
Abstract
Cushing’s syndrome is associated with excessive cortisol secretion by the adrenal gland or ectopic tumours and may result in diabetes, hypertension, and life-threatening infections with high mortality rates especially in the case of surgical resection. Although surgical resection is the treatment of choice, patients may benefit from preceding medical therapy. This may especially be useful as an adjunctive approach in emergency settings, if patients cannot undergo surgery, if surgery or radiotherapy fails, or if the tumour recurs. Medical therapy can be categorized in three different groups—inhibition of steroidogenesis, suppression of adrenocorticotropic hormone, and antagonism of the glucocorticoid receptor. However, the majority of common drugs are not available for parenteral administration, which may evoke a management problem in emergency settings or in patients unable to tolerate oral medication. The carboxylated imidazole etomidate is a well known parenteral induction agent for general anaesthesia. Besides its hypnotic properties, etomidate also has α-adrenergic characteristics and inhibits the enzyme 11-deoxycortisol ß-hydroxylase, which catalyzes the final step of the conversion of cholesterol to cortisol. Adverse outcomes have been reported when used for sedation in septic or trauma patients probably by its interference with steroid homeostasis. However, its capability of inhibition of the 11-deoxycortisol ß-hydroxylase leads to suppression of cortisol secretion which has been demonstrated to be a useful tool in severe and complicated hypercortisolemia. Within this article, we review the data concerning different pharmacological approaches with particular consideration of etomidate in order to suppress steroidogenesis in patients with Cushing’s syndrome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cushing’s syndrome (CS) is marked by glucocorticoid steroid hormone excess. The disease pertains patients of any age with higher prevalence in females [1]. The incidence of CS is 0.7–2.4 per million humans per year [1]. In the majority of cases (70%), CS is caused by an adrenocorticotropic hormone (ACTH) secreting adenoma of the pituitary gland, known as Cushing’s disease [2]. 15% of CS are caused by an adenoma of the adrenal gland and the remaining 15% of CS are attributed to an ectopic tumour producing ACTH [3].
The symptoms and clinical signs of CS are well known and have been well described in the literature [4]. However, CS may lead to a life-threatening clanger of blood glucose or blood pressure and is associated with high rates of surgical mortality (5.6%) and morbidity (40%) [5–7]. Therefore, early diagnosis and adequate therapy are inevitable.
Diagnostic options
The characteristic of CS is an inappropriate cortisol secretion insensitive to the normal feedback loop. Diagnostic tests are based on demonstration of excessive cortisol secretion, loss of circadian rhythm, and abnormal regulation of hypothalamo-pituitary-axis [8]. First line-screening diagnostic methods include urinary free cortisol (≥2 measurements), late night salivary cortisol (≥2 measurements), and a 1 mg overnight dexamethasone suppression test [8]. Dexamethasone-CRH suppression test and the serum midnight cortisol test have been proposed as second-line diagnostics [9].
Once the diagnosis of CS is made, the source of cortisol excess should be located. In these circumstances, the plasma ACTH should be determined as a first step. Plasma ACTH levels of <5 pg/ml are characteristic for an ACTH-independent disease; ACTH levels >15 pg/ml are typically found in ACTH-dependent diseases [10]. Magnetic resonance imaging and computer tomography are most useful for a precise localization of the reasonable tumour [9].
Surgical therapy
The etiology of hypercortisolism is manifold and likewise its therapeutic strategies. Therefore, different strategies have to be considered individually. First-line treatment of Cushing’s disease is the surgical resection of the pituitary tumor by transphenoidal approach. This microsurgical approach is still the most widely used technique, because of the excellent view of the surgical field during the operation [2, 11]. Remission rates after operation range from 65 to 90%. The recurrence rates are 5–10% at 5 years and 10–20% at 10 years. Repeated transphenoidal resection may be undertaken if disease persists after initial surgery [12, 13]. The success rate in these cases varies between 50 and 70% in specialized centres [2, 11]. In patients with persistent Cushing’s disease, bilateral adrenalectomy can be performed as a final option after at least two attempts of pituitary adenoma resection and persistent severe medical conditions which are not manageable by medical therapy or radiation [11, 13]. Additionally, adrenalectomy is the surgical therapy of choice in patients with cortisol secreting adrenal adenoma. This procedure provides immediate control of hypercortisolism, and the morbidity can be reduced by the use of endoscopic approaches [14]. Thompson et al. could show that 79.4% of patients after bilateral laparoscopic adrenalectomy had unverifiable serum cortisol levels during follow-up; 25.7% of the included patients had serum ACTH levels greater than 300 pg/ml [15]. However, this approach results in lifelong steroid replacement therapy and because of the risk of developing Nelson syndrome, MRI scans and ACTH evaluation have to be performed in periodic intervals [14–16].
