
Abstract
This study examines the association between neighborhood socioeconomic status (SES) and preterm birth among U.S. Black women. A composite variable for neighborhood SES, derived from 7 U.S. Census Bureau indicators, was assessed in relation to self-reported preterm birth (505 spontaneous and 452 medically indicated) among 6,390 women in the Black Women’s Health Study who delivered singleton births during 1995–2003. The odds ratio (OR) for preterm birth, comparing the lowest (most deprived) to the highest (least deprived) quartiles of neighborhood SES, was 0.98 (95 % CI, 0.80, 1.20) after adjustment for individual-level characteristics. Low neighborhood SES was not associated with spontaneous or medically indicated preterm birth overall or within strata of maternal age, education, or geographic region. The only significant finding was higher odds of medically indicated preterm birth associated with low neighborhood SES among unmarried women. Low neighborhood SES was not materially associated with preterm birth in this study of U.S. Black women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Preterm birth is the leading cause of neonatal mortality in the USA.1,2 Maternal predictors include intrauterine infections, having had a previous preterm birth, single marital status, and low personal socioeconomic status (SES).2,3 Black women are twice as likely as White women to deliver prematurely, even after controlling for maternal factors.3,4 Black women are also more likely than White women with the same personal SES to live in disadvantaged neighborhoods.5,6 There is growing evidence to suggest that residence in such neighborhoods may have detrimental effects on perinatal health, with possible mechanisms including decreased access to healthy foods and greater exposure to environmental or psychosocial stressors such as higher crime rates.7,8
Several studies have examined the association of neighborhood socioeconomic characteristics with preterm birth.9–19 All except one14 found statistically significant associations with at least one neighborhood-level indicator after adjustment for individual-level factors. Although many studies have assessed neighborhood characteristics as single variables,9–15 the complexities of neighborhood SES may be better captured by a summary variable comprised of multiple area-level factors.20 In four large studies based on vital statistic birth records, a summary variable of neighborhood deprivation was significantly associated with increased risk of preterm birth among women of various races/ethnicities.16–19 Although all previous studies except for a Canadian report15 included Black women, it is unclear whether the association between neighborhood deprivation and preterm birth is present for particular subgroups of Black women, such as well-educated women. It is possible that higher levels of personal educational attainment buffer adverse effects of neighborhood deprivation on birth outcomes in Black women. Identifying potential risk factors within subgroups of Black women may provide insight on why the prevalence of preterm birth for U.S. Black women is high.
We assessed whether a composite variable of seven neighborhood socioeconomic characteristics was related to self-reported preterm birth in a cohort of U.S. Black women who represented a variety of educational levels and lived in a wide variety of neighborhoods. We also evaluated associations according to subtypes of preterm birth, including spontaneous and medically indicated preterm births.
Methods
Study Population
The Black Women’s Health Study (BWHS) is a prospective cohort study established in 1995 to examine the determinants of various health outcomes among Black women in the USA.21–23 The study was approved by the Institutional Review Board of Boston University Medical Center. In 1995, 59,000 women aged 21 to 69 years enrolled by completing health questionnaires mailed to subscribers of Essence, a general magazine marketed to Black women. Other enrollees were family and friends of early participants and members of selected Black professional organizations. The vast majority, 93.6 %, of participants were Essence subscribers. Of those enrolled, 97 % had completed high school and 45 % had completed college. Most resided in California, Georgia, Illinois, Indiana, Louisiana, Maryland, Massachusetts, Michigan, New Jersey, New York, South Carolina, Virginia, and the District of Columbia. Cohort members have been followed through biennial questionnaires and the BWHS has maintained an average follow-up rate of 80 % since baseline.21,22,24 The present analysis was based on follow-up through 2003, after which we ceased asking about preterm birth due to the aging of the study population.
Source of Area-Level Data
Data from the 2000 U.S. Census at the block group level were used as proxies for neighborhood characteristics.25 Census block groups are geographic areas typically of homogeneous demographic composition and contain an average of 1,500 people.26 Block group data were linked to the 1995 addresses by a commercial firm that has been found to geocode accurately.27 We analyzed seven census variables that have been assessed in studies on neighborhood socioeconomic characteristics and preterm birth or were significantly associated with other outcomes in previous BWHS studies.28,29 These included: % adults who have completed college, % households with interest or dividends or net rental income (i.e., non-salary income), median household income, % white collar employment, % families with children headed by a single female, % adults living below the poverty line, and median housing value.
