
Abstract
Familial Mediterranean fever is an autosomal recessive disorder characterized by recurrent attacks of abdominal pain, synovitis and pleuritis. MEFV gene mutations are responsible for the disease. The objective of this study was to identify the frequency and distribution of 12 MEFV mutations in 153 Syrian patients and perform a genotype–phenotype correlation in the patients’ cohort. Of the 153 unrelated patients investigated, 97 (63.4%) had at least one mutation. The most frequent mutation was M694V (36.5%), followed by V726A (15.2%), E148Q (14.5%), M680I (G/C) (13.2%), and M694I (10.2%) mutations. Rare mutations (R761H, A744S, M680I (G/A), K695R, P369S, F479L and I692del) were also detected in the patients. M694V was associated with the severe form of the disease. The identification of a significant number of FMF patients with no mutations or only one known mutation identified indicates the presence of new mutations in the MEFV gene which will be investigated in the future.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Familial Mediterranean fever (FMF) (OMIM #249100) is a genetic disease with autosomal-recessive inheritance. The disease most commonly occurs in Arabs, Jews, Armenians and Turks [1]. FMF is clinically characterized by recurrent and self-limited attacks of fever accompanied by peritonitis, pleuritis, synovitis or erysipelas-like erythema and may be complicated by AA amyloidosis. Colchicine was found to be very effective in preventing attacks of FMF and in the development of amyloidosis [2].
The responsible gene, MEFV, has been mapped to chromosome 16p13.3 and consists of 10 exons and encodes a 781 amino acid protein called Pyrin which is expressed in granulocytes and is thought to be a negative regulator of inflammation. Since the cloning of the MEFV gene [3, 4], about 166 mutations have been associated with FMF [5]. Five founding mutations M694V, V726A, M680I, M694I (in exon 10) and E148Q (in exon 2) are the most frequently encountered mutations and account for 74% of FMF mutations in typical patients [6]. The carrier rate in the Syrian population is 17.5% [7, 8]. A previous study on 83 Syrian patients showed that the M694V, V726A, M694I, M680I and E148Q mutations account for 45.8, 26, 13.9, 4.8 and 6%, respectively [7].
The main aim of this study was to identify the frequency of 12 MEFV mutations and correlate the phenotypic features with the type of co-existing mutations in a large number of Syrian patients with FMF.
Patients and methods
This study was conducted in the Clinical Genetics Unit, Atomic Energy Commission of Syria (AECS) between April 2005 and February 2007. A total of 153 unrelated patients were referred by their physicians for FMF mutation detection and genetic counseling. A clinical diagnosis of FMF was made according to the international FMF criteria [9]. The disease severity was evaluated according to the previously described criteria [10] and assigned to 1 of 3 severity levels (mild, intermediate, or severe). Every patient was informed about the study and a written consent was signed either by the patient or his/her parent for blood sampling.
For all patients, EDTA blood was sampled and DNA was isolated from frozen blood samples by the phenol–chlorophorm extraction method [11].
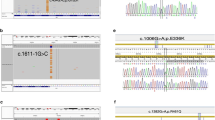
MEFV mutation analysis was performed for 12 mutations using a reverse-hybridization assay (FMF StirpAssay™) according to the manufacturer’s instructions (ViennaLab Labordiagnostika, Vienna, Austria). In a first step, exons 2, 3, 5, and 10 were amplified for each patient in a single, multiplex PCR reaction. A thermocycling program of 35 cycles (94°C for 15s, 58°C for 30s, and 72°C for 30s) with a final extension at 72°C for 3 min was performed, leading to four DNA fragments (206, 236, 295, and 318 bp). PCR products were selectively hybridized to a test strip presenting a parallel array of allele-specific oligonucleotide probes, and detected by enzymatic color reaction as described by Tchernitchko et al. [12]. The following MEFV mutations were investigated: E148Q in exon 2, P369S in exon 3, F479L in exon 5, and M680I (G/C), M680I (G/A), I692del, M694V, M694I, K695R, V726A, A744S, R761H in exon 10.
Statistical analysis
Differences between groups were assessed using the Z-test for two proportions and T-test for means. A P value <0.05 was accepted as statistically significant.
Results
Among the 153 patients, 75 (49%) were males and 78 (51%) were females (female to male ratio was 1.04). A positive family history of FMF was observed in 54 (35%) of the patients, whereas the parents of 49 (32%) patients proved to be relatives. The mean age of onset of FMF in Syrian patients was 11.5 years.
The main clinical characteristics of the patients were as follows: peritonitis was observed in 90% of the patients, fever in 85.5%, arthritis in 30.9%, pleuritis in 17.5%, rash and eryspilas-like erythema in 6%, pericarditis in 2% and myalgia in 3%. None of the patients developed amyloidosis but a 45 years old woman (who was homozygous for the mutation M694V) developed proteinurea (20 mg/dl) as she stopped taking colchicine at the age of 24. However, no renal biopsy was performed to confirm the diagnosis.