Management of patients with adrenal carcinomas requires a multidisciplinary approach, at presentation and at disease relapse. At presentation, the principal considerations are surgical, which is the only curative option [17]. Despite aggressive surgery, 70–85% of patients experience relapse locally or develop metastases. Therefore, it is not surprising that the 5-year survival rate after complete resection is only 16–35%. Incomplete resection of the carcinoma is followed by survival for less than 1 year [17]. Owing to the worse outcome, radiation of the surgical field has been performed in some studies. Whereas initial studies reported a lack of benefit with adjuvant radiation later studies claim high response rates with little toxicity [18, 19]. Finally, for patients in whom surgery is not possible, chemotherapy is often exerted, albeit with modest success (response rates 13–39%) [20, 21].
In patients presented with ectopic ACTH secretion, the source of ectopic ACTH production (e.g. a tumour) should be resected surgically. However, these patients may present two distinct problems: the tumor might not be completely resectable or is not identifiable. If surgery is not feasible or has failed, patients require adrenalectomy or medical therapy [10, 14].
Medical therapy
Although there is general agreement that surgery is the optimal therapy for Cushing’s syndrome, drug therapy may have either a primary or an adjunctive role if the patient cannot safely undergo surgery, if acute complications of hypercortisolism occur, if surgery fails, or if the tumour recurs [22, 23]. When medication is the only therapy, a major disadvantage is the need for lifelong therapy, as recurrence usually follows discontinuation of treatment. Drug therapy is also effective in controlling hypercortisolism in patients with ectopic ACTH secretion in whom the primary tumour has not been found or cannot be removed [2, 14, 22]. Different pharmacological agents are available to modulate cortisol production and ameliorate the clinical manifestation of CS. The majority of these drugs are old and some only show marginal results [24, 25]; the efficacy of newer drugs is not known and therefore needs to be evaluated in clinical trials.
The drugs which are used in the treatment of CS are summarized in Table 1 and can be divided into several groups:
-
Corticotropin inhibitors
-
Adrenal inhibitors
-
Adrenal receptor blockers
-
Glucocorticoid receptor antagonists
Corticotropin inhibitors
Cyproheptadine, PPAR-γ agonists and valproic acid are members of this group. Different reports and small clinical studies failed to show an adequate effect of these agents in the treatment of CS [26–28].
Most of the pituitary adenomas express somatostatin (ssr5) and dopamine (D2) receptors [29]. However, the somatostatin analogue octreotide failed to show clinical efficacy, which may be due to the down regulation of somatostatin receptors by glucocorticoids [30]. The available data for a potential role of octreotide in combination with ketoconazole in treating ectopic ACTH producing tumours are unconvincing [31].
The newer somatostatin analogue SOM-230 (pasireotide) showed encouraging data in initial studies. Pasireotide has a high affinity to all somatostatin receptor subtypes and a 40-fold higher affinity to ssr5 than octreotide [32]. Compared to octreotide, pasireotide leads to an increased suppression of ACTH release [33]. Preliminary results of an open label, single arm phase 2 study of fourteen patients with persistent or recurrent CS treated with pasireotide 600 μg subcutaneously twice daily for a period of fifteen days, showed normalization of serum cortisol levels to baseline in 21%. Half of the patients had serum cortisol levels that were reduced by more than 40% with significant improvement of typical CS symptoms [34].
Adrenal inhibitors
Aminoglutethimide
Aminoglutethimide has been used in adults and children in doses of 500–2,000 mg daily and prevents the conversion of cholesterol to pregnenolone [35]. In patients with CS, application of aminoglutethimide leads to clinical and biochemical remission in up to 42% of cases (50% reduction of morning serum cortisol levels or return to normal cortisol levels) [36]. The suppressive effect of aminoglutethimide can be reversed by the stimulating effect of ACTH [37]. Therefore, aminoglutethimide is not efficacious as a monotherapy [23].
