
Abstract
Background
The study investigates whether adolescents referred to specialty mental health services from local services differ from adolescents who only have received help for psychiatric problems locally. If so, which factors associate strongest with referral?
Method
Adolescents (n = 76) from an adolescent population sample (N = 2,538) who had received help during the last year for mental problems from local services were compared to a clinical sample of adolescents (N = 129) referred to specialty mental health services from such local services. Comparisons were made according to scores on the Youth Self-Report (YSR); depressive symptoms; family functioning; attachment to parents; self-concept; coping styles; response styles; dysfunctional attitudes; negative life events; daily hassles; socio-demographics.
Results
As compared to adolescents receiving help locally, adolescents in specialty mental health care scored higher on YSR internalising syndrome; YSR attention problems; YSR thought problems; suicidality; psychosocial stressors; knowing someone who had attempted suicide; parental divorce; substance use; recent moves; living in lodgings; lost a pal or boy/girlfriend; and lower on attachment to parents. Multivariate logistic regression analysis identified four factors associated with receiving specialty mental health care: low family functioning; moved previous year; knowing someone who had attempted suicide; own suicidality.
Conclusions
Family functioning as reported by the adolescents, and not mental health problems except for suicidality, was found to be the strongest associated with referral to specialty mental health services. Contrary to findings from many other studies, referral was associated with internalising problems, not externalising ones.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The prevalence of any DSM disorder among children and adolescents in the community is high, varying from 17% to 25% [1–11]. A significant proportion of such psychopathology in the community is unrecognised and untreated [1, 5, 9, 11, 12]. Zwaanswijk et al. [13] found in that 3.1% of a Dutch general population sample of adolescents had been referred for mental health services in the preceding year. Furthermore, among adolescents who scored in the borderline/clinical range of the Youth Self-Report (YSR) total score [14], and were thus at risk for psychopathology, only 7.7% had been referred for mental health services. Sourander et al. [15] reported that 7% of a Finnish child and adolescent community sample had been in contact with some kind of child mental health services during an 8-year follow-up. Only 13% of the adolescents within the deviant range of the YSR total score in their study had used child mental health services. Thus only a small proportion of children who have mental health problems are referred for treatment, and it may be unclear why some disturbed children are brought for treatment and others are not. Costello and Janiszewski [16] found no difference in the proportions receiving a psychiatric diagnosis between groups of treated and untreated children 7 through 11 years of age, and all of whom scored in the clinical range on the Child Behavior Checklist (CBCL).
Factors associated with selection to mental health services
The strongest correlate of specialty mental health care seems to be the effect of children’s symptoms on their parents [17]. Cohen et al. [18] found the specific diagnoses most associated with treatment seeking to be conduct disorder and oppositional/defiant disorder. Children’s internalising problems such as depression and anxiety appear to be associated with fewer burdens to others than other diagnoses, and children with depressive disorders have previously been found to be less likely to receive specialty mental health services [2, 17, 19]. However, self-reports of depression are higher than others’ report, and children’s own perception of the need for professional help is more related to depression than to disruptive disorders [19, 20]. Depressive problems in preadolescence tend to be underestimated by parents compared with teachers, and teachers’ evaluation of the child’s needs is among the best ors for referral [15, 21]. Thus professionals may be better at detecting internalising problems than parents, and hence to a greater extent refer children to psychiatric services for such problems. Internalising as well as externalising problems have been found to contribute to service use in the Netherlands [11] and in Finland [15], although the effect of externalising problems was the stronger one.
A range of other factors than psychiatric symptoms have been found to affect child psychiatric service utilisation as well: age [22, 23], gender [23, 24], family stress [11], family socio-economic status [22, 25, 26], parental use of mental health services [25, 26], and perceived parental burden [3, 17, 25]. These differences almost exclusively pertain to differences between child and adolescent psychiatric patients and the rest of the child and adolescent population. When a psychiatric problem is acknowledged, local treatment will be an option or it has already been tried. However, we know little about patients treated locally.
Child and adolescent psychiatry in Norway is defined as a second line service that receives referrals from the first line local services like GP’s, pre-school and school health services, school services, and child protective services. In 2001, in Norway, there were 68 outpatient county-based specialty mental health care clinics for children and adolescents with 934 professionals. The clinics are supposed to give general service. First line local somatic health care referred 55% of all cases to these clinics in 2001, school services 15.6%, social services 13%, other health care 10.2%, and patient or family 5.1%. Patients from all clinics in Norway are registered in a national database. This is a mandatory registration, and reimbursement to the clinics from the government is based on this registration. Mental health problems of moderate severity are expected to be treated in the first line services at a local level, whereas more serious problems will usually be referred to second line specialty mental health care.
