
Abstract
We conducted in-depth case studies of 10 health care professionals who actively provide primary medical care to adults with autism spectrum disorders. The study sought to understand their experiences in providing this care, the training they had received, the training they lack and their suggestions for encouraging more physicians to provide this care. Qualitative data were gathered by phone using a structured interview guide and analyzed using the framework approach. Challenges to providing care were identified at the systems, practice and provider, and education and training levels. Solutions and interventions targeting needed changes at each level were also proposed. The findings have implications for health care reform, medical school and residency training programs, and the development of best practices.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A new set of patients is seeking entrance to the adult health care system in growing numbers. Among the overall increase in the size of the population of children and youth with disabilities, the fastest growing subgroup between 1997 and 2008 was individuals with autism spectrum disorders (ASD) (Boyle et al. 2011). The timing of this trend coupled with the rising rate of diagnosis of ASD and the escalating use of health and related services associated with ASD has put pressure on providers of health care to adults to find ways to accommodate and care for individuals with ASD (Piven and Rabins 2011). The current medical workforce is not prepared to care for this influx of adults with ASD (McDougle 2013).
Gaining access to the health care system has long been problematic for youth, young adults, and adults with disabilities. Barriers to care include the lack of insurance or adequate coverage, accessible medical facilities, and trained providers (Iezzoni 2011; National Council on Disability 2009). Access to health care for individuals with disabilities particularly drops off in the transition from pediatric to adult care (Cooley 2013; Lotstein et al. 2008, 2010; Shattuck et al. 2011). One reason is the limited availability of physicians willing to accept youth with disabilities who are transitioned (American Academy of Pediatrics et al. 2011). Studies examining the shortage of providers caring for adults with disabilities point to inadequate education about various conditions and their associated disease processes as well as inadequate training in how to provide clinical care and counseling to these patients (Bruder et al. 2012; Patel and O’Hare 2010; Peter et al. 2009; Wilkinson et al. 2012). The lack of training is associated with an expressed discomfort in caring for patients with disabilities and chronic conditions and a need for greater exposure to and experience with these individuals (Okumura et al. 2008; Patel and O’Hare 2010; Wilkinson et al. 2012).
With more individuals with disabilities reaching adulthood and the persistent problem of connecting adolescents with disabilities to accessible and high quality health care (McManus et al. 2013), it is critical to study those health care professionals who do provide care to adults with disabilities. The purpose of this study is to better understand how these providers became interested in serving individuals with disabilities, their training, the challenges they face, and their ideas for growing the number of physicians who offer this care.
This study focused specifically on providers who care for adults with ASD. The focus on ASD acknowledges the general lack of research on adults with ASD (Bruder et al. 2012; Mandell 2013; Piven and Rabins 2011). This is problematic given that individuals with ASD will receive the majority of their health care as adults (Ganz 2007). It is also useful to understand the perspectives of providers who care for adults with ASD because this is a patient group whose characteristics make providing health care difficult. Youth and young adults with ASD are likely to need specialized care for common co-morbidities such as anxiety and depression, epilepsy, gastrointestinal problems, anxiety and depression, and respiratory, food, and skin allergies (American Academy of Pediatrics et al. 2011; Canitano et al. 2005; Gurney et al. 2006; Molloy and Manning-Courtney 2003). Also compounding the health care challenges for many youth and adults with ASD are their unusual sensory responses to some environmental stimuli as well as their often increased anxiety associated with entering new and highly stimulating environments (Aylott 2010; Ghaziuddin et al. 2002). Similarly, hypersensitivity to touch among individuals with ASD presents challenges to health care providers during examinations and diagnostic testing (Shea and Mesibov 2005; Williams 2003).
Methods
Design
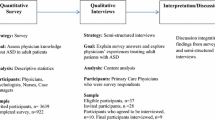
The study was designed as an in-depth case study of 10 health care professionals (9 physicians and one nurse) who are active providers of primary medical care to adults with ASD. In case study research, Yin (2009) stresses the importance of using a structured interview guide to increase the study’s validity and reliability by approaching data collection for each case in the same way. Thus, an interview guide was created that asked specified questions regarding (1) site characteristics; (2) provider experience and background with ASD; (3) practice environment and provision of care details; (4) care coordination; and (5) interactions with other medical providers including recommendations for increasing the number of adult providers willing to care for adults with ASD. The full interview guide is available from the authors.