Aminoglutethimide may cause gastrointestinal (nausea, vomiting) and neurological side effects (sedation, lethargy). Hypothyroidism can be found in 5% of treated patients. Cholestasis and bone marrow suppression are also rare side effects [35]. In addition, aminoglutethimide induces different P450 enzymes including CYP1A2 and CYP3A4 which may cause unintentional medication interactions [35].
Ketoconazole
Ketoconazole is the initial drug of choice and inhibits the synthesis of cholesterol by blocking demethylation of lanosterol. Additional mechanisms of action include inhibition of 17α-hydroxylase, 11β-hydroxylase and the cholesterol side chain cleavage [23]. A metaanalysis of patients with CS receiving 400–1,200 mg ketoconazole daily yielded an average remission rate of 70% [23].
Hepatotoxicity is the most common side effect, observed in 12% of cases [23]. Therefore, liver function should be monitored during application of ketoconazole (early markers include serum alkaline phosphatase, ALT, AST, and bilirubin). In addition to hepatic side effects, nausea, vomiting, headache, and sedation might occur [23, 38].
The use of ketoconazole during pregnancy is obsolete, because of its teratogenicity [13]. Similar to aminoglutethimide, ketoconazole interacts with cytochrome P450 enzymes and may cause significant drug interactions [38].
Mitotane
Mitotane is started with a dose of 250–500 mg doses nightly with slow elevation of the doses up to 4–12 g daily. The drug inhibits 11α-hydroxylase, 18-hydroxylase, 3α-hydroxylase, and hydroxysteroid dehydrogenase [24]. Luton et al. [39] found a remission rate of 83% after 8 months in 46 patients with Cushing’s disease. In 60% of these patients, the effect disappeared after the drug was discontinued [39].
Side effects of mitotane therapy include hypercholesterolemia, anorexia, nausea, diarrhoea, decreased memory, and gynecomastia [40]. At higher doses of mitotane, neurological side effects including ataxia, vertigo, confusion, and difficulty with language expression can be observed [24]. Finally, the drug is contraindicated in pregnant women owing to teratogenicity [41].
Adrenal aberrant receptor blockers
In very rare cases of CS, cortisol release is regulated non-physiologically via aberrant receptors independent of ACTH (caused by macronodular hyperplasia). Regulation via β-adrenergic receptors or luteinizing hormone receptors has been described in this context [42, 43]. Pharmacological treatment of these patients consists of β-blockade with propanolol or blockade of luteinizing hormone receptors using gonadotropin releasing hormone antagonists [42, 43].
Glucocorticoid receptor antagonists
Mifepristone has been proven to be effective in the treatment of adrenal cortical carcinoma, ectopic ACTH secretion and Cushing’s diseases in investigational, retrospective analyses [11, 44]. The steroid mifepristone binds competitively to the glucocorticoid, progestin and androgen receptor and inhibits the activation of their endogenous ligands. In nonpituitary cases of hypercortisolism, mifepristone is effective at doses of 10–25 mg/kg daily. Severe hypokalemia has been reported in some cases after application of mifepristone in higher doses [11].
Therapy with etomidate
Etomidate belongs to an older group of steroid synthesis inhibitors and has experienced a renewed interest during the last years [23, 45]. Indeed, an increasing number of reports have been published dealing with the effects of etomidate in vitro (Table 2) or with the use of intravenous etomidate to correct severe symptoms of hypercortisolism (Table 3). Etomidate can be used for long-term treatment as well as for emergency settings [3, 46–48]. Particularly in patients with rapidly developing hypercortisolism (e.g. patients with ectopic ACTH-producing tumors) followed by rapidly progressive metabolic disorders, severe hypertension or acute psychotic conditions, a rapid therapy has to be initiated [22, 45]. Etomidate has a rapid onset of action and is particularly useful in patients in emergency settings (e.g. ditched hypertension or acute psychosis which are unable to treat with conventional therapy). Furthermore, etomidate is the only drug in the therapy of hypercortisolism available for parenteral administration which is most valuable in patients who are unable to take oral medication [12, 46, 49]. Finally, etomidate is also used as therapeutic option in patients developing transient liver function disorders after application of ketoconazole [12, 45, 46].
