
Abstract
Purpose
The aim of the study was to investigate whether perceived family functioning of adolescent is moderating or mediating the longitudinal association of adolescent internalizing and externalizing psychopathology with quality of life (QoL) after 6 months in the general population.
Methods
Using a cluster sampling technique in one Norwegian county 1331, 10- to 16-year-old students were included in the study (51 % girls). Parents completed the Child Behavior Checklist for the assessment of adolescent psychopathology at Time 1. The students completed the General Functioning Scale of the McMaster Family Assessment Device and the Inventory of Life Quality in Children and Adolescents at time 2 6 months later. Psychopathology, family functioning and QoL were treated as latent variables in a structural equation model adjusted for sex, age and parent education.
Results
The regression coefficients for paths from psychopathology decreased (β = .199 for the internalizing and β = .102 for the externalizing model) in each case when including the indirect path via family functioning compared with the direct path from psychopathology to QoL. The sum of indirect effects on QoL via family functioning was significant for internalizing β = 0.093 (95 % CI 0.054–0.133) and externalizing β = 0.119 (95 % CI 0.076–0.162) psychopathology.
Conclusions
Family functioning significantly mediated the longitudinal association between psychopathology and QoL. Because the family remains an important social domain for adolescents, it must be an important consideration when attempting to reduce or alleviate psychopathology in youth and improve the quality of their life experience throughout this period.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Little is known about the specific connections between psychopathology, family functioning and quality of life (QoL) in the general adolescent population. Such knowledge would be important for both parents and professionals, for example, school counselors, family and child therapists, and psychiatrists, to optimize interventions for youth with emotional and behavioral problems. Adolescence represents a vulnerable developmental period when youth spend more time with friends outside the family and may appear less connected to their family [1]. However, the transformation model from childhood to adulthood [2] emphasizes that the family still plays a salient role, and in that an important developmental task for adolescents is to achieve psychological independence from parents while maintaining connectedness with them. At the same time, adolescence is the period in which many mental disorders begin to develop [3]. The overall prevalence of disorders with severe impairment and/or distress was 22.2 % in a nationally representative sample of US adolescents [4]. The median age of onset was 11 years for behavior disorders and 13 years for mood disorders. For one in five adolescents with psychopathology, this developmental task of transforming the relationship with family may represent even a larger challenge than for those without mental health problems. Poor mental health is strongly related to other health and developmental concerns in young people, notably lower educational achievements, substance abuse, violence [3] and criminal activity, and they are more likely to have conceived a child [5]. These material and social indicators provide important information about adolescents’ life conditions associated with psychopathology. In addition, a new focus on well-being and QoL of children has been established in psychology during recent years [6].
Here, we define QoL as the adolescent’s perceived subjective well-being and satisfaction with life that is best evaluated by the adolescent, according to his/her own experience with regard to several life domains [7]. This concept is partly comprised of positive and negative effects as an emotional appraisal of health and life circumstances, as well as an emotional state that is determined by interpersonal aspects and temperament. Although QoL is influenced by one’s psychological state, it can be distinguished from the concept of “psychopathology,” which refers specifically to mental health problems, symptoms or disorders [8]. Even though QoL is lower in child psychiatric patients compared with peers not in treatment but with equal levels of psychopathology [9], it is possible to improve QoL without psychiatric symptom reduction [10].
To further investigate the link between adolescent psychopathology and QoL, larger longitudinal studies in the general population are called for, but they have been sparse thus far. Chen and colleagues [11] have shown that mental disorders in adolescence may have more adverse long-term associations with QoL than do physical illnesses in adulthood 17 years later. Further, it has been shown that changes in mental health status are associated with children’s and adolescents’ health-related QOL over a 3-year period, in that improvements in mental health status may protect against poorer health-related QoL (HRQoL), while a worsening in mental health status is a risk factor for poorer HRQoL [12]. Adolescents’ self-rated physical and mental health declined significantly from 2001 to 2010, especially among those in low-income families [13].