Research aims
At present we know very little about children who are treated locally and children who are referred to specialty mental health care. We ask if there are differences between adolescents in a population sample having received local help for mental problems the previous year and adolescents in clinical specialty mental health care with respect to: demographics (gender, parental divorce and parental education); psychiatric symptoms and psychosocial problems (psychiatric symptoms, deliberate self-harm, suicide attempt, truancy, pain, alcohol and substance use); family (attachment and family functioning); psychological factors (self-concept, cognitive styles and coping styles); and stress (life events and daily hassles). Which factors would associate strongest with referral to specialty mental health care?
Subject and methods
Sample
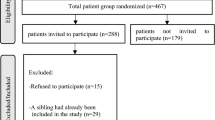
A representative clinical child psychiatric sample of 129 adolescents from all 9 outpatient clinics in Nordland County was compared with a representative community sample of 2,465 adolescents from the neighbouring counties of North Trøndelag and South Trøndelag. The clinical sample was drawn from specialty mental health care in Nordland County because no such sample was available in the counties of Trøndelag. The clinical sample and the population sample completed identical measures. The Regional Ethical Committees and the Norwegian Data Inspectorate approved the study of both samples. Informed written consent was obtained, and confidentiality was guaranteed.
The clinical sample
Nordland County is served by 9 child and adolescent psychiatric clinics. These are general service clinics. No differences in diagnoses or in reasons for referral between patients from Nordland (N = 685) and patients from the rest of Norway (N = 6,692) were detected. However, patients referred in the Nordland County were 14 days older than patients residing in the rest of Norway (t = 2.54, P < .05), and were somewhat more often girls (61.4% vs. 55.2%; χ2 = .002). The clinical sample (n = 129) consisted of outpatients aged 12–18 from June 2000 through 2001 recruited consecutively. Comparisons were made with those in Nordland County who did not participate with respect to gender, age, referral problems, and diagnoses. The sample was representative with respect to referral problems and diagnoses. No ICD-10 axis 1 diagnostic category occurred at different rates in these two groups. The largest diagnostic categories in the clinical sample were F32 Depressive episode (17.9%), F43 Reaction to stress, and adjustment disorders (22.5%), F90 Hyperkinetic disorders (5.5%), F91 Conduct disorders (3.1%), F92 Mixed disorders of conduct and emotions (2.4%), and F93 Emotional disorders with onset specific to childhood (5.6%). However, the study sample was slightly older (15.3 years vs. 14.8 years) and contained more girls (70.5% vs. 60.4%) than those who did not participate (both P = .04). Age and gender will, however, be correlated in a clinical population. In the total sample of 12–18 olds, girls were older when they were referred to child and adolescent psychiatry as compared to boys (15.1 years vs. 14.6 years). Information about referral problems and diagnoses were collected from the patient’s medical notes. The adolescents filled in the questionnaire alone at the clinic they were attending, but had the possibility to ask for assistance if they needed. The adolescents then put the questionnaire in an envelope and sealed it themselves.
The community sample
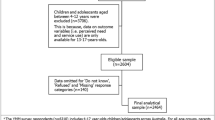
The community sample stems from a representative sample of 2,465 adolescents attending 22 private or public schools during 1999 in the two Norwegian counties of South- and North-Trøndelag (Total population, N = 9,292) (second wave of data collection in the “Youth and Mental Health Study”). The sample was stratified according to urbanity and geography. Details of the sampling procedure are reported elsewhere [27]. The two counties neighbour the county of Nordland. Cumulative participation rate was 84.5%. Almost none were out of school. Around 50.5% were girls and 49.5% boys. Schools were drawn with a probability according to size (proportional allocation). Mean age was 15.0 years (range 13.8–16.9, SD = 0.58).
