
Abstract
The Child Behavior Checklist-Dysregulation Profile has been utilized as a potential predictive measure of future psychopathology among children and adolescents. Previous studies have examined the differences between individuals with and without an elevated profile on variables such as parenting, temperament, parental psychopathology, personality, and more. The current study extended the literature to examine similar variables among an emerging adult population as well as gender differences among the profile groups determined from a parallel form of the Child Behavior Checklist for adults, the Adult Self Report. Emerging adults were recruited at a large Southern university in the United States (410 females and 189 males). A latent profile analysis was conducted to determine profile group membership (i.e., elevation of dysregulation) and differences were examined on temperament, parental and emerging adult psychopathology, parent-child relationship, and discipline and harsh parenting. Significant differences were demonstrated between the elevated dysregulated profile and the group with low dysregulation on all observed variables. Analyses of gender differences indicated that males with an elevated dysregulation profile may be particularly vulnerable on several variables.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The Child Behavior Checklist-Dysregulation Profile (CBCL-DP) was developed to represent children who were elevated on Attention Problems, Aggression, and Anxiety/Depression (Althoff et al. 2010). Children who are elevated on the CBCL-DP also are at risk for anxiety and disruptive behavior problems and even suicidality (Althoff et al. 2006; Haltigan et al. 2018; McGough et al. 2008; Volk and Todd 2007). Although researchers have studied the CBCL-DP in preschoolers, children, and adolescents, it appears that no studies have examined it in emerging adults despite a parallel form, the Adult Self Report (ASR), of the CBCL being widely available (Biederman et al. 2009; Meyer et al. 2009). Specifically, Kim et al. (2012) compared preschoolers’ temperament, personality, and psychopathology as well as their parents’ psychopathology, parenting behaviors, and martial functioning in a sample of preschoolers with and without an elevated CBCL-DP profile. They found that preschoolers with elevated CBCL-DP profiles were at greater risk for increased negative affect, lower effortful control, more depressive and oppositional defiant problems, and had more controlling and punishing parents. The current study expanded upon the study by Kim et al. (2012) by comparing emerging adults with and without elevated CBCL-DP (using the ASR and referred to as ASR-DP by the current study when referencing adults) on temperament, psychopathology, and parent-child relationships as well as parental psychopathology and discipline based on current self-report.
CBCL-DP and Child Psychopathology
The CBCL-DP has been examined in many studies to determine how children with elevated profiles differ from others. For example, Meyer et al. (2009) conducted a longitudinal study and found that approximately a third of school age children with an elevated CBCL-DP were at risk for developing bipolar disorder, ADHD, anxiety and personality disorders, as well as suicidal thoughts and behaviors as emerging adults. Similarly, other studies have found that the school age children with elevated CBCL-DP were at greater risk for psychological disorders like bipolar disorder and major depression, and an elevated profile even predicted hospitalization later in adulthood (Biederman et al. 2009). These results have been replicated in Germany and the Netherlands (Althoff et al. 2010; Holtmann et al. 2011). Thus, studies appear to show consensus that the CBCL-DP can predict risk for developing later psychological problems.
Few studies, however, have examined other child variables like temperament using the CBCL-DP. In one such study, Kim et al. (2012) found the CBCL-DP was associated with greater negative affect and less effortful control in a sample of preschoolers. Another study found the CBCL-DP was related to less effortful control in a sample of children 8 to 14 (Deutz et al. 2019). Although it appears that no studies have examined temperament and the ASR-DP in emerging adults, temperament in emerging adults has been associated with psychological problems including irritability and defiance (McKinney et al. 2018b). Specifically, effortful control was associated with less irritability and defiance for males and females, and negative affect was related to greater irritability in males and females. Thus, it is plausible that temperament will similarly be related to the ASR-DP in emerging adults.
CBCL-DP and Parenting Factors
Despite the consensus about the predictive value of the CBCL-DP regarding psychological problems later in life, relatively fewer studies have examined the connection to parenting variables. The studies that examined this connection have found strong links between the CBCL-DP and current family environment. For example, Jucksch et al. (2011) examined 4- to 18-year-old children and found the CBCL-DP was associated with greater parental psychopathology as well as poor communication and relationships. Additionally, Kim et al. (2012) found the CBCL-DP was associated with greater risk of harsh and controlling parenting for preschool children.
The biosocial developmental model argues that during the preschool years, children’s noradrenergic, serotonergic, and dopaminergic systems are developing and stress in the environment can result in difficulty controlling their behavior and emotions (Bremner and Vermetten 2001). Given that the development of emotion regulation skills occurs within the family, families with increased conflict, such as those where parents have mental health problems, are more likely to model and reinforce emotion dysregulation (Shipman and Zeman 2001). Therefore, increased stress in the home may result in deficiencies within many vital neurological systems which play a role in the development of emotion regulation skills. Homes with stress are those in which parents may have psychological problems and use poor parenting behaviors, resulting in poor modeling of emotion regulation within the home whereby children develop emotion dysregulation and psychological problems. The CBCL-DP, an indicator of child emotion dysregulation problems, likely would be one measure of emotion regulation difficulties among children who grow up in more stressful environments. In addition, these children may have poor functioning as adults later in life.
