
Abstract
Purpose
Uremic toxins produced by gut microbiota (indoxyl sulfate—IS, p-cresyl sulfate—p-CS, and indole-3-acetic acid—IAA) accumulate in hemodialysis (HD) patients and exhibit potent inflammatory effects. However, the impact of these toxins on nuclear E2-related factor 2 (Nrf2) and nuclear factor-kappa B (NF-κB) expression in HD patients remains poorly defined. The aim of this study was to evaluate the association between uremic toxins and Nrf2/NF-κB expression in vitro (RAW 264.7 macrophage-like cells) and in peripheral blood mononuclear cells from HD patients.
Methods
Uremic toxins, C-reactive protein (CRP), interleukin-6 (IL-6) and malondialdehyde (MDA) levels were measured in fifteen HD patients and nine healthy individuals. RAW 264.7 macrophage-like cells were incubated with IS, as a prototype of protein-bound uremic toxin. Nrf2 and NF-κB expressions were analyzed by RT-qPCR.
Results
HD patients presented high levels of inflammatory markers, MDA and uremic toxins. In addition, they presented high NF-κB and low Nrf2 expression. Uremic toxins were positively correlated with NF-κB expression (IS, ρ = 0.58, p < 0.003; p-CS, ρ = 0.71, p < 0.001; IAA, ρ = 0.62, p < 0.001) and negatively with Nrf2 (IS, ρ = − 0.48, p = 0.01; p-CS, ρ = − 0.46, p < 0.02). Uremic toxins also exhibited positive correlations with CRP and MDA levels. Multivariate analysis revealed that p-CS is a determinant factor of NF-κB expression. In RAW 264.7 culture, NF-κB mRNA expression was stimulated by IS, while Nrf2 was downregulated.
Conclusions
Thus, uremic toxins may stimulate NF-κB mRNA and decrease Nrf2 expression in HD patients and, consequently, trigger inflammation and oxidative stress.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Studies in chronic kidney disease (CKD) patients have identified an imbalance of the gut microbiota (the so-called dysbiosis) as a new factor that may contribute to cardiovascular disease (CVD) [1, 2]. Some uremic toxins produced by the altered gut such as indoxyl sulfate (IS), p-cresyl sulfate (p-CS) and indole-3-acetic acid (IAA) are accumulated in CKD patients and can lead to pathological conditions such as inflammation and oxidative stress which explain in part the risk of CVD in these patients [3, 4].
IS is an organic anion metabolized in the liver from indole, produced by the intestinal bacteria as a metabolite of tryptophan derived from dietary proteins [5]. This toxin is known to exert a wide range of toxic activities such as endothelial dysfunction and is independently associated with cardiovascular disease in CKD patients. Besides, IS exacerbates reactive oxygen species (ROS) production by NADPH oxidase activation and is related to inflammation in these patients [4, 6, 7].
Another uremic toxin formed by gut microbiota is p-CS, resulting from fermentation of tyrosine to p-cresol and endogenous sulfate conjugation [8, 9]. This toxin may also play a role in the development of endothelial dysfunction and vascular stiffness [10, 11]. Furthermore, p-CS appears to be strongly associated with progression of CKD and survival [11, 12]. This toxin also leads to increased ROS production, activates NADPH oxidase and induces an increase in inflammatory cytokines levels [12].
IAA is an end-product of tryptophan bacterial fermentation metabolized in the gut or in tissue from indole [5]. IAA is positively correlated with C-reactive protein (CRP) and malondialdehyde (MDA), which are commonly used to evaluate inflammation and oxidative stress, and consequently, IAA is considered a predictor of cardiovascular disease and mortality in CKD patients [13].
Although knowledge has increased about mechanisms involved in the interaction between gut microbiota and CKD, very few information exists about microbiota and its relationship with inflammation and oxidative stress in CKD patients. Bolati et al. [14] observed that HK-2 cells treated with IS presented a downregulation of nuclear E2-related factor 2 (Nrf2) through activation of nuclear factor-kappa B (NF-κB).
Nrf2–Kelch–like ECH-associating protein-1 (Keap1) pathway is known as a major transcription factor that stimulates cellular defense mechanism, such active expression of genes encoding phase II detoxifying enzymes and antioxidant enzymes. Nrf2 plays crucial roles in cellular defense, improving the removal of ROS and regulating cellular antioxidant responses by modulation of NF-κB [15].