Mutations in the MEFV gene were identified in 97 (63.4%) patients and the mutation detection was negative in 56 (36.6%) patients. Of those 97 patients with mutations, 19 (20%) were homozygous, 34 (35%) were compound heterozygous and 44 (45%) were heterozygous (Table 1). Complex alleles were observed in six patients (Table 1). Mutation detection allowed the identification of 12 of different MEFV mutations in 159 of the 194 tested alleles (Table 2). The most dominant mutations detected were M694V (36.5%), V726A (15.2%), E148Q (14.5%), M680I (G/C) (13.2%) and M694I (10.2%) (Table 2). The remaining seven mutations (R761H, A744S, M680I (G/A), K695R, P369S, F479L and I692del) were much less represented (Table 2). Of the 97 patients, 57 (58.7%) were treated with colchicine and 46 (80.7%) responded with complete remission or significant improvement (reduction of number and severity of FMF episodes).
In order to evaluate the phenotype–genotype correlation, 97 patients were divided into three groups according to the presence of the M694V mutation on both of the alleles (M694V/M694V), on only one allele (M694V/other), and on none of the alleles (other/other). Among those patients, 10 clinical features of the disease were compared (Table 3). There were no statistically significant differences between these groups with regard to male/female ratio, abdominal pain, fever, chest pain, erysipelas-like erythema, myalgia, and family history of FMF (Table 3). However, there were statistically significant differences between groups I and III, and groups II and III regarding arthritis. Moreover, there were statistical significant differences between groups I and III regarding age of onset (Table 3).
The severity of the disease and the genotype–phenotype correlation were assessed in all 97 patients (Table 3). There was an association between the severity and the M964V mutation. There were statistically significant differences between the mean severity scores of groups I and III (Table 3). More than half of the M694V homozygote patients showed the most severe clinical features. It should be also noted that 60% of the patients with the M694V/V726A genotype had severe clinical features.
Discussion
In this study, the frequency of 12 MEFV mutations and the genotype-phenotype correlation are described in 153 Syrian patients suffering from FMF.
The clinical features of FMF in the Syrian patients are different from those reported from other populations. Peritonitis was the most common symptom in the Syrian patients with similar frequency to that observed in Turks, Jews, Arabs, Armenians [13–15]. Fever is the most common symptom in the other populations (the frequency ranges from 93 to 100%) [15] whereas the frequency of fever in this study was 85.5%. The frequency of arthritis in our patients was similar to that reported from other ethnic groups (apart from the Jews) [15]. The frequency of pleuritis was lower in the Syrian patients compared to the other populations [14, 15]. The low rate of amyloidosis in the Syrian patients is similar to that reported in the other Arabs [16] and Iranian Azeri Turkish [17]. This might be due to the fact that these data were obtained after the introduction of colchicine as a recommended treatment for FMF. The frequency of erysipelas-like erythema in the Syrian patients was similar to that reported in the Arabs and Armenians but is less common than in the Jews and Turks [15]. The percentage of the colchicine non-responders in this study was 19.3% whereas it is 5–10% in the other ethnic groups [14, 15]. It has been previously suggested that colchicine treatment failure is associated with decreased concentration of the drug in the mononuclear cells, probably resulting from a genetic defect unrelated to the underlying FMF [18]. High carrier frequency of FMF in Syria (17.5%) [7] explains that only 32% of parents of those patients in this study proved to be relatives.
In the current study, 12 known mutations in the MEFV gene were screened among 153 FMF Syrian patients which led to positive identification of 1, 2, 3 or 4 mutations in 97 (63.4%) patients. The five most common mutations include M694V, V726A, E148Q, M680I (G/C) and M694I accounting for 89.1% of the total mutations and the remaining 10.9% mutations includes R761H, A744S, M680I (G/A), K695R, P369S, F479L and I692del (Table 1). None of the 12 mutations was detected in 56 (36.6%) patients. This could possibly be due to many factors, including the presence of other rare mutations, unknown mutations, or genetic heterogeneity.