The anesthetic drug etomidate is an imidazole derivate which consits of two isomers; the (+) isomer obtains the hypnotic characteristics of etomidate [50]. Its pharmacokinetics include rapid onset and recovery, minimal respiratory suppression, and hemodynamic stability [51]. At a physiological pH, etomidate is 75% protein bound (mostly to albumin), but only the unbound fraction is metabolically active [52]. Etomidate is degraded to inactive metabolites by hepatic enzymes and plasma esterases [53]. It has α-adrenergic agonist properties which may be the reason for the hemodynamic stability [54]. Furthermore, etomidate inhibits 17α-hydroxylase, 11α-hydroxylase, and 11-deoxycortisol β-hydroxylase which are important enzymes in the steroidogenesis [55].
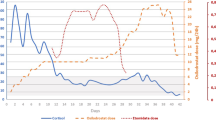
The main effect of etomidate is hypnosis. An induction dose of etomidate (0.2–0.4 mg/kg) results in apnoea and hypnosis 10–15 s after application [56]. Side effects include pain at the injection side, anaphylactic reactions, minimal change in heart rate, reduction in mean arterial pressure, mild decrease of systolic blood pressure and cardiac index, myoclonus, nausea, and vomiting [57–59]. However, the most critical adverse effect of etomidate is adrenal suppression, occurring approximately 30 min after application of a single dose and may last for about 24 h [60]. In emergency settings, infusion of 2–3 mg/h decreased serum cortisol levels to normal within 24 h [46, 47]. Prolonged application of etomidate in a sub-hypnotic dose (0.03–0.1 mg/kg/h) leads to suppression of cortisol secretion after 48 h without hypnotic or adverse effects [61, 62]. In children continuous infusion of a rate between 0.03 and 0.08 mg/kg/h is recommended [12]. Frequent monitoring of cortisol levels, electrolytes, and glucose levels are necessary in order to prevent adverse effects and hypocortisolemia [49]. Cortisol replacement is recommended when etomidate is applicated for more than 24 h, because cortisol levels decrease dramatically and may induce adrenal insufficiency [61].
Conclusion
In conclusion, hypercortisolism in the context of CS can be presented as a medical emergency with various complications and high mortality rates. Except for emergency settings, surgical resection of the underlying cause is the treatment of choice. Medical treatment is not the first-line therapy (apart from emergency settings), but it offers an excellent option as an adjuvant therapeutic agent or in order to control hypercortisolism pre- and peri-operatively. Adrenal suppression induced by etomidate can be used safely in sub-hypnotic dosages and presents an excellent short-term control of severe hypercortisolemia when surgery is impossible, other oral medications have failed or in emergency settings.
References
Lindholm J, Juul S, Jorgensen JO, Astrup J, Bjerre P, Feldt-Rasmussen U, Hagen C et al (2001) Incidence and late prognosis of cushing’s syndrome: a population-based study. J Clin Endocrinol Metab 86:117–123
Schteingart DE (2009) Drugs in the medical treatment of cushing’s syndrome. Expert Opin Emerg Drugs 14:661–671
Lutgers HL, Vergragt J, Dong PV, de Vries J, Dullaart RP, van den Berg G et al (2010) Severe hypercortisolism: a medical emergency requiring urgent intervention. Crit Care Med 38:1598–1601
Ross EJ, Linch DC (1982) Cushing’s syndrome–killing disease: discriminatory value of signs and symptoms aiding early diagnosis. Lancet 320:646–649
Sarlis NJ, Chanock SJ, Nieman LK (2000) Cortisolemic indices predict severe infections in cushing syndrome due to ectopic production of adrenocorticotropin. J Clin Endocrinol Metab 85:42–47
Watson RG, van Heerden JA, Northcutt RC, Grant CS, Ilstrup DM (1986) Results of adrenal surgery for cushing’s syndrome: 10 years′ experience. World J Surg 10:531–538