NF-κB downstream regulates gene transcription, including those associated with inflammation such as pro-inflammatory cytokines and leukocyte adhesion molecules (E-selectin, VCAM-1 and ICAM-1) [15]. In our previous study [16], we have observed an increased NF-κB and reduced Nrf2 expression in HD patients; however, there are currently no available data regarding the relationship between protein-bound uremic toxins and expression of Nrf2-Keap1 and NF-κB in hemodialysis (HD) patients. Thus, the aim of this study was to evaluate the association between uremic toxins and Nrf2 and NF-κB expression in peripheral blood mononuclear cells (PBMC) isolated from HD patients as well as in vitro (RAW 264.7 macrophage-like cells).
Subjects and methods
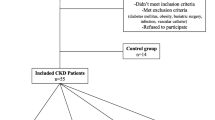
Fifteen HD patients were enrolled in this study (nine men and six women, mean age 61 ± 13 years old, average time on dialysis 98 ± 50 months, BMI, 24.1 ± 3.1 kg/m2). Data and blood samples from nine healthy individuals recruited into the observational study previously described [16] were analyzed for uremic toxins levels.
Inclusion criteria were age higher than 18 years and HD treatment for at least 6 months. Patients with active inflammatory diseases, cancer, AIDS, autoimmune disease, smokers, patients using catheter access for HD, and patients on antioxidant vitamin supplements or use of antibiotic, pre-, pro- or symbiotic were excluded. Dialysis duration was 3–4.5 h per session three times a week. Blood flow was greater than 250 mL/min, and dialysate flow was 500 mL/min.
The etiologies of renal disease were hypertensive (10 of 15), diabetic nephropathy (2 of 15), chronic glomerulonephritis (2 of 15) and polycystic kidney disease (1 of 15). The study protocol was reviewed and approved by the Ethics Committee of the School of Medicine—Federal University Fluminense (018/09), and all patients were asked to sign an informed consent.
Analytic procedures and sample processing
Blood samples were drawn from each subject in the morning, after an overnight fasting, into a syringe containing ethylene diamine tetra acetic acid (EDTA) (1.0 mg/mL) as anticoagulant. Plasma was separated (15 min, 3000×g, 4 °C) and stored in − 80 °C until analysis.
To isolate the peripheral blood mononuclear cells (PBMC), blood samples with EDTA were diluted in PBS, and cells were detached with Histopaque (Sigma-Aldrich®, Darmstadt, Germany) by centrifugation at 1800 rpm for 30 min at 18 °C. PBMCs were collected and washed twice with cold phosphate-buffered saline (PBS) and stored with 1 mL of Gibco™ Recovery™ Cell Culture Freezing Medium (Thermo Fisher Scientific Inc, Grand Island, New York) for RNA isolation.
Biochemical, oxidative stress and inflammation parameters
Serum urea nitrogen, phosphorus, potassium, calcium, albumin, creatinine, parathormone (PTH), blood hemoglobin, hematocrit levels and BMI were collected from medical records of patients. Dialysis dose (Kt/V) was calculated using values of blood urea nitrogen, pre- and post-dialysis, body weight and dialysis duration using a standard formula [17].
C-reactive protein (CRP) and interleukin-6 (IL-6) plasma levels were measured by ELISA, using R&D systems duoset kits (Minneapolis, MN, USA). Malondialdehyde (MDA) plasma levels were measured by reaction with thiobarbituric acid. Samples were diluted with thiobarbituric acid (0.6% m/v), brought to heating to 95 degrees, and the floating liquid was detached and read spectrophotometrically at 532 nm.
Real-time quantitative PCR analysis
Nrf2 and NF-κB mRNA levels were analyzed in PBMCs using quantitative real-time polymerase chain reaction (qRT-PCR). PBMCs were isolated from blood, and RNA was extracted with SV Total RNA Isolation System (PROMEGA). The cDNA was synthesized with the high-capacity cDNA reverse transcription kit (Applied Biosystems). Real-time PCR amplifications were performed in duplicate via TaqMan Gene Expression Assays on ABI Prism 7500 Sequence Detection System (Applied Biosystems). TaqMan Primer Assays (Applied Biosystems) for Nrf2 (Hs00975961_g1), NF-κB (Hs00765730_m1) and the control gene GAPDH (Hs02758991_g1) was performed in PCR protocol: 50 °C for 2 min, 95 °C for 10 min and 40 two-step cycles: 95 °C for 15 s and 60 °C for 1 min. The expression of Nrf2 and NF-κB was calculated using the ΔΔ CT (delta–delta threshold cycle) method.