Dysregulation and Parenting in Emerging Adulthood
Emotion dysregulation and risk for psychological disorders continue into emerging adulthood (Stearns and McKinney 2018; Zimmerman and Iwanski 2014). Similarly, parents continue to be an important part of their emerging adult children’s lives and are likely to parent the way they did during childhood unless intervention occurred (McKinney and Milone 2012). As stated above, the biosocial developmental model contributes to emotion dysregulation in childhood and into adulthood. The ASR-DP could serve as a tool to determine individuals who have emotion regulation difficulties in emerging adulthood and adulthood. Indeed, substantial work has been done to address the identification of children with emotion regulation difficulties, but adults could also benefit from being identified with the use of this profile.
Also, parents likely continue to play behavioral and social roles in emerging adult dysregulation even once their emerging adult children reach a level of independence and research has indicated that parents continue to influence their children’s mental health in emerging adulthood. Although it appears that no studies have examined the ASR-DP and parental psychopathology, discipline of emerging adults, and emerging adult relationship quality with their parents, studies have connected negative family environments to psychological problems in emerging adulthood. For example, parental internalizing and externalizing problems were related to emerging adult children’s internalizing and externalizing problems (Franz and McKinney 2018; Walker and McKinney 2015). More specifically, studies have found that parental psychopathology (e.g., anxiety, depression, and antisocial problems) was related to greater antisocial, depressive, and anxiety problems in children across development (Morris et al. 2014; Stearns and McKinney 2018).
Additionally, harsh parenting practices have been associated with greater risk for psychological problems in emerging adults. McKinney et al. (2018a) found that physical and psychological maltreatment by parents were correlated with oppositional defiant problems. Similarly, maternal and paternal harsh discipline were related to increased psychological problems in emerging adults (McKinney et al. 2018). Thus, it is conceivable that harsh discipline will similarly be related to an elevated ASR-DP profile in emerging adults. Moreover, poor relationship quality between emerging adults and their parents have been found to be associated with worse emerging adult psychopathology. For example, a recent study found that increased emerging adult internalizing and externalizing problems were related to worse parent-child relationships (Steele and McKinney 2019). Thus, parenting still plays a large role in emerging adult mental health and emerging adults with emotion dysregulation are more likely to suffer from poor relationships with their parents and increased psychological problems.
Current Study
The current study expanded upon the study by Kim et al. (2012) by examining elevations in the ASR-DP profile in connection to emerging adult temperament, psychopathology, and parent and emerging adult child relationships as well as parental psychopathology and discipline among parents of emerging adults with an elevated profile. A college-attending emerging adult sample was utilized to examine the ASR-DP profile, whereas previous studies have utilized a sample of preschoolers or school-age children (Biederman et al. 2009; Deutz et al. 2019). Moreover, this study expanded previous literature on predictive ability of the dysregulation profile to identify risk factors by examining temperament, emerging adult and their parents’ psychopathology, and their parents’ parenting behaviors similar to Kim et al. (2012), and also measured relationship quality between emerging adults and their parents. It was hypothesized that emerging adults with the ASR-DP (i.e., created using the syndrome scales of aggressive, attention, and anxious/depressed problems on the ASR reflecting similar scales utilized by Kim et al. 2012 and Althoff et al. 2010), as compared to those without, would report 1) more internalizing and externalizing problems (as identified using the DSM-oriented scales of the ASR), 2) lower effortful control and higher negative affect, 3) worse relationship quality with parents, 4) harsher discipline from their parents, and 5) greater parental psychopathology. Additionally, previous studies indicated both the influence of emerging adult and parental gender across the variables of interest.
Method
Participants
Participants consisted of 599 individuals aged 18 to 25 years (M = 19.60, SD = 1.40; 68% females). The sample consisted of 67.8% White, 27.2% Black, 2% Hispanic, 1% Asian, and 1.8% other. Participants claimed that their biological mother (95.8%) and/or biological father (74.5%) were present in their childhood home, with fewer participants reporting stepparents, single parents, or other family structures (i.e., grandparents, aunts/uncles, foster, adoptive, etc.). Participants reported that their mother (57.4%) or father (48.6%) completed a 4-year college degree or higher.
Procedure
Undergraduate students were recruited at a large Southern university in the United States via an online research program that allowed students to choose from a list of psychological studies to participate in for credit. Upon choosing the study, participants were presented with a consent form as part of the online survey and indicated consent by continuing with the study. Measures were completed in random order and according to current perspectives, and all participants were treated in accordance with APA Ethical Guidelines. Upon completion, participants were given a debriefing form and awarded research credit they could apply toward a class of their choosing.
Measures
The Adult Behavior Checklist (ABCL) and Adult Self-Report (ASR)
The ASR and ABCL (Auerbach et al. 2018) are 123-item instruments used to measure internalizing and externalizing problems within the self and others, respectively. Responses include 0 (not true), 1 (somewhat or sometimes true), and 2 (very true or often true). Participants used the ASR to report on themselves and the ABCL to report on their mothers and fathers separately. The syndrome scales of anxious/depressed (e.g., cries a lot; current study alphas = .92 to .93 across emerging adult, maternal, and paternal ratings), attention problems (e.g., is too forgetful; current study alphas = .90 to .93) and aggressive behavior (e.g., argues a lot; current study alphas = .91 to .93) were used to create a dysregulation profile for emerging adults.
