
Abstract
Objective
The study aimed to examine the construct validity and reliability of the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF) according to both classical test and item response theories.
Method
The psychometric properties of the French version of this instrument were investigated in a cross-sectional, multicenter study. A total of 124 outpatients with a substance dependence diagnosis participated in the study. Psychometric evaluation included descriptive analysis, internal consistency, test–retest reliability, and validity. The dimensionality of the instrument was explored using a combination of the classical test, confirmatory factor analysis (CFA), and an item response theory analysis, the Person Separation Index (PSI), in a complementary manner.
Results
The results of the Q-LES-Q-SF revealed that the questionnaire was easy to administer and the acceptability was good. The internal consistency and the test–retest reliability were 0.9 and 0.88, respectively. All items were significantly correlated with the total score and the SF-12 used in the study. The CFA with one factor model was good, and for the unidimensional construct, the PSI was found to be 0.902.
Conclusion
The French version of the Q-LES-Q-SF yielded valid and reliable clinical assessments of the quality of life for future research and clinical practice involving French substance abusers. In response to recent questioning regarding the unidimensionality or bidimensionality of the instrument and according to the underlying theoretical unidimensional construct used for its development, this study suggests the Q-LES-Q-SF as a one-dimension questionnaire in French QoL studies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Background
Over the last few decades, there has been an increased interest in quality of life (QoL). The core features of the definition proposed by the quality of life working group of the World Health Organization (WHOQOL) are that QoL offers a subjective, patient-centered focus and that the concept draws on a number of domains in addition to physical and emotional well-being [1]. In contrast to QoL research on chronic illnesses, only limited attention was given to QoL in the field of drug abuse research until the 1990s; since then, the attention to QoL has grown rapidly [2]. This shift has occurred in parallel with the recognition that alcohol and other drug disorders are complex chronic diseases that affect the medical, psychological, and social domains [2, 3]. Therefore, the assessment of QoL in patients with substance misuse and the impact of treatment interventions on QoL are emerging as important issues in the field of drug abuse research [4]. Both generic and specific instruments are used to measure the QoL of drug users, but the use of generic instruments prevails while specific instruments provide additional information that is relevant to a particular group [5]. QoL instruments vary in structure and in the domains they explore, and they need to be feasible, valid, and sensitive to change [6]. The Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q) is increasingly used in psychiatric research because it emphasizes the subjective perspective of patients within the physical, psychological, and social domains [7, 8]. The Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF) was developed from the original long form and fully represents its concepts [9]. The Q-LES-Q-SF was proven to exhibit sound psychometric properties in the assessment of various groups of people with psychiatric illnesses, including adults with ADHD, generalized anxiety disorder or bipolar disorder [10, 11]. However, the measurement properties of the Q-LES-Q-SF have not been demonstrated in a sample of alcohol- or opiate-dependent adults. The main objective of this study was to establish the validity and reliability of the French version of the Q-LES-Q-SF among substance abusers. Although the most recent psychometric study of the Chinese version of the Q-LES-Q-SF called into question the unidimensionality of the instrument and proposed two dimensions, one psychosocial and the other physical, this study aimed to examine the construct validity and reliability of the Q-LES-Q-SF in a French sample of substance abusers, combining both the classical test and item response theories [12, 13].
Methods
Population and sample
The study was conducted at four French specialized addiction treatment centers in two French regions and included adult female and male outpatients who met the DSM IV criteria for alcohol or opiate dependence [14]. General exclusion criteria included a main diagnosis on axis I of the DSM IV other than substance dependence. Although patients with polydrug dependence were not excluded from the study, clinicians were asked to identify the addictive substance causing the most salient dependence. Patients were assigned to the alcoholic or the opiate group according the main dependence (alcohol or opiate) on axis I of DSM IV. The diagnosis was made by clinicians who were certified in addiction pathologies and familiar with the DSM IV.
Each potential patient was informed that willingness to participate in the study would not affect the treatment that was received. Informed consent for participation in the study was obtained from each patient. The study protocol was approved by the Institutional Review Board (Comité National Informatique et Liberté DR-2013-156), ensuring the confidentiality of the information.
Sample size
Among the analyses employed to assess validity (factorial analysis and correlations), structural analysis is the most demanding. Based on the various published recommendations for calculating the number of patients required, we selected ten patients (the largest estimate) per item, that is, a total of 140 patients for the 14-item scale used to measure the QoL enjoyment and satisfaction [15].
Data collection
Quality of life assessment
Eligible patients were administered two self-report instruments: the Q-LES-Q-SF and the SF-12.
