted and divided into three categories: first order statistic, shape-based and texture. The latter includes Gray Level Co-occurrence Matrix (GLCM), Gray Level Run Length Matrix (GLRLM) and Gray Level Size Zone Matrix (GLSZM). All features except the shape-based also calculated on the original image and derived images obtained by applying several filters. Because the shape-based features were independent of gray value which extracted from the tumor mask. The filtering method includes wavelet, square, square root, logarithm and exponential. The features were extracted using Radcloud platform (Huiying Medical Technology (Beijing) Co., Ltd) [20].
Statistical analyses
Statistical analysis of the characteristic of patients in the training and validation sets was assessed using SPSS software (version 24, IBM). The continuous variables with normal distribution were shown as mean ± SD. An independent t test was used for continuous variables when the data are normally distributed and the variance is homogeneity. Fisher’s exact test or the Chi-square test was used for comparing categorical variables between the two groups, as appropriate. A two-sided P value < 0.05 was used to indicate statistical significance.
All of the other analysis was performed using Radcloud platform (Huiying Medical Technology (Beijing) Co., Ltd) [20].
Least absolute shrinkage and selection operator (LASSO) controls the complexity of the model through a series of parameters to avoid overfitting. For example, it has a tuning parameter to control the penalty of the linear model, which guarantees the minimum penalty when obtaining a model with a smaller number of features, where the penalty is mean square error (MSE). In addition, another parameter controls the correlation of features, making the selected features less relevant. The optimization goal of LASSO is
X the matrix of radiomic features, y the vector of the sample labels, n the number of samples, w the coefficient vector of the regression model, \( {\text{alpha}}^{*} \parallel w\parallel \), LASSO penalty.
The best parameter set was computed using a cross-validation method with fivefolds. After feature selection, the logistic regression (LR) model was established using fivefold cross-validation. Logistic regression is a classification model that mainly solves the two-classification problem. The process of logistic regression is to establish a cost function for a regression or classification problem and then iteratively obtain the optimal model parameters through the optimization method.
The function of the logistic regression model is
Among them, \( g\left( z \right) = \frac{1}{{1 + e^{ - z} }} \)
The L1 regularized logistic regression solves the following optimization problem:
X the matrix of radiomic features, y the vector of the sample labels, w the coefficient vector of the LR model, C inverse of regularization strength.
The training data were randomly divided into five groups, of which every four groups were chosen as the training set and the remaining group as the validation set. The average value of the five results was adopted to assess the generalization of the classification models and the accuracy of the algorithm.
We evaluated the performance of selected features in classifying patients according to their Ki-67 level. We evaluated the performance of selected features in classifying patients according to their Ki-67 level by receiver-operating characteristic (ROC) analysis, and calculated the area under the ROC curve (AUC), accuracy, sensitivity and specificity.
Result
The radiomics workflow and study flowchart of the study are depicted in Fig. 1.

Radiomics workflow and study flowchart
Patients’ characteristics
A total of 128 patients (53 ± 11 years) were recruited in this study. Among which, 25% were classified as Ki-67 negative, and 75% were Ki-67 positive. The detailed clinical characteristics of patients in the training and validation sets are listed in Table 2.
Radiomics feature selection
In total, 1029 features were extracted from the ADC maps. Eleven features were selected by Lasso (Fig. 2). Finally, eleven features were confirmed, and they are
wavelet-LLL_firstorder_Skewness,
squareroot_firstorder_RobustMeanAbsoluteDeviation, exponential_glrlm_RunLengthNonUniformityNormalized,
wavelet-HLH_firstorder_Skewness, wavelet-LHH_glcm_Correlation,
exponential_firstorder_Median, original_firstorder_Minimum,
original_shape_SurfaceVolumeRatio,
original_glcm_ClusterShade,
square_glcm_Idmn,
square_firstorder_Skewness (Table 3).