Determination of total concentrations of IS, p-CS and IAA by HPLC
Indoxyl sulfate (IS) and indole 3-acetic acid (IAA) were purchased from Sigma. p-Cresyl sulfate (p-CS) was a kind gift from Dr. Griet Glorieux (University Hospital Ghent, Belgium). The other reagents were of analytical or chromatographic grade.
Chromatographic determinations were performed with a Shimadzu Prominence system equipped with a Rheodyne injector (model 7125), a quaternary pump (Shimadzu LC-20AD), controlled by the LC Solution software, and a fluorescence detector (Shimadzu RF-20A). C8 Luna column (Phenomenex, Torrance, CA, USA) was used for separation (150 × 4.6 mm, 5 µm) and eluted with 50 mM ammonium formiate pH 3.0 and methanol, whose proportion increased from 35 to 70% (v/v) along the run, at a flow rate of 0.7 mL/min. The fluorescence wavelengths were λ exc = 280 nm/λ em = 383 nm for IS [18] and λ exc = 265 nm/λ em = 290 for p-CS and IAA [19].
Plasma samples were processed as described [18]. Briefly, plasma was diluted with water and heated (95 °C, 30 min). After 10 min in ice, samples were centrifuged (13,000 rpm in bench centrifuge, 4 °C, 20 min) and the supernatant was ultra-filtered with a 30-kDa cutoff membrane (Amicon Ultra, Millipore). The ultra-filtrate (10 μL) was injected in HPLC.
The calibrators were prepared in a pooled healthy plasma matrix and processed exactly as the plasma samples. The amounts added to the 100 μL matrix (IS 0.2–28 μmol; p-CS 0.63–79.6 μmol; IAA 0.02–3 μmol) were chosen to match plasma concentrations ranging from the normal to uremic concentrations of the three toxins [20]. The inferior limits of quantification (LOQ) of the toxins were determined as 10 × σ/S, where σ is the standard deviation of the response (calibrators at the lowest concentrations) and S is the slope of the linear regression.
Plasma samples (100 μL) were spiked with the three authentic standards in the normal or uremic ranges: IS (1.1 or 24 μmol), p-CS (2.6 or 42.5 μmol) and IAA (0.11 or 2 μmol), and processed as described above. Recovery (%) was calculated as (detected amount-basal amount) × 100/added amount.
The intraday precision was determined with five injections of healthy and uremic (from hemodialysis patient) plasma in the same day. The interday precision was determined with injections of three independent preparations of healthy and uremic plasma in three different days. Precision (%) was expressed as relative standard deviation.
Cell culture
Murine macrophage-like RAW 264.7 (Mus musculus) were obtained from RIKEN Bioresource Center (Tsukuba, Japan) and grew in 12-well plates in modified Eagle’s medium (MEM) (GlutaMAX, Invitrogen), supplemented with 100 IU/mL penicillin, 100 µg/mL streptomycin, 1% (v/v) nonessential amino acids and 10% (v/v) heat inactivated (30 min, 56 °C) fetal bovine serum. Cultures were maintained at 37 °C in a water-saturated atmosphere containing 5% (v/v) CO2. 16-h incubations of macrophages cultures were accomplished with IS accordance to the recommendations of the European Uremic Toxin Work Group (EUTox, www.eutox.org) and compared with K2SO4, as a control both diluted in serum-free medium containing 35 g/L of bovine serum albumin (BSA). RAW 264.7 macrophage-like cells were incubated with IS (250, 500, 1000 and 4000 µM).
Cell viability of IS
Cytotoxicity of IS on RAW macrophages cells was determined using Alarmar blue® AbD Serotec (Endeavour House, Langford Business Park, Langford Lane, Kidlington, Oxford) according to the manufacturer’s recommendations.
TNF-alpha assay in RAW 264.7 cells and Malondialdehyde
Culture medium was collected, and TNF-alpha was measured using an immunoassay (Mouse TNF-alpha, Peprotech, Neuilly-Sur-Seine, France) according to the manufacture’s recommendations. RAW 264.7 cells were scrapped, and MDA content was measured using HPLC with visible detection as described by Grotto et al. [21] and normalized to total protein content estimated by Bradford assay.
