
Abstract
Research links negative parenting and parental psychopathology to poorer outcomes among youth. Less research examines these effects simultaneously during late adolescence. The current study examines parenting, parental psychopathology, and late adolescent psychopathology as reported by late adolescents (N = 328) with the use of structural equation modeling. Results of measurement models indicate that parental psychopathology and parenting are related to late adolescent psychopathology. However, results of structural models indicate that the effect of parenting on late adolescent psychopathology becomes non-significant in the paternal model and reverses in the maternal model. Interestingly, maternal parenting is associated with higher levels of late adolescent psychopathology, suggesting that mothers provide their late adolescents with more supportive parenting when it is needed most. Overall, results suggest the importance of examining parenting characteristics simultaneously in the context of gender and other variables.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
A great deal of research has been conducted on the relationship between parental psychopathology and youth mental health. The saying “the apple doesn’t fall too far from the tree” appears to hold true after extensive research has been done. Much of the research conducted focuses on maternal psychopathology but more recent studies have incorporated paternal psychopathology as well. These studies have found that paternal psychopathology is related to negative outcomes in youth, suggesting that the negative consequences of parental psychopathology should not be limited to mothers [1]. Previous research also has examined various causes and outcomes of parent and youth psychopathology. These include the parent–child relationship, mediators between parent and youth psychopathology, bidirectional effects, and maternal and paternal differences [2]. However, less research focuses on how these variables extend into late adolescence. Thus, the current study attempts to integrate the research in this area by simultaneously examining the relationships among maternal and paternal psychopathology, maternal and paternal parenting, and late adolescent psychopathology.
Parental Psychopathology
Given that 1 in 5 women and 1 in 10 men will suffer from major depression over the course of their lifetimes [3], current research has grossly studied it and looked at its effect on youth. Although depression has received the most attention, various symptoms and diagnoses of parental psychopathology are predictive of youth maladjustment. For example, research demonstrates that youths whose parents have internalizing problems (i.e., an anxiety, depressive, or mixed anxiety/depressive disorder) are more likely than youth of non-disordered parents to have a disorder themselves [4]. Further, externalizing problems (i.e., antisocial tendencies) in parents have been associated with negative outcomes for youth [5].
Internalizing Problems
Associations between maternal depression and youth outcomes including emotional well-being and behavior problems are well documented [6]. Many studies suggest that rates of depression, ranging from 20 to 41%, are significantly higher in youths with depressed parents relative to youths of non-depressed parents [7]. Additionally, depression in youth of depressed parents relative to depression in same-age youth of non-depressed parents has an earlier age of onset, longer duration, and is associated with greater functional impairment and likelihood of recurrence [7]. Research suggests that depression during pregnancy is likely to expose the fetus to a number of risks for problems in development and that these variables in mothers cause both negative biological and behavioral changes [7, 8]. Additionally, depressed parents are less likely to be as responsive to their children, possibly leading to a sense of rejection and lowered self-esteem in their youth [8]. Overall, children of parents with a depressive disorder are at a greater risk for a range of psychological problems including major depression, anxiety disorders, increased guilt, interpersonal difficulties, and problems with attachment compared to children of parents without a depressive disorder [9–12]. The negative effects of parental depression also have been demonstrated across three generations as children who have a grandparent with major depression are at a greater risk of having psychological problems [13].
Similar to the findings with parental depression, research suggests that parental anxiety also may negatively impact child adjustment. Several studies consistently have documented the relation between parental anxiety and a greater likelihood of anxiety in children [10, 14]. However, research also suggests that having a parent with an anxiety disorder places children at risk for other problematic behaviors including anxious/fearful behaviors, worry, greater difficulties at school, somatic complaints, and social isolation when compared to children whose parents did not have an anxiety disorder [15]. Recent research suggests that parental anxiety also may interfere with the development of both parental and child adaptive coping skills [16]. Since parents with high levels of anxiety tend to perceive challenging/new situations as threatening for their child, they may employ increased parental control to avoid the threatening situation and prevent the youth from facing the new situation or they may model avoidance or rejection as a means of coping [16]. Furthermore, parental anxiety may not only impact their child’s coping ability but may also impact the parent–child relationship as parents with high levels of anxiety tend to show a reduction in the effort that they put into their interactions with their child [17].