Lasso algorithm on feature select. a Mean squared error (MSE) path, b Lasso path using Lasso model, 11 features which are correspond to the optimal alpha value were selected
Radiomics-based Ki-67 prediction
The linear combination of the features and their corresponding coefficients was as follows: Z = 0.22302
+ Wavelet-LLL_firstorder_Skewness × − 0.77799
+ Squareroot_firstorder_RobustMeanAbsoluteDeviation × − 0.46000
+ Exponential_glrlm_RunLengthNonUniformityNormalized × − 0.44454
+ Wavelet-HLH_firstorder_Skewness × − 0.47110
+ Wavelet-LHH_glcm_Correlation × − 0.20421
+ Exponential_firstorder_Median × − 0.04225
+ Original_firstorder_Minimum × − 0.02037
+ Original_shape_SurfaceVolumeRatio × − 0.09180
+ Original_glcm_ClusterShade × − 0.00001
+ Square_glcm_Idmn × 0.01408
+ Square_firstorder_Skewness × 0.278246
The radiomics classifier based on ADC map shows good performance for the classification of Ki-67 index with a ROC curve and is presented in Fig. 3. The classifier used eleven features to compute an AUC value of 0.75 ± 0.08 (95% CI 0.696, 0.833) in the training dataset and an AUC value of 0.72 (95% CI 0.495, 0.857) in the test dataset (Table 4).

ROC curve of radiomic models in discrimination of patients with negative and positive Ki-67 index. a Training set, b Test set
Discussion
In this study, we investigated whether features derived from ADC maps of patients with invasive ductal breast cancer could be used as a preoperative predictor of the Ki-67 index. The radiomics classifier demonstrated high performance for differentiation between low and high Ki-67 index.
Many previous studies have mentioned immunohistochemical expression of Ki-67 as a prognostic and predictive marker for breast cancer [21]. But as we mentioned, core needle biopsy testing only takes part of the tumor sample tissue, the value of the Ki-67 index may be limited because it ignores the possible heterogeneity of tumors. While, imaging can provide overall anatomical and functional properties of tumor tissue. Thus, there is room for radiological improvement to assist in assessing the actual Ki-67 index.
DWI as a supplementary diagnostic sequence for breast lesions shows an important clinical role [22]. The pathological mechanism of ADC value applied to breast tumors is that the proliferation of tumor cells can lead to an increase in cell quantity, a disordered tissue structure and the narrowing of extracellular space, which eventually result in a restricted motion of water molecules in the intercellular spaces of tissues [23]. Tumors with lower ADC values have a higher cell density, proliferation index and more aggressive. In previous studies of invasive duct cancer, ADC showed negative correlations with the Ki-67 index, as by Li, L and colleagues on 124 patients, and Molinari and colleagues on 115 patients [7, 24]. Supporting the potential of ADC value can be a great help to the development of predicting the Ki-67 index preoperatively. Another reason for us to compute the radiomic features on ADC maps is the ability to assess the motion of water molecules shows good reproducibility between different MR systems with same field strength and the same range of b-values [25, 26]. This characteristic indicates that they are useful in multicenter studies because the scanners are usually different.
The concept of radiomics was first proposed by Dutch scholar Lambin, the idea of which originated from tumor heterogeneity, in 2012 [27]. Compared with traditional proteomics and genomics methods, radiomics can noninvasively evaluate tumors, their microenvironment and predict tumor genetic heterogeneity [28]. Breast cancer has a high degree of heterogeneity, and there are different image performance because of its different lesion size, shape, brightness and texture features values [29]. In our study, we used radiomics to quantitatively extract the characteristics of the tumor’s internal diffusion based on the ADC map, thereby reflecting the inhomogeneous characteristics of the tumor’s internal structure. Certain researches have indicated that radiomics can provide more detailed information on the correlation between images and Ki-67 expression level. Liang and Ma [18, 31] reported that the T2WI- and DCE-MRI-based radiomics classifier were an important predictor of the Ki-67 index in breast cancer patients, with accuracy of 0.729 and 0.757, respectively. The accuracy of this study in validation set is 0.70 and is very approaching to those two accuracy values above. But in these studies, they only performed two-dimensional analysis of the largest section, which may not fully assess the heterogeneity of breast cancer. In our research, three-dimensional analysis of the entire tumor was used, which can take full account of the heterogeneity of the breast cancer.
This study used LR to construct a radiomics model for predicting the ki67 index of invasive ductal breast cancer. LR is capable for small data sets; its algorithm is clear and distinct. Moreover, the probability of LR can be explained reasonably, which means that the fitted parameters can reflect the impact of each feature on the result. Therefore, this algorithm has a good interpretability. Previous studies have shown the advantage of LR algorithms in building useful models for other tumors [32,33,34]. Fusco [30] reported that a multiple classifier system combining decision tree and Bayesian classifier can optimize the accuracy for breast lesion classification (twenty-six malignant and 22 benign breast lesions). However, only one common algorithm was used in our study and more algorithms should be tested in future research.