Real-time quantitative PCR analysis in RAW 264.7 cells
Total RNAs were extracted using TRI Reagent (Sigma-Aldrich). Total RNAs quantities and qualities were assessed using the Agilent 2100 bioanalyzer and RNA 6000 labChip kit (Agilent Technologies, Massy, France). Reverse transcriptions (RNAse H, Takara enzyme) were performed on 1 µg of total RNA. Real-time PCR assays for nrf2, nfkb2, and tbp genes were performed using a Rotor-GeneTM 6000 (QIAGEN). Values were normalized to tbp gene expression. The full list of genes and corresponding primer sequences is shown in Supplementary Table 1.
Statistical analysis
Normal distribution of data was defined using Shapiro–Wilk test, and values were expressed as mean ± standard deviation (SD) or median. Differences among continuous data were analyzed by two-tailed unpaired Student’s t test or Mann–Whitney. Pearson or Spearman correlation coefficient was used to examine the relationships between variables. A multivariate general linear model was used to evaluate the main effects of uremic toxins on Nrf2 and NF-κB mRNA expression. In RAW 264.7 macrophage-like cells, cell viability, Nrf2 and NF-κB mRNA expression, TNF-alpha and MDA content were compared using one-way ANOVA. Statistical significance was accepted as p < 0.05. Statistical analyses were accomplished with SPSS 23.0 (SPSS, Inc., Chicago, IL, USA) and GraphPad Prism v6.0 (Graphpad software, La Jolla, CA).
Results
In vivo
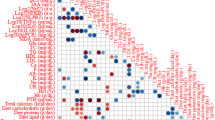
The chromatograms showed a good separation of the three toxins with no interference in their retention times in the plasma samples (Fig. 1). The calibration curves for each toxin presented excellent linearity, with r 2 > 0.99. The LOQs for IS, p-CS and IAA were 4.81, 8.16 and 0.31 pmol injected on column, respectively, corresponding to plasma concentrations of 1.73, 2.94 and 0.11 μM. The recoveries rates (%) were 97.2 ± 1.4 (1.1 μmol) and 99.1 ± 2.2 (24 μmol) for IS, 101.2 ± 6.1 (2.6 μmol) and 99.5 ± 1.9 (42.5 μmol) for p-CS, and 98.8 ± 6.9 (0.11 μmol) and 98.3 ± 3.1 (2 μmol) for IAA. The intraday and interday precision RSD were < 5% for the three toxins.

HPLC determination of indoxyl sulfate (IS), p-cresylsulfate (p-CS) and indole 3-acetic acid (IAA) in plasma. Representative chromatograms of a mixture of authentic standards and a CKD patient’s plasma are shown. The mixture of standards consisted of 122 pmol IS, 153 pmol p-CS and 7 pmol IAA on column. The toxins were separated by a C8 reversed-phase column eluted with 50 mM ammonium formate pH 3.0 with a methanol gradient (35–70%) at 0.7 mL/min. The excitation and emission wavelengths were Ex 280 nm/Em 383 nm for IS and Exc 265 nm/Em 290 for p-CS and IAA
Demographic data of studied groups are presented in Table 1. Age and gender were not different among healthy individuals and HD patients. Biochemical and clinical profile data of CKD patients are summarized in Table 2. CRP, IL-6, MDA and NF-κB values were significantly higher in patients when compared to healthy individuals (p < 0.001), as well as all uremic toxins (Table 3). Uremic toxins levels were positively correlated with NF-κB expression. On the other hand, uremic toxins were negatively correlated with Nrf2. IS levels also presented positive correlations with CRP levels. Besides, positive correlations between MDA and uremic toxins levels were found (Table 4).
Multivariate linear regression analysis adjusted for age, sex, IS, IAA and Nrf2 revealed that NF-κB mRNA expression was independently and positively associated with p-CS plasma levels (β = 0.6; p = 0.01).
In vitro
In RAW 264.7 macrophage-like cells, Nrf2 mRNA expression was decreased by IS exposure from a concentration of 250 µM (Fig. 2a), while exposing macrophage culture to IS stimulates NF-κB mRNA expression at IS concentration of 1000 µM (Fig. 2b). Furthermore, we measured MDA, a common biomarker of lipid peroxidation, as an index of the oxidative stress and was increased in macrophages culture treated with increasing concentrations of IS (Fig. 3). Incubation of RAW 264.7 macrophage-like cells with IS triggered the secretion of TNF-alpha into the culture medium (Fig. 4).