Neighborhood Socioeconomic Index
We included the seven area-level variables in a principal components analysis, a data reduction technique that empirically creates new summary variables (i.e., components).30,31 The principal components analysis retained only the first principal component. Each of the original census variables was weighted based on how strongly it was correlated (i.e., loaded) with the first principal component. The weights were summed to create a neighborhood score31 ranging from −3.42 to 4.03, where larger positive values indicated higher neighborhood SES.
Assessment of Preterm Birth
On every biennial follow-up questionnaire from 1997 to 2003, women reported whether they had given birth to a live born or stillborn infant in the previous 2 years. If yes, they reported whether their doctor said that the baby was born three or more weeks early. Mothers of preterm babies were then asked to provide the number of weeks the baby was born early in addition to the reason for the preterm birth. We classified subtypes of preterm birth as spontaneous (premature labor for no known reason or early rupture of membranes) or medically indicated (cesarean section or medical induction). Births for which it was unclear as to whether it was preterm or, if preterm, spontaneous or medically indicated were excluded.
The definition of preterm birth in the BWHS (“three or more weeks early”) differs slightly from the clinical definition (<37 weeks of gestation). In a validation study, medical records confirmed the outcome for 92 % of 25 participants who reported having a preterm birth and confirmed the stated reason for 87 % of 23 participants who truly had a preterm birth. In a separate validation study, preterm birth cases reported by women who delivered in Massachusetts were compared with birth certificates from the Massachusetts Department of Public Health birth registry. Preterm birth was confirmed for 21 of 23 (91 %) participants overall (11 of 12 reports of spontaneous preterm birth and 10 of 11 reports of medically indicated preterm birth). The proportion of preterm births in the BWHS (≤37 weeks of gestation) was similar to the proportion in national data (<37 weeks of gestation) among Black women with similar levels of education.32 In the BWHS, the proportion of preterm births was 15.3 % among women with 13–15 years of education and 13.1 % among women with 16 or more years of education, and the proportions among Black women in national data from 1998 to 2000 were 14.5 % and 12.8 %, respectively.32
Assessment of Individual-Level Factors
We used data from the baseline and follow-up questionnaires to identify maternal characteristics, including age at pregnancy (<30, 30–34, 35–39, ≥40 years), years of education in 1995 (≤12, 13–15, 16, ≥17), prepregnancy body mass index (BMI; <20, 20–24, 25–29, ≥30 kg/m2),33 marital status at pregnancy (married or living as married, divorced/separated/widowed, single), participant herself born preterm (no, yes, unsure), had a previous preterm birth (no, yes), smoked cigarettes during pregnancy (no, yes), parous (no, yes), and geographic region of residence in 1995 (Northeast, South, Midwest, West).26 Information on annual household income in US dollars (≤35,000, 35,001–50,000, 50,001–100,000, >100,000) was collected in the 2003 questionnaire cycle.
Exclusion Criteria
For the 1997, 1999, 2001, and 2003 questionnaires, a total of 8,697 singleton births were reported. We restricted our sample to the first reported pregnancy in the study period to avoid correlations arising from two or more births from the same woman, leaving 7,026 births. Of these, 587 were excluded because they had invalid addresses for geocoding (e.g., business addresses or post office boxes). Among the remaining 6,439 births, 1,006 preterm births were reported. We excluded 49 cases with preterm birth of unknown type. The final sample of 6,390 births included 5,433 term births and 957 preterm births, of which 505 were spontaneous and 452 were medically indicated.
