
Abstract
Familial Mediterranean fever (FMF) is the most common hereditary inflammatory periodic disease, characterized by recurrent episodes of fever, abdominal pain, synovitis and pleurisy. The aim of this study was to determine the frequency and distribution of Mediterranean fever (MEFV) gene mutations and to investigate the clinical characteristics and genotype–phenotype correlation in patients with FMF in Aydın, a province in western Anatolia, Turkey. Therefore, we retrospectively analysed MEFVgene mutations in 383 patients with suspected FMF and the clinical features of 327 among them. The MEFV gene mutations were investigated using the reverse dot-blot hybridization technique. We detected 26 different genotypes and 11 different mutations. The most common mutations in our cohort were p.M694V (41.15%), p.E148Q (20.35%), p.M680I(G/C) (12.39%) and p.R761H (9.73%). Abdominal pain (86.2%), fever (80.7%), arthralgia (57.2%), vomiting (36.1%), arthritis (34.6%), fatigue (31.5%), anorexia (22.9%) and chest pain (19.0%) were the most prevalent clinical features in our patients. This is the first study from Aydın in which the distribution of MEFVgene mutations and clinical features were evaluated in patients with FMF. We found that the most common mutation was p.M694V in our region, while the frequency of the p.R761H mutation was higher compared to other regions of Turkey with respect to extracted data from previous similar studies. Presented results supported the clinical findings in the literature that the homozygous p.M694V and compound heterozygous genotype were associated with more severe courses in FMF patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Familial Mediterranean fever (FMF, MIM# 249100) is inherited as an autosomal recessive disease, is particularly common in populations of Mediterranean ancestry: Turks, Armenians, nonAshkenazi Jews and Arabs (Touitou 2001). It is characterized by recurrent episodes of fever accompanied by abdominal pain, synovitis, pleurisy, or erysipelas-like rashes. The major complication of FMF is renal failure secondary to renal AA amyloidosis (Ben-Chetrit and Touitou 2012). The estimated prevalence of FMF is about 1/1000, and the carrier frequency is 20% in the Turkish population (Tunca et al. 2005). FMF is treated with oral colchicine to prevent future attacks and the development of reactive AA amyloidosis (Tunca et al. 2005).
The FMF disease is caused by mutations in the Mediterranean fever (MEFV) gene located on the short arm of chromosome 16p13.3. The gene consists of 10 exons and encodes a pyrin protein (also called marenostrin) consisting of 781 amino acids (Consortium 1997). Although the exact mechanism of pyrin action has not yet been determined, it is considered to be a negative inflammation regulator (Papin et al. 2007). To date, more than 300 gene alterations (mutations or polymorphisms) located in the MEFV gene have been identified (Touitou et al. 2004). In the Middle East, about 85% of all FMF patients have one of the following MEFV mutations: p.M694V, p.M694I, p.M680I, p.V726A, or p.E148Q (Ben-Chetrit and Touitou 2009). Genotype and phenotype correlations have not been explained definitively in patients with FMF. However, in several studies, the p.M694V mutation was reported to have a relatively severe clinical course, whereas p.V726A and p.E148Q have been correlated with a milder disease course (Jarjour 2010; Ece et al. 2014). MEFV gene mutations and genotype–phenotype correlations also cause different clinical manifestations in various ethnic groups and geographic regions.
We aimed to determine the frequency and spectrum of MEFV gene mutations in the Aydın region in western Anatolia, and to investigate the clinical characteristics, gender and genotype–phenotype association with MEFV gene mutations in our patients.
Materials and methods
In this study, the medical records of 383 FMF patients were reviewed retrospectively. They were referred to our laboratory and clinic (327 of the 383 came to the clinic) of Medical Genetics Departments, Faculty of Medicine, Adnan Menderes University for MEFV gene mutation analysis and clinical evaluation over three years. The clinical and demographical characteristics and MEFV gene mutation results were recorded and retrospectively analysed. A questionnaire requested the main clinical manifestations and features such as age, gender, age at onset of the disease, duration and frequency of the attacks, presence of arthritis, arthralgia, fever, abdominal pain, erysipelas-like erythema, pleurisy, headache, vomiting, diarrhea, constipation, myalgia, fatigue, family history of FMF or renal failure, colchicine usage, appendectomy, proteinuria and amyloidosis. Patients who benefited from colchicine treatment and used it regularly, designated as colchicine usage. The information was registered on a standard form. All patients were Turkish and living mainly in Aydın in Western Anatolia. The study protocol was approved by the local Ethical Committee.