The limitation of this study is that the number of patients is not large enough. External validation cannot be done due to insufficient data and the diagnostic accuracy might be overestimated. It must be emphasized that even if a radiomics classifier shows good results for a small number of patients, it must be validated with a larger sample before it can be extended to clinical use [35]. However, we believe that these data are sufficient enough to prompt a larger clinical research on the value of radiomics based on ADC maps in the Ki-67 index, allowing better decisions on preoperative prediction indications. In the end, future studies are required to assess the value as well as feature repeatability of radiomics biomarkers in independent and prospective validation cohorts by using larger sample size.
In summary, our ADC-based radiomics classifier can effectively predict Ki-67 index in patients with invasive ductal breast cancer before surgery. This radiomics classifier may help to preoperatively predict Ki-67 index in breast cancer patients.
References
Siegel RL, Miller KD, Jemal A (2017) Cancer Statistics, 2017. CA Cancer J Clin 67:7–30
Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thurlimann B, Senn HJ et al (2011) Strategies for subtypes–dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol 22:1736–1747
MacCallum DE, Hall PA (2000) The location of pKi67 in the outer dense fibrillary compartment of the nucleolus points to a role in ribosome biogenesis during the cell division cycle. J Pathol 190:537–544
Cheang MC, Chia SK, Voduc D, Gao D, Leung S, Snider J et al (2009) Ki67 index, HER2 status, and prognosis of patients with luminal B breast cancer. J Natl Cancer Inst 101:736–750
Petrelli F, Viale G, Cabiddu M, Barni S (2015) Prognostic value of different cut-off levels of Ki-67 in breast cancer: a systematic review and meta-analysis of 64,196 patients. Breast Cancer Res Treat 153:477–491
Park SH, Choi HY, Hahn SY (2015) Correlations between apparent diffusion coefficient values of invasive ductal carcinoma and pathologic factors on diffusion-weighted MRI at 3.0 Tesla. Journal of magnetic resonance imaging. J Magn Reson Imaging JMRI 41:175–182
Molinari C, Clauser P, Girometti R, Linda A, Cimino E, Puglisi F et al (2015) MR mammography using diffusion-weighted imaging in evaluating breast cancer: a correlation with proliferation index. Radiol Med (Torino) 120:911–918
Gillies RJ, Kinahan PE, Hricak H (2016) Radiomics: images are more than pictures, they are data. Radiology 278:563–577
Kumar V, Gu Y, Basu S, Berglund A, Eschrich SA, Schabath MB et al (2012) Radiomics: the process and the challenges. Magn Reson Imaging 30:1234–1248
Aerts HJ, Velazquez ER, Leijenaar RT, Parmar C, Grossmann P, Carvalho S et al (2014) Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat Commun 5:4006
Itakura H, Achrol AS, Mitchell LA, Loya JJ, Liu T, Westbroek EM et al (2015) Magnetic resonance image features identify glioblastoma phenotypic subtypes with distinct molecular pathway activities. Sci Transl Med 7:303ra138
Huang YQ, Liang CH, He L, Tian J, Liang CS, Chen X et al (2016) Development and validation of a radiomics nomogram for preoperative prediction of lymph node metastasis in colorectal cancer. J Clin Oncol Off J Am Soc Clin Oncol 34:2157–2164
Fusco R, Sansone M, Filice S, Granata V, Catalano O, Amato DM et al (2015) Integration of DCE-MRI and DW-MRI Quantitative parameters for breast lesion classification. Biomed Res Int 2015:237863
Liang C, Huang Y, He L, Chen X, Ma Z, Dong D et al (2016) The development and validation of a CT-based radiomics signature for the preoperative discrimination of stage I-II and stage III-IV colorectal cancer. Oncotarget 7:31401–31412
Liu Y, Kim J, Balagurunathan Y, Li Q, Garcia AL, Stringfield O et al (2016) Radiomic features are associated with EGFR mutation status in lung adenocarcinomas. Clin Lung Cancer 17(441–8):e6
Kickingereder P, Gotz M, Muschelli J, Wick A, Neuberger U, Shinohara RT et al (2016) Large-scale radiomic profiling of recurrent glioblastoma identifies an imaging predictor for stratifying anti-angiogenic treatment response. Clin Cancer Res 22:5765–5771