Statistical Analysis
Principal components analysis was carried out in SAS version 9.134 to create scores for the neighborhood SES index. Odds ratios (OR) and 95 % confidence intervals (CI) for preterm birth overall, in relation to quartiles of the composite neighborhood SES score, and of individual neighborhood SES variables, were calculated using generalized estimating equation (GEE) models. We used GEE models to account for the correlation of two or more women living within the same census block group. The median number of women per block group was one (range, 1–12 women) and the average number was 1.19. GEE models were employed using an empirical variance estimator, an exchangeable working correlation structure, and the logit link function.35 We also examined these associations separately according to subtypes of preterm birth, spontaneous and medically indicated, given that they may have different etiologies.3,36
All GEE models were adjusted for maternal age, education, and the following individual-level covariates that we identified as potential confounders37: prepregnancy BMI, marital status, and participant herself born preterm. Indicator terms for covariates with missing data were added to GEE models to maximize statistical power. There were 43 missing observations for education (0.7 % of the sample), 44 for prepregnancy BMI (0.7 %), and 111 for marital status at pregnancy (1.7 %).
Since the BWHS cohort is a highly mobile population,24,29 we repeated our analyses among the subgroup of women who remained in the same type of neighborhood socioeconomically as that in 1995 (n = 4,092). We also examined whether the association between neighborhood SES and preterm birth varied across levels of maternal age, education, marital status, and geographic region. Pair-wise p values were calculated for analyses stratified by geographic region; the category with the largest sample size, the South, was used as the referent category. Wald statistics were used to test for linear trend.
Results
The first principal component explained 64 % of the variance in the set of seven census variables (Table 1). There was considerable variation in the prevalence of each census variable across the quartiles of neighborhood SES score (Table 2). For example, the average percent of adults who had completed college was 13.1 % in the lowest quartile of SES score and 54.9 % in the highest, and the average percent of the population living below the poverty level was 31.6 % in the lowest quartile and 5.7 % in the highest.
With respect to individual level characteristics, mothers who lived in lower SES neighborhoods were more likely to be younger, unmarried, and parous (Table 3). They also had higher BMI, fewer years of education, lower household incomes, and were more likely to smoke during pregnancy. Women who were born preterm themselves or had a prior preterm birth were less likely to live in higher SES neighborhoods.
In analyses for the individual variables that contributed to the neighborhood SES score (Table 4), we found no statistically significant associations or trends. For median household income, which has been the subject of several previous investigations, the OR for preterm birth overall comparing lowest quartile of median household income to the highest quartile was 1.00 (95 % CI, 0.83, 1.21) before adjustment and 0.89 (95 % CI, 0.72, 1.09) after adjustment for confounding variables.
Neighborhood SES score was not associated with preterm birth overall in unadjusted models (Table 5), with an OR of 1.09 (95 % CI, 0.90, 1.32) for the comparison of the lowest (most deprived) quartile with the highest (least deprived). After adjustment for maternal factors (age, education, marital status, BMI, and mother born preterm), the OR was 0.98. An analysis restricted to women who had lived at the same address or in the same type of neighborhood throughout follow-up gave results similar to those presented: among the 4,092 women who lived in the same type of neighborhood during the entire study period, the adjusted OR for the comparison of the lowest quartile to the highest for preterm birth overall was 0.99 (95 % CI, 0.77, 1.29). The ORs for spontaneous and medically indicated preterm births, respectively, were 1.04 and 1.16 before adjustment and 0.96 and 0.99 after adjustment.
In stratified analyses (Table 6), we observed little evidence of an association between neighborhood SES score and preterm birth within strata of geographic region (South, Northeast, Midwest, West), maternal age (<30, ≥30), or education (<16 years, ≥16 years). In a sub-analysis among 598 women with ≤12 years of education, the adjusted odds ratio comparing low neighborhood SES to high for preterm birth overall was 1.02 (95 % CI, 0.42, 2.51). In contrast, there was some evidence of effect modification by marital status on the association between neighborhood SES and medically indicated preterm birth (P interaction = 0.02) but not spontaneous preterm birth (P interaction = 0.80): among unmarried mothers, residence in low SES neighborhoods was associated with elevated odds of medically indicated preterm births (quartile 1 vs. 4; OR = 1.67, 95 % CI, 0.95, 2.92; p value for linear trend = 0.03), whereas among married mothers, odds ratios ranged from 0.81 to 0.88 and were not statistically significant.
