
Abstract
Background
The aim of this study was to measure forces created by progressive mandibular advancement with an oral device, during natural sleep, in a sample of adult patients with obstructive sleep apnea syndrome (OSAS).
Methods
A pressure transducer system was placed on the acrylic arms of a two-piece oral appliance (Herbst type) used by nine moderate to severe OSAS patients, in addition to all captors routinely used for polysomnography. Strains on the left and right sides were collected, during stable sleep stages without arousal, for each step of 1 mm advancement.
Results
The mean force in this sample was 1.18 N/mm and showed an almost linear evolution. Measurements showed intra- and inter-individual variability.
Conclusion
The force values recorded in this study may explain the occlusal and skeletal side effects associated with long-term use of these oral appliances. They illustrate the influence of the extent of mandibular advancement, and indicate a possible dose-dependent effect.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea syndrome (OSAS) is characterized by the occurrence of repeated collapse of the upper airway during sleep [1]. Its symptoms generally include snoring interrupted with pauses, daytime drowsiness and the feeling of sleep not being refreshing. Repeated episodes of complete obstruction (apnea) or partial upper airway collapse (hypopnea) can cause many phases of hypoxia, followed by hyperventilation, and cortical micro-arousal.
The consequences of untreated OSA are potentially life-threatening, in part due to deleterious effects on cardiovascular morbidity and mortality (stroke) and may lead to sleep deprivation-associated driving accidents. OSAS is a public health problem, affecting 4 % of middle-aged men and 2 % of middle-aged women [2].
Continuous positive airway pressure (CPAP) is the reference treatment for OSAS; it creates a pneumatic splint which prevents the collapse of the pharyngeal walls during breathing, irrespective of the location of the obstruction [3]. Long-term observance of this treatment is good in 60–70 % of cases [4], and in combination with other conservative treatments, such as weight loss and sleep hygiene, the outcome is successful for many patients. However, the use of CPAP declines over the years, as it is perceived to be too constraining for some patients [3–6]; although weight loss effectively reduces the severity of OSAS it does not relieve all respiratory events [7]. Consequently, alternative forms of treatment are required.
Surgical treatment involves ENT examination to confirm the location and nature of the obstacle. Then, the airway can be enlarged, either by reducing the pharyngeal soft tissue content (i.e., soft palate, palatal or lingual tonsils) [8], or widening the skeletal frame, by maxillo-mandibular advancement surgery [9]. These procedures are highly effective, but invasive.
Mandibular advancement devices (MADs), which mechanically enlarge the airway, are currently widely used [10–13]. Similar to activators, which are functional devices used by orthodontists to correct class II discrepancies, MADs are anchored on teeth to force the mandible to an advanced position, pulling forward the tongue base and stretching pharyngeal soft tissues. MADs maintain patency during sleep by increasing the size and reducing the collapsibility of the airway. Experimental and clinical studies have demonstrated that the efficacy of MADs depends on the degree of mandibular advancement, with a dose-dependent effect [14–22]. Mandibular advancement correlates with the decrease in airway resistance to airflow [15, 18], an increase of airway cross-sectional area [14, 19, 21–23], and the reduction of the incidence of abnormal respiratory events [15, 16, 18]. Kato et al. [15] reported that mandibular advancement in paralyzed OSAS patients, under general anesthesia, produced a dose-dependent reduction of closing pressure in all pharyngeal segments: each 2-mm mandibular advancement step coincided with an approximately 20 % reduction in the number and severity of nocturnal desaturations.
MADs must therefore be titrated, and the degree of effective mandibular advancement (EMA) should be determined not simply on subjective clinical criteria, but also on objective data [1]. Nocturnal oximetry can help the clinician assess whether further advancement is required [23], but a full polymonography is necessary at the end of the process, to determine the final apnea–hypopnea index per hour (AHI). A previous study with a Herbst-type MAD, involving a hydraulic system to drive advancement, has shown that the appropriate value can be obtained during a single night polysomnography [18], as the authors could validate the recorded advancement value by a second night recording.
