
Abstract
Purpose
Estimating the underlying demand for immunoglobulin (Ig) is important to ensure that adequate provision is made for patients with primary immune deficiency (PID) in the context of the competing demands for Ig and to ensure optimal therapeutic regimens. The concept of latent therapeutic demand (LTD) was used to estimate evidence-based requirements and compared to the actual Ig consumption in different countries. The estimates were performed for common variable immunodeficiency (CVID) and X-linked Agammaglobulinaemia (XLA), the two most commonly studied PIDs using Ig.
Methods
The LTD model for CVID and XLA was derived using decision analysis methodology. Data for the epidemiology and treatment variables were obtained from peer-reviewed publications, clinical registries and publicly-available patient surveys. Incomplete data records from registries were excluded from analysis. The variables impacting LTD were ranked in order of sensitivity through a tornado diagram. The uncertainty surrounding the variables was modeled using probabilistic distributions and evaluated using Monte Carlo simulation.
Results
Treatment dosage and prevalence were determined to be the most sensitive variables driving demand. The average potential usage of Ig for the treatment of CVID and XLA was estimated at 72 g per 1,000 population, which is higher than the estimated Ig usage in CVID and XLA of 27–41 g per 1,000 population in the US.
Conclusion
The potential demand for treating CVID and XLA exceeds the currently observed usage of Ig in these disorders. Variable usage in different countries is due to varying prevalence and dosage practices. Under-reporting in patient registries represents a major obstacle to calculating the true prevalence of CVID and XLA. Modeling demand relies heavily upon accurate prevalence and practice estimates which reemphasize the importance of accurate registries and improved registry methods. As better data becomes available, revision of model variables provides opportunities to anticipate and prepare for evolving patient needs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Therapeutic preparations of polyclonal immunoglobulin G (Ig) have enhanced significantly the survival and quality of life of patients with a number of primary immunodeficiencies (PID) [1, 2]. The treatment of PID has evolved over the past 60 years as improvements in manufacturing technology have allowed high concentrations of Ig to be delivered safely with normal molecular structure and functionality [3, 4]. This has contributed to a substantial and continuing increase in the use of Ig over the past 20 years [5]. A number of other diseases are treated by Ig, particularly autoimmune disorders, including several neuropathies [6], which have resulted in this product’s key position in the therapeutic armamentarium and in the economics of the plasma fractionation industry.
The sourcing of Ig from human plasma makes it an inherently limited resource, and its usage varies greatly between countries [7], even when health care resources and general economic conditions are similar. This has drawn scrutiny on the usage of Ig and a number of guidelines have been developed, aimed at ensuring that usage is evidence-based [8, 9].
Despite data showing that usage is drawn from approved, evidence-based indications, applications of these criteria has not moderated the continuing increase of Ig consumption [10]. These data also demonstrate that the Ig treatment of PID constitutes approximately 20–30 % of all Ig usage [11]. The variation in Ig usage has led to suggestions that outcomes are not inferior in countries which used evidence-based guidelines to shape clinical use, and that higher than average usage should be questioned [12]. Hence, an understanding of the basis for Ig usage in PID is important to ensure continued access of this therapy by the prescriber and patient community. Given that many of the key clinical variables which may be expected to affect usage, such as treatment dosage and disease prevalence vary and are still subject to debate and uncertainty [13, 14], such an estimate is challenging.
Decision analysis may be useful in making choices when the consequences of action are uncertain [15]. We have previously described [16, 17] the use of decision analysis modeling to estimate the demand of coagulation Factor VIII (FVIII) concentrate in treating hemophilia A in the event of such treatment being unconstrained by any factors other than evidence-based clinical and epidemiological findings. In this study, we have applied similar methods to develop a model for the assessment of latent clinical demand (LTD) for Ig in the treatment of two major humoral primary immunodeficiencies—common variable immunodeficiency (CVID) and X-linked Agammaglobulinaemia (XLA). We define LTD as the underlying demand that represents how physicians would prescribe treatment and how patients would comply with the prescribed treatment if ample supplies were available and affordable, and access to therapy was unencumbered by issues other than evidence-based clinical need, such as financial constraints. Through this approach, we sought to relate the estimated LTD for CVID and XLA to the current Ig consumption across a range of countries.
Materials and Methods
Model Structure
The LTD for Ig in CVID and XLA was modeled using decision analysis methodology. The variables determined to influence LTD are shown in Table I, while their relationships within the model are shown in the influence diagram (Fig. 1). The model identifies nine random variables, seven of which influence (or are influenced by) other variables (e.g., patient weight is influenced by patient gender and age group of patient). The remaining two random variables, prevalence and treatment rate, do not influence other random variables in Fig. 1. Data obtained for the epidemiological-related variables were used to calculate the number of patients with CVID and XLA. Data obtained for treatment-related variables were used to calculate the treatment volume (Ig consumed) per patient. LTD was derived from the product of the number of patients and treatment volume per patient.