Indoxyl sulfate downregulate Nrf2 expression (a) and NF-κB (b) in RAW 264.7 macrophage-like cells. Cells were incubated for 16 h with 250–1000 µM of indoxyl sulfate (solid bars) or K2SO4 as a control (open bars), and expression of Nrf2 and NF-κB was measured by RT-qPCR as described in methods. Data are mean ± SE for n = 4–5 independent experiments. Data were compared using one-way ANOVA. Different letters indicate a significant difference between groups at the p < 0.05

Indoxyl sulfate exacerbates oxidative damages in RAW 264.7 macrophage-like cells. Cells were incubated for 16 h with 250–1000 µM of indoxyl sulfate (solid bars) or K2SO4 as a control (Open bars), and malondialdehyde (MDA) was measured as an index of lipid peroxidation. Data are mean ± SE for n = 4–5 independent experiments. Data were compared using one-way ANOVA. Different letters indicate a significant difference between groups at the p < 0.05

Indoxyl sulfate induces the secretion of TNF-alpha by RAW 264.7 macrophage-like cells. Cells were incubated for 16 h with 250–1000 µM of indoxyl sulfate (Solid bars) or K2SO4 as a control (Open bars), and TNF-alpha was measured in the culture medium using an immunoassay. Data are mean ± SE for n = 4–5 independent experiments. Data were compared using one-way ANOVA. Different letters indicate a significant difference between groups at the p < 0.05
Discussion
Our results showed increased plasma levels of protein-bound uremic toxins and the negative impact of these toxins on oxidative stress and inflammation in HD patients. In fact, the finding that uremic toxins levels are increased in HD patients has been observed in many studies [1, 3, 11]. However, the observation that NF-κB expression can be stimulated and Nrf2 expression reduced by these uremic toxins is novel. In good agreement, RAW 264.7 macrophage-like cells incubated with IS, as a prototype of protein-bound uremic toxin, exhibited an increased expression of NF-κB mRNA and a decreased expression of Nrf2 mRNA. Finally, this toxin triggered an increase in MDA content in cultured macrophage-like cells, suggesting that this toxin promotes oxidative stress in these cells, and triggered TNF-alpha secretion, a potent pro-inflammatory cytokine.
Protein-bound uremic toxins have received much attention lately, especially because of their effects on inflammation and CVD risk in CKD [22]. In a recent study across the CKD range, there was a significant increase in IS levels with the highest levels observed in the HD population. Further, the toxin was independently associated with CVD. Additionally, a meta-analysis involving patients with CKD stages 3–5 concluded that elevated levels of p-CS and IS were associated with increased mortality in CKD patients and that p-CS was associated with an increased risk of cardiovascular events [11, 23, 24].
Concerning the inflammation and oxidative stress relationships with uremic toxins, Rossi et al. in a recent observational cohort study with nondialysis CKD patients found that serum-free and total IS levels were independently associated with serum IL-6, TNF-alpha and IFN-γ. Besides promoting inflammation, IS may induce ROS production in several cells, such as vascular endothelial cells, vascular smooth muscle cells, renal tubular cells, monocytes and macrophages [11, 25,26,27,28].
Masai et al. demonstrated that IS enhances NADPH oxidase-derived ROS, which, in turn, stimulates the mitogen-activated protein kinase/NF-κB pathway in human umbilical vein endothelial cells (HUVEC). We recently also demonstrated that incubation of adipose cells with IS increased reactive oxygen species production through activation of NADPH oxidase [4, 29].
In agreement with our results, in vitro studies propose that the pathogenic actions of uremic toxins stem from the induction of ROS that stimulate the NF-κB signaling pathway, followed by both oxidative stress and pro-inflammatory cytokine production [30,31,32]. Bolati et al. [14] in a study using human proximal tubular cells (HK-2 cells) and rat kidney cells found that IS downregulates the expression of Nrf2 through activation of NF-κB, with subsequent decrement of antioxidants enzymes and increased production of ROS. Lekawanvijit et al. [32] showed that IS stimulated the mitogen-activated protein kinase (MAPK) and NF-κB pathways on cardiac cells. These findings may explain the correlations of uremic toxins and oxidative stress and inflammation in HD patients presented in our results.