Takagi S, Tanabe A, Tsuiki M, Naruse M, Takano K (2009) Hypokalemia, diabetes mellitus, and hypercortisolemia are the major contributing factors to cardiac dysfunction in adrenal cushing’s syndrome. Endocr J 56:1009–1018
Nieman LK, Biller BM, Findling JW, Newell-Price J, Savage MO, Stewart PM et al (2008) The diagnosis of Cushing’s syndrome: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 93:1526–1540
Newell-Price J (2009) Diagnosis/differential diagnosis of cushing’s syndrome: a review of best practice. Best Pract Res Clin Endocrinol Metab 23(Suppl 1):S5–S14
Newell-Price J, Bertagna X, Grossman AB, Nieman LK (2006) Cushing’s syndrome. Lancet 367:1605–1617
Chu JW, Matthias DF, Belanoff J, Schatzberg A, Hoffman AR, Feldman D (2001) Successful long-term treatment of refractory cushing’s disease with high-dose mifepristone (RU 486). J Clin Endocrinol Metab 86:3568–3573
Mettauer N, Brierley J (2009) A novel use of etomidate for intentional adrenal suppression to control severe hypercortisolemia in childhood. Pediatr Crit Care Med 10:e37–e40
Gross BA, Mindea SA, Pick AJ, Chandler JP, Batjer HH (2007) Medical management of cushing disease. Neurosurg Focus 23:E10
Porterfield JR, Thompson GB, Young WF Jr et al (2008) Surgery for cushing’s syndrome: an historical review and recent ten-year experience. World J Surg 32:659–677
Thompson SK, Hayman AV, Ludlam WH, Deveney CW, Loriaux DL, Sheppard BC (2007) Improved quality of life after bilateral laparoscopic adrenalectomy for cushing’s disease: a 10-year experience. Ann Surg 245:790–794
Malley D, Boris R, Kaul S et al (2008) Synchronous bilateral adrenalectomy for adrenocorticotropic-dependent cushing’s syndrome. J Soc Laparoendosc Surg 12:198–201
Assié G, Antoni G, Tissier F et al (2007) Prognostic parameters of metastatic adrenocortical carcinoma. J Clin Endocrinol Metab 92:148–154
Markoe AM, Serber W, Micaily B et al (1991) Radiation therapy for adjunctive treatment of adrenal cortical carcinoma. Am J Clin Oncol 14:170–174
Fassnacht M, Hahner S, Polat B et al (2006) Efficacy of adjuvant radiotherapy of the tumor bed on local recurrence of adrenocortical carcinoma. J Clin Endocrinol Metab 91:4501–4504
Abraham J, Bakke S, Rutt A et al (2002) A phase II trial of combination chemotherapy and surgical resection for the treatment of metastatic adrenocortical carcinoma: continuous infusion doxorubicin, vincristine, and etoposide with daily mitotane as a P-glycoprotein antagonist. Cancer 94:2333–2343
Williamson SK, Lew D, Miller GJ et al (2000) PhaseII evaluation of cisplatin and etoposide followed by mitotane at disease progression in patients with locally advanced or metastatic adrenocortical carcinoma: a southwest oncology group study. Cancer 88:1159–1165
Feelders RA, Hofland LJ, de Herder WW (2010) Medical treatment of cushing’s syndrome: adrenal-blocking drugs and ketaconazole. Neuroendocrinology 92:111–115
Engelhardt D, Weber MM (1994) Therapy of cushing’s syndrome with steroid biosynthesis inhibitors. J Steroid Biochem Mol Biol 49:261–267
Nieman LK (2002) Medical therapy of cushing’s disease. Pituitary 5:77–82
Colao A, Pivonello R, Tripodi FS, Orio F Jr, Ferone D, Cerbone G et al (1997) Failure of long-term therapy with sodium valproate in cushing’s disease. J Endocrinol Invest 20:387–392
Krieger DT, Amorosa L, Linick F (1975) Cyproheptadine-induced remission of cushing’s disease. N Engl J Med 293:893–896
Suri D, Weiss RE (2005) Effect of pioglitazone on adrenocorticotropic hormone and cortisol secretion in cushing’s disease. J Clin Endocrinol Metab 90:1340–1346
Mercado-Asis LB, Yanovski JA, Tracer HL, Chik CL, Cutler GB Jr (1997) Acute effects of bromocriptine, cyproheptadine, and valproic acid on plasma adrenocorticotropin secretion in Nelson’s syndrome. J Clin Endocrinol Metab 82:514–517