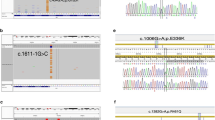
Total genomic DNA was isolated from peripheral blood samples with EDTA using a DNA extraction kit according to manufacturer’s instructions (Invitek Blood Kit, Berlin Germany). The DNA concentration was determined using a Nano-Drop spectrophotometer (Thermo-Scientific, Wilmington, USA) and samples were stored at −20 ∘C until polymerase chain reaction (PCR). Twelve common MEFV gene mutations located in exon 2, p.E148Q (c.442G >C, rs3743930); exon 3, p.P369S (c.1105C >T, rs11466023); exon 5, p.F479L (c.1437C >G, rs104895083); and exon 10, p.M680I (c.2040G >C, rs28940580), p.M680I (c.2040G >A), p.M694V (c.2080A >G, rs61752717), p.M694I (c.2082G >A, rs28940578), p.I692del (c.2076_2078del, rs104895093), p.K695R (c.2084A >G, rs104895094), p.V726A (c.2177T >C, rs28940579), p.A744S (c.2230G >T, rs61732874), and p.R761H (c.2282G >A, rs104895097) were detected via a reverse dot-blot (RDB) hybridization kit (Vienna Lab, FMF StripAssay, Vienna Austria). The assay includes four successive steps for which reagents are provided: (i) DNA isolation from blood samples, (ii) multiplex PCR was performed using biotinylated primers for exon 2, 3, 5 and 10 amplification, (iii) hybridization of PCR products to the strip absorbed immobilized wild type and mutated oligonucleotide probes, and (iv) hybridizations were illuminated by the reaction of streptavidin–alkaline phosphatase and colour substrate. The representative reverse dot-blot pictures of the genotypes are shown in figure 1 in electronic supplementary material at http://www.ias.ac.in/jgenet/.
We classified patients with mutation in the MEFV gene into two groups according to either compound heterozygote (group 1; n = 32) and heterozygote (group 2; n = 124) genotypes status. In addition to that, patients were classified into three groups according to the p.M694V allele status for genotype–phenotype correlations study of p.M694V: group 3 (n = 14) included patients with p.M694V/M694V; group 4 (n = 65) included patients with p.M694V/others; and group 5 (n = 96) included patients with genotypes other than p.M694V. The groups were compared with each other in terms of gender, presence of arthritis, arthralgia, fever, abdominal pain, erysipelas-like erythema, pleurisy, headache, vomiting, diarrhea, constipation, myalgia, fatigue, family history of FMF or renal failure, colchicine usage, appendectomy, proteinuria and amyloidosis.
Power analysis was performed for determining the minimum number of participants required to be involved in the study. The study needed at least 363 participants to have 80% power with an α= 0.05 level and 10% tolerance. Therefore, 383 patients are sufficient for the statistical safety of the results according to power analysis in this study. Statistical analyses were performed with SPSS 15.0 (Chicago, USA). The data were given as the median value (25th–75th percentiles) and frequency. Chi-square or Fisher exact tests were used to compare genotype–phenotype correlations and gender-related differences in the mutation types; P < 0.05 was considered statistically significant.
Results
MEFV gene mutations
In the present study, no mutations were found in 208 patients (54.3%), while at least one mutation was found in 175 (45.7%) patients. Twenty-six distinct genotypes and 11 distinct mutations were detected in these patients. Out of 175 patients, 124 (70.83%) were heterozygous, 32 (18.25%) were compound heterozygous and 19 (10.58%) were homozygous genotypes (table 1). The most common mutation was p.M694V with a frequency of 41.15%, followed by p.E148Q (20.35%), p.M680I(G/C) (12.39%), p.R761H (9.73%) and p.V726A (7.08%). Additionally, the p.A744S, p.F479L, p.M694I and p.K695R mutations were observed as rare mutations of the MEFVgene in our cohort, at 0.88, 0.88, 0.44 and 0.44% frequency, respectively. No patients had the p.I692del mutation (table 2). Upon analysing the distribution of patients’ genotypes, we found that the most common genotypes were p.M694V/Wt, p.E148Q/Wt, p.M694V/M694V and p.M680I(G/C)/Wt, which were found in 46 (26.28%), 35 (20.0%), 14 (8.0%), and 13 (7.43%) of these patients, respectively.