Long-term MAD treatment can lead to irreversible alterations of the occlusion [24–32], with significant reduction of incisor overbite and overjet, or an increase of posterior open-bite. A dose-dependent effect of mandibular advancement on occlusal changes has been suggested, but has not been demonstrated. According to Marklund et al. [26], the risk of dento-alveolar movements with a soft elastomeric MAD is lower for protrusions of 6 mm or less. However, in the same study, the authors could not find the same relationship for hard acrylic MADs. Few studies have measured the strain developed by MADs, whether in children as an orthopedic treatment, or in adults for OSAS [33–37].
The aim of this study was to measure the forces acting on a MAD used by adult apneic patients during natural sleep, for each step of 1 mm advancement. Our secondary objective was to evaluate, during titration, the mean force values created when reaching the EMA.
Materials and methods
Patients
The study population was composed of nine consecutive middle-aged OSAS patients (characteristics shown in Table 1): seven men, two women, aged from 30 to 58 years, body mass index (BMI) from 22 to 28 kg/m2. OSAS was confirmed by an all-night diagnostic sleep study: AHI values were in the range 10–31 per hour. All patients were intolerant of nasal continuous positive airway pressure (nCPAP).
The patients were informed of the various therapeutic options, and then invited to participate freely in this prospective pilot study. Written informed consent was obtained from all patients. The investigation was approved by the local ethics committee. Patients with inadequate dental structures for anchoring of the MAD, temporo-mandibular joint dysfunction and/or previous uvulo-palato-pharyngoplasty were excluded. None of the patients had used a MAD previously.
Sleep study
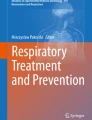
Measurements included sleep stage (electroencephalogram, electro-oculogram, and submental electromyogram), thoracic and abdominal movements, respiratory inductance (plethysmography), and arterial oxygen saturation (SaO2). Given the size of the MAD, which for some patients led to mouth opening, a face mask covering the nose and mouth was used to measure ventilatory flow (see Fig. 1). All polysomnographic data were analyzed visually by a sleep specialist. Sleep staging was performed according to standard criteria [38]. Apnea was defined as cessation of the airflow of more than 10 s. Hypopnea was defined as a reduction of the airflow, for at least 10 s, of 50 % from baseline, or a reduction of airflow that was less than 50 % but associated with a fall of SaO2 greater than 3 % [39].

Facial mask used to measure breathing variables and allowing mandibular forces on the oral appliance to be recorded
Mandibular advancement device
Alginate impressions of the upper and lower teeth were taken, the centric occlusion was recorded, and full coverage rigid acrylic splints were obtained. Maxillary and mandibular splints were connected by two lateral acrylic arms, fixed to the upper second molars and lower canines. Connectors allowed slight rotation movements (Fig. 2a); a metallic wire system, abutted to the upper acrylic arms, allowed the lower splint to be advanced relative to the upper splint. The metallic wires were sheathed with a plastic tube, and could slide within the lateral acrylic arms (see Fig. 2b and c).

a Oral appliance used in this study. b Mandibular advancement device with modified acrylic arms, metallic extensions and syringe. c Close-up view of the mandibular advancement device (modified acrylic arm)
During the experiment, the metallic wires imposed mandibular advancement mechanically, driven by a syringe pump (electric anesthetic syringe, pilot C, Fresenius Vial) connected to a computer outside the patient's room. Pressure data was displayed on the same screen as the polysomnographic readings.
Patients were able to accommodate to the appliance a couple of hours prior to undertaking the study.
Force sensors (clinical study)
The force sensors, chosen for their small size (6 mm diameter, 0.2 mm thickness; Fig. 3a and b), were used to measure static and dynamic compression forces, up to 5,000 N (Model XFL225D; FGP Sensors and Instrumentation, France). The test body was made of stainless steel and the sensitive element equipped with micro silicon gauges; it had a central hole in through which the wire of the MAD was received. Sensors, similar to electric resistors, were isolated by shielded cables, compatible with intra-oral use (4 Teflon conductors, standard length 2 m; 10-V dc voltage supply, input impedance of 1,000–3,000 ohms, output impedance of 500–1,000 ohms). The value of the electrical resistance decreased as the force level increased; its variation was analyzed after signal processing by a computer (calibration by Cidelec laboratory).