Externalizing Problems
Relative to internalizing problems, less research examines parental antisocial tendencies. This lack of research is not because parental antisocial behavior has less deleterious effects on youth adjustment. For example, one study [5] found that maternal depression and paternal antisocial tendencies both are associated independently with depression and conduct disorder in youth. Also, no interaction between the two parental disorders was found, suggesting that youth with either a depressed mother or an antisocial father is at risk for both major depression and conduct disorder. Further, maternal major depression and paternal antisocial tendencies appear to be related to major depression and conduct disorder in youth more so than maternal antisocial tendencies and paternal depression. This study [5] also suggests that when fathers are not included in maternal psychopathology studies, results may overestimate risks associated with having a depressed mother. Other research consistently links parental externalizing problems with a range of childhood problems. For example, research demonstrates that children of parents diagnosed with substance abuse have an increase risk of depressive and anxiety disorders as well as substance abuse/dependence and conduct disorder [12, 14, 18].
Influence of Both Parents
Although mothers influence youth as primary caregivers, maternal and paternal roles are becoming more similar over time and maternal and paternal symptoms of distress are more similar than different in predicting adjustment problems [4]. Whereas some studies find that paternal psychopathology is related to internalizing and externalizing symptoms in children [1], other studies find that paternal depression relates to externalizing behavior problems only [19]. Although a meta-analysis of 134 studies shows that both internalizing and externalizing problems in youth are associated more strongly with depression in mothers than in fathers [7], other research indicates that fathers’ depressive symptoms are associated with youths’ symptoms beyond mothers’ current and prior depression history [1]. For example, research demonstrates that two parents with psychopathology increase the risk of psychopathology in children compared to only one parent with psychopathology [14].
Parenting and Parental Psychopathology
Parenting is one of the most critical tools in raising a child. Styles of parenting have been derived from the dimensions of demandingness and responsiveness [20] and may be described as authoritative, authoritarian, permissive, or neglecting. Parenting that is high in responsiveness and demandingness (i.e., authoritative) appears to be the most beneficial style for youth, as it is related to positive outcomes [20–26]. In contrast, parenting that is low in responsiveness and high in demandingness (i.e., authoritarian), high in responsiveness and low in demandingness (i.e., permissive), or low in responsiveness and demandingness (i.e., neglecting) is related to less positive outcomes for youth [20–26].
Parental psychopathology may hinder parents’ ability to function effectively as parents and prevent their youth from receiving the attention necessary for healthy development. In general, parents’ symptoms of depression, anxiety, and antisocial tendencies are related to more problematic parenting practices (e.g., low warmth, greater disengagement, high control, poor modeling; 3). Parenting practices of mothers and fathers who are disordered also may reflect correlates of their symptoms (e.g., physical and emotional unavailability, unresponsiveness, confusion, self absorption, negative affect, irritability, and over-control; 3) and influence youth to model negative behaviors they observe in their parents who suffer from psychopathology [1]. Further, parental psychopathology may interfere with the ability of an infant to form a secure attachment and an adolescent to form an autonomous identity [6, 27].
Late Adolescent Considerations
Although the role of parenting and parental psychopathology on earlier developmental time periods has received recent attention, less attention has been given to how these factors are related to the functioning of late adolescents. Individuals aged 18–25 years may experience a unique developmental time period termed emerging adulthood [28]. During this period, late adolescents transition from adolescence to adulthood when they leave home for the first time, typically to attend college. This transition destabilizes family members to some extent and may destabilize many in a negative way [29]. Given that late adolescents are transitioning from a more dependent to a more independent relationship with their mothers and fathers, parenting may play an important role in helping late adolescents meet this challenge [29]. In fact, recent research indicates that late adolescents who are attending college away from home continue to rely on their parents and remain under the influence of their parental relationships at least to some extent [21, 23, 24, 30]. Further, the perceptions that late adolescents have of their parents are influential to their adjustment. For example, one study [26] examined youths’ perspectives of parent–child relationships and concluded that the development of internalizing and externalizing behaviors in youth may be dependent upon how they perceive their parents.
Current Study
Overall, much of the past research examines the effects of parental psychopathology and negative parenting separately, whereas more recent research has begun to examine these characteristics together. Although both parental psychopathology and negative parenting have been shown to have direct, negative effects for youth, other research suggests that parental psychopathology is associated strongly with negative parenting. Thus, it may be the case that parental psychopathology leads to negative parenting practices, which, in turn, lead to negative outcomes for youth. Additionally, much of the past research on parental psychopathology focuses on maternal psychopathology alone, whereas more recent research has included paternal psychopathology. However, other potential gender effects are not studied as well. For example, research demonstrates that parent–child dyads (i.e., mother–daughter, mother–son, father–daughter, father–son) experience both similar and dissimilar effects related to the parent–child relationship [23, 24]. Thus, examining parental psychopathology and parenting effects in the context of the gender of both parent and child is paramount. Finally, prior research examines these effects in younger children and adolescents, whereas the current study examines these characteristics in late adolescents/emerging adults.