Clinical features
The study group consisted of 383 patients (214 females, 169 males; female/male ratio of 1.27 : 1.0) with FMF and a median age of 8 years old (range 8–29). The median age at disease onset was 9 years old (range 9–13). The age at symptoms onset was between 0–9 years old in 172 patients (52%), followed by 10–19 years old in 99 patients (30%) and 20–29 years old in 32 (10%) of patients. Most patients (46%) had attacks lasting 24–72 h and 52% had 1–10 attacks per year (figure 1). A weak negative correlation was observed between the duration of attacks and number of attacks per year in patients (Pearson R = −0.128, P = 0.021). We also analysed the frequency and duration of attacks for each MEFV gene genotype. The frequencies of attack were between 1 and 10 attacks per year in majority of genotypes. The attacks resolved within three days in majority of genotypes, but the attacks lasted four or more days in a small number of our patients (figure 2). Typically, the attacks in FMF patients usually resolve approximately three days, and they vary in frequency from once a week to several times per year in the literature.

Duration (in days) and frequency (per year) of FMF attacks.

Genotype–phenotype correlation of each MEFV gene genotypes. (a) Frequency of attacks for each genotype (times per year). (b) Duration of attacks for each genotype (days).
The most frequent clinical findings were abdominal pain (86.2%), fever (80.7%), arthralgia (57.2%), vomiting (36.1%), arthritis (34.6%), fatigue (31.5%), anorexia (22.9%) and chest pain (19.0%). Also, 141 (43.1%) patients had a positive FMF history in their family. Ninety patients received oral colchicine regularly (table 3). Twenty-nine patients (8.9%) underwent surgery, all of which were appendectomies. Sixteen out of the 29 patients had a mutation in the MEFV gene and of these, the most common genotype was homozygous p.M694V. Only one patient presented as phenotype 2.
Genotype–phenotype correlation
In this study, we compared the three groups 3, 4 and 5 for the evaluation of genotype–phenotype correlations of the p.M694V mutation. Patients with the homozygous p.M694V genotype had higher frequencies of recurrent fever, arthralgia, arthritis, appendectomy, proteinuria, constipation and colchicine usage compared to other groups (table 4). There were statistically significant differences in colchicine usage, family history of FMF fever and myalgia between groups 4 and 5. In contrast, this cohort had no correlation with recurrent abdominal pain and amyloidosis. Also, we assessed an additional two groups of patients with compound heterozygote or heterozygote genotype (table 5). Patients with compound heterozygote more commonly experienced abdominal pain (P = 0.002), fever (P = 0.007), chest pain (P = 0.009), constipation (P = 0.015), appendectomy (P = 0.018) proteinuria (P = 0.006) and colchicine usage (P < 0.001). There were no statistically significant differences between the groups other clinical features are provided in supplementary tables 1 and 2.
Discussion
In this study, we investigated the frequency of 12 common mutations of the MEFV gene in 383 Turkish patients with FMF as well as clinical manifestations and the genotype–phenotype correlations in 327 of those patients. Evaluating the MEFV gene mutations, we identified that 45.7% of patients had at least one mutation, varying between heterozygous (70.83%), compound heterozygous (18.25%) and homozygous (10.58%). However, we did not detect any complex genotypes (the presence of mutations in three or more alleles) in our cohort. Lack of any complex genotypes and low frequency of homozygotes may partly be explained by the lower rate of consanguineous marriages in our region compared to other parts of Turkey. In a recent study, investigating consanguineous marriage rates with regard to different regions of Turkey, the highest rate was detected in the eastern region of Turkey (34.4%) and the lowest rates (11–13%) were in western Turkey (our study region) (Tunca et al. 2005; Akbayram et al. 2009). Analysing the distribution of patients’ genotypes, we found that the most common genotypes were p.M694V/Wt, p.E148Q/Wt, p.M694V/M694V and p.M680I(G/C)/Wt. The inheritance pattern of FMF is autosomal recessive, implying that only patients carrying two mutant alleles are symptomatic. However, many studies have shown that there are clinically diagnosed FMF patients who carry one or zero mutation in the MEFV gene (Inal et al. 2009; Akin et al. 2010; Dundar et al. 2011; Ozdemir et al. 2011; Kishida et al. 2014). In our study, only 13% of patients carried two mutant alleles, in agreement with the hypothesis that one mutant allele may be associated with mild FMF symptoms (Ceylan et al. 2012). In addition, we must consider that there might be rarer or unknown mutations in the MEFV gene, which are not contained on the strip assay.