a Positions of the force sensors on the oral appliance, metallic wires and mobile portion of the acrylic arms of the oral appliance. 1 Upper acrylic splint, 2 lateral connector, 3 lower acrylic splint, 4 metallic wire gained into plastic, 5 pressure sensor, 6 electric wire connected to sensor and computer, 7 segment related to the electric syringe. b Sensor used in this study
Validation and system calibration (laboratory test)
The friction forces applied by the wire/plastic tube interface and deformations associated with elasticity of the system were measured in the laboratory. The friction coefficient was defined as k=|F 1−F 2|/F 1. F 1 was the force at the syringe and F 2 is the force at the acrylic arms. Various forces were tested by a system of pulleys and weights, standardized for both forward and setback movement of the splint. The tests were performed initially with cables held in a straight position, and subsequently with cables in a relaxed position.
Titration of the MAD with force sensors
Mandibular advancement, by increments of 1 mm every 15 min, was started after the first episode of rapid eye movement (REM), such that one complete sleep cycle could be recorded before titration. Progressive advancement was continued during sleep until abnormal breathing events were significantly less severe or frequent than at baseline, or until the maximum position of the system was reached, pain was caused, or the patient woken.
For each millimeter of advancement, forces on the mandibular left and right sides were collected for 5 min, during phases of stable light sleep (N2) without arousal; these readings were used to calculate rigidity values. Rigidity was defined as the force required to obtain a displacement of 1 mm (Newtons per millimeter). Changes on the force sensors during micro-arousals were recorded as they occurred. When possible, the whole titration process was repeated during the night.
Results
Calibration of the system (Table 2) showed that the friction (k) within the plastic tubes varied with the magnitude of the force developed (see Table 3); k during mandibular advancement was estimated to be 0.25 for force values of 10 N or less, and up to 0.52 for forces up to 20 N. The influence of wire curvature was not significant (data not shown).
EMA was defined as the value in millimeters from which there were no abnormal respiratory events. In our sample, the mean EMA value was 11.4 mm (± 2.4), with a range from 8 to 14 mm. EMA could not be determined for all patients: one patient (patient number 3) displayed abnormal ventilatory events after 13 mm of mandibular advancement and was classified as “partial responder” to MAD therapy.
Maximal recorded force values at the syringe were 33.4 (±13.7) N and 26.2 (±6.7) N at the MAD. The force required to reach the EMA was 11.3 (±2.9) N on the left side and 14.7 (±4.6) N on the right side, giving a total value of 26.2 (±6.7) N. The mean force value for each 1 ml advancement step (or rigidity index) was 2.3 (±0.3) N/mm, with extremes of 1.92 and 3.35 N/mm.
The theoretical step displacement of the lower splint in relation to the upper splint in this experiment was 1 mm, corresponding to the mechanically symmetrical advancement driven by the syringe pump. However, friction between the plastic tube and the metallic wire is expected to result in the true advancement of the appliance being slightly lower, and the forces involved higher. Due to friction the effective forces were probably 25 % lower than those applied for values between 0 and 10 N and 52 % for those between 10 and 20 N. Therefore, the overall forces actually developed to reach EMA (11.4 ±2.4 mm) were close to 13.6 N (i.e., 1,387.4 gF). As the forces applied exceeded 10 N, the rigidity coefficients need to be corrected to a theoretical value of 1.18 N/mm (120.6 gf/mm).
The curves of the rigidity index plotted against force applied suggested a linear system with constant coefficient (correlation coefficient (r) = 0.92; Fig. 4). Inter-individual differences were especially marked in the first few millimeters of advancement.

Evolution of forces recorded during progressive mandibular advancement
The titration process could be repeated through the night for four of the nine patients, allowing intra-individual variability measures (see Table 4).