The five most frequent mutations in this study (Table 2) are similar to what previously reported in the Syrian patients [7] and the other Arabs (Lebanese, Jordanians, and Tunisians) [16] with different frequencies. M694V is the most prevalent mutation in this study (Table 2) as it was previously reported in other Arabs (except the Tunisians [19]) and other ethnic groups (Turks [20, 21], Armenians [22], Iranian Azeri Turks [17] and Jews [23]). There was an association between the severity of the disease and the M964V mutation. The M694V homozygotes accounted for 12.3% of all the patients and 63% of the homozygotes (Table 1). More than half of the M694V homozygote patients and 60% of the patients with the M694V/V726A genotype showed the most severe clinical features. The author found statistically significant differences between patients who had the M694V mutation and did not have it regarding arthritis. Moreover, there were statistically significant differences between patients with the M694V/M694V genotype and the patients with the other/other genotype regarding the age of onset of FMF and mean severity score of the patients. Since none of our patients developed amyloidosis, we could not conclude any association between M694V and the development of amyloidosis. The only patient who developed proteinurea was M694V homozygote and stopped taking colchicine at the age of 24. Several studies have reported that the mutation M694V is associated with severe disease, early onset, high frequency of attacks, the necessity of a high dose of colchicine to control attacks and high frequent occurrence of amyloidosis in untreated patients [24].
The V726A mutation was the second most common mutation observed (Table 2) which was similar to that reported in Arabs, Armenians and Jews. Unlike the previous study on the Syrian patients [7], E148Q was the third most common mutation in this group of Syrian patients (Table 2). This mutation is the least penetrant mutation and is associated with a mild clinical course [23]. M680I (G/C), which is mostly characteristic of Armenians and Turks, was the forth most common mutation in this study (Table 2). M694I was the fifth most common mutation in this study with a frequency of 10.2%, similar to its frequency in the Lebanese. Recent publications have shown that M694I was found mainly in Arabs (especially in North Africa [19]), whereas it is less common in Turks and Iranian Azeri Turks and not found in Jews. To the best of the author’s knowledge, this is the first report which detects rare mutations such as M680I (G/A), K695R, P369S, F479L and I692del in the Syrian patients (Table 2). The frequency of R761H was 4.4% in this study. This mutation was previously described in the Syrian [7], Lebanese [25] and Palestinian patients [26] but not in the Jordanians [25]. The A744S mutation was detected with a frequency of 1.8% in the patients screened here. This mutation was identified in Arabs [7, 25, 27, 28] and in an Ashkenazi Jew [29] and seems to be specific to Arabs. Interestingly, six patients presented with complex alleles (Table 1).
In conclusion, this study established new aspects related to the spectrum of MEFV mutations in the Syrian patients. M694V was the most common mutation and there was an association between this mutation and the severity of FMF symptoms. These results provide important tools for adapting a molecular diagnostic test for the Syrian population.
References
Sohar E, Gafni J, Pras M et al (1967) Familial Mediterranean fever. A survey of 470 cases and review of the literature. Am J Med 43:227–253. doi:10.1016/0002-9343(67)90167-2
Lidar M, Livneh A (2007) Familial Mediterranean fever: clinical, molecular and management advancements. Neth J Med 65:318–324
Consortium TFF (1997) A candidate gene for familial Mediterranean fever. Nat Genet 17:25–31. doi:10.1038/ng0997-25
Consortium TIF (1997) Ancient missense mutations in a new member of the RoRet gene family are likely to cause familial Mediterranean fever. Cell 90:797–807. doi:10.1016/S0092-8674(00)80539-5
INFEVERS The registry of Familial Mediterranean Fever (FMF) and hereditary Autoinflammatory Disorders Mutations. http://fmf.igh.cnrs.fr/ISSAID/infevers/. Accessed 11 Mar 2008
Touitou I (2003) Standardized testing for mutations in familial Mediterranean fever. Clin Chem 49:1781–1782. doi:10.1373/clinchem.2003.025791
Mattit H, Joma M, Al-Cheikh S et al (2006) Familial Mediterranean fever in the Syrian population: gene mutation frequencies, carrier rates and phenotype-genotype correlation. Eur J Med Genet 49:481–486. doi:10.1016/j.ejmg.2006.03.002
Al-Alami JR, Tayeh MK, Najib DA et al (2003) Familial Mediterranean fever mutation frequencies and carrier rates among a mixed Arabic population. Saudi Med J 24:1055–1059