The adolescents completed questionnaires at school in 1999. The adolescents answered the question whether they had received help for mental problems during the previous 12 months (Yes/No), and from whom. First line local services include GP’s, health nurses, school consultants, guidance counsellors, and others. The overwhelming majority of psychologist and psychiatrist in contact with adolescents will work in the second line specialty mental health services. Adolescents indicating psychologists or psychiatrists were excluded because these adolescents most likely had been in contact with these professionals in the second line specialty mental health services. This group was not analysed further because we did not know if it was representative. We did not amalgamate these two population sample groups because we wanted to have a “clean” group of adolescents who had received local help only. The adolescents who received help locally for mental problems were considered eligible to become cases, but we do not know about the possible later referrals to second line mental health services. The first line local and the second line clinical sample differed slightly in age (t = 2.76, P < .01), but not in gender.
Instruments
Symptoms
The YSR, which is the adolescent version of the CBCL [14], measures a variety of psychiatric symptoms. Several studies have shown significant associations between DSM diagnoses and CBCL scores as well as YSR scores [28–33]. The deviant range of the YSR scores is defined as a 60 t-score cut off for the YSR total, the YSR internalised, and the YSR externalised scores. The rest of the YSR dimensional scores have a 67 t-score cut off [14].
The Mood and Feelings Questionnaire (MFQ) is a measure of depressive symptoms in children and adolescents [34]. The MFQ has been useful in discriminating depressed and non-depressed clinical cases, and to persistence of major depression in clinical samples [35, 36]. A cut-off score of 27 was suggested by Wood et al. [37] from analysis of a clinical sample, and will be used in the present study.
The adolescents were asked if they ever had taken an overdose or otherwise tried to harm themselves (“Yes, several times”, “Once”, “no”). After this gateway question they were asked if they ever had tried to kill themselves (same options). Frequency of pains in various locations (head, arms and legs, stomach, back) was recorded.
Substance use
Frequency of smoking, cannabis use, solvents, and hard drugs were recorded for the previous 12 months, and the adolescents were asked how often they had drunk so much that they felt clearly intoxicated during the previous 12 months.
Socio-demographics and family functioning
The adolescents were asked to indicate the civil status of their parents and their educational level. Overall family functioning was measured by the general functioning part of the Family Assessment Device (FAD) [38]. Attachment to each parent was measured by the Inventory of Parent and Peer Attachment (IPPA) [39].
Psychological factors
Cognitive vulnerability to depression was measured by a short version of the Dysfunctional Attitudes Scale (DAS) [40] developed by Lewinsohn and coworkers [41]. Coping with stress was measured by 17 items from the Coping Inventory for Stressful Situations (CISS) [42]. CISS assesses three coping styles: Task-oriented, Emotion-oriented, and Avoidance-oriented coping. A shortened version of the Response Styles Questionnaire [43] measuring Rumination, Distraction, and Problem-solving was used. An abbreviation of the Self-consciousness scale [44] suggested by Andrews et al. [41] was applied. The Social acceptance, Physical appearance, and Global self-worth sub-scales of a revised version of the Self-perception profile for adolescents [45, 46] were included.
Stressors
Life-events were recorded by the Early Adolescent Stress Questionnaire (EASQ) [45]. EASQ is a 37-item measure that captures both stressful life events and chronic stressors during the preceding 12 months salient for the early adolescence period in the family, school and peer areas. Daily Hassles were recorded by a 9-item measure, capturing the occurrence of irritating, unpleasant or disappointing events of importance for young adolescents during the preceding month [45].
High scores on these instruments indicate high levels of problems, with the exception of IPPA where high scores indicate high levels of attachment. Adolescents in the population sample having received specialty mental health services were excluded (N = 69).
Statistics
Differences between the clinical sample and those receiving local help only were analysed with logistic regression and t-test. In search for multivariate potential correlates of referral to specialty mental health care, stepwise multivariate logistic regression was used. Since we had no strong argument for the primacy of particular variables, ors were entered into the model according to their L.R. Chi-sq. Since there was a slight difference in the age distribution between samples, age was controlled.
Results
In the population sample 5.3% (n = 135) reported to have received help for mental problems during the last year and 76 of those (27 boys and 49 girls) reported to have received local help only. Hence, about 2.6% could have received help from specialty mental health services. No significant gender difference was found between those who had received local help (n = 76) and those from the neighbouring county who had received help from specialty mental health care (n = 129), but a significant difference was found with respect to age (t (df = 198) = 2.76, P < .01). The adolescents in specialty mental health care were somewhat older (15.6 years vs. 15.1 years).
Clinical, family, and socio-demographiccharacteristics
Fifteen percent (N = 330) of the total population sample and 57.3% (N = 71) of the clinical sample had YSR Total Problem scores within the deviant range (OR = 7.56, CI = 5.20–11.00, P < .001). Among adolescents in the population sample with such high scores 86.1% reported not to have received help for mental problems during the previous year.