The current study seeks to address these gaps in the literature by examining the influence of parental psychopathology, parenting practices, and gender effects on late adolescent adjustment. Thus, it is expected that perceived parental psychopathology will be correlated negatively with perceived positive parenting. Furthermore, it is expected that perceived parental psychopathology will be correlated positively while perceived positive parenting will be correlated negatively with late adolescent psychopathology. Furthermore, paternal characteristics are hypothesized to have a weaker but significant effect on late adolescent psychopathology compared to maternal characteristics. Finally, the effects of perceived parental psychopathology on late adolescent psychopathology are expected to be mediated by perceived positive parenting.
Method
Participants
Some exclusion criteria were used to arrive at a final data set. First, participants who did not take adequate time to respond to the survey (i.e., more than two standard deviations below the mean time to respond) were excluded from data analyses. Second, participants who fell outside of the developmental time frame of late adolescents/emerging adulthood (28; i.e., 18–25 years of age) were excluded. Finally, participants who were not able to provide data in regards to their biological father and mother (e.g., reported single- or step-parent households, foster care, etc.) also were excluded. The final sample (N = 328) consisted of 127 males and 201 females attending college in the Southeast United States who ranged in age from 18 to 25 years (M = 19.17, SD = 1.19). Participants identified their race as Caucasian (68%), African–American (26%), Latino (2%), Asian (2%), or Other (2%). Participants predominantly reported a middle-class background as indicated by parental education (12% of parents were reported to have a high school diploma or lower, 19% to have a 2-year degree, 45% to have a 4-year degree, and 24% to have a graduate degree), and family income (9% reported family income of less than $29,999; 64% reported between $30,000 and $100,000; 27% reported greater than $100,000).
Materials
Parental Bonding Instrument (PBI)
The PBI [31] is a 25-item scale designed to measure maternal and paternal caring (opposite being indifference or rejection; e.g., Speaks to me with a warm and friendly voice; alpha = .83 in this study) and overprotection (opposite being autonomy granting; e.g., Invades my privacy; alpha = .79 in this study). Items on these scales are rated on a 4-point Likert scale ranging from Very Like to Very Unlike. Exhibiting good to excellent internal consistency, the PBI has split-half reliability coefficients of .88 for care and .74 for overprotection [31]. Showing good to adequate stability, the PBI has 3-week test–retest correlations of .76 for care and .63 for overprotection [31]. The PBI correlates significantly with independent rater judgments of parental caring and overprotection, demonstrating good concurrent validity [31]. Higher scores on each subscale indicate higher levels of care and overprotection.
Parental Authority Questionnaire (PAQ)
The PAQ [32] contains 30 items regarding maternal and paternal permissive (e.g.,…what children need is to be free to make up their own minds; alpha = .73 in this study), authoritarian (e.g.,…it is for our own good if we are forced to conform to what she/he thinks is right; alpha = .75 in this study), and authoritative (e.g.,…encourages verbal give-and-take; alpha = .84 in this study) parenting. Items are rated on a 5-point Likert scale ranging from Strongly Disagree to Strongly Agree. Test–retest reliabilities range from .77 to .92 and internal consistency reliabilities range from .74 to .87 on the subscales [32]. Demonstrating discriminant validity, authoritarianism is related inversely to permissiveness and authoritativeness, and permissiveness is unrelated to authoritativeness [32]. Criterion-related validity is established, with authoritativeness being related positively, authoritarianism being related negatively, and permissiveness being unrelated to parental nurturance [32]. Higher scores on each subscale indicate higher levels of the parenting style measured.
Parental Environment Questionnaire (PEQ)
The PEQ [33] consists of 42 questions which measure the maternal and paternal parent–child relationship. The PEQ assesses conflict (e.g., My mother/father and I often get into arguments; alpha = .81 in this study), parental involvement (e.g., My mother/father doesn’t know about my hobbies; alpha = .89 in this study), regard for parent (e.g., I am proud of my parent; alpha = .88 in this study), regard for child (e.g., and I know my parent loves me; alpha = .87 in this study), and structure (e.g., My mother/father makes it clear what he/she wants me to do or not do; alpha = .77 in this study). Items are rated on a 4-point Likert scale ranging from Definitely true to Definitely false. The scale has good internal consistency and validity [33]. Higher scores on each subscale indicate higher levels of the measured variable.