MEFV gene mutations have high allelic heterogeneity in Turkish patients (Tunca et al. 2005; Oztuzcu et al. 2014). Over 300 mutations in MEFV gene have been recorded in the Infevers database, the most common of which are p.M694V, p.M694I, p.V726A, p.M680I and p.E148Q (Touitou et al. 2004). These five hot-spot mutations account for more than 85% of mutations in classically-affected ethnic populations (Turks, Arabs, Armenians and Jews) (Ben-Chetrit and Touitou 2009). The five most common mutations in our study were p.M694V, p.E148Q, p.M680I, p.R761H and p.V726A with a combined frequency of 90.7%. The frequency of p.R761H mutation in this study was different from other studies in Turkey. The p.R761H mutation was detected more frequently in our population, found in 9.73% of patients. In addition to that, the number of homozygote individuals for M694V, R761H and M680I (G >C) were 14, 3 and 2 in our study respectively, but these were zero in the Exome Aggregation Consortium (ExAC) (2015) database.
In our study population we detected no mutation in 208 patients (54.3%). In other studies from Turkey, the ratio of finding no mutation in patients ranged between 38.2 and 61.4% (Akin et al. 2010; Dundar et al. 2011; Ece et al. 2014; Oztuzcu et al. 2014). This high rate of failure to find a mutation in these patients may be due to many factors, including the presence of other relatively rarer mutations, unknown mutations, genetic heterogeneity or detection of limited number of mutations via strip assay method.
In the present study, the most common mutation was p.M694V, identified in 79 patients. The allele frequency was 41.15%, similar to the percentage that has been reported in Turkish patients with FMF (reported between 14.6 and 51.4% of patients) (Tunca et al. 2005; Akin et al. 2010; Dundar et al. 2011; Ozdemir et al. 2011; Oztuzcu et al. 2014; Coşkun et al. 2015). The p.M694V mutation is common in Turks, Arabs, Armenians and Jews. Homozygote p.M694V mutation was related to a more severe clinical course, earlier onset and amyloidosis. However, Yalçinkaya et al. (2000) reported that MEFV mutations did not appear to be sufficient to explain the development of amyloidosis in Turkish FMF patients. Tunca et al. (2005) reported that patients with homozygote p.M694V genotype were shown to have an earlier age of onset and higher frequencies of arthritis and arthralgia, but there was no association with fever, abdominal pain, or amyloidosis. However, amyloidosis was remarkably frequent in their patients, prevalent even among patients with a disease onset occurring after age 40. We found that the homozygous p.M694V was associated with fever, arthritis, appendectomy and proteinuria, but not amyloidosis. Also, the compound heterozygous genotype was significantly related to a more severe course compared to the heterozygous genotype in FMF patients.
In the present study, p.E148Q was the second most common mutation, found in 20.35% of patients. The vast majority of p.E148Q mutations were in heterozygous form (n = 35, 20%), followed by compound heterozygous (n = 11, 6.27%). In agreement with our study, p.E148Q is one of the hot-spot mutations in all the reports and was found as the second most frequent mutation in many studies from Turkey (Ozdemir et al. 2011; Gunesacar et al. 2014, Oztuzcu et al. 2014; Coşkun et al. 2015). However, in a study from the southern region of Turkey, the p.E148Q mutation was shown to be the most common mutation in FMF patients (Ece et al. 2014; Uluca et al. 2015).