The influence diagram model estimates the latent therapeutic demand (LTD) of CVID and XLA (amount of grams of Ig treatment for CVID and XLA consumed per 1,000 population) by multiplying the number of patients with CVID and XLA and the Ig treatment volume per patient (ovals correspond to uncertainties and rounded rectangles are equations)
The analysis was performed in Microsoft Excel and the decision analysis software DPL (Syncopation Software, Inc. DPL 7.0 Professional, 1623 Main Street Concord, MA 01742 USA 2008). Excel was used to provide the organizational structure of the data obtained for the epidemiological-related and treatment-related variables. Excel was also used to provide the equations for calculating the number of patients, treatment volume per patient, and the LTD. DPL provided the tree diagram structure for Fig. 1, generated the tornado diagram from the data obtained, and generated probability distribution for LTD using the Monte Carlo simulation feature of DPL.
Data Sources
Data for the epidemiological-related and treatment-related variables were extracted from the peer-reviewed medical literature, and from patient registries and surveys. The patient registry of the European Society for Immunodeficiencies (ESID) [18, 19] was the main source of registry data. ESID maintains an internet-based database for clinical and research data on patients with primary immunodeficiency diseases. Anonymous treatment data from the ESID Registry was provided by the Plasma Protein Therapeutics Association in accordance with the ESID Database data access and publication rules. The analysis was approved by the ESID Registry Steering Committee (see www.esid.org/registry for respective documents). Patient surveys were primarily drawn from the publically-available data of the United States patient advocacy group—Immune Deficiency Foundation (IDF) [20–24].
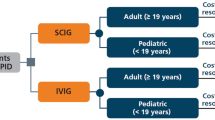
Treatment data (route of administration, treatment dosage, treatment frequency, and treatment compliance) were obtained from the ESID Registry on Sep. 14, 2011 [18]. At the time of this study, the ESID Registry included 4,016 clinical records for 2,065 patients with CVID and 1,151 clinical records for 623 patients with XLA. A patient can have multiple clinical records in the ESID Registry (e.g., when they change Ig treatment). To reduce the size and complexity of this large body of clinical records, specific inclusion criteria were developed (Fig. 2a and b). For example, the most-recent clinical record for each patient was included, thus eliminating multiple clinical records. Only clinical records that had complete treatment information were included. This resulted in 748 clinical records of CVID patients that were treated with IVIG (79 %) and 200 clinical records of CVID patients that were treated with SCIG (21 %), as well as 305 clinical records of XLA patients that were treated with IVIG (73 %) and 114 clinical records of XLA patients that were treated with SCIG (27 %).

a Process of selecting IVIG and SCIG treatment data for CVID b Process of selecting IVIG and SCIG treatment data for XLA
Analysis of Individual Variables
The sensitivity analysis of the LTD to the epidemiological-related and treatment-related variables was assessed by decision analysis. One-way (i.e., one variable at a time) sensitivity analysis was used to identify the variables that have the largest impact on LTD for CVID and XLA. The minimum and maximum values from the data obtained for each variable were used to analyze the sensitivity on LTD for each variable. The sensitivity of LTD from these variables was determined using a tornado diagram [25].
Probabilistic analysis of the epidemiological-related and treatment-related variables was used to generate a probability distribution of LTD. Table II describes the probability methods used for modeling the epidemiological-related and treatment-related variables. The uncertainty about a variable that has a discrete number of possible outcomes was modeled using a discrete probability distribution (e.g., patient gender). When the uncertainty about a variable has a continuum of possible outcomes the variable was modeled using a continuous probability distribution. For a continuous random variable when the data obtained were limited, the uniform or the triangular probability distribution was used (e.g., prevalence). For a continuous random variable when data were available, an empirical probability distribution of the data was derived and the extended Swanson-Megill approximation [26] was applied (e.g., treatment dosage). The extended Swanson-Megill approximation uses the 10th, 50th, and 90th percentiles of a probability distribution for a continuous random variable resulting in a three-point discrete probability distribution of the 10th, 50th, and 90th percentiles that are assigned probabilities of 0.3, 0.4, and 0.3, respectively.
Prevalence
Prevalence (the number of people alive diagnosed with CVID and XLA at a certain point in time) is expressed in this paper as the number of people with CVID and XLA per 100,000 population. The true prevalences of CVID and XLA are not known [13, 27, 28]. Table III shows country-specific prevalence data that were obtained either directly as reported in the literature or determined by dividing the number of patients with CVID and XLA in the country by its total population [29]. The minimum and maximum values from the prevalence data obtained in the open literature ranged from 0.11 to 30.01 per 100,000 population for CVID [13, 20, 30–42] and 0.09 to 11.25 per 100,000 population for XLA [30–35, 37–42]. These values were used in the one-way sensitivity analysis. The uncertainty about CVID prevalence was modeled with the triangular distribution using the above range for CVID and the epidemiological-based study of Joshi et al. [13] as the most-likely estimate (Table II). This model was used in the probabilistic analysis. There were no XLA cases reported in Joshi et al. [13] (personal communication, Joshi to Stonebraker, June 11, 2013). Since there was not an obvious most-likely estimate from analyzing the observed XLA prevalence data (Table III), the uncertainty about XLA prevalence was modeled with the uniform distribution using the above range estimates for XLA (Table II). This model was used in the probabilistic analysis.