Adult Self-Report (ASR) and Adult Behavior Checklist (ABCL)
The ASR [34] consists of 123 items used to assess internalizing and externalizing problems. The ABCL [35] is a parallel form of the ASR used to report on others. Problem behaviors are scored with 0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true. The statements constitute eight syndromes derived by factor analysis. The Withdrawn, Somatic, and Anxious/Depressed scales load on the Internalizing Problems scale. The Rule-Breaking Behavior, Aggressive Behavior, and Intrusive scales load onto the Externalizing Problems scale. Internal consistency alpha ranges from .87 to .93 in past studies [34, 35]. Higher scores on each subscale indicate higher levels of the problem behavior. In this study, the Internalizing (alphas ranged from .87 to .90 in this study) and Externalizing Problems (alphas ranged from = .87 to .91 in this study) scales of the ASR indicated late adolescent psychopathology and the same scales of the ABCL indicated perceived paternal and maternal psychopathology.
Procedure
Upon obtaining IRB approval, an online study was created. Participants seeking extra credit in their psychology courses were able to view the study online and choose to volunteer to participate. All participants who chose to participate finished the study. If they chose to participate, participants first provided informed consent and then completed the questionnaires described above in random order. Participants were instructed to complete questionnaires in regards to their current perceptions and completed questionnaires about their parents in regards to their mothers and fathers separately. Thus, late adolescents’ perceptions of maternal and paternal parenting and psychopathology are assessed as well as their perceptions of their own psychopathology. Participants were treated in accordance to the APA Code of Ethics.
Results
Examination of the subscales on the PBI, PAQ, PEQ, ASR, and ABCL revealed no significant differences for age (all Fs < 1.38, all ps > .22) and ethnicity (all Fs < 1.82, all ps > .13). Although some research indicates differences among Caucasian and African American populations on psychological problems, other research has found no such differences and is consistent with the current study [36].
Latent Constructs and Their Indicators
Structural equation modeling (SEM) analyses were performed using Statistica 9.1. Latent constructs included perceived positive parenting (indicated by the care and overprotection subscales of the PBI; the authoritative, authoritarian, and permissive subscales of the PAQ; and the conflict, involvement, regard for parent, regard for child, and structure scales of the PEQ), perceived parental psychopathology (indicated by the Internalizing and Externalizing subscales of the ABCL), and late adolescent psychopathology (indicated by the Internalizing and Externalizing subscales of the ASR).
Model Analyses
Models including perceived maternal parenting were conducted separately from models including perceived paternal parenting. Model analyses also were completed separately for male and female participants. This was done to examine differences between maternal and paternal parenting as well as between male and female late adolescents, particularly given that extant research demonstrates gender effects across parents and youths [21, 23, 24, 30, 37, 38]. Thus, four models (i.e., father–son, father–daughter, mother–son, mother–daughter) were examined.
In testing for son and daughter differences in paternal and maternal models, a multigroup analysis was conducted. First, the measurement model was established for sons in the father–son and mother–son models. Second, the factor loadings for the father–daughter and mother–daughter models were constrained to be equal to the factor loadings in the father–son and mother–son models, respectively. According to a Chi-square difference test, constraining the factor loadings to be equal for both sons and daughters in the paternal and maternal models did not significantly decrease model fit compared to a model in which factor loadings were free to vary for both groups. Thus, measurement invariance was demonstrated and allowed for direct across group comparisons [39]. Given that no significant differences were found between father–son and father–daughter models as well as between mother–son and mother–daughter models (i.e., path coefficients in son and daughter models did not significantly differ from each other), paternal and maternal models combining son and daughter participants are presented below.
For the purposes of SEM, a sample size of 328 is considered good [40]. The generalized least squares to maximum likelihood (GLS-ML) method of covariance structure analysis was used. Overall model fit was examined with the root mean square error of approximation (RMSEA), the comparative fit index (CFI), and the parsimonious fit index (PFI). RMSEA values less than or equal to .08 and CFI values greater than or equal to .95 have been used to indicate acceptable model fit [41]. PFI values greater than or equal to .60 signify that a model is sufficiently parsimonious [42]. Chi-square tests were not used to assess overall model fit due to their sensitivity to sample size and other biases [42]. Similar to other research, a two-stage modeling approach was taken [43, 44]. First, a measurement model that allows latent constructs to correlate freely was evaluated. Next, a structural model designed to test relationships among latent constructs was conducted. This approach decreases the possibility that relationships among latent constructs will be misinterpreted due to poor construct measurement [44].