The forces measured on the right and left sides differed for all patients, for all measures of mandibular advancement (Fig. 5): this difference was moderate in patient numbers 1, 2 and 5 (≈1–2 N), but was about 5–10 N in patients numbers 3 and 4. Cortical micro-arousals were coincided with a significant but transient increase in forces recorded on the sensors (shown in Fig. 6). These additional forces were not taken into account to calculate the average forces.

Left–right asymmetry of forces recorded during progressive mandibular advancement

Effects of micro-arousal on the forces recorded in one patient
Discussion
Recorded force
Several studies of the forces values created by mandibular advancement devices have been published. Graber and Neumann [36] reported forces of 500 gF for 5-mm advancement, and 1,000 gF for 10-mm advancement, very similar to our results after correction for friction. Katsavrias and Halazonetis [35] studied the antero-posterior intermaxillary forces developed by an activator (modified Harvold type) and reported a median value of 100 gF measured while standing, and of 123 gF when lying down (n = 10 adolescents). Higher values were reported by Witt and Komposh [34], with forces ranging from 315 to 395 gF (n = 30 adolescents).
Noro et al. [33] studied 30 teenagers and sought to evaluate the nature of the forces applied by activators of various heights (from 2 to 8 mm) adapted to the initial skeletal discrepancy. Subjects were evaluated by electromyography, electroencephalography and pressure transducers, during 2 h of sleep. The magnitude of forces generated by the passive tension of soft tissues was significantly increased, to values of between 80 and 160 gF in the Class II group and between 200 and 230 gF in the Class III group. Changing the height of the activators significantly changed the direction of the forces. Qualitatively, the forces generated by passive tension were significantly greater and lasted longer than the active contraction of the elevator muscles, regardless of the construction height. The authors concluded that the forces generated by passive tension were a consequence of the viscoelasticity of soft tissues playing a larger role than the reflex phasic contraction of the elevator muscles.
The force values found in our study were slightly higher than those reported in some previous studies. There are several possible explanations. Our sample was composed of adult patients, whereas all other studies have been conducted on adolescents. Also, the mandibular advancement in our patients was substantial, up to 14 mm, whereas the activators used in previous studies were mostly limited to an edge to edge position.
Clinical implications: occlusal side effects
In this study, measures were made perpendicular to the axis of the acrylic arms, describing a force vector in the antero-posterior direction (compressive forces on the distal part of the maxilla) and a vertical component vector (compressive forces of intrusion on the distal part of the maxilla), which was limited due to the reduced thickness of the acrylic splints. Newton's third law, or law of mechanical equilibrium, states that there must be reaction forces, of equal intensity and opposite direction. The lower arch is therefore subject to compression forces in the mesial direction, and intrusion forces in the anterior portion of the arch. The whole system is thus subjected to a moment of rotation.
Dental movement can be induced by light forces, and several experimental studies in humans report optimal force magnitudes of 0.9–2.5 N [40–44]. Even applied only intermittently, during night wear, forces of these magnitudes lead to dento-alveolar movements [45].
Various occlusal changes associated with MADs have been described: Fransson et al. [46] noted a reduction of the overjet and overbite, and Robertson et al. [29] described skeletal variations on cephalograms, in both studies after wearing a MAD for 6 months. Almeida et al. [31, 32] studied the long-term consequences of wearing a MAD: they used cast models and cephalograms to describe precisely dento-alveolar movements after 7.4 ± 2.2 years [31, 32], and there was occlusal stability in only 14.3 % of the patients. Many studies report a small but statistically significant increase in anterior facial height, lowering of the mandible in relation to the skull base, and extrusion of mandibular molars [27–29, 33]. Progressive reduction of overjet and overbite, after long-term use of a MAD, has been attributed to palatal tipping of the maxillary incisors and labial inclination of lower incisors [26–33]. These MAD-induced dental movements are unsurprising given the orientation of force vectors; some might be beneficial for some patients (41.4 % according to Almeida et al. [31, 32]) and be deleterious for others (44.3 %) according to the patient’s characteristics before the start of treatment.