The high burden of psychopathology has serious consequences for family functioning, in that psychopathology impact not just on the individuals affected but also on those around them, including immediate family and other relatives (p. 3) [14]. Further, mental disorders may be both a cause and a consequence of family difficulties [14]. Thus, adolescent report of family functioning problems was found to be the strongest correlate of referral to speciality mental health services, more so than mental health problems except for suicidality [15]. Studies indicate that family functioning of children and adolescents with depression is poorer than that of controls [16, 17] and that an increased amount of coexisting mental health problems in adolescents with ADHD were associated with poorer family functioning and QoL [18]. Findings also showed that both maternal and paternal anxiety and depression were significantly associated with subjective well-being, self-esteem, anxiety/depression, and social anxiety in both daughters and sons [19]. However, in a longitudinal community study, no evidence was found that family dysfunction played a causal role in subsequent adolescent depressive disorder [20]. At the same time, good family functioning or cohesion may also represent a protective factor promoting resilience [21]. For example, higher family cohesion has been associated with lower internalizing and externalizing problem behavior in children [22], and while adoption from foster care is negatively associated with family functioning, higher family cohesion mediate this influence on children’s ADHD symptomatology [23].
Aims of the study
The goal here was to investigate two possible mechanisms that could clarify the role of family functioning in the relationship between psychopathology and QoL in adolescence: (1) Family functioning could mediate this relationship such that higher adolescent pathology is associated with lower family functioning, which in turns is associated with poorer QoL and that this mechanism accounts for a significant portion of the association between adolescent psychopathology and QoL. (2) Family functioning could moderate the association between psychopathology and QoL, suggesting that good family functioning would protect against a link between psychopathology and poor QoL. We depict these two models in Fig. 1. Understanding the role of family functioning in the link between adolescent psychopathology and QoL may provide direction how the whole family can be a target for both prevention and treatment of adolescent psychopathology during a sensitive developmental period. Further, we wanted to examine these processes separately for internalizing and externalizing psychopathology, because it might be that family functioning is differentially associated with these two major dimensions of mental health problems.

Proposed mediation (upper panel) and moderation (lower panel) models. T2 is measured 6 months after T1
Method
Population, sample selection and participants
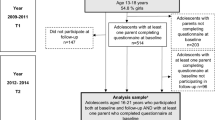
The present study is based on data from the study “Changes of QoL among Norwegian school children” [24], which employed a 6-month prospective cohort observational design. The students in the Norwegian county of Sør-Trøndelag were stratified according to geography and grade, and fourth, sixth, eighth and tenth grades were targeted in the sampling design. In this county, half of the population lives in an urban (the city of Trondheim) and the other half in rural areas. The national Norwegian database for primary education (GSI) was used to enumerate all students attending the targeted grades in all schools and relevant region, which led to that 426 school-grade cohorts were identified. We aimed to obtain a representative sample of about 2000 students who consented to participate in the study. We used a cluster sampling technique, and 61 school-grade cohorts were randomly selected for the study, containing 2902 students. Participation exclusion criteria were (a) insufficient competence in the Norwegian language or (b) having a developmental level more than 2 years below the relevant grade. To decide whether a student fulfilled the exclusion criteria, the local coordinator (a teacher at each school) discussed possible students being excluded from the study with the principal investigator, which led to 98 students being excluded. For 786 students, parents did not consent for their participation, and 21 students did not meet scheduled appointments. Thus, 1997 students (990 girls, 1007 boys) aged 8–16 years were enrolled in the study at T1, yielding a response rate of 71.2 % (of 2804). Of the 1909 students eligible, 1821 (95.4 %) completed the 6-month follow-up assessment at T2. The follow-up sample was representative of the population with regard to urban-to-rural resident ratio (1:1.1).
The fourth graders (8–10 years old) from the original sample were excluded for the present study that focused on adolescents, leaving, 447 sixth graders, 383 eighth graders and 501 tenth graders, for a total 1331 students, of which 678 were girls (51 %), mean age 13.1 years (SD = 1.5 years), and range 10–16 years. For these students, 1169 valid parent reports on the Child Behavior Checklist (see below) were available. Table 1 provides more descriptive information, and further details about the sample are provided in [24, 25].