MFQ scores in the deviant range (scores of 27 or higher) were obtained by 7.5% (N = 177) in the population sample, and by 46.0% (n = 58) in the clinical sample (OR = 10.49, CI 7.16–15.38, P < .001). The percentage of adolescents with high MFQ scores in the population sample that had not received help was 82.8.
Table 1 presents differences between those who had received help from local services only and those who had received help from specialty mental health care with respect to categorical risk factors such as demographic variables, pain, alcohol and substance use. Strongest differences were observed regarding living in lodgings, suicide attempts, overdose/deliberate self-harm, having moved last year, knowing someone who had tried to commit suicide, use of cannabis, and lost a friend or girl/boy friend last year. Less strong differences were found with respect to daily smoking, parental divorce, having had serious quarrels with parents, and pains.
Table 2 shows differences according to continuous measures: family functioning, attachment, cognitive styles, stresses, depression, and with scores on the MFQ, and YSR. Strongest differences were found on the FAD, on the MFQ, and scores on the YSR total. Moreover, adolescents in specialty mental health care experienced more stress and daily hassles, ruminated more, and had higher scores on YSR anxious/depressed, internalising, withdrawn, thought problems, and attention problems, respectively than adolescents who had received local help only. They also had poorer attachment to father, and also to mother, and friends.
Multivariate analysis
A stepwise logistic analysis (Table 3) identified four risk variables increasing the likelihood for referrals from local mental health services to adolescent specialty mental health services: family functioning as assessed by FAD, having moved last year, overdose or self-harm more than once, and knowing someone who have tried to commit suicide. None of the YSR scales correlated with referral to specialty mental health services, which also was the case with scores on the MFQ scale.
Discussion
In this study we found that a total of 5.3% of the Norwegian adolescents in the population sample reported to have received help for mental problems during the last year, whereof 56.3% reported to have received help from local services only. It is not surprising that adolescents referred to specialty mental health services are found to have higher levels of psychopathology than those treated locally. It may, however, be surprising that other factors than psychopathology increased most strongly the risk for referral except for suicidality. In the final multivariate analysis, those who had been referred from local services to specialty mental health services had poorer family functioning, they had moved more often, they knew more often someone who had attempted suicide, and they had higher rates of own self-harm compared to those who had received local help only.
Referrals to specialty mental health care
The proportion of adolescents who had received professional help for mental problems was somewhat lower than the 7% reported by Sourander et al. [15]. About 2.6% of the population sample provided responses indicating that they had received help from specialty mental health services. This figure is somewhat higher than the official 1.6% of the population aged 0–18 in these two counties that received help from these services in 1999 [47]. However, the rate of referral increases with age [48], and a larger proportion of adolescents are therefore expected to be referred than 0- to 18-year-olds. Hence, these figures indicate support to our data. Zwaanswijk et al. [13] reported that 3.1% of a Dutch sample was referred to specialty mental health services. Sayal [49] found in a prospective longitudinal study of children in a community based sample in the UK that 5.1% were referred to specialty mental health services over 4 years. In the longitudinal Great Smoky Mountains Study 7% of a community sample of children and adolescents, overall, in any year, used specialty mental health services [50]. Discrepancies between figures should be expected due to differences in the prevalence of problems, in the organising of mental health services, and in the availability of such services in different countries.
Problem severity
Not unexpectedly was suicidality associated with specialty mental health service use, as was self-harm in the final multivariate analysis. These behaviours are often defined as emergency referrals to specialty mental health services. We found that 15% of the adolescents in the total population sample scored within the deviant range on the YSR Total Problem scale, and that 86.1% of these reported not to have received any professional help for mental problems during the last year. This figure is almost identical with the 87% reported by Sourander et al. [15] and close to the 92.3% reported by Zwaanswijck et al. [13]. In the Great Smoky Mountains Study 21.1% of youths aged 9–17 years had one or more DSM-IV psychiatric disorders [3]. Our results thus confirm that the overwhelming majority of adolescents with serious mental problems do not get professional help, at least in a fairly recent time perspective. However, in our clinical sample 57.3% scored in the deviant range on the YSR Total Problems scale. Zwaanswijk et al. [13] report that 45% of the adolescents referred for specialty mental health services in a Dutch sample scored in the deviant range on the YSR Total Problems scale. It may thus seem that Norwegian adolescents referred to such services report somewhat more problems compared with Dutch adolescents.