Measurement and Structural Models
The original measurement models as described above failed to adequately fit the data (all RMSEA >.08, all CFI <.95), suggesting the need for respecification. The need to respecify is common as “initially specified measurement models almost invariably fail to provide acceptable fit” (43, p. 412). Examination of the standardized residuals associated with each model revealed several indicators that did not relate clearly to a latent construct. As a result, these indicators were deleted from future analyses. The respecified measurement models, shown in Fig. 1, adequately fit the data as indicated by the RMSEA (all <.08), CFI (all >.95), and PFI (all >.60). All factor loadings exceeded .60 (all ps < .0005), indicating convergent validity. Upon specifying appropriate measurement models, the hypothesized structural models were tested. Structural models adequately fit the data as indicated by the RMSEA (all <.08), CFI (all >.95), and PFI (all >.60). Correlations among the latent constructs are shown in Fig. 1, and model statistics for respecified measurement models and hypothesized structural models are shown in Table 1. Figure 2 displays the structural models with path coefficients.

Respecified measurement models. Standardized factor loadings (all ps < .0005) appear along horizontal arrows and correlations among latent constructs (all ps < .0005) appear along curved arrows. Values appear to the left for paternal models and to the right for maternal models. Measurement errors are omitted for clarity

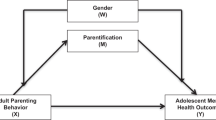
Fitted structural models. Standardized parameter estimates (all ps < .0005 unless noted as NS) appear to the left for paternal models and to the right for maternal models. Error effects are omitted for clarity
Hypotheses Revisited
Correlations among latent factors in the measurement models shown in Fig. 1 are examined first. The hypothesis that perceived parental psychopathology will be correlated negatively with perceived positive parenting is supported across both paternal and maternal models. Perceived parental psychopathology is associated negatively with perceived positive parenting in father-late adolescent (r = −62, p < .0005) and mother-late adolescent (r = −69, p < .0005) dyads. The hypothesis that perceived parental psychopathology will be correlated positively and perceived positive parenting will be correlated negatively with late adolescent psychopathology also is supported. Perceived parental psychopathology is associated positively with late adolescent psychopathology (r = .81, p < .0005 for the paternal model; r = .84, p < .0005 for the maternal model) and perceived positive parenting is associated negatively with late adolescent psychopathology (r = −.53, p < .0005 for both models). In fact, perceived parental psychopathology is correlated very strongly with late adolescent psychopathology. Overall, correlational results suggest that higher levels of parental psychopathology are associated with higher levels of late adolescent psychopathology and lower levels of perceived positive parenting, which also is associated with higher levels of late adolescent psychopathology.
Path coefficients among latent factors in the structural models shown in Fig. 2 are examined second. The hypothesis that paternal influences will be weaker than maternal influences but still significant is not supported. Specifically, both perceived paternal and maternal psychopathology share a similar path with late adolescent psychopathology (path coefficient = .83, p < .0005 for the paternal model; path coefficient = .87, p < .0005 for the maternal model) and perceived paternal positive parenting is not a significant predictor of late adolescent psychopathology. The hypothesis that perceived positive parenting will mediate the effects of perceived parental psychopathology on late adolescent psychopathology was tested using nested model comparisons. First, both the predictor construct and mediator construct must relate independently to the predicted variable to test for mediation. Establishing this criteria, models testing the direct relationship between perceived parental psychopathology and late adolescent psychopathology as well as models testing the direct relationship between perceived positive parenting and late adolescent psychopathology adequately fit the data. Second, a nested model where the expected mediated path (i.e., the path between perceived parental psychopathology and late adolescent psychopathology) was set to zero was compared to an exact model where the expected mediated path was allowed to vary. If the model with the path set to zero does not demonstrate a significant decrease in fit according to a Chi-square difference test, then full mediation is demonstrated.
Failing to support this hypothesis, the nested models where the expected mediated path was set to zero did not fit the data as well as the models where the expected mediated path was allowed to vary. The path coefficients between perceived parental psychopathology and late adolescent psychopathology remain significant and are largely the same as the relationships found in the measurement model. Instead, the effects of perceived positive parenting are altered when examined with structural models. Specifically, the relationship between perceived positive paternal parenting and late adolescent psychopathology found in the measurement model is brought to nil in the paternal structural model, and the same relationship changes from negative to positive in the maternal structural model. This suggests that perceived parental psychopathology maintains a strong relationship with late adolescent psychopathology as well as perceived positive parenting when examined simultaneously with structural models but that the effects of perceived positive parenting are removed for fathers and reversed for mothers.
Discussion
This study examines the relationships among perceived paternal and maternal parenting, perceived paternal and maternal psychopathology, and late adolescent psychopathology as reported by late adolescents. Consistent with prior research (e.g., 3, 4, 6, 7, 20, 23, 24, 25, 26, 27), results of measurement models suggest that positive parenting is associated with positive psychological adjustment in late adolescents. Further, parental psychopathology is associated with less effective parenting and poorer psychological adjustment in late adolescents. Adding to the extant literature, results of structural models suggest that the effects of perceived paternal parenting are eliminated and the effects of perceived maternal parenting are reversed on late adolescent psychopathology when examined with perceived parental psychopathology.