An elevated dysregulation profile has been indicative of significant impairment across multiple domains by Kim et al. (2012). Previous studies have computed the sum of the T scores for the syndrome subscales of attention problems, aggressive behavior, and anxious/depressed, using a cutoff score of ≥180 (or each scale ≥60). Similarly, Kim et al. (2012) summed scores on the attention problems, aggressive behavior, and anxious/depressed subscales and used a cutoff of 1 SD above the mean and median for the dysregulation positive group, and those below the cutoff were placed in the dysregulation negative group. The current study used a latent profile analysis to determine group membership (see planned analysis section for more information) to identify distinct groups based on the subscales rather than using a cutoff score.
The DSM-oriented scales include depressive problems (e.g., feels worthless; alphas for mother = .91, father = .91, emerging adult = .88), anxious problems (e.g., worries; alphas for mother = .80, father = .79, emerging adult = .80), avoidant personality problems (e.g., doesn’t get along with other people; alphas for mother = .86, father = .86, emerging adult = .83), antisocial problems (e.g., breaks rules at work or elsewhere; alphas for mother = .95, father = .95, emerging adult = .94), AD/H problems (e.g., fails to finish things he/she should do; alphas for mother = .91, father = .91, emerging adult = .88) and oppositional defiant problems (e.g., I blame others for my problems; alphas for mother = .86, father = .86, emerging adult = .80). Maternal, paternal, and emerging adult scores from these scales were compared between groups of emerging adults with and without an elevated dysregulation profile as described above.
Adult Temperament Questionnaire (ATQ)
The Adult Temperament Questionnaire Short Form (ATQ; Evans and Rothbart 2007) was used to measure emerging adult temperament. The 77 items are rated on a 7-point scale ranging from 1 (extremely untrue) to 7 (extremely true). Subscales used to indicate temperament in the current study included negative affect (e.g., I often feel sad and it doesn’t take very much to make me feel frustrated or irritated), effortful control (e.g., I can keep performing a task even when I would rather not do it and it is easy for me to inhibit fun behavior that would be inappropriate), and surgency (e.g., I usually like to talk a lot and sometimes minor events cause me to feel intense happiness). The measure has demonstrated good psychometrics as well as convergence with the Big Five personality framework (Evans and Rothbart 2007). Alphas in the current study ranged from .71 to .80.
Domains of Young Adult Discipline (DYADS)
The DYADS (Walker 2018) is a 25-item measure that assesses maternal and paternal discipline tactics. Items are rated on a 5-point scale ranging from 1 (never) to 5 (always). Subscales include behavioral control (e.g., permanently kicks me out of the house), psychological control (e.g., deliberately makes me feel ashamed or guilty), physical assault (e.g., punches or slaps me with hand), and non-violent/inductive reasoning (e.g., rewards me with extra money or gifts).
Items on this scale were developed during a study by Walker (2018). Items were based on theoretical relevance and review of existing measures of discipline as well as qualitative analysis of focus groups with emerging adults who were prompted with questions like What are some consequences for when you disagree with your parents? and What type of punishment have you received as a college student? This process resulted in 113 items. Based on prior theory about the domains of discipline (i.e., physical, behavioral, psychological, and inductive), items were loaded onto four constructs based on these domains. The initial confirmatory factor analysis (CFA) fit the data poorly (i.e., CFI < .51, SRMR > .13). To improve model fit, items with factors loadings < .20 were removed, followed by removal of redundant (i.e., highly correlated) items. This process resulted in the final 25-item scale that provided good model fit (i.e., CFI > .92, SRMR < .06). These four factors correlated as expected with other measures of discipline (e.g., the psychological control scale demonstrated r = .72 with the psychological aggression scale of the Conflict Tactics Scale: Parent-Child Version), parenting (e.g., the inductive reasoning scale demonstrated r = .63 with the authoritative style scale of the Parental Authority Questionnaire), and psychological functioning (e.g., inductive reasoning negatively correlated with psychological problems, whereas physical assault and control scales correlated positively). Finally, subscales demonstrated alphas higher than .75 in all cases in the validation study (Walker 2018). Alphas in the current study ranged from .75 to .91.
Network of Relationships Inventory (NRI)
The NRI (Furman and Buhrmester 2009) consists of items on several sub-dimensions of relationship quality pertaining to the participants’ relationship with their mothers and fathers. For each person, participants rated the items on a scale between 1 (Never or hardly at all) and 5 (Always or extremely much). For the current study, the subscale score for emotional support (e.g., how often do you turn to this person for support with personal problems) was used. Additionally, the composite scores of 5 subscales (15 items) were used to determine relationship closeness (e.g., how often does this person praise you for the person you are?) and another composite score of 5 subscales (15 items) were used to determine the amount of relationship discord (e.g., how often to you and this person disagree and quarrel with each other?) per the measures manual (Furman and Buhrmester 2009). Good construct validity has been established in previous studies, and the internal consistency alphas for the current study ranged from .90 to .92.