Age Group of Patients
The age group classification in the IDF surveys [21–24] was used ≤12 years, 13–17 years, 18–29 years, 30–44 years, 45–64 years, and ≥65 years. The percentage of patients in each age group was determined from these surveys [21, 24] and the ESID data [18] and used in the one-way sensitivity analysis. The IDF age group data were from the total PID patient population, whereas the ESID age group data were specifically CVID and XLA patients. The uncertainty about the age group of CVID and XLA patients was modeled as a discrete random variable using the percentage of patients in age category from the ESID Registry [18] (Table II). This model was used in the probabilistic analysis.
Patient Gender
Patients with CVID and XLA are male or female. Gender data were obtained from the open literature [20–24, 27, 30, 35, 37, 40–43]. Since patient gender has binary outcomes, the percentage of male CVID and XLA patients was varied from 0 % (no males) to 100 % males in the one-way sensitivity analysis. The uncertainty about patient gender was modeled as a discrete binary random variable using the percentage of male CVID and XLA patients [27, 43] (Table II). This model was used in the probabilistic analysis.
Patient Weight
The weight distribution data from the Centers for Disease and Control (CDC) [44] was used, broken down by gender and age group. To address the discordance in alignment between the CDC general population age breakdown and the IDF age group data used for CVID and XLA patients, the technique of Klein and Schonborn [45] was used by dividing the age-specific counts in the CDC data [44] by the total counts in that age group. An empirical probability distribution for patient weight was derived for each male and female age grouping. The 10th and 90th percentiles were determined from this distribution and were used in the one-way sensitivity analysis. The uncertainty about patient weight by gender and age group was modeled using the extended Swanson-Megill [26] (Table II). This model was used in the probabilistic analysis.
Treatment Rate
Data for the proportion of patients treated with CVID and XLA were obtained from the open literature [19–24, 37, 46–48]. The minimum and maximum values from the treatment rate data ranged from 78 % to 92 % for CVID and 88.9 % to 94 % for XLA. These values were used in the one-way sensitivity analysis. The uncertainty about treatment rate was modeled with the uniform distribution using the above range (Table II). This model was used in the probabilistic analysis.
Route of Administration
The routes of administration for treating CVID and XLA are IVIG and SCIG. Since the route of administration has binary outcomes, the proportion of CVID and XLA patients was varied from 0 % (no IVIG, i.e., all SCIG treatment) to 100 % IVIG treatment in the one-way sensitivity analysis. The uncertainty about the route of administration was modeled as a discrete binary random variable using the proportion of CVID and XLA patients treated with IVIG from the ESID Registry [18] (Table II). This model was used in the probabilistic analysis.
Treatment Dosage
Data for the treatment dosage (milligrams of Ig per kilogram of patient weight) for patients with CVID and XLA was obtained from the ESID Registry [18]. The minimum and maximum values for IVIG treatment dosage ranged from 49 to 1,091 for CVID and 104 to 1,036 for XLA. The minimum and maximum values for SCIG treatment dosage ranged from 24 to 291 for CVID and 21 to 589 for XLA. These values were used in the one-way sensitivity analysis. An empirical probability distribution was derived from the data obtained for each treatment dosage (e.g., IVIG treatment dosage for CVID) and modeled by approximating the distribution using the extended Swanson-Megill [26] (Table II). This model was used in the probabilistic analysis.
Treatment Frequency
Data for the number of treatment episodes per year was obtained from the ESID Registry [18]. The minimum and maximum values for IVIG treatment frequency ranged from 6 to 26 for CVID and 4 to 26 for XLA. The minimum and maximum values for SCIG treatment frequency ranged from 24 to 365 for CVID and 12 to 208 for XLA. These values were used in the one-way sensitivity analysis. The uncertainty about treatment frequency was modeled as a discrete random variable using the data obtained from ESID [18] (Table II). This model was used in the probabilistic analysis.
Treatment Compliance
Compliance describes a patient’s behavior in adhering to a physician’s prescribed treatment and is rarely reported in the literature because of the difficulty in obtaining compliance data from physicians and/or patients. For example, CVID treatment compliance was reported in only one study [49]. Data from the ESID Registry [18] were obtained on the treatment compliance and the minimum and maximum values from these data were used in the one-way sensitivity analysis. The uncertainty about treatment compliance was modeled as a mixed (a discrete component and a continuous component) random variable using the data obtained from ESID [18] (Table II). This model was used in the probabilistic analysis.
Results
One-Way Sensitivity Analysis
To analyze the impact on LTD of the epidemiological-related and treatment-related variables, each variable was varied one at time using its minimum and maximum values while leaving the other variables set at their base-case values. The use of minimum and maximum values rather than a point estimate to describe the possible outcomes of a variable addresses the level of uncertainty for each variable. In the tornado diagram (Fig. 3), the length of the bar for each variable represents how sensitive LTD is to each variable. The tornado diagram is arranged such that the variable with the greatest impact on LTD is the longest bar and it is located at the top whereas the least sensitive is shown at the bottom of the diagram. Figure 3 demonstrates that the most sensitive variables are treatment dosage, prevalence, and treatment frequency. In contrast, changes in patient gender (male or female), treatment rate, age group of patients, and route of administration (IV or SC) will have little impact on LTD. Since the tornado diagram provides one-way sensitivity analysis, a probabilistic analysis was used to provide a coherent, comprehensive way of characterizing the uncertainty of LTD by evaluating all the possible outcomes of the variables simultaneously.