Family burden
Poor family functioning was most strongly associated with referral in the final multivariate analysis in the present study. Other studies lend support to this result. Angold et al. [3] found the most critical issue for referrals of youth aged 9–17 years to be the impact of the child’s psychiatric problems as reported by the parents on the family’s income and the parents’ lives, whether through psychological strain or by disruption of relationships with family or friends. Family burden has also in other studies been found to be a main predictor of referrals of adolescents [13, 51]. Conversely, in a study of referred children aged 5–11 years and parental burden symptom severity was found to be the best predictor of referrals to specialty child mental health services [49]. However, the family impact of adolescent problems may be experienced differently and more strongly than the impact of child problems. Local services are the one who can refer to specialty mental health care in Norway. Possibly, such professionals detect depression more often than parents, and thus they may be more inclined to refer due to such problems. However, finding also the adolescents experience of family dysfunction to be the strongest correlate to referral to specialty mental health services in the present study, underline the importance of family functioning in the process leading to a referral. The significance of family factors is underscored by the fact that the adolescents’ attachment to the parents, and especially to the father, was significantly correlated to referral, as was parental divorce. Relationship with the father is found to be associated with depression among girls from divorced families [52].
Stressors and related factors
A strong relationship was found in the final model between having moved last year and referrals to specialty mental health services. Number of moves, however, was not significantly associated. A number of changes the previous year having moved, living in lodgings, having lost a pal or girl/boy friend differentiated those received help from specialty mental health services from those who had got local help. Such changes may imply a weakening of social support when faced with other negative life events or when facing mental health problems, and may be factors on the causal pathway to referral. A working social network has an important preventive function related to coping with stressful life events [53]. This lack of social support may increase the likelihood of local services to refer the adolescent further in the treatment line. Stressful life events and daily hassles were also associated with referrals. This may not be true associations as they were not independent relationships to referral, but the results are in line with the findings in a review article of 500 studies where Grant et al. [54] concluded that results overall suggest that stressors predict changes in rates of symptoms of psychopathology in children and adolescents over time. Daily smoking as well as use of cannabis was correlated with specialty mental health service use. Correspondingly, other studies on adolescents have found cannabis use to correlate with increased rates of serious adjustment problems [55], and cigarette smoking with elevated depressive symptoms especially in females [56, 57].
Depression
Importantly, internalising problems in general, and depression in particular, were more frequent among those referred to specialty mental health services as compared to those who received local help, whereas this was not the case for externalising problems. This finding could be seen as contrary to findings in other studies where youths with depressive disorders were less likely to receive specialty mental health services, possibly because the family burden associated with internalising problems are less than the burden of externalising behaviours [2, 17, 58]. Our results could indicate a lower threshold for referrals of internalising problems than externalising problems to the specialty mental health services for adolescents in Norway. On the other side, those participating in the clinical sample were somewhat more likely to be a girl and older than those not participating. Although age and gender will be correlated among patients, this could have resulted in overestimation of the prevalence of internalising behaviour. Importantly, those participating were not more likely to have been referred for internalising problems or to receive an axis 1 diagnosis of an internalising type. This differential attrition therefore most likely did not affect the overall results from this study. Our findings harmonise with a strong increase in referrals to specialty mental health care for sadness/depression in Norway during the last decade [48].
Coping with depression
None of the psychological variables were included in the final model in the present study. Psychological variables did not distinguish the two groups except for ruminative and emotion-oriented coping. Rumination as a response style has been found to correlate with depression and predict future depression [59, 60], and possibly mixed anxiety/depressive symptoms in particular [43]. Correspondingly, emotion-oriented coping is a coping strategy in stressful situations that is less adaptive and found to associate with depression [61]. The preponderance of these coping styles in the clinical sample may make these adolescents more vulnerable to the development of depression. In the present study the clinical sample scored higher on the YSR, and particularly so on anxiety/depression—and on the MFQ than adolescents receiving help locally. Problem scores in the deviant range on the YSR are correlated to DSM diagnoses [28, 30], and can thus be seen as indicators of psychopathology. The MFQ have furthermore been found to correlate with major depression [36]. However, neither YSR nor MFQ scores were multivariately associated with specialty mental health services use.