Sampling and Recruitment of Participants
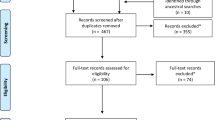
Participants were identified using purposive sampling techniques. First, recruitment efforts began by contacting sites within the Autism Treatment Network (ATN). The ATN is a network of ASD treatment centers in the United States and Canada designed “to create and develop the most effective approach to medical care for children and adolescents affected by autism” (Autism Speaks, 2013). As part of a previous project, the study team had recently been in contact with the leading pediatricians and site coordinators at 13 of these centers. Phone calls and emails to these providers and ATN personnel described the current study and asked them to identify physicians who actively provide care to adults with ASD. A total of 14 physicians were identified. All of these physicians were then contacted by email and phone to inform them of the study and ask for their participation. A total of 8 (57 %) physicians participated in the in-depth interviews through this recruitment process.
Second, additional participants were identified through the New England Index, a searchable, online registry of physicians throughout New England (http://www.disabilityinfo.org/). All physicians on the New England Index who met two criteria were selected: (1) identified themselves as a family practitioner or internist; and (2) indicated that they cared for patients with ASD and/or Asperger’s Syndrome. This search yielded 9 providers, one of whom had already been interviewed for this study. None of the providers were from the same medical practice. Of the remaining 8 physicians, 3 (37.5 %) agreed to participate. One of the three interviews was not used in the data analysis, however, as the physician reported working most often with infants and children. Thus, the final sample included a total of 10 providers. Table 1 presents descriptive information on the final sample.
Data Collection
Data were collected through phone interviews using the interview guide described above. Each participant was sent the guide prior to the call. Each interview was approximately 45 minutes long and was audio-recorded upon obtaining verbal consent from each respondent. Each participant was paid an honorarium for his or her participation. The work was approved by the Institutional Review Boards (IRB) at the Massachusetts General Hospital and Brandeis University.
Data Analysis
Data from the 10 providers were analyzed using the framework approach (Ritchie and Spencer 1994; Smith and Firth 2011). This technique has been used to analyze qualitative data derived from research of health care practices and policies (Smith and Firth 2011).
The framework approach has many similarities to thematic analysis (Boyatzis 1989) but emphasizes transparency in data analysis through three inter-connected stages that require the research team to explicitly describe the processes that guide the systematic analysis from initial data management to the development of descriptive accounts and then explanatory accounts (Smith and Firth 2011; Ritchie and Lewis 2003). In the first stage, data management, one member of the research team read the transcripts several times. Detailed notes were taken of each respondent’s answers to the questions to manage the volume of information gathered. During this stage as well as subsequent stages, a set of themes were identified using the respondents own words (“in vivo” codes) as a means of staying true to the data (Ritchie and Lewis 2003).
The initial themes derived during the data management stage are listed in Table 2.
In the second stage, descriptive accounts, a second researcher reviewed the transcripts several times prior to reviewing the themes listed in Table 2 and then refined the initial categories. The second researcher found instances of overlap between themes and instances where themes could be merged to better represent the data. For example, themes underlining the difficulties encountered when providing care were embedded within the responses to multiple sections as were themes about training and education needs. Overall, three primary themes emerged: (1) challenges in providing care; (2) training and education needs; and (3) solutions to address care challenges. Next, to ensure rigor, both researchers independently coded the data into the three primary themes, discussed discrepancies, and reached consensus on two final categories; (1) challenges to providing care and (2) solutions and interventions.
In the third stage, explanatory accounts, the task is to examine the data further to identify associations or patterns within or across categories. The two researchers again analyzed the data within each of the final two categories and determined that each could be coded into three subcategories: systems level; practice/provision level, and training and education level. Each researcher then independently coded the data from the final two categories into the three subcategories, discussed discrepancies, and reached consensus.