The p.M680I(G/C) was the third most common mutation in our group, followed by p.R761H and p.V726A (12.39%, 9.73% and 7.08%, respectively). p.M680I mutation was reported to be the second most common mutation only in Armenians and Turks (Touitou 2001). We detected two types of mutations of p.M680I. While p.M680I(G/C) (12.39%) was a relatively frequent mutation, p.M680I(G/A) (2.21%) was very rare in this study.
The p.R761H mutation is one of rare mutations of the MEFV gene in other studies from Turkey, but it was the fourth most common mutation observed in our study. The frequency of p.R761H mutation was found to range between 0.55 and 4.96% in large-scale studies of the Turkish population (Ozdemir et al. 2011; Gunesacar et al. 2014; Oztuzcu et al. 2014; Coşkun et al. 2015). The p.R761H was previously detected in the Syrian, Lebanese and Palestinian patients but not in Jordanians. According to one study, p.R761H mutation frequency was 4.4% in Syrian patients (Jarjour 2010). The p.R761H mutation was reported particularly frequently in Turkish FMF patients by Demirkaya et al. (2008) and all the mutations of p.R761H were compound heterozygote status in their study group. The p.R761H mutations were shown as either compound or heterozygous, but homozygous was not reported in literature as of 2007. In addition to that, another study reported that p.R761H is quite common in the Turkish population (Touitou 2001; Demirkaya et al. 2008). The p.R761H homozygote mutation was reported as the first case in literature in 2009 (Ureten et al. 2010). We also detected p.R761H heterozygote mutation in nine (5.14%) patients, homozygote mutation in three (1.71%) patients and compound heterozygote in seven (3.99%) patients. Our study showed the p.R761H mutation frequency was 9.73%, higher than a previous study group with the rate of 3.48% (Demirkaya et al. 2008).
We evaluated the age at disease onset in our patients. The disease onset was at age 0–9 years old in 52% and at age 10–19 years old in 30% of patients. These results show that disease onset was prior to 20 years of age in 82% of patients. Therefore, it is important to diagnose and treat FMF in childhood, to prevent the development of amyloidosis.
In our patients, the most common clinical features were abdominal pain, fever and arthralgia. Also, the most common symptoms were vomiting, fatigue and anorexia, which were not included as Tel–Hashomer criteria (Livneh et al. 1997). Anorexia was especially common in children. Frequencies of FMF clinical features in previous studies from other ethnic groups (Armenians, Jews and Arabs) have been reported as follows: fever, 100%; peritonitis, 82–96%; pleurisy, 40–87%; arthritis, 37–77%; and erysipelas-like erythema 3–46% (Sohar et al. 1967; Schwabe and Peters 1974; Rawashdeh and Majeed 1996). In studies on the Turkish population, frequencies of FMF clinical symptoms were reported as follows: fever, 92.5–95.2%; abdominal pain, 93.7–94.4%; chest pain, 13.7–31.2%; arthritis, 33.9–47.4% and erysipelas-like erythema, 4–20.9% (Tunca et al. 2005; Inal et al. 2009). In our study, fever and abdominal pain frequencies of our patients were found to be lower than those of previous reports. The milder disease course may be related to the lower frequencies of homozygous and compound heterozygous mutations in our study group compared with other reports. In a recent Japanese study, Kishida et al. (2014) reported that the main clinical symptoms and frequencies were fever in 83.6%, abdominal pain in 62.1%, pleurisy in 45.7%, arthritis in 41.4% and rash or erysipelas-like erythema in 6.8% of FMF patients. Also, in a study from Turkey by Ozalkaya et al. (2011), frequencies of clinical features including abdominal pain (83.1%), fever (55%), arthritis (17.1%), myalgia (4.5%), pleurisy (10%) and erysipelas-like erythema (7.7%) were reported in FMF patients.
Although most studies reported that FMF affects both genders in similar ratio, some reports are in accordance with female predominance in patients with FMF (Ozdemir et al. 2011; Ece et al. 2014; Oztuzcu et al. 2014). In the present study, we detected female predominance (1.27 : 1). In addition, we investigated the comparison of the main mutation groups as heterozygote, homozygote and compound heterozygote genotypes in female and male patients (table 6). There was no significant difference between groups (P = 0.231), which was in accordance with the results of Dundar et al. (2011).