Assessment procedures
One teacher at each school was appointed as a project coordinator and given information about the research project and procedures for collecting the data. The coordinator informed the students about the project and also sent a standard information letter to their parents. The principal investigator (the first author) or a research assistant was present at each school when the students completed the questionnaires at each assessment occasion. They stressed informant confidentiality and responded to questions, and read questions aloud for students with reading problems. Completed questionnaires marked with an ID number only were collected in sealed envelopes by the researchers .
Measures
Sociodemographic information
Participants completed a demographic form requesting information about age, sex and socioeconomic status (SES) at T1. The highest educational level of parents on a seven-point Hollingshead scale was used to estimate SES [26].
Psychopathology
The problem scales of the 2001 version of the Child Behavior Checklist (CBCL) [27] for children aged 6–18 years were completed by parents at T1. It consists of 118 Likert-type and two open-ended items rated on a 0–2 scale (0 = Not True, 1 = Somewhat or Sometimes True, or 2 = Very True or Often True). These items can be grouped into syndrome subscales, of which Anxious/depressed (range 0–26), Withdrawn/depressed (range 0–16) and Somatic Complaints (range 0–22) subscales are used to indicate Internalizing Problems, and Rule-breaking Behavior (range 0–34) and Aggressive Behavior (range 0–36) subscales as Externalizing Problems. The Norwegian version of the CBCL has shown satisfactory predictive, discriminant and convergent validity [28]. Reliability was also satisfactory for the scales used in this study [29].
Quality of life
The Inventory of Life Quality in Children and Adolescents (ILC) [30] consists of seven core items and two additional questions and was developed as a short and practical assessment tool for use in child mental health settings. The Norwegian version of the ILC [31] for adolescents was used to assess QoL over the past week. The seven ILC core items include one global QoL item and six items addressing school performance, family functioning, social integration, interests and hobbies, physical health, and mental health, respectively. Each item is rated on a 1–5 scale (1 = very good, 5 = very bad). After linear transformation, the ILC yields a score on a 0–100 scale (0 = Very low QoL, 100 = Very high QoL). Satisfactory reliability of the Norwegian ILC was evidenced by Cronbach’s alpha = 0.81 for adolescents and ICC test–retest = 0.89 for sixth graders. Validity of the Norwegian version was also satisfactory [31]. Data from the ILC at T2 were used in the present study. Also, for the present study the item addressing family functioning was excluded due to logical overlap with the construct of family functioning (see below), leaving six items to measure QoL.
Family functioning
The General Functioning Scale (GFS) of the Norwegian version [15] of the McMaster Family Assessment Device (FAD) [32] is a 12-item adolescent self-report measure of family functioning in six areas, including problem solving, communication, roles, affective responsiveness, affective involvement and behavioral control [33]. Each item is rated on 1–4 rating scales, (1 = Strongly agree and 4 = Strongly disagree). Every second item is negatively worded. Responses are transformed for negatively worded items and summed to obtain an overall family functioning score, ranging 12–48 [32] where a low score reflect healthy and a high score unhealthy family functioning [34]. The internal consistency reliability of the GFS is good, with a Chronbach’s alpha of 0.92 [32]. The construct validity of the GFS was supported in a large epidemiological study of all children from 4 to 16 years in [33]. Validity was assessed by hypothesizing the relationships expected between the GFS scores and other family variables such as parental deviance, alcohol abuse, emotional disorder, marital disharmony, parental separation, spouse abuse and mental health of parent included in the Ontario Child Health Study. Data from its administration at T2 were used in the present study.
Statistics
Due to our cluster sampling procedure, we first explored possible cluster effects by mixed linear models. The results of an analysis of unconditional random effects showed that only 3.6 % of the total variance of the ILC sum scores, the dependent variable in our analysis, could be explained by differences between the 61 school-grade cohorts in the study. Because the QoL measure in the sample was only minimally influenced by differences between grade cohorts, the main analyses were conducted on an individual level. Applying Full Information Maximum Likelihood (FIML), all further analyses were based on a complete dataset of N = 1331. Missing item values were low for the 1331 adolescents reporting on the ILC (0.2–1.5 %) and GFS (0.9–3.5 %), and higher for CBCL (12.2 %) and SES information (10.5 %).