Results
Challenges to providing care at the systems level, practice or provision level, and for training and education are presented first. Next, the solutions and interventions suggested at each level are described.
Challenges to Providing Care
Systems Level
Providers described several challenges including a shortage of medical and non-medical services and supports for youth and adults with ASD, a general lack of providers willing to work with adults with ASD, and financial disincentives for providers to include adults with ASD in their practice due to the related issues of time, reimbursement, and the need for additional staff.
The shortage of services and supports focused on both contrasting the experiences of different age groups and on the shortage of specific types of non-medical services. One provider noted “Although there aren’t enough services for and supports for children and adolescents with intellectual and developmental disabilities, when they age out of those services into adult services, almost everywhere there’s significantly less.” Specific shortages for adults were described in areas such as meaningful day activities and social skills training.
The lack of health care professionals available to provide care was described as universal; “The fundamental issues of finding someone who has knowledge and skills and unfortunately attitudes to appropriately look after people, in my limited experience, is no different in Canada, in Ontario, than it is in Tennessee.” The small community of physicians experienced in caring for adults with ASD was described as a close group; “You know many of the people personally, because you’ve seen them repeatedly at conferences.”
Related to the lack of professionals are the financial disincentives to provide care to adults with ASD. These disincentives are tied to the extra time it takes to care for an adult with ASD, the need to connect with other providers and utilize additional staff, and the lack of reimbursement for that time and support which results in lost revenue. One physician focused on the time issue; “The health system…is set up for the general population and the timelines are very limited. And that’s a huge barrier, because clients with ASD or any developmental disability, they take much longer to assess.” Another physician linked the additional time directly to lost revenue; “Because they take more time and the more time you spend with a patient the less money you’re making. Especially someone who has severe autism and who may be non-verbal and may have a guardian, you can’t do a 10–15 minute visit. You need a half hour visit. And that’s lost revenue” Time is also an issue outside of the office visit; “Last night I was on the phone for an hour with a therapist with a particularly difficult patient with an ASD trying to talk about what all the issues are.” The need to support other staff such as a case manager and social worker to provide care was also mentioned. These challenges all come to a head because of the lack of reimbursement; “Gosh how do I even tell you how much time I spend with this. It’s a problem, that’s why nobody wants to see people. It’s not compensated.”
Practice/Provision Level
Challenges identified at the practice/provision level also included the issue of time constraints but were focused on how to most efficiently organize patient care. Organizational difficulties included scheduling blocks of time for the visit, monitoring the amount of time patients spend in the waiting room, and designating time outside the visit for completing necessary paperwork. One physician noted that scheduling has to involve “timing in terms of when is the best time to see that client and, or when are they more difficult to assess?”
Other challenges at the service provision level include the complexity of family involvement, the physical environment not being appropriately designed and barriers to communicating with patients during the visit. One physician described the complexity of family member participation by saying, “Well, they (patients with ASD) are much more likely, almost 100 % likely to have someone with them. Which is different. You know, most adults tend to come to the doctors by themselves. Or at least if they bring someone with them the other person really isn’t participating in the visit. So right away you have two patients. You have the patient and then you have the patient’s significant others. So that’s very different. And that’s something that a lot of internists aren’t used to.”
The physical environment was also mentioned as another layer of complexity. One provider said, “I have a couple of patients that can’t—when I was on the second floor couldn’t come in. They won’t do elevators or stairs… and I had to see them in their cars.” The need for adaptations to the physical space was also described. One provider said, “To be able to get that client there to that kind of environment where, you know, sensory wise it’s very overloading. Even for someone in the general population, to go into a hospital it can be stressful. So for someone who has a lot of anxiety related to ASD to go into that environment and not have modifications, because the system just doesn’t have the ability to have a quiet room where they can be assessed. That’s a huge barrier.”