Limitations
Although the present study has many strengths, among them a large probability sample with favourable response rate and a long range of potential discriminators of different help-seeking groups, there are several limitations to be acknowledged. Firstly, the clinical sample was not completely representative of all adolescents referred to specialty mental health care. The patients were somewhat more likely to be a girl and older than those not participating.
In a similar vein, the differential attrition in the population sample may have resulted in underestimation of adolescents receiving help for mental problems, and in particular among those with externalising problems (for differential attrition in population samples in Norway see [58]). However, underrepresentation of externalising problems would also most likely be the case in the clinical sample as well, resulting in lesser problems when these two samples were compared.
Conclusions
The results in this study correspond to the findings of Angold et al. [3] where psychiatric diagnoses as reflected in the DSM-IV system did not increase the risk for specialty mental health services once their impact on parents was controlled. Family functioning as reported by the adolescents, and not mental health problems except for suicidality, was found to be the strongest correlate to referral to specialty mental health services.
References
Almqvist F, Puura K, Kumpulainen K, Tuompo-Johansson E, Henttonen I, Huikko E, Linna S, Ikaheimo K, Aronen E, Katainen S, Piha J, Moilanen I (1987) Psychiatric disorders in 8–9-year-old children based on a diagnostic interview with the parents. Eur Child Adolesc Psychiatry 1999 8(Suppl 4):17–28
Anderson JC, Williams S, McGee R, Silva PA (1987) DSM-III disorders in preadolescent children. Prevalence in a large sample from the general population. Arch Gen Psychiatry 44(1):69–76
Angold A, Erkanli A, Farmer EM, Fairbank JA, Burns BJ, Keeler G, Costello EJ (2002) Psychiatric disorder, impairment, and service use in rural African American and white youth. Arch Gen Psychiatry 59(10):893–901
Costello EJ, Angold A, Burns BJ, Stangl DK, Tweed DL, Erkanli A, Worthman CM (1996) The Great Smoky Mountains Study of Youth. Goals, design, methods, and the prevalence of DSM-III-R disorders. Arch Gen Psychiatry 53(12):1129–1136
Fergusson DM, Horwood LJ, Lynskey MT (1993) Prevalence and comorbidity of DSM-III-R diagnoses in a birth cohort of 15 year olds. J Am Acad Child Adolesc Psychiatry 32(6):1127–1134
Kroes M, Kalff AC, Kessels AG, Steyaert J, Feron FJ, van Someren AJ, Hurks PP, Hendriksen JG, van Zeben TM, Rozendaal N, Crolla IF, Troost J, Jolles J, Vles JS (2001) Child psychiatric diagnoses in a population of Dutch schoolchildren aged 6 to 8 years. J Am Acad Child Adolesc Psychiatry 40(12):1401–1409
Lavik NJ (1976) Ungdoms mentale helse. Universitetsforlaget, Oslo
McGee R, Feehan M, Williams S, Partridge F, Silva PA, Kelly J (1990) DSM-III disorders in a large sample of adolescents. J Am Acad Child Adolesc Psychiatry 29(4):611–619
Offord DR, Boyle MH, Fleming JE, Blum HM, Grant NI (1989) Ontario Child Health Study. Summary of selected results. Can J Psychiatry 34(6):483–491
Verhulst FC, Berden GF, Sanders-Woudstra JA (1985) Mental health in Dutch children: (II). The prevalence of psychiatric disorder and relationship between measures. Acta Psychiatr Scand Suppl 324:1–45
Verhulst FC, van der Ende J (1997) Factors associated with child mental health service use in the community. J Am Acad Child Adolesc Psychiatry 36(7):901–909
Costello EJ (1989) Child psychiatric disorders and their correlates: a primary care pediatric sample. J Am Acad Child Adolesc Psychiatry 28(6):851–855
Zwaanswijk M, Van der Ende J, Verhaak PF, Bensing JM, Verhulst FC (2003) Factors associated with adolescent mental health service need and utilization. J Am Acad Child Adolesc Psychiatry 42(6):692–700
Achenbach TM (1991) Manual for the child behavior checklist/4–18 and 1991 profile. University of Vermont: Department of Psychiatry, Burlington
Sourander A, Helstela L, Ristkari T, Ikaheimo K, Helenius H, Piha J (2001) Child and adolescent mental health service use in Finland. Soc Psychiatry Psychiatr Epidemiol 36(6):294–298