To explore the relationships among adolescent internalizing and externalizing psychopathology at T1 and family functioning and QoL at T2, these concepts were treated as latent variables. The CBCL subscales Anxious/depressed, Withdrawn/depressed and Somatic Complaints were indicators for Internalizing psychopathology, and the Rule-breaking and Aggression subscales were indicators for Externalizing psychopathology. An exploratory factor analysis (EFA) of the GSF indicated that “family functioning” should be divided into “positive family functioning” and “negative family functioning” according to positive or negative wording of the questions, see Table 2. “QoL” was measured by six ILC core items.
Because not all scales of the CBCL, and not all items of the ILC were used in this research, and because the factor structure of the Norwegian version of the GSF has not been established in previous research, the validity of the original scales could not be assumed to apply. Fit indices were therefore reported for the measurement model in order to validate the three latent variables in this study [35], including the Chi-square test (χ 2), comparative fit index (CFI), the Tucker–Lewis index (TLI), and root-mean-square error of approximation (RMSEA). With respect to CFI and TFI, values above 0.95 are considered indications of good fit, whereas values below 0.06 are considered indices of good fit with respect to the RMSEA.
The structural equation model was estimated with the weighted least-square parameter estimates using the WLSMV method due to the categorical nature of the ILC and GSF items. Completely saturated structural models where all latent variables were regressed on each other were tested (see Fig. 1). In accordance with our research questions, the path models are therefore explorative, and we will not report decomposable fit indices for the path model. We also calculated the sum of indirect effects with 95 % confidence intervals for the mediated paths in the models using bootstrapping [36]. The path model was adjusted for sex, age and SES in the analyses. Whereas we used Mplus, version 7.2 [36] for the structural equation analyses, IBM SPSS Statistics 19 was used for other statistics. Alpha level of two-sided p values <.01 was considered statistically significant.
Ethics
This study was approved by the Regional Committee for Medical Research Ethics in Central Norway, and all adolescents and parents who participated gave their written informed consent.
Results
Measurement model
Except for a significant Chi-square statistic (χ 2(262) = 1170, p < .0001), other measures of goodness of fit indicated a good measurement model fit (CFI = .957, TLI = .951, RMSEA = .051). A significant Chi-square statistic is, however, not surprising due to the large sample size. Table 2 displays the results of the measurement model with standardized factor loadings. Also indicative of an acceptable model fit, factor loadings were satisfactory for all indicators (≥0.549). Table 3 reports the correlations among the latent variables, which are from low to moderate, except for positive and negative family functioning which, as expected, showed a high correlation.
Family functioning as a mediator
Figure 2 displays the standardized regression weights for the statistically significant paths in the models. The indirect paths from psychopathology to QoL showed that increased internalizing and externalizing psychopathology were significantly associated with poor family functioning 6 months later. Further, both positive family functioning and negative family functioning were significantly associated with QoL both in the internalizing and externalizing model, where poor family functioning was associated with poor QoL. The regression coefficients for paths from psychopathology to QoL remained significant, but decreased (β = .199 for the internalizing and β = .102 for the externalizing model) in each case when including the indirect path via family functioning compared with only the direct path from psychopathology to QoL (β = .293 and β = .224, respectively). The sum of indirect effects were significant 0.093 (95 % CI 0.054–0.133) for internalizing and 0.119 (95 % CI 0.076–0.162) for externalizing psychopathology. Thus, family functioning can be interpreted significantly to mediate the longitudinal association between psychopathology and QoL.

Mediation model significant paths with standardized coefficients controlled for adolescent sex, age and family SES
Family functioning as a moderator
A moderation model was tested by including the interactions between the two family functioning latent variables and internalizing and externalizing psychopathology, respectively, together with the four main effects in a model being regressed on QoL. However, none of these interaction paths was significant. Thus, family functioning cannot be interpreted to moderate the association between psychopathology and QoL 6 months later.