The tornado diagram shows the changes in latent therapeutic demand (LTD) of CVID and XLA that result from varying each variable sequentially over its range of possible (minimum and maximum) values while leaving the other variables set at their base-case values
Probabilistic Analysis
Probabilistic analysis (Monte Carlo simulation) evaluated LTD for all of the uncertain outcomes of the epidemiological-related and treatment-related random variables, including the influencing relationships among the variables in Fig. 1. Using the modeling inputs from Table II in the model depicted in Fig. 1 resulted in a probability distribution of LTD for CVID and XLA. The mean and standard deviation of the probability distribution of LTD for CVID and XLA are 72 ± 40 g per 1,000 population (with the LTD for CVID and XLA averaging 52 and 20 g per 1,000 population, respectively). Figure 4 compares this distribution to the total observed Ig usage for various countries [7]. The total observed Ig usage in most of the countries in Fig. 4 was less than the median (64 g per 1,000 population) of LTD for CVID and XLA. In some countries, the total observed Ig usage is less than the lower quartile of the probability distribution of LTD for CVID and XLA, whereas the total observed Ig usage for Canada (140.1 g per 1,000 population), United States (137.5 g per 1,000 population), Australia (120.7 g per 1,000 population, and France (97.4 g per 1,000 population) exceeded the upper quartile. However, all of the countries in Fig. 4 include not only Ig usage for CVID and XLA, but also Ig usage in other diseases. It has been observed that approximately 20–30 % of the total observed Ig usage is attributed to CVID and XLA [11]. If this is factored in, then all of the countries shown in Fig. 4 would be less than the median of LTD for CVID and XLA. For example, the Ig usage for CVID and XLA of Canada would be approximately 28 to 42 g per 1,000 population.

The box-and-whisker plot shows the median value, interquartile range (box), and the 5th and 95th percentiles (whiskers) for the probability distribution of latent therapeutic demand (LTD) for CVID and XLA when compared to the total observed immunoglobulin usage for various countries (shown as dots). The median is 64 g per 1,000 population, 25th and 75th percentiles are 43 and 92 g per 1,000 population, and the 5th and 95th percentiles are 23 and 148 g per population. The mean and standard deviation of the distribution are 72 ± 40 g per 1,000 population
Discussion
High-dose immunoglobulin therapy has evolved into an accepted strategy for a number of diseases. Analysis of Ig usage in a number of advanced economies suggests that the treatment of PIDs now constitutes a minority of the use [50]. The significant variation between different countries suggests that therapy across the range of Ig indications is still not uniform despite the presence of similar consensus guidelines on Ig use in immunodeficiency [1, 9, 47] and high Ig usage neurological indications [10, 51–53].
In a recent study comparing United States and European practice [48], concordance was found in the types of disease treated, but significant differences were reported on dosage and frequency of Ig treatment. Intriguingly, dosages and frequencies tended to be higher when recommended by European specialist physicians, despite the lower Ig usage in Europe compared to the United States. The most striking difference in this comparative study involved the perception of the risk to patients resulting from effects of reimbursement processes on the access to Ig therapy, with strong concerns reported by United States, but not European physicians.
Such concerns may be due to the overall higher Ig use, and higher costs, in the United States coupled with the predominantly private-insurance-based reimbursement in that country compared to the government-based reimbursement in Europe. However, treatment access pressures are highly visible also in Europe, whose payers, such as the United Kingdom government [51] have instituted demand management strategies aimed at ensuring that reimbursed Ig usage is evidence-based. In this climate of pressure on usage, estimating the underlying demand for Ig in PID is important to ensure that adequate provision is made for patients with immunodeficiency in the context of the competing demands for Ig.
We chose to model the LTD for two primary immunodeficiencies which utilize Ig – CVID and XLA – as these are the commonest PIDs which consume Ig. An estimate of the potential demand is a good indicator for the Ig needs for PID. Our choice of using decision analysis to model LTD for CVID and XLA was based on the uncertainty surrounding two key factors influencing usage of Ig in PID. The sensitivity analysis (in Fig. 3) demonstrates that CVID and XLA Ig dosage and prevalence are highly influential to LTD. For example, if the level of Ig treatment increases there would be an increase in the LTD of CVID and XLA. Similarly, if the actual prevalence of CVID and XLA is higher than what has been observed, there would be an increase of LTD.
Despite more than three decades of use, the optimal dose of Ig treatment for PIDs that is needed to minimize infection in most patients remains uncertain [1, 14, 47] with estimates ranging from 200 to 1200 mg/kg body weight [49]. The recommended dose is 400 mg/kg [54], to result in trough levels with IVIG of 500 mg/dl. However, a number of studies have demonstrated improved outcomes with higher doses [55–57]. With both IVIG and SCIG [14, 58], analysis of many trials demonstrates that lower infection rates continue to be experienced as the trough level (IVIG) and steady state (SCIG), respectively, are increased through dosages of 800–1000 mg/kg. Classifying the clinical phenotypes of CVID continues to be pursued as a possible route to identifying which patients benefit from particular approaches to Ig therapy. Quinti et al. [59] have proposed an approach including factors such as patient IgA levels, response to vaccination and loss of memory B cells [60], in addition to clinical features and IgG levels as proposed by Chapel et al. and others [61–63]. The role of diagnostic variation has also been demonstrated [64]. So far, these approaches and a large European trial [65] have failed to yield a reliable parameter as to which disease phenotype predicts the need for/approach to Ig therapy.