Costello EJ, Janiszewski S (1990) Who gets treated? Factors associated with referral in children with psychiatric disorders. Acta Psychiatr Scand 81(6):523–529
Angold A, Messer SC, Stangl D, Farmer EM, Costello EJ, Burns BJ (1998) Perceived parental burden and service use for child and adolescent psychiatric disorders. Am J Public Health 88(1):75–80
Cohen P, Kasen S, Brook JS, Struening EL (1991) Diagnostic ors of treatment patterns in a cohort of adolescents. J Am Acad Child Adolesc Psychiatry 30(6):989–993
Wu P, Hoven CW, Bird HR et al (1999) Depressive and disruptive disorders and mental health service utilization in children and adolescents. J Am Acad Child Adolesc Psychiatry 38(9):1081–1090, discussion 1090–1092
Romano E, Tremblay RE, Vitaro F, Zoccolillo M, Pagani L (2001) Prevalence of psychiatric diagnoses and the role of perceived impairment: findings from an adolescent community sample. J Child Psychol Psychiatry 42(4):451–461
Mesman J, Koot HM (2000) Child-reported depression and anxiety in preadolescence: I. Associations with parent- and teacher-reported problems. J Am Acad Child Adolesc Psychiatry 39(11):1371–1378
Cohen P, Hesselbart CS (1993) Demographic factors in the use of children’s mental health services. Am J Public Health 83(1):49–52
Zahner GE, Daskalakis C (1997) Factors associated with mental health, general health, and school-based service use for child psychopathology. Am J Public Health 87(9):1440–1448
Goodman SH, Lahey BB, Fielding B, Dulcan M, Narrow W, Regier D (1997) Representativeness of clinical samples of youths with mental disorders: a preliminary population-based study. J Abnorm Psychol 106(1):3–14
Garralda ME, Bailey D (1988) Child and family factors associated with referral to child psychiatrists. Br J Psychiatry 153:81–89
John LH, Offord DR, Boyle MH, Racine YA (1995) Factors in use of mental health and social services by children 6–16 years old: findings from the Ontario Child Health Study. Am J Orthopsychiatry 65(1):76–86
Sund AM, Larsson B, Wichstrom L (2001) Depressive symptoms among young Norwegian adolescents as measured by the Mood and Feelings Questionnaire (MFQ). Eur J Child Adolesc Psychiatry 10:222–229
Edelbrock C, Costello AJ (1988) Convergence between statistically derived behavior problem syndromes and child psychiatric diagnoses. J Abnorm Child Psychol 16(2):219–231
Fisher PW, Shaffer D, Piacentini JC, Lapkin J, Kafantaris V, Leonard H, Herzog DB (1993) Sensitivity of the Diagnostic Interview Schedule for Children, 2nd edition (DISC-2.1) for specific diagnoses of children and adolescents. J Am Acad Child Adolesc Psychiatry 32(3):666–673
Kasius MC, Ferdinand RF, van den Berg H, Verhulst FC (1997) Associations between different diagnostic approaches for child and adolescent psychopathology. J Child Psychol Psychiatry 38(6):625–632
Kazdin AE, Heidish IE (1984) Convergence of clinically derived diagnoses and parent checklists among inpatient children. J Abnorm Child Psychol 12(3):421–435
Morgan CJ, Cauce AM (1999) ing DSM-III-R disorders from the youth self-report: analysis of data from a field study. J Am Acad Child Adolesc Psychiatry 38(10):1237–1245
Weinstein SR, Noam GG, Grimes K, Stone K, Schwab-Stone M (1990) Convergence of DSM-III diagnoses and self-reported symptoms in child and adolescent inpatients. J Am Acad Child Adolesc Psychiatry 29(4):627–634
Angold A (1989) Structured assessment of psychopathology in children and adolescents. In: Thompson C (ed) The instruments of psychiatric research. John Wiley, Chichester, pp271–304
Goodyer IM, Herbert J, Tamplin A, Secher SM (1997) Pearson J. Short-term outcome of major depression: II. Life events, family dysfunction, and friendship difficulties as ors of persistent disorder. J Am Acad Child Adolesc Psychiatry 36(4):474–480
Pellegrino JF, Singh NN, Carmanico SJ (1999) Concordance among three diagnostic procedures for identifying depression in children and adolescents. J Emotional Behav Disord 7:118–127
Wood A, Kroll L, Moore A, Harrington R (1995) Properties of the mood and feelings questionnaire in adolescent psychiatric outpatients: a research note. J Child Psychol Psychiatry 36(2):327–334
Byles J, Byrne C, Boyle MH, Offord DR (1988) Ontario Child Health Study: reliability and validity of the general functioning subscale of the McMaster Family Assessment Device. Fam Process 27(1):97–104