Livneh A, Langevitz P, Zemer D et al (1997) Criteria for the diagnosis of familial Mediterranean fever. Arthritis Rheum 40:1879–1885. doi:10.1002/art.1780401023
Mor A, Shinar Y, Zaks N et al (2005) Evaluation of disease severity in familial Mediterranean fever. Semin Arthritis Rheum 35:57–64. doi:10.1016/j.semarthrit.2005.02.002
Sambrook JFE, Maniatis T (1989) Molecular Cloning: a laboratory manual, 2nd edn. Cold Spring Harbor Laboratory Press, New york
Tchernitchko D, Legendre M, Delahaye A et al (2003) Clinical evaluation of a reverse hybridization assay for the molecular detection of twelve MEFV gene mutations. Clin Chem 49:1942–1945. doi:10.1373/clinchem.2003.021212
Tunca M, Akar S, Onen F et al (2005) Familial Mediterranean fever (FMF) in Turkey: results of a nationwide multicenter study. Medicine (Baltimore) 84:1–11. doi:10.1097/01.md.0000152370.84628.0c
Ben-Chetrit E, Levy M (1998) Familial Mediterranean fever. Lancet 351:659–664. doi:10.1016/S0140-6736(97)09408-7
Onen F (2006) Familial Mediterranean fever. Rheumatol Int 26:489–496. doi:10.1007/s00296-005-0074-3
El-Shanti H, Majeed HA, El-Khateeb M (2006) Familial mediterranean fever in Arabs. Lancet 367:1016–1024. doi:10.1016/S0140-6736(06)68430-4
Esmaeili M, Bonyadi M, Rafeey M et al (2008) Common MEFV mutation analysis in Iranian Azeri Turkish patients with familial Mediterranean fever. Semin Arthritis Rheum 37:334–338
Lidar M, Scherrmann JM, Shinar Y et al (2004) Colchicine nonresponsiveness in familial Mediterranean fever: clinical, genetic, pharmacokinetic, and socioeconomic characterization. Semin Arthritis Rheum 33:273–282. doi:10.1053/S0049-0172(03)00137-9
Chaabouni HB, Ksantini M, M’Rad R et al (2007) MEFV mutations in Tunisian patients suffering from familial Mediterranean fever. Semin Arthritis Rheum 36:397–401. doi:10.1016/j.semarthrit.2006.12.004
Gunesacar R, Kasap H, Erken E et al (2005) Comparison of amplification refractory mutation system and polymerase chain reaction-restriction fragment length polymorphism techniques used for the investigation of MEFV gene exon 10 point mutations in familial Mediterranean fever patients living in Cukurova region (Turkey). Genet Test 9:220–225. doi:10.1089/gte.2005.9.220
Yalcinkaya F, Cakar N, Misirlioglu M et al (2000) Genotype-phenotype correlation in a large group of Turkish patients with familial mediterranean fever: evidence for mutation-independent amyloidosis. Rheumatology (Oxford) 39:67–72. doi:10.1093/rheumatology/39.1.67
Cazeneuve C, Sarkisian T, Pecheux C et al (1999) MEFV-Gene analysis in armenian patients with Familial Mediterranean fever: diagnostic value and unfavorable renal prognosis of the M694V homozygous genotype-genetic and therapeutic implications. Am J Hum Genet 65:88–97. doi:10.1086/302459
Touitou I (2001) The spectrum of Familial Mediterranean Fever (FMF) mutations. Eur J Hum Genet 9:473–483. doi:10.1038/sj.ejhg.5200658
Shohat M, Magal N, Shohat T et al (1999) Phenotype–genotype correlation in familial Mediterranean fever: evidence for an association between Met694 Val and amyloidosis. Eur J Hum Genet 7:287–292. doi:10.1038/sj.ejhg.5200303
Medlej-Hashim M, Serre JL, Corbani S et al (2005) Familial Mediterranean fever (FMF) in Lebanon and Jordan: a population genetics study and report of three novel mutations. Eur J Med Genet 48:412–420. doi:10.1016/j.ejmg.2005.05.010
Ayesh SK, Nassar SM, Al-Sharef WA et al (2005) Genetic screening of familial Mediterranean fever mutations in the Palestinian population. Saudi Med J 26:732–737
Medlej-Hashim M, Rawashdeh M, Chouery E et al (2000) Genetic screening of fourteen mutations in Jordanian familial Mediterranean fever patients. Hum Mutat 15:384. doi:10.1002/(SICI)1098-1004(200004)15:4<384::AID-HUMU19>3.0.CO;2-U
Sabbagh AS, Ghasham M, Abdel Khalek R, et al (2008) MEFV gene mutations spectrum among Lebanese patients referred for Familial Mediterranean Fever work-up: experience of a major tertiary care center. Mol Biol Rep 35:447–451
Aksentijevich I, Torosyan Y, Samuels J et al (1999) Mutation and haplotype studies of familial Mediterranean fever reveal new ancestral relationships and evidence for a high carrier frequency with reduced penetrance in the Ashkenazi Jewish population. Am J Hum Genet 64:949–962. doi:10.1086/302327
Acknowledgments
I would like to thank Mrs Sumaya Al-Barrawi for technical assistance. I would also like to thank Prof. Ibrahim Othman, the Director General of AECS, and Dr. Nizar MirAli, Head of Department, for their support. This project was financially supported by Atomic Energy Commission of Syria (AECS).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jarjour, R.A. Familial Mediterranean fever in Syrian patients: MEFV gene mutations and genotype–phenotype correlation. Mol Biol Rep 37, 1–5 (2010). https://doi.org/10.1007/s11033-009-9475-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-009-9475-9