The true prevalence of CVID and XLA is uncertain. CVID constitutes a heterogeneous group of diseases whose genetic basis is in the majority unknown and likely to be polygenic [66] and whose disease prevalence has varied considerably (see below). As shown in Table III, there is high variability of the prevalence data reported in the literature. For example, other than the CVID prevalence data of 13.94 and 30.01 per 100,000 population from Joshi et al. [13] and Boyle and Buckley [32], respectively, the rest of the literature reported CVID prevalence data from registries that were under-reported and clustered around 1.0 per 100,000 population. In addition, the XLA prevalence data were under-reported and clustered around 0.2 per 100,000 population whereas the XLA prevalence from Boyle and Buckley [32] was 11.25 per 100,000 population. Incomplete records have introduce a bias in the prevalence data, and that for such data registries/studies specifically targeting prevalence (e.g., Joshi et al. [13]) are more reliable if they give more complete prevalence data even in the absence of more detailed clinical data.
The initial development of the LTD model reported at conferences [67] included cases of XLA from Joshi et al. [13]. Subsequent confirmation indicated that there were no XLA cases (personal communication, Joshi to Stonebraker June 11, 2013) requiring that the modeled maximum value of XLA be adjusted from 26.6 per 100,000 population to 11.25 per 100,000 population [32]. This resulted in a substantial decrease of the LTD of XLA from 48 g per 1,000 population as initially reported [67] to 20 g per 1,000 population in this study. This results in a more robust estimate of XLA LTD, and illustrates the difficulty in acquiring reliable data of prevalence for PIDs to inform models such as ours.
Difficulties in determining true prevalence place limitations on such models, but our results have implications for policy makers and others involved in the delivery of immunoglobulin therapy. The finding that the potential usage of Ig for PID (CVID and XLA) averages 72 g per 1,000 population suggests that Ig usage in most countries is still considerably below the potential demand. For example, when using its published CVID and XLA prevalence [39] the mean LTD for Canada was 5.5 g per 1,000 population. This represents only 3 % of Canada’s total Ig usage of 140.1 g per 1,000 population. The total observed Ig usage values in Table III include the Ig usage for CVID and XLA and other disease indications [7], but data from a range of sources indicates that PIDs account for 20–30 % of overall use [11]. Hence, using published data for specific countries’ prevalence generated from most current mechanisms projects lower Ig consumption than is actually observed, even in a clinical landscape of potentially higher LTD.
Analysis of Ig usage data from Australia, a country with a high overall Ig usage of 120.7 g per 1,000 population [10] and a strictly monitored evidence-based issue policy shows that the total Ig usage for PIDs is around 15 % of this amount at 21 g per 1,000 population, about a third of the estimated latent demand for the two main primary immunodeficiencies. The prevalence of CVID and XLA in Australia has been reported as 1.88 and 0.32 per 100,000, respectively [37]. The estimate for XLA is of the order reported globally and used in our study. However the estimate for CVID is considerably lower than our base case [13]. This Australian study reports from a patient registry with the possible under-reporting discussed above and it is therefore possible that these prevalence estimates are masking the true prevalence and the potential demand for Ig for CVID. Appropriate provision of Ig therapy is of the essence and depends upon robust diagnostic criteria that grow along with the immunologic and genetic understanding of the diseases. These are evolving towards less nebulous guidance with more specific structuring of certain components such as the interpretation of response to vaccination [64]. The differences between the different geographic regions demonstrate, even if there were to be substantive present under-reporting, that LTD is still substantive.
This accentuates the importance of improving diagnosis as a component to ensuring disease delivery, but the use of incomplete data in devising policy and planning treatment is fraught with risk. Recently, Germany has been proposed as an example of a socially sensitive wealthy social market health care system in which Ig consumption is considerably below that of the higher usage countries such as the United States, Canada and Australia [12]. It was suggested that health outcomes for patients in low usage countries are not inferior to those of high usage countries. That said, the potential benefits of higher usage may take years to become apparent and require robust data capture longitudinally [14]. Moreover, the PID landscape in Germany includes certain barriers in diagnosis and treatment (as can also found in other countries), particularly in transitioning pediatric patients into adult care [68]. This has perhaps resulted, amongst other features, in a remarkably lower prevalence of CVID and XLA in Germany [34] than in similar countries (Table III).
Conclusion
In summary, the present study suggests that, using literature-based data for the inputs proposed in our LTD model, the potential demand for treating the two main Ig-consuming PIDs approaches levels which exceed the usage of Ig for these disorders as currently recorded. The central finding of this research is that the average potential usage of Ig for the treatment of CVID and XLA is 72 g per 1,000 population, which is higher than the estimated Ig usage in CVID and XLA of 27–41 g per 1,000 population in the US. The US has the second highest total observed Ig usage of 137.5 g per 1,000 population [7]. Furthermore, the results from the LTD model exceed the total Ig usage in most countries where these data are available. Hence continued efforts to increase the supply of Ig through increasing the supply of plasma and the efficiency of manufacture are required. Ensuring that Ig treatment is focused on evidence-based indications is also an essential part in managing this precious resource.