Discussion
In the present study of U.S. Black women, we found no association between neighborhood SES and preterm birth overall. In addition, we observed no significant associations with spontaneous or medically indicated preterm birth, with one exception: unmarried mothers who lived in socioeconomically disadvantaged neighborhoods had greater odds of medically indicated—but not spontaneous—preterm birth compared with unmarried mothers who lived in high SES neighborhoods.
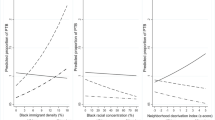
Several studies have examined the association between census-derived neighborhood SES variables and preterm birth. Null findings have been reported for percent of adults with less than a high school education,12,14 percent living below the poverty line,12,14 and percent of female headed households with children.11,13 Low median household income has been most consistently associated with increased risk of preterm birth,10,11,15 including among Black women only.11 Others have reported curvilinear associations such that increased risk of spontaneous preterm birth was associated with high and low levels of median household income among Black but not White women.9,12 Non-linear positive associations between neighborhood occupation-related variables (e.g., fraction of workers in professional occupations) and risk of spontaneous9,12 and overall preterm birth13 have been found among Black and White women. Thus, the literature suggests that some measures of neighborhood SES may be related to an increased risk of preterm birth, but the results have been inconsistent. In the present study, we found no association of preterm birth with any of the seven census variables considered, before or after adjustment for potential confounders.
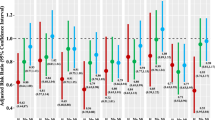
Our study included women from many regions of the USA and we found no differences in effect estimates across geographic region. Our results overall do not support the positive findings from some previous studies that assessed preterm birth in relation to neighborhood deprivation as a summary variable among African-American women in different geographic regions.16–19 O’Campo et al.16 presented a summary odds ratio of 1.15 (95 % CI, 1.08, 1.23) for Non-Hispanic Black women comparing the highest versus lowest quintile of neighborhood deprivation using data from four states. The authors also examined effect estimates for Non-Hispanic Black women across eight study areas and reported that six of the eight area-specific odds ratios, ranging from 0.88 to 1.40, were not statistically significant. The Masi study,17 conducted in Illinois, reported an odds ratio for Black women of 1.04 (p < 0.05), representing a 4 % increase in risk for a one unit increase in neighborhood economic disadvantage. The association lost significance after the addition of violent crime to one model and also after the addition of violent crime and racial group density to another model. Messer et al.18 reported a statistically significant odds ratio for Black women (OR = 1.6; 95 % CI, 1.1, 2.3) comparing the highest versus lowest quartile of neighborhood deprivation, using data from Wake County, North Carolina after adjusting for individual-level factors and measures of crime. Lastly, Janevic et al.19 presented an adjusted odds ratio for Non-Hispanic Black women of 1.12 (95 % CI, 1.02, 1.22) for preterm births at 33–36 weeks gestation in relation to living in the most deprived neighborhoods of New York City. No association was observed among Non-Hispanic Black women for preterm births at <32 weeks gestation. We conclude that the previous collective evidence does not clearly support an influence of neighborhood deprivation on preterm birth for Black women.
In disadvantaged neighborhoods, the effect of neighborhood on birth outcomes may be difficult to disentangle from the effects of individual poverty. In the present study, there were appreciable numbers of well educated women living in low SES neighborhoods. We observed no associations of neighborhood SES score with preterm birth according to level of education; specifically, risk of preterm birth was not elevated among women with lower levels of education who lived in neighborhoods with lower SES, nor was it elevated among women with high individual SES who lived in neighborhoods of low SES. However, there was a positive association between low neighborhood SES and medically indicated preterm birth among unmarried women. Effect modification by marital status, if real, supports the notion that risk of adverse health outcomes may be reduced when vulnerable individuals have social support,38 particularly from an intimate partner.39 However, we are unable to explain why this would be the case for medically indicated but not spontaneous preterm births.