The Q-LES-Q-SF is a self-report instrument comprising 16 items derived from the general activities scale of the original 93-item form [7]. For each patient, the 14 items evaluated satisfaction with his/her physical health, social relations, ability to function in daily life, ability to get around physically, mood, family relations, sexual drive and interest, ability to work on hobbies, work, leisure activities, economic status, household activities, living/housing situation, vision, and overall sense of well-being. The instrument also includes two additional items measuring satisfaction with medication and overall life satisfaction. Each of the 16 items is rated on a 5-point scale that indicates the degree of enjoyment or satisfaction experienced during the past week. The total score of items 1–14 is computed (ranging from 14 to 70) and expressed as a percentage (1–100) of the maximum total score. Higher scores on the Q-LES-Q-SF indicate greater contentment or satisfaction. The French translation of the original version was performed by J. Endicott. Participants completed the Q-LES-Q-SF for the first time and then completed the questionnaire for a second time as a retest between 2 and 4 weeks after the index visit.
Patients also completed version 1 of the SF-12 as a benchmark to compare against the Q-LES-Q-SF [16]. The SF-12 is a generic QoL instrument that includes a subset of 12 items from the SF-36 [16]. The SF-12 covers eight domains: physical functioning; role-physical, that is, role limitations due to physical problems; bodily pain; general health; vitality; social functioning; role-emotional, that is, role limitations due to emotional problems; and mental health. Information from all 12 items is used to construct the physical and mental component summary measures (PCS-12 and MCS-12, respectively). Higher summary scores (=100) indicate an improved QoL. Participants completed the SF-12 during the index visit.
Other data
Other data were collected in various fields deemed relevant: sociodemographics, psychiatry, and somatics. Therefore, the usual sociodemographic data collected included gender, age, marital status, and employment status. Psychiatric comorbidities, somatic comorbidities, and prior dependence history were assessed by the trained clinician, who completed a questionnaire used in routine clinical care.
Statistical analysis
A combination of the classical test and item response theories (CTT and IRT, respectively) was applied. The qualitative data were studied using chi-square tests. Quantitative data were analyzed using Student’s t test or variance analysis. Independent sample t tests were used to compare the Q-LES-Q-SF scores of alcohol and opiate users.
The statistical analyses were performed using SAS v9.3, RUMM2020 v4.1 software (Rumm Laboratory, Perth, Western Australia) and Mplus 6.12 (Muthén & Muthén, Los Angeles, CA, USA).
Classical test theory (CTT) analysis
Acceptability
The distribution of responses and missing data per item were studied to assess the acceptability of the questionnaire. Missing data should not exceed one-third of the unanswered items for an individual [17]. Furthermore, the mean and standard deviation of the responses to each item were calculated.
Construct validity
Because hypotheses on the expected construct already existed, the structural validity of the questionnaire was confirmed using confirmatory factor analysis (CFA) with categorical factor indicators and a robust weighted least squares estimator. Two CFA models that included one and two factors were used. The models were judged good if the root mean square error of approximation (RMSEA) < 0.08, comparative fit index (CFI) > 0.9, and Tucker–Lewis index (TLI) > 0.9 and excellent if RMSEA < 0.05, CFI > 0.95, and TLI > 0.95 [18, 19].
The internal consistency of Q-LES-Q-SF was assessed using Cronbach’s alpha coefficients and reflected the homogeneity of the items belonging to a given dimension [20]. Its value varies from 0 to 1, and the significance of internal consistency was classified as good from 0.80 to 0.89 and excellent if >0.90 [21].
All items should be correlated at a minimum of 0.4 to the total score corrected for overlap using Spearman’s correlation [22].
External construct validity is defined as the search for correlations between 2 or more instruments measuring the same concept [20]. The correlations between the Q-LES-Q-SF and the SF-12 were examined using Pearson’s correlation coefficients.
Reproducibility
Test–retest reliability of the Q-LES-Q-SF was evaluated using the intraclass correlation coefficient (ICC). Qualitative interpretations of the ICC were based on the recommended ranges: ICC < 0.40 was poor; 0.40–0.59 was fair; 0.60–0.74 was good; and 0.75–1 was excellent [23].