Data Analysis
A Bayesian latent profile analysis (LPA) was used to determine emerging adult dysregulation profiles performed using Markov chain Monte Carlo (MCMC) to obtain likelihood estimates with AMOS 24.0. The emerging adult dysregulation profile was calculated using scores of the attention problems, aggressive behavior, and anxious/depressed subscales from the emerging adults self-report on the ASR. LPA identifies distinct latent profiles based on observed continuous variables (Muthén and Muthén 2000). A two-group solution using 55,500 samples was chosen to capture a similar analysis as Kim et al. (2012; i.e., positive and negative dysregulation profile groups). Fit indices provided by AMOS included the Gelman et al. (2004) convergence criteria of <1.10 and posterior predictive p value of 0.50 as well as Nagin’s (2005) criterion of posterior probabilities of correct class assignment >0.70.
A 2 (dysregulation profile) × 2 (participant gender) MANCOVA was utilized with SPSS 24.0 to compare emerging adult males and females with and without an elevated dysregulation profile across several domains including emerging adult psychopathology, parental psychopathology, emerging adult temperament, and parental discipline and relationship quality. Covariates included parental education and ethnicity. Partial η2 served as the measure of effect size for the MANCOVAs, where values of 0.01 to 0.04, 0.04 to 0.14, and greater than 0.14 are considered small, medium, and large, respectively (Cohen 1988). Data was examined for consistent responding and cases were removed that did not consistently respond to reverse coded items.
Results
ASR-DP LPA
The two-group solution resulted in a convergence statistic of <1.0001, satisfying the Gelman et al. (2004) convergence criteria of <1.10 as well as the more conservative convergence criteria of <1.02 used by AMOS, and a posterior predictive p value of .56, indicating that the solution has a very high likelihood of being reproduced through resampling. Group membership was determined with a posterior predictive value > .70 as suggested by Nagin (2005). Participants were classified by the LPA into a group with low scores on all three subscales (i.e., attention problems, aggressive behavior, and anxious/depressed) which consisted of 385 individuals, whereas 200 participants were classified into a group with high scores across all three variables; 14 individuals were cut from analysis as they failed to meet Nagin’s (2005) criterion for inclusion. As shown in Table 1, the LPA notably identified an elevated dysregulation profile (DP-Positive) group which had mean and minimum T scores >60 across all three subscales as suggested by Kim et al. (2012), as well as a DP-Negative group which had mean and maximum scores well within the normal range according to the ASR.
MANCOVAs
Emerging adult temperament and psychopathology
Results of the MANCOVA using the dysregulation profiles and gender to predict emerging adult temperament are shown in Table 2. Race, parental education, and the gender x dysregulation group interaction effects were not significant. Gender, Wilk’s Λ = .947, F(3, 587) = 10.88, p < .001, partial η2 = .05, and dysregulation group membership, Wilk’s Λ = .918, F(3, 587) = 17.55, p < .001, partial η2 = .08, were significant multivariate effects. As shown in Table 2, females scored higher than males on negative affect and effortful control but not surgency. The DP-Positive profile scored significantly higher on negative affect and scored significantly lower on surgency and effortful control.
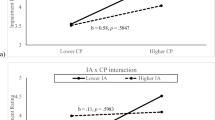
Results of the MANCOVA using the dysregulation profiles to predict emerging adult psychopathology are shown in Table 3. Race and parental education were not significant covariates. Gender, Wilk’s Λ = .927, F(6, 584) = 7.70, p < .001, partial η2 = .07, dysregulation profile membership, Wilk’s Λ = .299, F(6, 584) = 234.95, p < .001, partial η2 = .71, and the gender x dysregulation profile membership, Wilk’s Λ = .964, F(6, 584) = 3.59, p = .002, partial η2 = .04, were significant, suggesting significant differences among emerging adult dysregulation profiles across emerging adult psychopathology. Females scored significantly higher than males on anxiety problems, whereas male scored significantly higher than females on the ODD and antisocial subscales. The DP-Positive group scored significantly higher than the DP-Negative group on all psychopathology subscales, with substantially large effects. The interaction was significant for the ODD and antisocial scales. Males and females who did not have an elevated profile scored similarly on the ODD and antisocial scales, whereas males scored higher than females on these scales when examining the elevated profile (i.e., the negative effect of the dysregulation profile is particularly pronounced for males).
Perceived parental psychopathology
Results of the MANCOVA using the dysregulation profiles to predict perceived maternal psychopathology are shown in Table 4. Race and parental education were not significant covariate. Gender, Wilk’s Λ = .916, F(6, 584) = 8.92, p < .001, partial η2 = .08, dysregulation profile membership, Wilk’s Λ = .587, F(6, 584) = 68.37, p < .001, partial η2 = .41, and the gender x dysregulation group membership, Wilk’s Λ = .939, F(6, 584) = 6.35, p < .001, partial η2 = .06, were significant, suggesting significant differences among emerging adult dysregulation profiles across maternal psychopathology. Males, compared to females, reported significantly higher maternal psychopathology across subscales except the anxiety subscale. The DP-Positive group reported higher scores on all maternal psychopathology subscales. The interaction effect indicated that males in the DP-Positive group scored significantly higher than females within the DP-Positive group on all subscales except anxiety, whereas males and females in the DP-Negative group scored similarity.