Strengths of our study include the prospective design, control for a wide range of confounding factors, examination of associations in a population of Black women residing in many geographic regions of the U.S. with large heterogeneity in neighborhood SES characteristics, and examination of the association according to preterm birth subtypes. We used seven census measures of wealth, income, and education to capture the social and multidimensional concept of a neighborhood SES. While the study participants had a broad range of personal educational levels, women who had not graduated from high school were underrepresented.40 A limitation is that preterm birth was self-reported and not based on clinical assessment. However, we found good concordance between self-report of preterm birth and birth records in validation studies, and the proportion of preterm birth in the BWHS was similar to that in national data among Black women with similar levels of education.32 Random misclassification of the outcome would have tended to dilute results for the extreme categories of the exposure. The BWHS is a mobile population and misclassification of neighborhood characteristics for women who had moved since baseline could have led to distortion of associations. However, estimates from analyses confined to women whose neighborhood SES did not change during the entire study period were closely similar to those from the overall analysis.
In summary, we found no association between low neighborhood SES and preterm birth among Black women residing in various areas of the USA. Since nearly all the study participants had completed high school, we could not informatively assess associations in women with less educational attainment. If indeed such women are at increased risk of preterm birth, it will be desirable to identify specific factors associated with higher educational attainment that may potentially shield adverse effects of residing in disadvantaged neighborhoods.
References
Martin JA, Hamilton BE, Sutton PD, et al. Births: final data for 2003. Natl Vital Stat Rep. 2005; 54(2): 1–116.
Green NS, Damus K, Simpson JL, et al. Research agenda for preterm birth: recommendations from the March of Dimes. Am J Obstet Gynecol. 2005; 193(3 Pt 1): 626–635.
Berkowitz GS, Blackmore-Prince C, Lapinski RH, et al. Risk factors for preterm birth subtypes. Epidemiology. 1998; 9(3): 279–285.
Ananth CV, Misra DP, Demissie K, et al. Rates of preterm delivery among Black women and White women in the United States over two decades: an age-period-cohort analysis. Am J Epidemiol. 2001; 154(7): 657–665.
Cohen DA, Mason K, Bedimo A, et al. Neighborhood physical conditions and health. Am J Public Health. 2003; 93(3): 467–471.
Kawachi I, Berkman L. Neighborhoods and health. N.Y.: Oxford University Press; 2003.
Pickett KE, Pearl M. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: a critical review. J Epidemiol Community Health. 2001; 55(2): 111–122.
Culhane JF, Elo IT. Neighborhood context and reproductive health. Am J Obstet Gynecol. 2005; 192(5 Suppl): S22–S29.
Ahern J, Pickett KE, Selvin S, et al. Preterm birth among African American and white women: a multilevel analysis of socioeconomic characteristics and cigarette smoking. J Epidemiol Community Health. 2003; 57(8): 606–611.
Farley TA, Mason K, Rice J, et al. The relationship between the neighbourhood environment and adverse birth outcomes. Paediatr Perinat Epidemiol. 2006; 20(3): 188–200.
Kaufman JS, Dole N, Savitz DA, et al. Modeling community-level effects on preterm birth. Ann Epidemiol. 2003; 13(5): 377–384.
Pickett KE, Ahern JE, Selvin S, et al. Neighborhood socioeconomic status, maternal race and preterm delivery: a case-control study. Ann Epidemiol. 2002; 12(6): 410–418.
Reagan PB, Salsberry PJ. Race and ethnic differences in determinants of preterm birth in the USA: broadening the social context. Soc Sci Med. 2005; 60(10): 2217–2228.
Hillemeier MM, Weisman CS, Chase GA, et al. Individual and community predictors of preterm birth and low birthweight along the rural-urban continuum in central Pennsylvania. J Rural Health. 2007; 23(1): 42–48.
Luo ZC, Wilkins R, Kramer MS. Effect of neighbourhood income and maternal education on birth outcomes: a population-based study. Cmaj. 2006; 174(10): 1415–1420.
O’Campo P, Burke JG, Culhane J, et al. Neighborhood deprivation and preterm birth among non-Hispanic Black and White women in eight geographic areas in the United States. Am J Epidemiol. 2008; 167(2): 155–163.
Masi CM, Hawkley LC, Harry Piotrowski Z, et al. Neighborhood economic disadvantage, violent crime, group density, and pregnancy outcomes in a diverse, urban population. Soc Sci Med. 2007; 65(12): 2440–2457.
Messer LC, Kaufman JS, Dole N, et al. Neighborhood crime, deprivation, and preterm birth. Ann Epidemiol. 2006; 16(6): 455–462.