Discussion
This is the first study that we are aware of to investigate in adolescents in the general population whether their perceived family functioning is mediating and/or moderating the effect of psychopathology on their subjective QoL over a 6-month period. Both internalizing and externalizing psychopathology predicted QoL 6 months later. Further, the results supported the mediation model (see Fig. 1), for both internalizing and externalizing psychopathology. Adolescents with higher psychopathology according to their parents, in either the internalizing or externalizing domains, also perceived a reduced functioning of their family 6 months later, and poor family functioning was in turn associated with a reduced subjective QoL at that time. However, not all of the effect of adolescent psychopathology on QoL was mediated by family functioning, as indicated by a reduced but still significant direct prediction of QoL in the mediation model. For internalizing psychopathology, the mediation model reduced the direct effect on QoL by one-third and for externalizing psychopathology by one-half. There was no support for the model proposing that perceived family functioning moderated the effect of adolescent psychopathology on their subjective QoL 6 months later.
Our results are in accordance with the transformation model from childhood to adulthood [2], emphasizing that the family still plays a salient role during adolescence. An important developmental task for adolescents in this period is to achieve psychological independence from parents, while still maintaining connectedness with them. We have shown in an earlier study [24] that eighth graders in the community reported a decrease in QoL in the family domain over a 6-month follow-up period as compared to those in the sixth grade when measured with another QoL instrument, the KINDL [37]. These child-reported changes represented small effects and could be interpreted as reflecting normal psychological development during puberty together with contextual transitions in parent–child relationships. In the present study, which included adjustments for age and sex effects, we found that externalizing problems were associated over time with a reduced QoL, and that this association was partly mediated by a reduced family functioning. Thus, the family appears involved in adolescents who display behavioral problems. These results are in accordance with earlier research, for example reporting that family cohesion was negatively associated with adolescents’ externalizing problems [38]. Likewise, maternal warmth and overall parental emotional support, in addition to overall neighborhood support, were important predictors of externalizing behavior problems [39]. On the other hand, elevations in adolescent problem behavior prospectively predicted decreases in perceived family cohesion and increases in family conflict [40], but family cohesion and conflict did not predict problem behavior. Even if our study has a longitudinal design, we cannot draw conclusions with regard to causality. However, our study extends previous research by adding the adolescents QoL perspective. These results suggests it is important to address the whole family, either by strengthening it preventively or treating and supporting it when it includes an adolescent with externalizing problems, to increase his/her QoL.
We found that family functioning is also mediating the link between internalizing problems and QoL after 6 months. This result is consistent with several studies reporting that psychological well-being and self-esteem are reduced in children of mothers with depression [41]. Further, both maternal and paternal anxiety and depression were significantly associated with subjective well-being, self-esteem, anxiety/depression, and social anxiety in both adolescent daughters and sons [19]. Thus, family aggregation of internalizing mental health problems may have negative consequences for offsprings’ QoL and subjective well-being. Further, reduced psychological well-being may constitute a risk of depression [41], whereas high well-being protects against depression [42]. In our study, we did not find family functioning being a moderator of the association between internalizing problems and QoL. Thus, we cannot conclude from our study that a healthy family functioning is protecting adolescents with internalizing problems experiencing reduced QoL. However, our findings emphasize the important role of family functioning for adolescent QoL when the offspring suffers internalizing problems. The developmental task for adolescents to achieve psychological independence from parents, while maintaining connectedness with them, can become jeopardized in an overprotective family. In their conceptual overview Ballash and colleagues point out that extensive research is indicating that anxious parents or parents of anxious children are more controlling than non-anxious parents at various child ages [43]. Further, they hypothesize that anxious parents could be unable to adjust their controlling behavior appropriately to their child’s developmental progression. For adolescents with externalizing behavior problems, well-established interventions are available involving the family and community (e.g., Multisystemic Therapy [44]). However, therapy for internalizing problems as anxiety and depression are often individualized (e.g., cognitive behavioral therapy). Our results suggest that in treatment also of adolescents with internalizing problems, professionals should consider enhancing and inhibiting family processes beyond providing individual interventions, which could increase adolescents’ QoL during a vulnerable developmental period.
Strengths and limitations of the study
Strength of this study is the investigation of possible associations of psychopathology with QoL over time in the general population of adolescents. A sizable cohort could be followed prospectively over 6 months with quite low attrition (<5 %). Two hypothesized models of mechanisms for family functioning were examined with sophisticated analytic techniques with due consideration for measurement errors. One important limitation is the correlational design, which prohibits confirmation of causality. Moreover, not measuring all constructs at both time points removed the possibility to examine all possible concurrent and longitudinal associations using full cross-lagged or autoregressive models. For example, it is conceivable that family functioning is a causal mechanism primarily influencing adolescent psychopathology, contrary to the interpretation implied in the meditational model tested here. However, this could not be evaluated without measuring both constructs at both times. Another limitation may be the Norwegian population examined here, which is more homogeneous regarding ethnic and socioeconomic status compared to most others. All constructs were measured with questionnaires, each from a single source, and multi-informant and/or multi-method measurements would be an improvement.