Ouyang FS, Guo BL, Zhang B, Dong YH, Zhang L, Mo XK et al (2017) Exploration and validation of radiomics signature as an independent prognostic biomarker in stage III–IVb nasopharyngeal carcinoma. Oncotarget 8:74869–74879
Liang C, Cheng Z, Huang Y, He L, Chen X, Ma Z et al (2018) An MRI-based radiomics classifier for preoperative prediction of Ki-67 status in breast cancer. Acad Radiol 25:1111–1117
Freedman D, Pisani R, Purves R (2007) Statistics: fourth international student edition. W.W. Norton & Company. ISBN 9780393930436
Wu J, Tha KK, Xing L, Li R (2018) Radiomics and radiogenomics for precision radiotherapy. J Radiat Res 59:i25–i31
de Azambuja E, Cardoso F, de Castro G, Colozza M, Mano MS, Durbecq V et al (2007) Ki-67 as prognostic marker in early breast cancer: a meta-analysis of published studies involving 12,155 patients. Br J Cancer 96:1504–1513
Altay C, Balci P, Altay S, Karasu S, Saydam S, Canda T et al (2014) Diffusion-weighted MR imaging: role in the differential diagnosis of breast lesions. JBR-BTR: organe de la Societe royale belge de radiologie (SRBR) = orgaan van de Koninklijke Belgische Vereniging voor Radiologie (KBVR) 97:211–216
Jin G, An N, Jacobs MA, Li K (2010) The role of parallel diffusion-weighted imaging and apparent diffusion coefficient (ADC) map values for evaluating breast lesions: preliminary results. Acad Radiol 17:456–463
Li L, Wang K, Sun X, Wang K, Sun Y, Zhang G et al (2015) Parameters of dynamic contrast-enhanced MRI as imaging markers for angiogenesis and proliferation in human breast cancer. Med Sci Monit Int Med J Exp Clin Res 21:376–382
Ye XH, Gao JY, Yang ZH, Liu Y (2014) Apparent diffusion coefficient reproducibility of the pancreas measured at different MR scanners using diffusion-weighted imaging. J Magn Reson imaging JMRI 40:1375–1381
Thomassin-Naggara I, De Bazelaire C, Chopier J, Bazot M, Marsault C, Trop I (2013) Diffusion-weighted MR imaging of the breast: advantages and pitfalls. Eur J Radiol 82:435–443
Lambin P, Rios-Velazquez E, Leijenaar R, Carvalho S, van Stiphout RG, Granton P et al (2012) Radiomics: extracting more information from medical images using advanced feature analysis. Eur J Cancer 48:441–446
Gillies RJ (2015) Abstract CN01-01: The radiology reading room of the future. Mol Cancer Ther 14:CN01-CN
Joseph C, Papadaki A, Althobiti M, Alsaleem M, Aleskandarany MA, Rakha EA (2018) Breast cancer intra-tumour heterogeneity: Current status and clinical implications. Histopathology 73:717–731
Fusco R, Di Marzo M, Sansone C, Sansone M, Petrillo A (2017) Breast DCE-MRI: lesion classification using dynamic and morphological features by means of a multiple classifier system. Eur Radiol Exp 1:10
Ma W, Ji Y, Qi L, Guo X, Jian X, Liu P (2018) Breast cancer Ki67 expression prediction by DCE-MRI radiomics features. Clin Radiol 73:909
Liang M, Cai Z, Zhang H, Huang C, Meng Y, Zhao L, et al. (2019) Machine learning-based analysis of rectal cancer MRI radiomics for prediction of metachronous liver metastasis. Acad Radiol 26:1495–1504
Sui H, Liu L, Li X, Zuo P, Cui J, Mo Z (2019) CT-based radiomics features analysis for predicting the risk of anterior mediastinal lesions. J of Thorac Dis 11:1809–1818
Wang H, Hu D, Yao H, Chen M, Li S, Chen H, et al. (2019) Radiomics analysis of multiparametric MRI for the preoperative evaluation of pathological grade in bladder cancer tumors. Eur Radiol 29:6182–6190
Fusco R, Sansone M, Filice S, Carone G, Amato DM, Sansone C et al (2016) Pattern recognition approaches for breast cancer DCE-MRI classification: a systematic review. J Med Biol Eng 36:449–459
Acknowledgements
This research was supported in part by grants from the National Natural Science Foundation of China (#81771804).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing financial interests exist.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. IRB approval was obtained. This article does not contain any studies with animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhang, Y., Zhu, Y., Zhang, K. et al. Invasive ductal breast cancer: preoperative predict Ki-67 index based on radiomics of ADC maps. Radiol med 125, 109–116 (2020). https://doi.org/10.1007/s11547-019-01100-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-019-01100-1