Results of the MANCOVA using the dysregulation profiles to predict perceived paternal psychopathology are shown in Table 5. Race and parental education were not significant covariate. Gender, Wilk’s Λ = .939, F(6, 584) = 6.35, p < .001, partial η2 = .06, dysregulation profile membership, Wilk’s Λ = .552, F(6, 584) = 79.10, p < .001, partial η2 = .45, and the gender x dysregulation group membership, Wilk’s Λ = .942, F(6, 584) = 5.96, p < .001, partial η2 = .06 were significant. Males reported significantly higher scores for paternal psychopathology than females on all paternal psychopathology subscales. The DP-Positive group reported significantly higher scores across all paternal psychopathology subscales relative to the DP-Negative group. The interaction effect demonstrated that males reported higher paternal psychopathology than females when examining the DP-Positive group but that this gender difference did not occur in the DP-Negative group.
Perceived parenting characteristics
Results of the MANCOVA using the dysregulation profiles to predict perceived maternal parenting of emerging adults and relationship quality with mothers are shown in Table 6. Race, parental education, and the gender x dysregulation profile group membership were not significant. Gender, Wilk’s Λ = .927, F(7, 583) = 6.60, p < .001, partial η2 = .07, and dysregulation profile membership, Wilk’s Λ = .911, F(7, 583) = 8.10, p < .001, partial η2 = .09, were significant. Males scored higher than females on the maternal physical assault subscale, and females scored higher than males on maternal emotional support and closeness subscales. The DP-Positive group scored higher than the DP-Negative group on psychological control, behavioral control, physical assault, and discord subscales, whereas the DP-Negative group scored higher on inductive reasoning, emotional support, and closeness.
Results of the MANCOVA using the dysregulation profiles to predict perceived paternal parenting of emerging adults and relationship quality with fathers are shown in Table 7. Race, parental education, and the gender x dysregulation profile membership interaction were not significant. Gender, Wilk’s Λ = .975, F(7, 583) = 2.15, p = .04, partial η2 = .03, and dysregulation group membership, Wilk’s Λ = .929, F(7, 583) = 6.38, p < .001, partial η2 = .07) were significant. Males, compared to females, reported significantly higher scores for the paternal physical assault and discord subscales. The DP-Positive group, relative to the DP-Negative group, reported higher perceived paternal psychological control, behavioral control, physical assault, and discord, whereas the DP-Negative group reported higher scores on inductive reasoning, emotional support, and closeness subscales.
Discussion
The current study generalized the work by Kim et al. (2012) into emerging adulthood and examined differences on emerging adult temperament and psychopathology as well as emerging adults’ parents’ psychopathology and parenting characteristics between gender and dysregulation profile groups. Notably, the use of LPA supported theoretically relevant and distinct groups of individuals who had an elevated dysregulation profile. That is, data from the current study supports the existence of the dysregulation group as a latent profile rather than through the use of cutoff scores.
Remarkably, the current study demonstrated that emerging adult males with an elevated dysregulation profile may be more vulnerable than their female counterparts to psychopathological problems, parental psychopathological problems, and poor parent-child relationships (i.e., the significant interactions indicated the combination of elevated dysregulation profile and male gender had particularly pronounced effects). Males may experience more problems related to dysregulation given that they have been shown to have lower levels of emotional awareness in comparison to females (Donahue et al. 2014). Additionally, parents may respond more poorly to males, relative to females, who are dysregulated, thus causing their other more severe problems (e.g., Stearns and McKinney 2019).
Overall, emerging adult males scored significantly higher than females on aggressive problems, attention problems, and effortful control problems (i.e., lower effortful control), whereas females scored significantly higher than males on negative affect and anxiety problems. Consistent with previous research, females appear to be at an increased risk for negative affect and anxiety in comparison to males, who appear to be at an increased risk for aggressive, attention, and effortful control problems, especially when combined with the elevated dysregulation profile. Males may respond differently to their own negative affect than females, which may result in increased physical aggression, ODD problems, and poor emotion regulation overall (Donahue et al. 2014). Males’ utilization of poor emotion regulation strategies in response to their own negative affect may explain why they are more vulnerable than females (Donahue et al. 2014). Moreover, males are more likely to have been socialized to externalize emotional distress, whereas females have been socialized to internalize it (Leaper and Friedman 2007).
Furthermore, differences between dysregulation profiles suggest that some emerging adults continue to experience harsh discipline, controlling parenting, and poor parent-child relationship quality into emerging adulthood (Jucksch et al. 2011; McKinney et al. 2018). Research examining the influence of parenting practices on individuals who are dysregulated has demonstrated mixed results. Few studies have found that parenting practices influence the development or growth of the elevated dysregulation profile over time (McQuillan et al. 2017; Kim et al. 2012). Moreover, the socialization of dysregulation skills is heavily influenced by maltreatment by parents, suggesting that individuals who have experienced harsh discipline and poor relationships with parents may not develop effective emotion regulation strategies (Shipman and Zeman 2001).
Similar to the current study’s findings, previous research also has demonstrated a connection between parental psychopathology and emerging adult psychopathology (Morris et al. 2014; Stearns and McKinney 2018). One question not addressed by the current study is the direction of effect. Parental psychopathology may cause their emerging adult child’s psychopathology, emerging adult psychopathology may cause their parents’ psychopathology, or both. Similarly, individuals with dysregulation may cause parents to use harsh discipline or harsh discipline may cause dysregulation. Previous research has suggested a biological or genetic component to psychopathology within the family, whereas others have suggested that parental psychopathology contributes to inconsistent parenting, child maltreatment and harsh discipline, a lack of emotional support to the child, and poor parent-child relationship quality (McKinney et al. 2018; McQuillan et al. 2017; Voisin et al. 2017). Moreover, parents with psychopathology may socialize their children to utilize poor emotion regulation strategies in times of stress and contribute to stressful home environments that may influence self-regulation skill building (McQuillan et al. 2017).