The waiting room environment presents some challenges both in terms of how adults with ASD behave in the waiting room in general and how they behave in relation to other patients. One provider recalled a conversation with a practice colleague who said, “I appreciate that you’re trying to help these patients, but you know, your patient socked my female patient in the face.” The provider continued by saying, “I had another one with autism who was very low-functioning who urinated on the seat and one of my partner’s patients came in, didn’t realize it, and sat in it.”
Finally, communication challenges arise in the conduct of the visit, which can influence what the provider learns about the patient’s condition and the subsequent care provided. One provider said, “You know, figuring out, especially if it’s your first time with someone, figuring out are they verbal, do they make eye contact, do they want you to make eye contact, are they using an I-pad or other communication device? Do they use non-verbal communication? Establishing communication. Figuring out how they express pain or discomfort is different.” Others suggested that the lack of communication often requires some creative problem solving. One provider said, “A good example is a young adult, a woman in her mid-twenties that we have who is non-verbal, and for a couple of years of having very significant head banging. And actually the person who was taking care of her right before me after 2 years finally figured out hey, wait a minute. What are her periods like? And they started pre-medding her with Motrin right before her menstrual periods, and the head banging went away.”
Training and Education Level
Finally, at the training and education level, respondents specified that the most critical issues are the lack of formal education or training provided to physicians during medical school and residency and their lack of knowledge around working with individuals with ASD. These deficits make providers feel less confident in working with this population. One respondent said, “There was virtually no education or supervised experience for me during my residency (family medicine); and although that’s a little bit better today, it still is far from being where it needs to be.”
Many respondents claimed to have learned about this population through personal experience or through self-directed internships and conferences. One respondent stated, “I didn’t find a lot in the way of formal programs. I ended up working with people one-on-one actually; found a mentor who was great to connect me to specific people who are doing projects or who could teach me things. So it was more of a one-to-one basis on my own initiative.” Another physician explained, “I never, ever, ever heard of anything (related to training). If you’re interested in it, you just say I’m interested in it. I have a reasonably good training background in cognitive and behavioral neurology. There’s certainly nothing official and as far as I know; nothing unofficial either. It’s still trial by fire.” Overall, the respondents identified a serious need for formal education and training regarding caring for adults with ASD.
Solutions and Interventions
Findings within the category of solutions and interventions were also dispersed between the systems level, practice/provision level and training and education level.
Systems Level
Respondents provided ideas for addressing the capacity problems and the financial disincentives that they had identified as system level challenges. Providers mentioned creating incentives to increase provider capacity; “It’s really getting into things to incentivize adult providers to do this and to make their lives easier as well. If it’s seen as an additional burden with no additional benefits then no one would do it.” The need for specific resources was also discussed. One provider said, “I think, you know courses for guardianship, as a particular issue—internists don’t know anything about medical guardianship. Or the practical things like what are SSI, and what does it mean to be dual eligible if you have a severe medical condition. Housing issues, kind of the practical matters. Not so much the medical things.” Another provider honed in on structural issues; “I think the other things—sort of big picture—are getting the assistance out there to providers so short of having true sub-specialty clinics that specialize in taking care of these patients. I think we’re in the process of getting care coordinators and things like that.”
Eliminating or reducing the financial disincentives related to reimbursement and insurance were also raised as important. As mentioned by one physician, “I think that a lot of the changes that I would think would be most helpful would be on the policy level… reimbursing for the time that it takes to care for people who are more complex, maybe even reimbursing for the time it takes to talk with their patient’s pediatrician.” Another physician stated, “It’s not a question of refusing to take care of this patient population it’s a question of refusing or not accepting this insurance. So it’s an insurance driven issue more than anything else.”
Practice/Provision Level
Respondents also suggested practice/provision level solutions including creating a customized or localized list of inclusive supports, services, resources, and communication techniques. One physician noted, “Even having a couple of ideas, or a couple lists of resources that you can give to patients is very helpful.”