References
Shehata N, Palda V, Bowen T, Haddad E, Issekutz TB, Mazer B, et al. The use of immunoglobulin therapy for patients with primary immune deficiency: an evidence-based practice guideline. Transfus Med Rev. 2010;24 Suppl 1:S28–50.
Wood P. Immunotherapy for primary immunodeficiency diseases. Med Clin N Am. 2012;96(3):433–54.
Eibl MM. History of immunoglobulin replacement. Immunol Allergy Clin N Am. 2008;28(4):737–64.
Hooper JA. Intravenous immunoglobulins: evolution of commercial IVIG preparations. Immunol Allergy Clin N Am. 2008;28(4):765–78.
Buchacher A, Iberer G. Purification of intravenous immunoglobulin G from human plasma—aspects of yield and virus safety. Biotechnol J. 2006;1(2):148–63.
Jolles S, Sewell W, Misbah S. Clinical uses of intravenous immunoglobulin. Clin Exp Immunol. 2005;142(1):1–11.
Robert P. IVIG/SCIG: GLOBAL USAGE TRENDS. 2011. http://www.ipopi.org/uploads/Patrick%20Robert.pdf. Accessed 14 May 2013.
Orange JS, Hossny EM, Weiler CR, Ballow M, Berger M, Bonilla FA, et al. Use of intravenous immunoglobulin in human disease: a review of evidence by members of the primary immunodeficiency committee of the American academy of allergy, asthma and immunology. J Allergy Clin Immunol. 2006;117(4 Suppl):S525–53.
Australian National Blood Authority. Criteria for the clinical use of intravenous immunoglobulin in Australia, 2nd ed. http://www.blood.gov.au/pubs/ivig/index.html#/ivig/pdf/criteria.pdf. Accessed 1 August 2013.
Australian National Blood Authority. Issues of IVIg (grams) per 1000 head of population, 2007–08 to 2011–12. 2011. http://www.nba.gov.au/publications/1112report/chapter03/3.2.html#figure3_17. Accessed 1 August 2013.
Farrugia A, Cassar J. Is self-sufficiency in haemotherapies a practical or necessary goal? Blood Transfus. 2012;13:1–12.
Rossi F, Perry R, de Wit J, Evers T, Folléa G. How expanding voluntary non-remunerated blood donations would benefit patients, donors and healthcare systems? Vox Sang. 2011;101(2):176–7.
Joshi AY, Iyer VN, Hagan JB, St Sauver JL, Boyce TG. Incidence and temporal trends of primary immunodeficiency: a population-based cohort study. Mayo Clin Proc. 2009;84(1):16–22.
Orange JS, Grossman WJ, Navickis RJ, Wilkes MM. Impact of trough IgG on pneumonia incidence in primary immunodeficiency: a meta-analysis of clinical studies. Clin Immunol. 2010;137(1):21–30.
Goel V. Decision analysis: applications and limitations. The Health Services Research Group. CMAJ. 1992;147(4):413–7.
Stonebraker JS, Amand RE, Bauman MV, Nagle AJ, Larson PJ. Modelling haemophilia epidemiology and treatment modalities to estimate the unconstrained factor VIII demand. Haemophilia. 2004;10(1):18–26.
Stonebraker JS, Keefer DL. Modeling potential demand for supply-constrained drugs: a new hemophilia drug at Bayer Biological Products. Oper Res. 2009;57(1):19–31.
European Society for Immunodeficiencies Registry (ESID). 2011. http://www.esid.org. Accessed September 14, 2011.
Gathmann B, Grimbacher B, Beauté J, Dudoit Y, Mahlauoui N, Fischer A, et al. The European internet-based patient and research database for primary immunodeficiencies: results 2006–2008. Clin Exp Immunol. 2009;157 Suppl 1:3–11.
Immune Deficiency Foundation: Primary immune deficiency diseases in America. Prepared by Schulman, Ronca and Bucuvalas, Inc., 1995.
Immune Deficiency Foundation: Primary immune deficiency diseases in America: 2002. The second national survey of patients. Prepared by Schulman, Ronca and Bucuvalas, Inc., April 28, 2003
Immune Deficiency Foundation: Treatment experiences and preferences of patients with primary immune deficiency diseases: First national survey. Prepared by Schulman, Ronca and Bucuvalas, Inc., June 20, 2003.
Immune Deficiency Foundation: Primary immunodeficiency diseases in America: 2007. The third national survey of patients. Prepared by Abt SRBI, Inc., May 1, 2009.
Immune Deficiency Foundation: Treatment experiences and preferences among patients with primary immunodeficiency diseases. National survey of patients: 2008. Prepared by Abt, SRBI, Inc., May 6, 2009.
Briggs AH, Weinstein MC, Fenwick EAL, Karnon J, Sculpher MJ, Paltiel AD, et al. Model parameter estimation and uncertainty analysis: a report of the ISPOR-SMDM modeling good research practices task force working group—6. Med Decis Mak. 2012;32:722–32.