Our in vivo results confirm the hypothesis that IS may modulate NF-κB and Nrf2 mRNA expression. Nrf2 translocation to the nucleus leads to a rise in the transcription of ARE-regulated genes of antioxidants and phase II detoxifying enzymes, including NAD(P)H quinone oxidoreductase (NQO1), heme oxygenase-1 (HO-1), glutathione S-transferase (GST), glutathione peroxidase (GSH-Px), catalase, superoxide dismutase (SOD). These phase II enzymes perform a crucial function in cellular defense by intensifying the removal of ROS [33,34,35,36]. Therefore, Nrf2 appears to play an important role in cellular protection against oxidative stress.
Recently, Lau et al. analyzed the expression of inflammatory and tight junction proteins in the colon from CKD rats compared to healthy controls and demonstrated the impact of Nrf2 using a potent Nrf2 activator. The authors showed the role of Nrf2 system damage as another cause of the intestinal epithelial tight junction disorder in CKD. Increase in urea levels in body fluids leads to urea influx into the intestinal lumen and triggers local inflammation by enabling the influx of endotoxin. This inflammation further increases disruption of the epithelial barrier structure and function [37, 38].
The activation of Nrf2 in CKD appears to be an important pathogenic mechanism in response to the presence of ROS and other uremic toxins. According to Saito et al. [39], the suppressive effects of Nrf2 activation on the inflammatory reaction via NF-κB inhibition are likely to be important for preventing the progression of CKD. According to the current study, as uremic toxins issued from the gut microbiota may accentuate the imbalance between Nrf2 and NF-κB, therapeutic strategies such as the use of probiotics, prebiotics and symbiotic may represent novel therapeutic approaches to decrease the cardiovascular risk of CKD patients [40].
This study presents some limitations. First, the size sample is limited. Second, protein intake was not evaluated which prevented us to estimate intakes of tryptophan, as well as Keap1 and antioxidants enzymes expression. Moreover, the levels of the final functional protein product to Nrf2 and NF-κB were not evaluated by Western Blotting, to confirm that gene transcription was not affected by translational or posttranslational modifications. Lastly, the effects of IAA and p-CS in vitro were not evaluated. Besides that, it would better to cultivate PBMCs or monocytes cells from our patients to obtain more results than RAW 264.7. However, we do not have support to perform this cell culture. This was a very well-controlled protocol, which allowed us to conclude that the results are considerably relevant.
In conclusion, the present study reports that an increase in uremic toxins as observed in maintenance dialysis may activate the NF-κB mRNA expression and inhibit Nrf2 mRNA expression in HD patients, consequently contributing to inflammation and oxidative stress commonly observed in these patients.
References
Meijers BK, Evenepoel P (2011) The gut-kidney axis: indoxyl sulfate, p-cresyl sulfate and CKD progression. Nephrol Dial Transplant 26:759–761
Mafra D, Lobo JC, Barros AF, Koppe L, Vaziri ND, Fouque D (2014) Role of altered intestinal microbiota in systemic inflammation and cardiovascular disease in chronic kidney disease. Future Microbiol 9(3):399–410
Deltombe O, Biesen WV, Glorieux G, Massy Z, Dhondt A, Eloot S (2015) Exploring protein binding of uremic toxins in patients with different stages of chronic kidney disease and during hemodialysis. Toxins 7:3933–3946
Stockler-Pinto MB, Saldanha JF, Yi D, Mafra D, Fouque D, Soulage CO (2016) The uremic toxin indoxyl sulfate exacerbates reactive oxygen species production and inflammation in 3T3-L1 adipose cells. Free Radic Res 50(3):337–344
Sallée M, Dou L, Cerini C, Poitevin S, Brunet P, Burtey S (2014) The aryl hydrocarbon receptor-activating effect of uremic toxins from tryptophan metabolism: a new concept to understand cardiovascular complications of chronic kidney disease. Toxins 6:934–949