A second office-based strategy was to review patient lists on a daily basis to prioritize patients with ASD and help lessen their wait time. One provider emphasized, “The most important thing is to try to create a comfortable environment to move things along more efficiently; it makes a big difference that folks don’t have to wait because they don’t always understand why they’re waiting.” A related suggestion was to enhance the physical office space. One provider described how anticipating a visit can help; “You know a lot of people with autism are very noise sensitive, or light sensitive, or phobic of crowds. So what’s your waiting room set up like? How big is it? How loud is it? If you know someone is coming with autism can you arrange for them to immediately be taken into a smaller room?”
Finally, facilitating communication between physicians was suggested. One provider said; “Having the family doctor, after receiving the client, find out who the pediatrician was and spend a bit of time connecting with that pediatrician. Then, I think that would help.”
Training and Education Level
At the training and education level, suggestions focused on both providers and office staff. Suggestions for increasing the awareness of the needs and rewards of caring for adults with ASD included connecting physicians to existing programs and services. One respondent said; “I think exposure to students, and not just medical students, is a great thing. You know, Special Olympics is a wonderful model, a great way to do that. Best Buddies is a good way to do that. And then, for people that are training and in clinical disciplines, and I can really only talk about medicine, but a little bit of experience with some other clinical disciplines, it will always impress me that just being exposed to a positive experience had a number of people coming back. You know, I guess the context for this was often a mandatory day or half-day or something.”
Training for physicians also needs to set the expectation that, given the population trends, they will encounter these patients. One provider described it this way; “You know, a lot of times they say I’m not interested because I’m not going to treat people on this spectrum and I say to them well if you’re going into private practice, you are going to treat people on the spectrum. So you may think you’re not, but they’re going to show up in your office because somebody referred them for a bipolar disorder or something else. So I really contend that if you’re in private practice you’re going to treat people and you need to have formal training.”
Suggestions for training physicians also focused on the need to provide education to individuals early in their careers, either in medical school or in residency. One respondent supported this approach; “I think one way is to work on the individuals who are training to be physicians, particularly primary care doctors, to try to do—get some of these patients into those practices so that they gain exposure and interest. I think it’s a little harder to reintroduce these patients to much older physicians who are sort of set in their ways.”
Finally, two other physicians suggested that in some ways, patients with ASD are not as different from other medically complex patients, indicating that training might include taking lessons from caring for medically complex patients and applying them to individuals with ASD.
In addition to training for physicians, training for office staff was also emphasized as important and in-line with the practice and provision level challenges and solutions reported previously. One provider described how trained staff can make a huge difference in the success of an office visit by an individual with ASD. The provider said; “from the minute the person makes their first contact with the practice—or the guardian does—that could set up good things or that could set up disaster. So step one is training for staff on privacy issues and working with families. Rather than assuming that the patient can tell you everything they need to know. So staff training’s important. And then once they get to the visit, training staff about different communication techniques. You know how to respond to fears, to behavioral difference. So that training is important.”
Discussion
The number of adults with ASD who need medical care from physicians trained to care for adults is rapidly increasing. Given the dearth of providers ready to assume the care of this growing population, we sought to better understand the experiences and perspectives of health care professionals who do care for adults with ASD. Our in-depth interviews identified challenges in providing care at the systems level, practice and provision level, and education and training level. Respondents also described solutions and interventions that they felt would address these challenges.
Taken together, the findings indicate that changes coming under health care reform could support provider’s efforts to address the needs of adults with ASD. The findings also have implications for medical school and residency training programs and the development of best practices.
Although many provisions within the Affordable Care Act may have implications for supporting physicians who provide care to adults with ASD, specific changes related to the integration of physical and mental health care, the redesign of primary care to operationalize the medical home for adults, and the reformulation of reimbursements have been identified as most pertinent (American Academy of Pediatrics et al. 2011; Mandell 2013; Rosenthal 2008). In the medical home, responsibility for care and care coordination resides with the patient’s personal primary care provider working with a health care team created to meet the patient’s evolving needs. The health care team may include specialists, nurses, social workers, care managers, dietitians, pharmacists, physical and occupational therapists, family members, and community service providers (Barr 2006). Studies of medical home models have found that their success depends on how well they focus on the individual’s needs and their ability to access social services and specialty medical services to solve problems as they arise (Rosenthal 2008).