IRT analysis
Whereas CTT statistics depend on the items included in the test and the persons examined, the IRT item and person parameters are invariant, depending neither on the subset of items used nor on the distribution of latent traits in the population of respondents [24]. Rasch models are a modern psychometric method that transforms raw ordinal scores into interval-level measurements (expressed in logits). The Rasch model computes item difficulty (item θ measure) in relation to the ability of the person (person measure) by placing both on the same linear continuum. The model assumes unidimensionality (i.e., all items on a measure assess the same single construct of interest) and that the item and person parameters are independent of the sample or items used [25]. The IRT model (partial credit model, Rasch family model) was used to confirm unidimensionality. The Person Separation Index (PSI) was calculated for each factor as an indicator of the internal consistency reliability. PSI values of 0.90 or greater indicated excellent results, and individual item fit residual statistics were acceptable when the value ranged from −2.5 to 2.5 [26].
Results
Sociodemographic characteristics
Overall, 124 patients were included, with 83.3 % men and 16.7 % women. The participants were classified into two groups based on the substance use disorder. Their sociodemographic and clinical characteristics are presented in Table 1.
CTT analysis
Psychometric properties of items
Table 2 shows the distributional data of the Q-LES-Q-SF items. None of the subjects left more than one-third of the items unanswered.
Psychometric properties of the scale
The CFA with one factor model was found to have a 0.077 RMSEA [90 % CI (0.054–0.098)], a 0.968 CFI, and a 0.962 TLI, with loadings between 0.523 and 0.851. The CFA with two factors had a 0.076 RMSEA [90 % CI (0.054–0.098)], a 0.969 CFI, and a 0.963 TLI, with loadings between 0.525 and 0.870.
The internal consistency reliability of the scale was 0.90. The test–retest reliability was determined using data from 67 participants who were administered the Q-LES-Q-SF on two occasions. At 0.88, the intraindividual correlation coefficient was markedly high, showing good reproducibility.
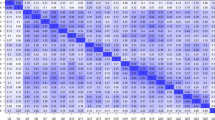
All items were significantly correlated to the total score, and the correlations ranged between 0.54 and 0.79 (Table 3). The latest uncommitted item on overall life satisfaction showed a correlation of 0.73 to the total. Finally, the Q-LES-Q-SF was correlated to the PCS-12, MCS-12, and SF-12 total score at values of 0.65, 0.74, and 0.77, respectively (Table 3).
Independent sample t tests were conducted to evaluate the hypothesis that there was a difference in the mean QoL Q-LES-Q-SF scores between alcohol and opiate substance users. Alcohol-dependent outpatients presented significantly higher scores than did opiate-dependent outpatients (p = 0.002). Patients with somatic or psychiatric comorbidities presented a poorer QoL than did those without comorbidities (52.6 vs 62.1; p = 0.01). Neither the duration of addiction nor gender was significantly related to the Q-LES-Q-SF score.
IRT analysis
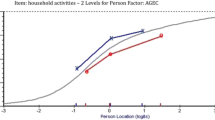
For the unidimensional construct, PSI was equal to 0.902, and the item residuals were between −2.5 and +2.5 with no statistical significance, indicating that the model was consistent with the theoretical model. The hierarchy of item difficulty ranged from the easiest item, “ability to get around physically without feeling” (indicating that this item was the easiest for patients to obtain a high score) to the hardest item, “economic status” (for which one patient had the greatest difficulty in obtaining a high score).
Discussion
This study aimed to describe the construct validity and reliability of the Q-LES-Q-SF in a French sample of substance abusers, combining the classical theory test and an item response theory model. According to the CFA, both the model with one dimension and the model with two dimensions are equally good. Therefore, the decision to use one or two dimensions should be based on the content of the questionnaire. As the underlying theoretical construct used for its development was unidimensional, it is reasonable to maintain that feature. To the best of our knowledge, the factor structure of the Q-LES-Q-SF using IRT has not previously been reported. The internal consistency of the French version of the Q-LES-Q-SF, as indicated by Cronbach’s alpha coefficient, was satisfactory, demonstrating that the instrument coherently investigates the QoL as measured by its items. All items correlated significantly to the total score, but the correlations varied among the items, indicating that some items might be more relevant than others in assessing QoL. The Q-LES-Q-SF test–retest reliability was high, implying its stability in repeated assessments. The convergent validity of the Q-LES-Q-SF with the SF-12 was in the expected direction, indicating that both QoL instruments are conceptually congruent. In this study, the use of the Q-LES-Q-SF allowed the detection of a significant difference in QoL score between alcohol and opiate users, whereas no significant difference was detected using the SF-12. This result suggests that the French version of the Q-LES-Q-SF constitutes a reliable research instrument for measuring QoL among French substance abusers.