In comparison to the study by Kim et al. (2012), the current study demonstrated different results across several dimensions that may suggest a temporal shift from pre-school age risks of the elevated dysregulation profile to emerging adulthood risk. Kim et al. (2012) found that individuals in the elevated dysregulation profile group reported higher scores for negative affect and surgency, and lower scores on effortful control than the lower dysregulation profile group. Among emerging adults, the DP-Positive group reported significantly higher scores only on negative affect, and lower scores on effortful control and surgency in comparison to the DP-Negative group. Similar results have been found among adolescents and emerging adults when examining surgency, which may suggest that continued approach behavior may be subdued after interpersonal difficulties which are often associated with individuals who are dysregulated (Wichstrøm et al. 2018). Moreover, paternal psychopathology was not found to be significantly different between groups among preschool age children in the study by Kim et al. (2012). Among emerging adults in the current study, however, paternal psychopathology scores were significantly higher among all subscales analyzed for the DP-Positive group, suggesting a significant difference in reported problems over the lifetime.
Limitations and Strengths
Limitations
The current study was not without limitations. Generalizability is limited by the reliance on a predominantly White college-attending sample. Future studies should endeavor to examine the elevated dysregulation profile and associated risk factors across a more diverse sample (e.g., clinical populations, diverse ethnic and racial backgrounds, a wider range of socioeconomic status, etc.). Although college attending samples are likely higher functioning than some community or clinical samples, research shows that emerging adults are at a higher risk for substance use in college (Gonzalez 2019), higher stress levels (Peer et al. 2015), and rising mental health problems (Auerbach et al. 2018) and has consistently demonstrated that even successful college students demonstrate a range of psychological problems (e.g., Coiro et al. 2017). Our study found consistent patterns of mental health problems as compared to recent studies on college populations (e.g., Auerbach et al. 2018; Bruffaerts et al., 2018). The study utilized emerging adult reports across variables and may be inflated by a shared method bias. Future studies should explore the usage of parent and emerging adult reports of psychological problems, temperament, and parent-child relationship quality to receive a more complete picture of these variables. Similarly, the use of cross-sectional data restricted the implications that could be reasonably gathered regarding the changes among examined variables across age as discussed above. Additionally, many items from the DSM-oriented subscales of the ASR/ABCL overlap with content from the elevated dysregulation profile, although other researchers have made this same comparison (e.g., Kim et al. 2012). Overlapping items on multiple scales may inflate the statistical relationship between the constructs and variables of interest. Future studies should endeavor to examine these relationships without this shared bias.
Strengths
The current study replicated the variables from Kim et al. (2012), generalized the findings to an emerging adult sample, and included gender differences across all variables. Indeed, identifying the interaction for males (i.e., higher scores than females only in the DP-Positive group) suggests that this possible male vulnerability should be further examined.
The study also utilized what appears to be an innovative approach to the elevated dysregulation profile. Previous research has used cut-off values for clinical and non-clinical populations, adding subscale T-scores to determine group membership (Kim et al. 2012; Meyer et al. 2009). The use of an LPA allowed for the discovery of distinct groups that demonstrated large between-group differences and minor within-group differences. Contrary to the summing method used by Kim et al. (2012), the LPA created groups where individuals scored either clinical elevations on all three subscales or scored within the normal range on all three subscales. For example, the summing method may result in inflated scores on the dysregulation profile as a result of an abnormally high score on only one or two of the three subscales (e.g., a T score of 80 on aggressive and attention and T score of 50 on anxious/depressed may result in inclusion of the DP-Positive group even though all three subscales are not elevated), whereas the LPA by the current study suggested a profile clinically elevated as well as a profile in the normal range across all three subscales.
Summary
Previous research has utilized the dysregulation profiles as predictive measures of future psychopathology risk among children (Wang et al. 2017) and the current study extended this research by examining the concurrent risk of psychopathology among emerging adults. Consistent with the current study, Kim et al. (2012) demonstrated significant differences between dysregulation profiles on offspring temperament, psychopathology, parental psychopathology, and parent-child relationships. Results of the current study suggest that emerging adults included in the elevated dysregulation profile exhibited significantly higher psychological and temperamental problems when compared to their counterparts as well as poorer parent-child relationships and maladaptive discipline techniques, consistent with previous research (Althoff et al. 2010; Holtmann et al. 2011). Meta-analyses have shown that dysregulation is fairly stable throughout the lifespan (McQuillan et al. 2017). Individuals who exhibit resistance to control and behavioral issues as children have higher initial scores of dysregulations which then remain stable into adulthood. Thus, children’s temperament may predict poor dysregulation later in life. Additionally, poor social skill development in early childhood may contribute to continued interpersonal difficulties, emotion dysregulation, and impulsivity that lasts into adulthood.