Conclusion
Problems in adolescence do not inevitably develop as previously held [45]; however, adolescence may be a challenging period for some. When psychopathology develops in adolescence, this inevitable interacts with the functioning of the family. In the present study, family functioning significantly mediated the longitudinal association between psychopathology and QoL in the adolescent general population, also with regard to internalizing problems. The family remains the most important social domain for the vast majority of adolescents [2, 46], and it must be an important consideration when attempting to reduce or alleviate psychopathology in youth and improve their quality of their life experience throughout this period.
References
Larson, R. W., Richards, M. H., Moneta, G., Holmbeck, G., & Duckett, E. (1996). Changes in adolescents’ daily interactions with their families from ages 10 to 18: Disengagement and transformation. Developmental Psychology, 32(4), 744–754. doi:10.1037/0012-1649.32.4.744.
Collins, W. A., & Laursen, B. (2004). Changing relationships, changing youth: Interpersonal contexts of adolescent development. Journal of Early Adolescence, 24(1), 55–62. doi:10.1177/0272431603260882.
Patel, V., Flisher, A. J., Hetrick, S., & McGorry, P. (2007). Mental health of young people: A global public-health challenge. Lancet, 369(9569), 1302–1313. doi:10.1016/s0140-6736(07)60368-7.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., et al. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980–989. doi:10.1016/j.jaac.2010.05.017.
Vander Stoep, A., Beresford, S. A., Weiss, N. S., McKnight, B., Cauce, A. M., & Cohen, P. (2000). Community-based study of the transition to adulthood for adolescents with psychiatric disorder. American Journal of Epidemiology, 152(4), 352–362.
Holte, A., Barry, M. M., Bekkhus, M., Borge, A. I. H., Bowes, L., Casas, F., et al. (2014). Psychology of child well-being. In A. Ben-Arieh, F. Casas, I. Frønes, & J. E. Korbin (Eds.), Handbook of child well-being : Theories, metods and policies in global perspective (pp. 555–632). Netherlands: Springer.
Mattejat, F., & Remschmidt, H. (1998). Zur Erfassung der Lebensqualität bei psychisch gestörten Kindern und Jugendlichen—Eine Übersicht (Assessment of life quality in children and adolescents with mental disorders—An overview). Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie, 26, 183–196.
Koot, H. M. (2001). The study of quality of life: Concepts and methods. In H. M. Koot & J. L. Wallander (Eds.), Quality of life in child and adolescent illness (pp. 3–20). New York: Brunner-Routledge.
Jozefiak, T., Larsson, B., Wichstrom, L., Wallander, J., & Mattejat, F. (2010). Quality of Life as reported by children and parents: A comparison between students and child psychiatric outpatients. Health Qual Life Outcomes, 8, 136. doi:10.1186/1477-7525-8-136.
Bastiaansen, D., Koot, H. M., & Ferdinand, R. F. (2005). Psychopathology in children: Improvement of quality of life without psychiatric symptom reduction? European Child and Adolescent Psychiatry, 14(7), 364–370. doi:10.1007/s00787-005-0481-8.
Chen, H., Cohen, P., Kasen, S., Johnson, J. G., Berenson, K., & Gordon, K. (2006). Impact of adolescent mental disorders and physical illnesses on quality of life 17 years later. Archives of Pediatrics and Adolescent Medicine, 160(1), 93–99. doi:10.1001/archpedi.160.1.93.
Rajmil, L., Palacio-Vieira, J. A., Herdman, M., Lopez-Aguila, S., Villalonga-Olives, E., Valderas, J. M., et al. (2009). Effect on health-related quality of life of changes in mental health in children and adolescents. Health Qual Life Outcomes, 7, 103. doi:10.1186/1477-7525-7-103.