The relationship between recorded force and mandibular advancement is almost linear; the force gradually increased with mandibular advancement. As the forces applied to attain the large EMA values required were substantial, they may cause potentially irreversible changes of occlusion. Other factors, such as appliance design, composition, extent of bite opening and patient compliance also contribute to any such effects [26, 30, 33, 47]. Smaller EMA may lessen the risk of dento-alveolar movements, as suggested by Marklund for protrusion of 6 mm or less with soft elastomeric devices [26].
An adapted follow-up schedule could be planned for patients with known risk factors, such as reduced periodontal support, when high EMA are needed to treat OSAS. If there are severe dental side effects, combined CPAP/MAD, used alternately, may be an option for treating potentially life-threatening OSAS [48].
Force variability
Inter-individual variability
The forces recorded showed some variability between subjects.
This may reflect anatomical differences between subjects: these forces are essentially viscoelastic (i.e., passive stretching of the muscles and ligaments attached to maxilla, mandible and hyoid bones), and may be influenced by several factors, including patient sex, age or facial pattern.
The intra-individual variability of the forces tended to be lower after than before the seventh millimeter of advancement (not statistically significant). Seven millimeter of advancement corresponds approximately to the range of functional movements, and could reflect a particular behavior of soft tissues, involving increased resistance beyond a given stretching value. The small sample of our study does not allow further analysis of this issue.
The longitudinal study by Katsavrias and Halazonetis [35] about activator treatment similarly reported substantial variability of the forces observed, both between patients and for the same patient at different times, while awake. The authors explained this intra-individual variability as a consequence of transient increases in muscular force during swallowing, during involuntary muscle contractions, or more generally an increase in muscle tone in relation to the psychological mood of the subject. The authors did not use specific sensors to monitor muscle activity in parallel [35].
A larger study would be required to isolate and compare different subpopulations. In particular, the possible influence of the facial type should be studied, given the functional differences described by some authors. For instance, subjects with short faces (brachyfacial type) show higher occlusal forces [49] and higher muscular activity values [50] compared with dolichofacial subjects, and may display more resistance to mandibular advancement. With a larger sample, the effects of differences in scale (or size) between subjects could also be investigated (allometry).
Influence of micro-arousal
We observed a symmetrical increase in recorded force during cortical arousals. A physiological rhythmic contraction of the elevator muscles has been described during sleep [51], and is exacerbated in sleep bruxism in association with micro-arousal [52]. These strains are presumably superimposed on the strains generated by the MAD and explain the occurrence of pain and increased tooth movements in some patients. Amoric [37] used an electro-dynamometer on Herbst appliances, and described a large difference in the recorded forces between when the mandible was kept loose (200 gF), and when the patient actively kept his teeth in contact (600 gF). It has also been shown that maximal bite force is significantly higher in subjects with bruxism than controls [53]. Future studies should screen for bruxism and study it consequences in detail, as it is a potentially important and relevant variable.
Asymmetry
A difference was found between forces recorded on the right and left sides. This may reveal asymmetry in the elasticity of structures stretched by the MAD (viscoelasticity) or asymmetry of muscle contraction during sleep.
Asymmetrical tooth movements after long-term wear of a MAD have been reported by Almeida et al. in 2006 [32]. They described a possible asymmetrical "vector" of forces, directed mesially and to the right on the mandibular arch. This putative asymmetry of forces had been attributed to the existence of a preferential side during function (e.g., swallowing, speech, or bruxism), or to a kinetic asymmetry. The authors were careful to check the symmetry of movement in the mandibular condyle when the MAD was worn. In our sample, we did not detect significant functional or occlusal asymmetry.
Other studies describe asymmetry in the interdental forces [54] or occlusal forces [55], with a predominance of functional forces on the right side. These findings are in agreement with the suggestion by Almeida et al. [32], of right-side dominance, that could be associated with hemispheric lateralization.
Conclusion
The settings of MADs have implications for the efficacy of OSAS treatment, and also for the severity of side effects. We report a regular dose-dependent increase of force values with increasing mandibular advancement, reaching 1.18 N per millimeter of advancement (i.e., 120, 6 gF/mm). The EMA to treat OSAS was 11.4 (±2.4) mm in this sample, corresponding to forces of 13.6 N (i.e., 1,387.36 gF).