In conclusion, to our knowledge, this is the first report from Aydın, and the study evaluated the distribution of mutations of the MEFV gene, clinical symptoms and the genotype–phenotype correlations in patients with FMF. We confirmed that the most common mutations were p.M694V and p.E148Q. The distribution of mutations was similar to that of other regions of Turkey. However, the frequency of the p.R761H mutation was higher compared to other regions of Turkey as reported in English literature. Since there are many ethnic groups in Turkey, our study group also confirmed the mutational heterogeneity of FMF. The RDB hybridization is a reliable, rapid and time-saving method. However, this technique can only screen a limited number of mutations and is not sufficient for detecting rare and unknown mutation. Therefore, investigating the whole MEFV gene via advanced analysis techniques could be useful for detection of uncommon or novel mutations. The homozygous p.M694V was associated with fever, arthritis, appendectomy and proteinuria. In addition, the compound heterozygous genotype was associated with a more severe course compared to heterozygous genotype in FMF patients. Further prospective comprehensive studies with more patients are necessary to verify our results.
References
Akbayram S., Sari N., Akgün C., Doğan M., Tuncer O., Caksen H. et al. 2009 The frequency of consanguineous marriage in eastern Turkey. Genet. Couns. 20, 207–214.
Akin H., Onay H., Turker E., Cogulu O. and Ozkinay F. 2010 MEFV mutations in patients with familial Mediterranean fever from the Aegean region of Turkey. Mol. Biol. Rep. 37, 93–98.
Ben-Chetrit E. and Touitou I. 2009 Familial Mediterranean fever in the world. Arthritis Rheum. 61, 1447–1453.
Ben-Chetrit E. and Touitou I. 2012 The impact of MEFV gene identification on FMF: an appraisal after 15 years. Clin. Exp. Rheumatol. 30, S3–S6.
Ceylan G. G., Ceylan C. and Ozturk E. 2012 Frequency of alterations in the MEFV gene and clinical signs in familial Mediterranean fever in Central Anatolia, Turkey. Genet. Mol. Res. 11, 1185–1194.
Consortium F. F. 1997 A candidate gene for familial Mediterranean fever. Nat. Genet. 17, 25–31.
Coşkun S., Ustyol L., Bayram Y., Selçuk Bektaş M., Gulsen S., Çim A. et al. 2015 The spectrum of MEFV gene mutations and genotypes in Van province, the eastern region of Turkey, and report of a novel mutation (R361T). Gene 562, 128–131.
Demirkaya E., Tunca Y., Gok F., Ozen S. and Gul D. 2008 A very frequent mutation and remarkable association of R761H with M694V mutations in Turkish familial Mediterranean fever patients. Clin. Rheumatol. 27, 729–732.
Dundar M., Emirogullari E. F., Kiraz A., Taheri S. and Baskol M. 2011 Common familial Mediterranean fever gene mutations in a Turkish cohort. Mol. Biol. Rep. 38, 5065–5069.
Ece A., Cakmak E., Uluca U., Kelekci S., Yolbas I., Gunes A. et al. 2014 The MEFV mutations and their clinical correlations in children with familial Mediterranean fever in southeast Turkey. Rheumatol. Int. 34, 207–212.
Exome Aggregation Consortium (ExAC) 2015 C., MA (http://exac.broadinstitute.org) (accessed 4 of April 2015).
Gunesacar R., Celik M. M., Arica V., Elmacioglu S. and Ozturk O. H. 2014 Frequency of MEFV gene mutations in Hatay province, Mediterranean region of Turkey and report of a novel missense mutation (I247V). Gene 546, 195–199.
Inal A., Yilmaz M., Kendirli S. G., Altintas D. U. and Karakoc G. B. 2009 The clinical and genetical features of 124 childrenwith familial Mediterranean fever: experience of a single tertiary center. Rheumatol. Int. 29, 1279–1285.
Jarjour R. A. 2010 Familial Mediterranean fever in Syrian patients: MEFV gene mutations and genotype–phenotype correlation. Mol. Biol. Rep. 37, 1–5.