Implementing the medical home will also require changes in reimbursement policy (Rosenthal 2008). It is estimated that 40 % of the work done by a primary care provider (e.g., arranging referrals, completing forms, communicating with patients) is not reimbursed in a fee-for-service model (Gottschalk and Flocke 2005). Thus, within a medical home system, a revised and likely complicated payment formula would need to take account of the number of team members involved, the health information technology used, email and telephone consultation time, and the complexity of the patient’s needs among other factors (Landon et al. 2007). The payment formula must also provide incentives for practices to invest in staff, electronic records, and building connections with community agencies as well as incentives to care for more complex patients (Campbell et al. 2008; McDonald et al. 2007; McDougle 2013). Studies suggest that more complex patients have more to gain under a medical home model (Snyder and Neubauer 2007). Despite the promise of these changes, however, needed payment reforms have not materialized (American Academy of Pediatrics et al. 2011).
Beyond health reform, the study’s findings have implications for medical school and residency training programs. Several studies have found that providing specific training to medical students as well as opportunities for them to encounter patients with disabilities yields benefits in terms of improving student’s attitudes and comfort level regarding people with disabilities and increasing their knowledge and skills in providing care to these patients (Brown et al. 2010; Karl et al. 2013; Long-Bellil et al. 2011). Few medical schools or residency programs currently offer these kinds of training experiences although this has begun to change (Graham et al. 2009; Moroz et al. 2010; Symons et al. 2009) and research is being conducted to better assess the efficacy of these efforts (Symons et al. 2012; Lam et al. 2010). Rather than simply adding a single lecture to an existing course, however, medical schools and residency programs must integrate into their curricula required courses and clinical rotations focused on individuals with ASD across the lifespan (McDougle 2013). Internet-based sharing and coordination of the materials created to educate medical students and residents could speed the expansion of these training efforts. Continuing education for practicing physicians has also been identified as an important need (Bruder et al. 2012).
Another set of findings from the study focused on both the challenges of providing health care to adults with ASD within general practice settings as well as the strategies for successfully providing individualized care. The suggestions offered and used by the study’s respondents represent current best practices. More research is needed to evaluate these strategies as well as internet-based methods for sharing them.
Health reforms to be instituted under the Affordable Care Act offer opportunities to incorporate new procedures that could substantially improve health care provision to adults with ASD. Expanding training for medical students and residents around caring for this population and further development of best practices could increase the likelihood that the reforms will be implemented and the health improvements realized.
References
American Academy of Pediatrics, American Academy of Family Physicians, & American College of Physicians, Transitions Clinical Report Authoring Group. (2011). Clinical report—Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics, 128(1), 182–200.
Autism Speaks Inc. (2013). What is the ATN? http://www.autismspeaks.org/science/resources-programs/autism-treatment-network/what-atn. Accessed 20 July 2013.
Aylott, J. (2010). Improving access to health and social care for people with autism. Nursing Standard, 24(27), 47–56.
Barr, M. (2006). The advanced medical home: A patient-centered, physician-guided model of health care. Philadelphia, PA: American College of Physicians.
Boyatzis, R. E. (1989). Transforming qualitative information: Thematic analysis and code development. Thousand Oaks, CA: Sage Publications Inc.
Boyle, C. A., Boulet, S., Schieve, L. A., Cohen, R. A., Blumberg, S. J., Yeargin-Allsopp, M., et al. (2011). Trends in the prevalence of developmental disabilities in U.S. children, 1997–2008. Pediatrics, 127(6), 1034–1042.
Brown, R., Graham, C. L., Richeson, N., Wu, J., & McDermott, S. (2010). Evaluation of medical student performance on objective structured clinical exams with standardized patients with and without disabilities. Academic Medicine, 85(11), 1766–1771.
Bruder, M. B., Kerins, G., Mazzarella, C., Sims, J., & Stein, N. (2012). Brief report: The medical care of adults with autism spectrum disorders: Identifying the needs. Journal of Autism and Developmental Disorders, 42, 2498–2504.