Cui, W., & Zack, M. M. (2013). Trends in health-related quality of life among adolescents in the United States, 2001–2010. Preventing Chronic Disease, 10, E111. doi:10.5888/pcd10.120334.
Robinson, E., Rodgers, B., & Butterworth, P. (2008). Family relationships and mental illness. AFRC Issues (pp. 1–19). Commonwealth of Australia: Australian Government, Australien Institute of Family Studies.
Reigstad, B., Jorgensen, K., Sund, A. M., & Wichstrom, L. (2006). Adolescents referred to specialty mental health care from local services and adolescents who remain in local treatment: What differs? Social Psychiatry and Psychiatric Epidemiology, 41(4), 323–331. doi:10.1007/s00127-005-0027-x.
Tamplin, A., Goodyer, I. M., & Herbert, J. (1998). Family functioning and parent general health in families of adolescents with major depressive disorder. Journal of Affective Disorders, 48(1), 1–13. doi:10.1016/s0165-0327(97)00105-5.
Stein, D., Williamson, D. E., Birmaher, B., Brent, D. A., Kaufman, J., Dahl, R. E., et al. (2000). Parent–child bonding and family functioning in depressed children and children at high risk and low risk for future depression. Journal of the American Academy of Child and Adolescent Psychiatry, 39(11), 1387–1395. doi:10.1097/00004583-200011000-00013.
Schei, J., Jozefiak, T., Novik, T. S., Lydersen, S., & Indredavik, M. S. (2013). The impact of coexisting emotional and conduct problems on family functioning and quality of life among adolescents with ADHD. J Atten Disord,. doi:10.1177/1087054713507976.
Ranøyen, I., Klöckner, C., Wallander, J., & Jozefiak, T. (2014). Associations between internalizing problems in adolescent daughters versus sons and mental health problems in mothers versus fathers (the HUNT study). Journal of Child and Family Studies,. doi:10.1007/s10826-014-0001-x.
Tamplin, A., & Goodyer, I. M. (2001). Family functioning in adolescents at high and low risk for major depressive disorder. European Child and Adolescent Psychiatry, 10(3), 170–179.
von Soest, T., Mossige, S., Stefansen, K., & Hjemdal, O. (2010). A validation study of the resilience scale for adolescents (READ). Journal of Psychopathology and Behavioral Assessment, 32(2), 215–225. doi:10.1007/s10862-009-9149-x.
Henderson, A. D., Sayger, T. V., & Home, A. M. (2003). Mothers and sons: A look at the relationship between child behavior problems, marital satisfaction, maternal depression, and family cohesion. The Family Journal,. doi:10.1177/1066480702238469.
Crea, T. M., Chan, K., & Barth, R. P. (2014). Family environment and attention-deficit/hyperactivity disorder in adopted children: Associations with family cohesion and adaptability. Child: Care, Health and Development, 40(6), 853–862. doi:10.1111/cch.12112.
Jozefiak, T., Larsson, B., & Wichstrom, L. (2009). Changes in quality of life among Norwegian school children: A six-month follow-up study. Health Qual Life Outcomes, 7, 7. doi:10.1186/1477-7525-7-7.
Jozefiak, T., Larsson, B., Wichstrom, L., Mattejat, F., & Ravens-Sieberer, U. (2008). Quality of life as reported by school children and their parents: A cross-sectional survey. Health Qual Life Outcomes, 6, 34. doi:10.1186/1477-7525-6-34.
Hollinghead, A. B. (1958). Two factor index of social position. New Heaven, CT: Yale University.
Achenbach, T. M., & Rescorla, L. (2001). Manual for the ASEBA school-age forms & profiles (p. 238). Burlington: ASEBA.
Novik, T. S. (1999). Validity of the child behaviour checklist in a Norwegian sample. European Child and Adolescent Psychiatry, 8(4), 247–254.
Jozefiak, T., Larsson, B., Wichstrom, L., & Rimehaug, T. (2012). Competence and emotional/behavioural problems in 7-16-year-old Norwegian school children as reported by parents. Nordic Journal of Psychiatry, 66(5), 311–319. doi:10.3109/08039488.2011.638934.