The elevated dysregulation profile may assist researchers in identifying emerging adults who may be experiencing additional risk factors beyond the scales of the ASR DSM subscales as demonstrated in the current study. For example, individuals who match the elevated dysregulation profile were also at a higher risk for experiencing lower social support, difficult temperament, more conflict and harsh discipline from parents, and higher likelihood of parental psychopathology. Future studies should examine the use of the profiles to identify other risk factors for emerging adults, gender differences on these scales and profiles to identify risk profiles, and examine the longitudinal development and maintenance of the profiles into adulthood.
References
Althoff, R. R., Rettew, D. C., Faraone, S. V., Boomsma, D. I., & Hudziak, J. J. (2006). Latent class analysis shows strong heritability of the child behavior checklist-juvenile bipolar phenotype. Biological Psychiatry, 60, 903–911.
Althoff, R. R., Verhulst, F. C., Rettew, D. C., Hudziak, J. J., & van der Ende, J. (2010). Adult outcomes of childhood dysregulation: A 14-year follow-up study. Journal of the American Academy of Child and Adolescent Psychiatry, 49, 1105–1116.
Auerbach, R. P., Mortier, P., Bruffaerts, R., Alonso, J., Benjet, C., Cuijpers, P., et al. (2018). WHO world mental health surveys international college student project: Prevalence and distribution of mental disorders. Journal of Abnormal Psychology, 127(7), 623–638.
Biederman, J., Carter, P. R., Monuteaus, M. C., Evans, M., Parcell, T., Faraone, S. V., et al. (2009). The child behavior checklist-pediatric bipolar disorder profile predicts a subsequent diagnosis of bipolar disorder and associated impairments in ADHD youth growing up: A longitudinal analysis. Journal of Clinical Psychiatry, 70, 732–740.
Bremner, J. D., & Vermetten, E. (2001). Stress and development: Behavioral and biological consequences. Development and Psychopathology, 13, 473–489.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Erlbaum
Coiro, M. J., Bettis, A. H., & Compas, B. E. (2017). College students coping with interpersonal stress: Examining a control-based model of coping. Journal of American College Health, 65(3), 177–186.
Donahue, J. J., Goranson, A. C., McClure, K. S., & van Male, L. M. (2014). Emotion dysregulation, negative affect, and aggression: A moderated, multiple mediator analysis. Personality and Individual Differences, 70, 23–28.
Evans, D. E., & Rothbart, M. K. (2007). Developing a model for adult temperament. Journal of Research in Personality, 41, 868–888.
Deutz, M. H. F., Geeraerts, S. B., Belsky, J., Dekovic, M., Baar, A. L., Prinzie, P., & Patalay, P. (2019). General psychopathology and dysregulation profile in a longitudinal community sample: Stability, antecedents and outcomes. Child Psychiatry and Human Development., 51, 114–126. https://doi.org/10.1007/s10578-019-00916-2.
Franz, A. O., & McKinney, C. (2018). Parental and child psychopathology: Moderated mediation by gender and parent-child relationship quality. Child Psychiatry and Human Development, 49, 843–852.
Furman, W., & Buhrmester, D. (2009). Methods and measures: The network of relationships inventory: Behavioral systems version. International Journal of Behavioral Development, 33, 470–478.
Gelman, A., Carlin, J. B., Stern, H. S., & Rubin, D. B. (2004). Bayesian data analysis (2nd ed.). Boca Raton: Chapman and Hall/CRC.
Gonzalez, V. M. (2019). Factors linking suicidal ideation with drinking to cope and alcohol problems in emerging adult college drinkers. Experimental and Clinical Psychopharmacology, 27(2), 166–177.
Haltigan, J. D., Aitken, M., Skilling, T., Henderson, J., Hawke, L., Battaglia, M., Strauss, J., Szatmari, P., Andrade, B. F., & Andrade, B. (2018). “P” and “DP”: Examining symptom-level bifactor models of psychopathology and dysregulation in clinically referred children and adolescents. Journal of American Academy of Child & Adolescent Psychiatry, 57, 384–396.
Holtmann, M., Buchmann, A. F., Esser, G., Schmidt, M. H., Banaschewski, T., & Laucht, M. (2011). The child behavior checklist-Dysregulation profile predicts substance use, suicidality, and functional impairment: A longitudinal analysis. Journal of Child Psychology and Psychiatry, 52, 139–147.
Jucksch, V., Salbach-Andrae, H., Lenz, K., Goth, K., Döpfner, M., Poustka, F., et al. (2011). Severe affective and behavioral dysregulation is associated with significant psychosocial adversity and impairment. Journal of Child Psychology and Psychiatry, 52, 686–695.
Kim, J., Carlson, G. A., Meyer, S. E., Bufferd, S. J., Doughtery, L. R., Dyson, M. W., Laptook, R. S., Olino, T. M., & Klein, D. N. (2012). Correlates of the CBCL-dysregulation profile in preschool-aged children. The Journal of Child Psychology and Psychiatry, 53, 918–926.
Leaper, C., & Friedman, C. K. (2007). The socialization of gender. In J. H. Grusec & P. D. Hastings (Eds.), Handbook of socialization: Theory and research (pp. 561–587). New York: Guilford Publications.
McGough, J. J., Loo, S. K., McCracken, J. T., Dang, J., Clark, S., Nelson, S. F., & Smalley, S. L. (2008). CBCL pediatric bipolar disorder profile and ADHD: Comorbidity and quantitative trait loci analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1151–1157.