Campbell, S. M., McDonald, R., & Lester, H. (2008). The experience of pay for performance in English family practice: A qualitative study. The Annals of Family Medicine, 6, 228–234.
Canitano, R., Luchetti, A., & Zappella, M. (2005). Epilepsy, electroencephalographic abnormalities, and regression in children with autism. Journal of Child Neurology, 20(1), 27–31.
Cooley, W. C. (2013). Adolescent health care transition in transition. JAMA Pediatrics, 167(10), 897–899.
Ganz, M. (2007). The lifetime distribution of the incremental societal costs of autism. Archives of Pediatric and Adolescent Medicine, 161(4), 343–349.
Ghaziuddin, M., Ghaziuddin, N., & Greden, J. (2002). Depression in persons with autism: Implications for research and clinical care. Journal of Autism and Developmental Disorders, 32(4), 299–306.
Gottschalk, A., & Flocke, S. A. (2005). Time spent in face-to-face patient care and work outside the examination room. The Annals of Family Medicine, 3, 488–493.
Graham, C. L., Brown, R. S., Zhen, H., & McDermott, S. (2009). Teaching medical students about disability in family medicine. Family Medicine, 41(8), 542–544.
Gurney, J. G., McPheeters, M. L., & Davis, M. M. (2006). Parental report of health conditions and health care use among children with and without autism: National survey of children’s health. Archives of Pediatric & Adolescent Medicine, 160(8), 825–830.
Iezzoni, L. I. (2011). Eliminating health and health care disparities among the growing population of people with disabilities. Health Affairs, 20(10), 1947–1954.
Karl, R., McGuigan, D., Withiam-Leitch, M. L., Akl, E. A., & Symons, A. B. (2013). Reflective impressions of a precepted clinical experience caring for people with disabilities. Intellectual and Developmental Disabilities, 51(4), 237–245.
Lam, W. Y., Gunukula, S. K., McGuigan, D., Isaiah, N., Symons, A. B., & Akl, E. A. (2010). Validated instruments used to measure attitudes of healthcare students and professionals towards patients with physical disability: A systematic review. Journal of Neuroengineering and Rehabilitation, 7, 55–61.
Landon, B. E., Schneider, E. C., & Normand, S. T. (2007). Quality of care in Medicaid managed care and commercial health plans. Journal of the American Medical Association, 298, 1674–1681.
Long-Bellil, L., Robey, K. L., Graham, C. L., Minihan, P. M., Smeltzer, S., & Kahn, P. (2011). Teaching medical students about disability: The use of standardized patients. Academic Medicine, 86(9), 1163–1170.
Lotstein, D. S., Inkelas, M., Hays, R. D., Halfon, N., & Brook, R. (2008). Access to care for youth with special health care needs in the transition to adulthood. Journal of Adolescent Health, 43(1), 23–29.
Lotstein, D. S., Kuo, A. A., Strickland, B., & Tait, F. (2010). The transition to adult health care for youth with special health care needs: Do racial and ethnic disparities exist? Pediatrics, 126, S129–S136.
Mandell, D. S. (2013). Adults with autism: A new minority. Journal of General Internal Medicine, 28(6), 751–752.
McDonald, R., Harrison, S., Checkland, K., & Campbell, S. M. (2007). Impact of financial incentives on clinical autonomy and internal motivation in primary care: Ethnographic study. BMJ, 334, 1357–1359.
McDougle, C. J. (2013). Sounding a wake-up call: Improving the lives of adults with autism. Journal of the American Academy of Child and Adolescent Psychiatry, 52(6), 566–568.
McManus, M. A., Pollack, L. R., Cooley, W. C., McAllister, J. W., Lotstein, D., Strickland, B., & Mann, M. Y. (2013). Current status of transition preparation among youth with special needs in the United States. Pediatrics, 131(6), 1090–1097.
Molloy, C. A., & Manning-Courtney, P. (2003). Prevalence of chronic gastrointestinal symptoms in children with autism and autistic spectrum disorders. Autism., 7(2), 165–171.