Prospective studies are required to evaluate the link between these forces, MAD design, and both patient compliance and resistance to dental movement (baseline occlusal features and periodontal anchorage, dental implants). Given the magnitude of the forces involved, a customized follow-up protocol may be appropriate for patients needing high EMA values.
References
American Sleep Disorders Association (1995) Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances. Sleep 18:511–513
Young T, Peppard PE, Gottieb DJ (2002) Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med 165:1217–1239
Giles TL, Lasserson TJ, Smith BH, White J, Wright J, Cates CJ (2006) Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev 19(3):CD001106
Engleman HM, Martin SE, Douglas NJ (1994) Compliance with CPAP therapy in patients with the sleep apnoea/hypopnoea syndrome. Thorax 49(3):263–266
Weaver TE, Grunstein RR (2008) Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc 5:173–178
Haniffa M, Lasserson TJ, Smith I (2004) Interventions to improve compliance with continuous positive airway pressure for obstructive sleep apnoea. Cochrane Database Syst Rev 18(4):CD003531
Anandam A, Akinnusi M, Kufel T, Porhomayon J, El-Solh AA (2012) Effects of dietary weight loss on obstructive sleep apnea: a meta-analysis. Sleep Breath Feb 29. doi:10.1111/j.1747-0285.2012.01402.x
Sundaram S, Bridgman SA, Lim J, Lasserson TJ (2005) Surgery for obstructive sleep apnoea. Cochrane Database Syst Rev 19(4):CD001004
Pirklbauer K, Russmueller G, Stiebellehner L, Nell C, Sinko K, Millesi G, Klug C (2011) Maxillomandibular advancement for treatment of obstructive sleep apnea syndrome: a systematic review. J Oral Maxillofac Surg 69(6):165–176
Gagnadoux F, Fleury B, Vielle B, Pételle B, Meslier N, N'Guyen XL, Trzepizur W, Racineux JL (2009) Titrated mandibular advancement versus positive airway pressure for sleep apnoea. Eur Respir J 34(4):914–920
Mehta A, Qian J, Petocz P, Darendeliler MA, Cistulli PA (2001) A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Crit Care Med 163:1457–1461
Marklund M, Stenlund H, Franklin KA (2004) Mandibular advancement devices in 630 men and women with obstructive sleep apnea and snoring: tolerability and predictors of treatment success. Chest 125(4):1270–1278
Lowe AA, Sjöholm TT, Ryan CF, Fleetham JA, Ferguson KA, Remmers JE (2000) Treatment, airway and compliance effects of a titrable oral appliance. Sleep 23:S172–S178
Ryan CF, Love LL, Peat D, Fleetham JA, Lowe AA (1999) Mandibular advancement oral appliance therapy for obstructive sleep apnoea: effect on awake calibre of the velopharynx. Thorax 54:972–977
Kato J, Isono S, Tanaka A, Watanabe T, Araki D, Tanzawa H, Nishino T (2000) Dose-dependent effects on pharyngeal mechanics and nocturnal oxygenation in patients with sleep-disordered breathing. Chest 117:1065–1072
Walker-Engstrom ML, Ringqvist I, Vestling O, Wilhelmsson B, Tegelberg A (2003) A prospective randomized study comparing two different degrees of mandibular advancement with a dental appliance in treatment of severe obstructive sleep apnea. Sleep Breath 7(3):119–130
Aarab G, Lobbezoo F, Hamburger HL, Naeije M (2010) Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig 14(3):339–345
Pételle B, Vincent G, Gagnadoux F, Rakotonanahary D, Meyer B, Fleury B (2002) One-night mandibular advancement titration for obstructive sleep apnea syndrome: a pilot study. Am J Respir Crit Care Med 165(8):1150–1153
Tsuiki S, Hiyama S, Ono T, Imamura N, Ishiwata Y, Kuroda T et al (2001) Effects of a titratable oral appliance on supine airway size. Sleep 24:554–560