McKinney, C., Brown, K., & Malkin, M. L. (2018). Parenting style, discipline, and parental psychopathology: Gender dyadic interactions in emerging adults. Journal of Child and Family Studies, 27, 290–301.
McKinney, C., & Milone, M. C. (2012). Parental and late adolescent psychopathology: Mothers may provide support when needed most. Child Psychiatry and Human Development, 43, 747–760.
McKinney, C., Stearns, M., & Szkody, E. (2018a). Maltreatment and affective and behavioral problems in emerging adults with and without oppositional defiant disorder symptoms: Mediation by parent-child relationship quality. Journal of Interpersonal Violence., 088626051876001. https://doi.org/10.1177/0886260518760014.
McKinney, C., Stearns, M., & Szkody, E. (2018b). Temperament and oppositional defiant problems in emerging adults: Moderation by parental psychopathology. Manuscript submitted for publication.
McQuillan, M. E., Kultur, E. C., Bates, J. E., O'Reilly, L. M., Dodge, K. A., Lansford, J. E., & Pettit, G. S. (2017). Dysregulation in children: Origins and implications from age 5 to age 28. Development and Psychopathology, 30, 695–713.
Meyer, S. E., Carlson, G. A., Youngstrom, E., Ronsaville, D. S., Martinez, P. E., Gold, P. W., Hakak, R., & Radke-Yarrow, M. (2009). Long-term outcomes of youth who manifested the CBCL pediatric bipolar disorder phenotype during childhood and/or adolescence. Journal of Affective Disorders, 113, 227–235.
Morris, B. H., McGrath, A. C., Goldman, M. S., & Rottenberg, J. (2014). Parental depression confers greater prospective depression risk to females than males in emerging adulthood. Child Psychiatry and Human Development, 45, 78–89.
Muthén, B., & Muthén, L. K. (2000). Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcoholism: Clinical and Experimental Research, 24, 882–891.
Nagin, D. S. (2005). Group-based modeling of development. Cambridge: Harvard University Press.
Peer, J. W., Hillman, S. B., & Van Hoet, E. (2015). The effects of stress on the lives of emerging adult college students: An exploratory analysis. Adultspan Journal, 14(2), 90–99.
Shipman, K. L., & Zeman, J. (2001). Socialization of children's emotion regulation in mother-child dyads: A developmental psychopathology perspective. Development and Psychopathology, 13, 317–336.
Stearns, M., & McKinney, C. (2018). Parent and child antisocial problems: Moderation by emerging adult religiosity and gender. Personality and Individual Differences, 134, 182–189.
Stearns, M., & McKinney, C. (2019). Perceived parental anxiety and depressive problems and emerging adult oppositional defiant problems: Moderated mediation by psychological and physical maltreatment and gender. Family Process. https://doi.org/10.1111/famp.12459.
Steele, E. H., & McKinney, C. (2019). Emerging adult psychological problems and parenting style: Moderation by parent-child relationship quality. Personality and Individual Differences, 146, 201–208.
Voisin, D. R., Harty, J., Kim, D. H., Elsaesser, C., & Takahashi, L. M. (2017). Assessing the relationship between parental influences and wellbeing among low income African American adolescents in Chicago. Child & Youth Care Forum, 46, 223–242.
Volk, H. E., & Todd, R. D. (2007). Does the child behavior checklist juvenile bipolar disorder phenotype identify bipolar disorder? Biological Psychiatry, 62, 115–120.
Walker, C. S. (2018). Parental discipline in emerging adulthood: The creation and validation of the Domains of Young Adult Discipline Scale (DYADS) (doctoral dissertation). Retrieved from Mississippi State University ETD-db. (etd-04062018-084610).
Walker, C. S., & McKinney, C. (2015). Parental and emerging adult psychopathology: Moderated mediation by gender and affect toward parents. Journal of Adolescence, 44, 158–167.
Wang, B., Brueni, L. G., Isensee, C., Meyer, T., Bock, N., Ravens-Sieberer, U., et al. (2017). Predictive value of dysregulation profile trajectories in childhood for symptoms of ADHD, anxiety and depression in late adolescence. European Child & Adolescent Psychiatry, 27, 767–774.
Wichstrøm, L., Penelo, E., Rensvik Viddal, K., Osa, N., & Ezpeleta, L. (2018). Explaining the relationship between temperament and symptoms of psychiatric disorders from preschool to middle childhood: Hybrid fixed and random effects models of Norwegian and Spanish children. Journal of Child Psychology and Psychiatry, 59, 285–295.
Zimmerman, P., & Iwanski, A. (2014). Emotion regulation from early adolescence to emerging adulthood and middle adulthood: Age differences, gender differences, and emotion-specific developmental variations. International Journal of Behavioral Development, 38, 182–194.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All participants were treated according to APA ethical standards. IRB approval was received from Mississippi State University. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare they have no conflicts of interest. No funding was received for this project.
Informed Consent Statement
Informed consent was obtained from every participant in the study in accordance with APA ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Szkody, E., Stearns, M. & McKinney, C. Correlates of the Dysregulation Profile Among Emerging Adults. J Psychopathol Behav Assess 43, 343–354 (2021). https://doi.org/10.1007/s10862-020-09807-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10862-020-09807-6