The finding that perceived parenting did not mediate the effects of perceived parental psychopathology is counter to some research (e.g., 8). Instead, the current study finds that perceived parenting is the variable that changes when examined in the context of perceived parental psychopathology. Specifically, it appears that perceived paternal psychopathology accounts for the correlation between perceived paternal parenting and late adolescent psychopathology. Further, the reversal in the effect of perceived maternal psychopathology on late adolescent psychopathology is noteworthy. Although this finding appears counterintuitive, other research finds similar effects. Specifically, one study [45] indicates that mothers may influence their youth most strongly with support compared to fathers who rely more on autonomy granting. Further, youth who experience situations that evoke psychopathology receive more of this positive parenting from mothers. Another explanation for this finding may be that perceived positive parenting increases the likelihood of late adolescent psychopathology in the context of high perceived parental psychopathology. That is, children may identify more strongly and be more involved with parents who provide positive parenting. This higher level of identification and involvement may lead to a stronger transmission of parental psychopathology.
The elimination of the effect of perceived paternal positive parenting and reversal of perceived maternal positive parenting on late adolescent psychopathology also indicates the importance of examining parenting characteristics and youth adjustment simultaneously in the context of other variables. Without the simultaneous examination of these variables, it may have been concluded that increases in perceived positive parenting were associated with decreases in late adolescent psychopathology as found with correlations in both the paternal and maternal measurement models, a finding that is drastically different when examined with structural models. Finally, the differences found in the paths between perceived paternal and maternal positive parenting on late adolescent psychopathology emphasizes the importance of examining parenting characteristics in the context of gender.
Implications for Research and Practice
The results presented in this study hold implications for researchers. Given the differences related to gender noted above, the current study lends further evidence that the relationships among various parenting characteristics and late adolescent adjustment must be examined in the context of the gender. Although many similarities exist across gender-dyadic models, important differences also exist. Thus, examining parenting as a global variable may not best explain the intricacies of parenting. Future research also is encouraged to explore the relationship between parenting and psychopathology further. Specifically, understanding more about how parents may respond to problems experienced by their youth (e.g., a mother providing more support to her troubled youth) is important. It may be the case that effective parents provide more and less support at appropriate times, whereas ineffective parents do not. Additionally, research should examine how this targeted parental support specifically influences outcomes in youth. Finally, researchers are encouraged to examine characteristics related to outcomes in youth in the context of other variables. Certain relationships examined in isolation may not exist or change when examined simultaneously with other characteristics.
Individuals interacting with youth (e.g., mental health professionals, parents, teachers) also may use the findings reported. For example, working with parents to increase effective parenting practices (e.g., encourage warmth and demandingness, resolve conflict) may potentially lead to positive effects on late adolescents’ psychological adjustment. Further, it may be the case that healthy parents promote healthy youth, so improving parental mental health may lead to improvements in both parenting practices and youth adjustment. Individuals interacting with youth also should understand the potentially subtle differences between how fathers and mothers may parent their youth. Finally, prior research examines the role of parental psychopathology in infants (e.g., 45) and early to middle adolescence (e.g., 8). The current study extends this research into late adolescence or emerging adulthood and suggests that childhood experiences may continue to influence late adolescent and emerging adult development.
Limitations
The findings of this study must be viewed in the context of its limitations. One limitation may be the generalizability of the findings. The sample consisted of traditional-aged college students who were predominately Caucasian and African American and reported a predominantly middle-class background. Further, only participants who reported on a biological father and mother were included. Thus, it is recommended that future studies explore various ethnic, socioeconomic, and family backgrounds under more rigorous methodological conditions. Another limitation of this study is that it relied on the self-report of late adolescents. Although perceptions that youth hold of their parents are influential [26], what late adolescents experience and recall may differ from what mothers and fathers recall, all of which may differ from what actually happens. Although self-report may be subject to bias, one study [46] notes that it is a valid method for gathering information about parenting practices from emerging adults and is related to their outcomes. This study even argues that emerging adult perceptions may be more accurate than a child’s perceptions as the emerging adult is “freer to speak their minds than are children… [because they] are no longer constrained by their parents’ control” (46, p. 65). Further, developers of the ABCL note that the individuals who are familiar with the person they are rating provide reliable and valid perceptions [35]. Another limitation of this study is its design. Correlational in nature, this study is unable to determine causation. Further, participants reported on their own psychopathology as well as their parents’ psychopathology, leading to the possibility that the relationships among constructs may be due to a shared method effect and partly contributing to the high correlations between parental and late adolescent psychopathology. Finally, many other factors not studied here may influence late adolescent outcomes.