Janevic T, Stein CR, Savitz DA, et al. Neighborhood deprivation and adverse birth outcomes among diverse ethnic groups. Ann Epidemiol. 2010; 20(6): 445–451.
Messer LC, Laraia BA, Kaufman JS, et al. The development of a standardized neighborhood deprivation index. J Urban Health. 2006; 83(6): 1041–1062.
Rosenberg L, Palmer JR, Wise LA, et al. Perceptions of racial discrimination and the risk of preterm birth. Epidemiology. 2002; 13(6): 646–652.
Rosenberg L, Wise LA, Palmer JR. Hair-relaxer use and risk of preterm birth among African-American women. Ethn Dis. 2005; 15(4): 768–772.
Rosenberg L, Adams-Campbell L, Palmer JR. The Black Women’s Health Study: a follow-up study for causes and preventions of illness. J Am Med Womens Assoc. 1995; 50(2): 56–58.
Russell C, Palmer JR, Adams-Campbell LL, et al. Follow-up of a large cohort of Black women. Am J Epidemiol. 2001; 154(9): 845–853.
Krieger N, Williams DR, Moss NE. Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu Rev Public Health. 1997; 18: 341–378.
Census 2000 Basics. Washington, DC: US Census Bureau, 2002.
Krieger N, Waterman P, Lemieux K, et al. On the wrong side of the tracts? Evaluating the accuracy of geocoding in public health research. Am J Public Health. 2001; 91(7): 1114–1116.
Cozier YC, Palmer JR, Horton NJ, et al. Relation between neighborhood median housing value and hypertension risk among black women in the United States. Am J Public Health. 2007; 97(4): 718–724.
Rosenberg L, Wise LA, Palmer JR, et al. A multilevel study of socioeconomic predictors of regular mammography use among African-American women. Cancer Epidemiol Biomarkers Prev. 2005; 14(11 Pt 1): 2628–2633.
Floyd FJ, Widaman KF. Factor analysis in the development and refinement of clinical assessment instruments. Psychol Assessment. 1995; 7: 286–299.
Kleinbaum DG, Kupper LL, Muller KE. Applied regression and other multivariable methods. 2nd ed. Boston: PWS-Kent; 1998.
Committee on Understanding Premature Birth and Assuring Healthy Outcomes, Board on Health Sciences Policy. Preterm birth: causes, consequences, and prevention. Washington: The National Academie Press; 2007.
World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. 1995.
SAS Institute Inc. SAS/STAT User’s Guide. Cary: SAS Institute Inc; 2003.
Horton NJ, Lipsitz SR. Review of software to fit generalized estimating equestion (GEE) regression models. Am Stat. 1999; 53: 160–169.
Pickett KE, Abrams B, Selvin S. Defining preterm delivery—the epidemiology of clinical presentation. Paediatr Perinat Epidemiol. 2000; 14(4): 305–308.
Greenland S. Modeling and variable selection in epidemiologic analysis. Am J Public Health. 1989; 79(3): 340–349.
Halpern D. Minorities and mental health. Soc Sci Med. 1993; 36(5): 597–607.
Hoffman S, Hatch MC. Stress, social support and pregnancy outcome: a reassessment based on recent research. Paediatr Perinat Epidemiol. 1996; 10(4): 380–405.
Blackmore CA, Savitz DA, Edwards LJ, et al. Racial differences in the patterns of preterm delivery in central North Carolina, USA. Paediatr Perinat Epidemiol. 1995; 9(3): 281–295.
Acknowledgments
The authors are grateful to the participants and staff of the Black Women’s Health Study for their contributions.
Funding
This work was supported by National Cancer Institute grant R01 CA058420 and by Association of Schools of Public Health grant S324-16/18 given through the ASPH/CDC/ATSDR Cooperative agreement.
At the time the study was conducted, Ghasi Phillips was a doctoral student at the Harvard School of Public Health, Boston, Massachusetts.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Phillips, G.S., Wise, L.A., Rich-Edwards, J.W. et al. Neighborhood Socioeconomic Status in Relation to Preterm Birth in a U.S. Cohort of Black Women. J Urban Health 90, 197–211 (2013). https://doi.org/10.1007/s11524-012-9739-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-012-9739-x