Moroz, A., Gonzalez-Ramos, G., Festinger, T., Langer, K., Zefferinoi, S., & Kalet, A. (2010). Immediate and follow-up effects of a brief disability curriculum on disability knowledge and attitudes of PM&R residents: A comparison group trial. Medical Teacher, 32, e360–e364.
National Council on Disability. (2009). The current state of health care for people with disabilities. Washington, DC: National Council on Disability.
Okumura, M. J., Heisler, M., Davis, M. M., Cabana, M. D., Demonner, S., & Kerr, E. A. (2008). Comfort of general internists and general pediatricians in providing care for young adults with chronic illnesses of childhood. Journal of General Internal Medicine, 23(10), 1621–1627.
Patel, M. S., & O’Hare, K. (2010). Residency training in transition of youth with childhood-onset chronic disease. Pediatrics, 126(Supplement 3), 190–193.
Peter, N. G., Forke, C. M., Ginsburg, K. R., & Schwarz, D. F. (2009). Transition from pediatric to adult care: Internists’ perspectives. Pediatrics, 123(2), 417–423.
Piven, J., & Rabins, P. (2011). Autism spectrum disorders in older adults: Toward defining a research agenda. Journal of the American Geriatrics Society, 59(11), 2151–2155.
Ritchie, J., & Lewis, J. (Eds.). (2003). Qualitative research practice: A guide for social science students and researchers. London: Sage.
Ritchie, J., & Spencer, L. (1994). Qualitative data analysis for applied policy research. In A. Bryman & R. Burgess (Eds.), Analyzing qualitative data (pp. 173–194). London: Routledge.
Rosenthal, T. C. (2008). The medical home: Growing evidence to support a new approach to primary care. Journal of the American Board of Family Medicine, 21(5), 427–440.
Shattuck, P. T., Wagner, M., Narendorf, S., Sterzing, P., & Hensley, M. (2011). Post-high school service use among young adults with an autism spectrum disorder. Archives of Pediatric and Adolescent Medicine, 165(2), 141–146.
Shea, V., & Mesibov, G. B. (2005). Adolescents and adults with autism. In F. R. Volkmar, R. Paul, A. Klin, & D. Cohen (Eds.), Handbook of autism and pervasive developmental disorders, vol 1: Diagnosis, development, neurobiology, and behavior (3rd ed., pp. 288–311). Hoboken: Wiley.
Smith, J., & Firth, J. (2011). Qualitative data analysis: The framework approach. Nurse Researcher, 18(2), 52–62.
Snyder, L., & Neubauer, R. L. (2007). Pay-for-performance principles that promote patient-centered care: An ethics manifesto. The Annals of Internal Medicine, 147, 792–794.
Symons, A. B., Fish, R., McGuigan, D., Fox, J., & Akl, E. A. (2012). Development of an instrument to measure medical students’ attitudes toward people with disabilities. Intellectual and Developmental Disabilities, 50(3), 251–260.
Symons, A. B., McGuigan, D., & Akl, E. A. (2009). A curriculum to teach medical students to care for people with disabilities: Development and initial implementation. BMC Medical Education, 9, 78–84.
Wilkinson, J., Dreyfus, D., Cerreto, M., & Bokhour, B. (2012). ‘‘Sometimes I feel overwhelmed’’: Educational needs of family physicians caring for people with intellectual disability. Intellectual and Developmental Disabilities, 50(3), 243–250.
Williams, D. (2003). Exposure anxiety—The invisible cage: An exploration of self-protection responses in the autism spectrum and beyond. London: Jessica Kingsley Publishers.
Yin, R. K. (2009). Case study research: Design and methods (4th ed.). Thousand Oaks, CA: Sage.
Acknowledgments
This project was supported with funding from a Grant, R40 MC 19925 through the U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Research Program. We thank the providers who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Warfield, M.E., Crossman, M.K., Delahaye, J. et al. Physician Perspectives on Providing Primary Medical Care to Adults with Autism Spectrum Disorders (ASD). J Autism Dev Disord 45, 2209–2217 (2015). https://doi.org/10.1007/s10803-015-2386-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-015-2386-9