Compared with validation studies of the Q-LES-Q-SF conducted in other countries, the following observations were made. The internal consistency reliability coefficient of the French version is similar to those of the original (0.90), Portuguese (0.90), Italian (0.92), and Serbian versions (0.90) [5, 7, 9, 27]. The test–retest reliability coefficient of the French version is similar to that of the Italian version (0.89) and highest for the Serbian Q-LES-Q-SF [9, 27]. French correlations between the SF-12 subscales with the overall Q-LES-Q-SF were higher than those in the Chinese version [13]. Differences in the characteristics of samples might explain some of the differences in the results from CTT analysis in validation studies.
As anticipated, psychiatric or somatic comorbidities were associated with a lower QoL, which is consistent with observations of those patients [4, 9]. Neither the duration of illness nor gender was significantly related to QoL among substance users of our sample according to a cohort of opiate-dependent patients and consistent with findings on patients with anxiety and affective disorders who were administered the Q-LES-Q-SF [4, 28]. Drawing comparisons with studies previously conducted among substance users is hindered by the fact that they used the Q-LES-Q, which includes eight summary scales that reflect satisfaction with physical health, subjective feelings, work, household duties, school, leisure activities, social relationships, and general activities [29–31].
This study had a limitation. As all patients were recruited through specialty treatment services, the sample could not be considered a reflection of patients with alcohol or opiate dependence in routine medical practice. If the study revealed that the measure could produce reliable and valid assessments of individuals, certain properties, such as responsiveness, were not determined and might be evaluated in a future study. It is relevant to note that the Q-LES-Q-SF appeared to discriminate QoL more precisely according the type of substance in this study than did the SF-12 although the latter instrument has been used in numerous studies of patients with alcohol or opiate dependence. Similarly, although the SF-12 and the original Q-LES-Q form have been used for longitudinal repeated measures in QoL assessments among substance abusers, future research might be based on the Q-LES-Q-SF, in particular using IRT, allowing an exploration of whether the answer to a questionnaire item could be influenced by patient characteristics.
In conclusion, in response to recent questioning on the unidimensionality or bidimensionality of the instrument and according to the underlying theoretical unidimensional construct used for its development, this study suggests the Q-LES-Q-SF as a one-dimension questionnaire in French QoL studies.
References
Hope, M., Page, A., & Hooke, G. (2009). The value of adding the Quality of Life Enjoyment and Satisfaction Questionnaire to outcome assessments of psychiatric inpatients with mood and affective disorders. Quality of Life Research, 18, 647–655.
De Maeyer, J., Vanderplasschen, W., & Broekaert, E. (2010). Quality of life among opiate-dependent individuals: A review of the literature. International Journal of Drug Policy, 21, 364–380.
Rudolf, H., & Watts, J. (2002). Quality of life in substance abuse and dependency. International Review of Psychiatry, 14(3), 190–197.
De Maeyer, J., Vanderplasschen, W., Lammertyn, J., Van Nieuwenhuizen, C., Sabbe, B., & Broekaert, E. (2011). Current quality of life and its determinants among opiate-dependent individuals five years after starting methadone treatment. Quality of Life Research, 20, 139–150.
Zubaran, C., & Foresti, K. (2009). Quality of life and substance use: Concepts and recent tendencies. Current Opinion in Psychiatry, 22(3), 281–286.
Luquiens, A., Reynaud, M., Falissard, B., & Aubin, H. J. (2012). Quality of life among alcohol-dependent patients: How satisfactory are the available instruments? A systematic review. Drug and Alcohol Dependence, 125, 192–202.
Endicott, J., Nee, J., Harrisson, J., & Blumenthal, R. (1993). Quality of life enjoyment and satisfaction questionnaire: A new measure. Psychopharmacology Bulletin, 29, 321–326.
Ritsner, M., Kurs, R., Kostizky, H., Ponizovsky, A., & Modai, I. (2002). Subjective quality of life in severely mentally ill patients: A comparison of two instruments. Quality of Life Research, 11(6), 553–561.
Stevanovic, D. (2011). Quality of Life Enjoyment and Satisfaction Questionnaire-short form for quality of life assessments in clinical practice: A psychometric study. Journal of Psychiatric and Mental Health Nursing, 18, 747–750.
Mick, E., Faraone, S., Spencer, T., Zhang, H., & Biederman, J. (2008). Assessing the validity of the quality of life enjoyment and satisfaction questionnaire-short form in adults with ADHD. Journal of attention disorders, 11, 504–509.