Lee WC, Li LC, Chen JB, Chang HW (2015) Indoxyl sulfate-induced oxidative stress, mitochondrial dysfunction, and impaired biogenesis are partly protected by vitamin C and N-acetylcysteine. Sci World J 2015:1–6
Tang WH, Wang CP, Chung FM, Huang LL, Yu TH, Hung WC et al (2015) Uremic retention solute indoxyl sulfate level is associated with prolonged QTc interval in early CKD patients. PLoS ONE 10(3):e0119545
Poesen R, Windey K, Neven E, Kuypers D, De Preter V, Augustijns P et al (2015) The influence of CKD on colonic microbial metabolism. J Am Soc Nephrol 27(5):1389–1399
Gao C, Ji S, Dong W, Qi Y, Song W, Cui D, Shi J (2015) Indolic uremic solutes enhance procoagulant activity of red blood cells through phosphatidylserine exposure and microparticle release. Toxins 7:4390–4403
Jourde-Chiche N, Dou L, Cerini C, Dignat-George F, Vanholder R, Brunet P (2009) Protein-bound toxin—update 2009. Semin Dial 22(4):334–339
Rossi M, Campbell KL, Johnson DW, Staton T, Vesey DA, Coombes JS et al (2014) Protein-bound uremic toxins, inflammation and oxidative stress: a cross-sectional study in stage 3–4 chronic kidney disease. Arch Med Res 45(4):309–317
Watanabe H, Miyamoto Y, Honda D, Tanaka H, Wu Q, Endo M et al (2013) p-Cresyl sulfate causes renal tubular cell damage by inducing oxidative stress by activation of NADPH oxidase. Kidney Int 83:582–592
Dou L, Sallée M, Cerini C, Poitevin S, Gondouin B, Jourde-Chiche N (2014) The cardiovascular effect of the uremic solute indole-3 acetic acid. J Am Soc Nephrol 26(4):876–887
Bolati D, Shimizu H, Yisireyili M, Nishijima F, Niwa T (2013) Indoxyl sulfate, a uremic toxin, downregulates renal expression of Nrf2 through activation of NF-kappaB. BMC Nephrol 4(14):56
Pedruzzi LM, Stockler-Pinto MB Jr, Leite M, Mafra D (2012) Nrf2-keap1 system versus NF-kappaB: the good and the evil in chronic kidney disease? Biochimie 94:2461–2466
Leal VO, Saldanha JF, Stockler-Pinto MB, Cardozo LF, Santos FR, Albuquerque AS et al (2015) NRF2 and NF-κB mRNA expression in chronic kidney disease: a focus on nondialysis patients. Int Urol Nephrol 47(12):1985–1989
Daugirdas JT (1993) Second generation logarithmic estimates of single-pool variable volume Kt/V: an analysis of error. J Am Soc Nephrol 4:1205–1213
de Loor H, Meijers BK, Meyer TW, Bammens B, Verbeke K, Dehaen W, Evenepoiel P (2009) Sodium octanoate to reverse indoxyl sulfate and p-cresyl sulfate albumin binding in uremic and normal serum during sample preparation followed by fluorescence liquid chromatography. J Chromatogr A 1216(22):4684–4688
Meert N, Schepers E, Glorieux G, Landschoot MV, Goeman JL, Waterloos MA et al (2012) Novel method for simultaneous determination of p-cresylsulphate and p-cresylglucuronide: clinical data and pathophysiological implications. Nephrol Dial Transplant 27(6):2388–2396
Boelaert J, Lynen F, Glorieux G, Eloot S, Van Landschoot M, Waterloos MA et al (2013) A novel UPLC-MS-MS method for simultaneous determination of seven uremic retention toxins with cardiovascular relevance in chronic kidney disease patients. Anal Bioanal Chem 405(6):1937–1947
Grotto D, Santa Maria LD, Boeira S, Valentini J, Charão MF, Moro AM et al (2007) Rapid quantification of malondialdehyde in plasma by high performance liquid chromatography-visible detection. J Pharm Biomed Anal 43(2):619–624
Neirynck N, Vanholder R, Schepers E, Eloot S, Pletinck A, Glorieux G (2013) An update on uremic toxins. Int Urol Nephrol 45:139–150
Liabeuf S, Barreto DV, Barreto FC, Meert N, Glorieux G, Schepers E (2010) Free p-cresylsulphate is a predictor of mortality in patients at different stages of chronic kidney disease. Nephrol Dial Transplant 25(4):1183–1191
Lin CJ, Wu V, Wu PC (2015) Meta-analysis of the associations of p-cresyl sulfate (PCS) and indoxyl sulfate (IS) with cardiovascular events and all-cause mortality in patients with chronic renal failure. PLoS ONE 10(7):e0132589