de Bruin C, Pereira AM, Feelders RA, Romijn JA, Roelfsema F, Sprij-Mooij DM et al (2009) Coexpression of dopamine and somatostatin receptor subtypes in corticotroph adenomas. J Clin Endocrinol Metab 94:1118–1124
Kraus J, Woltje M, Schonwetter N, Hollt V (1998) Alternative promoter usage and tissue specific expression of the mouse somatostatin receptor 2 gene. FEBS Lett 428:165–170
Bertagna X, Favrod-Coune C, Escourolle H, Beuzeboc P, Christoforov B, Girard F et al (1989) Suppression of ectopic adrenocorticotropin secretion by the long-acting somatostatin analog octreotide. J Clin Endocrinol Metab 68:988–991
Boerlin V, van der Hoek J, Beglinger C, Poon KW, Hartmann S, Dutreix C et al (2003) New insights on SOM230, a universal somatostatin receptor ligand. J Endocrinol Invest 26:14–16
Hofland LJ, van der Hoek J, Feelders R, van Aken MO, van Koetsveld PM, Waaijers M et al (2005) The multi-ligand somatostatin analogue SOM230 inhibits ACTH secretion by cultured human corticotroph adenomas via somatostatin receptor type 5. Eur J Endocrinol 152:645–654
Dang CN, Trainer P (2007) Pharmacological management of Cushing’s syndrome: an update. Arq Bras Endocrinol Metabol 51:1339–1348
Santen RJ, Misbin RI (1981) Aminoglutethimide: review of pharmacology and clinical use. Pharmacotherapy 1:95–120
Misbin RI, Canary J, Willard D (1976) Aminoglutethimide in the treatment of cushing’s syndrome. J Clin Pharmacol 16:645–651
Schteingart DE, Conn JW (1967) Effects of aminoglutethimide upon adrenal function and cortisol metabolism in Cushing’s syndrome. J Clin Endocrinol Metab 27:1657–1666
Loose DS, Kan PB, Hirst MA, Marcus RA, Feldman D (1983) Ketoconazole blocks adrenal steroidogenesis by inhibiting cytochrome P450-dependent enzymes. J Clin Invest 71:1495–1499
Luton JP, Mahoudeau JA, Bouchard P, Thieblot P, Hautecouverture M, Simon D et al (1979) Treatment of Cushing’s disease by O, p′DDD. Survey of 62 cases. N Engl J Med 300:459–464
Schteingart DE, Tsao HS, Taylor CI, McKenzie A, Victoria R, Therrien BA (1980) Sustained remission of cushing’s disease with mitotane and pituitary irradiation. Ann Intern Med 92:613–619
Leiba S, Weinstein R, Shindel B, Lapidot M, Stern E, Levavi H et al (1989) The protracted effect of o, p′-DDD in Cushing’s disease and its impact on adrenal morphogenesis of young human embryo. Ann Endocrinol (Paris) 50:49–53
Lacroix A, Tremblay J, Rousseau G, Bouvier M, Hamet P (1997) Propranolol therapy for ectopic beta-adrenergic receptors in adrenal cushing’s syndrome. N Engl J Med 337:1429–1434
Lacroix A, Hamet P, Boutin JM (1999) Leuprolide acetate therapy in luteinizing hormone–dependent cushing’s syndrome. N Engl J Med 341:1577–1581
Castinetti F, Fassnacht M, Johanssen S, Terzolo M, Bouchard P, Chanson P et al (2009) Merits and pitfalls of mifepristone in cushing’s syndrome. Eur J Endocrinol 160:1003–1010
Dabbagh A, Sa’adat N, Heidari Z (2009) Etomidate infusion in the critical care setting for suppressing the acute phase of cushing’s syndrome. Anesth Analg 108:238–239
Greening JE, Brain CE, Perry LA, Mushtaq I, Sales Marques J, Grossman AB et al (2005) Efficient short-term control of hypercortisolaemia by low-dose etomidate in severe paediatric cushing’s disease. Horm Res 64:140–143
Drake WM, Perry LA, Hinds CJ, Lowe DG, Reznek RH, Besser GM (1998) Emergency and prolonged use of intravenous etomidate to control hypercortisolemia in a patient with cushing’s syndrome and peritonitis. J Clin Endocrinol Metab 83:3542–3544
Krakoff J, Koch CA, Calis KA, Alexander RH, Nieman LK (2001) Use of a parenteral propylene glycol-containing etomidate preparation for the long-term management of ectopic cushing’s syndrome. J Clin Endocrinol Metab 86:4104–4108