Summary
Although parenting effects on child and adolescent adjustment have been studied extensively, less research has examined parenting effects in the context of gender and late adolescence. Further, research has examined the effects of parental psychopathology on children and early to middle adolescence, but less research has investigated these effects in late adolescence. Consistent with past research, perceived paternal and maternal psychopathology are related to late adolescent psychopathology. Adding to the extant research, perceived positive paternal parenting is not associated significantly with late adolescent psychopathology, whereas perceived positive maternal parenting is associated with increases in late adolescent psychopathology. This suggests that mothers provide more support to their youth when they need it most. Additionally, given the differences across the paternal and maternal models, the importance of exploring the effects of parent and late adolescent gender is demonstrated.
References
Kane P, Garber J (2008) Parental depression and child externalizing and internalizing symptoms: unique effects of fathers’ symptoms and perceived conflict as a mediator. J Child Fam Stud 18:465–472
Cortes R, Fleming C, Catalano R, Brown E (2006) Gender differences in the association between maternal depressed mood and child depressive phenomena from grade 3 through grade 10. J Youth Adolesc 35:815–826
Middleton M, Scott S, Renk K (2009) Parental depression, parenting behaviors, and behavior problems in young children. Infant Child Dev 18:323–336
Papp L, Cummings E, Goeke-Morey M (2005) Parental psychological distress, parent-child relationship qualities, and child adjustment: Direct, mediating, and reciprocal pathways. Parent Sci Pract 5:259–283
Marmorstein N, Malone S, Iacono W (2004) Psychiatric disorders among offspring of depressed mothers: Associations with paternal psychopathology. Am J Psychiatry 161:1588–1594
Gross H, Shaw D, Burwell R, Nagin D (2009) Transactional processes in child disruptive behavior and maternal depression: a longitudinal study from early childhood to adolescence. Dev Psychopathol 21:139–156
Goodman S (2007) Depression in mothers. Annu Rev Clin Psychol 3:107–135
Elgar FJ, Mills RSL, McGrath PJ, Waschbusch DA, Brownridge DA (2007) Maternal and paternal depressive symptoms and child maladjustment: the mediating role of parental behavior. J Abnorm Child Psychol 35:943–955
Beardslee WR, Versage EM, Gladstone TRG (1998) Children of affectively ill parents: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry 37:1134–1141
Mufson L, Weissman MM, Warner V (1992) Depression and anxiety in parents and children: a direct interview study. J Anxiety Disord 6:1–13
Nomura Y, Wickramaratne PJ, Warner V, Mufson L, Weissman MM (2002) Family discord, parental depression and psychopathology in offspring: ten-year follow-up. J Am Acad Child Adolesc Psychiatry 41:402–409
Warner V, Mufson L, Weissman MM (1995) Offspring at high and low risk for depression and anxiety: mechanisms of psychiatric disorder. J Am Acad Child Adolesc Psychiatry 34:786–797
Warner V, Weissman MM, Mufson L, Wickramaratne PJ (1999) Grandparents, parents, and grandchildren at high risk for depression: a three-generation study. J Am Acad Child Adolesc Psychiatry 38:289–296
Merikangas KR, Dierker LC, Szamari P (1998) Psychopathology among offspring of parents with substance abuse and/or anxiety disorders. A high risk study. J Child Psychol Psychiatry 39:711–720
Turner SM, Beidel DC, Costello A (1987) Psychopathology in the offspring of anxiety disorders patients. J Consult Clin Psychol 55:229–235
van der Bruggen CO, Stams GJJM, Bögels SM (2008) Research review: the relation between child and parent anxiety and parental control: a meta-analytic review. J Child Psychol Psychiatry 49:1257–1269
Edwards S, Rapee R, Kennedy S (2010) Prediction of anxiety symptoms in preschool-aged children: examination of maternal and paternal perspectives. J Child Psychol Psychiatry 51:313–321
Chassin L, Pitts SC, DeLucia C, Todd M (1999) A longitudinal study of children of alcoholics: predicting young adult substance use disorders, anxiety, and depression. J Abnorm Psychol 108:106–119
Brennan P, Hammen C, Katz A, Le Brocque R (2002) Maternal depression, paternal psychopathology, and adolescent diagnostic outcomes. J Consult Clin Psychol 70:1075–1085
Baumrind D (1991) Effective parenting during the early adolescent transition. In: Cowan PA (ed) Family transitions. Lawrence Erlbaum Associates, Hillsdale, NJ, pp 111–163