Kishida D., Nakamura A., Yazaki M., Tsuchiya-Suzuki A., Matsuda M. and Ikeda S. 2014 Genotype–phenotype correlation in Japanese patients with familial Mediterranean fever: differences in genotype and clinical features between Japanese and Mediterranean populations. Arthritis Res. Ther. 16, 439.
Livneh A., Langevitz P., Zemer D., Zaks N., Kees S., Lidar T. et al. 1997 Criteria for the diagnosis of familial Mediterranean fever. Arthritis Rheum. 40, 1879–1885.
Ozalkaya E., Mir S., Sozeri B., Berdeli A., Mutlubas F. and Cura A. 2011 Familial Mediterranean fever gene mutation frequencies and genotype–phenotype correlations in the Aegean region of Turkey. Rheumatol. Int. 31, 779–784.
Ozdemir O., Sezgin I., Kurtulgan H. K., Candan F., Koksal B., Sumer H. et al. 2011 Prevalence of known mutations in the MEFV gene in a population screening with high rate of carriers. Mol. Biol. Rep. 38, 3195–3200.
Oztuzcu S., Ulasli M., Ergun S., Igci Y. Z., Igci M., Bayraktar R. et al. 2014 Screening of common and novel familial Mediterranean fever mutations in south-east part of Turkey. Mol. Biol. Rep. 41, 2601–2607.
Papin S., Cuenin S., Agostini L., Martinon F., Werner S., Beer H. -D. et al. 2007 The SPRY domain of Pyrin, mutated in familial Mediterranean fever patients, interacts with inflammasome components and inhibits proIL-1beta processing. Cell Death Differ. 14, 1457–1466.
Rawashdeh M. O. and Majeed H. A. 1996 Familial Mediterranean fever in Arab children: the high prevalence and gene frequency. Eur. J. Pediatr. 155, 540–544.
Schwabe A. D. and Peters R. S. 1974 Familial Mediterranean fever in Armenians: analysis of 100 cases. Medicine (Baltimore) 53, 453–462.
Sohar E., Gafni J., Pras M. and Heller H. 1967 Familial Mediterranean fever: a survey of 470 cases and review of the literature. Am. J. Med. 43, 227–253.
Touitou I. 2001 The spectrum of familial Mediterranean fever (FMF) mutations. Eur. J. Hum. Genet. 9, 473–483.
Touitou I., Lesage S., McDermott M., Cuisset L., Hoffman H., Dode C. et al. 2004 Infevers: an evolving mutation database for auto-inflammatory syndromes. Hum. Mutat. 24, 194–198.
Tunca M., Akar S., Onen F., Ozdogan H., Kasapcopur O., Yalcinkaya F. et al. 2005 Familial Mediterranean fever (FMF) in Turkey: results of a nationwide multicenter study. Medicine (Baltimore) 84, 1–11.
Uluca Ü., Ece A., Şen V., Coşkun S., Güneş A., Yel S. et al. 2015 High frequency of E148Q sequence variation in children with familial Mediterranean fever in southeast Turkey. Arch. Argent. Pediatr. 113, 133–140.
Ureten K., Gönülalan G., Akbal E., Güneş F., Akyürek O., Ozbek M. et al. 2010 Demographic, clinical and mutational characteristics of Turkish familial mediterranean fever patients: results of a single center in Central Anatolia. Rheumatol. Int. 30, 911–915.
Yalçinkaya F., Tekin M., Cakar N., Akar E., Akar N. and Tümer N. 2000 Familial mediterranean fever and systemic amyloidosis in untreated Turkish patients. QJM 93, 681–684.
Author information
Authors and Affiliations
Corresponding author
Additional information
[Coşkun S., Kurtgöz S., Keskin E., Sönmez F. and Bozkurt G. 2015 Frequency of mutations in Mediterranean fever gene, with gender and genotype–phenotype correlations in a Turkish population . J. Genet. 94, xx–xx]
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
COŞKU, S., KURTGÖZ, S., KESKIN, E. et al. Frequency of mutations in Mediterranean fever gene, with gender and genotype–phenotype correlations in a Turkish population. J Genet 94, 629–635 (2015). https://doi.org/10.1007/s12041-015-0568-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12041-015-0568-z