Mattejat, F., & Remschmidt, H. (2006). ILK - Inventar zur Erfassung der Lebensqualität bei Kindern und Jugendlichen. Bern: Verlag Hans Huber, Hogrefwe AG.
Jozefiak, T., Mattejat, F., & Remschmidt, H. (2012). Inventory of life quality in children and adolescents manual, Norwegian version. Stockholm: Hogrefe.
Epstein, N. B., Baldwin, Lawrence M., & Bishop, Duane S. (1983). The McMaster family assessment divice. Journal of Marital and Family Therapy, 9(2), 9.
Byles, J., Byrne, C., Boyle, M. H., & Offord, D. R. (1988). Ontario child health study: Reliability and validity of the general functioning subscale of the McMaster family assessment device. Family Process, 27(1), 97–104.
Ryan, C. E., Epstein, N. B., Keitner, G. I., Miller, I. W., & Bishop, D. S. (2005). Evaluating and treating families: The McMaster approach. London: Routledge, Taylor & Francis Group.
Raykov, T., & Marcoulides, G. A. (2006). Model-testing and fit evaluation. A first course in structural equation modeling (2nd ed.). New Jersey: Lawrence Erlbaum Associates.
Muthén, L. K., & Muthén, B. O. (1998–2012). Mplus User’s Guide (Seventh ed.). Los Angeles, CA: Muthén & Muthén.
Ravens-Sieberer, U., & Bullinger, M. (2000). KINDL-R. Questionnaire for measuring health-related quality of life in children and adolescents - Revised version 2000. http://www.kindl.org.
Richmond, M. K., & Stocker, C. M. (2006). Associations between family cohesion and adolescent siblings’ externalizing behavior. Journal of Family Psychology, 20(4), 663–669. doi:10.1037/0893-3200.20.4.663.
White, R., & Renk, K. (2012). Externalizing behavior problems during adolescence: An ecological perspective. Journal of Child and Family Studies, 21(1), 158–171. doi:10.1007/s10826-011-9459-y.
Lubenko, J., & Sebre, S. (2010). Longitudinal associations between adolescent behaviour problems and perceived family relationships. Wcpcg, 2010(5), 785–790. doi:10.1016/j.sbspro.2010.07.185.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27. doi:10.1007/s10567-010-0080-1.
Lewinsohn, P. M., Redner, J., & Seeley, J. (1991). The relationship between life satisfaction and psychosocial variables: New perspectives. In M. A. F. Strack & N. Schwarz (Eds.), Subjective well-being: An interdisciplinary perspective (pp. 141–169). Oxford: Pergamon Press.
Ballash, N., Leyfer, O., Buckley, A. F., & Woodruff-Borden, J. (2006). Parental control in the etiology of anxiety. Clinical Child and Family Psychology Review, 9(2), 113–133. doi:10.1007/s10567-006-0007-z.
Henggeler, S. W., Schoenwald, S. K., Borduin, C. M., Rowland, M. D., & Cunningham, P. B. (1998). Multisystemic treatment of antisocial behavior in children and adolescents. New York: Guilford Press.
Hollenstein, T., & Lougheed, J. P. (2013). Beyond storm and stress: Typicality, transactions, timing, and temperament to account for adolescent change. American Psychologist, 68(6), 444–454. doi:10.1037/a0033586.
Arnett, J. J. (1999). Adolescent storm and stress, reconsidered. American Psychologist, 54(5), 317–326.
Acknowledgments
Funding
This study was funded by the Norwegian National Council of Mental Health/EXTRA.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest. The first author receives royalities from publisher Hogrefe/Psykologiförlag Stockholm for authorship of the "Norwegian Manual - ILC QoL measure, 2012" which is used in this study.
Informed consent
All adolescents and parents who participated gave their written informed consent. This study was approved by the Regional Commitee for Medical Research Ethics in Central Norway. The procedures in this study were in accordance with the 1964 Declaration of Helsinki and its later amendments.
Rights and permissions
About this article

Cite this article
Jozefiak, T., Wallander, J.L. Perceived family functioning, adolescent psychopathology and quality of life in the general population: a 6-month follow-up study. Qual Life Res 25, 959–967 (2016). https://doi.org/10.1007/s11136-015-1138-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-015-1138-9