Johnson TN, Canada TW (2007) Etomidate use for cushing’s syndrome caused by an ectopic adrenocorticotropic hormone-producing tumor. Ann Pharmacother 41:350–353
Hadzija BW, Lubarsky DA (1995) Compatibility of etomidate, thiopental sodium, and propofol injections with drugs commonly administered during induction of anesthesia. Am J Health Syst Pharm 52:997–999
Van Hamme MJ, Ghoneim MM, Ambre JJ (1978) Pharmacokinetics of etomidate, a new intravenous anesthetic. Anesthesiology 49:274–277
Meuldermans WE, Heykants JJ (1976) The plasma protein binding and distribution of etomidate in dog, rat and human blood. Arch Int Pharmacodyn Ther 221:150–162
de Ruiter G, Popescu DT, de Boer AG, Smeekens JB, Breimer DD (1981) Pharmacokinetics of etomidate in surgical patients. Arch Int Pharmacodyn Ther 249:180–188
Paris A, Philipp M, Tonner PH, Steinfath M, Lohse M, Scholz J et al (2003) Activation of alpha 2B-adrenoceptors mediates the cardiovascular effects of etomidate. Anesthesiology 99:889–895
Fry DE, Griffiths H (1984) The inhibition by etomidate of the 11 beta-hydroxylation of cortisol. Clin Endocrinol (Oxf) 20:625–629
Reddy RV, Moorthy SS, Dierdorf SF, Deitch RD Jr, Link L (1993) Excitatory effects and electroencephalographic correlation of etomidate, thiopental, methohexital, and propofol. Anesth Analg 77:1008–1011
Wells JK (1985) Comparison of ICI 35868, etomidate and methohexitone for day-case anaesthesia. Br J Anaesth 57:732–735
McCollum JS, Dundee JW (1986) Comparison of induction characteristics of four intravenous anaesthetic agents. Anaesthesia 41:995–1000
Scheffer GJ, Ten Voorde BJ, Karemaker JM, Ros HH, de Lange JJ (1993) Effects of thiopentone, etomidate and propofol on beat-to-beat cardiovascular signals in man. Anaesthesia 48:849–855
Lundy JB, Slane ML, Frizzi JD (2007) Acute adrenal insufficiency after a single dose of etomidate. J Intensive Care Med 22:111–117
Schulte HM, Benker G, Reinwein D, Sippell WG, Allolio B (1990) Infusion of low dose etomidate: correction of hypercortisolemia in patients with cushing’s syndrome and dose-response relationship in normal subjects. J Clin Endocrinol Metab 70:1426–1430
Allolio B, Stuttmann R, Fischer H, Leonhard W, Winkelmann W (1983) Long-term etomidate and adrenocortical suppression. Lancet 322:626
Gärtner R, Albrecht M, Müller OA (1986) Effect of etomidate on hypercortisolism due to ectopic ACTH production. Lancet 1:275
Allolio B, Schulte HM, Kaulen D, Reincke M, Jaursch-Hancke C, Winkelmann W (1988) Nonhypnotic low-dose etomidate for rapid correction of hypercortisolaemia in cushing’s syndrome. Klin Wochenschr 66:361–364
Herrmann BL, Mitchell A, Saller B (2001) Transsphenoidal hypophysectomy of a patient with an ACTH-producing pituitary adenoma and an “empty sella” after pretreatment with etomidate. Dtsch Med Wochenschr 126:232–234
Bilgin YM, van der Wiel HE, Fischer HR, De Herder WW (2007) Treatment of severe psychosis due to ectopic cushing’s syndrome. J Endocrinol Invest 30:776–779
Lamberts SW, Bons EG, Bruining HA, de Jong FH (1987) Differential effects of the imidazole derivatives etomidate, ketoconazole and miconazole and of metyrapone on the secretion of cortisol and its precursors by human adrenocortical cells. J Pharmacol Exp Ther 240:259–264
Varga I, Rácz K, Kiss R et al (1993) Direct inhibitory effect of etomidate on corticosteroid secretion in human pathologic adrenocortical cells. Steroids 58:64–68
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Heyn, J., Geiger, C., Hinske, C.L. et al. Medical suppression of hypercortisolemia in Cushing’s syndrome with particular consideration of etomidate. Pituitary 15, 117–125 (2012). https://doi.org/10.1007/s11102-011-0314-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-011-0314-3