Ito S, Osaka M, Higuchi Y, Nishijima F, Ishii H, Yoshida M (2010) Indoxyl sulfate induces leukocyte-endothelial interactions through up-regulation of E-selectin. J Biol Chem 285(50):38869–38875
Adelibieke Y, Shimizu H, Muteliefu G, Bolati D, Niwa T (2012) Indoxyl sulfate induces endothelial cell senescence by increasing reactive oxygen species production and p53 activity. J Ren Nutr 22(1):86–89
Adesso S, Popolo A, Bianco G, Sorrentino R, Pinto A, Autore G et al (2013) The uremic toxin indoxyl sulphate enhances macrophage response to LPS. PLoS One 8(9):e76778.30
Shimizu H, Yisireyli M, Higashiyama Y, Nishijima F, Niwa T (2013) Indoxyl sulfate upregulates renal expression of ICAM-1 via production of ROS and activation of NF-kappa b and p53 in proximal tubular cell. Life Sci 92(2):1143–1148
Masai N, Tatebe J, Yoshino G, Morita T (2010) Indoxyl sulfate stimulates monocyte chemoattractant protein-1 expression in human umbilical vein endothelial cells by inducing oxidative stress through activation of the NADPH oxidase-nuclear factor-kB pathway. Circ J 74:2216–2224
Gelasco AK, Raymond JR (2006) Indoxyl sulfate induces complex redox alterations in mesangial cells. Am J Physiol Ren Physiol 290:1551–1558
Goundouin B, Cerini C, Dou L, Salée M, Durvai-Sabatier A, Pletinck A et al (2013) Indolic uremic solutes increase tissue factor production in endothelial cells by the aryl hydrocarbon receptor pathway. Kidney Int 84:733–744
Lekawanvijit S, Adrahtas A, Kelly DJ, Kompa AR, Wang BH, Krum H (2010) Does indoxyl sulfate, a uraemic toxin, have direct effects on cardiac fibroblasts and myocytes? Eur Heart J 31:1771–1779
Jung KA, Kwak MK (2010) The Nrf2 system as a potential target for the development of indirect antioxidants. Molecules 15(10):7266–7291
Singh S, Vrishni S, Singh BK, Rahman I, Kakkar P (2010) Nrf2-ARE stress response mechanism: a control point in oxidative stress-mediated dysfunctions and chronic inflammatory diseases. Free Radic Res 44(11):1267–1288
Baird L, Dinkova-Kostov AT (2011) The cytoprotective role of the Keap1-Nrf2 pathway. Arch of Toxicol 85(4):241–272
Kim HJ, Vaziri ND (2010) Contribution of impaired Nrf2-Keap1 pathway to oxidative stress and inflammation in chronic renal failure. Am J Physiol Ren Physiol 98(3):662–671
Lau WL, Liu SM, Pahlevan S, Yuan J, Khazaeli M, Ni Z et al (2014) Role of Nrf2 dysfunction in uremia-associated intestinal inflammation and epithelial barrier disruption. Dig Dis Sci 60(5):1215–1222
Koppe L, Mafra D, Fouque D (2015) Probiotics and chronic kidney disease. Kidney Int 88(5):958–966
Saito H, Yoshimura M, Saigo C, Komori M, Nomura Y, Yamamoto Y et al (2014) Hepatic sulfotransferase as a nephropreventing target by suppression of the uremic toxin indoxyl sulfate accumulation in ischemic acute kidney injury. Toxicol Sci 141(1):206–217
Gao H, Liu S (2017) Role of uremic toxin indoxyl sulfate in the progression of cardiovascular disease. Life Sci 185:23–29
Acknowledgements
This study was supported by Conselho Nacional de Pesquisa (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Clinical Research Unit (UPC) at Fluminense Federal University (UFF), Comité Français d´Evaluation de la Coopération Universitaire avec le Brésil (COFECUB), Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ), Institut National de la Santé et de la Recherche Medicale (INSERM) and Institut National des Sciences Appliquées de Lyon (INSA-Lyon).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of Medicine Faculty of Federal University Fluminense and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individuals participants included in the study.
Statement of animal studies
This article does not contain any studies with animals performed by any of the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Stockler-Pinto, M.B., Soulage, C.O., Borges, N.A. et al. From bench to the hemodialysis clinic: protein-bound uremic toxins modulate NF-κB/Nrf2 expression. Int Urol Nephrol 50, 347–354 (2018). https://doi.org/10.1007/s11255-017-1748-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-017-1748-y