Wyrwich, K., Harnam, N., Revicki, A., Locklear, J., Svedsater, H., & Endicott, J. (2011). Assessment of Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form responder thresholds in generalized anxiety disorder and bipolar disorder studies. International Clinical Psychopharmacology, 26(3), 121–129.
Stevanovic, D. (2014). Is the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF) a unidimensional or bidimensional instrument? Quality of Life Research, 23(4), 1299–1300.
Lee, Y. T., Liu, S. I., Huang, H. C., Sun, F. J., Huang, C. R., & Yeung, A. (2014). Validity and reliability of the Chinese version of the Short Form of Quality of life Enjoyment and Satisfaction Questionnaire (Q-LES-Q-SF). Quality of Life Research, 23(3), 907–916.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, 4th edition, Text revision. Washington, DC: American Psychiatric Association.
Nunnally, J. C., & Bernstein, I. (1994). Psychometric theory (3rd ed., p. 736). New York, NY: McGraw-Hill Humanities.
Gandek, B., Ware, J., Aaronson, N., Apolone, G., Bjorner, J., Brazier, J., et al. (1998). Cross-Validation of Item Selection and Scoring for the SF-12 Health Survey in Nine Countries: Results from the IQOLA Project. Journal of Clinical Epidemiology, 51(11), 1171–1178.
Terwee, C. B., Bot, S. D., van der De Boer, M. R., Windt, D. A., Knol, D. L., Dekker, J., et al. (2007). Quality criteria were proposed for measurement properties of health status questionnaires. Journal of Clinical Epidemiology, 60, 34–42.
Schermelleh-Engel, K., Moosbrugger, H., & Muller, H. (2003). Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods Psychol Res Online, 8(2), 23–74.
Yu, C. Y. (2002). Evaluating cutoff criteria of model fit indices for latent variable models with binary and continuous outcomes. Los Angeles, CA: University of California.
Dickes, P., Tournois, J., Flieller, A., & Kop, J. L. (1994). La psychométrie (p. 288). Paris: Presses Universitaires France.
Saad, S., Carter, G. W., Rothenberg, M., & Israelson, E. (1999). Testing and assessment: An employer’s guide to good practices. Washington, DC: U.S. Department of Labor of Employment and Training Administration.
Fayers, P. M., & Machin, D. (2000). Quality of life: Assessment, analysis and interpretation. Chichester: Wiley.
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6, 284–290.
Stark, S., Chernyshenko, O. S., Chan, K. Y., Lee, W. C., & Drasgow, F. (2001). Effects of the testing situation on item responding: Cause for concern. Journal of Applied Psychology, 86(5), 943–953.
Reise, S. P., & Henson, J. M. (2003). A discussion of modern versus traditional psychometrics as applied to personality assessment scales. Journal of Personality Assessment, 81(2), 93–103.
Linacre, J. M. (2002). What do infit and outfit, mean-square and standardized mean? Rasch Measurement Transactions, 16, 878.
Rossi, A., Rucci, P., Mauri, M., Maina, G., Pieraccini, F., Pallanti, S., et al. (2005). Validity and reliability of the Italian version of the Quality of Life, Enjoyment and Satisfaction Questionnaire. Quality of Life Research, 14, 2323–2328.
Rapaport, M., Clary, C., Fayyad, R., & Endicott, J. (2005). Quality of life impairment in depressive and anxiety disorders. American Journal of Psychiatry, 162, 1171–1178.
Ponizovsky, A., & Grinshpoon, A. (2007). Quality of life among heroin users on buprenorphine versus methadone maintenance. The American Journal of Drug and Alcohol Abuse, 33(5), 631–642.
Stedman, M., Pettinati, H., Brown, E., Kotz, M., Calabrese, J., & Raines, S. (2010). A double-blind, placebo-controlled study with quetiapine as adjunct therapy with lithium or divalproex in bipolar I patients with coexisting alcohol dependence. Alcoholism, Clinical and Experimental Research, 34(10), 1822–1831.
Johnson, B., Ait-Daoud, N., Akhtar, F., & Ma, J. (2004). Oral topiramate reduces the consequences of drinking and improves the quality of life of alcohol-dependent individuals: A randomized controlled trial. Archives of General Psychiatry, 61, 905–912.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bourion-Bédès, S., Schwan, R., Epstein, J. et al. Combination of classical test theory (CTT) and item response theory (IRT) analysis to study the psychometric properties of the French version of the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF). Qual Life Res 24, 287–293 (2015). https://doi.org/10.1007/s11136-014-0772-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-014-0772-y