Keefer DL, Bodily SE. Three-point approximation for continuous random variables. Manag Sci. 1983;29:595–609.
Park MA, Li JT, Hagan JB, Maddox DE, Abraham RS. Common variable immunodeficiency: a new look at an old disease. Lancet. 2008;372(9637):489–502.
Yong PFK, Tarzi M, Chua I, Grimbacher B, Chee R. Common variable immunodeficiency: an update on etiology and management. Immunol Allergy Clin N Am. 2008;28(2):367–86.
World Population Prospects: The 2012 Revision. In: United Nations, Department of Economic and Social Affairs, Population Division. 2013. http://esa.un.org/wpp/unpp/panel_indicators.htm. Accessed July 10, 2013.
Abuzakouk M, Feighery C. Primary immunodeficiency disorders in the Republic of Ireland: first report of the National Registry in children and adults. J Clin Immunol. 2005;25(1):73–7.
Beauté J et al. The French national registry of primary immunodeficiency diseases. Clin Immunol. 2010;135:264–72.
Boyle JM, Buckley RH. Population prevalence of diagnosed primary immunodeficiency diseases in the United States. J Clin Immunol. 2007;27:497–502.
Edgar JDM, Buckland M, Guzman D, Conlon NP, Knerr V, et al. The United Kingdom Primary Immune Deficiency (UKPID) Registry: report of the first 4 years’ activity 2008–2012. Clin Exp Immunol doi: 10.1111/cei.12172.
Gathmann B, Goldacker S, Klima M, et al. The German national registry for primary immunodeficiencies (PID). Clin Exp Immunol. 2013;173(2):372–80.
Golan H et al. The incidence of primary immunodeficiency syndromes in Israel. IMAJ. 2002;4(Suppl):868–71.
Ishimura M et al. Nationwide survey of patients with primary immunodeficiency diseases in Japan. J Clin Immunol. 2011;31:968–76.
Kirkpatrick P, Riminton S. Primary immunodeficiency diseases in Australia and New Zealand. J Clin Immunol. 2007;27(5):517–24.
Flori NM, Llambi JM, Boren TE, Borja SR, Casariego GF. Primary immunodeficiency syndrome in Spain: first report of the National Registry in children and adults. J Clin Immunol. 1997;17(4):333–9.
Modell V, Gee B, Lewis DB, Orange JS, Rolfman CM, Routes JM, et al. Global study of primary immunodeficiency diseases (PI)—diagnosis, treatment, and economic impact: an updated report from the Jeffrey Modell Foundation. Immunol Res. 2011;51:61–70.
Resnick ES, Bhatt P, Sidi P, Cunningham-Rundles C. Examining the use of ICD-9 Diagnosis Codes for primary immune deficiency diseases in New York State. J Clin Immunol. 2013;33:40–8.
Ryser O, Morell A, Hitzig WH. Primary immunodeficiencies in Switzerland: first report of the National Registry in adults and children. J Clin Immunol. 1988;8(6):479–85.
Stray-Pedersen A, Abrahamsen TG, Frøland SS. Primary immunodeficiency diseases in Norway. J Clin Immunol. 2000;20(6):477–85.
Furst DE. Serum immunoglobulins and risk of infection: how long can you go? Semin Arthritis Rheum. 2009;39(1):18–29.
McDowell MA, Fryar CD, Ogden CL, Flegal KM. Anthropometric reference data for children and adults: United States, 2003–2006. National Health Statistics Reports: no. 10. Hyattsville: National Center for Health Statistics; 2008.
Klein RJ, Schoenborn CA. Age adjustment using the 2000 projected U.S. population. Healthy People Statistics notes, no. 20. Hyattsville: National Center for Health Statistics; 2001.
Ballow M, Notarangelo L, Grimbacher B, Cunningham-Rundles C, Stein M, Helber M, et al. Immunodeficiencies. Clin Exp Immunol. 2009;158 Suppl 1:14–22.
Yong PL, Boyle J, Ballow M, Boyle M, Berger M, Bleesing J, et al. Use of intravenous immunoglobulin and adjunctive therapies in the treatment of primary immunodeficiencies: a working group report of and study by the Primary Immunodeficiency Committee of the American Academy of Allergy Asthma and Immunology. Clin Immunol. 2010;135(2):255–63.
Hernandez-Trujillo HS, Chapel H, Lo Re 3rd V, Notarangelo LD, Gathmann B, Grimbacher B, et al. Comparison of American and European practices in the management of patients with primary immunodeficiencies. Clin Exp Immunol. 2012;169(1):57–69.
Lucas M, Lee M, Lortan J, Lopez-Granados E, Misbah S, Chapel H. Infection outcomes in patients with common variable immunodeficiency disorders: relationship to immunoglobulin therapy over 22 years. J Allergy Clin Immunol. 2010;125(6):1354–60.
Farrugia A, Cassar J. Plasma-derived medicines: access and usage issues. Blood Transfus. 2012;10(3):273–8.
National Health Service. Demand Management Programme for Immunoglobulin. 2009. http://www.ivig.nhs.uk. Accessed 14 May 2013.