Kyung SH, Park YC, Pae EK (2005) Obstructive sleep apnea patients with the oral appliance experience pharyngeal size and shape changes in three dimensions. Angle Orthod 75:15–22
Zao, Liu, Gao (2008) Three-dimensional upper-airway changes associated with various amounts of mandibular advancement in awake apnea patients. Am J Orthod Dentofac Orthop 133:661–668
Choi JK, Hur YK, Lee JM, Clark GT (2010) Effects of mandibular advancement on upper airway dimension and collapsibility in patients with obstructive sleep apnea using dynamic upper airway imaging during sleep. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109(5):712–719
Fleury B, Rakotonanahary D, Petelle B, Vincent G, Pelletier Fleury N, Meyer B, Lebeau B (2004) Mandibular advancement titration for obstructive sleep apnea: optimization of the procedure by combining clinical and oximetric parameters. Chest 125(5):1761–1767
Fleury B, Nguyen XL, Rakotonanahary D, Cohen-Levy J, Pételle B (2009) The set-up of obstructive sleep apnea treatment. Rev Pneumol Clin 65(4):214–218
Fritsch KM, Iseli A, Russi EW, Bloch KE (2001) Side effects of mandibular advancement devices for sleep apnea treatment. Am J Respir Crit Care Med 164(5):813–818
Marklund M, Franklin KA, Persson M (2001) Orthodontic side-effects of mandibular advancement devices during treatment of snoring and sleep apnoea. Eur J Orthod 23(2):135–144
Robertson CJ (2001) Dental and skeletal changes associated with long-term mandibular advancement. Sleep 24(5):531–537
Rose EC, Staats R, Virchow C Jr, Jonas IE (2002) Occlusal and skeletal effects of an oral appliance in the treatment of obstructive sleep apnea. Chest 122(3):871–877
Robertson C, Herbison P, Harkness M (2003) Dental and occlusal changes during mandibular advancement splint therapy in sleep disordered patients. Eur J Orthod 25(4):371–376
Battagel JM, Kotecha B (2005) Dental side-effects of mandibular advancement splint wear in patients who snore. Clin Otolaryngol 30(2):149–156
Almeida FR, Lowe AA, Sung JO, Tsuiki S, Otsuka R (2006) Long-term sequellae of oral appliance therapy in obstructive sleep apnea patients: part 1. Cephalometric analysis. Am J Orthod Dentofac Orthop 129(2):195–204
Almeida FR, Lowe AA, Otsuka R, Fastlicht S, Farbood M, Tsuiki S (2006) Long-term sequellae of oral appliance therapy in obstructive sleep apnea patients: part 2. Study-model analysis. Am J Orthod Dentofac Orthop 129(2):205–213
Noro T, Tanne K, Sakuda M (1994) Orthodontic forces exerted by activators with varying construction bite heights. Am J Orthod Dentofac Orthop 2:169–179
Witt E, Komposch G (1971) Intermaxilläre Kraftwirkung bimaxillärer Geräte. Fortschr Kieferorthop 32:345–352
Katsavrias EG, Halazonetis DJ (1999) Intermaxillary forces during activator treatment. Am J Orthod Dentofac Orthop 115(2):133–137
Graber TM, Neumann (1985) Functional appliances. In: Graber TM, Swain BF (eds) Orthodontics, current principles and techniques. C.V. Mosby, St. Louis, pp 369–404
Amoric M (2008) Bielles de Herbst décolettées, intérêt et limites. Rev Orthop Dento Faciale 42:27–34
Reschaffen A, Kales AA (1968) A manual of standardized terminology: techniques and scoring system for sleep stages of human subjects. Brain Information Service/Brain Research Institute, Los Angeles, p 204
Dauvilliers Y, Arnulf I, d’Ortho MP, Coste A, Ducluzeau P, Grillet Y, Jondeau G, Kessler R, Moncely L, Philip P, Philippe C, Weitzenblum E, Pepin JL (2010) Quelle evaluation préthérapeutique d’un patient avec SAHOS nouvellement diagnostiqué? Rev Mal Respir 27(3):124–136
Reitan K (1967) Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am J Orthod 53(10):721–745