Armsden GC, Greenberg MT (1987) The inventory of parent and peer attachment: individual differences and their relationships to psychological well-being in adolescence. J Youth Adolesc 16:427–454
Weissman AN, Beck AT (1978) Development and validation of the Dysfunctional Attitude Scale
Andrews JA, Lewinsohn PM, Hops H, Roberts RE (1993) Psychometric properties of scales for the measurement of psychosocial variables associated with depression in adolescence. Psychol Rep 73:1019–1046
Endler NS, Parker JDA (1990) Multidimensional assessment of coping: a critical evaluation. J Personality Soc Psychol 58:844–854
Nolen-Hoeksema S (2000) The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J Abnorm Psychol 109(3):504–511
Fenigstein A, Scheier MF, Buss AH (1975) Public and private self-consciousness assessment and theory. J Consult Clin Psychol 43:522–527
Sund AM, Larsson B, Wichstrom L (2003) Psychosocial correlates of depressive symptoms among 12–14-year-old Norwegian adolescents. J Child Psychol Psychiatry 44(4):588–597
Wichstrom L (1995) Social, psychological and physical correlates of eating problems. A study of the general adolescent population in Norway. Psychol Med 25(3):567–579
Anderson HW, Halsteinli V (2000) Hvordan kan mål om 5 prosent nås? (How can the goal of 5 percent be met?). Hagen H. Psykiatritjenesten 1999 – omstilling og vekst (Psychiatric Services 1999 – Restructuring and Growth). Unimed NIS, SAMDATA/Kommuneforbundet, Trondheim, Norway, pp 85–94
Reigstad B, Jørgensen K, Wichstrøm L (2004) Changes in referrals to child and adolescents psychiatric services in Norway 1992–2001. Soc Psychiatry Psychiatr Epidemiol 39(10): 818–827
Sayal K (2004) The role of parental burden in child mental health service use: longitudinal study. J Am Acad Child Adolesc Psychiatry 43:1328–1333
Farmer EMZ, Burns BJ, Philips SD, Angold A, Costello EJ (2003) Pathways into and through mental health services for children and adolescence. Psychiatr Serv 54:60–66
Logan DE, King CA (2002) Parental identification of depression and mental health service use among depressed adolescents. J Am Acad Child Adolesc Psychiatry 41:296–304
Palosaari U, Aro H, Laippala P (1996) Parental divorce and depression in young adulthood: adolescents’ closeness to parents and self-esteem as mediating factor. Acta Psychiatr Scand 93(1):20–26
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS (1994) Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey 51:8–19
Grant KE, Compas BE, Thurm AE, McMahon SD, Gipson PY (2004) Stressors and child and adolescent psychopathology: measurement issues and prospective effect. J Clin Child Adolesc Psychol 33:412–425
Fergusson DM, Horwood LJ, Swain-Campbell N (2002) Cannabis use and psychosocial adjustment in adolescence and young adulthood. Addiction 97:1123–1135
Poulin C, Hand D, Boudreau B, Santor D (2005) Gender differences in the association between substance use and elevated depressive symptoms in a general adolescent population. Addiction 100:525–535
Steuber TL, Danner F (2006) Adolescent smoking and depression: which comes first? Addict Behav 44(1):69–76
Wichstrom L (2000) ors of adolescent suicide attempts: a nationally representative longitudinal study of Norwegian adolescents. J Am Acad Child Adolesc Psychiatry 39(5):603–610
Just N, Alloy LB (1997) The response styles theory of depression: tests and an extension of the theory. J Abnorm Psychol 106(2):221–229
Nolen-Hoeksema S (1991) Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol 100(4):569–582
McWilliams LA, Cox BJ, Enns MW (2003) Use of coping inventory for stressful situations in a clinically depressed sample: factor structure, personality correlates, and prediction of distress. J Clin Psychol 59:423–437
Acknowledgement
This study was funded with a grant from the Norwegian Research Council.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Reigstad, B., Jørgensen, K., Sund, A.M. et al. Adolescents referred to specialty mental health care from local services and adolescents who remain in local treatment: what differs?. Soc Psychiat Epidemiol 41, 323–331 (2006). https://doi.org/10.1007/s00127-005-0027-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-005-0027-x