McKinney C, Milone M, Renk K (2011) Parenting and late adolescent emotional adjustment: mediating effects of discipline and gender. Child Psychiatry Hum Dev 42:463–481
McKinney C, Renk K (2011) A multivariate model of parent-adolescent relationship variables in early adolescence. Child Psychiatry Hum Dev 42:442–462
McKinney C, Renk K (2008) Differential parenting between mothers and fathers: implications for late adolescents. J Fam Issues 29:806–827
McKinney C, Renk K (2008) Multivariate models of parent-late adolescent gender dyads: the importance of underlying processes in predicting emotional adjustment. Child Psychiatry Hum Dev 39:147–170
Paulussen-Hoogeboom MC, Stams GJJM, Hermanns JMA, Peetsma TTD, Wittenboer GLH (2008) Parenting style as a mediator between children’s negative emotionality and problematic behavior in early childhood. J Genet Psychol 169:209–226
Yahav R (2006) The relationship between children’s and adolescents’ perceptions of parenting style and internal and external symptoms. Child Care Health Dev 33:460–471
Wan M, Green J (2009) The impact of maternal psychopathology on child–mother attachment. Arch Womens Ment Health 12:123–134
Arnett JJ (2000) Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol 55:469–480
Hardie D (1999) The transition from late adolescence to young adulthood: student life. In: Hindle D, Smith MV (eds) Personality development: a psychoanalytic perspective. Taylor and Frances/Routledge, Florence, KY, pp 158–174
McKinney C, Donnelly R, Renk K (2008) Perceived parenting, positive and negative perceptions of parents, and late adolescent emotional adjustment. Child Adolesc Ment Health 13:66–73
Parker G, Tupling H, Brown LB (1979) A parental bonding instrument. Br J Med Psychol 52:1–10
Buri JR (1991) Parental authority questionnaire. J Pers Assess 57:110–119
Elkins I, McGue M, Iacono W (1997) Genetic and environmental influences on parent son relationships: evidence for increasing genetic influence during adolescence. Dev Psychol 33:351–363
Rescorla LA, Achenbach TM (2004) The Achenbach system of empirically based assessment (ASEBA) for ages 18 to 90 years. The use of psychological testing for treatment planning and outcomes assessment: Volume 3: Instruments for adults, 3rd ed. Lawrence Erlbaum Associates, Mahwah, NJ, pp 115–152
Achenbach TM, Rescorla LA (2003) Manual for the ASEBA adult forms and profiles. University of Vermont, Research Center for Children, Youth, and Families, Burlington, VT
McLaughlin KA, Hilt LM, Nolan-Hoeksema S (2007) Racial/ethnic differences in internalizing and externalizing symptoms in adolescents. J Abnorm Child Psychol 35:801–816
Gryczkowski MR, Jordan SS, Mercer SH (2010) Differential relations between mothers’ and fathers’ parenting practices and child externalizing behavior. J Child Fam Stud 19:539–546
Phares V, Fields S, Kamboukos D (2009) Fathers’ and mothers’ involvement with their adolescents. J Child Fam Stud 18:1–9
Vanderberg RJ, Lance CE (2000) A review and synthesis of the measurement invariance literature: suggestions, practices, and recommendations for organizational research. Organ Res Methods 3:4–70
Kline RB (1998) Principles and practice of structural equation modeling. The Guilford Press, New York, NY
Hu L, Bentler PM (1999) Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model 6:1–55
James LR, Mulaik SS, Brett JM (1982) Causal analysis: assumptions, models, and data. Sage Publications, Beverly Hills, CA
Anderson JC, Gerbing DW (1988) Structural equations modeling in practice: a review and recommended two-step approach. Psychol Bull 103:411–423
Barry B, Stewart GL (1997) Composition, process, and performance in self-managed groups: the role of personality. J Appl Psychol 82:62–78
van der Bruggen CO, Stams GJJM, Bögels SM, Paulussen-Hoogeboom MC (2010) Parenting behavior as a mediator between young children’s negative emotionality and their anxiety/depression. Infant Child Dev 19:354–365
Finley GE, Mira SD, Schwartz SJ (2008) Perceived paternal and maternal involvement: factor structures, mean differences, and parental roles. Fathering 6:62–68
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McKinney, C., Milone, M.C. Parental and Late Adolescent Psychopathology: Mothers May Provide Support When Needed Most. Child Psychiatry Hum Dev 43, 747–760 (2012). https://doi.org/10.1007/s10578-012-0293-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-012-0293-2