Tuncer BB, Ozmeriç N, Tuncer C, Teoman I, Cakilci B, Yücel A, Alpar R, Baloş K (2005) Levels of interleukin-8 during tooth movement. Angle Orthod 75(4):631–636
Perinetti G, Serra E, Paolantonio M, Bruè C, Meo SD, Filippi MR, Festa F, Spoto G (2005) Lactate dehydrogenase activity in human gingival crevicular fluid during orthodontic treatment: a controlled, short-term longitudinal study. J Periodontol 76(3):411–417
Batra P, Kharbanda O, Duggal R, Singh N, Parkash H (2006) Alkaline phosphatase activity in gingival crevicular fluid during canine retraction. Orthod Craniofac Res 9(1):44–51
Sugiyama Y, Yamaguchi M, Kanekawa M, Yoshii M, Nozoe T, Nogimura A, Kasai K (2003) The level of cathepsin B in gingival crevicular fluid during human orthodontic tooth movement. Eur J Orthod 25(1):71–76
Gibson JM, King GJ, Keeling SD (1992) Long-term orthodontic tooth movement response to short-term force in the rat. Angle Orthod 62(3):211–215
Fransson AM, Tegelberg A, Leissner L, Wenneberg B, Isacsson G (2003) Effects of a mandibular protruding device on the sleep of patients with obstructive sleep apnea and snoring problems: a 2-year follow-up. Sleep Breath 7(3):131–141
Hoffstein V (2007) Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath 11(1):1–22
El-Solh AA, Moitheennazima B, Akinnusi ME, Churder PM, Lafornara AM (2011) Combined oral appliance and positive airway pressure therapy for obstructive sleep apnea: a pilot study. Sleep Breath 15(2):203–208
Gomes SG, Custodio W, Jufer JS, Del Bel CA, Garcia RC (2010) Mastication, EMG activity and occlusal contact area in subjects with different facial types. Cranio 28(4):274–279
Custodio W, Gomes SG, Faot F, Garcia RC, Del Bel Cury AA (2011) Occlusal force, electromyographic activity of masticatory muscles and mandibular flexure of subjects with different facial types. J Appl Oral Sci 19(4):343–349
Farella M, Palla S, Gallo LM (2009) Time frequency analysis of rhythmic masticatory muscle activity. Muscle Nerve 39(6):828–836
Dutra KM, Pereira FJ Jr, Rompré PH, Huynh N, Flemming N, Lavigne GJ (2009) Oro-facial activities in sleep bruxism patients and in normal subjects: a controlled polygraphic and audio–video study. J Oral Rehab 36(2):86–92
Dıraçoğlu D, Alptekin K, Cifter ED, Güçlü B, Karan A, Aksoy C (2011) Relationship between maximal bite force and tooth wear in bruxist and non-bruxist individuals. Arch Oral Biol 56(12):1569–1575
Jonke E (2011) Left/right asymmetries and open/closed differences of interdental forces in the mandible. Eur J Orthod 33(6):642–646
Cohen-Levy J, Cohen N (2011) Computerized analysis of occlusal contacts after lingual orthodontic treatment in adults. Int Orthod 9(4):410–431
Acknowledgements
We thank Prof. Robert Garcia for his advice. We also thank Prof. Alain Lautrou for his critical comments on the manuscript and his expertise in functional therapy. Special thanks to Prof. Claude Lévy and Dr Max Ganem for their kind assistance with translation. This study was supported by grants from the Programme Hospitalier de Recherche Clinique (Angers, France), ANTADIR and the Etablissement Public, Chancellerie de Paris (both Paris, France).
Conflict of interest
Dr. Boris Pételle and Dr. Bernard Fleury are consultants for Orthosom, a society selling oral appliances in France. All others authors declare no conflict of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cohen-Levy, J., Pételle, B., Pinguet, J. et al. Forces created by mandibular advancement devices in OSAS patients. Sleep Breath 17, 781–789 (2013). https://doi.org/10.1007/s11325-012-0765-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-012-0765-4