Elovaara I, Apostolski S, van Doorn P, Gilhus NE, Hietaharju A, Honkaniemi J, et al. EFNS guidelines for the use of intravenous immunoglobulin in treatment of neurological diseases: EFNS task force on the use of intravenous immunoglobulin in treatment of neurological diseases. Eur J Neurol. 2008;15(9):893–908.
Patwa HS, Chaudhry V, Katzberg H, Rae-Grant AD, So YT. Evidence-based guideline: intravenous immunoglobulin in the treatment of neuromuscular disorders: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2012;78(13):1009–15.
Bonilla FA, Bernstein IL, Khan DA, Ballas ZK, Chinen J, Frank MM, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. Ann Allergy Asthma Immunol. 2005;94(5 Suppl 1):S1–S63.
Roifman CM, Levison H, Gelfand EW. High-dose versus low-dose intravenous immunoglobulin in hypogammaglobulinaemia and chronic lung disease. Lancet. 1987;1(8541):1075–7.
Liese JG, Wintergerst U, Tympner KD, Belohradsky BH. High- vs low-dose immunoglobulin therapy in the long-term treatment of X-linked agammaglobulinemia. Am J Dis Child. 1992;146(3):335–9.
Eijkhout HW, van Der Meer JW, Kallenberg CG, Weening RS, van Dissel JT, Sanders LA, et al. The effect of two different dosages of intravenous immunoglobulin on the incidence of recurrent infections in patients with primary hypogammaglobulinemia. A randomized, double-blind, multicenter crossover trial. Ann Intern Med. 2001;135(3):165–74.
Berger M. Incidence of infection is inversely related to steady-state (Trough) serum IgG level in studies of subcutaneous IgG in PIDD. J Clin Immunol. 2011;31(5):924–6.
Quinti I, Soresina A, Guerra A, Rondelli R, Spadaro G, Agostini C, et al. Effectiveness of immunoglobulin replacement therapy on clinical outcome in patients with primary antibody deficiencies: results from a multicenter prospective cohort study. J Clin Immunol. 2011;31(3):315–22.
Carsetti R, Rosado MM, Donnanno S, Guazzi V, Soresina A, Meini A, et al. The loss of IgM memory B cells correlates with clinical disease in common variable immunodeficiency. J Allergy Clin Immunol. 2005;115(2):412–7.
Chapel H, Lucas M, Lee M, Bjorkander J, Webster D, Grimbacher B, et al. Common variable immunodeficiency disorders: division into distinct clinical phenotypes. Blood. 2008;112(2):277–86.
Chapel H, Cunningham-Rundles C. Update in understanding common variable immunodeficiency disorders (CVIDs) and the management of patients with these conditions. Br J Haematol. 2009;145(6):709–27.
Chapel H, Lucas M, Patel S, Lee M, Cunningham-Rundles C, Resnick E. Confirmation and improvement of criteria for clinical phenotyping in common variable immunodeficiency disorders in replicate cohorts. J Allergy Clin Immunol. 2012;130(5):1197–1198e9.
Orange JS, Ballow M, Stiehm ER, Ballas ZK, Chinen J, De La Morena M, et al. Use and interpretation of diagnostic vaccination in primary immunodeficiency: a working group report of the Basic and Clinical Immunology Interest Section of the American Academy of Allergy, Asthma & Immunology Genome-wide association identifies diverse causes of common variable immunodeficiency. J Allergy Clin Immunol. 2012;130:S1–S24.
Wehr C, Kivioja T, Schmitt C, Ferry B, Witte T, Eren E, et al. The EUROclass trial: defining subgroups in common variable immunodeficiency. Blood. 2008;111(1):77–85.
Orange JS, Glessner JT, Resnick E, Sullivan KE, Lucas M, Ferry B, et al. Genome-wide association identifies diverse causes of common variable immunodeficiency. J Allergy Clin Immunol. 2011;127:1360–7.
Stonebraker JS, Farrugia A, Gathmann B. A decision analysis model to estimate latent therapeutic demand for immunoglobulin therapy in primary immunodeficiencies. Proceedings of the 15th Meeting of the European Society of Immunodeficiencies—ESID (October 3–6, 2012, Florence, Italy). 2013;29–34.
Schöndorf I. Resolving barriers to the treatment of primary immunodeficiencies. The Source. 2011;19–20.
Acknowledgment
Research was supported by the Plasma Proteins Therapeutics Association grant to Stonebraker.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
The ESID Registry is based on contributions by the following national registries: CEREDIH (France), REDIP (Spain), PID-NET (Germany), UKPIN (UK), IPINET (Italy), AGPI (Austria), the Netherlands, Czech Republic. Additional contributions are received from the following countries: Turkey, Poland, Ireland, Portugal, Belgium, Switzerland, Slovakia, Sweden, Slovenia, Croatia, Serbia, Greece, Belarus, Russia, Hungary, Romania, Ukraine, Estonia, Lithuania, Egypt, and Israel.
Rights and permissions
About this article
Cite this article
Stonebraker, J.S., Farrugia, A., Gathmann, B. et al. Modeling Primary Immunodeficiency Disease Epidemiology and Its Treatment to Estimate Latent Therapeutic Demand for Immunoglobulin. J Clin Immunol 34, 233–244 (2014). https://doi.org/10.1007/s10875-013-9975-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-013-9975-1